Jonas' Introduction to the U.S. Health Care System [9th Revised] 0826174027, 9780826174024
This revised ninth edition of the best-selling introductory text to the U.S. health care system is fully updated to refl
225 12 15MB
English Pages 350 [415] Year 2020
Cover
Title
Copyright
Contents
Preface
Reference
Acknowledgments
List of Abbreviations
Part I: U.S. Health Care System: Present State
1. Introduction
Learning Objectives
Health and Health Care
The Population Served
U.S. Health Care System
References
Further Reading
2. The Settings for Health Care Delivery
Learning Objectives
Introduction
Community-Based Care
Hospitals: Inpatient Acute Care
Postacute Care
References
Further Reading
3. The People Who Provide Health Care
Learning Objectives
Introduction
Health Care Occupations, Overall
Physicians
Nurses
Physician Assistants
Other Health Care Occupations
Primary Care and Its Providers
References
Further Reading
4. Medicines, Devices, and Technology
Learning Objectives
Introduction
Pharmaceuticals
Medical Devices
Other Medical Devices
References
5. Government and the Health Care System
Learning Objectives
The Constitutional Basis of Governmental Authority in Health Care
The Health Care Functions of Government
The Federal Government’s Role in Health Care
State Government’s Role in Health Care
Local Government’s Role in Health Care
References
Further Reading
6. Financing the Health Care System
Learning Objectives
Introduction
How Much is Spent?
Where the Money Goes
Insurance, Intermediaries, and Other Third Parties
Where the Money Comes from Within the System
Prices
References
Further Reading
7. Health Care System Performance
Learning Objectives
Introduction
Health Care Quality
Equity in Health Care
Health Care Efficiency
A National Scorecard
Data and Information Technology
References
Further Reading
Part II: U.S. Health Care System in Transition: How We Got Here and Where We Are Going
8. Debates That Have Structured Health Care System Change
Learning Objectives
Introduction
Ideology and the Health Care System
A Mixed Health Care System
Making Policy and Bringing Change
U.S. Health Care System Compared to Peer Countries
Framework for Analyzing Health Care Policy
References
Further Reading
Appendix
9. History of Change from 1900 to 2010: Incrementalism
Learning Objectives
Introduction
Access to Health Care
Organization and Financing of Health Care
References
Further Reading
10. History of Change from 1900 to 2010: Comprehensive Reform
Learning Objectives
Introduction
National Health Insurance
Comprehensive Health Care Reform Under the Clinton Administration
References
Further Reading
11. The Affordable Care Act: Achievements, Limitations, and Opposition
Learning Objectives
Introduction
Health Care Reform Under the Obama Administration
“Repeal and Replace” Efforts by Republicans
References
Further Reading
12. Trends in the U.S. Health Care System
Learning Objectives
Current State of U.S. Health Policy
U.S. Health Care System Trends
Zigzag or a Private System?
References
Further Reading
Index
Recommend Papers
![Jonas' Introduction to the U.S. Health Care System [9th Revised]
0826174027, 9780826174024](https://ebin.pub/img/200x200/jonas-introduction-to-the-us-health-care-system-9th-revised-0826174027-9780826174024-k-5787921.jpg)
![Introduction to US Health Policy: The Organization, Financing, and Delivery of Health Care in America [5 ed.]
1421446464, 9781421446462](https://ebin.pub/img/200x200/introduction-to-us-health-policy-the-organization-financing-and-delivery-of-health-care-in-america-5nbsped-1421446464-9781421446462.jpg)


![Introduction to Health Care [4 ed.]
9781305574779](https://ebin.pub/img/200x200/introduction-to-health-care-4nbsped-9781305574779.jpg)
![Introduction to Health Care [5 ed.]
9780357123072, 9780357123164, 2019912555](https://ebin.pub/img/200x200/introduction-to-health-care-5nbsped-9780357123072-9780357123164-2019912555.jpg)


![The Patient and Health Care System: Perspectives on High-Quality Care [1st ed.]
9783030465667, 9783030465674](https://ebin.pub/img/200x200/the-patient-and-health-care-system-perspectives-on-high-quality-care-1st-ed-9783030465667-9783030465674.jpg)
![Jonas' Introduction to the U.S. Health Care System [9th Revised]
0826174027, 9780826174024](https://ebin.pub/img/200x200/jonas-introduction-to-the-us-health-care-system-9th-revised-0826174027-9780826174024.jpg)
File loading please wait...
Citation preview
Jonas’ Introduction to the U.S. Health Care System
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd i
3/20/20 2:49 PM
Raymond L. Goldsteen, DrPH, MA, is Professor Emeritus of Preventive Medicine at Stony Brook University School of Medicine. He was founding director of the MPH Program and professor of Population Health in the School of Medicine and Health Sciences, University of North Dakota. He was also founding director of the Graduate Program in Public Health and professor of Preventive Medicine in the School of Medicine at Stony Brook University. Dr. Goldsteen has an extensive background in health care and was formerly a director of the health policy research centers at the University of Illinois in Urbana-Champaign, University of Oklahoma College of Public Health, and the West Virginia University School of Medicine. He is a coauthor of Introduction to Public Health, now in its second edition, and many peerreviewed publications in health and health care. Karen Goldsteen, PhD, MPH, is an Affiliated Public Health Faculty member in the Program in Public Health at Stony Brook University. Prior to this, she was a research associate professor of Population Health in the MPH Program, School of Medicine and Health Sciences, at the University of North Dakota. She was also a research associate professor of Health Technology and Management in the Graduate Program in Public Health at Stony Brook University. She was awarded her MPH degree from Columbia University School of Public Health and her PhD in Community Health from the University of Illinois at Urbana-Champaign. She was a Pew Health Policy Fellow at the University of California, San Francisco. Dr. Goldsteen is a coauthor of Introduction to Public Health, now in its second edition, and many peer-reviewed publications on health and health care. Benjamin Z. Goldsteen, MBA, earned his master’s degree from Columbia University in New York. He has 20 years of experience as an innovator in health care and life sciences organizations. While working at one of the largest consulting firms in the world, he led multiple strategy and performance-improvement engagements for health care clients across the United States from assessment through implementation. He is highly knowledgeable about all aspects of health care delivery and the policies that impact the health care system. He currently serves as Chief Analytics Officer of a division dedicated to driving transformation across the largest municipal health care system in the United States.
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd ii
3/20/20 2:49 PM
Jonas’ Introduction to the U.S. Health Care System Ninth Edition Raymond L. Goldsteen, DrPH, MA Karen Goldsteen, PhD, MPH Benjamin Z. Goldsteen, MBA
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd iii
3/20/20 2:49 PM
Copyright © 2021 Springer Publishing Company, LLC All rights reserved. First Springer Publishing edition 1982 No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior permission of Springer Publishing Company, LLC, or authorization through payment of the appropriate fees to the Copyright Clearance Center, Inc., 222 Rosewood Drive, Danvers, MA 01923, 978-750-8400, fax 978-646-8600, [email protected] or on the Web at www.copyright.com. Springer Publishing Company, LLC 11 West 42nd Street, New York, NY 10036 www.springerpub.com connect.springerpub.com/ Acquisitions Editor: David D’Addona Compositor: S4Carlisle Publishing Services ISBN: 978-0-8261-7402-4 ebook ISBN: 978-0-8261-7404-8 DOI: 10.1891/9780826174048 Qualified instructors may request supplements by emailing [email protected] Instructor’s Manual: 978-0-8261-7405-5 PowerPoints: 978-0-8261-7408-6 Test Bank: 978-0-8261-7407-9 eChapter: The ACA in 2020: An Update: 978-0-8261-7412-3 20 21 22 23/ 5 4 3 2 1 The author and the publisher of this Work have made every effort to use sources believed to be reliable to provide information that is accurate and compatible with the standards generally accepted at the time of publication. The author and publisher shall not be liable for any special, consequential, or exemplary damages resulting, in whole or in part, from the readers’ use of, or reliance on, the information contained in this book. The publisher has no responsibility for the persistence or accuracy of URLs for external or third-party Internet websites referred to in this publication and does not guarantee that any content on such websites is, or will remain, accurate or appropriate. Library of Congress Cataloging-in-Publication Data Names: Goldsteen, Raymond L., author. | Goldsteen, Karen, author. | Goldsteen, Benjamin Z., author. Title: Jonas’ introduction to the U.S. health care system / Raymond L. Goldsteen, Karen Goldsteen, Benjamin Z. Goldsteen. Other titles: Introduction to the U.S. health care system Description: Ninth edition. | New York : Springer Publishing Company, LLC, 2021. | Includes bibliographical references and index. Identifiers: LCCN 2020005922 (print) | LCCN 2020005923 (ebook) | ISBN 9780826174024 (paperback) | ISBN 9780826174048 (ebook) | ISBN 9780826174055 (instructor’s manual) | ISBN 9780826174086 (powerpoints) | ISBN 9780826174079 (test bank) Subjects: MESH: Delivery of Health Care | Health Services Administration | Insurance, Health | Health Policy | Health Services–trends | United States Classification: LCC RA395.A3 (print) | LCC RA395.A3 (ebook) | NLM W 84 AA1 | DDC 362.10973–dc23 LC record available at https://lccn.loc.gov/2020005922 LC ebook record available at https://lccn.loc.gov/2020005923
Contact us to receive discount rates on bulk purchases. We can also customize our books to meet your needs. For more information please contact: [email protected]
Publisher’s Note: New and used products purchased from third-party sellers are not guaranteed for quality, authenticity, or access to any included digital components.
Printed in the United States of America.
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd iv
3/20/20 2:49 PM
This book is dedicated to children and grandchildren everywhere, in the hope that they will have access to quality health care in their future.
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd v
3/20/20 2:49 PM
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd vi
3/20/20 2:49 PM
Contents Preface xiii Acknowledgments xvii List of Abbreviations xix
PART I. U.S. HEALTH CARE SYSTEM: PRESENT STATE 1.
Introduction 3 Learning Objectives 3 Health and Health Care
5
What Is Health? 5 Determinants of Health What Is Health Care?
The Population Served
1
6 9
10
Mortality 10 Morbidity 13 Health Behavior 14 Other Issues Affecting Need for Health Care
U.S. Health Care System
14
18
Health Care Facilities 19 Health Care Workforce 19 Medical Products 19 Leadership and Governance 20 Health Care Financing 22 Health Care System Performance and Information Technology Types of Health Services Provided 23
22
Summary 25 Data Sources 25 Study Questions 26 Note 26 References 27 Further Reading 30 2.
The Settings for Health Care Delivery Learning Objectives 33 Introduction 33
33
Vertical and Horizontal Integration in Health Care
Community-Based Care Self-Care 35 Ambulatory Care
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd vii
34
35 36
3/20/20 2:49 PM
viii
Contents
Hospitals: Inpatient Acute Care Historical Background Community Hospitals
Postacute Care
53
53 57
65
Long-Term Care
66
Summary 70 Data Sources 70 Study Questions 71 Notes 71 References 72 Further Reading 77 3.
The People Who Provide Health Care Learning Objectives 79 Introduction 80 Health Care Occupations, Overall 81
79
Wages for Health Care Occupations 82 Practice Settings of Health Care Workers 84 Demographic Characteristics of Health Care Workers Complexity of the Health Care Workforce 86
Physicians
87
Historical Background 87 Medical Education 88 Medical Practice 90 Physician Supply 95 Physician Workforce Projections
Nurses
84
95
99
Historical Background 99 Nursing Education 102 Nursing Practice 104 From Nursing Shortage to Nursing Oversupply, and Back Again
Physician Assistants 108 Other Health Care Occupations Primary Care and Its Providers
106
109 109
Functions 111 Historical Background 112 Primary Care Workforce 113 Primary Care and the Health Care Delivery System
113
Summary 114 Data Sources 114 Study Questions 115 Notes 116 References 116 Further Reading 123 4.
Medicines, Devices, and Technology Learning Objectives 125 Introduction 126 Pharmaceuticals 126
125
Regulatory Process 127 Who Decides, Who Pays 131 Drug Research, Development, and Manufacturing 132 Small Number of Large Companies, Large Number of Small Companies
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd viii
134
3/20/20 2:49 PM
Contents
Medical Devices
ix
135
Regulatory Process 135 Who Decides, Who Pays 138 Company/Market Structure 140
Other Medical Devices Summary 142 Data Sources 142 Study Questions 142 References 143 5.
141
Government and the Health Care System 149 Learning Objectives 149 The Constitutional Basis of Governmental Authority In Health Care 150 The Health Care Functions of Government 151 The Legislative Branch 151 The Judiciary 152 The Executive Branch 152 Provision of Personal Health Services 152 Provision of Community Health Services 152 Health Care Financing 153
The Federal Government’s Role in Health Care Department of Health and Human Services Other Federal Departments 158
State Government’s Role in Health Care Health Statistics Licensing 161
153 153
161
161
Local Government’s Role in Health Care Public Health Contributions
162
163
Summary 163 Data Sources 164 Note 164 Study Questions 164 References 165 Further Reading 166 6.
Financing the Health Care System Learning Objectives 169 Introduction 170
169
Source of Information About Health Care Financing
How Much Is Spent? 171 Where the Money Goes 175 Insurance, Intermediaries, and Other Third Parties
170
181
Matching Different Provider and Patient Payment Approaches Maintaining a Network of Providers 188 Price and Provider Expertise 188 Provider Payment Approaches 189 Risk Transfer and Good Intentions 192
Where the Money Comes From Within the System
184
193
Private Health Insurance (or Managed Care) 194 Self-Pay and Out-of-Pocket Expenditures 197 Government Spending on Health Care 198
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd ix
3/20/20 2:49 PM
x
Contents
Prices 204 Summary 205 Data Sources 205 Study Questions 206 Notes 206 References 207 Further Reading 212 7.
215
Health Care System Performance Learning Objectives 215 Introduction 216 Health Care Quality 217
Population Health Outcomes 218 Clinical (or Healthcare-Associated) Outcomes 222 Organizations With Major Influence on Health Care Quality 226 Health Care-Associated Infections: An Example of Health Care Quality Improvement 238
Equity in Health Care
246
Equity in Health Care Quality and Access Before the Affordable Care Act Equity in Health Care Quality and Access After the ACA 248
Health Care Efficiency
246
249
Microlevel Health Care Efficiency Macrolevel Health Care Efficiency
A National Scorecard 252 Data and Information Technology
250 250
253
Where Are the Health Data? 254 Health Information Exchange: The HIT Dream 257 Barriers to Achieving the HIT Dream 258 A Health Information Example: National Healthcare Safety Network
259
Summary 261 Data Sources 262 Study Questions 263 References 263 Further Reading 269
PART II. U.S. HEALTH CARE SYSTEM IN TRANSITION: HOW WE GOT HERE AND WHERE WE ARE GOING 273 8.
Debates That Have Structured Health Care System Change Learning Objectives 275 Introduction 276 Ideology and the Health Care System 278 Health Care as a Public Good 278 Health Care as a Private Good 279 Health Care: Public or Private Enterprise?
A Mixed Health Care System
280
281
Historical Roots 281 Pragmatism 282 Preference for Checks and Balances Mixed-Enterprise Trade-Offs 283
Making Policy and Bringing Change Future of the Mixed Enterprise
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd x
275
283
283 284
3/20/20 2:49 PM
Contents
U.S. Health Care System Compared to Peer Countries Framework for Analyzing Health Care Policy 286
xi
285
What Information Is Needed to Understand Specific Health Policy Proposals 286 Context of Health Care Policy Debates 287 Factors Affecting How a Health Care System Is Organized to Achieve Equity, Efficiency, and Quality 287 How Preference for Private or Public Involvement Impacts the U.S. Health Care System 287 How Economic Principles Apply to Health Care Economics in the United States 288
Summary 289 Data Sources 290 Study Questions 292 Note 292 References 292 Further Reading 293 Appendix 294 9.
History of Change From 1900 to 2010: Incrementalism Learning Objectives 297 Introduction 298 Access to Health Care 298 Providing Health Insurance Building Hospitals 302
297
299
Organization and Financing of Health Care
303
Expansion of Capitation and the Rise of Managed Care 303 Growth of Vertical and Horizontal Integration of Health Care Organizations Increase in For-Profit Health Care Organizations 310
308
Summary 311 Data Sources 311 Study Questions 313 References 314 Further Reading 316 10.
History of Change From 1900 to 2010: Comprehensive Reform Learning Objectives 319 Introduction 319 National Health Insurance 320 NHI: World Historical Background 320 NHI in the United States 321 NHI by Contract, or the Personal Health Care System
325
Comprehensive Health Care Reform Under the Clinton Administration Political Context of the Health Security Act 326 Introduction of the Health Security Act 326 The Health Security Act Plan 327 Opposition to the Health Security Act 328 After Defeat of the Health Security Act: 1994 to 2010
319
325
329
Summary 331 Data Sources 331 Study Questions 333 Notes 334 References 334 Further Reading 340
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xi
3/20/20 2:49 PM
xii
Contents
11.
341
The Affordable Care Act: Achievements, Limitations, and Opposition Learning Objectives 341 Introduction 342 Health Care Reform Under the Obama Administration 342 Problems That Motivated Change 342 How the Obama Administration Planned to Achieve Its Goals 346 How the ACA Was Financed 348 Supreme Court Challenges to the ACA During the Obama Administration Status of the ACA at the End of the Obama Administration 350
“Repeal and Replace” Efforts by Republicans Republican Objections to the ACA End of ACA “Repeal and Replace”?
349
352
352 354
Summary 359 Data Sources 360 Study Questions 362 References 362 Further Reading 366 12.
Trends in the U.S. Health Care System Learning Objectives 369 Current State of U.S. Health Policy 369 Zigzag Theory of U.S. Health Care Reform
U.S. Health Care System Trends
Index
370
372
Consolidation in the Health Care System Big Data and Health Information 373 Prevention and Mental Health 374 Cost of Prescription Drugs Under Scrutiny Impact of New Technology 374 Hospital Versus Ambulatory Care 374 Consumerism 375
Zigzag or a Private System? Study Questions 378 References 378 Further Reading 379
369
373
374
376
381
eChapter: The Affordable Care Act in 2020: An Update
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xii
3/20/20 2:49 PM
Preface This is the ninth edition of An Introduction to the U.S. Health Care System, now titled Jonas’ Introduction to the U.S. Health Care System. It was our privilege, and indeed an honor, to be asked by Dr. Steven Jonas to coauthor the sixth edition in preparation for assumption of full authorship of subsequent editions. In the ninth edition, we continue the practice of Drs. Roemer and Jonas, providing both descriptions of and commentary on the health care system. As Dr. Jonas wrote in the Preface to the seventh edition,“this book has a political and philosophical point of view. Although it always attempts to be objective, it is not neutral. Its primary social value is that the principal purpose of the U.S. health care delivery system, taking precedence over any other purpose, should be to meet and serve the health care needs of the American people. If other purposes, such as the production of private profit, power, prestige, and political advantage, are achieved at all, they should very much take a back seat to the stated primary purpose.” The ninth edition provides an update of the health care system and its history of change. Two significant developments in the period that has elapsed since the sixth edition in 2007— the rise of the Tea Party and the passage of the Affordable Care Act (ACA)—encapsulate the conflict within the larger society, which continues to prevent the health care system from fully achieving equity, quality, and efficiency—the criteria used to evaluate all health systems (Aday, Begley, Lairson, & Slater, 1993). The Tea Party’s success in rousing public opinion against government ensured that in health care, as in all other areas of society, private-sector interests would be defended even if doing so maintained inequity, inefficiency, and poor quality care. The ACA represents the best efforts of those who believe that government has a responsibility to ensure an equitable, efficient, and quality health care system but who were constrained by antigovernment sentiment and its converse, preference for the private sector. The options for public action were limited during development of the ACA legislation, and, even now, the most important facets of the legislation for bringing about needed reforms—the individual mandate and funding for prevention—have been overturned. The tension between public and private action continues to define the kind of health care system we have in the United States. Indeed, the tension seems greater today than at the time of earlier editions. Antigovernment sentiment seems stronger and policy even more constrained. For our readers, the book is intended as a guide to the future, as well as a description of the past and present. The pressures to change the health care system are enormous. They include:
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xiii
3/20/20 2:49 PM
xiv
P re f a c e
• • •
• •
Rising costs that continue to consume a greater percentage of our gross national product than in any peer nation. A large and growing population with high expectations for access to quality health care. Inequality in access and quality of health care, particularly with the decline in employer-based insurance as the economy uses more part-time and contract labor. Technological advances that continually expand the range and cost of health care. Big data analytics that uncovers previously unknown information about health and health care, much like excavations of archaeological sites provide clues to the past.
With so much pressure to change, readers beginning their journey into the U.S. health care terrain should conclude that change is inevitable. The road does not end here. However, the form that change will take is unknown. Choices will be made about the health care system based on a complex calculus of history, resources, technological advancements, demographic imperatives, and ideological preferences. Perhaps the most important factor in this equation will be preference for a public or private health care system. Will future policies “zigzag” between public and private solutions or settle on one? As were the earlier editions of An Introduction to the U.S. Health Care System, this edition is intended primarily for undergraduate courses introducing the U.S. health care system; graduate survey courses; courses for medical, nursing, and other clinical students; and courses for practicing health professionals who simply want a relatively brief overview of the health care system. The subject matter is organized into two sections. Part I (Chapters 1–7) describes the present state of the U.S. health care system. Chapter 1 is an overview of the system. Chapter 2 covers the settings for health care delivery—hospitals, long-term care, and ambulatory care. Chapter 3 discusses the professions that deliver health care. Chapter 4 examines the medicines, devices, and technology used in treatment and diagnosis. Chapter 5 describes the role of government in the health care system. In Chapter 6, the financing and cost of health care are reviewed. In Chapter 7, the principles and practices of performance improvement are presented. Part II (Chapters 8–12) describes the U.S. health care system’s transitions—investigating how we got here and where we are going. Chapter 8 summarizes important debates and conflicts that have structured health care change in the United States since 1900. Chapter 9 is a history of the “piecemeal” approach to solving problems within the health care system, from 1900 to the present. Chapter 10 is devoted to the history of efforts to establish comprehensive reform prior to passage of the ACA. Chapter 11 is a detailed discussion of the ACA, along with its limitations and the challenges to this legislation. Finally, Chapter 12 describes trends in the U.S. health care system, including the future of the ACA. Finally, to keep abreast of trends and changes affecting the U.S. health care system we have updated and will continue to publish our supplement on The Affordable Care Act: An Update each year. You can access it at the following link: http://connect.springerpub.com/content/ book/978-0-8261-7404-8 Once again, we have interjected a bit of humor in the form of cartoons that capture a theme, highlight an issue, or point out an absurdity or contradiction in policy or practice. We hope these add to the readers’ understanding, even enjoyment, of the material. The problem of providing quality health care, efficiently, to all people is grave, but unfortunately, our approach has provided grist for humorists, as well as reformers.
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xiv
3/20/20 2:49 PM
P re f a c e
xv
In addition to the book itself, a robust ancillary package, including an Instructor’s Manual, PowerPoints, a Test Bank, and student exercises to deepen learning, is available to qualified instructors. To access these materials, email textbook@springerpub .com Raymond L. Goldsteen, DrPH, MA Professor Emeritus of Preventive Medicine Stony Brook University, SUNY Stony Brook, New York Karen Goldsteen, PhD, MPH Affiliated Public Health Faculty, Program in Public Health Stony Brook University, SUNY Stony Brook, New York Benjamin Z. Goldsteen, MBA Chief Analytics Officer OneCity Health NYC Health + Hospitals New York, New York
REFERENCE Aday, L. A., Begley, C. E., Lairson, D. R., & Slater, C. H. (1993). Evaluating the medical care system: Effectiveness, efficiency, and equity. Ann Arbor, MI: Health Administration Press.
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xv
3/20/20 2:49 PM
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xvi
3/20/20 2:49 PM
Acknowledgments It is an honor and pleasure to author Jonas’ Introduction to the U.S. Health Care System. Our goal has been to maintain the high standards set by the original authors—Drs. Steven Jonas and Milton Roemer—and to keep abreast of the continual, significant changes that occur in the field so that each new edition is useful to its readers. Fortunately, we have had help from the dedicated and highly professional team at Springer Publishing Company that patiently and expertly guided us to the final product. This team includes David D’Addona, senior editor; Jaclyn Shultz, assistant editor of Medicine and Health Sciences; and Cindy Yoo, managing editor. We acknowledge and thank them and their staffs, most sincerely. We are so grateful for their work. We also thank their predecessors—especially Sheri Sussman, former executive editor— who encouraged and supported us during the writing of earlier editions. Finally, as in the preceding edition, we acknowledge Dr. Ursula Springer (deceased), who led Springer Publishing for 34 years, and Theodore Nardin, former chief executive officer and publisher at Springer, who shepherded the company into the 21st century.
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xvii
3/20/20 2:49 PM
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xviii
3/20/20 2:49 PM
List of Abbreviations AACN AAFP AALL AAM AAMC AANP AAPA ABFM ABIM ABP ACA ACCME ACEP ACGME ACS ADN AFDC AHA AHCA AHRQ AIDS AMA ANA ANDA AOA APhA APHA APIC APRN ASCA
American Association of Colleges of Nursing American Academy of Family Physicians American Association for Labor Legislation Association for Accessible Medicines Association of American Medical Colleges American Academy of Nurse Practitioners American Academy of Physician Assistants American Board of Family Medicine American Board of Internal Medicine American Board of Pediatrics Affordable Care Act or Obamacare. See PPACA Accreditation Council for Continuing Medical Education American College of Emergency Physicians Accreditation Council for Graduate Medical Education American Community Survey Associate degree in nursing Aid to Families With Dependent Children American Hospital Association American Health Care Act Agency for Healthcare Research and Quality Acquired immunodeficiency syndrome American Medical Association American Nurses Association Abbreviated New Drug Application American Osteopathic Association American Pharmacists Association American Public Health Association Association for Professionals in Infection Control and Epidemiology Advanced practice registered nurse Ambulatory Surgery Center Association
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xix
3/20/20 2:49 PM
xx
ASHP ASTHO ATSDR BBA BCRA BLA BLS BRFSS BSN CABSI CAHPS CAM CANHR CAUTI CBO CCMC CCNE CCS CCSQ CDC CGMP CHC CHIP CHPA CIHQ CLABSI CMI CMS CNPP COPC CPS CSA CSR DALY DEA DHHS DHQP DNP DOD DPEI DRG ED EHR
L i s t o f A b b re v i a t i o n s
American Society of Health-System Pharmacists Association of State and Territorial Health Officials Agency for Toxic Substances and Disease Registry Balanced Budget Act Better Care Reconciliation Act Biologics license application Bureau of Labor Statistics Behavioral Risk Factor Surveillance System Bachelor’s degree in nursing Catheter-associated bloodstream infection Consumer Assessment of Healthcare Providers and Systems Complementary and alternative medicine California Advocates for Nursing Home Reform Catheter-associated urinary tract infection Congressional Budget Office Committee on the Costs of Medical Care Commission on Collegiate Nursing Education Clinical Classification Software Center for Clinical Standards & Quality Centers for Disease Control and Prevention Current Good Manufacturing Practice Community health center Children’s Health Insurance Program. See SCHIP Consumer Healthcare Products Association Center for Improvement in Healthcare Quality Central line–associated bloodstream infection Center for Medicare Innovation Centers for Medicare & Medicaid Services Center for Nutrition Policy and Promotion Community-oriented primary care Current Population Survey Controlled Substance Act Cost Sharing Reductions Disability adjusted life years Drug Enforcement Administration Department of Health and Human Services Division of Healthcare Quality Promotion Doctor of nursing practice Department of Defense Division of Preparedness and Emerging Infections Diagnosis-Related Group Emergency department Electronic health record
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xx
3/20/20 2:49 PM
L i s t o f A b b re v i a t i o n s
EIP EMR EMTALA ENA EPA EPO ERISA ESI ESRD FDA FDCA FPL FQHC FTE GAO GDP GME GOP GPO GRASE HAI HALE HCAHPS HCE HCUP HEDIS HFAP HICPAC HIE HIPAA HIT HITECH HMO HOS HPSA HRSA HSA ICU IDS IHI IMD IMG
xxi
Emerging Infections Program Electronic medical record Emergency Medical Treatment and Labor Act Emergency Nurses Association Environmental Protection Agency Exclusive provider organization Employee Retirement Income Security Act of 1974 Emergency Severity Index; Employer-sponsored insurance End–stage renal disease Food and Drug Administration Federal Food, Drug, and Cosmetic Act Federal Poverty Level Federally Qualified Health Center Full-time equivalent Government Accountability Office Gross Domestic Product Graduate Medical Education Grand Old Party (Republican Party) Group purchasing organization Generally regarded as safe and effective Healthcare-associated infection Healthy life expectancy Hospital Consumer Assessment of Healthcare Providers and Systems Survey Health Consumption Expenditures Healthcare Cost and Utilization Project Healthcare Effectiveness Data and Information Set Healthcare Facilities Accreditation Program Healthcare Infection Control Practices Advisory Committee Health information exchange Health Insurance Portability and Accountability Act Health information technology Health Information Technology for Economic and Clinical Health Act Health maintenance organization Health Outcomes Survey Health Professional Shortage Area Health Resources and Services Administration Health Savings Account Intensive care unit Integrated delivery system Institute for Healthcare Improvement Implantable medical devices International medical graduates
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xxi
3/20/20 2:49 PM
xxii
IMR IMS IOM IPA IT ITA JCAHO KFF LCME LHD LOS LPN LTACHS LUPA M&A MA MCO MD MedPAC MEPS MIPS MMA MN MRI MRSA MSA MSN NACCHO NAICS NAMCS NASAA NCCDPHP NCHS NCQA NHANES NHC NHE NHEA NHI NHS NHII NHIS NHSN
L i s t o f A b b re v i a t i o n s
Infant mortality rate Indicator Measurement System Institute of Medicine Independent physician association Information technology International Trade Association Joint Commission on Accreditation of Healthcare Organizations Kaiser Family Foundation Liaison Committee on Medical Education Local health department Length-of-stay Licensed practical nurse Long-term acute care hospital Low Utilization Payment Adjustment Merger and acquisition Medicare Advantage Managed care organization Medical degree Medicare Payment Advisory Commission Medical Expenditure Panel Survey Merit-Based Incentive Payment System Medicare Prescription Drug, Improvement, and Modernization Act of 2003 Master of nursing Magnetic resonance imaging Methicillin-resistant Staphylococcus aureus Metropolitan statistical area Master of science degree in nursing National Association of County and City Health Officials North American Industry Classification System National Ambulatory Medical Care Survey National Adult Day Services Association National Center for Chronic Disease Prevention and Health Promotion National Center for Health Statistics National Committee for Quality Assurance National Health and Nutrition Examination Survey Neighborhood health center National Health Expenditures National Health Expenditure Accounts National health insurance National Health Service Nebraska Health Information Initiative National Health Interview Survey National Healthcare Safety Network, formerly NNIS
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xxii
3/20/20 2:49 PM
L i s t o f A b b re v i a t i o n s
NIH NIOSH NIS NLN CNEA NNIS NQF NQS NSLCP NUCC NVSS OECD OES ONC OPD ORYX OSHA OTC PA PBM PCORI PCP PHCE PHCS PHO PHS PMA POS PPACA PPGP PPO PPS PRP PSM QI R&D RN RUS SAMHSA SCHIP SENIC SES SHEA
xxiii
National Institutes of Health National Institute for Occupational Safety and Health National Inpatient Sample. See HCUP National League for Nursing Commission for Nursing Education Accreditation National Nosocomial Infections Surveillance System. See NHSN National Quality Forum National Quality Strategy National Study of Long-Term Care Providers National Uniform Claim Committee National Vital Statistics System Organisation for Economic Co-operation and Development Occupational Employment Statistics Office of the National Coordinator for Health Information Outpatient department ORYX Performance Measurement Initiative, JCAHO Occupational Safety and Health Administration Over-the-counter Physician assistant Pharmacy benefit manager Patient-Centered Outcomes Research Institute Primary care physician Personal Health Care Expenditures Personal health care system Physician–hospital organization Public Health Service Premarket approval Point-of-service Patient Protection and Affordable Care Act or Obamacare. See ACA Prepaid group practice Preferred provider organization Prospective payment system Policy Research Perspective Physician Supply Model Quality initiatives Research and development Registered nurse Rural Utilities Service Substance Abuse and Mental Health Services Administration State Children’s Health Insurance Program. See CHIP Study on the Effectiveness of Nosocomial Infection Control Socioeconomic status Society for Healthcare Epidemiology of America
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xxiii
3/20/20 2:49 PM
xxiv
SHOP SIR SSI STLDI TB TQM UDI UN USDA USMLE VA VAE VAP WHO WIC WISQARS WRIISC YHL YPLL
L i s t o f A b b re v i a t i o n s
Small Business Health Options Program Standardized infection ratio Surgical site infection Short-term limited duration insurance Tuberculosis Total Quality Management Unique Device Identification United Nations U.S. Department of Agriculture U. S. Medical Licensing Examination Veterans Affairs Ventilator-associated events Ventilator-associated pneumonia World Health Organization Women, Infants, and Children Program Web-based Injury Statistics Query and Reporting System War Related Illness and Injury Study Center Years of healthy life Years of potential life lost
Goldsteen74024_00_FM_i-xxiv_03-18-20.indd xxiv
3/20/20 2:49 PM
I U.S. Health Care System: Present State
Goldsteen74024_01_CH01_1-32_03-18-20.indd 1
3/19/20 3:06 PM
Goldsteen74024_01_CH01_1-32_03-18-20.indd 2
3/19/20 3:06 PM
1 Introduction
© Artizans Entertainment Inc. By Chris Wildt.
LEARNING OBJECTIVES After completing this chapter, students will be able to: • Describe the elements common to all health care systems. • Define health and identify and describe the determinants of health. • Discuss the influence of basic demographic characteristics on mortality and morbidity. • Define and describe the differences between primary, secondary, and tertiary prevention and primary, secondary, and tertiary health care. • Identify the components of the U.S. health care system and describe how it is organized. • Identify and define Aday’s criteria for evaluating health care system performance.
Goldsteen74024_01_CH01_1-32_03-18-20.indd 3
3/19/20 3:06 PM
4
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
System: A set of connected parts or components that function together to form a complex whole. A good health system delivers quality services to all people, when and where they need them. The exact configuration of services varies from country to country, but in all cases requires a robust financing mechanism; a well-trained and adequately paid workforce; reliable information on which to base decisions and policies; wellmaintained facilities and logistics to deliver quality medicines and technologies. (World Health Organization [WHO], 2015) Each nation has a health care system, but as a knowledgeable colleague said, “When you’ve seen one health care system, you’ve seen one health care system. No two are exactly the same.” Every country’s health care system is organized to provide the diagnosis and treatment of individuals’ health problems and consists of a health care workforce, practice setting, and organizations responsible for workforce training, research, and system oversight. However, there is enormous variation in how this important societal function is actually realized. The variation arises from differences in fundamental beliefs about what constitutes a health problem, who are legitimate health care providers, what are fitting and effective methods of diagnosis and treatment, what are suitable settings for the provision of health care, how health care should be financed, and what constitutes appropriate oversight and evaluation of health care providers and the health care system. Differences also result from variation in national resources, which differentiate nations’ health care systems even if their fundamental beliefs about health and health care are similar. In general, all societies designate some persons or positions as legitimate providers of health care. These designated providers are empowered in their society to identify health problems, determine their causes, and provide alleviation or cure. Some providers are designated as dominant or vie with others for dominance. There is also a defined role for the recipients of health care services: for example, the“sick role,”as defined by Parsons (1951), which posits the rights and obligations of sick persons in Western societies. The sum of all the institutions and processes that support the work of diagnosis and healing can be called the health care system of that society. These systems are organized to facilitate the diagnosis and treatment of legitimate patients by legitimized providers using approved tools in appropriate settings. We also recognize that conditions defined as health problems may differ from society to society and over time. In the United States today, people who are obese are considered in poor health, and they are treated with everything from diet to bariatric surgery. In other societies, obesity is a desirable trait, emulated if possible by those who are thin. Diagnosis and treatment models may differ between societies. The social position, training, and authority of healers may differ. The organization of the system and the expected outcomes may differ among countries and among cultures. Let us consider an example of fundamental differences in beliefs about what constitutes a health problem, a legitimate provider, and appropriate methods of treatment of health problems. Traditional Chinese medicine (Liu, 1988) offers an entirely different perspective on health and health care than the model developed in the Western European countries. Written records about the origins of traditional Chinese medicine can be traced back further than 200 BCE. According to Chinese medicine, the human body must maintain homeostasis in order to maintain a state of health, that is, an internal, bodily balance between two inseparable and opposing forces of nature: yin and yang. Yin represents the cold, or passive, principle, whereas yang represents the hot, or active, principle. Any imbalance of these two forces can lead to a blockage of flow in the qi (vital energy) or in the blood, both of which run along interconnected channels in the body called meridians. When there is a disturbance in the energy flow, the appropriate type of treatment is selected to unblock the flow
Goldsteen74024_01_CH01_1-32_03-18-20.indd 4
3/19/20 3:06 PM
1
■
I n t ro d u c t i o n
5
through the meridians: materia medica (herbology), acupuncture, bodywork (massage and manipulation), or health-benefiting exercises (exercising the body–mind connection). This is quite different from the Western approach to understanding health problems and their treatment. Western medicine perceives the human body as a collection of interconnected health systems—heart, circulatory, endocrine, reproductive, and so forth—each with a set of functions and normal operating processes. Health problems result from dysfunction in a system or systems, resulting from injury, infection, toxic exposure, or other causes. They are treated with surgery and/or medication to restore normal functioning (cure), if possible, or to interrupt a downward spiral and provide rehabilitation, stabilization, or comfort care. The focus of this book is the U.S. health care system, with some comparisons to certain peer industrialized countries, including Western European nations, Canada, Australia, and Japan. The United States shares with these nations (as well as many others around the globe) the same basic understanding of health and health care, including what constitutes a health problem; what are legitimate and effective diagnostic and treatment theories, methods, and tools; and which persons should be designated as health care providers, with physicians dominant among them. This set of beliefs about health and health care, which originated and developed over a period of centuries in Western Europe, is generally referred to as“Western medicine.” Western medicine is also called allopathic medicine after the medical faction (allopath) that gained dominance in the 19th century over groups of healers, including homeopaths, chiropractors, and osteopaths (Starr, 1982). Among the countries in which Western medicine is the primary means of dealing with the problems of health and disease, there are also certain similarities in the basic structures and organization used to deliver health care. Moreover, the United States and its peer nations have similar economies and abilities to finance their health care systems. However, as discussed, there are very real differences between the United States and its peer nations relating to the methods of paying for health care, the equity and efficiency of health care as provided, and population health outcomes. These differences make the U.S. health care system unique, even among its peer nations.
HEALTH AND HEALTH CARE What Is Health? The most famous and influential definition of health is the one developed by the World Health Organization (WHO): “Health is a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.” It was adopted in 1946 and has not been amended since 1948 (WHO, 1948, p. 100). Many subsequent definitions have taken an equally broad view of health, including: A state characterized by anatomical, physiological and psychological integrity; ability to perform personally valued family, work and community roles; ability to deal with physical, biological, psychological and social stress; a feeling of well-being; and freedom from the risk of disease and untimely death. (Porta, 2014, p. 128) Both definitions exemplify the tendency over the second half of the 20th century to enlarge the definition of health beyond morbidity, mortality, and disability to include sense of well-being, ability to adapt to change, and social functioning. However, in practice, the more limited view of health usually guides the provision of health services and efforts to improve health status. As Young (1998) wrote: “Indeed, the WHO definition is ‘honored in repetition, rarely in application.’ Health may become so inclusive that virtually all human endeavors, including the pursuit of happiness, are considered within its domain” (p. 2).
Goldsteen74024_01_CH01_1-32_03-18-20.indd 5
3/19/20 3:06 PM
6
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Determinants of Health Individual and population health are determined by many factors, only one of which is health care. It is generally accepted that the determinants of health include genetic inheritance, the physical environment—natural and built, and the social environment. The impact of these factors on health is mediated by an individual’s response to them, both behavioral and biologic. This concept is argued well by Evans and Stoddart (1994) and more recently in Marmot and Wilkinson’s (2006) Social Determinants of Health. Note that, although we talk about the “determinants of health,” they are usually discussed in terms of how they are related to poor health. A brief overview of the determinants of health follows.
Genetic Inheritance Our knowledge about the effects of genetic inheritance on health is growing rapidly. It is understood that, with few exceptions, disease processes are … determined both by environmental and by genetic factors. These often interact, and individuals with a particular set of genes may be either more or less likely, if exposed, to be at risk of developing a particular disease. These effects can be measured by showing that the relative risk of exposure to the environmental factor is significantly greater (or lesser) for the subgroup with the abnormal gene, than the risk in those without. (Pencheon, Guest, Melzer, & Gray, 2001, p. 544)
Physical Environment Physical environment factors include health threats from exposure to toxins and unsafe conditions, particularly in occupational and residential settings. Many occupations can expose workers to disease-causing substances, high risk of injury, and other physical risks. For example, the greatest health threats to U.S. farmworkers are injuries from farm machinery and falls that result in sprains, strains, fractures, and abrasions (Myers, 2001). There are well-documented health threats to office workers from indoor air pollution, found by research beginning in the 1970s, including passive exposure to tobacco smoke, nitrogen dioxide from gas-fueled cooking stoves, formaldehyde exposure,“radon daughter”exposure, and other health problems encountered in sealed office buildings (Samet, Marbury, & Spengler, 1987; U.S. Environmental Protection Agency, 2006). In residential settings, exposure to pollutants from nearby industrial facilities, power plants, toxic waste sites, or a high volume of traffic presents hazards for many (Organisation for Economic Co-operation and Development, 2012). In the United States, these threats are increasingly known to have a disproportionately heavy impact on low-income and minority communities (Centers for Disease Control and Prevention, 2003; Institute of Medicine [IOM], 1999). The effects of the built environment on health are increasingly studied: The built environment refers to the presence of (and proximity to) health-relevant resources as well as to aspects of the ways in which neighborhoods are designed and built (including land use patterns, transportation systems, and urban planning and design features). (National Research Council, 2013)
Social Environment Sociodemographic characteristics, particularly race, ethnicity, and socioeconomic status, are associated with significant variations in health status and risk for health problems. There is a large literature demonstrating the relationship between low socioeconomic status and poor
Goldsteen74024_01_CH01_1-32_03-18-20.indd 6
3/19/20 3:06 PM
1
■
I n t ro d u c t i o n
7
health, including a gradient in which the higher the socioeconomic status, the better the health (e.g., Lynch & Kaplan, 2000; Williams, 1990). Similarly, much research indicates that disparities in health status exist between racial and ethnic groups. Minority Americans, including African Americans, Hispanics/Latinos, Native Americans, and Pacific Islanders, generally have poorer health outcomes than do Whites. The preventable and treatable conditions for which disparities have been shown include cardiovascular disease, diabetes, asthma, cancer, and HIV/AIDS (U.S. Department of Health and Human Services [DHHS], 1998). Although race and ethnicity do not“explain” these disparities, they point to the need for explanations. Discrimination and its consequences are a recent focus for investigations attempting to explain racial and ethnic disparities (Krieger, 2000; Mays, 2007). Nonphysical occupational factors also affect health. For example, a great deal of research demonstrates the relationship between poor health outcomes and the psychosocial work environment. The demand-control model is one well-known theory, hypothesizing that employees with the highest psychological demands and the lowest decision-making latitude are at the highest risk for poor health outcomes (Theorell, 2000). In addition, job loss and threat of job loss have a negative impact on health (Kasl & Jones, 2000). Another large body of research on the social environment and health focuses on social integration, social networks, and social support (Berkman & Glass, 2000). For example, numerous studies over the past 20 years have found that people who are isolated or disengaged from others have a higher risk of premature death. Also, research has found that survival of cardiovascular disease events and stroke is higher among people with close ties to others, particularly emotional ties. Social relations have been found to predict compliance with medical care recommendations, adaptation to adverse life events such as death of a loved one or natural disaster, and coping with long-term difficulties such as caring for a dependent parent or a disabled child. In 2008, the WHO (2008) released a major report on the social determinants of health: Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health. The premise and evidence of the report are that “Social justice is a matter of life and death. It affects the way people live, their consequent chance of illness, and their risk of premature death. We watch in wonder as life expectancy and good health continue to increase in parts of the world and in alarm as they fail to improve in others” (p. iii). Areas studied include early child development, globalization, urbanization, employment conditions, social exclusion, priority public health conditions, and women and gender equity.
Health Behavior The term health behavior can refer to behaviors that are beneficial to health. However, the term is generally used in the negative to refer to behaviors that harm health, including smoking, abusing alcohol or other substances, failing to use seat belts or other poor safety behaviors, making unhealthy food choices, and not engaging in adequate physical activity. The effect of health behaviors on health status has been widely studied and found to be an important determinant of health. For example, most of the leading causes of death in the United States can be explained largely in terms of health behaviors that relate to them. Consider the 10 leading causes of death, as of 2014, as characterized by diagnosed disease or condition: diseases of heart; malignant neoplasms (cancer); chronic lower respiratory diseases; unintentional injuries (accidents); cerebrovascular diseases (stroke); Alzheimer’s disease; diabetes mellitus; influenza and pneumonia; nephritis, nephrotic syndrome, and nephrosis; and intentional self-harm (suicide). The next five leading causes of death were septicemia, chronic liver disease and cirrhosis, essential hypertension and hypertensive
Goldsteen74024_01_CH01_1-32_03-18-20.indd 7
3/19/20 3:06 PM
8
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
renal disease, Parkinson’s disease, and pneumonitis caused by inhalation of solids and liquids (National Center for Health Statistics [NCHS], 2015). In one way or another, personal health behavior has an impact on the occurrence in any given individual of most of the diseases and conditions on this list. Looking at the cause of death in a different way—that is, by major contributing cause of the disease to which the death was attributed rather than by the disease itself—in the first study of its kind, McGinnis and Foege (1993) showed that, as of 1990, the leading factors were tobacco use, dietary patterns, sedentary lifestyle, alcohol consumption, microbial agents, toxic agents, firearms, sexual behavior, motor vehicles, and use of illicit drugs. As of 2002, the situation remained the same (McGinnis, Williams-Russo, & Knickman, 2002). Even though there is widespread agreement that health is a response to the physical and social environments in which the individual lives and is influenced by the individual’s genetic inheritance, health behaviors are often seen as the best target for health improvement efforts. For example, the emphasis of Healthy People 2010 (DHHS, 2000), which is the U.S. nationwide health-promotion and disease-prevention agenda, is on health behaviors and medical care. The leading health indicators cited in Healthy People 2010 are level of physical activity, overweight and obesity, tobacco use, substance abuse, responsible sexual behavior, mental health, exposure to injury and violence, environmental quality, immunization status, and access to health care. Only the environmental quality indicator deals substantially with factors other than personal behavioral change or the availability of medical care. However, the interrelationships among biology, behavior, environment, and health are increasingly recognized and acted upon. Healthy People 2020 (DHHS, 2010), for example, acknowledges the narrow focus of the past and has expanded its approach for improving population health: Because significant and dynamic inter-relationships exist among (these) different levels of health determinants, interventions are most likely to be effective when they address determinants at all levels. Historically, many health fields have focused on individual-level health determinants and interventions. Healthy People 2020 should therefore expand its focus to emphasize health-enhancing social and physical environments. (p. 2)
Health Care as a Determinant of Health The central focus of health care is to restore health or prevent exacerbation of health problems. If we argue that health is the product of multiple factors, including genetic inheritance, the physical environment, and the social environment, as well as an individual’s behavioral and biologic response to these factors, we see that health care has an impact late in the causal chain leading to disease, illness, and infirmity. Often by the time the individual interacts with the health care system, the determinants of health have had their impact on his or her health status, for better or worse. Thus, the need for health care may be seen as a failure to prevent the determinants of health from adversely affecting the individual patient. As examples, consider the health care required for treating lung disease among miners and smokers. The failure of the coal industry to protect coal miners from regular inhalation of airborne dust had resulted, by 1970, in coal workers’ pneumoconiosis in 33% of miners with 25 years or more in the mines, 20% with 20 to 24 years, and nearly 15% with 15 to 19 years’ tenure (National Institute for Occupational Safety and Health, 2019). Our failure at many levels—parents, schools, public health—to prevent adolescents from beginning to smoke results in three out of four teens who smoke cigarettes in high school smoking as adults. People who begin smoking early are more likely to develop a severe nicotine addiction than those who begin at a later age (American Lung Association, 2019; SmokeFree.gov, 2019). In both cases, failure to address the determinants of health results in increased need for health care.
Goldsteen74024_01_CH01_1-32_03-18-20.indd 8
3/19/20 3:06 PM
1
■
I n t ro d u c t i o n
9
What Is Health Care? Health care can be categorized in terms of its relationship to prevention—primary, secondary, and tertiary. Fos and Fine (2000) define these terms as follows: “Primary prevention is concerned with eliminating risk factors for a disease. Secondary prevention focuses on early detection and treatment of disease (subclinical and clinical). Tertiary prevention attempts to eliminate or moderate disability associated with advanced disease” (pp. 108–109). Primary prevention intends to prevent the development of disease or injury before it occurs in individuals, and thus to reduce the incidence of disease in the population. Examples of primary prevention include the use of automobile seat belts, condom use, skin protection from ultraviolet light, and tobacco-use cessation programs. Secondary prevention is concerned with reducing the burden of existing disease after it has developed; early detection is emphasized. Secondary prevention activities are intended to identify the existence of disease early so treatments that might not be as effective when applied later can be of benefit. Tertiary prevention focuses on the optimum treatment of clinically apparent, clearly identified disease so as to reduce the incidence of later complications to the greatest possible degree. In cases where disease has been associated with adverse effects, tertiary prevention involves rehabilitation and limitation of disability. Health care is primarily concerned with secondary and tertiary prevention: (a) early detection, diagnosis, and treatment of conditions that can be cured or limited in their consequences (secondary prevention); and (b) treatment of chronic diseases and other conditions to prevent exacerbation, stabilize conditions, and minimize future complications (tertiary prevention). The health care system undoubtedly has its smallest impact on primary prevention—that group of interventions that focus on stopping the development of disease and illness, and the occurrence of injury. And as Evans and Stoddart (1994) argue, other than for immunization, the major focus of the health care system’s primary prevention activities is on the behavioral determinants of health, rather than the physical and social environments: The focus on individual risk factors and specific diseases has tended to lead not away from but back to the health care system itself. Interventions, particularly those addressing personal lifestyles, are offered in the form of “provider counseling” for smoking cessation, seatbelt use, or dietary modification. These in turn are subsumed under a more general and rapidly growing set of interventions attempting to modify risk factors through transactions between clinicians and individual patients. The “product line” of the health care system is thus extended to deal with a more broadly defined set of “diseases”: unhealthy behaviors. The boundary becomes blurred between, e.g., heart disease as manifest in symptoms, or in elevated serum cholesterol measurements, or in excessive consumption of fats. All are “diseases” and represent a “need” for health care intervention …. The behavior of large and powerful organizations, or the effects of economic and social policies, public and private, [are] not brought under scrutiny. (pp. 43–44) The success of any health care system is also affected by the other determinants of health. Genetic predisposition to breast cancer may limit the long-term success rates of cancer treatment. Continued exposure to toxins in the environment or at work may decrease the likelihood that the physician can stabilize an individual with allergies. Health behaviors, such as smoking or substance abuse, may stymie the best health care system when treating
Goldsteen74024_01_CH01_1-32_03-18-20.indd 9
3/19/20 3:06 PM
10
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
an individual with lung disease. The lack of support at home for changes in behaviors or adherence to medical regimens may undermine the ability of the health care system to treat an individual with diabetes successfully. Poverty, race, and ethnicity often limit access to health care, and therefore, the ability of physicians to diagnose and treat health problems effectively (IOM, 2003). We recognize that health, as well as health care, exist within a biological, physical, and social context, and all of these factors influence the health care system’s probability of success.
THE POPULATION SERVED The determinants of health lead to the health problems that are diagnosed and treated in the health care system. It can be argued that those people who use the health care system have as great an influence on the system as those who provide health care. What are some of the major characteristics of the U.S. population—the aggregate user of health care—that influence the health care system? The demographic characteristics of any population have a huge impact on health and, therefore, on health care. They differentiate people’s risk of mortality and causes of morbidity, as well as their health behaviors. In this section, we provide a brief discussion of some demographic characteristics—age, sex, race and ethnicity, and poverty—and their relationship to mortality, morbidity, and health behaviors in the population.
Mortality
Deaths per 100,000 population (log scale)
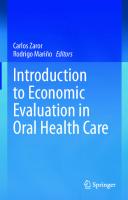
Age and death are decidedly related, and mortality figures are instructive on this point. There were 2.7 million deaths in the United States in 2016. Most deaths occurred among people 65 and older (73%). People 45 to 64 years old accounted for 19.7% of all deaths, and each younger age group accounted for a smaller percentage of total deaths than the one preceding it (see Figure 1.1). The crude death rate for each 10-year age group differed dramatically. In 2016, infants had a death rate of 583/100,000, which dropped to 25/100,000 for children 1 to 4 years old 10,000 65 years and over
1,000
65+ 45–64 25–44 15–24 1–14
45–64 years
How have death rates changed from 2006 to 2016? Decrease Decrease Increase Decrease Increase Increase Decrease Decrease Stable Distribution of deaths, by age: 2016 1–14 years, 15–24 years, 0.3% 1.2% Less than 1 year, 25–44 years, 0.8% 4.9%
25–44 years 100 15–24 years 1–14 years
45–64 years, 19.7%
10 2006
2016
65 years and over, 73.0%
FIGURE 1.1 Death rates for all causes, by age, 2016. Source: National Center for Health Statistics. (2018b). Health, United States, 2017: With special feature on mortality. Hyattsville, MD: U.S. Department of Health and Human Services. Retrieved from http:// www.cdc.gov/nchs/data/hus/hus17.pdf
Goldsteen74024_01_CH01_1-32_03-18-20.indd 10
3/19/20 3:06 PM
1
■
I n t ro d u c t i o n
11
TABLE 1.1 Crude Death Rates for Underlying Cause of Death, by Age, 2016 10-Year Age Group
Population
Deaths
Crude Rate/100,000
8y >100 >20
2 140 >30
2%
3 m–3 y >160 >40
No 3
FIGURE 2.3 Emergency Severity Index triage algorithm, version 4. HR, hazard ratio; RR, relative risk; SaO2, oxygen saturation. Source: © Emergency Nurses Association. Reproduced with permission.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 41
3/19/20 10:52 AM
42
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
uninsured people with health insurance, better health insurance, and comprehensive primary care that would address the problem. A recent study using the National Hospital Ambulatory Care Survey from 2006 through 2016 suggests that the ACA succeeded to some extent, but not entirely. The authors concluded, Proportions of ED visits and hospital discharges by uninsured patients decreased considerably after the implementation of the 2014 ACA insurance provisions. Despite these changes, approximately 1 in 10 ED visits and 1 in 20 hospital discharges were made by uninsured individuals in 2014 to 2016. This suggests that continued attention is needed to address the lack of insurance in US hospital visits, particularly among people aged 18 to 64 years who have less access to government-sponsored insurance. (Singer, Thode, & Pines, 2019)
Emergency Department Utilization In 2016, there were 145,591 million visits to an ED (Rui et al., 2016). Most ED patients were insured, and the expected source of payment was private insurance, Medicaid or CHIP, and Medicare. These three payers accounted for 85% of ED visits. Only 8.4% of ED patients had no health insurance (Rui , Kang, and Ashman, 2016). The top 10 reasons for visiting the ED were as follows: • • • • • • • • • •
Stomach and abdominal pain, cramps, and spasms Chest pain and related symptoms (not referable to body systems) Fever Cough Headache, pain in head Back symptoms Pain, site not referable to a specific body system Shortness of breath Accident, not otherwise specified Vomiting
The level of urgency of ED visits was distributed over the five ESI levels, with most visits considered level 3 (urgent) or level 4 (semiurgent)—32.4% and 24.5%, respectively. Very few visits were level 5 (nonurgent). There was little difference in triage status by expected source of payment. Only visits expected to be covered by Medicare and Medicare/Medicaid were a bit more likely to be level 2 (emergent) than other visits. For the most part, these visits would be persons older than 65 years, and therefore, it is not entirely unexpected that they needed more immediate attention (see Table 2.5). Like physician office visits, there was a geographic variation in utilization of EDs. However, unlike the physician office visit, the greatest ED utilization per person was in the West and the lowest was in the Northeast. Also, the highest rate of ED utilization was in the non-MSAs (64.5 visits/100 persons in non-MSAs vs. 42.9 visits/100 persons in MSAs). This is in contrast to physician office visits, where the rate of visits was much higher in MSAs than in non-MSAs (see Table 2.6). Utilization of the ED also varied by the age and sex of patients. Overall, women had a higher utilization rate than men (49 visits/100 women vs. 42.5 visits/100 men). However, the age variation in rates was not uniform. For women under 15 years, the rate was lower than for men in the same age category (43/100 women vs. 47/100 men). Beginning at 15 years, women had substantially higher rates than men through 44 years. Starting at 45 years, the rates for women and men began to converge until they were almost identical for both men and women aged 75 years and older (62/100 women vs. 61/100 men; see Table 2.7).
Goldsteen74024_02_CH02_33-78_03-18-20.indd 42
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
43
TABLE 2.5 Triage Status of Emergency Department Visits, by Expected Source of Payment Expected Source of Paymenta
Number of Visits in Level 1 Level 2 Level 3 Level 4 Level 5 No Thousands (Immediate) (Emergent) (Urgent) (Semiurgent) (Nonurgent) Triageb Unknown Percentage Distribution (Standard Error)
All visits
145,591
0.6 (0.1)
8.1 (0.7)
32.4 (2.1)
24.5 (1.5)
4.3 (0.5)
6.5 (1.9)
23.5 (3.7)
Private insurance
46,332
0.6 (0.1)
9.1 (0.9)
33.8 (2.4)
23.6 (1.6)
3.5 (0.7)
7.3 (2.2)
22.1 (3.6)
Medicaid or CHIP or other state-based program
54,949
0.5 (0.2)
6.8 (0.7)
32.8 (2.0)
28.3 (1.8)
5.3 (0.7)
6.5 (1.8)
19.8 (3.3)
Medicare
25,916
0.8 (0.2)
13.9 (1.5)
38.8 (2.6)
15.7 (1.4)
2.8 (0.6)
5.9 (1.7)
22.1 (3.5)
Medicare and Medicaidc
5,523
0.4 (0.3)
14.0 (2.4)
40.1 (3.4)
15.9 (2.2)
3.4 (0.9)
*
21.2 (4.5)
No insuranced
12,287
0.5 (0.3)
6.0 (1.0)
31.8 (2.8)
30.3 (2.2)
5.9 (1.3)
*
20.2 (3.7)
1,581
*
*
22.9 (4.6)
34.9 (4.8)
*
*
22.8 (6.3)
Worker’s compensation a
Total exceeds “All visits” and percentage exceeds 100% because more than one source of payment may be reported per visit. A visit in which the emergency service area (ESA) coded nursing triage as zero (had admitted to hospital or treated immediately) or visit occurred in ESA that does not conduct triage. c Visits also included in both the “Medicaid or CHIP or other state-based program” and “Medicare” categories. d Defined as having only self-pay, no charge, or charity as payment sources. CHIP, Children’s Health Insurance Program. NOTE: *Estimate does not meet NCHS standards of reliability. b
SOURCE: Rui, P., Kang, K., & Ashman, J. J. (2016). National hospital ambulatory medical care survey: 2016 emergency department summary tables.
TABLE 2.6 ED Visits, by Geographic Region and Metropolitan Status of ED, 2016 Number of Visits in Thousands (Standard Error in Thousands)
Percentage Distribution (Standard Error of Percentage)
Number of Visits Per 100 Personsa (Standard Error of Rate)
Northeast
24,514 (2,991)
16.8 (2.0)
44.2 (5.4)
Midwest
31,428 (3,834)
21.6 (2.4)
46.9 (5.7)
South
53,485 (5,412)
36.7 (2.9)
44.6 (4.5)
West
36,165 (4,940)
24.8 (2.8)
47.9 (6.5)
117,189 (8,454)
80.5 (3.2)
42.8 (3.1)
28,402 (5,057)
19.5 (3.2)
64.5 (11.5)
Geographic Region of ED
Metropolitan Status of EDb,c MSA Non-MSA a
Visit rates are based on the July 1, 2016, set of estimates of the civilian noninstitutional population of the United States as developed by the U.S. Census Bureau, Population Division. b Population estimates by MSA definitions status are based on estimates of the U.S. civilian noninstitutional population as of July 1, 2016, from the 2016 National Health Interview Survey. c For geographic region and MSA, population denominators are different for each category and thus do not add to total population rate. For other variables, the denominator is the total population. ED, emergency department; MSA, metropolitan statistical area. SOURCE: Rui, P., Kang, K., & Ashman, J. J. (2016). National hospital ambulatory medical care survey: 2016 emergency department summary tables.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 43
3/19/20 10:52 AM
44
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 2.7 Emergency Department Visits, by Patient Age and Sex, 2016 Patient Number of Visits in Thousands Characteristics (Standard Error in Thousands) All visits
145,591 (8,798)
Percentage Distribution (Standard Error of Percentage) 100.0
Number of Visits Per 100 Personsa (Standard Error of Rate) 45.8 (2.8)
Sex and age Female
79,595 (4,803)
54.7 (0.5)
49.0 (3.0)
Under 15 years
12,810 (1,244)
8.8 (0.6)
43.0 (4.2)
15–24 years
12,680 (781)
8.7 (0.3)
60.2 (3.7)
25–44 years
22,883 (1,488)
15.7 (0.4)
54.3 (3.5)
45–64 years
18,346 (1,203)
12.6 (0.4)
42.7 (2.8)
65–74 years
5,757 (450)
4.0 (0.2)
38.1 (3.0)
75 years and over
7,119 (601)
4.9 (0.3)
62.3 (5.3)
Male
65,996 (4,119)
45.3 (0.5)
42.5 (2.7)
Under 15 years
14,625 (1,380)
10.0 (0.6)
47.0 (4.4)
15–24 years
7,995 (613)
5.5 (0.2)
37.2 (2.9)
25–44 years
17,131 (1,105)
11.8 (0.3)
41.8 (2.7)
45–64 years
16,013 (982)
11.0 (0.3)
39.6 (2.4)
65–74 years
5,228 (445)
3.6 (0.2)
39.4 (3.3)
75 years and over
5,004 (470)
3.4 (0.2)
61.6 (5.8)
a Visit rates for age, sex, and private residence are based on the July 1, 2016, set of estimates of the civilian noninstitutionalized population of the United States as developed by the U.S. Census Bureau Population Division.
SOURCE: Rui, P., Kang, K., & Ashman, J. J. (2016). National hospital ambulatory medical care survey: 2016 emergency department summary tables.
Hospital Outpatient Departments The other major setting of ambulatory visits is the hospital outpatient department (OPD). As the name implies, OPDs are part of a hospital or hospital system. The majority of OPD visits occur in voluntary (not-for-profit) hospitals (68.2%) and in government-owned hospitals (30.4%). The majority of OPD visits occur in general medicine clinics (54.5%). The other top clinic types for OPD visits are surgery, pediatrics, obstetrics and gynecology, and substance abuse (see Table 2.8).
Historical Background In the 19th century, clinic service was part of the function of most hospitals serving the poor in urban areas (Freymann, 1974). By 1916, 495 hospitals had clinics, often serving a health care personnel educational function as well as a charitable one (Roemer, 1981). Indeed, many of these clinics were originally established to care for persons who for one reason or another were not being served by a public institution. Hospital-based emergency services came into being to meet observed needs as well. For example, in 1908, the Goshen (New York) Emergency Hospital was established. Its creation
Goldsteen74024_02_CH02_33-78_03-18-20.indd 44
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
45
TABLE 2.8 Outpatient Department Visits, by Type of Clinic and Ownership, 2011 Number of Visits in Thousands (Standard Error in Thousands)
Percentage Distribution (Standard Error of Percentage)
General medicineb
68,458 (7,447)
54.5 (2.8)
Surgery
24,341 (3,595)
19.4 (1.9)
Pediatrics
13,129 (2,507)
10.4 (1.6)
Obstetrics and gynecology
10,669 (1,482)
8.5 (1.0)
Substance abuse or otherc
9,125 (1,273)
7.3 (1.1)
Voluntary (not-for-profit)
85,763 (10,353)
68.2 (5.2)
Government
38,176 (7,661)
30.4 (5.2)
1,782d (773)
1.4d (0.6)
Clinic Typea
Ownership
Proprietary (for-profit) a
Only clinics under the supervision of a physician were included. Clinics specializing in radiology, laboratory services, physical rehabilitation, or other ancillary services were excluded. b General medicine clinics include clinics in the specialties of family medicine and internal medicine and in the internal medicine subspecialties. c Other includes psychiatric, mental health, and miscellaneous specialty clinics. d Figure does not meet standards of reliability or precision. SOURCE: National Center for Health Statistics. (2011). National hospital ambulatory medical care survey: 2011 outpatient department summary tables. Retrieved from https://www.cdc.gov/nchs/ahcd/web_tables.htm#2016
was stimulated by the building of one of New York State’s early trunk highways, Route 17. The road went through the center of the village of Goshen. Traffic accidents occurred with increasing frequency. Thus, a hospital was needed, and with strong local effort, it was built.1 In the beginning, voluntary hospital OPDs were staffed on a rotating basis by the members of the hospital–medical staff working there without pay. Voluntary (not-for-profit) hospital–medical staffs consisted primarily of physicians practicing privately in the community. Thus, they were much more important in setting the style for the organization of medical practice in hospital OPDs than were those of the local government hospitals, which were much more likely to rely on the services of paid medical staff. OPDs have changed in the past 20 years. They have become more sophisticated. In many hospitals, they have been reorganized to improve their efficiency and effectiveness by providing the care that patients need rather than simply serving the functions of the hospital as it perceived them, that is, organizing hospital services to first meet the training and educational needs of medical students and house staff. Whereas the average length of inpatient stays has decreased sharply over the past 20 years, often placing financial strains on the hospital, clinic revenue as a percentage of total revenue had risen. A study by the American Hospital Association found that outpatient revenue was 95% of inpatient revenue in 2017 (Advisory Board, 2019). As examples of the improved care being offered, many hospitals now provide longer and more flexible clinic hours and have integrated care throughout the clinic system.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 45
3/19/20 10:52 AM
46
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Hospital Outpatient Utilization In 2011, the most recent year for which this information is available, approximately 125,721 million visits were made to hospital OPDs. Overall, there were 41 visits per 100 persons per year (NCHS, 2011). Private health insurance, Medicaid, the CHIP, and Medicare were the most common payment sources for OPD visits. The 10 most common reasons for these visits were: • • • • • • • • • •
Progress visit (follow-up to previous visit) General medical examination Postoperative visit Medication Counseling Cough Routine prenatal examination Diabetes Symptoms of the throat Well-baby examination
Like physician office and ED visits, the rate of OPD visits varied by geography. And similar to physician office visits, the highest rate of OPD visits was in the Northeast and the lowest in the West (65.7/100 persons vs. 27.5/100 persons). However, unlike physician office visits and similar to ED visits, there were more OPD visits per year in non-MSAs than that in MSAs (45.7/100 persons vs. 40.1/100 persons, see Table 2.9). TABLE 2.9 OPD Visits, by Geographic Region and Metropolitan Status of Clinic, 2011 Geographic Number of Visits in Thousands Region of OPD (Standard Error in Thousands)
Percentage Distribution (Standard Error of Percentage)
Number of Visits Per 100 Personsa,b,c (Standard Error of Rate)
Northeast
35,987 (7,847)
28.6 (4.9)
65.7 (14.3)
Midwest
34,820 (5,744)
27.7 (4.1)
52.6 (8.7)
South
35,179 (5,770)
28.0 (4.1)
30.9 (5.1)
West
19,735 (4,094)
15.7 (3.1)
27.5 (5.7)
103,340 (10,697)
82.2 (4.5)
40.1 (4.2)
22,381 (6,258)
17.8 (4.5)
45.7 (12.8)
Metropolitan status of OPD MSA Non-MSA a
Visit rates are based on the July 1, 2011, set of estimates of the civilian noninstitutional population of the United States as developed by the Population Division, U.S. Census Bureau. b Population estimates of metropolitan statistical status are based on estimates of the civilian noninstitutional population of the United States as of July 1, 2011 from the 2011 National Health Interview Survey. c For geographic region and MSA, population denominators are different for each category and thus do not add to total population rate. For other variables, the denominator is the total population. MSA, metropolitan statistical area; OPD, outpatient department. SOURCE: National Center for Health Statistics. (2011). National hospital ambulatory medical care survey: 2011 outpatient department summary tables. Retrieved from https://www.cdc.gov/nchs/ahcd/web_tables.htm#2016
Goldsteen74024_02_CH02_33-78_03-18-20.indd 46
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
47
Paralleling physician office and ED utilization, women had higher visit rates than men (48.6/100 women vs. 33.1/100 men), and this discrepancy persisted throughout the life span (see Table 2.10).
Hospital Outpatient Departments in Teaching Hospitals Although not all clinics are found in teaching hospitals (those affiliated with medical schools), nearly 41% were in 2011 (NCHS, 2011). Given the way medical education is structured, teaching hospitals have over time found that the best way of organizing OPDs to TABLE 2.10 Outpatient Department Visits, by Patient Age and Sex, 2011 Percentage Distribution Patient Number of Visits in Thousands (Standard Error of Characteristics (Standard Error in Thousands) Percentage) All visits
Number of Visits Per 100 Personsa (Standard Error of Rate)
125,721 (11,963)
100.0
41.0 (3.9)
Female
76,286 (7,166)
60.7 (0.9)
48.6 (4.6)
Under 15 years
11,520 (1,491)
9.2 (0.8)
38.5 (5.0)
15–24 years
8,790 (875)
7.0 (0.4)
41.4 (4.1)
25–44 years
19,799 (2,006)
15.7 (0.8)
48.4 (4.9)
45–64 years
22,606 (2,325)
18.0 (0.7)
53.5 (5.5)
65–74 years
7,115 (828)
5.7 (0.4)
59.8 (7.0)
75 years and over
6,456 (895)
5.1 (0.5)
60.6 (8.4)
Male
49,435 (5,013)
39.3 (0.9)
33.1 (3.4)
Under 15 years
12,555 (1,786)
10.0 (1.1)
40.2 (5.7)
15–24 years
3,949 (454)
3.1 (0.2)
18.3 (2.1)
25–44 years
8,596 (1,023)
6.8 (0.4)
21.8 (2.6)
45–64 years
15,373 (1,745)
12.2 (0.6)
38.7 (4.4)
65–74 years
5,414 (759)
4.3 (0.4)
52.2 (7.3)
75 years and over
3,549 (565)
2.8 (0.3)
49.4 (7.9)
Sex and Age
a
Visit rates are based on the July 1, 2011, set of estimates of the civilian noninstitutional population of the United States as developed by the Population Division, U.S. Census Bureau. SOURCE: National Center for Health Statistics. (2011). National hospital ambulatory medical care survey: 2011 outpatient department summary tables. Retrieved from https://www.cdc.gov/nchs/ahcd/web_tables.htm#2016
Goldsteen74024_02_CH02_33-78_03-18-20.indd 47
3/19/20 10:52 AM
48
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
provide opportunities for teaching and research is to have separate disease-, organ-, or organ system–specific clinics (Freymann, 1974). This is still largely the case, although there has been an increase in clinics that specialize in treatment of a demographic group (e.g., women or the elderly) as well as conditions that cross disease- or organ-specific boundaries (e.g., pain management clinics). The larger teaching hospitals often have more than 100 different specialty and subspecialty clinics. Thus, a hospital-based physician working in the usual hospital clinic organization can concentrate on diabetes, peripheral vascular disease, or stroke in his or her teaching and research. This is useful for the provider focusing on a particular disease or condition. It may also be helpful to the patient who has a single disease or problem of a rather complex or unusual nature. OPDs in teaching hospitals are staffed by a variety of physicians. Most fall under the following categories: • •
• •
•
Attending physicians who exchange admitting privileges for teaching in hospital clinics Medical school faculty. By the 1980s, many medical schools had become increasingly dependent for their financial support on taking a share of the income physicians earned in the clinics. The money was received primarily from third-party payers. Today, many clinics in medical school–owned teaching hospitals are staffed by medical school faculty whose work there generates some of their own income and money for the school’s general fund. The management system for dividing this income between the physicians and the institution providing the space and supporting staff is usually referred to as the clinical practice plan. Full-time salaried inpatient physicians, usually junior staff, to the clinics who carry out teaching, supervisory, and research functions assigned by the hospital House staff (physicians in postmedical school, graduate specialty training, including interns, residents, and fellows) who usually draw significant clinic duty from time to time throughout the course of their training Outside physicians hired to work exclusively in the clinics on a sessional or part-time salaried
Other Established Ambulatory Care Settings Public Health Clinics In many parts of the United States, local government provides ambulatory health care services in public hospitals, through local health departments (LHDs), and in other venues. LHDs operate an array of special clinics (National Association of County and City Health Officials [NACCHO], 2016). In 2016, they provided many services, important among them clinics for tuberculosis control (often providing treatment as well as case finding and contact investigation services), child health (where immunizations, examinations, and education on child rearing are provided), prenatal care, sexually transmitted disease control, and certain mental health problems. In recent years, some public health agencies have broadened the scope of their services to include family planning, chronic disease detection, and general primary care. Precisely how much care is provided is not known. Although there are more than 2,000 LHD units providing some kind of care, public health services are not a major factor in the overall ambulatory care picture (Association of State and Territorial Health Officials [ASTHO], 2006; Health Resources and Services Administration [HRSA], 2006). The provision of ambulatory care service by LHDs has been a subject of controversy ever since the practice began in the 19th century (Rosen, 1971; Winslow, 1929). Battles with the
Goldsteen74024_02_CH02_33-78_03-18-20.indd 48
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
49
private physician sector over the role of LHDs were especially fierce during the 1920s, when some LHDs developed plans to expand their general disease treatment services (Myers, Steinhardt, Mosley, & Cashman, 1968; Rosen, 1971; Winslow, 1929). The efforts of the organized representatives of U.S. physicians to stop these developments were generally met with success. To this day, LHD ambulatory care services are usually limited to those medical areas in which private physicians are not very interested (e.g., routine well-baby examinations), not especially competent (e.g., treatment, case finding, and contact investigation for sexually transmitted diseases and tuberculosis), or not available (e.g., primary care in underserved areas). Lately, there has been a diminution in organized medicine’s opposition to the involvement of LHDs in the provision of direct medical services to the poor. Some hard-pressed urban and suburban health departments have done this, especially where access to ambulatory care is limited or nonexistent.
Neighborhood and Community Health Centers In the late 1960s and early 1970s, the neighborhood health center (NHC) movement emerged on the U.S. health care scene. The NHC was based on the concepts of full-time salaried physician staffing, multidisciplinary team health care practice, and community involvement in both policy-making and facility operations (Davis & Schoen, 1978; Zwick, 1972). The movement was strongly stimulated by the federal Office of Economic Opportunity (OEO). The OEO was the lead agency for the “war on poverty” initiated by President Lyndon Johnson from 1964 to 1968. For poor people, the NHCs sought to provide one-stop shopping for comprehensive ambulatory care—a full range of preventive and rehabilitative as well as treatment services that were affordable and of high quality. The NHCs also aimed to intervene in the cycle of poverty by providing jobs and skills/career development opportunities for the residents of the communities they served. The movement did not meet with overwhelming success, in terms of patient visits provided. Conceptually, though, it was very important, leading to, among other things, the community-oriented primary care model mentioned earlier. The NHC did not represent an entirely new concept in the United States. The 19th-century freestanding urban “dispensary” was an early general ambulatory care center that primarily served the poor. Although it was organized differently, it performed some functions similar to those of the modern NHC or the community health center (CHC), the NHC’s successor. Health department ambulatory care programs developed during the last quarter of the 19th century had some elements that would also appear later in NHCs, such as districting and comprehensiveness (Rosen, 1971). The experience with prepaid group practice (PPGP) in the 1930s, 1940s, and 1950s influenced the development of the NHC movement of the 1960s and 1970s (Light & Brown, 1967). With varying degrees of vigor and success, the NHCs attempted to make multidisciplinary group practice work. Along with physicians and nurses, they employed social workers, neighborhood health workers (usually people from the area served, specially trained by the NHC with a combination of basic nursing and social service skills), and, sometimes, lawyers, all on salary. These health care teams helped patients deal with both social and medical problems. At the movement’s peak in the early 1970s, there were an estimated 200 NHCs nationally (Callan & Fein, 1972). In the mid-1970s, the Nixon and Ford administrations more narrowly defined the scope of the NHC program and renamed its facilities CHCs. The CHCs, which included many of the original NHCs, were to concentrate on the delivery of primary care services. They were to deemphasize other NHC roles, such as providing employment opportunities and training programs, stimulating social and economic development in their communities, and concerning themselves with communitywide as well as personal health problems.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 49
3/19/20 10:52 AM
50
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
By the early 1980s, there were more than 800 CHCs serving more than 4.5 million people (Sardell, 1983), a remarkable resurgence for a program that received little publicity. By the early 1990s (Starfield, 1992), there were fewer CHCs (540), but with a total of 2,000 locations and sublocations serving close to 6 million poor people in all 50 states, the District of Columbia, and the major U.S. territories. In 2001, President George W. Bush initiated an expansion of the CHCs. As a result, by 2006, there were more than 3,800 community and migrant worker health centers providing care for more than 14.6 million people (Health Resources and Services Administration [HRSA], 2006). Since the passage of the ACA in 2010, health centers have become even more important to the nation’s health care system and have increased their number of patients served by nearly 5 million while adding more than 64,000 new full-time staff nationwide (HRSA, 2015a). Today, “health centers” refer to all the diverse public and nonprofit organizations and programs that receive federal funding under Section 330 of the Public Health Service (PHS) Act, as amended by the Health Centers Consolidated Act of 1996 (P.L. 104–299) and the Safety Net Amendments of 2002.They include Community Health Centers, Migrant Health Centers, Health Care for the Homeless Health Centers, and Primary Care Public Housing Health Centers. Health centers are characterized by five essential elements that differentiate them from other providers (HRSA, 2012): • •
• • •
They must be located in or serve a high-need community, that is,“medically underserved areas” or “medically underserved populations.” They must provide comprehensive primary care services as well as supportive services, such as translation and transportation services, that promote access to health care. Their services must be available to all residents of their service areas, with fees adjusted upon patients’ ability to pay. They must be governed by a community board with health center patients constituting a majority of members. They must meet other performance and accountability requirements regarding their administrative, clinical, and financial operations.
As of 2014, 27.9% of CHC patients were uninsured, and 92.4% had incomes below 200% of the federal poverty level (HRSA, 2015b). Racial and ethnic minorities comprised 62.2% of CHC patients. In 1999, a disproportionate share had special health care needs (11% were substance abusers, 5% were homeless, and 2.5% were HIV positive). The CHCs provide a broad range of support services, including transportation, translation, health education, nutrition, and AIDS management, and have been considered by those who use them to provide high-quality care (McAlearney, 2002). Many of the CHCs were on the brink of financial insolvency in the late 1990s, but the Bush Administration initiative to expand CHCs has eased the financial difficulties of these health care providers (Bush, 2007).
Industrial and Other Workplace Health Clinics A range of industrial health hazards exist, from traumatic injury to occupational exposure to harmful substances (e.g., silica, asbestos, lead). The number of “in-plant” health units in the United States is not known, but there are thousands of them. In small plants (fewer than 100 workers), health services are ordinarily quite rudimentary. They are often limited to a first-aid kit and arrangements with some local health facility to which injured workers may be sent. Very large plants (with more than 2,500 workers) usually have some systematic in-plant health service. Customarily, it is staffed with trained industrial nurses and part-time or full-time physicians. In a few companies, in-plant health services are comprehensive, providing employees with complete medical care for all disorders, job connected or not.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 50
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
51
The long-term trend in American industry is toward greater concentration of production in fewer large corporations. Although, at one time, it seemed that concentration might enhance the prospects for improving occupational health programs, in the 1980s, there were actually reductions in service in many large corporations in the name of cost savings (D. Parkinson, personal communication, October 25, 1990). This situation may be changing because of increasing recognition that health is an important factor in worker productivity and the workplace is a viable and practical place to begin (National Institute for Occupational Safety and Health [NIOSH], 2015).
School Health Clinics In 2013, there were more than 77.8 million students in primary and secondary schools, colleges, and universities, both private and public. More than 41 million were enrolled in primary schools and 16.6 million in secondary schools (U.S. Census Bureau, 2013). Almost all educational institutions provide some type of organized ambulatory health service. About half of the school health services are run by LHDs, the balance being run by boards of education, on their own or in cooperation with the LHD. Very little disease treatment is done in school health programs. Usually carried out by school nurses, the work of most of these programs is confined to case finding and prevention for certain chronic or epidemic diseases, for example, screening for vision and hearing difficulties and providing immunizations. Referrals are made to physicians for diagnosis and treatment, should they be indicated. College and university health services are more likely to provide general diagnostic and treatment care. Some pay special attention to mental and substance-abuse problems. This is changing in some schools because of increasing numbers of children with chronic diseases, such as asthma and diabetes, who frequently need medical attention during the day (U.S. Department of Health and Human Services [DHHS], 2011; Perrin, Bloom, & Gortmaker, 2007).
Emerging and Expanding Ambulatory Settings Telehealth/Telemedicine Although the next level of care after self-care has historically been a“trip to the doctor”or“office visit,”telehealth/telemedicine has recently become much more practical and affordable with the continuing decline in costs and increased performance of enabling technologies, such as highspeed computers and networking. New companies, such as Teledoc, and hospitals are now offering these services as a more convenient and lower-cost modality for diagnosing patients whose ailments do not appear to require physical examination. Additionally, “apps” and other home monitoring devices are blurring the lines between self-care, wellness, and medical care.
Physician Home Visits Although the “house call” was thought to be relegated to a delivery system of another time, there has been some resurgence in physician home visits as a convenience or tool to improve access for those with limited modality. Although technology has made it more practical for physicians to perform increasingly sophisticated examinations outside dedicated clinical space, the economics of this model are challenging, given physician salaries, travel times, and projected physician supply and shortages (Yao, Ritchie, Camacho, & Leff, 2016).
Retail Pharmacies “A pharmacy is a facility whose primary function is to store, prepare and legally dispense prescription drugs under the professional supervision of a licensed pharmacist” (National Uniform Claim Committee [NUCC], 2019). In the United States—and many Western countries—prescribing and dispensing drugs are two separate acts carried out by two different health practitioners. This separation of duties—a physician who diagnosis the patient and a
Goldsteen74024_02_CH02_33-78_03-18-20.indd 51
3/19/20 10:52 AM
52
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
pharmacist who prepares and dispenses the indicated remedy—dates back to the 11th century, and it is believed to reduce the conflict of interest (Trap, 2019). As this separation persists today across most of the sites of care, pharmacies exist in not just community care settings but more acute care settings such as hospitals, long-term care facilities, and infusion centers (discussed later). In the community, most prescriptions are filled by retail pharmacies and mail-order pharmacies with compounding pharmacies and, almost by definition, specialty pharmacies filling a small minority (see Figure 2.4).² Expenditures for retail drug prescriptions were about US$329 million in 2016, or about 13% of health care spending (CMS, 2017). Retail pharmacies are defined as pharmacies designed to serve a “local patient population in accordance with federal and state law; counsel patients and caregivers (sometimes independent of the dispensing process); administer vaccinations; and provide other professional services associated with pharmaceutical care such as health screenings, consultative services with other health care providers, collaborative practice, disease state management, and education classes” (NUCC, 2019). Retail pharmacies and pharmacists are increasingly being depended upon to engage patients with their unique knowledge of complex pharmaceuticals with complicated side effects and interactions. Increasingly, they are assuming this expansive designation. In 2015, 4 billion prescriptions, or 12.7 prescriptions per-capita, were filled at community pharmacies in the United States [1], and more than 90% of Americans live within 2 miles to one of these pharmacies [2]. Pharmacies are also expanding their operations beyond dispensing to include preventative care, such as health screenings and medication therapy management [3, 4], especially at retail chains. Thus, pharmacies supply and facilitate access to prescription medications and are a vital, and increasingly important, component of health care delivery in the United States. (Qato et al., 2017) As another example, CVS Health has announced plans to expand new stores that will “provide dietitians, help people monitor chronic diseases and add community rooms that can be used for yoga classes. The drugstore chain, which quit selling tobacco several years ago, said it will open 1,500 of these so-called HealthHub stores nationally by the end of 2021” (Murphy, 2019).
Ambulatory Surgery Centers and Other Expanding Ambulatory Care Settings From the 1980s onward, hospitals have been developing community-based facilities both within their walls and at satellite sites. These facilities provide services that traditionally have
Chain Independent Mass retail Food Clinic Government
FIGURE 2.4 Types of retail pharmacies. Source: Data from Qato, D. M., Zenk, S., Wilder, J., Harrington, R., Gaskin, D., & Alexander, G. C. (2017). The availability of pharmacies in the United States: 2007–2015. PLoS One, 12(8), e0183172. Retrieved from https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0183172
Goldsteen74024_02_CH02_33-78_03-18-20.indd 52
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
53
required inpatient stays but, with advances in medical practice and technology, can now safely be offered on an outpatient basis (Anderson, 1990; Ermann & Gabel, 1985; Lin, Yang, Wen, & Chang, 2006; Podolsky, 1996). Such facilities include satellite OPDs, which may separate specialty clinics as do many hospitals, or may be more like a CHC; comprehensive diagnostic centers for laboratory, x-ray, and related testing; and ASCs (Medical Group Management Association, 2002), where surgery that can be safely performed on an outpatient basis is done. ASCs are quickly increasing in number, and many of them are part of hospital systems. Surgeries in these settings are replacing inpatient surgeries. There were more than 5,300 ASCs in the United States in 2012. They perform 23 million surgeries annually, and Medicare approves them to perform more than 3,500 procedures (Ambulatory Surgery Center Association [ASCA], 2012). New technologies, such as arthroscopic surgery, which allow for the use of noninvasive or minimally invasive procedures, certainly are at the center of this rapid growth. The payers of care strongly support this transformation because the cost of surgery done in an outpatient setting is much less expensive than that for inpatient surgery. Patients generally view ambulatory surgery favorably because of a better physical environment, the ease of access that many centers provide, and the overriding factor that the patients do not have to be admitted to a hospital. Although they began as physician-owned enterprises, hospitals and others operate ASCs: Given the history of their involvement in making ASCs a reality, it is not surprising that physicians continue to have at least some ownership in virtually all (90%) ASCs. But what is more interesting to note is how many ASCs are jointly owned by local hospitals that now increasingly recognize and embrace the value of the ASC model. According to the most recent data available, hospitals have ownership interest in 23% of all ASCs and 2% are owned entirely by hospitals. (ASCA, 2019) Other health services besides surgery that are increasingly being taken out of the hospital and often, but not always, owned by a physician or physician practice are diagnostic imaging centers and clinical laboratories. Also, urgent care centers have grown out of physician practices wanting to offer extended hours on a walk-in basis and hospitals wanting to provide an alternative to their more expensive ED.
HOSPITALS: INPATIENT ACUTE CARE The most intensive health care is provided in hospitals, and although less than 10% of the population experience an overnight stay in a hospital during a 12-month period (Lucas & Benson, 2018), hospitals accounted for about one-third of national health expenditures (the largest portion) in 2017, a trend that goes back until at least 1960 (CMS, 2018). This section provides a brief historical background on this important health care setting and an overview of hospital utilization and then describes the current structure of hospitals.
Historical Background Historically, the hospital has been the institutional center of the health care delivery system (Knowles, 1965). The word hospital shares its Latin root with the words hostel and hotel. Most frequently under church sponsorship, the institution originated in the Middle Ages primarily as a place of refuge for the poor, the sick, and the weary, rather than as a place for treating illness. As recently as the turn of the 19th century, a person entering a hospital had less than a 50% chance of leaving it alive. By the beginning of the 21st century, most
Goldsteen74024_02_CH02_33-78_03-18-20.indd 53
3/19/20 10:52 AM
54
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
patients could expect to benefit from a hospital stay—about 97% of patients expect to leave the hospital alive. Even though the quality of care could still be significantly improved (Institute of Medicine [IOM], 2000, 2002), the hospital has evolved from a place where a person went to spare his family the anguish of watching him or her die to a multiservice institution providing interdisciplinary medical care, ambulatory as well as in bed (Freymann, 1974; Rosenberg, 1979; Stern, 1946). In the European settlements in America, the earliest hospitals were infirmaries attached to poorhouses. (A poorhouse was an institution operated by a local governmental authority to house persons who were unemployed, orphans or abandoned children, the mentally ill or retarded, the ill elderly, and those otherwise incapable of self-care.) The first of these was established at Henricopolis in Virginia (1612), and the second in 1732 in Philadelphia (Stern, 1946). The first public institution established solely for the care of the sick was the “almshouse” built in 1736 on Manhattan Island. It was located north of midtown, at a place called Belle Vue (“beautiful vista”). In a reverse of the earlier pattern, the New York City public workhouse (a later version of the poorhouse) was moved to the grounds of the almshouse in 1816. New York City’s famous Bellevue Hospital is still at that location. Nongovernmental charity (private, voluntary) hospitals to care for the sick poor were first established in the American colonies during the 18th century (Freymann, 1974, pp. 22–24). The first was the Pennsylvania Hospital in Philadelphia, founded by Benjamin Franklin in 1751. By 1873, there were an estimated 178 hospitals in the United States, many of them solely for the mentally ill (Stevens, 1971, p. 52). At about that time, however, the development of modern medical science was under way, and a general hospital building boom began. By the early 20th century, a patient admitted to a general hospital did, in fact, have a better-than-even chance of getting out alive. That milestone was achieved largely through the development of general hospital hygiene, surgical asepsis (keeping surgical sites scrupulously clean and free of microbial contamination), and surgical anesthesia. After the turn of the 20th century, overall medical care quickly became far too complex for average physicians to be able to carry their entire armamentarium in a black bag. By 1910, general hospitals had been established in many communities. There were nearly 4,400 of them, with a total of 421,000 beds (Stevens, 1971, p. 52). It was the rapid advance of medical science that led to the expansion of the hospital system and of individual hospitals, as well as to the evolution of hospitals as the center of the medical care system (MacEachern, 1962; Rosenberg, 1979). The mold from which today’s health care system was cast took its shape around 1850s. There were still relatively few general hospitals or health care facilities of any type in either Great Britain (our most important medical organizational forebear) or the fledgling United States, but the institutional organization of health care was already firmly established. The physical separation, for the most part, as well as separate provision for administration and staffing of the curative services for acute, chronic, and psychiatric illnesses became firmly established in the 19th century. That very strong precedent continues to control the physical and administrative design of the health care delivery system even when all three components have a common source of support, as they do now in Britain.
Present-Day Hospitals The American Hospital Association (AHA) is the primary association that represents and coordinates among hospitals, health systems, and other related organizations. In its role to represent the hospital sector, it surveys nearly all hospitals in the United States each year. Using this survey, a detailed overview of each hospital is provided in the AHA Guide, whereas summaries are available in the companion AHA Hospital Statistics. This chapter utilizes AHA Hospital Statistics 2019, which contains information from the AHA’s 2017 annual survey of hospitals.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 54
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
55
The AHA classifies hospitals as one of four types based on the primary function of its diagnostic and therapeutic services (AHA, 2019b): • • • •
General: for patients presenting with a variety of medical conditions Special: for patients who have specified medical conditions Rehabilitation and chronic disease: for handicapped or disabled individuals requiring restorative and adjustive services Psychiatric: for patients who have psychiatric-related illnesses
Most hospitals are General, accounting for 4,680 of the 6,210 hospitals in the United States in 2017. The next largest group is Psychiatric, with 631 hospitals in 2017. Another important characteristic of hospitals besides their diagnostic and therapeutic purpose is control and ownership. The AHA defines control as “The type of organization responsible for establishing policy concerning the overall operation of hospitals. The three major categories are government (including federal, state, and local); nongovernment (nonprofit); and investor-owned (for-profit)” (AHA, 2019b, p. 205). Investor-owned (formerly called proprietary) hospitals may be owned by an individual, a partnership, or a corporation. Nongovernment, nonprofit hospitals were historically called voluntary. In addition to diagnostic and therapeutic purpose and control, the length of patient stay is an important distinguishing feature of hospitals. Short-term hospitals, with patient stays under 30 days on average, predominate over long-term hospitals. Long-term hospitals have an average length of stay (LOS) of 30 days or more. The AHA has a descriptor that encompasses the majority of hospitals: the community hospital. The designation community hospital is based on a hospital’s diagnostic and therapeutic purpose, control and ownership, and length of patient stay. It is defined as follows: All nonfederal, short-term general, and special hospitals whose facilities and services are available to the public. (Special hospitals include obstetrics and gynecology; eye, ear, nose and throat; rehabilitation; orthopedic, and other individually described specialty services.) Short-term general and special children’s hospitals are also considered to be community hospitals. (AHA, 2019b, p. 205) The key to understanding the current hospital sector is knowing the role of the community hospital (AHA, 2019a). Community hospitals clearly dominate the hospital sector in number of hospitals and percent of the total. • •
Of the 6,210 hospitals of all types, most hospitals were nonfederal (96.7% or 6,002 hospitals). Of the 6,002 nonfederal hospitals, the 5,262 community hospitals accounted for 87.7% of them (see Table 2.11).
They are also dominant in other ways, including the staffed beds, admissions, and expenses. In 2017, community hospitals accounted for: • • •
85.8% of total staffed beds in all U.S. hospitals (798,921 of the 931,203 total staffed beds) 94% of total admissions in all U.S. hospitals (34,305,620 of the 36,510,207 total admissions) 91.1% of total expenses for all U.S. hospitals (US$966 billion of US$1.060 trillion total expenses)
Goldsteen74024_02_CH02_33-78_03-18-20.indd 55
3/19/20 10:52 AM
56
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 2.11 Hospitals by Type and Ownership, United States, 2017 Number of Hospitals
Percentage of All Hospitals
Percentage of Community Hospitals
All hospitals
6,210
100.0
—
Community hospitals
5,262
84.7
—
Nongovernment (not-for-profit)
2,968
—
56.4
Investor-owned (for-profit)
1,322
—
25.1
State and local government
972
—
18.5
Federal government hospitals
208
3.3
—
Nonfederal psychiatric hospitals
620
10.0
—
Other hospitalsa
120
2.0
—
a Other hospitals are defined as nonfederal long-term care hospitals and hospital units not accessible to the general public (e.g., prison hospital, school infirmary, or other hospital unit within an institution). Long-term care hospitals include other hospitals with an average length of stay of 30 days or more. (Long-term hospitals may be defined by different methods.)
SOURCE: Data from the AHA. (2019). Fast facts on U.S. hospitals. Retrieved from https://www.aha.org/statistics/fast-facts-us-hospitals
Other significant features of community hospitals in 2017 are their control and ownership, and their system and network affiliations. Of the 5,262 community hospitals in 2017, • • •
56.4% were not-for-profit (n = 2,968). 18.5% were state- or local-government owned (n = 972). 25.1% were for-profit (n = 1,322; see Table 2.11).
In 2017, hospitals continued the trend toward consolidation in networks and systems. The AHA defines hospitals in a network as “Hospitals participating in a group that may include other hospitals, physicians, other providers, insurers, and/or community agencies that work together to coordinate and deliver a broad spectrum of services to the community” (AHA, 2019b, p. 208). Hospitals in a system are defined as “Hospitals belonging to a corporate body that owns and/or manages health provider facilities or health-related subsidiaries; the system may also own non-health-related facilities” (AHA, 2019b, p. 208). These are not mutually exclusive categories. A hospital can be in both a system and a network. • •
In 2017, 66.4% of community hospitals were part of a hospital system, compared to 62% in 2012 (AHA, 2018, Table 3). In 2017, 33.2% of community hospitals were in a network, compared to 30.2% in 2012 (AHA, 2018, Table 3).
The trend toward creating hospital systems accelerated in the 1990s. In 2003, Cuellar and Gertler wrote, The past decade has seen profound changes in how the hospital industry organizes itself. Standing out among these changes has been the extensive consolidation of
Goldsteen74024_02_CH02_33-78_03-18-20.indd 56
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
57
hospitals through merger and the rising importance of hospital systems. Researchers either have tended to focus on the effects of merger transactions, ignoring system acquisitions, or they have portrayed system formation as primarily an issue of hospital ownership conversion, thereby focusing on the expansion of national, for-profit systems. Relatively little attention has been paid to the rising local presence of hospital systems and how this could affect consumers and health care markets. Hospital consolidation can occur through either merger or acquisition. Mergers—transactions in which separate hospitals come together under a shared license—typically occur among hospitals located near one another. Acquisitions occur when joining hospitals retain their licenses but are owned by a common governing body; they can occur among hospitals that are near or far away. (Cuellar & Gertler, 2003, p. 77)
Community Hospitals Within the category of community hospitals, Table 2.12 displays their basic characteristics by control—not-for-profit, for-profit, and state and local. Of note is that the not-for-profit hospital predominates among community hospitals. In 2017, not-for-profit community hospitals had the greatest number of hospitals, beds, and annual admissions and the largest average daily census. They also had the lowest average LOS (see Table 2.12). The community hospital is the workhorse of the hospital system and has been, historically. However, community hospitals continuously adapt to major political, economic, and technological changes in the United States. A review of changes in basic characteristics over the past 40 years provides insight. Table 2.13 displays trends since 1976 in the number of hospitals and beds, control of hospitals, and other basic characteristics. Although annual admissions to community hospitals rose slightly over the 40-year period (33.9 to 34.3 million, a 1% increase), community hospitals declined in number, size, average daily census, and LOS. These downward trends are largely the result of patients spending less time in the hospital than in prior years (shorter LOS). • • •
The number of community hospitals has decreased since 1976 from 5,857 to 5,262, a 10% decline. Total number of beds in community hospitals decreased from 956,000 to 798,000, a 16% drop. The average daily census also dropped, from 713,000 to 510,000, 28% decline. This followed a similar decline in average length of patient stay (7.7 days in 1976 to 5.4 days in 2017).
TABLE 2.12 Basic Characteristics of U.S. Community Hospitals, by Control, 2017 Characteristic Number of hospitals Beds Annual admissions Average daily census Average length of stay (days)
Not-for-Profit
For-Profit
State and Local
2,968
1,322
972
545,129
142,386
111,406
24,788,938
5,432,727
4,083,955
357,258
81,349
71,516
5.3
5.5
6.4
SOURCE: Adapted from American Hospital Association. (2019b). Hospital statistics, 2019. Chicago, IL: Health Forum.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 57
3/19/20 10:52 AM
58
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 2.13 Basic Characteristics of U.S. Community Hospitals, 1976 to 2017 Characteristic
1976
1997
2017
Percent Change 1976–2017
Total number of hospitals
5,857
5,057
5,262
−10.2
Not-for-profit hospitals
3,345
3,000
2,968
−11.3
Investor-owned hospitals
752
797
1,322
75.8
State and local government hospitals
1,760
1,260
972
−44.8
956,000
853,000
798,000
−16.5
33,979,000
31,577,000
34,306,000
+1.0
713,000
528,000
510,000
−28.5
Beds Annual admissions Average daily census Average length of stay (in days) Outpatient visits FTE personnel Total expenses (in millions of dollars; US$) Total expenses adjusted per inpatient day (in dollars; US$)
7.7
6.1
5.4
−29.9
201,247,000
450,140,000
786,077,000
290.6
2,475,000
3,790,000
5,215,000
110.7
45,240
305,763
966,204
2,035.7
153
1,033
2,424
1,484.3
FTE, full-time-equivalent. SOURCE: Adapted from American Hospital Association. (2019b). Hospital statistics, 2019. Chicago, IL: Health Forum. (Table 1).
Even though the community hospital sector has fewer hospitals and fewer staffed beds and spends fewer days caring for inpatients now, the expenses have gone up dramatically. • •
Total expenses (in millions of dollars) were 21.3 times greater in 2017 than in 1976 (US$45,240 vs. US$966,204). Total expenses adjusted per inpatient day (in dollars) were 15.8 times higher than in 1976 (US$153 vs. US$2,424).
This discrepancy between demand and expenses may be partially explained by the large increase in personnel and outpatient visits in the community hospital sector. • •
The number of full-time-equivalent (FTE) personnel grew from 2,475,000 to 5,215,000, a 110% increase in staff. Outpatient visits in the clinics of community hospitals rose from 201,247,000 to 786,077,000, a 290% increase.
Another trend is related to control of community hospitals. Not-for-profit hospitals still predominate, but investor-owned hospitals have become more numerous and state and local hospitals have declined precipitously since 1976. In the period between 1976 and 2017, •
• •
Investor-owned hospitals doubled in their percent of the total number of community hospitals—from 12.8% in 1976 to 25.1% in 2017. They were the only category that increased their percent over this period. State and local hospitals declined as a percent of the total number of community hospitals from 30% to 18.5%. Not-for-profit hospitals saw a small decline from 57.1% to 56.4% of the total number of community hospitals.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 58
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
59
Special Categories of Community Hospitals Rural Hospitals In 2017, 35.6% of community hospitals were rural, and 64.4% were urban or suburban. Rural community hospitals are vital in the sparsely populated regions of the country both to meet health care needs and for economic stability.Yet, they are particularly vulnerable because the populations they serve are not sufficiently large to support even small hospitals. Hospitals are classified by the “number of beds regularly maintained (set up and staffed for use) for inpatients as of the close of the reporting period. This excludes newborn bassinets” (AHA, 2019b, p. 204). The AHA groups hospitals into eight categories based on bed size: six to 24 beds, 25 to 49 beds, 50 to 99 beds, 100 to 199 beds, 200 to 299 beds, 300 to 399 beds, 400 to 499 beds, and 500 beds or more. In 2017, rural community hospitals had an average of 60 beds, with 62% of hospitals having fewer than 50 beds. For these reasons, over 70% of rural hospitals had implemented telemedicine by 2017 (AHA, 2019b).
Teaching Hospitals In the past, the AHA used the term teaching hospital to refer to hospitals providing undergraduate or graduate education for medical students and medical house staff (interns, residents, and specialty fellows). The term was not applied to hospitals with teaching programs for other health care providers. Although the AHA formerly presented data for the teaching hospitals separately, those data are now subsumed under the general categories of hospital, of which the teaching hospitals are a part. In one of the last years for which teaching hospital data were presented separately, 1989, there were 1,054 teaching community hospitals (about 19% of all community hospitals), with 393,000 beds (more than 42% of all beds in community hospitals; AHA, 1990, Tables 6 and 8). More recently, only about 20% of the U.S. hospitals were considered teaching hospitals, but they provided about 50% of hospital-based services (AHA, 2013).
Public General Hospitals The public general hospital was defined by the Commission on Public General Hospitals of the AHA (1978, p. v) as “short-term general and certain special hospitals excluding federal (those operated by the Department of Defense and the Department of Veterans Affairs), psychiatric, and tuberculosis hospitals that are owned by state and local governments.” Public general hospitals provide care for many persons unable to be treated elsewhere: the poor, the uninsured, the homeless, alcoholics and other substance abusers, disruptive psychiatric patients, and prisoners. In certain areas, such as isolated rural areas, the public general hospital is also the only source of care for patients with special medical problems, regardless of income: the badly burned, at-risk newborns, high-risk mothers, and victims of criminal or noncriminal life-threatening trauma. Although only a minority of hospitals are under public ownership today, in a nation without universal health care coverage, they play an important role beyond their numbers (Felt-Lisk, McHugh, & Howell, 2002; Friedman, 1997; Huang, Silbert, & Regenstein, 2005; May, 2004; Verghese, 1996). The public hospital sector is shrinking. In 1975, there were 1,761 state and local general hospitals with 210,000 beds. As of 1995, there were 1,350 state and local general hospitals, with a total of about 157,000 beds. By 2017, the numbers had shrunk to 972 state and local hospitals, with about 111,000 beds. The average daily census for these hospitals had declined from 148,000 in 1975, to 100,000 in 1995, and to 72,000 in 2017 (AHA, 2019b). Despite the low occupancy rate, public general hospitals are still the primary health services resource for the nation’s poor and for those with no health insurance. Compared to not-for-profit and investor-owned hospitals, they are far more likely to care for uninsured persons, persons living in low-income areas, and those covered by Medicaid. They provide a large amount of unreimbursed care (Fraze, Elixhauser, Holmquist, & Johann, 2010). Yet as of
Goldsteen74024_02_CH02_33-78_03-18-20.indd 59
3/19/20 10:52 AM
60
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
2002, these hospitals were in serious trouble. Noting the shrinking number of public general hospitals, Haugh (2002), writing in the AHA’s Hospitals and Health Networks, highlighted their financial straits: [In] an era of tax cuts and disappearing [budget] surpluses, the well is dry. Officials are recommending deep austerity measures ... [that] might foreshadow a looming crisis throughout the nation. The U.S. health care safety net is frayed; without changes, critics fear, it will unravel—and drag other hospitals down with it. (p. 44) As the ax falls on mental health funding, public hospitals’ EDs fill the gap. In many areas, officials recommend privatizing these hospitals.
Health Conditions Treated in Community Hospitals The health conditions treated in a hospital are those requiring specialized diagnostic and treatment resources and the associated health professionals to administer them. Hospitalizations—their number and diagnosis—are not random events. They reflect the health status of the population served and the demographic and other characteristics of that population. Hospitalizations may be monitored for trends, and these trends may be used to predict and plan the demand for hospital services. Following is a discussion about the most frequent diagnoses for hospitalizations in 2005 and 2014 using data provided by the Agency for Healthcare Research and Quality (AHRQ), an authoritative source of information on inpatient hospitalizations at community hospitals (excluding rehabilitation and long-term acute care hospitals). Each year, AHRQ collects data on these inpatient stays through the Healthcare Cost and Utilization Project (HCUP), National Inpatient Sample (NIS). “The NIS is the largest publicly available all-payer inpatient health care database in the United States, yielding national estimates of hospital inpatient stays” (HCUP, 2018). Table 2.14 lists the most common inpatient diagnoses in 2005 and 2014 from HCUP’s NIS. (At the time of this publication, 2014 was the most recent data publicly available from HCUP; McDermott, Elixhauser, & Sun, 2017). These 12 conditions accounted for 44.7% of hospital stays in 2005 and 44.9% in 2014. There are several findings to note in Table 2.14. Overall, there was significant change over this nine-year period, which reflects the variability in health and health care. First, some diagnoses had the same importance in 2005 and in 2014. • • •
Pregnancy and childbirth and the care of newborns were the number 1 and 2 causes of inpatient stays in both years. This has been true historically, as well. Congestive heart failure ranked number 5 in both years. Acute myocardial infarction ranked number 10 in both years.
Two conditions were in the top 10 in 2005, but were not on the list at all in 2014. These were: • •
Coronary atherosclerosis and other heart disease Nonspecific chest pain
Two conditions ranked in the top 10 in 2014, but were not on the list at all in 2005. These were: • •
Septicemia, which increased an enormous 192% between 2005 and 2014 Complication of device/implant/graft with an increase of 6.2% over 2005
Two conditions were among the most common diagnoses in both 2005 and 2014, but increased by a large percentage between 2005 and 2014. These were: • •
Osteoarthritis, with a 49.5% increase over 2005 Mood disorders, with a 23.2% increase over 2005
Goldsteen74024_02_CH02_33-78_03-18-20.indd 60
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
61
TABLE 2.14 Most Common Diagnoses for Hospital Stays Ranked by Their Frequency, 2005 and 2014 2005 Principal Diagnosis
Rank
All stays
Number of Stays
2014 Percent Rank
Number of Stays
Percentage Change Percentage in Number of Stays
37,843,000
100.0
35,358,800
100.0
−6.6
Pregnancy, childbirth
1
4,564,000
12.1
1
4,153,700
11.7
−9.9
Newborns, neonates
2
4,288,300
11.3
2
3,954,100
11.2
−8.5
Septicemia
—
518,000
1.4
3
1,514,100
4.3
192.3
Osteoarthritis
7
715,900
1.9
4
1,070,500
3.0
49.5
Congestive heart failure
5
1,053,100
2.8
5
901,400
2.5
−14.4
Pneumonia
3
1,303,900
3.4
6
882,700
2.5
−32.3
Mood disorders
8
690,900
1.8
7
851,100
2.4
23.2
Cardiac dysrhythmias
9
674,200
1.8
8
665,600
1.9
−1.3
Complication of device/ implant/graft
—
596,000
1.6
9
633,000
1.8
6.2
Acute myocardial infarction
10
641,700
1.7
10
608,800
1.7
−5.1
Coronary atherosclerosis and other heart disease
4
1,076,100
2.8
—
397,700
1.1
−63.0
Nonspecific chest pain
6
798,200
2.1
—
295,800
0.8
−62.9
NOTE: Number of stays is rounded to the nearest 100. Percent is based on unrounded values. Maternal and neonatal stays are grouped by Major Diagnostic Category (MDC 14: Pregnancy, Childbirth, and Puerperium and MDC 15: Newborn and Other Neonates [Perinatal Period]). Nonmaternal and nonneonatal principal diagnoses are grouped using the Clinical Classification Software (CCS). Minor discrepancies with other data sources such as HCUPnet may appear because of differences in the coding systems in use at the time analyses were performed. Dashes indicate that the diagnosis was not ranked among the 10 most common. SOURCE: McDermott, K. W., Elixhauser, A., & Sun, R. (2017, June). Trends in hospital inpatient stays in the United States, 2005–2014 (HCUP Statistical Brief #225). Rockville, MD: Agency for Healthcare Research and Quality. Retrieved from www.hcup-us.ahrq .gov/reports/statbriefs/sb225-Inpatient-US-Stays-Trends.pdf
Note: In certain cases, these data on the number of admissions differ somewhat from those provided by the AHA because of different exclusion and inclusion criteria. The diagnoses in Table 2.14 include inpatient stays for all people in 2005 and 2014, including all ages, genders, races, ethnicities, and so forth. A table that presents the most common diagnoses by age and other demographic characteristics discloses a different set of health conditions accounting for most frequent hospital visits. Table 2.15 contains information from HCUP’s NIS for the most common diagnoses by age, excluding pregnancy and newborn inpatient stays (McDermott et al., 2017). The comparison of Tables 2.14 and 2.15 demonstrates the impact of age on hospitalization. For example, comparing the most common diagnoses for all inpatient stays in 2014 (Table 2.14) to those in Table 2.15 discloses marked age-specific differences. For example: • • •
In Table 2.14, osteoarthritis was ranked 4 in 2014, but was among the top five diagnoses in Table 2.15, only for 45- to 74-year-olds. In Table 2.14, mood disorders were ranked 7, while they were not among the top five diagnoses in Table 2.15, except for persons under 65 years. In Table 2.14, congestive heart failure was ranked 5, but it was not among the top five diagnoses in Table 2.15, except for persons over 65 years.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 61
3/19/20 10:52 AM
62
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 2.15 Top Five Nonmaternal, Nonneonatal Principal Diagnoses for Hospital Stays, by Age Group, 2005 and 2014 2005
2014
Rank Principal Diagnosis
Number of Stays Percentage Principal Diagnosis
Number of Stays
Percentage
Ages 0–17 Years
6,814,500
5,595,100
100.0
1
Pneumonia
179,800
2.6
Mood disorders
117,200
2.1
2
Asthma
147,300
2.2
Asthma
103,300
1.8
3
Acute bronchitis
139,200
2.0
Pneumonia
88,200
1.6
4
Fluid and electrolyte disorders
123,400
1.8
Acute bronchitis
85,700
1.5
5
Appendicitis and other appendiceal conditions
86,800
1.3
Epilepsy, convulsions
63,800
1.1
Ages 18–44 Years
9,718,900
100.0
8,714,900
100.0
1
Mood disorders
352,200
3.6
Mood disorders
405,500
4.7
2
Schizophrenia and other psychotic disorders
190,600
2.0
Schizophrenia and other psychotic disorders
197,700
2.3
3
Skin and subcutaneous tissue infections
162,100
1.7
Septicemia
189,100
2.2
4
Spondylosis, intervertebral disc disorders, other back problems
162,000
1.7
Diabetes mellitus with complications
166,100
1.9
5
Nonspecific chest pain
150,800
1.6
Skin and subcutaneous tissue infections
152,700
1.8
100.0
Ages 45–64 Years
8,372,600
100.0
8,709,300
1
Coronary atherosclerosis and other heart disease
447,000
5.3
Osteoarthritis
444,000
5.1
2
Nonspecific chest pain
375,500
4.5
Septicemia
440,600
5.1
3
Osteoarthritis
263,400
3.1
Mood disorders
257,500
3.0
4
Pneumonia
261,300
3.1
Spondylosis, intervertebral disc disorders, other back problems
238,700
2.7
5
Spondylosis, intervertebral disc disorders, other back problems
257,900
3.1
Complication of device, implant, or graft
233,600
2.7
100.0
5,150,500
100.0
Ages 65–74 Years
4,748,600
100.0
1
Coronary atherosclerosis and other heart disease
297,500
6.3
Osteoarthritis
381,700
7.4
2
Osteoarthritis
234,100
4.9
Septicemia
317,700
6.2
3
Congestive heart failure, nonhypertensive
221,000
4.7
Congestive heart failure, nonhypertensive
195,400
3.8 (continued)
Goldsteen74024_02_CH02_33-78_03-18-20.indd 62
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
63
TABLE 2.15 Top Five Nonmaternal, Nonneonatal Principal Diagnoses for Hospital Stays, by Age Group, 2005 and 2014 (continued) 2005 Rank Principal Diagnosis
2014
Number of Stays Percentage Principal Diagnosis
Number of Stays
Percentage
4
Pneumonia
215,700
4.5
Chronic obstructive pulmonary disease and bronchiectasis
171,600
3.3
5
Chronic obstructive pulmonary disease and bronchiectasis
174,400
3.7
Cardiac dysrhythmias
167,900
3.3
Ages 75+
8,138,200
100.0
7,177,300
100.0
1
Congestive heart failure, nonhypertensive
565,600
6.9
Septicemia
543,700
7.6
2
Pneumonia
533,700
6.6
Congestive heart failure, nonhypertensive
451,400
6.3
3
Cardiac dysrhythmias
301,000
3.7
Pneumonia
335,200
4.7
4
Coronary atherosclerosis and other heart disease
280,400
3.4
Cardiac dysrhythmias
281,600
3.9
5
Acute cerebrovascular disease
245,700
3.0
Acute cerebrovascular disease
254,300
3.5
NOTE: Number of stays is rounded to the nearest 100. Percentage is based on unrounded values. Principal diagnosis is grouped using the CCS. Minor discrepancies with other data sources such as HCUPnet may appear because of differences in the coding systems in use at the time analyses were performed. SOURCE: McDermott, K. W., Elixhauser, A., & Sun, R. (2017, June). Trends in hospital inpatient stays in the United States, 2005–2014 (HCUP Statistical Brief #225). Rockville, MD: Agency for Healthcare Research and Quality. Retrieved from www.hcup-us.ahrq .gov/reports/statbriefs/sb225-Inpatient-US-Stays-Trends.pdf
Mention should be made of septicemia, which is a serious and potentially fatal condition. Septicemia is a bacterial infection that spreads into the bloodstream. Sepsis is the body’s response to that infection, when the immune system produces whole-body inflammation. Septicemia and sepsis are often used interchangeably. Hamm, Blaine, Salavaci, and Jacoby (2018) report on sepsis: … the incidence of sepsis continues to be on the rise according to three decades of epidemiological data. Readmissions, mortality, and length of stay were all higher among septic patients when compared to patients treated for other conditions. The cost of treating sepsis is remarkably high and exceeds the cost of treating patients with congestive heart failure and acute myocardial infarction. The overall cost of sepsis is reflective of not only the cost of initial hospitalization but also the postdischarge care costs, including postsepsis syndrome and cognitive and functional disabilities that require a significant amount of health care resources long term. (p. 90) In 2005, septicemia was not ranked among the most common diagnoses for hospital stays. Yet by 2014, it was ranked number 3, just behind pregnancy and newborn stays—a 192% increase in nine years (see Table 2.14). Furthermore, in 2014, septicemia was a major cause of inpatient visits among all age groups except 0 to 17—ranked 3 for persons 18 to 44 years;
Goldsteen74024_02_CH02_33-78_03-18-20.indd 63
3/19/20 10:52 AM
64
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
ranked 2 for persons 45 to 64 years; ranked 2 among those 65 to 75 years; and ranked 1 among persons aged 75 years and older (see Table 2.15). This extraordinary finding is an example of how demand for hospital services can change rapidly, without a full understanding of causes. It also illustrates the importance of data to monitor trends needed for effective planning.
Community Hospital Organization As the modern hospital has grown in the breadth and complexity of services offered, so has the complexity of its organizational structure. By Joint Commission standards, there should be three leadership groups: a governing body (typically a “board of directors”), a chief executive and other senior managers (often referred to as the “C-suite”), and the leaders of the medical staff. The medical staff should be accountable to the governing body as well as self-organizing (Joint Commission, 2009). Beyond that, Joint Commission standards require a chief nursing officer to whom all nurses have at least a dotted-line reporting relationship. Practically speaking, the organization must have a designated chief financial officer and supporting finance function.2 “Structure follows strategy,”as Alfred Chandler said (Chandler, 1962). Each hospital’s structure will follow based on the scale and different lines of business. A small, acute care hospital with half a dozen nursing units will necessarily have a different structure than a large, multistate integrated delivery system. Most commonly, hospital departments will fall into a few divisions: • • • • •
Administration: including common corporate functions, such as finance and human resources Nursing: clinical departments such as inpatient nursing units Ancillary services: other clinical departments, such as electrocardiology and radiology, which may serve a mix of inpatients and outpatients Support services: facility services such as plant maintenance, housekeeping, and food service Outpatient services: typically, ambulatory clinics and other outpatient-only departments
Medical Staff Organization The physician has traditionally been described both as a “guest in the hospital” and as its “primary customer.”The hospital has sometimes been described as the “doctors’ workshop” (Olson, 1983). Except when a physician chooses to run a hospital for profit, however, he or she has no personal responsibility to see that the hospital is functioning and available to provide care for his or her patients. Nor does the individual physician carry any financial liability for the success or failure of the hospital, unless, again, he or she is an owner. A physician traditionally has been largely free to order whatever tests or treatments he or she deems necessary for a particular patient. In recent years, certain limitations have been placed on this particular physician’s freedom. An example is the use by hospitals of formularies, which are limited lists of pharmaceuticals that will be provided by the hospital pharmacy for physician prescription. This is an attempt both to ensure that the medications used in the hospital are being used correctly and to keep the number of pharmaceuticals that need to be held in stock under control. Insurers may specify formularies as well, in the attempt to contain costs. Regardless of these kinds of limitations, because the individual physician orders all the hospital tests, services, and drugs provided to its patients, he or she is a major determinant of hospital costs, even though traditionally he or she has borne no personal responsibility for them. Physicians in a given specialty (e.g., cardiology/cardiac surgery, oncology/cancer surgery, or children’s services) can also influence the direction of the growth and expansion of the institution, affecting costs in another way.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 64
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
65
In the traditional hospital–medical staff arrangement, in exchange for the privilege of admitting patients, the physician participates in the self-governance of the medical staff. Physicians may have to share the load for providing care in areas of the hospital for which the medical staff accepts collective responsibility, such as the ED or outpatient clinics. A variety of medical staff patterns of organization exist. Roemer and Friedman’s (1971) review of them is still largely valid, although some elements are beginning to change. Under managed care, for example, in an arrangement called the physician–hospital organization (PHO), groups of medical staff are joining with hospital corporations to negotiate contracts with third-party payers, often a managed care organization (MCO), most often an HMO, to provide both medical and hospital services (Kongstvedt, Plocher, & Stanford, 2001). Assuming that the payments from the MCO to the PHO or HMO are made on another than fee-for-service basis, and increasingly they are (Thrall, 1996), such an arrangement does put the medical staff at some financial risk should patient utilization exceed projections. Responsible for overseeing the physicians’ clinical work are a set of medical staff committees. These include the executive committee, which provides overall coordination and sets general policy; the joint conference committee, which serves as liaison between the medical staff and the hospital’s governing board; the credentials committee, which reviews applications to join the medical staff and controls the periodic reappointment process; the infections control committee, which is responsible for preventing infections and monitoring and correcting any outbreaks that do occur; and the pharmacy and therapeutics committee, which reviews pharmaceutical agents for inclusion in the list of drugs approved for use in the hospital (i.e., those included in the formulary). There are also the tissue committee, which reviews all surgical procedures that produce “bodily tissues” the medical records committee, which is responsible for certifying the completeness and clinical accuracy of the documentation of patient care; and the quality assurance committee, which has the overall responsibility for monitoring and correcting any deficiencies in the quality of care provided by the medical staff.
Other Hospital Divisions Another principal health care organizational division besides the medical staff is nursing, which accounts for the largest number of clinical staff members in any hospital. The nonphysician diagnostic and therapeutic services, which may or may not be administratively attached to one of the medical departments, include laboratory (usually under the direction of the department of pathology); electrocardiography or EKG (usually a part of internal medicine); electroencephalography (part of neurology); radiotherapy technology (supporting diagnostic imaging); pharmacy; clinical psychology; social service; inhalation therapy (usually part of either anesthesiology or pulmonary medicine); nutrition as therapy; physical, occupational, and speech therapy (often attached to the department of rehabilitation medicine, if there is one); home health care; medical records; adult day care; screening; end-of-life/hospice services; pain management; sports medicine/fitness center; and women’s health services (AHA, 2007).
POSTACUTE CARE Postacute care includes many settings whose purpose is to restore patient health and mobility, as much as possible, after acute care for injury or illness or to provide continuing care for people with chronic conditions who can no longer live at home without assistance. Most of these settings are designated as long-term care. Other postacute care settings include long-term care acute hospitals (LTCAHs) and other specialty hospitals. They also include ambulatory rehabilitation facilities. This discussion will focus on long-term care.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 65
3/19/20 10:52 AM
66
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Long-Term Care The most common postacute care is paid, regulated long-term care.“The term long-term care encompasses a range of supportive, rehabilitative, nursing, and palliative services provided to people—from young to old—whose capacity to perform daily activities is restricted due to chronic disease or disability” (Feldman, Nadash, & Gursen, 2005, p. 201). There are five major sectors of long-term care: •
•
•
•
•
Adult day services centers In 2016, there were 4,600 adult day services centers with 286,300 participants (Harris-Kojetin et al., 2019). The National Adult Day Services Association defines them as safe, professional care settings for adults who need supervision outside the home during the day. They serve older adults, adults with dementia, and adults with disabilities requiring individualized therapeutic, social, or health services during part of the day. They provide social and some health services in community-based group settings. In serving this population, they are also providing respite for their caregivers (National Adult Day Services Association [NADSA], 2019). Home health agencies In 2016, there were 12,200 home health agencies and 4,455,700 patients were discharged from them in 2015 (Harris-Kojetin et al., 2019). According to Strahan (1996), home health care is provided to individuals and families in their place of residence to promote, maintain, or restore health or to maximize the level of independence while minimizing the effects of disability and illness, including terminal illness. These agencies are often referred to today as “hospitals without walls” because advances in technology allow dozens of complex illnesses, once treated almost exclusively in the hospital, to be treated at home. (p. 1) Hospice In 2016, there were 4,300 hospices, and 1,426,000 patients received hospice services in 2015 (Harris-Kojetin et al., 2019). Hospice care is defined as a program of palliative and supportive care services that provides physical, psychological, social, and spiritual care for dying persons, their families, and other loved ones. Hospice services are available in both the home and inpatient settings. Nursing home In 2016, there were 15,600 nursing homes with 1,347,600 residents (Harris-Kojetin et al., 2019). Nursing homes, also called skilled nursing facilities, provide a wide range of health and personal care services. Their services focus on medical care more than most assisted living facilities. These services typically include nursing care, 24-hour supervision, three meals a day, and assistance with everyday activities. Rehabilitation services, such as physical, occupational, and speech therapy, are also available.... Some people stay at a nursing home for a short time after being in the hospital. After they recover, they go home. However, most nursing home residents live there permanently because they have ongoing physical or mental conditions that require constant care and supervision (National Institute on Aging, 2019). Residential care communities In 2016, there were 28,900 residential care communities serving 811,500 residents (Harris-Kojetin et al., 2019).
Goldsteen74024_02_CH02_33-78_03-18-20.indd 66
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
67
This level of care and supervision is for people who are unable to live by themselves but who do not need 24 hour nursing care. They are considered non-medical facilities and are not required to have nurses, certified nursing assistants or doctors on staff. Other terms used to refer to this level of care are assisted living facilities, board and care homes, rest homes and that component of Continuing Care Retirement Communities (CCRCs) that provide personal care and supervision (California Advocates for Nursing Home Reform [CANHR], 2019). In 2016, the sectors differed in ownership, supply, and chain status. “The majority of home health agencies, hospices, nursing homes, and residential care communities were for profit, while a minority of adult day services centers were for profit. The majority of nursing homes and residential care communities and a minority of adult day services centers were chain-affiliated. The supply of residential care beds per 1,000 persons aged 65 and over was higher in the Midwest and West than in the Northeast and the South, and the capacity of adult day services centers was higher in the West than in the other regions” (Harris-Kojetin et al., 2019, p. 2). See Figures 2.5 and 2.6. More than half of the financial support for nursing homes and adult day services comes from public funds, much of it under the Medicaid program, as Medicare provides little long-term care coverage. In 2016, almost 66% of adult day-care users and 62% of nursing home occupants used Medicaid as their source of payment (see Figure 2.7). Much of Medicaid expenditures goes for the elderly (21%) and disabled (42%), although these groups comprise 9% and 15% of Medicaid enrollees, respectively (Kaiser Family Foundation, 2015). Further, a substantial portion of expenditures for the disabled and elderly is for long-term care. However, by no means are all of the people benefiting from this payment mechanism of receiving public assistance at the time they entered a nursing home (if they are institutionalized), and many had never received public assistance. In response, a number 50 45 39
40 34
33
Percent
30 25
24 21
20 20
18
17
10 10
7
6
6 3
0 Total
Northeast
Adult day services center maximum participants allowed
Midwest Certified nursing home beds
South
West
Licensed residential care community beds
FIGURE 2.5 Long-term care services provider capacity per 1,000 people aged 65 years and older, by sector and region, 2015 to 2016. Source: Harris-Kojetin, L., Sengupta, M., Lendon, J. P., Rome, V., Valverde, R., & Caffrey, C. (2019). Long-term care providers and services users in the United States, 2015–2016. National Center for Health Statistics. Vital and Health Statistics, 3(43), 1–88.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 67
3/19/20 10:52 AM
68
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
1.3 Government and other 4.6
100
4.6 14.1
7.2
14.8
17.7
Nonprofit
81.0
For profit
23.5
80
22.8 50.8
Percent
60
80.6
40
63.0
69.3
44.7 20
0
Adult day services center
Home health agency
Hospice
Nursing home Residential care community
FIGURE 2.6 Percent distribution of long-term care services providers, by sector and ownership, 2016. Source: Harris-Kojetin, L., Sengupta, M., Lendon, J. P., Rome, V., Valverde, R., & Caffrey, C. (2019). Long-term care providers and services users in the United States, 2015–2016. National Center for Health Statistics. Vital and Health Statistics, 3(43), 1–88.
65.8
70
61.8
60
Percent
50 40 30 16.5 20 9.5 10 0
Adult day services Home health center agency
Nursing home
Residential care community
FIGURE 2.7 Percentage of long-term care services users with Medicaid as payer source, by sector, 2015 to 2016. Source: Harris-Kojetin, L., Sengupta, M., Lendon, J. P., Rome, V., Valverde, R., & Caffrey, C. (2019). Long-term care providers and services users in the United States, 2015–2016. National Center for Health Statistics. Vital and Health Statistics, 3(43), 1–88.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 68
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
69
of states have instituted “asset transfer” systems. These permit people of means to transfer property and other assets to others, usually their children, so that on paper they become “poor,” and thus Medicaid eligible, after some period of time following the asset transfer.
Utilization of Long-Term Care In 2016, adult day services center participants tended to be younger than services users in other sectors. Persons aged 85 years and older were less likely to use adult care services centers (16.3%) and more likely to use hospice (47.8%) and residential care communities (52.1%). In all sectors, women were the majority of users, varying from 58% in adult day services centers and hospice to 70% in residential care communities. At least 25% of services users in each of the five sectors had Alzheimer’s disease or other dementias, arthritis, heart disease, or hypertension. However, the prevalence of these and six other reported diagnosed chronic conditions varied widely between sectors. Fewer adult day services center participants needed assistance with four of six activities of daily living (ADLs, such as bathing, dressing, toileting, and walking or locomotion) than services users in other sectors (Harris-Kojetin et al., 2019; see Table 2.16).
TABLE 2.16 Long-Term Care Services Users, by Selected Characteristics and Sector, 2015 to 2016 Characteristic
Adult Day Services Center
Home Health Agency
Hospice
Nursing Home
Residential Care Community
286,300
4,455,700
1,426,000
1,347,600
811,500
Users
Age
Percent
Under 65
37.4
18.1
5.5
16.5
6.6
65 and over
62.5
81.9
94.6
83.5
93.4
65–74
20.3
26.8
17.5
18.2
11.0
75–84
25.9
29.9
29.3
26.7
30.3
85 and over
16.3
25.2
47.8
38.6
52.1
Sex
Percentage Distribution
Men
41.8
39.1
41.3
35.4
29.4
Women
58.2
60.9
58.7
64.6
70.6
Diagnosis
Percentage
Alzheimer’s disease or other dementia
30.9
32.3
44.5
47.8
41.9
Arthritis
37.9
59.6
28.7
26.2
42.4
Asthma
8.3
23.7
8.4
—
6.8
Chronic kidney disease
7.2
46.9
35.9
—
8.3
Chronic obstructive pulmonary disease
10.0
31.9
20.7
—
14.0
Depression
28.2
39.4
23.4
46.3
30.9
31.4
45.1
27.0
32.0
18.1
27.1
55.0
38.7
38.1
34.3
Diabetes a
Heart disease
(continued)
Goldsteen74024_02_CH02_33-78_03-18-20.indd 69
3/19/20 10:52 AM
70
■
I
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 2.16 Long-Term Care Services Users, by Selected Characteristics and Sector, 2015 to 2016 (continued) Adult Day Services Center
Home Health Agency
Hospice
Nursing Home
Residential Care Community
Hypertension
50.3
88.9
51.0
71.5
51.2
Osteoporosis
21.2
15.3
7.2
12.3
23.7
Characteristic
Need Assistance in Physical Functioning
Percentage
Eating
23.2
61.2
—
59.9
19.2
Bathing
38.6
97.2
—
96.7
63.6
Dressing
36.0
92.0
—
92.7
48.2
Toileting
33.5
81.1
—
89.3
40.0
Walking
45.8
95.4
—
92.0
56.5
Transferring in and out of bed or chair
28.5
91.3
—
86.8
29.2
—, data not available. For adult day services center participants and residential care community residents, heart disease includes congestive heart failure, coronary or ischemic heart disease, heart attack, and stroke. For home health and hospice patients, heart disease refers to ischemic heart disease. For nursing home residents, heart disease refers to coronary artery disease, congestive heart failure, and stroke.
a
SOURCE: National Center for Health Statistics. (2019). Long-term care providers and services users in the United States, 2015-2016. Vital and Health Statistics, 3(43), 1–88. Retrieved from https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf
SUMMARY The U.S. health care system consists of an extensive array of settings for health care. These settings include community-based facilities for ambulatory care, hospitals for acute care, and postacute care facilities—community based as well as institutional. These settings offer long-term treatment, rehabilitation, assistance with daily life, and comfort. Most health care occurs in the ambulatory setting, and most ambulatory care is provided in physician offices, outpatient hospital clinics, and hospital EDs. However, two shifts are occurring. First, some ambulatory services that used to be performed only in physician offices and outpatient clinics are being provided in other settings. These include urgent care centers, retail pharmacies, and telehealth services offering primary and urgent care outside the traditional ambulatory settings. Second, a substantial amount acute health care that was traditionally provided in hospitals is now available in ambulatory settings, including ASCs and diagnostic imaging and laboratory centers. These shifts in health care delivery are resulting in increasing vertical integration in the U.S. health care system as hospitals and hospital systems purchase new ambulatory sites of care in order to maintain their preeminent role in health care delivery.
DATA SOURCES Several authoritative sources of information on health care settings include:
Ambulatory Care •
National Ambulatory Medical Care Survey (NAMC). This survey is conducted by the NCHS and provides the most recent data on ambulatory care visits to physician
Goldsteen74024_02_CH02_33-78_03-18-20.indd 70
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
71
offices in the United States. Begin exploring here: www.cdc.gov/nchs/ahcd/index. htm •
Hospital Ambulatory Medical Care Survey (NHAMCS). The NHAMCS is also conducted by the NCHS and is designed to collect information about utilization and services provided in hospital ED and OPDs and in ambulatory surgery locations. Begin here: www.cdc.gov/nchs/ahcd/index.htm
Hospitals •
American Hospital Association. The AHA is an independent, nonprofit organization that conducts an annual survey of hospitals in the United States, which includes current and historical data on utilization, personnel, revenue, expenses, managed care contracts, community health indicators, physician models, and more. The results are published in the AHA Hospital Statistics each year.
•
Healthcare Cost and Utilization Project. The HCUP is conducted by the AHRQ, Center for Delivery, Organization, and Markets. It includes the largest collection of longitudinal hospital care data in the United States. HCUP FastStats, Most Common Diagnoses for Inpatient Stays can be accessed at: www.hcup-us.ahrq.gov/faststats/ landing.jsp). FastStats are based on the HCUP NIS. HCUPnet is a free, online query system based on data from HCUP. The system provides health care statistics and information for hospital inpatient, ED, and ambulatory settings, as well as population-based health care data on counties. Begin here: https://hcupnet.ahrq.gov/#setup
Long-Term Care •
National Study of Long-Term Care Providers (NSLCP). The NSLCP is a biennial study conducted by the NCHS. It monitors trends in the supply, provision, and use of the major paid, regulated long-term care services: nursing homes, home health, hospice, assisted living, and adult day services. The NCHS also produces reports on long-term care using “data from multiple sources, including two main sources: administrative data from CMS on nursing homes, home health agencies, and hospices,” as well as its own NSLCP. Start here: www.cdc.gov/nchs/nsltcp/index.htm
STUDY QUESTIONS 1. What is self-care? 2. What is ambulatory care, and what ambulatory care settings serve the most patients? 3. What are the emerging ambulatory care settings? 4. What is the community hospital, and what is its importance in the hospital sector? 5. What kinds of health problems are treated in ambulatory settings, and how do they differ from those seen in acute care hospitals? 6. What are the five different sectors of long-term care, and what role does each sector play?
NOTES 1. This particular example is chosen because Dr. Jonas’ grandmother happened to have been a member of the hospital’s founding board of directors, and his stepmother was a longtime member of the board of its successor, Arden Hill Hospital. 2. Compounding pharmacies specialize in the preparation of components into a drug preparation as the result of a practitioner’s prescription drug order or initiative based on the practitioner/patient/pharmacist relationship in the course of professional practice.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 71
3/19/20 10:52 AM
72
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
3. A mail-order pharmacy is one that uses common carriers to deliver the medications to patients or their caregivers. Mail-order pharmacies are licensed in the state where they are located and may also be licensed or registered as nonresident pharmacies in other states. 4. Specialty pharmacies generally dispense low-volume and high-cost medicinal preparations to patients who are undergoing intensive therapies for illnesses that are generally chronic, complex, and potentially life-threatening. Often, these therapies require specialized delivery and administration (NUCC, 2019).
REFERENCES Advisory Board. (2019, January 8). The outpatient shift continues: outpatient revenue now 95% of inpatient revenue, new report reveals. Daily Briefing. Retrieved from https://www.advisory .com/daily-briefing/2019/01/08/hospital-revenue Alavy, B., Chung, V., Maggiore, D., Shim, C., & Dhuper, S. (2006). Emergency department as the main source of asthma care. Journal of Asthma, 43(7), 527–532. doi: 10.1080/02770900600857069 Ambulatory Surgery Center Association. (2012). History. Retrieved from www.ascassociation .org/Home Ambulatory Surgery Center Association. (2019). Ambulatory surgery centers: A positive trend in health care. Retrieved from https://www.ascassociation.org/advancingsurgicalcare/ aboutascs/industryoverview/apositivetrendinhealthcare American College of Emergency Physicians. (2010). ACEP policy statements: Triage scale standardization. Retrieved from https://www.acep.org/patient-care/policy-statements/ triage-scale-standardization/ American Hospital Association. (2007). Hospital statistics. Chicago, IL: Health Forum. American Hospital Association. (2013). Teaching hospitals: Vital for tomorrow’s health care. Retrieved from http://www.aha.org/research/policy/infographics/teaching-hospitals.shtml American Hospital Association. (2018). Hospital statistics, 2018. Chicago, IL: Health Forum. American Hospital Association. (2019a). Fast facts on US hospitals. Retrieved from http:// www.aha.org/research/rc/stat-studies/fast-facts.shtml American Hospital Association. (2019b). Hospital statistics, 2019. Chicago, IL: Health Forum. Anderson, H. (1990, August 5). Out-patient care: A nationwide revolution. Hospitals, p. 28. Association of State and Territorial Health Officials. (2006). Access to care. Retrieved from www.astho.org/?template=access.html Bush, G. W. (2007). Fact sheet: Meeting the health care needs of uninsured and underserved Americans. White House. Retrieved from https://georgewbush-whitehouse.archives .gov/news/releases/2007/12/20071205-2.html California Advocates for Nursing Home Reform. (2019). Residential care/assisted living. Retrieved from http://www.canhr.org/RCFE/rcfe_what.htm Callan, D., & Fein, O. (1972, June). NENA: Community control in a bind. Health PAC Bulletin, 41, 3–12. Retrieved from http://www.healthpacbulletin.org/healthpac-bulletin-june-1972/ Centers for Medicare & Medicaid Services. (2018). Table 2. National health expenditures; aggregate, annual percent change, percent distribution and per capita amounts, by type of
Goldsteen74024_02_CH02_33-78_03-18-20.indd 72
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
73
expenditure: Selected calendar years 1960-2017. Retrieved from https://www.cms.gov/ Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealth ExpendData/NationalHealthAccountsHistorical.html Centers for Medicare & Medicaid Services. (2019). Place of service code set. Retrieved from https://www.cms.gov/Medicare/Coding/place-of-service-codes/Place_of_Service _Code_Set.html Centers for Medicare & Medicaid Services. (2020). Home health quality reporting. Retrieved from https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/ HomeHealthQualityInits Centers for Medicare & Medicaid Services, Office of the Actuary, National Health Statistics Group, National Health Expenditure Accounts. (2017). National health expenditures. Retrieved from https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics -Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsHistorical.html Chandler, A. (1962). Strategy and structure: Chapters in the history of industrial enterprise. New York, NY: Doubleday. Commission on Public General Hospitals. (1978). The future of the “public” general hospital. Chicago, IL: Hospital Research and Educational Trust. Cuellar, A. E., & Gertler, P. J. (2003). Trends in hospital consolidation: The formation of local systems. Health Affairs, 22(6), 77–87. doi: 10.1377/hlthaff.22.6.77 Data.CMS.gov. (2019). Crosswalk Medicare provider/supplier to health care providers. Retrieved from https://data.cms.gov/Medicare-Enrollment/CROSSWALK-MEDICARE -PROVIDER-SUPPLIER-to-HEALTHCARE/j75i-rw8y/data Davis, K., & Schoen, C. (1978). Health and the war on poverty. Washington, DC: Brookings Institution. Dean, K. (1981). Self-care responses to illness: A selected review. Social Science & Medicine: Part A, 15(5), 673–687. doi: 10.1016/0271-7123(81)90091-2 Ermann, D., & Gabel, J. (1985). The changing face of American health care: Multi-hospital systems, emergency centers, and surgery centers. Medical Care, 23(15), 401–420. doi: 10.1097/00005650-198505000-00006 Feldman, P. H., Nadash, P., & Gursen, M. D. (2005). Long term care. In A. R. Kovner & S. Jonas (Eds.), Jonas and Kovner’s health care delivery in the United States (8th ed., pp. 274–325). New York, NY: Springer Publishing Company. Felt-Lisk, S., McHugh, M., & Howell, E. (2002). Monitoring local safety-net providers: Do they have adequate capacity? Health Affairs, 21(5), 277–283. doi: 10.1377/hlthaff.21.5.277 Fraze, T., Elixhauser, A., Holmquist, M. A., & Johann, J. (2010). Public hospitals in the United States, 2008 (HCUP Statistical Brief #95). Rockville, MD: Agency for Healthcare Research and Quality. Freymann, J. G. (1974). The American Health Care System: Its genesis and trajectory. New York, NY: Medcom. Friedman, E. (1997). California public hospitals: The buck has stopped. Journal of the American Medical Association, 277(7), 577–581. doi: 10.1001/jama.1997.03540310075039 Hamm, J., Blaine, N., Salavaci, J., & Jacoby, D. (2018, September). The “Centrality of Sepsis”: A review on incidence, mortality, and cost of care. Healthcare, 6(3), 90–95. doi: 10.3390/ healthcare6030090
Goldsteen74024_02_CH02_33-78_03-18-20.indd 73
3/19/20 10:52 AM
74
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Harris-Kojetin, L., Sengupta, M., Lendon, J. P., Rome, V., Valverde, R., & Caffrey, C. (2019). Long-term care providers and services users in the United States, 2015-2016. National Center for Health statistics. Vital Health Statistics, 3(43), 1–88. Retrieved from https:// www.cdc.gov Haugh, R. (2002, April). Nowhere else to turn. Hospitals and Health Networks, 76(4), 44. Retrieved from https://europepmc.org/article/med/11974409 Healthcare Cost and Utilization Project. (2018, August). Overview of the National (nationwide) inpatient sample (NIS), Rockville, MD: Agency for Healthcare Research and Quality. Retrieved from https://www.hcup-us.ahrq.gov/nisoverview.jsp Health Resources and Services Administration. (2015a). What is a health center? Retrieved from http://bphc.hrsa.gov/about/what-is-a-health-center/index.html Health Resources and Services Administration. (2015b). 2014 Health center data. Retrieved from http://bphc.hrsa.gov/uds/datacenter.aspx Health Resources and Services Administration, Bureau of Primary Care. (2012). About the health center program Retrieved from http://bphc.hrsa.gov/about/index.html Huang, J., Silbert, J., & Regenstein, M. (2005). America’s public hospitals and health systems, 2003. Washington, DC: National Association of Public Hospitals and Health Systems. Institute of Medicine. (2000). To err is human: Building a safer health system. Washington, DC: National Academies Press. Institute of Medicine. (2002). Unequal treatment: Confronting racial and ethnic disparities in health care. Washington, DC: National Academies Press. The Joint Commission. (2009). Leadership in healthcare organizations: A guide to joint commission leadership standards. Retrieved from https://psnet.ahrq.gov/issue/ leadership-healthcare-organizations-guide-joint-commission-leadership-standards The Joint Commission. 2018. Facts about ambulatory care accreditation. Retrieved from https:// www.jointcommission.org/facts_about_ambulatory_care_accreditation/ Kaiser Family Foundation. (2015). Medicaid moving forward. Retrieved from http://kff.org/ health-reform/issue-brief/medicaid-moving-forward/ Kaufman, Hall and Associates. (2018). 2017 in review: The year M&A shook the healthcare landscape. Retrieved from https://www.kaufmanhall.com/sites/default/files/legacy_files/ kh_report-ma-year-in-review_d4-rebrand.pdf Knowles, J. H. (1965). The role of the hospital: The ambulatory clinic. Bulletin of the New York Academy of Medicine, 41(1), 68–79. Retrieved from https://www.ncbi.nlm.nih.gov/ pubmed/14230869 Kongstvedt, P. R., Plocher, D. W., & Stanford, J. C. (2001). Integrated health care delivery systems. In P. R. Kongstvedt (Ed.), The managed health care handbook (4th ed., pp. 42–71). Gaithersburg, MD: Aspen. LaPointe, J. (2019). How hospital merger and acquisition activity is changing health care. RevCycle Intelligence. Retrieved from https://revcycleintelligence.com/features/ how-hospital-merger-and-acquisition-activity-is-changing-healthcare Levin, L. S., & Idler, E. L. (1983). Self-care in health. Annual Review of Public Health, 4, 181-201. doi: 10.1146/annurev.pu.04.050183.001145
Goldsteen74024_02_CH02_33-78_03-18-20.indd 74
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
75
Light, H. L., & Brown, H. J. (1967). The gouverneur health services program: An historical view. Milbank Memorial Fund Quarterly, 45(4), 375–390. doi: 10.2307/3348859 Lin, W. C., Yang, Y., Wen, Y. K., & Chang, C. C. (2006). Outpatient versus inpatient renal biopsy: A retrospective study. Clinical Nephrology, 66(1), 17–24. doi: 10.5414/CNP66017 Lucas, J. W., & Benson, V. (2018). Tables of summary health statistics for the U.S. population: 2017 National Health Interview Survey. National Center for Health Statistics. Retrieved from https://www.cdc.gov/nchs/nhis/SHS/tables.htm MacEachern, M. T. (1962). Hospital organization and management. Berwyn, IL: Physician’s Record. May, E. L. (2004). Strengthening the safety net. Healthcare Executive, 19(1), 10–15. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/14716922 McAlearney, J. S. (2002, March–April). The financial performance of community health centers, 1996–1999. Health Affairs, 21(2), 219–225. doi: 10.1377/hlthaff.21.2.219 McDermott, K. W., Elixhauser, A., & Sun, R. (2017, June). Trends in hospital inpatient stays in the United States, 2005–2014 (HCUP Statistical Brief #225). Rockville, MD: Agency for Healthcare Research and Quality. Retrieved from www.hcup-us.ahrq.gov/reports/ statbriefs/sb225-Inpatient-US-Stays-Trends.pdf McHugh, M., & Tanabe, P. (2011, June). The emergency severity index is the most commonly used triage system in the U.S. presented at the Society of Academic Emergency Medicine Annual Meeting, Boston, MA: National Center for Injury Prevention and Control. Medical Group Management Association. (2002). Ambulatory surgery center performance survey: 2001 report. Englewood, CO: Author. Moon, T. D., Laurens, M. B., Weimer, S. M., & Levy, J. A. (2005). Nonemergent emergency room utilization for an inner-city pediatric population. Pediatric Emergency Care, 21(6), 363–366. doi: 10.1097/01.pec.0000166725.76685.4a Murphy, T. (2019, June 4). At stores and online, health care moves closer to customers. U.S. News & World Report. Retrieved from https://www.usnews.com/news/business/ articles/2019-06-04/cvs-announces-further-expansion-into-health-care-services Myers, B. A., Steinhardt, B. J., Mosley, M. L., & Cashman, J. W. (1968). Medicare’s effects on medical care: The medical care activities of local health units. Public Health Reports, 83(9), 757–769. doi: 10.2307/4593407 National Adult Day Services Association. (2019). About adult day services. Retrieved from https://www.nadsa.org/learn-more/about-adult-day-services/ National Association of County and City Health Officials. (2016). 2016 National profile of local health departments. Retrieved from http://nacchoprofilestudy.org/ National Center for Health Statistics. (2011). National hospital ambulatory medical care survey: 2011 outpatient department summary tables. Retrieved from https://www.cdc.gov/nchs/ ahcd/web_tables.htm#2016 National Center for Health Statistics. (2019). Long-term care providers and services users in the United States, 2015-2016. Vital and Health Statistics, 3(43), 1–88. Retrieved from https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf National Institute on Aging. (2019). Long-term care. Retrieved from https://www.nia.nih.gov/ health/residential-facilities-assisted-living-and-nursing-homes
Goldsteen74024_02_CH02_33-78_03-18-20.indd 75
3/19/20 10:52 AM
76
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
National Institute for Occupational Safety and Health. (2015). What is total worker health?. Retrieved from http://www.cdc.gov/niosh/twh/ National Uniform Claim Committee. (2019). Definition for pharmacy. Retrieved from http:// nucc.org/index.php/code-sets-mainmenu-41/provider-taxonomy-mainmenu-40/ code-lookup-mainmenu-50 Perrin, J. M., Bloom, S. R., & Gortmaker, S. L. (2007). The increase of childhood chronic conditions in the United States. Journal of the American Medical Association, 297(24), 2755–2759. doi: 10.1001/jama.297.24.2755 Podolsky, D. (1996, August 12). Breaking down the walls. U.S. News and World Report, p. 61. Qato, D. M., Zenk, S., Wilder, J., Harrington, R., Gaskin, D., & Alexander, G. C. (2017). The availability of pharmacies in the United States: 2007-2015. PLoS One, 12(8), e0183172. doi: 10.1371/journal.pone.0183172 Roemer, M. I. (1981). Ambulatory health services in America. Gaithersburg, MD: Aspen Systems. Roemer, M. I., & Friedman, J. W. (1971). Doctors in hospitals. Baltimore, MD: Johns Hopkins. Rosen, G. (1971). The first neighborhood health center movement: Its rise and fall. American Journal of Public Health, 61(8), 1620–1637. doi: 10.2105/AJPH.61.8.1620 Rosenberg, C. E. (1979). The origins of the American hospital system. Bulletin of the New York Academy of Medicine, 55(1), 10–21. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/ articles/PMC1807593/ Rui, P., Kang, K., & Ashman, J. J. (2016). National hospital ambulatory medical care survey: 2016 emergency department summary tables. Rui, P., & Okeyode, T. (2016). National ambulatory medical care survey: 2016 national summary tables. Retrieved from https://www.cdc.gov/nchs/data/ahcd/namcs_summary/2016 _namcs_web_tables.pdf Sardell, A. (1983). Neighborhood health centers and community-based care: Federal policy from 1965 to 1982. Journal of Public Health Policy, 4(4), 484–503. doi: 10.2307/3342224 Sg2. (2016). Health systems find large opportunity in microhospitals. Retrieved from https://newsroom.vizientinc.com/vizient-blog/clinical-performance/health-systems -find-large-opportunity-microhospitals Singer, A. J., Thode, H. C., & Pines, J. M. (2019). US emergency department visits and hospital discharges among uninsured patients before and after implementation of the Affordable Care Act. JAMA Network Open, 2(4), e192662. doi: 10.1001/jamanetworkopen.2019.2662 Starfield, B. (1992). Primary care. New York, NY: Oxford University Press. Stern, B. J. (1946). Medical services by government. New York, NY: The Commonwealth Fund. Stevens, R. (1971). American medicine and the public interest. New Haven, CT:Yale University Press. Strahan, G. W. (1996, April 24). An overview of home health and hospice care patients: 1994 national home and hospice care survey (Advance data). Hyattsville, MD: National Center for Health Statistics. Thrall, T. H. (1996, September). What PHOs know. Hospitals and Health Networks, p. 54. Trap, B. (2019). Practices of dispensing doctors—Drug use and health economics. World Health Organization, International Conferences on Improving Use of Medicines. Retrieved from http://archives.who.int/icium/icium1997/posters/4b4_fin.html
Goldsteen74024_02_CH02_33-78_03-18-20.indd 76
3/19/20 10:52 AM
2
■
Th e S e t t i n g s f o r H e a l t h C a re D e l i v e r y
77
U.S. Census Bureau. (2013). School enrollment: Enrollment status of the population 3 years old and over, by sex, age, race, Hispanic origin, foreign born, and foreign-born parentage: October 2013. Retrieved from https://www.census.gov/topics/education/school-enrollment/data/tables.2013.html U.S. Department of Health and Human Services. (2011, July). HHS announces new investment in school-based health centers. Retrieved from http://wayback.archive-it.org/3926/2014010 8162123/http://www.hhs.gov/news/press/2011pres/07/20110714a.html Verghese, A. (1996, November 30). My hospital, dying a slow death. The NewYork Times. Retrieved from www.nytimes.com/1996/11/30/opinion/my-hospital-dying-a-slow-death.html Winslow, C. E. A. (1929). The life of Herman Biggs. Philadelphia, PA: Lea & Febiger. World Health Organization. (2019). Primary health care. Retrieved from https://www.who .int/news-room/fact-sheets/detail/primary-health-care Yao, N., Ritchie, C., Camacho, F., & Leff, B. (2016). Geographic concentration of home-based medical care providers. Health Affairs, 35(8), 1404–1409. doi: 10.1377/hlthaff.2015.1437 Zwick, D. I. (1972). Some accomplishments and findings of neighborhood health centers. Milbank Memorial Fund Quarterly, 50(4), 387–420. doi: 10.2307/3349428
FURTHER READING Agency for Healthcare Research and Quality. (2004). Emergency severity index (ESI): A triage tool for the emergency department. Retrieved from ww.ahrq.gov/professionals/systems/ hospital/esi/esiappb.html Agency for Healthcare Research and Quality. (2009). HCUP facts & figures: Cost by diagnosis. Retrieved from www.hcup-us.ahrq.gov/reports/factsandfigures/2009/exhibit4_1.jsp American Hospital Association. (1990). Hospital statistics 1990–1991. Chicago, IL: Author. American Hospital Association. (2011a). AHA guide, 2011. Chicago, IL: Health Forum. American Hospital Association. (2011b). Hospital statistics, 2011. Chicago, IL: Health Forum. American Hospital Association. (2013). Hospital statistics, 2013. Chicago, IL: Health Forum. Centers for Medicare & Medicaid Services. (2015a). What’s home health care & what should I expect? Centers for Medicare & Medicaid Services. (2015b). What are long-term care hospitals? Eisen, R., & Sloan, F. A. (Eds.). (1997). Developments in health economics and public policy (Vol. 5). New York, NY: Springer Publishing Company. Gresenz, C. R., Studdert, D. M., Campbell, N., & Hensler, D. R. (2002). Patients in conflict with managed care: A profile of appeals in two HMOs. Health Affairs, 21(4), 189–196. doi: 10.1377/hlthaff.21.4.189 Hall, M. J., & Owings, M. F. (2002, June 19). National Hospital Discharge Survey 2000 (Advance data no. 329). Hyattsville, MD: National Center for Health Statistics. Health Resources and Services Administration. (2006). HSS awards $10 million to expand health center services for farmworkers, homeless. HRSA News. Kaiser Family Foundation. (2015). Medicaid and Medicare at 50:Trends and challenges. Retrieved from http://kff.org/slideshow/medicaid-and-medicare-at-50-trends-and-challenges/ Kovner, A. R., & Channing, A. H. (2001). A career guide for the health services manager (3rd ed.). Chicago, IL: Health Administration Press.
Goldsteen74024_02_CH02_33-78_03-18-20.indd 77
3/19/20 10:52 AM
78
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Kovner, A. R., & Neuhauser, D. (2001). Health services management: Readings and commentary (7th ed.). Chicago, IL: Health Administration Press. Landy, J. (2001, September 25). September 25 NYC forum on the threats to primary care in the U.S. New York, NY: Physicians for a National Health Program. McCaig, L. F., & Nawar, E. W. (2006). National hospital ambulatory medical care survey: 2004 Emergency department summary (Advance Data No. 372). Hyattsville, MD: National Center for Health Statistics. National Association for Home Care & Hospice. (2010). Basic statistics about home care. Retrieved from www.nahc.org/facts/10HC_Stats.pdf National Center for Health Statistics. (2007). Health, United States, 2006. Hyattsville, MD: U.S. Department of Health and Human Services. National Center for Health Statistics. (2009). Number, rate and average length of stay for discharges from short-stay hospitals by age, region, and sex: United States, 2009. Retrieved from www.cdc.gov/nchs/data/nhds/1general/2009gen1_agesexalos.pdf National Center for Health Statistics. (2010). Number, rate and average length of stay for discharges from short-stay hospitals by age, region, and sex: United States, 2010. Retrieved from http://www.cdc.gov/nchs/data/nhds/1general/2010gen1_agesexalos.pdf National Center for Health Statistics. (2013). National ambulatory medical survey: 2012 state and national summary tables. Retrieved from http://www.cdc.gov/nchs/data/ahcd/ namcs_summary/2012_namcs_web_tables.pdf National Center for Health Statistics. (2014). Health, United States, 2013: With special feature on prescription drugs. Hyattsville, MD: U.S. Department of Health and Human Services. Retrieved from http://www.cdc.gov/nchs/data/hus/hus13.pdf National Center for Health Statistics. (2018). Health, United States, 2017: With special feature on mortality. Hyattsville, MD: U.S. Department of Health and Human Services. National Center for Health Statistics. (2019). Ambulatory health care data. Retrieved from https://www.cdc.gov/nchs/ahcd/index.htm National Prevention Council. (2011). National prevention strategy. Washington, DC: U.S. Department of Health and Human Services, Office of the Surgeon General. Pear, R. (2002, February 18). 9 of 10 nursing homes in U.S. lack adequate staff, a government study finds. The New York Times, p. A11. Pfuntner, A., Wier, L. M., & Stocks, C. (2013). Most frequent conditions in U.S. hospitals, 2011 (HCUP Statistical Brief #162). Rockville, MD: Agency for Healthcare Research and Quality. Retrieved from http://www.hcup-us.ahrq.gov/reports/statbriefs/sb162.pdf
Goldsteen74024_02_CH02_33-78_03-18-20.indd 78
3/19/20 10:52 AM
3 The People Who Provide Health Care
© Randy Glasbergen.
LEARNING OBJECTIVES After completing this chapter, students will be able to: • Describe the history of physicians in the United States. • Outline the medical education system in the United States and educational requirements for physicians. • Describe the settings in which physicians practice and their roles. • Define “nursing” and describe the origins of the modern profession of nursing. • List and describe the categories of nurses and the corresponding educational requirements for each. • Describe the settings in which nurses practice and their roles. • List other health care professions and occupations and describe their roles.
Goldsteen74024_03_CH03_79-124_03-18-20.indd 79
3/19/20 10:53 AM
80
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
INTRODUCTION A wide variety of settings in which health care is delivered in the United States—from hospitals to homes—are staffed with a large and varied workforce. Some health care occupations are mainly diagnostic; others are chiefly concerned with treatment. Some focus on prevention, others on acute health problems, and others on postacute care for chronic conditions. Some provide highly technical services, others highly personal care. Thus, the people who provide health care include physicians practicing in ambulatory care offices, nurses staffing urgent care clinics, radiology technicians practicing in hospital emergency departments (ED), dieticians and nutritionists serving patients in physician offices, pharmacists working in retail stores, paramedics providing ambulance services, orthotists and prosthetists tending to patients in their private clinics, and medical records and health information technicians in community hospitals. In addition to differences in occupational skills and practice settings, health care occupations are distinct in other important ways. They differ in the amount and type of training required, with some needing a postbaccalaureate degree or more, some only baccalaureate degree, and some the completion of a technical training program. In order to practice, many, although not all, health care occupations mandate certification or licensing (U.S. Department of Labor, Bureau of Labor Statistics [BLS], 2019a). In practice, health care occupations differ in salary prospects and occupational autonomy, both of which are highly related to the amount of education required. Despite their differences, health care occupations have notable similarities. First, they are constantly evolving in response to changes in technology, health policy, health care economics, and culture. Changes can take the form of new training criteria, new practice patterns, and different kinds of practice settings. For example, the rise in ambulatory surgery centers has decreased the proportion of nurses and medical technicians working in hospitals. Although some of the older occupations, such as physician and nursing, are more tradition bound than others, all innovate and transform to some extent as the health care system changes. Second, the importance of ethical standards of practice is common to all health care occupations. As Limentani (1998) wrote in the British Medical Journal,“Ethics are not optional in medicine: they are an essential and integral part of health care”(p. 1458). A few core ideas guide the health care occupations, including “doing no harm,” providing competent care, maintaining the confidentiality of patients and their records, respecting patient autonomy and primacy, and engaging honestly with patients and fellow workers. Each health occupation has an ethics statement or set of principles that reflect these tenets, and the American Medical Association’s (AMA) Principles of Medical Ethics is an example (AMA, 2019). Third, in addition to being essential for the delivery of health care services, the health care workforce is important at the societal and community levels. Health care workers in every occupation are a source of economic stability in many communities. In small and rural communities, a health care organization is often the major employer and, as a result, is vital to the community’s economic viability. In some distressed communities, where manufacturing and related industries have declined, health care organizations have become a significant source of employment, especially for women. Health care occupations also offer a gateway to middle-class life for unskilled workers through support positions that can be earned in noncollege settings. For example, persons with only a high school diploma or equivalent can be trained in a health care facility to be nursing assistants. Upon completion of the training program, nursing assistants provide basic patient care, such as feeding, bathing, and moving patients, under direction of the nursing staff (BLS, 2019b). Building on their training, these jobs can lead to more skilled and well-paying positions in the health care system.
Goldsteen74024_03_CH03_79-124_03-18-20.indd 80
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
81
HEALTH CARE OCCUPATIONS, OVERALL The BLS is the most authoritative source of information about the number of health care occupations and important attributes, including wages, demographic characteristics, and geographic region of practice. The Bureau of Labor Statistics (BLS) of the U.S. Department of Labor is the principal federal agency responsible for measuring labor market activity, working conditions, and price changes in the economy. Its mission is to collect, analyze, and disseminate essential economic information to support public and private decision making. ... The Occupational Employment Statistics (OES) program conducts a semiannual survey designed to produce estimates of employment and wages for specific occupations. The OES program collects data on wage and salary workers in nonfarm establishments in order to produce employment and wage estimates for about 800 occupations. (BLS, 2019c) The statistics produced by the BLS are the basis for the following discussion of the health care occupations, overall. Health care occupations account for a large portion of employed persons in the United States. Furthermore, health care occupations have been increasing as a percentage of employed individuals. In 2018, about 13 million people, or 8.5% of all civilians employed in nonagricultural occupations in the United States, were providing health care. This was up from 11.1 million people, or 8.1% of all employed persons, working in health care in 2010, and up from about 9 million, or 6.8%, in 2002 (the earliest year in which the health care occupation categories matched 2018 data; BLS, 2004a, 2011a, 2019d). The BLS has two major categories of health care workers: (a) Healthcare Practitioners and Technical Occupations and (b) Healthcare Support Occupations. These categories are used throughout this discussion of health care occupations. They do not include occupations that are strictly managerial, that is, medical and health services managers (n = 372,670). They also do not include educators including health educators (n = 58,780), postsecondary health teachers (n = 255,190), postsecondary health specialties teachers (n = 199,480), and community health workers (n = 56,130), who are health educators working in communities to help people adopt healthy behaviors. The categories do include a small number of occupations that will not be discussed in this book including, those in dentistry and veterinary services. In 2018, there were about 9 million persons employed in the occupations within Practitioners and Technical Occupations. The largest of the occupations in this category, accounting for about 78% of all persons employed in Practitioners and Technical Occupations, were (BLS, 2019e): • •
• •
•
RNs (n = 2,951,960) Health practitioner support technologists and technicians (n = 801,590) • Includes dietetic, pharmacy, psychiatric, respiratory therapy, surgical, and other technicians and technologists Licensed practical and licensed vocational nurses (n = 701,690) Therapists (n = 687,790) • Includes occupational, physical, radiation, respiratory, exercise, and other therapists Physicians and surgeons (n = 679,280) • Includes anesthesiologists, family and general practitioners, general internists, obstetricians and gynecologists, pediatricians, psychiatrists, surgeons, and others
Goldsteen74024_03_CH03_79-124_03-18-20.indd 81
3/19/20 10:53 AM
82
I
•
• • • •
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Diagnostic-related technologists and technicians (n = 390,630) • Includes cardiovascular technologists and technicians, diagnostic medical sonographers, nuclear medicine technologists, radiologic technologists, magnetic resonance imaging technologists, and others Pharmacists (n = 309,550) Medical records and health information technicians (n = 208,650) Nurse practitioners (n = 179,650) Physician assistants (PAs; n = 114,710)
In 2018, there were about 4 million persons employed in occupations within the Healthcare Support Occupations. The largest of the occupations in this category, accounting for about 77% of all persons employed in Healthcare Support Occupations, were (BLS, 2019e): • • • •
Nursing assistants (n = 1,450,960) Home health aides (n = 797,670) Medical assistants (n = 673,660) Physical therapist assistants and aides (n = 141,510)
Wages for Health Care Occupations In 2018, the average annual wage for all occupations in the United States was US$51,960. The lowest annual wage was US$22,140 for combined food preparation and serving workers, including fast food. Other occupations with annual wages below US$25,000 included fast food and counter workers, fast food cooks, dishwashers, laundry and dry-cleaning workers, child care workers, and food preparation workers. The highest annual wages were for health care occupations—specifically, physicians and surgeons—followed by chief executives (see Table 3.1). The wages for these occupational categories exceeded US$200,000. In this context, the largest health care occupations are notable in several ways: •
•
At US$82,000 in 2018, the average wage for all health care workers in the Healthcare Practitioners and Technical Occupations far exceeded the average annual wage for all occupations in the United States—US$51,960. Only three of these occupational categories had an annual wage lower than US$51,960—licensed practical and licensed vocational nurses (US$47,050); medical records and health information technicians (US$44,010); and health practitioner support technologists and technicians (US$36,930). This was not the case for the Healthcare Support Occupations. In 2018, at US$32,380, the average annual wage for all health care workers in the Healthcare Support Occupations was very much lower than the average annual U.S. wage for all occupations. Furthermore, within this category, two occupations fell below US$30,000 annually—nursing assistants (US$29,580) and home health aides (US$25,330).
Trends in wages for health care occupations between 2003 and 2018 are also notable. Overall, workers in Healthcare Practitioners and Technical Occupations saw wages increase about 29% between 2003 and 2010, and even though wages increased for these occupations between 2010 and 2018, the rate was much lower, at 15%. The increases between 2010 and 2018 were greatest for family and general practitioners (21.8%); PAs (24.4%); and medical records and health information technicians (25.7%).
Goldsteen74024_03_CH03_79-124_03-18-20.indd 82
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
83
Overall, workers in Healthcare Support Occupations saw wages increase about 18% between 2003 and 2010, and somewhat more between 2010 and 2018—about 20%. The increases between 2010 and 2018 were similar for the two occupations with trend data. Medical assistants and home health aides experienced about 16% growth in wages between 2010 and 2018. TABLE 3.1 Wages for Largest Health Care Occupations, 2003 to 2018 Mean Annual Wage Occupational Category Healthcare Practitioners and Technical Occupations (All)
2003 (US$)
2010 (US$) 2018 (US$)
55,380
71,280
82,000
—
—
210,980
Surgeons
190,280
225,390
255,110
Family and general practitioners
139,640
173,860
211,780
General internists
160,130
189,480
196,490
78,620
109,380
123,670
All physicians and surgeons
Pharmacists Nurse practitioners Physician assistants
110,030 64,790
87,140
108,430
—
—
79,530
51,230
67,720
75,510
—
—
65,260
Licensed practical and licensed vocational nurses
33,210
41,360
47,050
Medical records and health information technicians
26,550
35,010
44,010
—
—
36,930
22,750
26,920
32,380
—
—
47,980
Medical assistants
24,940
29,760
34,540
Nursing assistants
—
—
29,580
Home health aides
19,180
21,760
25,330
Therapists (including occupational, physical, radiation, respiratory, and other) RNs Diagnostic-related technologists and technicians (including cardiovascular technologists and technicians, diagnostic medical sonographers, nuclear medicine technologists, radiologic technologists, magnetic resonance imaging technologists, and others)
Health practitioner support technologists and technicians (including dietetic, pharmacy, psychiatric, respiratory therapy, surgical, and other technicians and technologists) Healthcare Support Occupations (All) Physical therapist assistants and aides
NOTE: 2018 occupations were compared to those in 2003 and 2010 when the occupational category matched. SOURCE: U.S. Department of Labor, Bureau of Labor Statistics. (2004b). May 2003 national occupational employment and wage estimates. Retrieved from https://www.bls.gov/oes/tables.htm; U.S. Department of Labor, Bureau of Labor Statistics. (2011b). May 2010 national occupational employment and wage estimates. Retrieved from https://www.bls.gov/oes/tables.htm; U.S. Department of Labor, Bureau of Labor Statistics. (2019e). May 2018 national occupational employment and wage estimates. Retrieved from https://www.bls.gov/oes/current/oes_nat.htm#29-0000
Goldsteen74024_03_CH03_79-124_03-18-20.indd 83
3/19/20 10:53 AM
84
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Finally, it should be noted that many factors lead to wage variation “within” health care occupations. Among these are state and regional differences. For example, the average annual salary for RNs in 2019 varied from a low in South Dakota of US$57,010 to a high in California of US$102,700. States on the West Coast and in the Northeast tended to have higher salaries than other parts of the country (Indeed, 2019). Another factor is unionization. Some studies have shown that unionized workers in all fields earn more than nonunionized workers in the same occupation. In 2018, among Healthcare Practitioners and Technical Occupations, 11.4% were union members, while 8.1% of Healthcare Support Occupations were union members (BLS, 2019g).
Practice Settings of Health Care Workers The BLS also categorizes health care workers by their practice setting: (a) those who work in hospitals and (b) those who work in nonhospital settings, including offices of physicians, chiropractors, and optometrists; outpatient care centers; home health care services; and skilled nursing care facilities (BLS, 2019d). Table 3.2 contains information on practice settings between 2003 and 2018. In 2018, 40% of health care workers practiced in hospitals, up from about 37% in 2003. Employment in physician offices and nursing care facilities declined, while employment in outpatient care centers and home health care services increased as a percentage of all health care employment. These trends reflect the changing emphasis within the health care system on providing care in ambulatory settings other than physician offices, and in homes. Table 3.2 also confirms the continuing importance of the hospital in providing care.
Demographic Characteristics of Health Care Workers Table 3.3 contains information about the gender, race, and ethnicity of persons employed the largest health care occupations in both categories: (a) Practitioners and Technical Occupations and (b) Healthcare Support Occupations. Several observations stand out related to the nonrandom variation in the demographic features of the occupations:
TABLE 3.2 Percentage of Health Care Workforce Employed in Selected Practice Settings, 2003 to 2018 Percentage of Health Care Workforce Practice Setting
2003
2010
2018
Hospitals
36.9
39.9
40.0
Physician offices
12.3
9.9
9.0
Outpatient care centers
6.4
7.5
10.7
Home health care services
5.4
6.6
8.3
13.8
11.8
9.3
6.9
10.9
8.7
18.3
13.4
14.0
Nursing care facilities Other health care services All other
SOURCE: U.S. Department of Labor, Bureau of Labor Statistics. (2004b). May 2003 national occupational employment and wage estimates. Retrieved from https://www.bls.gov/oes/tables.htm; U.S. Department of Labor, Bureau of Labor Statistics. (2011b). May 2010 national occupational employment and wage estimates. Retrieved from https://www.bls.gov/oes/tables.htm; U.S. Department of Labor, Bureau of Labor Statistics. (2019d). Current population survey: Employment and earnings, 2018. Retrieved from http://www.bls.gov/cps/cpsa2018.pdf, Table 18.
Goldsteen74024_03_CH03_79-124_03-18-20.indd 84
3/19/20 10:53 AM
3
•
•
•
•
•
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
85
Although 46.9% of the entire U.S. workforce is comprised of women, all of the largest health care occupations are majority female. The occupation with the lowest percentage of women is pharmacy, with 63.4%. Most occupations are above 70% women, with the highest proportion of women being in medical records and health information technicians (93.6%). While the total U.S. employed population is 78% White, eight of the largest health care occupations have fewer than 78% White workers, and Whites are overrepresented in the remaining five—physicians and surgeons, diagnostic-related technologists and technicians, nurse practitioners, PAs, and physical therapist assistants and aides. Physicians and surgeons and PAs have a particularly high percentage of White workers (90.3% in both). African Americans comprise 12.3% of the U.S. employed population. They are overrepresented in the health care occupations in six of the largest—RNs, health practitioner support technologists and technicians; licensed practical and licensed vocational nurses; medical records and health information technicians; nursing, psychiatric, and home health aides; and medical assistants. Given the percentage of their overall workforce participation (12.3%), African Americans comprise a particularly high percentage of licensed practical nurses (30.4%) and nursing, psychiatric, and home health aides (35.8%). Asian Americans comprise 6.3% of the U.S. employed population. They are overrepresented in the health care occupations in eight of the largest categories, and they comprise a particularly high proportion of physicians and surgeons (19.8%), pharmacists (23.1%), and physical therapists (14.3%), given their overall workforce participation (6.3%). Hispanic Americans comprise 17.3% of the U.S. employed population. They are overrepresented in only one of the largest health care occupations—medical assistants (28.6%). They are particularly underrepresented in the following occupations— RNs, physical therapists, physicians and surgeons, pharmacists, nurse practitioners, PAs, and physical therapist assistants and aides.
Therefore, in thinking about demographic trends in health care occupations, the information in Table 3.3 should be considered a “snapshot” that is different now than in the past and will inevitably change again as the health care system and society evolve. For example, women are increasingly entering occupations in which they were previously scarce, and therefore, the results in Table 3.3 may be age-specific. This is especially true of physicians. Women were once a small proportion of entering medical school classes. Since at least 2009, they have been about 47% of entering classes (Association of American Medical Colleges [AAMC], 2019a). In 2017, for the first time, more women than men enrolled in medical school (50.7%; AAMC, 2017a). Therefore, younger physicians are more likely to be women than older physicians. Similarly, percentages regarding race and ethnicity in Table 3.3 may also reflect changes within the society. For example, prior to the passage of Medicare, hospitals were segregated, especially in the South. The Medicare legislation of 1965 mandated desegregation in order for hospitals to receive these funds (Smith, 2016). Now, we see the legacy of the Medicare legislation in the demographic diversity of health care occupations. Education varies by health care occupation, as well. Eighty-five percent of health care employment was in occupations that typically require some education beyond high school for entry. Occupations that typically require training and a certificate or license beyond high school but not a college degree made up nearly one-third of health care employment in May 2014. Nursing
Goldsteen74024_03_CH03_79-124_03-18-20.indd 85
3/19/20 10:53 AM
86
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
assistants and licensed practical and licensed vocational nurses are examples of these occupations. Occupations that typically require an associate’s degree made up another third of health care employment; registered nurses represented over 71 percent of these jobs. Pharmacy technicians and home health aides were the largest health care occupations for which workers typically need a high school diploma or less education for entry. Education categories represent the most common education level needed for entry. These levels may differ from the educational levels of workers in the occupation. (BLS, 2014)
Complexity of the Health Care Workforce In 2012, the AMA reported 826,000 active physicians (those with an MD or DO degree and working in patient care; NCHS, 2015a, Table 93). The ratio of other health personnel to physicians reflects the complexity of the U.S. health care system. With about 1,000,000 physicians
TABLE 3.3 Demographic Characteristics of Workers in the Largest Health Care Occupations, 2018 Percentage of Employed Population Women
White
African American
Hispanic
Asian
Health Care Practitioners and Technical Occupations
75.0
75.2
12.6
8.5
9.9
RNs
88.6
75.5
13.1
7.2
9.0
Health practitioner support technologists and technicians
80.6
75.5
14.1
15.0
6.9
Licensed practical and licensed vocational nurses
87.8
62.0
30.4
11.5
5.1
Physical therapists
69.5
76.4
7.4
4.3
14.3
Physicians and surgeons
72.1
90.3
2.9
8.2
19.8
Diagnostic-related technologists and technicians
67.9
79.5
11.8
14.7
5.6
Pharmacists
63.4
67.9
7.2
4.4
23.1
Medical records and health information technicians
93.6
72.3
15.5
9.2
9.2
Nurse practitioners
87.2
79.1
11.2
2.6
8.8
PAs
72.1
90.3
2.9
8.2
5.1
Health Care Support Occupations
87.1
64.3
26.2
18.3
5.7
Nursing, psychiatric, and home health aides
89.3
55.8
35.8
16.3
5.4
Medical assistants
90.6
74.1
15.3
28.6
4.5
Physical therapist assistants and aides
67.4
85.0
6.1
7.1
6.7
U.S. Employed Population, 16 Years and Older
46.9
78.0
12.3
17.3
6.3
Occupational Category
PA, physician’s assistant; RN, registered nurse. NOTE: Estimates for the above race groups (White, Black or African American, and Asian) do not sum to totals because data are not presented for all races. Persons whose ethnicity is identified as Hispanic or Latino may be of any race. SOURCE: U.S. Department of Labor, Bureau of Labor Statistics. (2019f). Labor force statistics from the current population survey, 2018. Retrieved from https://www.bls.gov/cps/cpsaat11.htm
Goldsteen74024_03_CH03_79-124_03-18-20.indd 86
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
87
in active practice, there were more than 19 other health care workers for each physician. In 1988, there were close to 13 other health care workers for each physician. This compares to about three other health care workers per doctor in 1920 (Donabedian, Axelrod, & Wyszewianski, 1980). Most of these other personnel have skills learned through special training. Only about one-fifth is “nonhealth care”—specifically clerical, custodial, or similar personnel. Under the laws of most states, only physicians, dentists, and a few other types of practitioners may serve patients directly, without being authorized to do so by another health professional who is licensed for independent practice. Among the other independent health professions are chiropractic, optometry, podiatry, psychotherapy, and, in some states, midwifery and physical therapy. For the most part, nurses work on the orders of physicians, although in certain circumstances and in some states, nurses with specific advanced degrees, called“nurse practitioners” or“advanced practice nurses”(see later discussion), can work independently. Other types of health care providers working on the orders and under at least the general supervision of physicians include clinical laboratory, x-ray, electrocardiographic, and other specialized technicians such as cardiorespiratory therapists, those who operate kidney dialysis machines, and those who work in rehabilitation services. In dentistry, one finds dental hygienists, dental technicians, and dental assistants working under the orders of dentists. Certain other health professionals (e.g., nutritionists and dietitians; physical, occupational, and speech therapists and audiologists; statisticians and statistical clerks; and medical record librarians and information technology specialists) work both under physicians’ orders and, in certain circumstances, such as school or industrial settings, independently. Many of these “other health” occupations originally developed out of the nursing profession. Today, in countries less developed than the United States, work done in the United States by a laboratory technician, physical therapist, or dietitian is often done by a nurse (and at times even by a physician). At the same time, in the United States, medical practice itself has become more and more specialized. It is interesting to note that the same phenomenon has occurred within the largest health profession, nursing. Consider, for example, the development of the nurse specialties such as operating room nurse, intensive care nurse, nurse anesthetist, nurse midwife, and nurse practitioner. In the next two sections, we consider the two most influential health professions— medicine and nursing—in more detail.
PHYSICIANS Among health care occupations, physicians are not the largest group. Nursing is the largest, with about 3 million nurses employed in the United States in 2018. In contrast, there were 679,280 physicians practicing that year. Of these, 114,130 were family and general practitioners, 37,820 were general internists, 34,390 were surgeons, 31,060 were anesthesiologists, 28,490 were pediatricians, and 18,590 were obstetricians and gynecologists. The remaining 389,180 physicians were among the many specialists in the field of medicine (BLS, 2019e). However, as the professionals with authority over most health care delivery and most other health professionals, physicians’ importance transcends their numbers. Despite changes in the health care system that have usurped some of their traditional functions, their authority as leader remains intact.
Historical Background The profession of medicine in America has changed dramatically over the course of history. The role, training, and expectations of pre-Revolutionary War physicians are practically unrecognizable to us today, as the following description of the profession in the 18th century attests:
Goldsteen74024_03_CH03_79-124_03-18-20.indd 87
3/19/20 10:53 AM
88
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
[There were] 3,500 practicing physicians in the colonies in 1775. Of these, less than 300 had received a medical degree. Only a handful had graduated from the tenyear-old Philadelphia Medical College. The remainder, mainly from the middle and southern colonies, attended the European medical schools. Admission requirements included a knowledge of the classics and a husky bankroll. By the time the graduating thesis had been written in Latin, the student had been exposed to all the latest theories that Edinburgh, London, or the Continent had to offer. Theories aplenty—but the fledgling M.S.’s returned to America without having seen a patient! (Wilbur, 1980, p. 2) The bulk of the practicing physicians in the colonies—including all of the independent New Englanders—were apprentice trained. Some had undergraduate degrees, whereas others were no more than 15 years old when starting their medical careers. Benjamin Rush noted that the only prerequisite for a “doctor’s boy” was the ability to stand the sight of blood! His teacher was likely to be a prominent physician-surgeon, well qualified to guide the student through the maze of anatomy, osteology, the compounding of medicine, surgery, and the writings of Hippocrates. Toward the end of the three- to six-year apprenticeship, the doctor’s boy was doing his own bloodletting, tooth-pulling, wound dressing, and some minor surgery. His certificate of proficiency gave the same practicing privileges as a medical student from the continent (Wilbur, 1980). Since then, a vast health care system has developed in the United States to facilitate the practice of the allopathic physician (MD), whose early days in America are described in the foregoing passage. This next section of the chapter describes physician training and practice today.
Medical Education In the United States, including Puerto Rico, there were 154 fully accredited allopathic medical schools in 2019 (Liaison Committee on Medical Education [LCME], 2019). Allopathic (MD) medical schools in the United States and Canada are accredited by a voluntary agency called the LCME. This agency comprises representatives from the AMA and the AAMC and their Canadian counterparts. There were also 35 osteopathic (DO) medical schools accredited by the American Osteopathic Association (AOA) in 2019 (AOA, 2019). All but a few medical schools are attached to a university. In the university, the medical school is invariably a separate college with its own dean (or the equivalent), sometimes loosely linked with other health professional schools in a “health sciences center.” About 60% of the medical schools are sponsored by state governments as part of state public universities; the rest are under private auspices. All the schools have received substantial, although primarily indirect, financial support from the federal government for many years.
Undergraduate Medical Education Entry to the U.S. medical schools usually requires a university bachelor’s degree. The standard medical school program lasts another four years and is termed “undergraduate” medical education even though, in the university sense, it is graduate education. This is because, in medical training, the postmedical degree, a residency experience, is considered“Graduate Medical Education” (GME). Admission to medical school is selective. For the class entering in 2018 to 2019, there were 52,757 applicants, of whom 21,622 found places (matriculants), a ratio of about 2.4:1
Goldsteen74024_03_CH03_79-124_03-18-20.indd 88
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
89
(AAMC, 2019a). The ratio of applicants to places has fallen slightly since the 1990s, from a high of 2.7:1 for the 1995 to 1996 applicants (AAMC, 2006a). Of the applicants for 2018 to 2019, about 51% were women, about 47% were White, 21% were Asian, 8% African American, and 6% Hispanic or Latino. The race and ethnicity of the remaining 18% were mainly combinations of these (AAMC, 2019a). As for graduates of medical school, among the class of 2017 to 2018 47% were women, about 56% were White, 21% Asian, 5.7% African American, and 5.4% Hispanic or Latino (AAMC, 2019a). This profile of graduates is similar to the matriculants for 2018 to 2019, but with a lower percentage of women and a higher proportion of Whites and a lower percent of African Americans and Hispanics. The proportion of women in medicine has been increasing since the 1960s. In 1965, women comprised less than 10% of applicants, matriculants, and graduates. This percent began rising steeply in 1970, and by 1990, it was about 40%. Between 1990 and 2009, women increased their numbers to about 48% of applicants, matriculants, and graduates (AAMC, 2016). And as previously noted, women comprised over half of medical school matriculants in 2017 (AAMC, 2017). The record for increasing the admission rates for African Americans does not match that for women. From the 1970s to 1990, the percentage of African American admissions remained unchanged, at about 6%. By 1995, this number had increased to 9%. However, by 2000, it had fallen to 7.5% and to 6.6% in 2006 (AAMC, 2006b). It had risen to 8.3% by 2019 (AAMC, 2019c). Between 2016 and 2019, Hispanic admissions remained around 6%. During the same period, Asian Americans accounted for just over one-fifth of all admissions (AAMC, 2019c). The ratio of full-time faculty to students is very high, much higher than in virtually any other branch of education. In fact, in medical education, the number of faculty actually exceeds the number of students by a ratio of close to 1.77:1 (Barzansky & Etzel, 2005). This is one of the reasons medical education is so expensive (Krakower, Ganem, & Jolly, 1996). Although tuition and fees account for only about 4% of total medical school expenditures, it is not unusual for a student to graduate with upward of US$100,000 in debt accumulated for undergraduate and medical education. An unusual aspect of the U.S. medical education is that a significant number of U.S. citizens are trained to be physicians in offshore, for-profit medical schools, established for the purpose of providing places for at least some of those applicants to the U.S. schools who cannot gain entry to them. These offshore schools are not recognized by the LCME. A number of states, with New York in the lead (Jonas, 1981, 1984), over the years have established their own programs for certifying graduates of these programs as eligible to take the state licensing examinations, as well as certifying the schools for the purpose of permitting their students to take clinical clerkship training in hospitals in the respective states (Monahan, 2001). This is true in the 21st century, as well.
Graduate Medical Education Before entering a residency and/or fellowship program, new physicians must complete four years of medical education, in either an allopathic (MD) or an osteopathic (DO) medical school. In academic year 2016 to 2017, there were 10,672 Accreditation Council for Graduate Medical Education (ACGME)-accredited residency programs, an increase from 8,814 in 2009 to 2010. There were 4,037 specialty programs and 5,307 subspecialty programs.1 The majority of residency programs take three to four years to complete. Family medicine, internal medicine, obstetrics and gynecology, surgery, psychiatry, emergency medicine, and pediatrics have the most residency programs (n = 540, 469, 278, 269, 226, 212, and 207, respectively; ACGME, 2017).
Goldsteen74024_03_CH03_79-124_03-18-20.indd 89
3/19/20 10:53 AM
90
■
I
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Sponsoring institutions are those are responsible for meeting the ACGME criteria for residency programs and maintaining accreditation. In 2016 to 2017, there were 821 sponsoring institutions, of which 171 (20.8%) were in the initial phase of accreditation. Sponsors with one program and those with two to five programs accounted for the majority of all sponsoring institutions (32.3% and 28%, respectively). Sponsoring institutions are largely general/teaching hospitals (n = 402, 52.6%) and academic medical centers/medical schools (n = 112, 14.7%). However, the academic medical centers/medical schools accounted for the same number of programs and residents as the general/teaching hospitals (ACGME, 2017). A total of 752 residency programs were newly accredited during the year 2016 to 2017. Of the newly accredited programs, 331 (44%) were medical programs, 177 (23.5%) were hospital based, and 244 (32.4%) were surgical programs. The specialties with the highest number of newly accredited programs were internal medicine, family medicine, and interventional radiology. Maternal–fetal medicine, gynecologic oncology, and reproductive endocrinology and infertility (all subspecialties of obstetrics and gynecology) had the highest number of new programs among all subspecialties. About 75% of physicians enrolled in GME in 2013 to 2014 were graduates of the U.S. allopathic medical schools, and 8.6% were graduates of osteopathic medical schools. About 41,500 persons completed residency training in 2013 to 2014 (ACGME, 2015). More than 31,000 persons enrolled in GME in 2013 to 2014 were international medical graduates (IMGs; ACGME, 2015). IMGs who are not U.S. citizens or permanent residents can enter GME programs under the temporary work (H) or training (J) visa programs. Those IMGs with a J visa can participate in the J-1 visa waiver program, which allows physicians to remain in the United States if they provide primary care in federally designated health professional shortage areas (HPSAs) for at least three years after completing their GME program.
Medical Practice Describing medical practice includes discussions of licensing, employment status, practice type, and practice setting.
Licensure A license is required for all physicians who wish to practice medicine. In the United States, medical licenses are granted by the states. To qualify for a medical license in New York state, for example, a physician must be of good moral character, be at least 21 years of age, and meet education, examination, and experience requirements. These are: •
•
•
Education: have received an education, including a degree of Doctor of Medicine (MD) or Doctor of Osteopathy (DO) or equivalent degree in accordance with the commissioner’s regulations; Experience: have experience satisfactory to the board and in accordance with the commissioner’s regulations. In our time, few medical school graduates enter practice before completing at least three years of residency training; and Examination: pass an examination satisfactory to the board and in accordance with the commissioner’s regulations (NYSED.gov, 2019).
All states have requirements similar to these.
Goldsteen74024_03_CH03_79-124_03-18-20.indd 90
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
91
Ownership or Salaried Position? The percentage of U.S. physicians who own their practices has been declining. AMA Research reported on the 2018 AMA Physician Practice Benchmark Survey, which obtained information on this issue. The survey included 3,500 practicing physicians nationwide providing at least 20 hours of patient care per week and not working for the federal government. The study found that only 45.9% of practicing physicians owned their practices, compared to 47.4% who were employees. Furthermore, between 2012 and 2018, physician ownership declined: •
•
In 2018, 54% of physicians worked in practices that were entirely owned by physicians, but that number had fallen since 2012, when it was 60.1%. However, the downward trend in physician practice ownership may be slowing as half of the decline occurred in the first two years of the six-year period. In 2018, the number of physicians working for a hospital or in a practice at least partly owned by a hospital had increased to 26.7% from 23.4% in 2012. (Henry, 2019)
Characteristics of physicians who are more likely to own their own practice were: •
• • •
Sex—In 2018, 52.1% of men had practice ownership, compared to 34.3% of women. Some of these differences may be due to the specialties that women choose, which have higher employment rates; these would include pediatrics. In 2018, 17% of women were pediatricians, compared to 7% of men. Also, women physicians tend to be younger than men physicians, and younger physicians are more favorable to employed positions. In 2018, about 22% of women physicians were under the age of 40, compared to 12% of men. Age—Older physicians are more likely to have practice ownership. About 54% of physicians 55 and older had ownership, compared to 25.5% of physicians under 40. Subspecialists—Nearly 65% of surgical subspecialists owned their practices, as did 52% of internal medicine subspecialists and almost 51% of radiologist subspecialists. Emergency physicians—These physicians had the lowest percentage of physician owners—26.2%. (Henry, 2019)
Solo, Small-, or Large-Group Practice? There has been rapid consolidation in the health care industry, particularly among physician groups. The percentage of U.S. physicians practicing in independent solo or small-group practices declined, whereas the percentage of physicians practicing in larger practices increased. The percentage of physicians practicing in independent or solo practices declined from 37.2% in 2000 (National Center for Health Statistics [NCHS], 2002 Table 2) to 31.5% in 2010 (NCHS, 2015b, Table 2), whereas the percentage of physicians practicing in larger practices (two or more) increased from 61.5% in 2000 to 68.1% in 2010. About one-fifth, or 22.6%, of visits occurred in multispecialty practices, and 45.8% were to single-specialty practices in 2010. The remaining 31.5% of office visits were to solo practitioners (NCHS, 2015b). In 2018, AMA Research reported changes in physician practices obtained from the 2018 AMA Physician Practice Benchmark Survey. Between 2012 and 2018, only the percentage of physicians belonging to a single-specialty group (43%) was stable. Solo practice declined from 18.4% in 2012 to 15% in 2018, while the size of group practices increased. In 2012, 61.4% of physicians were in practices of 10 or fewer, and in 2018, that number had declined to 57%. Consequently, the percentage of physicians in practices of 50 or more increased from 12.2% in 2012 to 15% in 2018 (Henry, 2019).
Goldsteen74024_03_CH03_79-124_03-18-20.indd 91
3/19/20 10:53 AM
92
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
The trend toward group practice is especially true for younger physicians when they do not own the practice, but are employed by it. Among the reasons for this mode of employment that younger physicians find attractive are receiving a regular income and comprehensive fringe benefits; the provision of medical malpractice insurance by the employer; regular hours and regular night and weekend coverage schedules; avoiding the difficulties associated with entering into private practice in many desirable living areas, many of which have an overabundance of physicians; avoiding the high costs of starting a private practice, a particular burden to so many of today’s new physicians who start professional life with a large debt accumulated during their medical training; and, finally, avoiding the tribulations of office practice dealing with managed-care-company scrutiny.
Primary Care or Other Specialty? Practice patterns vary greatly depending upon whether the physician has chosen primary care or another specialty. Specialization is one of the most prominent features of the organization of American medical practice. It is one of the major results of the explosion of biomedical knowledge and technology that began in the last third of the 19th century. In the arenas of complex pathophysiological states and complicated surgery, it has become ever more difficult for a physician to master in depth more than one small area of what biomedical science and technology make possible and have to offer. Thus, even within specialties, there is further subspecialization. For example, certain ophthalmic (eye) surgeons “do only retinas,” and certain orthopedic surgeons “do only hips.” Whereas the high-tech specialties demand a great depth of knowledge and skill in one particular area, the specialties of family medicine, primary care pediatrics, and primary care internal medicine demand a great breadth of knowledge and competency (Starfield, 1992). It is the case that many of the nonprimary care specialties focus on a relatively narrow range of knowledge and skills, although both are developed in great depth. In one sense, then, most of the developments in medical specialization in terms of ever-narrowing focus have made the practice of medicine easier for the physician within each specialty than it is in primary care. The knowledge–technology explosion is certainly one factor that accounts for the everincreasing specialization of American medicine. Another is the financial incentive that is part of specialization: There has almost always been more money to be made in the specialties than in primary care. At the same time, there has never been a health personnel planning policy in this country that might exert some external controls on the distribution of physicians between the primary care and specialty sectors and within each specialty sector itself. Specialization does have its advantages for patients. The high degree of knowledge and skill that specialists possess is beneficial to the patient who has a problem in that particular area of specialization. However, it also has its disadvantages. Specialists tend to focus on their specialty’s organ or organ system to the exclusion of others. Some, when facing a patient, see only the organ of their own specialty, not the whole person first. The patient’s overall well-being may suffer if there is no professional who can (a) see the patient as a whole person, (b) put together into one clinical picture observations derived from a variety of patient complaints arising from different organ systems, (c) guide the patient through an intelligent use of the knowledge of several specialists, and (d) set up an organized means for communication among specialists. This is not an argument against specialization per se; the vast expansion of medical knowledge requires such specialization, at least for a certain proportion of the profession. It is, however, an argument for a more rational approach to the organization of specialists and a significant improvement in the provision of primary care physician services, an argument that has a long history (Colwill, 1986; Geyman, 1986; Starfield, 1992; White, 1968). It is an argument for the“pro-patient”variant of the gatekeeper, as originally described by Somers (1983).
Goldsteen74024_03_CH03_79-124_03-18-20.indd 92
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
93
Internal medicine, geriatrics, family practice, general practice, and pediatrics are considered primary care specialties. Primary care includes health promotion and disease prevention, as well as diagnosis and treatment of acute and chronic health care problems. Primary care providers work in all health care settings, including ambulatory, hospital, long-term care, and the home. Their care is comprehensive—not limited to a specific organ system or diagnosis. While the primary care provider is often the first contact for patients, primary care emphasizes coordination of care. Primary care physicians collaborate with other health professionals and consult and refer patients, as appropriate, to specialists. Primary care providers are responsible for the overall health of a population of patients. Their relationship with patients is usually long term. As a result, primary care stresses effective patient communication and encourages patients to be partners in health care with their physician. Primary care providers serve as their patients’ advocate, and they assist their patients in utilizing the total health care system (AAFP, 2019). Primary care physicians work in all settings, but most provide care on an ambulatory basis. Specialists may also see patients on an ambulatory basis, but often the specialist uses the hospital or ambulatory surgical centers more frequently. This model seems to be leading physicians in the United States to emulate a pattern based on the system in the United Kingdom, where primary care physicians, still called “general practitioners,” see patients almost exclusively on an ambulatory basis. The specialists, although seeing patients on both an ambulatory and inpatient basis, are virtually the only ones who handle hospitalized patients.
The Hospitalist In most other countries, physicians either see ambulatory patients only or work full time in hospitals. An important feature of medical practice organization in the United States is that most physicians see patients both on an ambulatory basis and as hospital inpatients. (A small percentage of doctors do not have hospital appointments.) However, the relatively new position of hospitalist is changing that. In 1996, Wachter and Goldman coined the term hospitalist to describe physicians who see patients solely on an inpatient basis. As they noted (Wachter & Goldman, 1996): [Taking into account] the realities of managed care [in the United States] and its emphasis on efficiency ..., we anticipate the rapid growth of a new breed of physicians we call“hospitalists”—specialists in inpatient medicine—who will be responsible for managing the care of hospitalized patients in the same way that primary care physicians are responsible for managing the care of outpatients. (p. 514) Their prediction seems to be a reality. This movement has grown in strength over the past decade. Reported advantages of the hospitalist approach include reduced patient length of stay, reduced per-case cost, decreased cost under several different risk-based payment systems, fewer inappropriate admissions through the ED, improved patient satisfaction, reduced readmission rates, increased admissions from remote physicians, and standardized care protocols and disease management programs (Haugh, 2002). Six years after they published their first article on the hospitalist concept, based on a literature review of studies of the new model, Wachter and Goldman (2002) concluded: Empirical research supports the premise that hospitalists improve inpatient [care] efficiency without harmful effects on quality or patient satisfaction. ... [T]he clinical use of hospitalists is growing rapidly, and hospitalists are also assuming prominent roles as teachers, researchers, and quality leaders. The hospitalist field ... seems destined to continue to grow. (p. 487)
Goldsteen74024_03_CH03_79-124_03-18-20.indd 93
3/19/20 10:53 AM
94
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
The BLS defines hospitalist as a physician specializing in caring for patients throughout a hospital stay. This specialty is relatively new, departing from the past practice of having hospital physicians admit patients only for referring them to surgeons or other specialists for treatment. Hospitalists perform medical procedures, design treatment plans, and communicate and coordinate with patients and hospital staff, among other duties. (Royster, 2015) Recertification to become a hospitalist is offered to board-certified specialists by the American Board of Internal Medicine (ABIM), American Board of Family Medicine (ABFM), and American Board of Pediatrics (ABP). The Society of Hospital Medicine (2019) is accredited by the Accreditation Council for Graduate Medical Education (ACGME) to provide continuing education for physicians in hospital care only.
Medical Practice Issue: Physician Satisfaction The profession of physician has changed quite substantially in the last 50 years, becoming less autonomous as physician practices are incorporated into hospital systems, more physicians are salaried, and greater oversight of physicians is sought by health care payers like the Centers for Medicare & Medicaid Services (CMS) and the private insurance companies. Some studies have found physician dissatisfaction growing—for example, this survey, reported in 2017 by the Merritt Hawkins Team (2017): One of the largest physician surveys ever completed in the United States, Survey of America’s Physicians: Practice Patterns and Perspectives, paints a portrait of an evolving physician workforce whose practice styles and attitudes are changing. Based on over 17,263 physicians nationwide, this physician survey is conducted by Merritt Hawkins on behalf of The Physicians Foundation, a non-profit organization that seeks to advance the work of practicing physicians and help facilitate the delivery of health care to patients. Data about today’s doctors derived from the survey include: • • • • • • • • •
80% of physicians are overextended or are at capacity, with no time to see additional patients. 48% of physicians said their time with patients is always or often limited. Employed physicians see 19% fewer patients than practice owners. 46.8% of physicians plan to accelerate their retirement plans. 20% of physicians practice in groups of 101 doctors or more, up from 12% in 2012. Only 17% of physicians are in solo practice, down from 25% in 2012. 27% of physicians do not see Medicare patients, or limit the number they see. 36% of physicians do not see Medicaid patients, or limit the number they see. Only 6% of physicians said ICD-10 has increased efficiency in their practices. (Merritt Hawkins Team, 2017)
The Physicians Foundation (2019) was founded in 2003, after a class-action lawsuit was brought against private sector payers by physicians, 19 state medical societies, and three county medical societies. The suit resulted in a monetary settlement that established the Physicians Foundation, which now serves as a voice for physicians to express their dissatisfaction with the profession.
Goldsteen74024_03_CH03_79-124_03-18-20.indd 94
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
95
Physician Supply In 2012, about 785,000 (>95%) of all physicians worked in patient care. Of those, 75% were in office-based practice, about 15% were house staff (residents in training), and more than 10.5% were fully qualified physicians working full time in hospitals (NCHS, 2015a). About 26% of the active MDs received their medical training outside the United States and Canada. That is quite a remarkable percentage, considering the size of and the ongoing investment in the U.S. medical education system. As Mullan (1995) has pointed out in an observation that is still true, despite the output of the U.S. medical schools, physician needs in many medically underserved areas could not be met without a steady influx of IMGs (both the U.S. citizens and foreign nationals who have attended non-U.S. medical schools) to U.S. residency programs, especially those in hospitals situated in those same underserved areas. Slightly more than 20,000 of the physicians active in 2002 were in federal governmental service, most of them in the armed forces or units of what was formerly the U.S. Public Health Service. More than 80% of the federal physicians worked in patient care services. These percentages have varied marginally since 1975. (Since 2003, Census reports have merged both federal and nonfederal physicians.) The slightly more than 41,000 professionally active physicians who were not engaged in patient care worked in medical teaching, administration, research, state and local health services, the pharmaceutical industry, and the like. Among the several medical specialties, the largest numbers were found in internal medicine (about 117,000), general and family practice (about 79,000), pediatrics (>57,000), obstetrics and gynecology (close to 34,600), and general surgery (close to 24,000; NCHS, 2015a). In 2012, the overall MD physician/population ratio was 28.3 per 10,000 (NCHS, 2015a, Table 92). This is up from a post–World War II low in 1960 of 14.5 and from the 1980 figure of 20 per 10,000. There was a wide variation in physician/population ratio by geographic area. The state with the highest ratio, Massachusetts (many medical schools, given the population size), had about 44.6 per 10,000, whereas the state with the lowest ratio, Idaho, had just under 18.4 per 10,000. Although there are no known differences in health status that vary consistently with physician/population ratios, utilization of health services is generally higher in those areas that have more physicians (Eisenberg, 1986, pp. 15–17; Wennberg, Fisher, & Skinner, 2002; Wennberg & Members of the Dartmouth Atlas of Health Care Working Group, 1996). Among the factors influencing the amount of work physicians do are income goals, desired practice style, personal characteristics, practice setting, and standards established by clinical leadership (Eisenberg, 1986).
Physician Workforce Projections In 1986, Steven Jonas had this to say about the issue of physician supply (Jonas, 1986): At the same time that geographical distribution is quite uneven and remains a serious problem, the nation is confronting a general oversupply of physicians. ... This situation creates a different set of problems [from that created by the former perceived undersupply of physicians]. To determine rationally the size of the physician manpower pool, some measure of need or demand for services is necessary ... but need and demand alone cannot be the base for determining manpower [supply]. Patterns of practice vary ... , productivity varies ..., and supply affects demand. ... One can try to rely on the force of an economic market to [manage] the size of the pool, or one can regulate supply, or do some of both. This is, in general, what has been tried to date; it has [obviously] not been very effective. (p. 65)
Goldsteen74024_03_CH03_79-124_03-18-20.indd 95
3/19/20 10:53 AM
96
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
And so it seemed at that time that there was an impending oversupply of physicians. Now turn to 2002. The leading journal of health policy analysis, Health Affairs, devoted a good portion of its January to February 2002 issue to eight articles on the subject (see Health Affairs, 21[1], pp. 140–171). The lead article (Cooper, Getzen, McKee, & Laud, 2002) held that the nation was moving back to a stage of undersupply. However, that position was disputed strongly (e.g., Weiner, 2002). The fact is the answers still are not clear. Of course, proper supply cannot be determined until demand and its relationship to supply are understood; some controls over what doctors do and do not do and what other health professionals could do just as well are established; and some arrangements for rationalizing the geographic distribution of physicians are made (see Mullan, 2002). That, however, would require a national physician supply and distribution policy and a planning program to implement it. Historically, neither has ever existed in the United States, despite the fact that the first national study on the issue that recommended that such a policy be created was published in 1959 (Fordham, 1980). Given our national aversion to health services planning, it is unlikely that one will be implemented in the foreseeable future. Despite what has just been said about the total absence of organized health care services planning in the United States, forecasting is a function in which we are still engaged. Trying to forecast how many and what types of physicians are needed to meet the health care needs of the U.S. population as it grows and ages over the next several decades is a complex process. One major factor that must be considered is trends in health care usage. Over the past 50 years, the adequacy of the future supply of physicians in the United States has been analyzed regularly. This has been done in order to provide for timely changes to be made to educate future generations of physicians efficiently and effectively. However, the changes that have been made have been the result of medical schools, and in certain cases, state governments, acting independently. Previous physician workforce planning analyses have resulted in the improvement of and changes to the medical education infrastructure, and prompted governmental increases in funding of medical education resources. In the 1950s and 1960s, for example, reactions to projections of physician shortages prompted the U.S. medical schools to expand their programs, and immigration of physicians, trained at foreign medical schools, was promoted successfully to increase physician supply. In the 1980s and 1990s, with the increase in health care costs mounting sharply, and the emphasis on greater efficiency and cost containment, there was an increased reliance on the use of primary care physicians, that is, family practitioners, pediatricians, and internists. This shift led health care analysts to forecast a surplus of specialists and a corresponding need for more generalists. Today, there is concern about the growth of undergraduate medical education without a commensurate growth in GME, that is, residency programs. As discussed earlier, graduates of medical school must complete a residency program in order to practice medicine. However, GME is not expanding, and this problem is being discussed by policy makers, as summarized by Edelman and Romeiser: There is general, but not universal, agreement that we either have or will have a shortage of physicians. All recognize that GME is the rate-limiting step in the production of practicing physicians in this country. The output of U.S. nationals who will be candidates for medical residencies is in the process of being accelerated significantly by expansion in size and number of U.S. schools offering training for the MD and DO degrees and also by rapid expansion of the “offshore” model (i.e., schools located abroad training mostly U.S. nationals for entry into the U.S. GME
Goldsteen74024_03_CH03_79-124_03-18-20.indd 96
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
97
system). Thus, both public demand for additional physicians as well as demand from an increasing number of U.S. medical school graduates seeking residency positions will apply significant pressure for additional GME training opportunities. An interesting consequence of the projected substantial increase in demand for GME training by U.S. nationals is that availability as opposed to choice will play an increasingly important role in specialty selection. Thus, for example, if newly funded GME positions are confined to primary care, we can predict a significant increase in the numbers of U.S. nationals training in those specialties. ... On the other hand, public funding, which is the main source of GME support, has been effectively “capped” since the passage of the Balanced Budget Act (BBA) of 1997, and there are few signs that the political process favors provision of significant new resources. (Edelman & Romeiser, 2010, p. 149)
Physician Supply Model In 1993, the Health Resources and Services Administration’s (HRSA) Bureau of Health Professions, now the Bureau of Health Workforce (BHW), developed the Physician Supply Model (PSM), a demographic utilization-based computerized system, to forecast the supply and specialization areas for 18 medical specialties required to maintain a high quality of physician services in the United States through 2020 (Cooper, 1995). Since 2000, the PSM has modeled physician supply needs utilizing figures obtained from the NCHS, the AMA, and the AOA regarding the supply of physicians in the workforce in a given year, the number of newly graduated medical doctors from United States and international medical schools during that year, and the depletion of that year’s physician supply as a result of death, disability, retirement, or career change. The PSM calculates the number of active physicians in a given year, with breakdowns by demographic characteristics, including age, gender, type of medical degree (MD or DO), medical specialty, whether the medical degree was earned in the United States or internationally (USMG or IMG), and the physician’s primary activity. The PSM also determines the number of full-time equivalent (FTE) physicians (where one FTE equals the average annual patient care hours per physician in the year 2000), varying by specialty. Since calculation of PSM FTEs began in 2000, gender and age have been found to influence the estimate of FTEs, with women and older physicians tending to work fewer FTEs. Accordingly, as the population of active physicians has aged and more women have become physicians, the number of FTEs per active physician has decreased over the past several years (BHW, 2008). Physician productivity, which must be taken into account when forecasting the supply of physician services, is estimated on the basis of several factors, including the number of hours during which patient care is provided, and the number of patients seen. The PSM takes into consideration trends in the average number of hours worked and whether changes in health care delivery can alter the duration and number of patient visits, thereby affecting physician supply needs. A report by the BHW in 2008 suggested supply imbalances in many medical specialties, although rebalancing residency programs to areas of greatest need will help mitigate severe imbalances. The supply of primary care physicians is growing slightly faster than demand, and this trend could help to relieve the current undersupply of primary care physicians in some federally designated shortage areas. The projections suggested a growing shortage of specialists, with demand growing by approximately 62,000 more physicians than will be supplied. Surgical specialties account for more than half of this shortfall, although nonsurgical specialties such as cardiology and pathology show demand growing significantly faster than supply (BHW, 2008).
Goldsteen74024_03_CH03_79-124_03-18-20.indd 97
3/19/20 10:53 AM
98
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
One challenge with linear forecasts is that changes in technology and standards of care may flip a shortage to a surplus. For example, demand and volumes for open heart surgery have declined as treatments have shifted to minimally invasive and pharmacological. Nevertheless, projections continue to be made. The AAMC has been projecting physician supply every few years. The current projections from The Complexities of Physician Supply and Demand, 2017-2032: 2019 Update forecast the following shortages: •
•
•
•
•
•
We continue to project that physician demand will grow faster than supply, leading to a projected total physician shortfall of between 46,900 and 121,900 physicians by 2032. This projected shortfall range reflects updates to model inputs including updated population projections, revised starting demand and supply projections, updated estimates of physician specialty choice, larger starting-year shortfall estimates based on recently revised federal health professional shortage area (HPSA) designations for primary care and mental health, and lower projections of future insurance coverage expansion. The projected range is similar to the previous (2018) study’s projected shortfall range for 2030 of between 42,600 and 121,300 physicians. A primary care physician shortage of 21,100 to 55,200 physicians is projected by 2032. The shortfall range reflects the projected rapid growth in the supply of APRNs and PAs and their role in care delivery, trends that might strengthen the nation’s primary care foundation and improve access to preventive care, and an estimate by the Health Resources and Services Administration that nearly 14,472 primary care physicians are needed to remove the primary care shortage designation from all currently designated shortage areas. Projected shortfalls in non-primary care specialty categories of 24,800 to 65,800 physicians, including a 14,300 to 23,400 shortfall in 2032 for surgical specialties. The range reflects different assumptions about shifting workforce patterns for physicians and other professionals. In the surgical specialties, a largely stagnant projected supply also contributes to projected shortages. Demographics—specifically, population growth and aging—continue to be the primary driver of increasing demand from 2017 to 2032. During this period, the U.S. population is projected to grow by 10.3%, from about 326 million to 359 million. The population under age 18 is projected to grow by only 3.5%, while the population aged 65 and over is projected to grow by 48.0%. Because seniors have much higher per capita consumption of health care than younger populations, the percentage growth in demand for services used by seniors is projected to be much higher than the percentage growth in demand for pediatric services. Achieving population health goals will raise demand for physicians in the long term. This scenario models the implications for physician demand associated with achieving select population health goals like reducing excess body weight; improving control of blood pressure, cholesterol, and blood glucose levels; and reducing smoking prevalence. Under this scenario, the longevity associated with improved population health would result in greater demand for services by 2032. The demand for physicians would thus be 33,900 FTEs higher in 2032 relative to demand levels in the absence of achieving these goals. Although prevention efforts likely will reduce demand for some specialties, like endocrinology, demand for other specialties, like geriatric medicine, will increase. If underserved populations had care utilization patterns like those of populations with fewer access barriers, demand for physicians could rise
Goldsteen74024_03_CH03_79-124_03-18-20.indd 98
3/19/20 10:53 AM
3
•
•
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
99
substantially. Improved access to care is a national goal. We updated two hypothetical scenarios around the effects of removing access barriers. The health care utilization equity scenario models the implications for physician demand if currently underserved populations utilized health care at similar rates to populations facing fewer barriers to care. These estimates, which are excluded from the shortfall projection ranges, help illuminate the magnitude of current barriers to care and provide an additional reference point when gauging workforce adequacy. More than two out of five currently active physicians will be 65 or older within the next decade, and changes in physician retirement decisions could have the greatest impact on supply (Exhibit ES-2). Analysis of the AMA Masterfile to develop the starting supply finds that physicians over age 65 account for 15% of the active workforce, and those between ages 55 and 64 make up 27% of the active workforce. Thus, over 40% of the physician workforce is at risk for retiring over the next decade. The trend toward fewer weekly hours worked is reducing FTE-physician supply. Over the past decade, there has been a trend toward physicians of all ages working fewer hours, with the decline in hours worked particularly large when comparing recent hours-worked patterns of younger physicians relative to physicians of a similar age a decade ago. If this trend continues and hours worked decline even further, then by 2032 the national supply will be 20,900 FTE physicians lower than if physician hours-worked patterns remained unchanged (AAMC, 2019b).
Next we turn to a discussion of the nursing profession.
NURSES2 Nurses comprise the largest group of health care professionals in the United States, and their numbers are growing. Within nursing, RNs are the largest category, with 2.95 million active RNs in 2018, up from 2.2 million in 2001. In addition to RNs, nursing includes advanced nursing practice occupations: nurse practitioner (n = 179,650), nurse anesthetist (n = 43,520), and nurse midwife (n = 6,250; BLS, 2019e). However, the large number of nurses is not the sole basis for nursing’s significance. As the pillars and guardians of patient care, the importance and influence of nursing and nurses on the delivery of health care cannot be overstated.
Historical Background Women have provided the basic caring function in Western health care institutions since these institutions first developed in Europe during the first millennium CE. The development of the modern nursing profession is customarily dated to 1854, when the English nurse Florence Nightingale traveled to the Russian Crimea in response to a British government mandate to improve hospital care during the Crimean War. To accomplish this objective, the first task Nightingale needed to deal with was finding qualified nurses. The second was convincing the military physicians that the care she and her nurses proposed to provide would not spoil the soldiers by “coddling the brutes.”Third, Nightingale had to show that she had special skills and knowledge that, when incorporated into the management of sick and wounded soldiers, would lead to positive outcomes that could benefit the war effort. The nursing reforms she introduced eventually reduced hospital
Goldsteen74024_03_CH03_79-124_03-18-20.indd 99
3/19/20 10:53 AM
100
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
mortality from 60% to about 1%. This did not prevent repeated attempts on the part of her male military and medical superiors to undermine the program and eliminate the nurses, despite the fact that she had been sent to the Crimea by the British government. In the U.S. Army during the Spanish–American War and World War I, sick and wounded soldiers suffered unnecessarily while nurses struggled for the right to provide high-quality nursing care. It was not until 1944 that nurses in the military forces were granted temporary status as officers. Only in 1947 did Congress establish permanent Army and Navy Nurse Corps (Kalisch & Kalisch, 1978).
Definitions of Nursing Change As with physicians, the roles and responsibilities of nurses have evolved since the first days of the profession. Thus, the definition of nursing has changed as medical care changes. More than 20 years ago, nursing was defined by the American Nurses Association (ANA, 1990) as: assessment, diagnosis, planning, intervention, and evaluation of human responses to health or illness; the provision of direct nursing care to individuals to restore optimum function, or to achieve a dignified death; ... the provision of health counseling and education; the establishment of standards of practice for nursing care in all settings, including the development of nursing policies, procedures, and protocols for specific settings; ... collaboration with other independently licensed health care professionals in case finding and the clinical management and execution of interventions identified to be appropriate in a plan of care; and the administration of medication and treatments as prescribed by those persons qualified under the provision of the [law]. (p. 8) In 1995, the ANA added the concept that the “authority of the profession is based on a social contract between society and the profession” (Kovner & Salsberg, 2002, p. 73). According to the Nursing Practice Act of New York State (Article 139, Para. 6902 of the State Education Law; University of the State of New York [USNY], 1995b): The practice of the profession of nursing as a registered professional nurse is defined as diagnosing and treating human responses to actual or potential health problems through such services as case finding, health teaching, health counseling, and provision of care supportive to or restorative of life and well-being, and executing medical regimens prescribed by a licensed or otherwise legally authorized physician or dentist. A nursing regimen shall be consistent with and not vary [from] existing medical regimen. (p. 41) Furthermore, the act states (Para. 6901; USNY, 1995b): “Diagnosing” in the context of nursing practice means the identification of and discrimination between physical and psychosocial signs and symptoms essential to effective execution and management of the nursing regimen. Such diagnostic privilege is distinct from medical diagnosis. “Treating” means selection and performance of those therapeutic measures essential to the effective execution and management of the nursing regimen, and execution of any prescribed medical regimen.“Human responses” means those signs, symptoms and processes which denote the individual’s interaction with an actual or potential health problem. (p. 41)
Goldsteen74024_03_CH03_79-124_03-18-20.indd 100
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
101
According to the ANA (1995), the areas of concern include care and self-care processes; physiological and pathophysiological processes in areas ranging from rest and sleep to nutrition and sexuality; physical and emotional comfort, discomfort, and pain; emotional difficulties; decision and choice making; perceptual orientation; relationships and role performance; and social policies. Nurturing is basic to all nursing functions. Nursing is more recently defined by the ANA (2003, 2011) as follows: “Nursing is the protection, promotion, and optimization of health and abilities, prevention of illness and injury, alleviation of suffering through the diagnosis and treatment of human response, and advocacy in the care of individuals, families, communities, and populations” (ANA, 2003, pp. 25–26). This definition emphasizes the current importance of understanding the patient’s social context, promoting social justice, and advancing scholarship for the practice of nursing. Although these activities may always have been understood to be important to nursing practice, the current definition makes their importance explicit.
Nurses in Expanded Roles The scope of nurse practice has expanded since the days of Florence Nightingale. Each expansion first occurred along the route of on-the-job experience and training. Only later would such developments be formalized into an educational program. Thus, for example, the first public health nurses, who appeared during World War I; the first maternal and child health nurses, who also came on the scene in the early 1920s; the first nurse anesthetists, nurse midwives, and clinical nurse specialists; and, ultimately, nurse practitioners were all first prepared outside of any formal educational system. In each instance, the initial informal efforts to create a new arena for nursing were followed by the establishment of standards, formal curricula in approved programs, and, more recently, the preparation for advanced levels through master’s and doctoral degree programs in universities. The development of each new form of, and forum for, nursing was also accompanied by a serious struggle for acceptance, especially within the medical profession. This was especially true if the new form was or could be taken to be in economic competition with physicians. Over time, the acceptance of new roles for nurses as first demonstrated in practice has led to continuing changes in nursing practice laws across the country. For example, in welldefined primary care practice, an in-depth review of research carried out in the 1970s found no differences between the quality of care provided by qualified nurses and that provided by physicians (Record, 1981). This finding has been confirmed more recently (Mundinger et al., 2000). Properly prepared nurses in advanced practice, the nurse practitioners, can provide primary ambulatory care, normal pregnancy care and delivery, and routine anesthesia at least as well as physicians (Mundinger, 2002). In 1988, New York state, following the lead of a number of other states, formalized the nurse practitioner role in its education law, to wit (New York State Education Department, Office of the Professions, 2005): The practice of registered professional nursing by a nurse practitioner . . . may include the diagnosis of illness and physical conditions and the performance of therapeutic and corrective measures . . . in collaboration with a licensed physician . . . provided such services are performed in accordance with a written practice agreement and written practice protocols. The written practice agreement shall include explicit provisions for the resolution of any disagreement between the collaborating physician and the nurse practitioner regarding . . . diagnosis or treatment . . . within
Goldsteen74024_03_CH03_79-124_03-18-20.indd 101
3/19/20 10:53 AM
102
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
the scope of practice of both. To the extent the practice agreement does not so provide, then the collaborating physician’s diagnosis or treatment shall prevail. (para. 6902[3]) This sort of legislation opened the door for truly expanded nurse practice. It is proving to be a boon to patients, especially in such areas as primary care and chronic/multiple disease management, prevention, and early detection (Mundinger, 2002). The number of APRNs—RNs with specialized training and advanced degrees—has risen from about 30,000 in 1990 to about 140,000 in 2010 (American Academy of Nurse Practitioners [AANP], 2010). “APRN” is the title used to encompass those nurses who have master’s or doctoral degrees with specialty education and often certification that confers prescriptive authority. The growth of the APRN profession is linked to numerous factors. A major factor is the decline in the number of doctors choosing primary care as their specialty, a trend that is expected to continue. From 1998 to 2005, medical school surveys showed that the percentage of third-year residents intending to pursue careers in general internal medicine went down from 54% to 20%. Many new doctors are choosing more lucrative specialties, in part because of the debt they incur during medical school, and less time-demanding ones with more regular hours as well. The supply of family practice physicians is falling just as the baby boomer population is aging and their need for medical care is rising. APRNs in many cases can and do fill this need. APRNs can perform many of the duties of primary care doctors, such as performing physical exams; diagnosing and treating common health problems; prescribing medications (from a specified list); ordering and interpreting x-rays; providing prenatal care, family planning services, and gynecological exams; and giving immunizations. In addition, APRNs are considered to be less rushed and more holistic in their approach to patients, factors increasing patient satisfaction. Today, some states allow APRNs to practice more independently and comprehensively than others. Furthermore, a national model of licensure is afoot for nurse practitioners, whereby requirements would be more consistent and licenses more portable throughout the United States for them (NursingLicensure.org, 2019).
Nursing Education Nursing offers several levels and types of practice, each requiring different educational experiences.
Registered Nurses Most nurses are RNs. To become an RN, completion of a training program is required, followed by a licensing exam that is administered by each state. Training programs still are of three types: (a) diploma in nursing from a hospital-based two- to three-year program; (b) associate degree in nursing (ADN) from a two-year community college or similar; and (c) bachelor of science degree in nursing (BSN) from a four-year college or university. There are about 100 diploma programs at present. Compared to the BSN programs, the two-year programs leading to an ADN focus more on technical skills than theory, and today they are often used as a stepping stone to the BSN. Graduates of all three types of programs are eligible through state licensing exams to become RNs. The landmark report, The Future of Nursing, was released by the Institute of Medicine (IOM) in 2010. The report recommended that at least 80% of the nursing workforce hold a baccalaureate degree or higher by 2020, compared to 50% in 2010 (IOM, 2010). It also recommended doubling the number of nurses with a doctorate by 2020. The report emphasized the need for education:
Goldsteen74024_03_CH03_79-124_03-18-20.indd 102
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
103
This report offers recommendations that collectively serve as a blueprint to (1) ensure that nurses can practice to the full extent of their education and training, (2) improve nursing education, (3) provide opportunities for nurses to assume leadership positions and to serve as full partners in health care redesign and improvement efforts, and (4) improve data collection for workforce planning and policy making. (IOM, 2010, p. 1) Currently, there are more than 840 baccalaureate programs in the United States. The American Association of Colleges of Nursing (AACN) has reported total enrollment in 2014 in all nursing programs leading to the baccalaureate degree was 320,074, an increase from 299,118 in 2013. Within this population, 189,729 students were enrolled in entry-level baccalaureate nursing programs. In graduate programs, 113,788 students were enrolled in master’s programs, 5,290 were enrolled in research-focused doctoral programs, and 18,352 were enrolled in practice-focused doctoral programs in nursing (AACN, 2015). The IOM recommendations, it seems, are being taken seriously.
Advanced Degree Nurses There are also traditional master’s and doctoral programs for RNs. The master’s degree in nursing (MSN) is the preferred preparation for nursing leaders and managers. There are more than 330 master’s degree programs accredited by the Commission on Collegiate Nursing Education (CCNE) or the National League of Nursing Accrediting Commission (NLNAC). There is a wide variety of master’s degree programs, including the master of science degree in nursing (MSN), the master of nursing degree (MN), the master of science degree with a major in nursing (MS), and the master of arts degree with a major in nursing (MA). Advancing from the RN to the MSN usually takes about three years. “The number of RN to MSN programs has more than tripled in the past 20 years, from 70 programs in 1994 to 214 programs today. According to AACN’s 2014 survey of nursing schools, 31 new RN to MSN programs are in the planning stages” (AACN, 2015, p. 1). Proceeding from an RN to a BSN takes one to two years. There are more than 679 RN to BSN programs nationwide, including more than 400 programs that are offered at least partially online. “Enrollment in RN to BSN programs is increasing in response to calls for a more highly educated nursing workforce. From 2013 to 2014, enrollments increased by 10.6%, marking the 12th consecutive year of increases in RN to BSN programs” (AACN, 2015, p. 2). The doctoral degree in nursing is also increasingly popular, particularly for nurses who wish to teach and conduct research. The 2011 AACN survey found significant growth in research-focused doctoral programs (i.e., PhD, doctor of nursing science [DNS]), which had climbed to 125 programs by 2011. The number of schools offering the doctor of nursing practice (DNP) degree increased from 20 programs in 2006 to 184 programs in 2011, with another 101 programs in the planning stages. By 2012, enrollment in these programs grew by 28.9%, with 9,094 students now enrolled in DNP programs (AACN, 2015).
Advanced Practice Degree Nurses APRN preparation is preferred for positions with prescriptive and diagnostic responsibilities. These programs are designed and expected to advance the professional practice of nursing and meet expected workforce shortages, as well as provide better employment opportunities for individuals. Nurse anesthetists, nurse midwives, and nurse practitioners must earn a master’s degree from an accredited program. These programs are a mix of classroom and
Goldsteen74024_03_CH03_79-124_03-18-20.indd 103
3/19/20 10:53 AM
104
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
clinical experience. An APRN must be a RN before starting a program, and a BSN is preferred. Prospective nurse anesthetists must have clinical experience as a prerequisite for admission to an accredited nurse anesthetist program. Candidates typically have experience working as an RN in an acute care or critical care setting.
Nursing Practice The BLS (2016) has outlined the roles of both RNs and APRNs. They are similar, but the APRNs have more responsibility and require greater independent judgment. For example, APRNs can conduct research, while RNs typically do not. RNs do not “diagnose various health problems,” but APRNs do. Here are the two lists of functions: RNs typically do the following: • • • • • • • • • •
Assess patients’ conditions. Record patients’ medical histories and symptoms. Observe patients and record the observations. Administer patients’ medicines and treatments. Set up plans for patients’ care or contribute information to existing plans. Consult and collaborate with doctors and other health care professionals. Operate and monitor medical equipment. Help perform diagnostic tests and analyze the results. Teach patients and their families how to manage illnesses or injuries. Explain what to do at home after treatment.
APRNs typically do the following: • • • • • • • • • • • •
Take and record patients’ medical histories and symptoms. Perform physical exams and observe patients. Create patient care plans or contribute to existing plans. Perform and order diagnostic tests. Operate and monitor medical equipment. Diagnose various health problems. Analyze test results or changes in a patient’s condition, and alter treatment plans, as needed. Give patients medicines and treatments. Evaluate a patient’s response to medicines and treatments. Consult with doctors and other health care professionals, as needed. Counsel and teach patients and their families how to stay healthy or manage their illnesses or injuries. Conduct research.
Settings for Practice: RN or APRN? Commensurate with their differences in training, roles, and responsibilities, RNs and APRNs have different practice-setting patterns (see Table 3.4). Most notably, APRNs rarely work in home health or nursing facilities, while these are common settings for RNs. Also APRNs work in college, university, or professional schools, unlike RNs. The most common setting for APRNs is the physician office, and for RNs, it is the hospital.
Goldsteen74024_03_CH03_79-124_03-18-20.indd 104
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
105
TABLE 3.4 Most Common Employment Settings for RNs and APRNs, 2016 Industry
RN
Nurse Anesthetist
Nurse Practitioner
Nurse Midwife
Number of Nurses General medical and surgical hospitals
1,698,700
13,320
44,160
1,730
Offices of physicians
197,790
23,890
84,720
2,560
Home health care services
181,180
—
—
Nursing care facilities (Skilled nursing facilities)
153,120
—
—
Outpatient care centers
141,830
2,050
17,270
1,130
Offices of other health practitioners
—
1,890
5,750
420
Colleges, universities, and professional schools
—
1,220
5,390
130
APRN, advanced practice registered nurse; RN, registered nurse. SOURCE: U.S. Department of Labor, Bureau of Labor Statistics. (2016). Occupational outlook handbook. Retrieved from https://www .bls.gov/ooh/home.htm
Nursing Practice Issues Job satisfaction among nurses has often been the subject of concern. One important issue for job satisfaction and retention among nurses is hours worked. The working hours of RNs in hospitals have changed. The use of extended work shifts and overtime has escalated as hospitals cope with nurse shortages. While systematic national data on trends in the number of hours worked per day by nurses are lacking, anecdotal reports suggest that hospital staff nurses are working long hours with few breaks and often little time for recovery between shifts. Scheduled shifts may be eight, twelve, or even sixteen hours long and may not follow the traditional pattern of day, evening, and night shifts. (Rogers, Hwang, Scott, Aiken, & Dinges, 2004, p. 202) Another issue is the nurse-to-patient ratio. In 1999, California became the first —and at this point—only state to set a minimum nurse-to-patient ratio. The California hospitals and the California Healthcare Association have fought the law on the basis of cost, other performance activities, and the nursing shortage. The governor issued an emergency regulation to void the law, but the California Superior Court voided the governor’s order. To deal with the nursing shortage, hospitals have used a variety of tactics, including competitive compensation and the use of temporary staff. However, hospitals are unsure whether they can maintain or meet future needs and the increased costs associated with these tactics (May, Bazzoli, & Gerland, 2006). Today, 14 states have addressed nurse staffing in hospitals in law or with regulations: CA, CT, IL, MA, MN, NV, NJ, NY, OH, OR, RI, TX, VT, and WA (ANA, 2019). Both long working hours and high nurse-to-patient ratios are a concern from a patient safety perspective. In a 1997 outcome study covering 6 million discharges from 800 hospitals in 11 states (Needleman, Buerhaus, Mattke, Stewart, & Zelevinsky, 2002, p. 1715), the
Goldsteen74024_03_CH03_79-124_03-18-20.indd 105
3/19/20 10:53 AM
106
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
authors found that a “higher proportion of hours of nursing care provided by RNs and a greater number of hours of care by RNs per day are associated with better care for hospitalized patients.” Nurses are justifiably concerned about patient safety and their own well-being. For example, a study conducted for AFT Health care, a union, found that nurses view understaffing as a serious problem for nurse burnout and the quality of care that patients receive: Not surprisingly, nurses perceive a serious staffing shortfall. Fully three in five (61%) hospital nurses say the nurses at their hospital are responsible for too many patients, whereas only 2% believe that the nurses at their hospital could safely provide care for more patients. ... Fully four in five (82%) hospital nurses support legislation that would establish a maximum number of patients that nurses can be required to care for at one time, with 57% strongly favoring and 25% somewhat favoring such legislation. Just 13% say they are opposed. (Hart & Research Associates, 2003, pp. 3–4) Another issue is that of worker protection for nurses. In 2006, the National Labor Relations Board exempted RNs from union membership if they have certain kinds of supervisory duties. In the majority decision, the board’s three Republicans adopted a broad definition of “supervisor,”which included those who assigned others to location, shift, or significant tasks, such as a nurse overseeing a shift who might assign another nurse to a particular patient. The board’s majority ruled that workers should be considered supervisors, exempt from union membership, if they oversaw another employee and could be held accountable for that subordinate’s performance. The board’s majority also ruled that workers could be considered supervisors if supervisory duties were only 10% to 15% of their total work time. In dissenting, the board’s two Democrats said,“Today’s decision threatens to create a new class of workers under federal labor law: workers who have neither the genuine prerogatives of management, nor the statutory rights of ordinary employees” (Greenhouse, 2006). At the beginning of the new millennium, at least some members of all health care occupations have been found to be dissatisfied with their current working conditions. For example, 40% or more of hospital employees other than physicians wanted better pay, a better work environment, better benefits, and more advancement opportunities. One-third of all health care employees were disappointed both in physician leadership and in the quality of institutional management and supervision. The problems for nurses in particular, however, seemed not to be new, except that they appeared to be getting worse (Steinbrook, 2002). As Steinbrook put it,“Nursing is an embattled profession” (p. 1757).
From Nursing Shortage to Nursing Oversupply, and Back Again Like the supply of physicians, over time the supply of nurses has rarely been in tune with either the real or the perceived need. Nursing shortages have occurred periodically in the United States (Aiken, 1982). One shortage in the early 1950s led to the formalization of licensed practical nurse (LPN) training and the requirements previously mentioned. In the early 1990s, another shortage appeared to be on the horizon (Aiken & Mullinix, 1987; Secretary’s Commission on Nursing, 1988). In 1990, the U.S. Department of Health and Human Services estimated the nursing shortage to be about 200,000 (Moses, 1992). It predicted shortages of about 350,000 in the year 2000, 520,000 in 2010, and 875,000 in 2020. In 1988, the RN position vacancy rate in hospitals was over 11%. Nevertheless, nursing school enrollments were actually declining, and minority recruitment was lagging. However, one striking feature of the nursing profession is that a significant number of its members of working age were not employed in nursing. If half of the approximately 400,000 RNs not
Goldsteen74024_03_CH03_79-124_03-18-20.indd 106
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
107
working in nursing in 1990 (Moses, 1992) had been employed, there would have been no nursing shortage. In the 1980s, authorities on the subject cited many reasons to account for this employment gap (Igelhart, 1987). Among the reasons were low salaries (the average starting salary for a staff nurse in 1988 was US$25,000), limited chances for significant increases in pay over the life of a career (the average maximum salary for a head nurse in 1988 was US$45,000), poor working conditions (high-tech work creates much stress, and shift work is a serious problem), poor professional image, and greater career opportunities for women. Among steps suggested to solve the nursing shortage at that time were more creative solutions to the nights-and-weekends shifts problem, giving nurses more control over their own work, expanding nurse participation in hospital decision-making, improving continuing professional education, restructuring the work of the nurse, and developing better career ladders for nurses (Helmer & McKnight, 1989). Another key factor in the nursing shortage (especially given the fact that so many nurses of working age were not employed in nursing) was the doctor–nurse relationship and what was wrong with it from the nurses’ point of view (Stein, Watts, & Howell, 1990). As Aiken and Mullinix (1987) pointed out,“Much of the dissatisfaction of nurses with hospital practice is related to the absence of satisfying professional relationships with physicians” (p. 645). At the center of the nursing shortage, then, remained the need to change the rules of the “doctor–nurse game” (Stein et al., 1990), the source of much of the dissatisfaction noted by Aiken and Mullinix. After all, not all of those 400,000 RNs who in 1990 were not in nursing chose to leave the profession simply because they were burned out, too old, having children, wanted to stay at home, or thought some other line of work would be better. Suddenly the nurse supply situation seemed to change. There were both closures and size shrinkages of hospitals. By the mid-1990s, not only was there no longer a nursing shortage, but nurse layoffs were occurring in certain areas of the country (Rosenthal, 1996). The University of California’s Pew Center for the Health Professions (1999) predicted that 200,000 to 300,000 hospital nurse positions could be eliminated by the year 2000. Suddenly, a vast surplus appeared to be on the horizon. Regardless of what the true situation was, however, as with physician supply, no comprehensive national planning was occurring to deal with the supply, distribution, and role and function of either the existing nurse pool or the nursing education system. But then, the situation changed rapidly once again. The new nursing shortage appeared as quickly as had the apparent oversupply of the mid-1990s. Once again, the predictions of future severe nursing shortages made in the late 1980s seemed to be at least somewhat on target. In 2001, the American Hospital Association (AHA) reported that for hospitals alone there were about 126,000 RN vacancies (Parker, 2002). But this time, the shortage problem went beyond just nurses. A New York Times headline reported “Worker Shortage in Health Fields Worst in Decades” (Steinhauer, 2000). The president of the AHA (Davidson, 2001, p. 1) proclaimed: “The single greatest challenge for hospitals today and in the future is the recruitment and retention of high quality staff across many disciplines.” According to data compiled by the AHA, the reasons for these shortages echoed those of earlier times (Selvam, 2001). In 2004, the AACN documented the continued shortage of nurses in the United States at that time. For example, the number of first-time candidates for the NCLEX-RN® declined significantly from 1995 to 2003 for BSNs, ADNs, and diploma nurses. The overall decline for all categories was 96,438 to 76,618 (U.S. House of Representatives, 2005). The AACN’s concern continued: “The U.S. is projected to experience a shortage of Registered Nurses (RNs) that is expected to intensify as Baby Boomers age and the need for health care grows. Compounding the problem is the fact that nursing schools across the country are struggling to expand capacity to meet the rising demand for care given the national move toward health
Goldsteen74024_03_CH03_79-124_03-18-20.indd 107
3/19/20 10:53 AM
108
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
care reform” (AACN, 2019b, p. 1). The AACN cited numerous statistics that suggested a looming shortage. For example, According to the BLS’ Employment Projections 2012–2022 released in December 2013, Registered Nursing (RN) is listed among the top occupations in terms of job growth through 2022. The RN workforce is expected to grow from 2.71 million in 2012 to 3.24 million in 2022, an increase of 526,800 or 19%. The Bureau also projects the need for 525,000 replacement nurses in the workforce bringing the total number of job openings for nurses due to growth and replacements to 1.05 million by 2022. (AACN, 2019b, p. 1) A particularly chilling fact reflecting on the nursing shortage and its projected future was that in 2015, almost 40% of RNs were over 50 years old. The number of nurses leaving the field had been growing. In 2010, it was about 40,000. Concurrently, nursing school enrollment had begun to level off after dramatic growth since 2000 (AACN, 2019a).
PHYSICIAN ASSISTANTS The health profession of PA has developed in the United States since the Vietnam War (1965–1973). The early development of the PA profession occurred just as the war was getting under way; it received a big boost from the return of Vietnam-veteran medical corpsmen. One can only speculate whether or not the PA profession would have been more than a blip on the radar screen of the history of health services had there been no Vietnam War. Had the PA profession not developed as it did, would the profession of nurse practitioner be more prominent in the United States? But the war did occur, and whether the two are integrally related, the PA profession has become an established U.S. health services profession. By the mid-1980s, the PA profession had become a complex and multifaceted one (Schafft & Cawley, 1987). According to Schafft and Cawley (p. 6), the PA’s role involves: •
•
• •
•
Approaching a patient of any age group in any setting to elicit a detailed and accurate history, perform an appropriate physical examination, delineate problems, and record and present patient data Analyzing health status data obtained via interview, examination, and laboratory diagnostic studies and delineating health care problems in consultation with the physician Formulating, implementing, and monitoring an individualized treatment or management plan for a patient in consultation with the physician Instructing and counseling patients regarding compliance with the prescribed therapeutic regimen, normal growth and development, family planning, emotional problems of daily living, and health maintenance Performing routine procedures essential to managing simple conditions produced by infection or trauma, assisting in the management of more complex illness and injury, and initiating evaluations and therapeutic procedures in response to life-threatening situations
By the mid-1990s, it was estimated that PAs could perform 80% of the primary functions of a primary care physician practice and would be widely accepted by patients (American Academy of Physician Assistants [AAPA], 1996). From its beginnings, the PA profession was conceived as an extension of the profession of medicine. Unlike nursing, it was not meant to be another, separate profession. In each
Goldsteen74024_03_CH03_79-124_03-18-20.indd 108
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
109
state, PA licensure is provided for under the medical practice act rather than under a separate law, as is the case with nursing. Although the gender balance within the PA profession has changed over the years to approximately 72% women (BLS, 2019f), in the beginning it was predominantly male. For these reasons, many of the power issues that have sometimes clouded the relationship between physicians and nurses have not appeared. This status is reflected in the AAPA (2006) definition of a PA: Physician assistants are health care professionals licensed to practice medicine with physician supervision. ... As part of their comprehensive responsibilities, PAs conduct physical exams, diagnose and treat illnesses, order and interpret tests, counsel on preventive health care, assist in surgery, and in virtually all states can write prescriptions. Within the physician–PA relationship, physician assistants exercise autonomy in medical decision making and provide a broad range of diagnostic and therapeutic services. A PA’s practice may also include education, research, and administrative services. (p. 1) In 2019, there were more than 250 accredited PA training programs. Most of them were offered through medical schools, teaching hospitals, or schools of the allied health professions in four-year colleges. PA programs have been accredited by the Accreditation Review Commission on Education for the Physician Assistant since 2001 (ARC-PA, 2020). Some PAs work for individual physicians, but most are employed in hospitals, clinics, group practices, and other organized health care settings. As noted earlier, like nurse practitioners, for the same kinds of patients, PAs provide care that is comparable in quality to that provided by physicians.
OTHER HEALTH CARE OCCUPATIONS There are many other categories of health worker. In mental health centers, for example, the staff includes psychologists, psychiatric social workers, nurses, and other support staff, in addition to psychiatrists. Community outreach workers are a new type of health care worker, trained in recent years by certain ambulatory care programs, both general and mental. In local health department centers, public health nurses are the mainstay of the clinics that focus on preventive services. These nurses work with part-time physicians who are otherwise mainly in private practice. Other personnel in public health clinics include health educators, nutritionists and dietitians, and sexually transmitted disease investigators. Besides the personnel staffing the clinics, public health agencies employ sanitarians, statisticians, community health educators with specialized skills, and family planning counselors. In sum, the health personnel picture in the United States is complex. On the technical side, it is highly developed, and many patients greatly benefit from the availability of so many different health care personnel with so much detailed education, training, and experience. There are gaps and overlaps, however, and maldistribution by geographic area and differing levels of patient access to care are significant problems.
PRIMARY CARE AND ITS PROVIDERS Much of the health care workforce provides primary care. Members of all health care occupations participate in primary care, including physicians, nurses, PAs, and so forth. In this section, we discuss primary care—what it is, its purpose, and its role in health care delivery in the United States.
Goldsteen74024_03_CH03_79-124_03-18-20.indd 109
3/19/20 10:53 AM
110
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Primary care and ambulatory care go together like apple pie and ice cream. This is so even though not all primary care is delivered in an ambulatory setting, nor is all ambulatory care primary care. Nevertheless, because they are in most instances closely associated, they will be covered in the same chapter. As noted in Chapter 1, Introduction, by sheer volume, primary health care services are predominant in the health care delivery system, but primary care has proved challenging to define precisely. Over the years, many definitions have been offered. One such normative definition is the following (Jonas, 1973): Primary care is medical attention to the great majority of ills. It should be provided continuously over a significant period of time by the same appropriately trained individual (or team) who is sympathetic, understanding, knowledgeable and equipped, who is as capable of keeping people well as he is of returning them to health when they fall ill. (p. 177) Unfortunately, to this day, the coordination of preventive and curative services occurs less often than it should in much of American medical practice (McGinnis, Williams-Russo, & Knickman, 2002; Stange, Woolf, & Gjeltma, 2002). In 1977, the IOM reviewed 33 different definitions of the term “primary care” (Ruby, 1977). Its summary definition from 1978, both normative and descriptive, was the following (Eisenberg, 1997): [Primary care is] the provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health needs, developing a sustained partnership with patients, and practicing in the context of family and community. (p. 615) Barbara Starfield (1996) provided one normative definition, covering both what primary care is and, in the best of all possible worlds, what it ought to be: Primary care is the means by which the two goals of a health services system— optimization of health and equity in distributing resources—are balanced. It is the basic level of care provided equally to everyone. It addresses the most common problems in the community by providing preventive, curative, and rehabilitative services to maximize health and well-being. It integrates care when more than one health problem exists, and deals with the context in which illness exists and influences people’s responses to their health problems. It is care that organizes and rationalizes the deployment of all resources, basic as well as specialized, directed at promoting, maintaining, and improving health. (p. 1365) In 1997, Eric Cassell, expressing a career-long concern for the personal and interpersonal aspects of medical practice, addressed a different kind of “balance” in offering his own “ought to be” definition of primary care (Geiger, 1997): [Primary care is] careful history taking ... artfully enhanced by skillful questioning at every point in the illness ... supplemented by discerning scrutiny of patients’ presentation to the world, behavior, mood and feelings, environment and context ... plus the physical examination, supplemented by the mediated investigations offered by modern tests and imaging. (p. 1637) For achieving the best in primary care (and, indeed, for all of medicine), as White (1968), anticipating Cassell, so splendidly put it:
Goldsteen74024_03_CH03_79-124_03-18-20.indd 110
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
111
One wants to avoid the confusion inherent in the encounter between the patient who implicitly says to the doctor,“I hope you treat what I’ve got” and the physician who implicitly says to the patient,“I hope you’ve got what I treat.” (p. 362) According to many authorities, the ideal primary care environment is one that provides classic “comprehensive care” (Reader & Soave, 1976). In terms that still apply, Knowles (1965) defined the latter at a conference held in 1964: Comprehensive medicine in this [ambulatory care] context means the coordination of all the various caring elements in the community with those of the medical profession by a team of individuals representing all disciplines, with all the techniques and resources available to the physician and his patient. The aim of these individuals would be to provide total care—somatic, psychic, and social—to those in need, and to study and research the expanding social and economic problems of medical care with the intent of improving the organization and provision of health services. (p. 73) The concept of community-oriented primary care (COPC) was developed back in the 1980s (Madison, 1983; Mullan, 1982; Mullan & Conner, 1982; Nutting, Wood, & Conner, 1985). It grew out of the concept of comprehensive care as defined by Knowles (1965). According to Rhyne, Cashman, and Kantrowitz (1998): COPC is a process by which a defined population’s health problems are systematically identified and addressed. Ideally, it combines principles of primary care, epidemiology, and public health. ... [It] could [also] be called community-responsive health care, community-based primary care, or something else. The process is the important element. The community is a partner at every step. (p. 2) These are all ideal or, at least in part, normative definitions of primary and comprehensive care. In functional terms, however, primary care is that care which most people need, and use, most of the time, for most of their health and illness concerns.
Functions The primary feature of “comprehensive” primary care is its integrating role in medical practice. In the past, when nearly all medical services were rendered by a family’s general practitioner, coordination was almost automatic. Today, a primary care doctor or team can still provide most of the care that is necessary most of the time. But in the context of modern medical knowledge and technology, organization and planning for such a practice must be undertaken. Medical complications or new problems at times will require the expertise of others. Coordination of care can be ensured if the primary provider assesses the situation correctly, helps the patient with a proper referral, then integrates the outcome of the referral into the patient’s ongoing care (Bodenheimer, Lo, & Casalino, 1999). This important function of the primary provider prevents fragmentation of care and the hit-or-miss nature of patient self-referral to specialists and promotes comprehensive care, for the patient as a whole person, not merely a set of parts. The term “gatekeeper” was originally applied to this function by Somers (1983). In the still-applicable sense that Somers used the term, the “gatekeeper” function of the primary care practitioner can only benefit the patient. In the managed care era, however,“gatekeeper” has taken on a different meaning in describing the main function of the primary care physician: to monitor, regulate, and control the use of medical and related services by managed care organizations’ (MCOs) patients. Thus, a fiscal responsibility has now been added to the
Goldsteen74024_03_CH03_79-124_03-18-20.indd 111
3/19/20 10:53 AM
112
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
task list of the primary care physician (Alexander, Hall, & Lantos, 2006; Shortell, Waters, Clarke, & Budetti, 1998). In this version, the gatekeeper function as carried out may not always be to the patient’s benefit. Under managed care, primary responsibilities that the physician may have to the payer for the patient’s care may on occasion conflict with the responsibility the physician has for the care of the patient. In some MCOs, for example, physicians receive monetary bonuses for holding down utilization of services by their patients (Alexander et al., 2006). As Bodenheimer et al. (1999) noted: Primary care gatekeeping [in MCO terms], in which the goal of the primary care physician (PCP) is to reduce patient referrals to specialists and thereby reduce costs, is not an adequate system in which to practice medicine. However, returning to the pre–managed care model of uncoordinated open access to specialists is a poor solution. The primary care model should be retained, but PCPs should be transformed from gatekeepers into coordinators of care, in which the goal of the PCP is to integrate both primary and specialty care to improve quality. (p. 2045) In contrast to the situation in many other countries, the primary care relationship in the United States traditionally has not ended at the hospital admitting office. Instead, primary care physicians have provided a good deal of the inpatient care. Most board-certified family practitioners, general internists, and general pediatricians in this country have hospital admitting privileges. In most other industrialized nations, primary care physicians work only in ambulatory care offices and health centers. Specialists provide inpatient and hospital clinic care. However, with the growth of managed care in the United States, the development of the hospitalist model is occurring. It remains to be seen how far this development will go.
Historical Background Thinking about primary care in conceptual terms has hardly been confined to recent decades (Roemer, 1975, 1981; Roemer, Kramer, & Frink, 1975). Nor has its implementation been without its early champions in the United States. As far back as the 1930s, primary care received a strong endorsement from the Committee on the Costs of Medical Care and, in the intervening years, from many other authorities (Somers, 1983). In the United Kingdom, the concept goes back at least as far as the 1920 Dawson report on the structure of health services (Sidel & Sidel, 1983). Despite these recommendations, in the United States, as physician specialization and subspecialization increased dramatically in the period following World War II, much of the ambulatory care provided in private offices and groups and in hospital outpatient departments became highly fragmented (Freymann, 1974). The need to restore continuity and coordination was recognized in the 1960s and led to a revitalization of the primary care concept (IOM, 1978). Many of the health services entities called “neighborhood health centers” that developed in the 1960s and 1970s fostered the primary care approach, as did many of the original health maintenance organizations (HMOs) developed in the 1970s and 1980s. Nevertheless, in the 1990s, it was still the case that most people in the United States did not have access to comprehensive primary care, even with (or perhaps because of) the advent of for-profit managed care (Starfield, 1996). There is no reason to believe that this situation has changed for the better in the 21st century. For instance, a report on primary care access in Texas deems the situation a crisis (Nelson, Banning, Kroll & Bailey, 2006).
Goldsteen74024_03_CH03_79-124_03-18-20.indd 112
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
113
Primary Care Workforce In the ideal primary care setting, an appropriately trained health professional or team provides most of the preventive and curative care for an individual or family over a significant period of time. In the late 1960s, a task list for the ideal primary care system and primary care provider was developed, one that is still valid (Committee on Medical Schools, 1968, p. 753): • • • • • • •
Assessment of total patient needs before these are categorized by specialty Elaboration of a plan for meeting those needs in the order of their importance Determination of who shall meet the defined needs—physicians (generalist or specialist), nonphysician members of the health care team, or social agencies Follow-up to see that needs are met Provision of such care in a continuous, coordinated, and comprehensive manner Attention at each step to the personal, social, and family dimensions of the patient’s problem Provision of health maintenance and disease prevention at the same level of importance as the provision of cure and rehabilitation
This description of functions shows that primary care is not simply a collection of services. Above all it is a state of mind, to wit (Committee on Medical Schools, 1968): The primary-care physician must be capable of establishing a profile of the total needs of the patient and his family. This evaluation should include social, economic, and psychological details as well as the more strictly“medical”aspects. He [sic] must know what resources are available for meeting those needs. He should then define a plan of care, deciding which parts are to be carried out by himself and which by others. The plan should have a long-range dimension. It should be understandable to the patient and his family, and it should include a follow-up on whether indicated measures have been undertaken and whether they have been effective. (p. 74) Today, both the task list and state-of-mind requirements apply as well to primary care nurse practitioners and PAs as to primary care physicians. Among physicians, primary care is provided variously by family practitioners (prepared to deliver primary care services to entire families), general pediatricians, specialists in general internal medicine, and for many women of childbearing age, obstetrician-gynecologists. As noted previously, it has now been shown that nurse practitioners/advanced practice nurses (Mundinger, 2002) and PAs can provide primary care for most patients that is at least equal in quality to that provided by physicians. It is thus likely that the debate over who should be doing what to whom in primary care will continue for many years to come.
Primary Care and the Health Care Delivery System Some observers believe that the level and quality of primary care provision serve as good markers for the quality of a nation’s health care delivery system as a whole (Davis, Schoenbaum, & Audet, 2005). Concerning the variation in primary care quality among nations, Starfield (1996) has noted: First, countries with better primary care tend to be countries that strive toward equity in distribution of health services and toward more equitable income distributions. Apparently, a commitment to social equity goes along with a commitment to
Goldsteen74024_03_CH03_79-124_03-18-20.indd 113
3/19/20 10:53 AM
114
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
equity in the distribution of health care resources. Second, it is not the number of primary care physicians, or even the ratio of primary care physicians to specialists, that accounts for the differential effects of the health services across those countries. Rather, the differences are a result of how the resources are distributed, whether or not they are organized to achieve the functions of primary care, and whether they clearly specify the roles and interrelationships between primary care and specialist physicians. (p. 1365) As stated at the outset of this section, primary care goes with ambulatory care as ice cream goes with apple pie (neither of which is unhealthy if eaten only occasionally). Historically, there is movement in the right direction. Much remains to be done.
SUMMARY The health care workforce is large, complex, and in the case of most health workers, well educated and well paid. Health care occupations account for a large portion of employed persons in the United States. In 2018, about 13 million people, or 8.5% of all civilians employed in nonagricultural occupations in the United States, were providing health care services. This was up from 11.1 million people, or 8.1% of all employed persons, working in health care in 2010, and up from about 9 million, or 6.8%, in 2002. There are over 100 health care occupations, and the single largest is RNs with over 2.9 million persons. The health occupations are expected to continue to be leading sources of jobs for Americans in the coming years because of projected growth in health care, as the population ages. Many of these jobs are well-paying and most offer health benefits. The professionals who work in the health care sector should continue to be highly valued by the society at large, and by the persons who directly receive their services.
DATA SOURCES Most of the following websites do not have interactive data. However, each is a source of information—through reports and other documents—about health care professions, including their numbers, licensure, wages, duties, education, practice settings, and trends in these.
All Health Care Occupations •
U.S. Department of Labor, Bureau of Labor Statistics The BLS is the definitive source of information about the U.S. health care workforce. Through its OES survey, a semiannual survey of approximately 200,000 nonfarm business establishments, the BLS produces employment and wage estimates annually for over 800 occupations. These estimates are available for the nation as a whole, for individual states, and for metropolitan and nonmetropolitan areas; national occupational estimates for specific industries are also available. Start here: www.bls.gov/oes/home.htm The Occupational Outlook Handbook contains information on health care occupations including number of employees, salaries, job roles, practice settings, education required, job outlook, and other occupation-related information. Start here: www .bls.gov/ooh/home.htm
Goldsteen74024_03_CH03_79-124_03-18-20.indd 114
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
115
Medicine •
Association of American Medical Colleges The AAMC serves as the academic home for medical educators. The AAMC offers a range of resources, initiatives, and learning opportunities to support the medical education community. It provides reports on medical school applicants, matriculants, enrollees, and graduates based on its surveys. Start here: www.aamc.org/data
•
Liaison Committee on Medical Education The LCME accredits medical education programs leading to the MD degree in the United States and Canada. U.S. graduates of LCME-accredited programs are eligible for residency programs accredited by the ACGME and are eligible to take the United States Medical Licensing Examination (USMLE). Start here: http://lcme.org
•
Accreditation Council for Graduate Medical Education The ACGME is an independent, not-for-profit, physician-led organization that sets and monitors the professional educational standards for residency programs. Public data available on the ACGME website are related to residency programs and students. Start here: https://apps.acgme.org/ads/public
•
American Osteopathic Association The AOA serves as the professional organization for osteopathic physicians and medical students in the United States. The AOA is the primary certifying body for DOs and the accrediting agency for all osteopathic medical schools. Start here: https://osteopathic.org/about
Nursing •
American Nurses Association The ANA Enterprise is the family of organizations that is composed of the American Nurses Association, American Nurses Credentialing Center, and American Nurses Foundation. The three organizations work to advance nursing values. An annual report presents current information about the nursing profession. Start here: www .nursingworld.org/ana/about-ana/annual-reports
•
American Association of Colleges of Nursing The AACN is the primary organization advancing nursing education, research, and practice. It produces reports on enrollment, graduation, demographics, and other characteristics of nursing students and faculty. Start here: www.aacnnursing.org/ News-Information/Research-Data
STUDY QUESTIONS 1. Which are the largest health professions? Which are the smallest health professions? 2. Which health occupations require the most education? Which require the least education?
Goldsteen74024_03_CH03_79-124_03-18-20.indd 115
3/19/20 10:53 AM
116
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
3. Which health professions have the highest wages? Which have the lowest? 4. Is required educational attainment associated with wages? If so, how? 5. How are the demographics of the health care workforce changing? 6. What are the most common practice settings for health care professionals? 7. What is primary care? What is its significance? 8. What health care occupations are included in the primary care workforce?
NOTES 1. A particularly detailed history of the development of specialization in American medical practice is presented by Rosemary Stevens in her still-relevant history, American Medicine and the Public Interest (New Haven, CT: Yale University Press, 1971). 2. For more discussion on nursing, see Kovner and Salsberg (2002) and the Springer series Advanced Practice Nursing.
REFERENCES Accreditation Council for Graduate Medical Education. (2015). 2013–2014 annual report. Retrieved from http://www.acgme.org/acgmeweb/Portals/0/PDFs/2013-14ACGME _AnnRep.pdf Accreditation Council for Graduate Medical Education. (2017). Data resource book, academic year 2016-2017. Retrieved from https://www.acgme.org/About-Us/Publications-and -Resources/Graduate-Medical-Education-Data-Resource-Book Accreditation Review Commission on Education for the Physician Assistant. (2020). About. Retrieved from http://www.arc-pa.org/about/ Aiken, L. H. (Ed.). (1982). Nursing in the 1980’s: Crises, opportunities, challenges. Philadelphia, PA: Lippincott. Aiken, L. H., & Mullinix, C. F. (1987). The nurse shortage. Myth or reality? New England Journal of Medicine, 317(10), 645. doi:10.1056/NEJM198709033171030 Alexander, G. C., Hall, M. A., & Lantos, J. D. (2006). Rethinking professional ethics in the cost-sharing era. American Journal of Bioethics, 6(4), W17–W22. doi:10.1080 /15265160600755813 American Academy of Family Physicians. (2019). Primary care. Retrieved from https://www .aafp.org/about/policies/all/primary-care.html American Association of Colleges of Nursing. (2019a). Fact sheet: Degree completion programs for registered nurses: RN to Master’s degree and RN to baccalaureate programs. Retrieved from https://www.aacnnursing.org/News-Information/Fact-Sheets/Degree -Completion-Programs American Association of Colleges of Nursing. (2019b). shortage fact sheet. Retrieved from https://www.aacnnursing.org/news-information/fact-sheets/nursing-shortage American Association of Nurse Practitioners. (2010). Frequently asked questions. Retrieved from www.aanp.org/AANPCMS2/ResearchEducation/EducationPageOne/Continuing+Edu cation/CEFAQ.htm
Goldsteen74024_03_CH03_79-124_03-18-20.indd 116
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
117
American Association of Nurse Practitioners. (2019). NP fact sheet. Retrieved from https:// www.aanp.org/about/all-about-nps/np-fact-sheet American Academy of Physician Assistants. (1996). Information on the physician assistant profession. Alexandria, VA: Author. American Academy of Physician Assistants. (2006). Information about PAs and the PA profession. Retrieved from www.aapa.org/the_pa_profession/what_is_a_pa.aspx American Academy of Physician Assistants. (2011). Quick facts. Retrieved from www.aapa .org/the_pa_profession/quick_facts.aspx American Association of Colleges of Nursing. (2015). New AACN data show an enrollment surge in baccalaureate and graduate programs amid calls for more highly educated nurses. Retrieved from http://www.tmcnet.com/usubmit/2012/03/22/6207435.htm Association of American Medical Colleges. (2006a). Data warehouse: Table 6: Applicants, accepted applicants, and matriculants by sex, 1995–2006. Retrieved from www.aamc.org/ data/facts Association of American Medical Colleges. (2006b). Data warehouse: Table 8: Hispanic ethnicity and non-Hispanic race by acceptance status, 2004–2006. Association of American Medical Colleges. (2016). The state of women in academic medicine: The pipeline and pathways to leadership, 2015–2016. Retrieved from https://www.aamc .org/data-reports/faculty-institutions/data/state-women-academic-medicine-pipeline -and-pathways-leadership-2015-2016 Association of American Medical Colleges. (2017, December 18). More women than men enrolled in U.S. medical schools in 2017. AAMC News. Retrieved from https://news.aamc .org/press-releases/article/applicant-enrollment-2017/ Association of American Medical Colleges. (2019a). Results of the 2018 medical school enrollment survey, July 2019. Retrieved from https://www.aamc.org/data-reports/students-residents/ interactive-data/2019-facts-enrollment-graduates-and-md-phd-data Association of American Medical Colleges. (2019b). The complexities of physician supply and demand, 2017–2032: 2019 update. Retrieved from https://www.aamc.org/data/workforce/ Association of American Medical Colleges. (2019c). Table A-8: Applicants to U.S. medical schools by selected combinations of race/ethnicity and sex, 2016–2017 through 2019–2020. Retrieved from https://www.aamc.org/data-reports/students-residents/ interactive-data/2019-facts-applicants-and-matriculants-data American Medical Association. (2019). AMA principles of medical ethics. Retrieved from https:// www.ama-assn.org/about/publications-newsletters/ama-principles-medical-ethics American Nurses Association. (1990). Suggested state legislation: Nursing practice act, nursing disciplinary diversion act, prescriptive authority act. Kansas City, MO: Author. American Nurses Association. (1995). Nursing’s social policy statement. Kansas City, MO: Author. American Nurses Association. (2003). Nursing’s social policy statement (2nd ed.). Silver Spring, MD: Nursebooks.org. American Nurses Association. (2011). What is nursing? Retrieved from www.nursingworld .org/EspeciallyForYou/What-is-Nursing American Nurses Association. (2019). Nurse staffing. Retrieved from https://www.nursing world.org/practice-policy/advocacy/state/nurse-staffing/
Goldsteen74024_03_CH03_79-124_03-18-20.indd 117
3/19/20 10:53 AM
118
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
American Osteopathic Association. (2019). Osteopathic medical schools. Retrieved from https://osteopathic.org/about/affiliated-organizations/osteopathic-medical-schools/ Barzansky, B., & Etzel, S. I. (2005). Educational programs in U.S. medical schools, 2004– 2005. Journal of the American Medical Association, 294(9), 1068–1074. doi:10.1001/ jama.294.9.1068 Bodenheimer, T., Lo, B., & Casalino, L. (1999). Primary care physicians should be coordinators, not gatekeepers. Journal of the American Medical Association, 281(21), 2045–2049. doi:10.1001/jama.281.21.2045 Bureau of Health Workforce, Health Resources & Services Administration. (2008). The physician workforce: Projections and research into current issues affecting supply and demand. Retrieved from https://bhw.hrsa.gov/health-workforce-analysis/research/projections Center for the Health Professions. (1999). Primary care tries to find its footing in the new century. Front and Center, 3(6), 1. Retrieved from https://healthforce.UCSF.edu Colwill, J. M. (1986). Education of the primary physician: A time for reconsideration? Journal of the American Medical Association, 255(19), 2643–2644. doi:10.1001/jama.255.19.2643 Committee on Medical Schools of the Association of American Medical Colleges in Relation to Training for Family Practice. (1968). Planning for comprehensive and continuing care of patients through education. Journal of Medical Education, 43(6), 751–759. doi:10.1097/00001888-196806000-00011 Cooper, R. A. (1995). Perspectives on the physician workforce to the year 2020. Journal of the American Medical Association, 274(19), 1534–1543. doi:10.1001/jama.1995 .03530190048033 Cooper, R. A., Getzen, T. E., McKee, H. J., & Laud, P. (2002). Economic and demographic trends signal an impending physician shortage. Health Affairs, 21(1), 140. doi:10.1377/ hlthaff.21.1.140 Davidson, D. (2001, August 6). A message. AHA News (Suppl.), p. 1. Davis, K., Schoenbaum, S. C., & Audet, A. M. (2005). A 2020 vision of patient-centered primary care. Journal of General Internal Medicine, 20(10), 953–957. doi:10.1111/ j.1525-1497.2005.0178.x Donabedian, A., Axelrod, S. A., & Wyszewianski, L. (1980). Medical care chartbook (7th ed.). Ann Arbor, MI: AUPHA Press. Edelman, N. E., & Romeiser, J. (2010, October). Financing of graduate medical education. In M. E. Johns (Chair), Ensuring an effective physician workforce for America. Proceedings Association of Academic Health Centers, Atlanta, GA. Eisenberg, J. (1997). Primary care—America’s health in a new era [Book review]. New England Journal of Medicine, 336(22), 1615. doi:10.1056/NEJM199705293362221 Eisenberg, J. M. (1986). Doctors’ decisions and the cost of medical care. Ann Arbor, MI: Health Administration Press. Fordham, C. C. (1980). The Bane report revisited. Journal of the American Medical Association, 244(4), 354–357. doi:10.1001/jama.1980.03310040036023 Freymann, J. G. (1974). The American health care system: Its genesis and trajectory. New York, NY: Medcom.
Goldsteen74024_03_CH03_79-124_03-18-20.indd 118
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
119
Geiger, H. J. (1997). Doctoring: The nature of primary care medicine [Book review]. New England Journal of Medicine, 337(22), 1637. doi:10.1056/NEJM199711273372221 Geyman, J. P. (1986).Training primary care physicians for the 21st century. Journal of the American Medical Association, 255(19), 2631–2635. doi:10.1001/jama.1986.03370190115035 Greenhouse, S. (2006, October 4). Board redefines rules for union exemption. The New York Times. Retrieved from www.nytimes.com/2006/10/04/washington/04labor.html? pagewanted=all Hart, P. D., & Research Associates. (2003). Patient-to-nurse staffing ratios: Perspectives from hospital nurses. Washington, DC: AFT Healthcare. Haugh, R. (2002, January). Finance: Patience required. Hospitals and Health Networks, p. 18. Helmer, F. T., & McKnight, P. (1989). Management strategies to minimize nursing turnover. Health Care Management Review, 14(1), 73. doi:10.1097/00004010-198924000-00009 Henry, T. A. (2019, May 10). Employed physicians now exceed those who own their practices. AMA Research. Retrieved from https://www.ama-assn.org/about/research/ employed-physicians-now-exceed-those-who-own-their-practices Igelhart, J. K. (1987). Problems facing the nursing profession. New England Journal of Medicine, 317(10), 646. doi:10.1056/NEJM198709033171031 Indeed. (2019). Nursing salary guide. Retrieved from https://nursesalaryguide.net/registered -nurse-rn-salary/ Institute of Medicine. (1978). A manpower policy for primary health care. Washington, DC: National Academy of Sciences. Institute of Medicine. (2010). The future of nursing: Leading change, advancing health. Washington, DC: National Academies Press. Jonas, S. (1973). Some thoughts on primary care: Problems in implementation. International Journal of Health Services, 3(2), 177. doi:10.2190/JPKP-X80P-7H03-NTQ3 Jonas, S. (1981). Sounding boards. State approval of foreign medical schools: Ensuring the quality of the training of the students and graduates from foreign medical schools entering New York State. New England Journal of Medicine, 305(1), 45. doi:10.1056/ NEJM198107023050109 Jonas, S. (1984). The historical and theoretical basis for the New York State Board of Regents’ policy concerning U.S. foreign medical graduates. New York State Journal of Medicine, 84(7), 345–347. Jonas, S. (1986). Health manpower. In S. Jonas (Ed.), Health care delivery in the United States (3rd ed., pp. 54–89). New York, NY: Springer Publishing Company. Kalisch, P. A., & Kalisch, B. J. (1978). The advance of American nursing. Boston, MA: Little, Brown. Knowles, J. H. (1965). The role of the hospital: The ambulatory clinic. Bulletin of the New York Academy of Medicine, 41(2), 68–79. Retrieved from https://www.ncbi.nlm.nih.gov/ pubmed/14230869 Kovner, C. T., & Salsberg, E. S. (2002). The health care workforce. In A. R. Kovner & S. Jonas (Eds.), Jonas and Kovner’s health care delivery in the United States (7th ed., pp. 68–106). New York, NY: Springer Publishing Company.
Goldsteen74024_03_CH03_79-124_03-18-20.indd 119
3/19/20 10:53 AM
120
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Krakower, J. Y., Ganem, J. L., & Jolly, P. (1996). Review of U.S. medical school finances, 1994–1995. Journal of the American Medical Association, 276(9), 720–724. doi:10.1001/ jama.276.9.720 Liaison Committee on Medical Education. (2019). Medical school directory. Retrieved from http://www.lcme.org/directory/ Limentani, A. E. (1998). An ethical code for everybody in health care. British Medical Journal, 316(7142), 1458. doi:10.1136/bmj.316.7142.1458a Madison, D. L. (1983). The case for community-oriented primary care. Journal of the American Medical Association, 249, 1279–1282. doi:10.1001/jama.1983.03330340021024 May, J. H., Bazzoli, G. J., & Gerland, A. M. (2006). Hospitals’ responses to nurse staffing shortages. Health Affairs, 25, w316–w323. doi:10.1377/hlthaff.25.w316 McGinnis, J. M., Williams-Russo, P., & Knickman, J. R. (2002, March–April). The case for more active policy attention to health promotion. Health Affairs, 21(2), 78–93. doi:10.1377/ hlthaff.21.2.78 Merritt Hawkins Team. (2017, September 22). Survey of America’s physicians: Practice patterns and perspectives. Retrieved from https://www.merritthawkins.com/news-and -insights/thought-leadership/survey/survey-of-americas-physicians-practice-patterns -and-perspectives/ Monahan, T. J. (2001). New York State evaluation of foreign medical schools: An update. Journal of Medical Licensure and Discipline, 87(4), 154–156. Retrieved from jmr-archives .fsmb.org/archives/archive-2000s/ Moses, E. B. (1992). The registered nurse population: Findings from the national sample survey of registered nurses. Rockville, MD: U.S. Department of Health & Human Services, Bureau of Health Professions, Division of Nursing. Mullan, F. (1982). Sounding board: Community-oriented primary care: An agenda for the 80’s. New England Journal of Medicine, 307(17), 1076–1078. doi:10.1056/ NEJM198210213071710 Mullan, F. (1995). Beware of medical quick fixes. Public Health Reports, 110(6), 668–673. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1381803/ Mullan, F. (2002). Perspective: Some thoughts on the white-follows-green law. Health Affairs, 21(1), 158–159. doi:10.1377/hlthaff.21.1.158 Mullan, F., & Conner, E. (Eds.). (1982). Community-oriented primary care—Conference proceedings. Washington, DC: National Academies Press. Mundinger, M. O. (2002). Perspective: Through a different looking glass. Health Affairs, 21(1), 162–164. doi:10.1377/hlthaff.21.1.163 Mundinger, M. O., Kane, R. L., Lenz, E. L., Totten, A. M., Tsai, W.Y., Cleary, P. D., & Shelanski, M. L. (2000). Primary care outcomes in patients treated by nurse practitioners or physicians: A randomized trial. Journal of the American Medical Association, 283(1), 59–68. doi:10.1001/jama.283.1.59 National Center for Health Statistics. (2002). National ambulatory medical care survey: 2000 summary. Advanced Data From Vital and Health Statistics. Retrieved from http://www .cdc.gov/nchs/data/ad/ad328.pdf National Center for Health Statistics. (2015a). Health, United States, 2014: With special feature on adults aged 55–64. Hyattsville, MD: U.S. Department of Health and Human Services. Retrieved from http://www.cdc.gov/nchs/data/hus/hus14.pdf
Goldsteen74024_03_CH03_79-124_03-18-20.indd 120
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
121
National Center for Health Statistics. (2015b). National ambulatory medical care survey: 2010 summary tables. Retrieved from http://www.cdc.gov/nchs/data/ahcd/namcs_sum mary/2010_namcs_web_tables.pdf Needleman, J., Buerhaus, P., Mattke, S., Stewart, M., & Zelevinsky, K. (2002). Nurse-staffing levels and the quality of care in hospitals. New England Journal of Medicine, 346(22), 1715. doi:10.1056/NEJMsa012247 Nelson, J., McCann, K., Banning, T., Kroll, C., & Romero, M. (2008). The Primary solution: Mending Texas’ fractured health care system. Retrieved from https://www.tafp.org/news/ tfp/fall-2008/cover New York State Education Department, Office of the Professions. (2005). Education law (Article 139, nursing). Retrieved from www.op.nysed.gov/prof/nurse/article139.htm NursingLicensure.org. (2019). Nurse practitioner license requirements: Change is in the air. Retrieved from https://www.nursinglicensure.org/articles/nurse-practitioner-license.html Nutting, P. A., Wood, M., & Conner, E. M. (1985). Community-oriented primary care in the United States. Journal of the American Medical Association, 253(12), 1763–1766. doi:10.1001/jama.1985.03350360089025 NYSED.gov. (2019). License requirements: Physician. Retrieved from http://www.op.nysed .gov/prof/med/medlic.htm Parker, C. (2002, October 1). Nursing shortage, working conditions, intertwined at Congressional hearing. AHA News, p. 1. The Physicians Foundation. (2019). Our history. Retrieved from https://physiciansfounda tion.org/about/our-history/ Reader, G. G., & Soave, R. (1976, Fall). Comprehensive care revisited. Milbank Memorial Fund Quarterly: Health and Society, p. 391. Record, J. C. (1981). Staffing primary care in 1990: Physician replacement and cost savings. New York, NY: Springer Publishing Company. Rhyne, R., Cashman, S., & Kantrowitz, M. (1998). An introduction to community-oriented primary care. In R. Rhyne, R. Bogue, G. Kukulka, & H. Fulmer (Eds.), Communityoriented primary care: Health care for the 21st century (pp. 2–31). Washington, DC: American Public Health Association. Roemer, M. I. (1975, March 1). From poor beginnings, the growth of primary care. Hospitals, p. 38. Roemer, M. I. (1981). Ambulatory health services in America. Gaithersburg, MD: Aspen Systems. Roemer, R., Kramer, C., & Frink, J. E. (1975). Planning urban health services: From jungle to system. New York, NY: Springer Publishing Company. Rogers, A. E., Hwang, W. T., Scott, L. D., Aiken, L. H., & Dinges, D. F. (2004). The working hours of hospital staff nurses and patient safety. Health Affairs, 23(4), 202–212. Rosenthal, E. (1996, August 19). Once in big demand, nurses are targets for hospital cuts. The New York Times, A16. Royster, S. (2015, July). Hospitalist. Career Outlook—U.S. Bureau of Labor Statistics. Retrieved from https://www.bls.gov/careeroutlook/2015/youre-a-what/hospitalist.htm Ruby, G. (1977). Definitions of primary care [Staff paper]. Washington, DC: Institute of Medicine. Schafft, G. E., & Cawley, J. F. (1987). The physician assistant. Rockville, MD: Aspen.
Goldsteen74024_03_CH03_79-124_03-18-20.indd 121
3/19/20 10:53 AM
122
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Secretary’s Commission on Nursing. (1988). Final report. Washington, DC: U.S. Department of Health and Human Services. Selvam, A. (2001, April). The state of the health care workforce. Hospitals and Health Networks, 75(4), 40. Shortell, S. M., Waters, T. M., Clarke, K. W. B., & Budetti, P. P. (1998). Physicians as double agents. Journal of the American Medical Association, 280(12), 1102–1108. doi:10.1001/ jama.280.12.1102 Sidel, V. W., & Sidel, R. (1983). A healthy state (Rev. ed.). New York, NY: Pantheon. Smith, D. B. (2016). The power to heal: Civil rights, Medicare, and the struggle to transform America’s health care system. Nashville, TN: Vanderbilt University Press. Society of Hospital Medicine. (2019). Hospital medicine certification. Retrieved from https:// www.hospitalmedicine.org/professional-development/hospital-medicine-certification/ Somers, A. R. (1983). And who shall be the gatekeeper? The role of the primary physician in the health care delivery system. Inquiry, 20(4), 301–313. Retrieved from https://www .ncbi.nlm.nih.gov/pubmed/6229480 Stange, K. C., Woolf, S. H., & Gjeltma, K. (2002). One minute for prevention: The power of leveraging to fulfill the promise of health behavior counseling. American Journal of Preventive Medicine, 22(4), 320–323. doi:10.1016/S0749-3797(02)00413-0 Starfield, B. (1992). Primary care. New York, NY: Oxford University Press. Starfield, B. (1996). Public health and primary care: A framework for proposed linkages. American Journal of Public Health, 86(10), 1365–1369. doi:10.2105/AJPH.86.10.1365 Stein, L. I., Watts, D. T., & Howell, T. (1990). The doctor-nurse game revisited. New England Journal of Medicine, 322(8), 546. doi:10.1056/NEJM199002223220810 Steinbrook, R. (2002). Nursing in the crossfire. New England Journal of Medicine, 346(22), 1757–1766. doi:10.1056/NEJM200205303462225 Steinhauer, J. (2000, December 25). Worker shortage in health fields worst in decades. The New York Times, p. 1. University of the State of New York. (1995b). Nursing handbook. Albany, NY: New York State Education Department. U.S. Department of Labor, Bureau of Labor Statistics. (2004a). Current population survey: Employment and earnings, 2003. Retrieved from http://www.bls.gov/cps/cpsa2003.pdf U.S. Department of Labor, Bureau of Labor Statistics. (2004b). May 2003 national occupational employment and wage estimates. Retrieved from https://www.bls.gov/oes/tables.htm U.S. Department of Labor, Bureau of Labor Statistics. (2011a). Current population survey: Employment and earnings, 2010. Retrieved from http://www.bls.gov/cps/cpsa2010.pdf U.S. Department of Labor, Bureau of Labor Statistics. (2011b). May 2010 national occupational employment and wage estimates. Retrieved from https://www.bls.gov/oes/tables.htm U.S. Department of Labor, Bureau of Labor Statistics. (2014). Spotlight on statistics. Retrieved from https://www.bls.gov/spotlight/2015/employment-and-wages-in-health care-occupations/home.htm U.S. Department of Labor, Bureau of Labor Statistics. (2016). Occupational outlook handbook. Retrieved from https://www.bls.gov/ooh/home.htm
Goldsteen74024_03_CH03_79-124_03-18-20.indd 122
3/19/20 10:53 AM
3
■
Th e P e o p l e W h o P ro v i d e H e a l t h C a re
123
U.S. Department of Labor, Bureau of Labor Statistics. (2019a). Data on certifications and licenses. Retrieved from https://www.bls.gov/cps/certifications-and-licenses.htm U.S. Department of Labor, Bureau of Labor Statistics. (2019b). Occupational employment statistics. Retrieved from https://www.bls.gov/oes/current/oes311014.htm U.S. Department of Labor, Bureau of Labor Statistics. (2019c). About the U.S. Bureau of Labor Statistics. Retrieved from https://www.bls.gov/bls/infohome.htm U.S. Department of Labor, Bureau of Labor Statistics. (2019d). Current population survey: Employment and earnings, 2018. Retrieved from http://www.bls.gov/cps/cpsa2018.pdf U.S. Department of Labor, Bureau of Labor Statistics. (2019e). May 2018 national occupational employment and wage estimates. Retrieved from https://www.bls.gov/oes/current/ oes_nat.htm#29-0000 U.S. Department of Labor, Bureau of Labor Statistics. (2019f). Labor force statistics from the current population survey, 2018. Retrieved from https://www.bls.gov/cps/cpsaat11.htm U.S. Department of Labor, Bureau of Labor Statistics. (2019g). Table 3. Union affiliation of employed wage and salary workers by occupation and industry. Retrieved from https://www .bls.gov/news.release/union2.t03.htm U.S. House of Representatives, Subcommittee of the Committee on Appropriations. (2005). Departments of Labor, Health and Human Services, Education, and Related Agencies: Hearings on appropriations for 2006. Washington, DC: House of Representatives. Wachter, R. M., & Goldman, L. (1996). The emerging role of “hospitalists” in the American health care system. New England Journal of Medicine, 335(7), 514–517. doi:10.1056/ NEJM199608153350713 Wachter, R. M., & Goldman, L. (2002). The hospitalist movement 5 years later. Journal of the American Medical Association, 287(4), 487–494. doi:10.1001/jama.287.4.487 Weiner, J. P. (2002). A shortage of physicians or a surplus of assumptions? Health Affairs, 21(1), 160–162. doi:10.1377/hlthaff.21.1.160 Wennberg, J. E., Fisher, E. S., & Skinner, J. S. (2002). Geography and the debate over Medicare reform. Health Affairs, 21, W96–W114. doi:10.1377/hlthaff.W2.96 Wennberg, J. E., & Members of the Dartmouth Atlas of Health Care Working Group. (1996). The Dartmouth atlas of health care. Chicago, IL: American Hospital Publishing. White, K. L. (1968, January). Organization and delivery of personal health services: Public policy issues. Milbank Memorial Fund Quarterly, 46, 225–258. doi:10.2307/3349156 Wilbur, C. K. (1980). Revolutionary medicine, 1700–1800. New York, NY: Chelsea House.
FURTHER READING Accreditation Council for Graduate Medical Education. (2012). The ACGME at a glance. Retrieved from www.acgme.org/acWebsite/newsRoom/newsRm_acGlance.asp Association of American Medical Colleges. (2017). The complexities of physician supply and demand, 2015-2030: 2017 update. Retrieved from https://www.aamc.org/data/workforce/ Association of American Medical Colleges. (2018). 2018 physician specialty data report. Retrieved from https://www.aamc.org/data/workforce/reports/492922/snapshot.html
Goldsteen74024_03_CH03_79-124_03-18-20.indd 123
3/19/20 10:53 AM
124
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
American Nurses Association. (2010). Nursing: Scope and standards of practice (2nd ed.). Silver Spring, MD: NursesBooks.org. American Osteopathic Association. (2011). Colleges of osteopathic medicine. Retrieved from www.osteopathic.org/inside-aoa/about/affiliates/Pages/osteopathic-medical-schools.aspx Dalen, J. E., Ryan, K. J., & Alpert, J. S. (2017). Where have the generalists gone? They became specialists, then subspecialists. The American Journal of Medicine, 130(7), 766–768. doi:10.1016/j.amjmed.2017.01.026 Ferris, T. G., Chang, Y., Blumenthal, D., & Pearson, S. D. (2001). Leaving gatekeeping behind: Effects of opening access to specialists for adults in a health maintenance organization. New England Journal of Medicine, 345(18), 1312–1317. doi:10.1056/NEJMsa010097 Henderson, R. (2012, January). Employment outlook: 2010–2020: Industry employment and output projections to 2020. Monthly Labor Review, pp. 65–83. Kacik, A. (2018, March 16). Rapid rise in hospital-employed physicians increases costs. Modern Healthcare. Retrieved from https://www.modernhealthcare.com/article /20180316/TRANSFORMATION02/180319913/rapid-rise-in-hospital-employed-phy sicians-increases-costs Kaiser Family Foundation. (2010). Registered nurses per 100,000 population, 2010. StateHealthFacts.org. Lumsdon, K. (1995, December 5). Faded glory. Hospitals and Health Networks, p. 31. National Center for Health Statistics. (2011). Health, United States, 2010. Hyattsville, MD: U.S. Department of Health and Human Services. University of the State of New York. (1995a). Medicine handbook. Albany, NY: New York State Education Department. Wunderlich, G. S., Sloan, F. A., & Davis, S. (Eds.). (1996). Nursing staff in hospitals and nursing homes: Is it adequate? Washington, DC: National Academies Press.
Goldsteen74024_03_CH03_79-124_03-18-20.indd 124
3/19/20 10:53 AM
4 Medicines, Devices, and Technology
© Randy Glasbergen.
LEARNING OBJECTIVES After completing this chapter, students will be able to: • Describe the major categories of products and their users, purchasers, and deciders. • Describe the typical research, development, and regulatory cycles of each category. • Describe the makeup of the firms working in each market.
Goldsteen74024_04_CH04_125-148_03-18-20.indd 125
3/19/20 3:06 PM
126
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
INTRODUCTION Medicines, devices, and technology encompass the medical devices (supplies and equipment), pharmaceuticals, and other health care-specific technology unique to health care delivery. Also important in the delivery system’s supply chain are the goods and services typically needed by all industries, including structures such as offices and buildings, information technology tools, paper and other supplies, and consulting and other business services. Such expenditures represent about 20% of the national health expenditure. Medical products can be categorized based on how they work, how they are purchased, and how they are used. Medical devices that are used once are referred to as medical supplies, while medical equipment can be used again and again. Those that work on a biochemical level are referred to as pharmaceuticals. Products may be purchased by providers who use or administer them to their patients; retail products are purchased directly by consumers (typically the user or a family member). Some retail products may only be available with a prescription from the patient’s treating provider (e.g., opioids or contact lenses), while other “nonprescription drugs” and sundries are available “over the counter” (OTC; e.g., ibuprofen or reading glasses).
PHARMACEUTICALS Products intended to cure, treat, mitigate, diagnose, or prevent disease in humans or otherwise affect the structure or function of the human body through chemical action in and/or metabolized by the human body are considered human drugs or biological products (U.S. Food & Drug Administration [FDA], 2016a). Biological products are generally large, complex molecules “produced through biotechnology in a living system, such as a microorganism, plant cell, or animal cell” (FDA, 2019a). This is contrast to conventional drugs, what most people think of when they imagine a medicine—typically a tablet or capsule, taken by mouth and containing a single chemically synthesized active ingredient, like aspirin. Conventional drugs are also referred to as “small molecule drugs” (FDA, 2019b; PhRMA, 2015). In general, such drugs include an “active pharmaceutical ingredient” (API) that can be obtained from a chemical supply company and formulated into a drug product. Drugs generally have well-defined chemical structures, and a finished drug can usually be analyzed to determine all its various components (Bio, 2019). On the other hand,“biologics are complex mixtures that are not easily identified or characterized” (FDA, 2018a). In fact, there are some licensed biologics where the mode of action is not completely understood (FDA, 2019b). For biologics, “the product is the process,” and manufacturers must ensure the process remains consistent over time. This differs from the manufacture of conventional drugs, where the process can change as long as the result retains the same components and structure as the originally approved drug and API (Bio, 2019). Despite their challenges, biologics are “revolutionizing the treatment of cancer and autoimmune disorders and are critical to the future of the industry” (U.S. Department of Commerce, International Trade Administration, 2016) and “represent the cutting-edge of biomedical research and, in time, may offer the most effective means to treat a variety of medical illnesses and conditions that presently have no other treatments available” (FDA, 2018a). Biologics grew from 8% of all drug approvals in 2005 to 17% in 2016 (U.S.
Goldsteen74024_04_CH04_125-148_03-18-20.indd 126
3/19/20 3:06 PM
4
■
M e d i c i n e s , D e v i c e s , a n d Te c h n o l o g y
127
Government Accountability Office [GAO], 2017) and three of the top medicines by non-discounted spending in 2017 were biologics (IQVIA Institute, 2018). Biologics are also considered a “specialty” drug, which are drugs that are available in very limited supply, require special handling (e.g., constant temperature regulation or biohazard or similar toxicity), and/or come with a very high price tag. Historically, drugs meeting those criteria were only used for rare diseases so the impact on overall drug spending controlled (Ellis, 2016). In 2017, four of the top five medicines by nondiscounted spending were specialty drugs, and specialty share of net spending on drugs rose from 24.7% in 2008 to 46.5% in 2017 (IQVIA Institute, 2018).
Regulatory Process In the United States, drug companies must apply and receive approval from the FDA that their drugs are safe and effective before they can be sold or marketed for human use (GAO, 2017). Note that marketing of so-called OTC drugs is regulated by the FDA (FDA, 2019c). Additionally, drugs may be “scheduled” as “controlled substances,” which requires adherence to Drug Enforcement Administration (DEA) regulations for manufacturing, distribution, and sales (Pharma Logistics, 2018). Finally, states and local government may further regulate where and how some drugs are distributed and dispensed (U.S. Department of Justice, DEA, 2019a). Drugs that are habit-forming or toxic have too great a potential for harmful effects, are for medical conditions that can’t be readily self-diagnosed and/or believed cannot be used safely without professional supervision, and can only be dispensed with a prescription (“a prescription is an order for medication which is dispensed to or for an ultimate user”; FDA, 2016b; U.S. Department of Justice, DEA, 2019b). These are known as “prescription drugs” and must dispensed to a patient by a pharmacy.* Prescriptions are intended to be used by one person and generally written by a doctor (or other provider as allowed by the state such as a physician’s assistant [PA] or nurse practitioner [NP]) (FDA, 2017a). On the other hand, a drug must be made available OTC if consumers can use it safely and effectively without professional guidance by following the labeling (FDA, 2016b). The FDA has interpreted this requirement by allowing drugs that have already been determined as “generally regarded as safe and effective” (GRAS/E or GRASE) to be sold OTC if they are marketed in a way that is “consistent with the conditions set forth under a final monograph and all other general applicable OTC requirements.” Monographs are “a kind of ‘rule book’ of conditions for each therapeutic category covering acceptable ingredients, uses (indications), doses, formulations, labeling, and testing” that the FDA developed in the early 1970s as part of its implementation of the “OTC Drug Review” to bring an estimated 100,000 to 500,000 OTC drug products under its regulatory purview without doing a product-by-product review. Instead, the FDA developed monographs covering roughly 200 different, active ingredients across 26 therapeutic categories that could then be used by manufacturers to avoid having to submit a New Drug Application (NDA; FDA, 2019d). * In institutional settings such as hospitals, drugs are usually dispensed in response to a “medication order” and typically administered by a nurse or other authorized staff (www.cms.gov/Regula tions-and-Guidance/Guidance/Transmittals/2018Downloads/R183SOMA.pdf); “an order to dispense a drug to an inpatient for immediate administration in a hospital is not a prescription” (www.deadiver sion.usdoj.gov/pubs/manuals/pract/section5.htm).
Goldsteen74024_04_CH04_125-148_03-18-20.indd 127
3/19/20 3:06 PM
128
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
In order to be designated GRASE, a drug must satisfy three criteria: • • •
First, the particular drug product must have been subjected to adequate and well-controlled clinical investigations that establish the product as safe and effective. Second, those investigations must have been published in the scientific literature available to qualified experts. Third, experts must generally agree, based on those published studies, that the product is safe and effective for its intended uses. At a minimum, the general acceptance of a product as GRASE must be supported by the same quality and quantity of scientific and/or clinical data necessary to support the approval of an NDA (FDA, 2019d).
Otherwise, a drug sponsor must ask the FDA to consider approving a new drug for marketing in the United States via the NDA process (FDA, 2017a). The NDA process for new drugs is nominally a 12-step process in which the sponsor shares all drug ingredients and all animal and human data and analyses of the data, as well as information about how the drug behaves in the body and how it is manufactured. A simplified overview created by the FDA is reproduced here: 1. Preclinical (animal) testing 2. An investigational NDA (IND) outlines what the sponsor of a new drug proposes for human testing in clinical trials. 3. Phase 1 studies (typically involve 20–80 people) 4. Phase 2 studies (typically involve a few dozen to about 300 people) 5. Phase 3 studies (typically involve several hundred to about 3,000 people) 6. The pre-NDA period, just before an NDA is submitted; a common time for the FDA and drug sponsors to meet 7. Submission of an NDA is the formal step asking the FDA to consider a drug for marketing approval. 8. After an NDA is received, the FDA has 60 days to decide whether to file it so it can be reviewed. 9. If the FDA files the NDA, an FDA review team is assigned to evaluate the sponsor’s research on the drug’s safety and effectiveness. 10. The FDA reviews information that goes on a drug’s professional labeling (information on how to use the drug). 11. The FDA inspects the facilities where the drug will be manufactured as part of the approval process. 12. FDA reviewers will approve the application or issue a complete response letter (FDA, 2015a). Note that the NDA is also used for direct-to-OTC reviews (i.e., a drug that wasn’t previously regarded as GRAS/E but for which the sponsor believes can be made safely available OTC). Additionally, NDA are used for the so-called “Rx-to-OTC switch,” in which drugs that were previously only available by prescription are switched to OTC status (FDA, 2019d). Table 4.1 provides for a comparison of the NDA and OTC Monograph approval process. Section 351 of the Public Health Service (PHS) Act as amended by the Biologics Price Competition and Innovation Act of 2009 (otherwise known as the BPCI Act) defines a biological product as a “virus, therapeutic serum, toxin, antitoxin, vaccine, blood, blood component or derivative, allergenic product, or analogous product, … applicable to the prevention, treatment, or cure of a disease or condition of human beings.” Additionally, FDA regulations and
Goldsteen74024_04_CH04_125-148_03-18-20.indd 128
3/19/20 3:06 PM
4
■
M e d i c i n e s , D e v i c e s , a n d Te c h n o l o g y
129
policies have established that biological products include vivo diagnostic allergenic products, immunoglobulin products, products containing cells or microorganisms, and most protein products, including monoclonal antibodies for in vivo use and cytokines, growth factors, enzymes, immunomodulators, and thrombolytics (FDA, 2015b, 2017b). Note that while all biologics are also considered drugs regulated under the Federal Food, Drug, and Cosmetic Act (FDCA) as well as the PHS Act, hormones such as insulin, glucagon, and human growth hormone are not considered biological products under the PHS Act and only covered under the FDCA. This becomes particularly important for the question of how to introduce competition for these products into the market. For biologics subject to the PHS Act, a biologics license application (BLA) replaces the NDA and emphasis is placed on appropriate manufacturing control for products covering all aspects of the manufacturing process. While the concept of the BLA is similar to the NDA process (in fact, the same form is used for both), with a sequence of initial laboratory and animal testing followed by clinical trials in humans, the BLA provides that the product, the manufacturing process, and the manufacturing facilities meet applicable requirements to ensure the continued safety, purity, and potency of the product (FDA, 2015b). While a successful NDA or BLA allows a drug’s sponsor to market a drug in the United States, the drug may be subject to additional controls on its distribution and acceptable prescribing by the Controlled Substance Act (CSA), which is enforced by the DEA. The CSA categorizes controlled substances into “schedules” ranging from I to V. Schedule I includes drugs, substances, or chemicals with no currently accepted medical use and a high potential for abuse, and may not be prescribed (they are essentially illegal under all circumstances). Schedule II drugs have high potential for abuse, with use potentially leading to severe psychological or physical dependence, but may be prescribed under strict rules. Schedule III to V drugs have progressively fewer risks with somewhat fewer restrictions. Schedule V drugs may be available OTC in some states, though extensive documentation for each purchase must be maintained (U.S. Department of Justice, Drug Enforcement Administration, 2019a). In the same way that drugs that were once prescription-only may become available OTC, drugs may also be rescheduled or de-controlled (i.e., removed from the schedules and no longer subject to DEA oversight). In fact, some previously scheduled drugs, such as loperamide and propylhexedrine, are now available OTC (U.S. Department of Justice, DEA, 2019c). Final determination of a drug’s schedule is made by the DEA’s administrator (Yeh, 2012). Additionally, there are some drugs which are effectively “behind the counter.”This refers to drugs that do not require a prescription but must be dispensed by a pharmacist (and, as such, are typically stored behind the counter at the pharmacy). These include human insulin (Goldstein, McCrary, & Lipska, 2018) as well as pseudoephedrine (a decongestant that was abused as a starter chemical for methamphetamine production) and Plan B (an emergency contraceptive originally approved by the FDA in 2006 as a nonprescription product for women aged 18 years and above and now nonprescription for those aged 17 years and above) (Pray & Pray, 2011). While there is some debate on the cost of bringing a new drug to market, estimates typically range from the hundreds of millions of dollars to billions of dollars (Prasad & Mailankody, 2017), and it is generally accepted that the process can take up to 15 years. As such, intellectual property protections and market exclusivity are considered critical requirements for attracting investment for new drug development. In the United States, patents are issued by the U.S. Patent and Trademark Office, and once granted, other drug companies are excluded from making, using, or selling the patented aspect of the drug during the term of the patent, which generally expires after 20 years from filing (GAO, 2017). Additionally, the law authorizes market exclusivity through delays and prohibitions on approval of competitor drugs for applications that meet statutory requirements such as “orphan drug exclusivity” (drugs that treat rare diseases) or“pediatric exclusivity”(for conducting additional studies specific to pediatric patients;
Goldsteen74024_04_CH04_125-148_03-18-20.indd 129
3/19/20 3:06 PM
130
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
FDA, 2016c, 2018b, 2018c). For drugs that generate hundreds or even billions of dollars per year in sales and are relatively low cost to manufacture (especially true of small molecule drugs), the duration of these exclusivity periods can have substantial impact on drug company profits. However, once these protections expire (or a competitor wishes to challenge them), an Abbreviated New Drug Application (ANDA) may be filed. The ANDA allows the competitor to produce and market a drug equivalent to an approved brand-name drug—commonly referred to as“generic”—without conducting the same clinical trials. The ANDA needs only to show that its version of the drug is the same in terms of “active ingredient, dosage form, safety, strength, route of administration, quality, performance characteristics and intended use”(GAO, 2017). Biologics have proven more challenging in this respect since they are inherently “complex mixtures that are not easily identified or characterized.”Given their growing significance (and cost), the BPCI Act established a regulatory framework of “biosimilars” that are highly similar to an FDA-approved biological product and have no clinically meaningful differences in terms of safety and effectiveness (GAO, 2017). If a proposed biosimilar can show it has no clinically meaningful differences in safety, purity, and potency (safety and effectiveness) from an existing FDA-approved reference product, the safety and effectiveness of the proposed product does not need to be independently established. This generally reduces the need for as many expensive and lengthy clinical trials before a biosimilar can be marketed (FDA, 2017c). While the FDA premarketing approval process is extensive, once a drug is on the market, the FDA has several postmarketing surveillance programs to identify adverse events that did
TABLE 4.1 Pharmaceutical Approval Process, 2019 NDA Approval Process
OTC Monograph Process
Premarket approval—FDA reviews and approves formulation and labeling prior to marketing.
No premarket approval—FDA sets forth specific conditions for GRASE, or in the case of a developing monograph, sets forth conditions that allow for continued marketing pending a final monograph. Oversight occurs on a postmarketing basis.
Confidential filing
Public process
Drug-product specific
Active-ingredient specific and evaluated by OTC drug category
May require a user fee
No user fees
Potential for marketing exclusivity
No marketing exclusivity
FDA reviews timelines
Manufacturers responsible for ensuring compliant product with no FDA-mandated review (either pre- or postmarket)
May require clinical studies, including studies on label comprehension and actual use
Generally, does not require clinical studies. Label comprehension and actual use studies are not required for ingredients already covered by a final or tentative final monograph.
Approved labeling is unique to the drug.
Labeling is defined by the monograph. Once marketed, the FDA can review the complete labeling at any time to determine whether it is truthful or misleading.
Approved NDA is your “license” to market.
Final monograph is open to anyone.
Trade name is reviewed prior to marketing.
No review of trade name prior to marketing. Once marketed, FDA can review the trade name at any time.
GRASE, generally regarded as safe and effective; NDA, new drug application; OTC, over-the-counter. SOURCE: U.S. Food and Drug Administration. (2019d). Regulation overview. Retrieved from https://www.accessdata.fda.gov/scripts/cder/ training/OTC/topic3/topic3/index03.htm
Goldsteen74024_04_CH04_125-148_03-18-20.indd 130
3/19/20 3:06 PM
4
■
M e d i c i n e s , D e v i c e s , a n d Te c h n o l o g y
131
not appear during the drug approval process. From these events, the FDA may require updates to drug labeling, recalls, or reevaluation of the approval or marketing decision. These programs include: • • • •
•
Centralization of adverse events in a computerized reporting system (FAERS) Voluntary reporting of adverse serious reactions and problems with medical products, through MedWatch Identification of products that have no effect or are toxic, through Therapeutic Inequivalence Reporting Capturing and reporting on discontinuances and interruptions of the manufacture of any drug that is life supporting, life sustaining, or intended for use in the prevention or treatment of a debilitating disease or condition, through Drug Shortage Management Unannounced inspections of drug production and control facilities (FDA, 2016d)
Who Decides, Who Pays While OTC drugs are sold in retail settings and purchased and used like many other consumer products, the market is more complicated for prescription drugs purchased in retail settings. Inherently, purchase of a prescription drug requires a prescription from a health care provider who decides which drug to prescribe, how much, and how frequently, based on the provider’s medical judgment in the context of the patient and the patient’s needs. Such health care providers “may not be well-informed about, or incentivized to consider, the prices involved” (GAO, 2017). Additionally, third-party payers (i.e., health insurance or managed care companies, discussed in a later chapter) may insulate the patient from the cost of different medicines, and patients’ preferences may not be as significantly influenced by differences in prices as if they were paying the full amount. Restricted formularies with tiered copays and/or coinsurance are an attempt to incentivize patients toward lower-cost solutions, but these can generate a lot of conflict between the payers, providers, and patients. Some drug companies have worked around this by providing coupons to consumers to make up the difference—allowing the patients to stay on the familiar drug without paying a premium over their payers’ preference. While this may result in a lower price for the patient, it likely increases overall drug spending (GAO, 2017). Much of these negotiations play about between pharmacy benefit managers (PBMs), which insurance plans use to help them manage their prescription drug benefits, drug manufacturers, and retail pharmacies. PBMs sit between these three, negotiating rebates from manufacturers and contract terms and rates with pharmacies, and sharing in rebates to the insurance plans. The PBMs’ negotiating leverage derives from the purchasing power they control versus the numbers of competitors negotiating with the drug manufacturers (GAO, 2017). In 2017, the top three PBMs managed over 70% of the prescriptions filled in the United States (Fein, 2018). The result is different prices for the same drug depending on who is paying the bill, though the exact net price is often difficult to ascertain as the rebates and discounts are confidential (Ellis, 2016). Additionally, depending on how the rebates and discounts are structured, they may not reduce the costs patients pay at the register, as their coinsurance or deductibles are often based on the list prices and not the rebates that typically flow directly to the insurance companies (presumably resulting in reduced premiums; Dieguez, Alston, & Tomicki, 2018; PhRMA, 2017). However, the Centers for Medicare & Medicaid Services (CMS) has recently proposed new regulations that would require that all such discounts and rebates would be credited to the prices on which the patients’ cost-sharing responsibilities would be based for those covered by a Medicare or Medicaid plan, starting in 2020 (Roy, 2019).
Goldsteen74024_04_CH04_125-148_03-18-20.indd 131
3/19/20 3:06 PM
132
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
While there is some debate whether PBMs bring net savings to the health care systems or add cost as an additional intermediary, there is little debate that the resulting system is complicated. Outside of the retail setting, prescription drugs are also a critical supply for providers. In addition to the US$333 billion spent on prescription drugs in the retail setting in 2017 (9.5% of National Health Expenditures [NHE]), an estimated US$148 billion (4.2% of NHE) was spent in nonretail settings: • • • •
Hospitals: 26.3% Physician and clinical service: 58.3% Nursing homes: 11.5% Home health: 3.9% (Roehrig, 2019)
Prescription drugs are charged to payers as (a) bundled into other services provided or (b) separately charged with a service fee. The latter is the current approach used by CMS’s Medicare Part B (discussed in later chapters) to cover physician-administered drugs for treating cancer or immunological disorders when provided as a service in a physician’s office. In this situation, Medicare pays the physician’s office using a fee schedule based on the average U.S. sales price for these drugs and biologics. As constructed, the physician is effectively paid a percentage of the approved drug price and there is no incentive for the provider to choose a lower-cost drug. Similarly, there is no incentive for the drug manufacturer to lower its prices (Antos & Capretta, 2019; Bishop, Ramsay, Gustafsson, & Martin, 2018). On the other hand, drugs used in the course of an inpatient hospital stay covered by Medicare Part A are treated the same way as other supply costs that the hospital incurs in treating that patient, and it is up to the hospital to manage those costs (CMS, 2019a, 2019b). Techniques for controlling such costs include contract negotiations (possibly with the assistance of a group purchasing organization [GPO]), formulary management, and utilization management (American Society of Health-System Pharmacists, 2008). One other approach large health providers such as hospitals have taken is compounding their own drugs rather buying them from manufacturers (when not covered by patent). While this would seem regressive to the general trend of specialization and leveraging economies of scale in manufacturing, it seems some hospitals have taken this approach to insulate themselves from price spikes and shortages (Fry, 2018).
Drug Research, Development, and Manufacturing In summarizing the U.S. pharmaceutical market, the U.S. International Trade Association (ITA) writes, [T]he United States has one of the world’s most supportive domestic environments for the development and commercialization of pharmaceuticals with minimal market barriers. Its strengths include an intellectual property system that rewards innovation through patent and data protection, a science-based regulatory system that is considered the most rigorous in the world, the world’s largest scientific research base fostered by academic institutions and decades of government research funding, and robust capital markets. The United States attracts the majority of global venture capital investments in start-up biopharmaceutical enterprises… . All of these factors contribute to it being, by far, the world’s largest pharmaceutical market …, about triple the size of its nearest rival, China. The United States will remain
Goldsteen74024_04_CH04_125-148_03-18-20.indd 132
3/19/20 3:06 PM
4
■
M e d i c i n e s , D e v i c e s , a n d Te c h n o l o g y
133
the world’s most important market for the foreseeable future with healthy growth expected across all product sectors. (U.S. Department of Commerce, ITA, 2016) In financial terms, net payments to pharmaceutical companies for prescription drugs sold in the United States were about US$325 billion in 2017, with about 77% of this for patented drugs and 23% for generic prescription drugs, though the latter accounted for about 90% of prescriptions filled (Association for Accessible Medicines, 2018). An additional US$34.6 billion was spent on OTC drugs and other health-related products in 2017 (Consumer Healthcare Products Association, 2019). This revenue was used to employ over 800,000 people and fund an estimated US$90 billion in research and development (R&D) in 2016 (PhRMA, 2018). However, the reported spending on R&D has been controversial both in what it includes and the amount relative to spending on selling, marketing, and promotion expenses. In 2017, this was estimated at 19% of revenues among the U.S. pharmaceutical companies (Florko, 2019), which relatively speaking was down from 2004, when such expenses were estimated to be double the amount spent on R&D. Such allocation of resources supported “the position that the U.S. pharmaceutical industry is marketing-driven and challenges the perception of a research-driven, life-saving, pharmaceutical industry” (Gognon & Lexchin, 2008). So while the ITA celebrated “U.S. laws allowing direct-to-consumer advertising [that] creates immense demand for specific patented drugs,” such spending has engendered a backlash especially when“prices [for drugs] are comparatively high to make up for lower profits in other countries and to cover R&D costs” (U.S. Department of Commerce, ITA, 2016). Also controversial are the results from all that is spent on R&D and how much of this results in truly“novel drugs,”which are commonly defined as“innovative products that serve previously unmet medical need or help advance patient care.” These have averaged about 13% of all FDA-approved NDA each year (GAO, 2017). Prior to the preclinical testing phase that kicks off the sequence typically detailed in an NDA regulatory filing, compounds that are both safe and effective must be created. This typically follows from a combination of basic research and focused drug discovery. Basic research focuses on acquiring new knowledge or understanding independent of commercial application or use (GAO, 2017). This includes trying to understand the basic biological processes and implications for disease. When sufficient understanding is reached—such as when a specific receptor or target is identified—a process of drug discovery is undertaken to find and identify compounds (e.g., small molecules or biologics) capable of safely and effectively treating or curing a disease (e.g., by triggering or blocking a biological process in the body). Generally, “development” is the largest component of pharmaceutical companies’ R&D budget, while basic research is the smallest. For example, pharmaceutical companies reported allocating 13% of total reported domestic R&D spending on basic research, 21% on applied research, and 66% on development in 2014. Converted to 2015 dollars, the GAO estimated this totaled US$89 billion, or about US$11.5 billion for basic research (GAO, 2017). During the same period, federal spending on basic research totaled about US$28 billion. This is also consistent with a pattern of interaction outlined by Kesselheim, Tan, and Avorn, whereby academic scientists identify and conceptualize a therapeutic approach based on basic research about disease mechanisms, and then demonstrate the proof of concept for a given molecule. Industry collaborators then develop the product for more extensive clinical testing. In their study, most of the approved “novel drugs” were based on discoveries made by academic researchers who were supported by federal government funding, others were born of collaborative programs, and least common were drugs that originated solely within the pharmaceutical industry (Kesselheim et al., 2015). Smaller companies are also increasingly part of the process for drug development. So-called “emerging biopharma” (EBP) are defined as companies having less than US$200 million in
Goldsteen74024_04_CH04_125-148_03-18-20.indd 133
3/19/20 3:06 PM
134
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
estimated annual spending on R&D or under US$500 million in global revenue. In 2018, there were over 3,000 such companies and they accounted for 73% of late-stage research. Additionally, such companies were the original patentee for 29 of the current top 100 drugs, which accounted for 40% of sales and 42% of the new drugs launched in the United States in 2018. The IQVIA Institute (2019) estimates that 80% of the industry’s total development pipeline comes from EBP. However, their products generally reach the market faster if acquired and launched by traditional large pharmaceutical companies (IQVIA Institute, 2019). As the GAO summarized experts’ consensus, “innovation comes from multiple sources and increasingly from smaller innovative biotechnologies companies,” while large drug companies are needed “to invest in the expensive clinical trials needed to develop and bring new innovations to market” (GAO, 2017). The motivation for large companies to acquire is looming patent expiration or pipeline gaps, while small companies look to be acquired in response to financial challenge (Danzon, Epstein, & Nicholson, 2007). Acquisition and asset licensing resulted in 415 deals, with an aggregate disclosed value of US$272 billion, in 2018 (IQVIA Institute, 2019). Estimates of how much it costs to bring a new drug to market range from an average of US$0.6 billion to US$1.4 billion on average, and US$2.7 billion for a new cancer drug (DiMasi, Grabowski, & Hansen, 2016; Prasad & Mailankody, 2017). Regardless of whether the low end or the high end of the estimates is more accurate, it costs a lot of money to bring a new drug to market. For drugs that will be used by millions, the per-patient costs can be kept lower while still covering the initial research costs. However, for drugs that treat rare diseases, the costs can be extreme. For example, about 300 to 500 babies are born each year with spinal muscular atrophy, from which most babies born with it will die within two years, and a new gene therapy promises to cure it but with pricing projected at US$2 million. While this is likely lower than the lifetime costs of current treatments, this and similar therapies and biologics are expected to put tremendous pressure on the current payment models and health insurance market in general (Roland, 2019). After a drug has been discovered, taken through clinical trials, and approved by the FDA, it needs to be manufactured. For branded small-molecule drugs, these are typically mass produced in a plant with lines dedicated to making one to two drugs. Once a drug is available for production as a generic, lines may alternate among 30 to 50 drugs and single plants may produce hundreds of different drugs (Gottlieb, 2016). All such manufacturing operations are subject to strict controls and quality assurance programs that meet the FDA’s Current Good Manufacturing Practice (CGMP) regulations (FDA, 2018d). It should also be noted that 40% of finished drug products, 64% of biologics, and 80% of API are sourced from abroad (FDA, 2019e; GAO, 2016). The shift to overseas manufacturing of drugs largely occurred in the early 2000s, and regulation of drugs for import into the United States has been a challenge for the FDA (FDA, 2018e; GAO, 2016).
Small Number of Large Companies, Large Number of Small Companies During the past several years, a series of mergers and acquisitions have resulted in concentration within the global industry among both innovative and generics companies of all sizes. Additionally, biosimilars, with their higher manufacturing and regulatory cost, are becoming more prevalent, leading generic companies’ business model and investment cycle to more resemble those of innovator companies: “The lines between innovator and generic companies or between pharmaceutical and biotechnology companies have become increasingly blurred, and most major multinationals now incorporate both biologics and generics subsidiaries in their portfolios” (U.S. Department of Commerce, International Trade Administration, 2016).
Goldsteen74024_04_CH04_125-148_03-18-20.indd 134
3/19/20 3:06 PM
4
■
M e d i c i n e s , D e v i c e s , a n d Te c h n o l o g y
135
Drugs no longer covered by patents may also be made and sold at retail by compounding pharmacies as long as they are not copies of commercially available drugs (Tallapragada, 2016). In addition to providing customized drugs to meet unique patient needs, they have also been an alternative source for drugs for which a sole manufacturer significantly increased the price or discontinued its manufacture (Goldman, 2014; Sternberg, 2015). As such, compounding drugs serve an important public health need and an estimated 1% to 3% of all pharmaceuticals dispensed in the United States are compounded (Goldman, 2014). Compounding pharmacies are generally regulated by state boards of pharmacy, though the FDA does conduct surveillance as well (FDA, 2019f). After a particularly“troubling”incident in 2012, compounding pharmacies received increased scrutiny and additional federal oversight laws were passed in 2013 (American Pharmacists Association [APhA], 2019; Goldman, 2014). Among other changes were the establishment of FDA oversight for what are now called“outsourcing facilities,” which can compound drugs from approved API in larger batches than a local compounding pharmacy without an NDA or ANDA (APhA, 2019; Goldman, 2014).
MEDICAL DEVICES Medical devices are items that are items used for the diagnosis, cure, mitigation, treatment, or prevention of disease but are not absorbed or metabolized by the body. This includes everything from latex gloves and syringes to advanced imaging equipment and implantable devices such as pacemakers (Medicare Payment Advisory Commission [MedPAC], 2017). As the MedPAC notes, the medical device industry is an “important component of the larger health care system and plays an essential role by developing new medical technologies that can improve the ability to diagnose and treat illness” (MedPAC, 2017). Medical devices are generally categorized along two dimensions: • •
Medical supplies versus equipment Conventional versus high-technology
Medical supplies are intended to be used once (e.g., latex gloves or disposable syringes), while medical equipment (e.g., an MRI system) is expected to be used multiple times over its life (MedPAC, 2017). Conventional devices are what economists might refer to as “commodities”—products that are easy to manufacture with relatively few barriers for entry for new companies and relatively little product differentiation. Manufacturers typically compete on price and need high sales volumes to be profitable (MedPAC). High-technology devices typically require significant investment in R&D to design, often resulting in patents and greater regulatory scrutiny from the FDA. This market is characterized by greater barriers to entry, fewer competitors, and higher profit margins (MedPAC).
Regulatory Process Medical devices were relatively unregulated at the federal level until 1976, when Congress expanded the FDA’s regulatory authority with the Medical Device Amendment of 1976 to include preapproval of medical devices before manufacturers could market and sell them. Prior to that, the agency could prosecute only individuals who misused medical devices (MedPAC, 2017). Similar to the situation that the FDA faced with a large number of OTC drugs on the market when it introduced the OTC Drug Review, there were a large number of medical devices already on the market that had been in use for decades if not longer. As such, the devices already on the market were “grandfathered” into the regulatory system and were
Goldsteen74024_04_CH04_125-148_03-18-20.indd 135
3/19/20 3:06 PM
136
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
not required to go through the same regulatory processes to stay on the market that new products would have to go through. Devices that existed on the market prior to the 1976 amendment are referred to as “preamendment devices” and those that came after are, not surprisingly, known as “postamendment devices” (MedPAC, 2017). However, drugs are by definition designed to be absorbed or metabolized in the body, while medical devices are not; and the breadth of medical devices and the risks they pose to patients spans a much wider range. As such, the FDA designed a tiering system whereby the amount of scrutiny a device needs to undergo before it can be marketed is aligned to the risk such devices are believed to pose to patients. These tiers range from Class I (lowest risk) to Class III (highest risk; MedPAC, 2017): •
•
•
Class I includes elastic bandages, examination gloves, and hand-held surgical instruments, and manufacturers simply need to register the device before bringing to market (preapproval is not required). Class II includes surgical drapes, infusion pumps, and powered wheelchairs, and these devices require preapproval before they may be sold; but manufacturers only need to demonstrate that the medical device is substantially equivalent to one already on the market—they do not need to demonstrate that their particular model is safe or effective. Class III includes heart valves, silicone breast implants, and implanted cerebella stimulators, and manufacturers of these devices are generally required to demonstrate that they are safe and effective before they may be marketed.
Most Class II devices are approved through a so-called 510(k) process (named after the section of the FD&C Act); some Class I and Class III devices may also use the 510(k) process. It should be noted that since a device needs to demonstrate only that it is substantially equivalent to a device already on the market and that device may have been approved through a similar 510(k) and so forth, it is possible—and not uncommon—for a product to be approved through a sequence of 510(k) approvals that trace back to a preamendment device (i.e., a device that was grandfathered for continued availability on the market without ever having to demonstrate that it was safe or effective). About 31% of new devices brought to market came through the 510(k) process (MedPAC, 2017). Most Class III devices are approved through a “premarket approval” (PMA) process that is conceptually similar to the NDA process. Clinical data must be submitted to provide assurance that the device is both safe and effective and outside experts may be convened to help evaluate the application. However, while the NDA process often requires two randomized controlled studies, most PMA applications relied on one study that did not meet the criteria of a randomized controlled trial. The FDA reviews about 40 applications a year, representing about 1% of new medical devices brought to the market, and the estimated cost to a manufacturer to take a device through the process is about four to 10 times that of a 510(k) (MedPAC, 2017). Also, the design of devices approved under the PMA process may be modified over time by filing a supplement to the previous application rather than an entirely new application. This may happen dozens of times over the life of a device (MedPAC, 2017). This has led to serious issues in some cases, such as an example of implanted cardiac defibrillators used to shock a heart out of a deadly rhythm known as ventricular fibrillation. One manufacturer filed a supplement to the PMA with what probably seemed like a minor change to the design to use thinner electrical leads into the heart. However, the new wires were prone to fracture, causing some patients to be repeatedly shocked and others not to receive any therapy when they needed it (Lenzer & Brownlee, 2019). As such, whether through approval under the 510(k) process or as a supplement to the PMA process, many, if not most, Class II
Goldsteen74024_04_CH04_125-148_03-18-20.indd 136
3/19/20 3:06 PM
4
■
M e d i c i n e s , D e v i c e s , a n d Te c h n o l o g y
137
or Class III devices on the market never underwent any randomized clinical trials of the particular design being sold. Additionally, many devices may have never undergone any randomized clinical trials if they could trace a lineage back to a premarket device (MedPAC, 2017). The stethoscope may be the most common example of a medical device frequently sold and used today that would probably not pass modern standards (Sataline, 1998). While nearly ubiquitous among physicians,“as a reliable medical test, it is mediocre,”according to Dr. Harlan Krumholz, cardiologist and the Harold H. Hines, Jr. Professor of Medicine and Epidemiology and Public Health at Yale University School of Medicine. In a study of patients with serious valvular heart disease, general practitioners were able to discern the problem in fewer than half the patients (Krumholz, 2018). Or as Dr. Eric Topol, a cardiologist and founder and director of Scripps Research Translational Institute noted, “It has very little utility compared to how it continues to be so highly revered” (Abbott, 2019). A more serious example is “surgical meshes.” All surgical meshes entering the United States are cleared for clinical use through the 510(k) process. However, since the process has to show only that a product is substantially the same as a previously approved product, it is technically acceptable for a new product to be approved by showing it is substantially the same as a previously approved but since recalled product. This has happened many times with surgical meshes; 16% of meshes approved between 2013 and 2015 were based on three preamendment meshes that were recalled for design and material-related flaws causing serious adverse events (Zargar & Carr, 2018). More generally, the Institute of Medicine’s (IOM) assessment of the 510(k) process in 2011 concluded that it is flawed based on its legislative foundation. Rather than continuing to modify the 35-year-old 510(k) process, the committee concludes that the FDA’s finite resources would be better invested in developing an integrated premarket and postmarket regulatory framework that provides a reasonable assurance of safety and effectiveness throughout the device life cycle. (IOM, 2011, p. 3) Not surprisingly then, the FDA has expanded its “postmarket surveillance” since the 2011 report in the context that “no premarket regulatory system for medical devices can guarantee that all new medical devices will be completely safe and effective when they reach the market” (IOM, 2011, p. 3). Echoing the IOM report, MedPAC also noted that “devising an effective system of postmarket surveillance can be challenging because devices typically evolve over time as manufacturers make incremental changes to their designs” (MedPAC, 2017). With those caveats, the FDA now uses a variety of methods to monitor medical devices after they enter the market: • • •
Requiring medical device manufacturers and health care facilities such as hospitals to report any adverse events that involve the use of a medical device Requiring manufacturers to study a device’s safety and effectiveness after it enters the market† Acquiring access to electronic health data such as medical records, claims, and registries to gain more timely and complete information on medical device performance and assess for safety problems through a new National Evaluation System for health Technology (NEST)
†
Note that research has found that these studies can take a long time to complete and may be of limited value (www.MedPAC.gov/docs/default-source/reports/jun17_ch7.pdf).
Goldsteen74024_04_CH04_125-148_03-18-20.indd 137
3/19/20 3:06 PM
138
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
When it does identify a medical device that poses a health risk, the FDA may issue a recall. In federal fiscal year 2016, the agency issued recalls for about 2,900 products and 4% were deemed to pose a“serious risk.”Most recalls are carried out with the cooperation of the device manufacturers (MedPAC, 2017). Another initiative the FDA has underway is to establish a unique device identification system that will enable individual medical devices to be traced from manufacturing through distribution to patient use and into postmarket surveillance (FDA, 2019f; MedPAC, 2017). The goal is for these efforts to support “data mining” or “big data” analysis of databases to identify nonobvious correlations with device underperformance for further investigation, identify all the impacted devices if appropriate, and then accurately and precisely identify those patients affected (MedPAC, 2017). One of the challenges of implanted devices is that even when they are flawed, it is unclear whether the risk of replacement is better than the risk of living with the defective device (Lenzer & Brownlee, 2019).
Who Decides, Who Pays While drugs are most frequently purchased by consumers—with a prescription except in the case of OTC drugs—most medical devices are purchased by health care providers to use in the course of treating their patients. Medical devices are thus an input to care delivery rather than a product directly consumed, and the device manufacturers must engage physicians and hospitals (which typically employ product approval committees to select their products for use in delivering their services). Depending on whether insurance pays for the item directly, the device is one of many items a health system purchases, or the item is purchased by an independent physician’s office, the purchasing decision may be more or less disconnected from the price (MedPAC, 2017; Mercer Capital, 2018). With its responsibility to undertake complex procedures, provide care for the most acute patients, and establish a workforce to support advanced equipment, hospitals in particular are one of the major purchasers and users of medical devices (IBISWorld, 2019). Sales cycles to such organizations are long and typically depend on financial coverage by a third-party payer (e.g., health insurance or managed care company), GPO inclusion, and physician preference (MedPAC, 2017). Similar to the situation when a provider delivers a drug to a patient, the cost of the medical device may be bundled into the overall payment for performing a service. Typically, Medicare and Medicaid consider medical devices as input to the delivery of health care services and not services by themselves, and the cost of a medical device is the provider’s responsibility to be paid out of the overall payment received for the services provided. For example, an implantable medical device (IMD) such as an artificial lens for a cataract replacement surgery isn’t paid separately, and it is expected the payment the hospital receives for the surgery will cover the cost of the lens in addition to whatever other costs the hospital bears in providing the service (MedPAC, 2017). In these situations, the cost of the device is covered as long as it relates to an existing service, which is paid at a rate sufficient to cover use of the device and other required costs. In the case of a new procedure or use of a device not related to already covered services, hospitals typically want payers to extend coverage to the new device or service covering use of the device or it will have to bear the cost, which is typically not financially sustainable. For device manufacturers, gaining payer coverage for their new devices may be critical to its market success, and FDA approval alone does not ensure coverage by any payer, including Medicare (MedPAC, 2017).
Goldsteen74024_04_CH04_125-148_03-18-20.indd 138
3/19/20 3:06 PM
4
■
M e d i c i n e s , D e v i c e s , a n d Te c h n o l o g y
139
As such, device manufacturers will typically first seek Medicare coverage for a new device that does not fit into existing service codes through a public review process. With Medicare coverage in hand, it is often easier to gain coverage from other insurers. However, private insurers are also now requiring evidence not only that devices are safe and effective (the requirement for FDA approval), but how performance compares with existing products (MedPAC, 2017). With FDA approval and third-party payer coverage as appropriate, the next step for a device manufacturer is inclusion in the catalogs of GPOs. GPOs are entities created to represent groups of buyers (e.g., hospitals) in negotiations with medical device companies (and other suppliers) to obtain lower prices. As high-technology devices are often purchased outside of GPO contracts, they are more important for the sale of conventional medical devices. However, virtually all hospitals are part of at least one GPO and about 75% of hospital supplies are purchased through a GPO (MedPAC, 2017). Finally, a device must be selected by the provider. While GPOs often maintain an abbreviated catalog limiting the number of different manufacturers of each type of device, they usually include at least two options. In the case of high-technology devices—especially IMDs, these are often purchased outside of the GPO contract with significant physician involvement in the selection (MedPAC, 2017). IMDs are part of a more general category of medical products referred to as “physician preference items” (PPI): items for which physicians express strong preferences but don’t generally bear the cost of their choice. Although hospitals are typically the purchaser (and may or may not be able to pass the cost along to a third-party payer), hospitals want to accommodate physicians’ preferences, especially when physicians can control where their patients are admitted. While there are advantages to physicians working with the devices with which they are most familiar, strong preferences without consideration for price can dampen competition and make it more difficult for hospitals to negotiate prices with the products’ manufacturers. This is particularly significant for IMD, where the purchase price can equal 30% to 80% of the insurer’s payment to the hospital for the procedure. IMDs typically fall into the high-technology category and are often regulated as Class III devices, meaning that competition and devices are often not completely interchangeable (MedPAC, 2017). As medical devices are often the tools of the physician as their final customers, device makers, more so than drug manufacturers, often seek the input of physicians about the design and potential uses for a new product. In some cases, physicians bring their ideas for new and improved products to manufacturers, and physicians accounted for 20% of the patents issued for medical devices between 1990 and 1996 in one study (MedPAC, 2017). These closer ties between physicians and device companies have also raised concerns about independence in physicians making treatment decisions, and potential conflicts of interest. On the positive side, these close relationships can foster the development of improved medical devices and greater opportunity for training of physicians on the safe and effective use of new devices. On the other hand, there is a risk that they lead to higher delivery-system costs and persistence of lower-quality products based on relationship rather than objective performance (Carreyrou & McGinty, 2011; MedPAC, 2017; O’Connor, Pollner, & Fugh-Berman, 2016). For hospitals trying to negotiate better prices, negotiations are challenged by limited long-term performance data as older designs are frequently replaced by newer, likely creating significant learning curves for physicians to use new devices that may require different techniques to master (for which the training would likely take place on patients), and lack of pricing information. Manufacturers often require that their prices be kept confidential, and manufacturers often charge widely varying prices for the same device to different hospitals (MedPAC, 2017).
Goldsteen74024_04_CH04_125-148_03-18-20.indd 139
3/19/20 3:06 PM
140
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Company/Market Structure MedPAC characterizes the medical device industry as having a “relatively small number of large, diversified companies and a large number of smaller companies that are mainly engaged in research and development of new devices for specific therapeutic areas. The industry is distinctive both for its tendencies to make frequent, incremental changes to its products and its extensive ties with physicians.” Overall, U.S. spending on medical devices was estimated at between US$125 billion and US$172 billion in 2013, and the industry employed an estimated 330,000 to 365,000 people across an estimated 5,300 to 5,600 companies (MedPAC, 2017, p. 207). Similar to brand-name drugs, the market for high-technology medical devices such as IMDs is similar in many respects to brand-name prescription drugs even if not directly regulated the same way. Both require high R&D costs, gaining regulatory approval, and extensive marketing and distribution networks. Economists typically characterize such markets as oligopolies, where there are a small number of sellers that can control their prices to some extent (MedPAC, 2017). On the other hand, medical devices, unlike drugs, can and often are modified over their life cycles. Most medical devices are replaced every 18 to 24 months with newer (and, typically, incrementally different) devices. While the shorter life cycle means that the payback period for R&D is shorter, patents are less applicable and individual devices are typically not as profitable as blockbuster drugs. Still, large medical device companies have been consistently profitable, with typical operating margins between 20% and 30% (MedPAC, 2017). Also, large companies typically sell a mix of conventional and high-technology devices rather than specializing in one or the other. The ongoing sales of conventional devices provides cash flow in between the sales of more expensive devices, which can also serve to mark the manufacturer as a high-performing, technologically advanced company. Additionally, the conventional sales can be used to maintain ongoing relationships with buyers in between sales of higher-margin high-technology devices (MedPAC, 2017). Similar to the EBP companies in the drug market, the medical device market also has its share of smaller, publicly traded device companies whose profit margins are much lower and typically experience net losses each year. Such companies’ success often hinges on a single device and they may lose money for several years while they pursue the long sales cycles required to persuade physicians and hospitals to use and buy their products. Once successful, these startup companies are often acquired by one of the larger device companies. Similar to the drug market, small companies can find it challenging to market their products, while major device companies have established distribution networks and relationships with hospitals and other providers. From there, the large companies can invest additional capital into the product to fund continuing R&D to refine the product further (i.e., fund the incremental improvements required to stay competitive). As with the drug industry, acquiring smaller companies can enhance a larger firm’s pipeline of products or allow it to branch into a new therapeutic area (MedPAC, 2017). Similar to the pharmaceutical industry, there are a few large companies that account for the majority of the revenue and employment while the vast majority of the many thousands of other firms employ fewer than 20 people. And while R&D is higher than other industrial firms, it is generally lower than pharmaceutical firms (MedPAC, 2017). One interesting difference between the pharmaceutical industry and the medical device industry is that the latter has not quite engendered the public outcry over prices despite seemingly similar levels of profitability. Possible explanations are: •
Medical devices are more tangible, with relatively less of the product price tied up in intellectual property as compared to branded small-molecule drugs
Goldsteen74024_04_CH04_125-148_03-18-20.indd 140
3/19/20 3:06 PM
4
• • •
■
M e d i c i n e s , D e v i c e s , a n d Te c h n o l o g y
141
Medical devices are more often single purchases rather than ongoing purchases, like drugs for chronic diseases Medical devices are a small proportion of NHE Medical devices, especially the expensive items, are most often purchased by providers, so patients typically don’t experience the prices firsthand (MedPAC, 2017)
OTHER MEDICAL DEVICES Historically, companies specialized in pharmaceuticals (e.g., Pfizer’s Lipitor) or medical devices (e.g., Boston Scientific’s stents), but the lines continue to blur as medical device companies have incorporated drugs in their designs (e.g., drug-eluding stents) and drug companies have looked to package their drugs for easier administration (e.g., prefilled drug syringes). These products are regulated by the FDA as so-called “combination products” (FDA, 2018g). Additionally, apps as medical devices are becoming important. Mobile medical apps have been used to promote wellness, treat and diagnose disease, aid clinical decisionmaking, and manage patient care in hospitals and homes (Shuren, Patel, & Gottlieb, 2018). However, one of the attributes of mobile devices that makes them attractive for hosting medical apps is that rich applications can be developed and deployed at a low cost; and this also created the need for a dividing line between a helpful app and a regulated medical device. Similar to the need for a dividing line between self-care or care by a family member and the practice of medicine, the FDA needed to determine what it was going to regulate without attempting to regulate every application that might have implications for human health. The FDA’s resulting approach is not to try to regulate the sale or general/conventional consumer use of smartphones or tablets. FDA’s oversight applies to mobile apps performing medical device functions, such as when a mobile medical app transforms a mobile platform into a medical device. However, as previously noted, we intend to apply this oversight authority only to those mobile apps whose functionality could pose a risk to a patient’s safety if the mobile app were to not function as intended. (FDA, 2019g) On the other hand, the FDA wanted to ensure that just because what was previously considered a medical device wasn’t suddenly exempted if hosted on a mobile platform and as such requires similar approval processes for mobile medical apps if they meet the criteria of a medical device and: • •
Are intended to be used as an accessory to a regulated medical device or Transform a mobile platform into a regulated medical device (FDA, 2018h)
Nonetheless, challenges remain for physicians with regards to which apps to prescribe, how it changes the overall physician–patient interaction, and the overall effectiveness of these apps (Comstock, 2018; IQVIA Institute, 2017; Medical Economics, 2015). To address overall effectiveness as well as gain regulatory approval when necessary, some of these apps are now undergoing randomized clinical trials. Another open issue is whether thirdparty payers (e.g., health insurance or managed care organizations) will pay for such apps if prescribed by a physician, similar to how third-party payers usually pay for prescription drugs.
Goldsteen74024_04_CH04_125-148_03-18-20.indd 141
3/19/20 3:06 PM
142
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
SUMMARY Medical devices, medicines, and technology comprise an important and costly sector of the U.S. health care delivery system, which is also important to the general economy. As noted previously the U.S. pharmaceutical sector alone is about triple the size of China’s, its nearest rival and both the pharmaceutical and medical device manufactures make use of the U.S.’s extensive research and scientific base as well as capital markets. The approval and regulation of medical devices, medicine, and technology is a vital and complex process. Safety must be assured while also ensuring that products reach the market within a reasonable amount of time. The European Union (EU) and the United States go about the approval and regulatory process quite differently. The EU has a decentralized system, which requires coordination between the countries with approval and regulatory activities, while the United States has a centralized process, which is headed by the federal FDA. The FDA premarketing approval process is extensive, although once a product is on the market, the FDA also has several postmarketing surveillance programs to identify adverse events that did not appear during the approval process. This can result in updates to drug labeling, recalls, or reevaluation of the original decision.
DATA SOURCES The following websites do not have interactive data. However, each is a source of information—through reports and other documents—about the development, approval, marketing, and use of medicines, devices, and medical technology. •
U.S. Food and Drug Administration. The FDA regulates the following products: drugs, medical devices, and vaccines, blood, and biologics. The publicly available data from the FDA are in the form of reports, which contain budgets, the strategic action plan, performance plans, economic analyses of FDA regulations, and reports on FDA policies and initiatives. Start here to find out more about the development, approval, and regulation of medical devices, medicines, and technology by the FDA: www.fda.gov/about-fda/reports-manuals-forms
•
Medicare Payment Advisory Commission. MedPAC is a nonpartisan, legislativebranch agency that provides analysis and policy advice on the Medicare program to Congress. One of its research areas is drugs, devices, and tests, and its data are in the form of reports. Begin here to review MedPAC reports: www.medpac.gov
•
IQVIA Institute. IQVIA is a private organization focused on health care research, with a particular focus on drugs. The publicly available data from IQVIA are in the form of reports. Some examples are “Orphan Drugs in the United States,”“Medicine Use and Spending in the U.S.: A Review of 2018 and Outlook to 2023,” and “Lifetime Trends in Biopharmaceutical Innovation.” Begin here to review IQVIA’s reports: www.iqvia.com/institute/reports
STUDY QUESTIONS 1. How do the regulatory cycles compare between medical devices and drugs? 2. What is the role of patents and other intellectual property protections in the medical products markets? 3. What are the implications and alternatives for per-use (e.g., per-pill) pricing?
Goldsteen74024_04_CH04_125-148_03-18-20.indd 142
3/19/20 3:06 PM
4
■
M e d i c i n e s , D e v i c e s , a n d Te c h n o l o g y
143
REFERENCES Abbott, B. (2019, August 26). The humble stethoscope gets a high-tech makeover. The Wall Street Journal. Retrieved from https://www.wsj.com/articles/the-humble -stethoscope-gets-a-high-tech-makeover-11556204510. American Pharmacists Association. (2019). Frequently asked questions about pharmaceutical compounding. Retrieved from https://www.pharmacist.com/frequently-asked -questions-about-pharmaceutical-compounding American Society of Health-System Pharmacists. (2008). ASHP guidelines on medication cost management strategies for hospitals and health systems. American Journal of Health-System Pharmacists, 65, 1368–1384. doi:10.2146/ajhp080021 Antos, J. R., & Capretta, J. C. (2019, July 9). A market-oriented framework for reforming Medicare Part B drug payment. Health Affairs Blog. Retrieved from https://www.health affairs.org/do/10.1377/hblog20190708.831097/full/ Association for Accessible Medicines. (2018). Generic drug access & savings in the U.S. Retrieved from https://accessiblemeds.org/sites/default/files/2018_aam_generic_drug_access_and _savings_report.pdf Bio. (2019). How do drugs and biologics differ? Retrieved from https://www.bio.org/articles/ how-do-drugs-and-biologics-differ Bishop, S., Ramsay, C., Gustafsson, L., & Martin, K. (2018). HHS proposes to link Medicare Part B payment for prescription drugs to international prices. Commonwealth Fund— To the Point (blog). Retrieved from https://www.commonwealthfund.org/blog/2018/ medicare-part-b-payment-prescription-drugs-international-prices Carreyrou, J., & McGinty, T. (2011, October 8). Taking double cut, surgeons implant their own devices. The Wall Street Journal. Retrieved from https://www.wsj.com/articles/SB10 001424053111904106704576582621677354508 Centers for Medicare & Medicaid Services. (2019a). Medicare drug coverage under Medicare Part A, Part B, Part C, & Part D. Retrieved from https://www.cms.gov/outreach-and -education/outreach/partnerships/downloads/11315-p.pdf Centers for Medicare & Medicaid Services. (2019b). Acute inpatient PPS. Retrieved from https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatient PPS/index.html Comstock, J. (2018, May 9). Study: There’s still very little evidence that health apps work. Mobihealthnews. Retrieved from https://www.mobihealthnews.com/content/ study-theres-still-very-little-evidence-health-apps-work Consumer Healthcare Products Association. (2019). OTC sales by category 2015-2018. Retrieved from https://www.chpa.org/OTCsCategory.aspx Danson, P. M., Epstein, A., & Nicholson, S. (2007). Mergers and acquisitions in the pharmaceutical and biotech industries. Managerial and Decision Economics, 28(4/5), 307–328. doi:10.1002/mde.1343 Dieguez, G., Alston, M., & Tomicki, S. (2018). A primer on prescription drug rebates: Insights into why rebates are a target for reducing prices. Retrieved from http://www.milliman.com/ insight/2018/A-primer-on-prescription-drug-rebates-Insights-into-why-rebates-are -a-target-for-reducing-prices/
Goldsteen74024_04_CH04_125-148_03-18-20.indd 143
3/19/20 3:06 PM
144
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
DiMasi, J. A., Grabowski, H. G., & Hansen, R. W. (2016). Innovation in the pharmaceutical industry: New estimates of R&D costs. Journal of Health Economics, 47, 20–33. doi:10.1016/j.jhealeco.2016.01.012 Ellis, L. (2016, July 14). Snapshot of the American pharmaceutical industry. Retrieved from https:// www.hsph.harvard.edu/ecpe/snapshot-of-the-american-pharmaceutical-industry/ Fein, A. J. (2018). The outlook for pharmacy benefit management: Evolution or disruption? Retrieved from http://drugchannelsinstitute.com/files/PBMI-PBM_Outlook-Drug_Channels-Fein -Mar2018-Handouts.pdf Florko, N. (2019, May 14). A new study sparks a war of words over the drug industry’s commitment to research. Retrieved from https://www.statnews.com/2019/05/14/ war-of-words-over-pharma-commitment-to-research/ Fry, E. (2018, May 22). Critical condition: Inside Pfizer’s drug supply problem. Fortune. Retrieved from https://fortune.com/longform/pfizer-drug-problem-fortune-500/ Gognon, M., & Lexchin, J. (2008, January 3). The cost of pushing pills: A new estimate of pharmaceutical promotion expenditures in the United States. PLoS Medicine, 5(1), e1. doi:10.1371/journal.pmed.0050001 Goldman, T. R. (2014, May 1). Health policy brief: Regulating compounding pharmacies. Health Affairs. Retrieved from https://www.healthaffairs.org/do/10.1377/ hpb20140501.628394/full/ Goldstein, J. N., McCrary, M., & Lipska, K. J. (2018). Is the over-the-counter availability of human insulin in the United States good or bad? JAMA Internal Medicine, 178(9), 1157– 1158. doi:10.1001/jamainternmed.2018.3332 Gottlieb, S. (2016). How Obama’s FDA keeps generic drugs off the market. Missouri Medicine, 113(6), 444–445. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC6139764/ IBISWorld. (2019). Medical device manufacturing industry in the U.S.—Market research report. Retrieved from https://www.ibisworld.com/industry-trends/market-research-reports/ manufacturing/computer-electronic-product/medical-device-manufacturing.html Institute of Medicine. (2011). Medical devices and the public’s health: The FDA 510(k) clearance process at 35 years. Retrieved from http://www.nationalacademies.org/hmd/~/media/ Files/Report%20Files/2011/Medical-Devices-and-the-Publics-Health-The-FDA-510k -Clearance-Process-at-35-Years/510k%20Clearance%20Process%202011%20 Report%20Brief.pdf IQVIA Institute. (2017, November 7). The growing value of digital health. Retrieved from https://www.iqvia.com/institute/reports/the-growing-value-of-digital-health IQVIA Institute. (2018, April 19). Medicine use and spending in the U.S.: A review of 2017 and outlook to 2022. Retrieved from https://www.iqvia.com/institute/reports/ medicine-use-and-spending-in-the-us-review-of-2017-outlook-to-2022 IQVIA Institute. (2019). Emerging biopharma’s contribution to innovation. Retrieved from https:// www.iqvia.com/institute/reports/emerging-biopharmas-contribution-to-innovation Kesselheim, A. S., Tan, Y. T., & Avorn, J. (2015). The roles of academia, rare diseases, and repurposing in the development of the most transformative drugs. Health Affairs, 34(2), 1–8. doi:10.1377/hlthaff.2014.1038
Goldsteen74024_04_CH04_125-148_03-18-20.indd 144
3/19/20 3:06 PM
4
■
M e d i c i n e s , D e v i c e s , a n d Te c h n o l o g y
145
Krumholz, H. (2018, May 31). It’s time to get rid of the stethoscope. The Wall Street Journal. Retrieved from https://blogs.wsj.com/experts/2018/05/31/its-time-to-get-rid -of-the-stethoscope/ Lenzer, J., & Brownlee, S. (2019, January 4). The FDA is still letting doctors implant untested devices into our bodies. The Washington Post. Retrieved from https://www.washington post.com/outlook/the-fda-is-still-letting-doctors-implant-untested-devices-into-our -bodies/2019/01/04/d85207ae-0edf-11e9-831f-3aa2c2be4cbd_story.html Medical Economics. (2015, June 22). Prescribing mobile apps: What to consider. Retrieved from https://www.medicaleconomics.com/medical-economics/news/prescribing-mobile -apps-what-consider MedPAC. (2017, June). An overview of the medical device industry. Retrieved from www.MedPAC .gov/docs/default-source/reports/jun17_ch7.pdf Mercer Capital. (2018, April 19). Five trends to watch in the medical device industry in 2018. Retrieved from https://mercercapital.com/insights/5-trends-to-watch-in-the -medical-device-industry-in-2018/ O’Connor, B., Pollner, F., & Fugh-Berman, A. (2016, August 3). Salespeople in the surgical suite: Relationships between surgeons and medical device representatives. PLoS One, 11(8), e0158510. doi:10.1371/journal.pone.0158510 PhRMA. (2015). Biologics: What makes them different? Retrieved from https://www.phrma .org/fact-sheet/biologics-what-makes-them-different PhRMA. (2017). Follow the dollar. Retrieved from http://phrma-docs.phrma.org/files/dmfile/ Follow-the-Dollar-Report.pdf PhRMA. (2018). 2018 biopharmaceutical research industry profile and toolkit. Pharma Logistics. (2018, September 20). The“ABCs”of pharmacy compliance: FDA, DEA and EPA modern healthcare. Retrieved from https://www.modernhealthcare.com/article/20180920/ SPONSORED/180929983/the-abcs-of-pharmacy-compliance-fda-dea-and-epa Prasad, V., & Mailankody, S. (2017). Research and development spending to bring a single cancer drug to market and revenues after approval. JAMA Internal Medicine, 177(11), 1569–1575. doi:10.1001/jamainternmed.2017.3601 Pray, W. S., & Pray, G. E. (2011, September 20). Behind-the-counter products: A third class of drugs. U.S. Pharmacist. Retrieved from https://www.uspharmacist.com/article/ behind-the-counter-products-a-third-class-of-drugs Roehrig, C. (2019). Projections of the prescription drug share of national health expenditures including non-retail. Retrieved from https://altarum.org/sites/default/files/uploadedpublication-files/Projections%20of%20the%20Prescription%20Drug%20Share%20 of%20National%20Health%20Expenditures%20June%202019.pdf Roland, D. (2019, May 7). A $2 million drug is about to hit the market. The Wall Street Journal. Retrieved from https://www.wsj.com/articles/a-2-million-drug-is-about -to-hit-the-market-11557221401 Roy, A. (2019, February 2). Trump’s new pharmacy benefit manager rebate rule will reshape prescription drug prices. Forbes. Retrieved from https://www.forbes.com/sites/theapoth ecary/2019/02/02/trumps-new-pharmacy-benefit-manager-rebate-rule-will-reshape -prescription-drug-prices/#66b05bda40e3
Goldsteen74024_04_CH04_125-148_03-18-20.indd 145
3/19/20 3:06 PM
146
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Sataline, L. (1998, February 23). Vanishing stethoscopes. The New York Times, Section A, p. 18. Retrieved from https://www.nytimes.com/1998/02/23/opinion/l-vanishing-stetho scopes-705659.html Shuren, J., Patel, B., & Gottlieb, S. (2018). FDA regulation of mobile medical apps. JAMA, 320(4), 337–338. doi:10.1001/jama.2018.8832 Sternberg, S. (2015, December 15). Can compounding pharmacies circumvent big pharma? U.S. News & World Report. Retrieved from https://health.usnews.com/ health-news/hospital-of-tomorrow/articles/2015-12-15/can-compounding -pharmacies-circumvent-big-pharma Tallapragada, N. P. (2016). Off-patent drugs at brand-name prices: A puzzle for policymakers. Journal of Law and the Biosciences, 3(1), 238–247. doi:10.1093/jlb/lsw008 U.S. Department of Commerce, International Trade Administration. (2016). 2016 top markets report pharmaceuticals. Retrieved from https://www.trade.gov/topmarkets/pdf/Pharma ceuticals_Executive_Summary.pdf U.S. Department of Justice, Drug Enforcement Administration. (2019a). Part 1306—Prescriptions, controlled substances listed in schedules III, IV, and V, §1306.26 dispensing without prescription. Retrieved from https://www.deadiversion.usdoj.gov/21cfr/cfr/1306/1306_26.htm U.S. Department of Justice, Drug Enforcement Administration. (2019b). Section V—Valid prescription requirements. Retrieved from https://www.deadiversion.usdoj.gov/pubs/manuals /pract/section5.htm U.S. Department of Justice, Drug Enforcement Administration (2019c). Lists of: Scheduling actions, controlled substances, regulated chemicals. Retrieved from https://www.deadiver sion.usdoj.gov/schedules/orangebook/orangebook.pdf U.S. Food and Drug Administration. (2015a). FDA’s drug review process: Continued. Retrieved from https://www.fda.gov/drugs/drug-information-consumers/fdas-drug -review-process-continued U.S. Food and Drug Administration. (2015b). Frequently asked questions about therapeutic biological products. Retrieved from https://www.fda.gov/drugs/therapeutic-biologics -applications-bla/frequently-asked-questions-about-therapeutic-biological-products U.S. Food and Drug Administration. (2016a). How do I know if my product is regulated by FDA? Retrieved from https://www.fda.gov/industry/fda-basics-industry/ how-do-i-know-if-my-product-regulated-fda U.S. Food and Drug Administration. (2016b). Now available without a prescription. Retrieved from https://www.fda.gov/drugs/drug-information-consumers/now-available -without-prescription U.S. Food and Drug Administration. (2016c). Qualifying for pediatric exclusivity under section 505A of the Federal Food, Drug, and Cosmetic Act: Frequently asked questions on pediatric exclusivity (505A). Retrieved from https://www.fda.gov/drugs/development-resources/ qualifying-pediatric-exclusivity-under-section-505a-federal-food-drug-and-cosmetic -act-frequently U.S. Food and Drug Administration. (2016d). Postmarketing surveillance programs. Retrieved from https://www.fda.gov/drugs/surveillance/postmarketing-surveillance-programs U.S. Food and Drug Administration. (2017a). Prescription drugs and over-the-counter (OTC) drugs: Questions and answers. Retrieved from https://www.fda.gov/drugs/questions-answers/ prescription-drugs-and-over-counter-otc-drugs-questions-and-answers
Goldsteen74024_04_CH04_125-148_03-18-20.indd 146
3/19/20 3:06 PM
4
■
M e d i c i n e s , D e v i c e s , a n d Te c h n o l o g y
147
U.S. Food and Drug Administration. (2017b). Therapeutic biologics applications (BLA). Retrieved from https://www.fda.gov/drugs/types-applications/therapeutic-biologics -applications-bla U.S. Food and Drug Administration. (2017c). Biosimilar development, review, and approval. Retrieved from https://www.fda.gov/drugs/biosimilars/biosimilar-development-review -and-approval U.S. Food and Drug Administration. (2018a). What are “Biologics” questions and answers. Retrieved from https://www.fda.gov/about-fda/about-center-biologics-evaluation -and-research-cber/what-are-biologics-questions-and-answers U.S. Food and Drug Administration. (2018b). Frequently asked questions on patents and exclusivity. Retrieved from https://www.fda.gov/drugs/development-approval-process-drugs/ frequently-asked-questions-patents-and-exclusivity U.S. Food and Drug Administration. (2018c). Designating an orphan product: Drugs and biological products. Retrieved from https://www.fda.gov/industry/developing-products -rare-diseases-conditions/designating-orphan-product-drugs-and-biological-products U.S. Food and Drug Administration. (2018d). Facts about the current good manufacturing practices (CGMPs). Retrieved from https://www.fda.gov/drugs/pharmaceutical-quality-resources/ facts-about-current-good-manufacturing-practices-cgmps U.S. Food and Drug Administration. (2018e). Statement from FDA Commissioner Scott Gottlieb, M.D., on the agency’s global efforts to help assure product quality and transparency at foreign drug manufacturing facilities. Retrieved from https://www.fda.gov/news-events/ press-announcements/statement-fda-commissioner-scott-gottlieb-md-agencys -global-efforts-help-assure-product-quality-and U.S. Food and Drug Administration. (2018f). Compounding and the FDA: Questions and answers. Retrieved from https://www.fda.gov/drugs/human-drug-compounding/compounding -and-fda-questions-and-answers U.S. Food and Drug Administration. (2018g). Combination product definition combination product types. Retrieved from https://www.fda.gov/combination-products/about-combination -products/combination-product-definition-combination-product-types U.S. Food and Drug Administration. (2018h). Mobile medical applications. Retrieved from https://www.fda.gov/medical-devices/digital-health/mobile-medical-applications U.S. Food and Drug Administration. (2019a). Biological product definitions. Retrieved from https://www.fda.gov/files/drugs/published/Biological-Product-Definitions.pdf U.S. Food and Drug Administration. (2019b). Overview of FDA and CBER. Retrieved from https://www.fda.gov/media/81631/download U.S. Food and Drug Administration. (2019c). Consumer Product Safety Commission. Retrieved from https://www.accessdata.fda.gov/scripts/cder/training/otc/topic4/topic4/da_01_04 _0150.htm U.S. Food and Drug Administration. (2019d). Regulation overview. Retrieved from https:// www.accessdata.fda.gov/scripts/cder/training/OTC/topic3/topic3/index03.htm U.S. Food and Drug Administration. (2019e). Fact sheet: FDA at a glance. Retrieved from https://www.fda.gov/about-fda/fda-basics/fact-sheet-fda-glance
Goldsteen74024_04_CH04_125-148_03-18-20.indd 147
3/19/20 3:06 PM
148
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
U.S. Food and Drug Administration. (2019f). Unique device identification system (UDI system). Retrieved from https://www.fda.gov/medical-devices/device-advice-comprehensive -regulatory-assistance/unique-device-identification-system-udi-system U.S. Food and Drug Administration. (2019g). Digital health. Retrieved from https://www.fda .gov/medical-devices/digital-health U.S. Government Accountability Office. (2016, December). FDA has improved its foreign drug inspection program, but needs to assess the effectiveness and staffing of its foreign offices. Retrieved from https://www.gao.gov/assets/690/681689.pdf U.S. Government Accountability Office. (2017, December 19). Drug industry: Profits, research and development spending, and merger and acquisition deals. Retrieved from https://www .gao.gov/products/GAO-18-40 Yeh, B. T. (2012). The Controlled Substances Act: Regulatory requirements. Retrieved from https:// fas.org/sgp/crs/misc/RL34635.pdf Zargar, N., & Carr, A. (2018). The regulatory ancestral network of surgical meshes. PLoS One, 13(6), e0197883. doi:10.1371/journal.pone.0197883
Goldsteen74024_04_CH04_125-148_03-18-20.indd 148
3/19/20 3:06 PM
5 Government and the Health Care System
© Cagel Cartoons, Inc. By Cameron Cardow.
LEARNING OBJECTIVES After completing this chapter, students will be able to: • Explain the constitutional basis of government authority in health care in the United States. • Discuss the major health care functions of the federal government. • Identify and explain the roles of the key federal departments and agencies that are involved in the health care system. • Describe the state governments’ role in health care.
Goldsteen74024_05_CH05_149-168_03-18-20.indd 149
3/17/20 2:43 PM
150
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
The U.S. government operates neither the health care delivery system nor the health services financing system in anything close to their entirety. In fact, in the United States, government is less involved with the provision of health care (in contrast to the payment for health services, with which it is heavily involved) than in any other industrialized country in the world. The government’s role in the U.S. health care system has developed and expanded gradually over a long period of time. In his preface to Stern’s (1946) seminal book on governmental medical services in the 1940s, Smillie, one of the first medical sociologists (as was Stern) and a noted public health authority of the day, said: Our forefathers certainly had no concept of responsibility of the Federal Government, nor of the state government, for health protection of the people. This was solely a local governmental responsibility. When Benjamin Franklin wrote “Health is Wealth” in the Farmers’ Almanac, he was saying that health was a commodity to be bought, to be sold, to be conserved, or to be wasted. But he considered that health conservation was the responsibility of the individual, not of government. The local community was responsible only for the protection of its citizens against the hazards of community life. Thus government responsibility for health protection consisted of (a) promotion of sanitation and (b) communicable disease control. The Federal Constitution, as well as the Constitutions of most of the states, contains no reference or intimation of a federal or state function in medical care. The care of the sick poor was a local community responsibility from earliest pioneer days. This activity was assumed first by voluntary philanthropy; later, it was transferred, and became an official governmental obligation. (p. xiii) Nevertheless, the government at all levels—federal, state, and local—now plays a major role in the U.S. health care system. Although it is restricted compared with the governments of other nations, in terms of dollars spent and policies developed, its role looms rather large.
THE CONSTITUTIONAL BASIS OF GOVERNMENTAL AUTHORITY IN HEALTH CARE It is argued that a very significant role for government in health care delivery is justified by the amount of money government spends on it. This says nothing about the calls for major reforms that could be undertaken by no agency other than government that echo down to us from the early 1930s and resonate in many voices today. But such a role has a constitutional basis as well. To understand government operations in the health care delivery system, it is essential to understand the structure of the government itself.1 A basic principle of the U.S. Constitution is that sovereign power is to be shared between the federal and state governments, a principle called federalism. At its heart, the U.S. Constitution is an agreement among the original 13 states to delegate some of their inherent powers to a federal government, on behalf not of themselves as separately sovereign entities, but of, as the preamble to the Constitution says, “the people of the United States.”As part of this agreement, in the 10th Amendment to the Constitution, the states explicitly reserved to themselves the rest of the power: “The powers not delegated to the United States by the Constitution, nor prohibited by it to the states, are reserved to the states respectively, or to the people.” Because it is not explicitly mentioned in the Constitution, among the powers reserved to the states is the “police power.” It is the latter that forms the basis of the states’ role in health (Mustard, 1945, pp. 17–21). As Grad (2005) points out:
Goldsteen74024_05_CH05_149-168_03-18-20.indd 150
3/17/20 2:43 PM
5
■
G o v e r n m e n t a n d t h e H e a l t h C a re S y s t e m
151
In the states, government authority to regulate for the protection of public health and to provide health services is based on the “police power”—that is, the power to provide for the health, safety, and welfare of the people. It is not necessary that this power be expressly stated, because it is a plenary power that every sovereign government has, simply by virtue of being a sovereign government. For purposes of the police power, the state governments—which antedate the federal government—are sovereign governments …. [T]he exercise of the police power is really what government is about. It defines the very purpose of government. (p. 11) Among the states’ other inherent powers are those of delegation of their own authority. The states used this power to create a third tier of government, local government. Most states have delegated some of their own health powers to that tier. The constitutional basis of the federal government’s health authority is found in the powers to tax and spend to provide for the general welfare, and regulate interstate and foreign commerce (see the preamble and Article 1, Section 8 of the Constitution; Grad, 2005, pp. 11–15). The other basic constitutional principle affecting health and health services is“separation of powers.”The Constitution divides the sovereign power of the federal government among three branches of government: executive, legislative, and judicial. Under separation of powers, each branch of the federal government has its own authority and responsibility, spelled out in the Constitution. Furthermore, the Constitution spells out curbs on the powers of each branch, exercised by the other two. This arrangement is called the system of checks and balances. One very important check on the power of both the federal legislative and executive branches,“judicial review”of the constitutionality of their actions, is not found in the Constitution, however. It was established early in the 19th century by the third chief justice of the Supreme Court, John Marshall, and his colleagues on the bench. It has become an accepted part of the U.S. constitutional system only because the other two branches have granted the court that authority in practice and have followed its determinations. In organizing themselves, the state governments have followed fairly closely the tripartite form of government established under the U.S. Constitution, with checks and balances and separation of powers. At the tertiary level of government, the boundaries between the branches at times become blurred, however. For example, in some suburban and rural areas, the local chief executive officer presides over the local legislative body. Nevertheless, in most U.S. jurisdictions, separation of powers is a major principle of government.
THE HEALTH CARE FUNCTIONS OF GOVERNMENT The Legislative Branch At each level of government, federal, state, and local, the three branches of government have responsibility and authority for health and health services. Legislatures create the laws that establish the means to safeguard the public’s health in matters ranging from the assurance of a pure water supply to protecting the health of workers in their places of employment. The legislatures also enact the legal framework within which the health care delivery system functions, determining which individuals and institutions are authorized to deliver what services to which persons under what conditions and requirements. In the past, legislatures have imposed certain requirements for planning and development on the system, although in most jurisdictions that function has been minimized or has disappeared entirely. If the government is to participate in health care financing, directly deliver services, or support research efforts, the legislature must first establish the legal authority for those programs.
Goldsteen74024_05_CH05_149-168_03-18-20.indd 151
3/17/20 2:43 PM
152
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
The Judiciary The judiciary generally supports the work of the other two branches of government. The judicial branches at the three levels of government have important powers relating to health and health services. In the criminal law arena, working in concert with the law enforcement arms of the executive branches under the authority granted to them by their respective legislatures, the judiciary can try apprehended transgressors of the criminal law and determine punishment for those successfully prosecuted. For example, although it is a state legislature that creates the licensing law for physicians and the executive branch that administers it, it is the judicial system that determines the guilt or innocence of a person charged with “practicing medicine without a license.”The criminal justice system also plays a vital role in safeguarding the public’s health. For example, it enforces sanitary protection and pollution control legislation, with criminal sanctions if necessary. In the civil arena, the judicial system handles disputes arising from the provision of health services, for example, through the process of malpractice litigation. The judicial system adjudicates contract cases arising from health care system disputes, such as those between providers or patients, on one side, and a third-party payer on the other. It protects the rights of individuals under the due process and equal protection clauses of the Fifth and 14th Amendments to the Constitution. Together, then, the judicial and executive branches form the civil and criminal justice systems at the federal, state, and local levels.
The Executive Branch In common parlance, the term “government in health care” refers to the executive branch that delivers health care services, drafts and enforces provider/payer regulations, and administers financing programs, not the legislature that creates the programs or regulatory authority, nor the courts that settle disputes arising under the laws and adjudicate violations of them. Therefore, in the remainder of this chapter the term “government” refers to the executive branch of government.
Provision of Personal Health Services At the federal level, personal health services are provided, for the most part, to “categories of persons”: members of the uniformed services and their families, Native Americans, and military veterans, for example. State governments provide personal health services, for the most part, to “persons who have specific diseases,” such as mental illness and tuberculosis. Local governments’ personal health services are “stratified by class.” Generally, they are for the poor. There are occasional overlaps; for example, governments at all levels provide health services for prisoners, one category of person.
Provision of Community Health Services Government at all levels is the major provider of the traditional communitywide public health services, such as pure water supply and sanitary sewage disposal, food and drug inspection and regulation, communicable disease control (e.g., immunization and the control of sexually transmitted diseases), vital statistics, environmental regulation and protection, and public health laboratory work. Certain community health activities are shared with the private sector. For example, in public health education, voluntary agencies such as the American Cancer Society and the
Goldsteen74024_05_CH05_149-168_03-18-20.indd 152
3/17/20 2:43 PM
5
■
G o v e r n m e n t a n d t h e H e a l t h C a re S y s t e m
153
American Heart Association are important participants. Private refuse companies do much of the solid waste collection and, in certain states, supply the water. Private organizations such as the Sierra Club and the Natural Resources Defense Council are active in environmental protection. Private institutions also play a vital role in health sciences education and research.
Health Care Financing As will be described in more detail in Chapter 6, Financing the Health Care System, government participates in the financing system in three ways. First, it pays for the operation of its own programs, both personal and community. It does this directly, for example, through the federal government’s Department of Veterans Affairs (VA) hospital system or a municipal hospital serving primarily the poor. It also does this indirectly, for example, through the federal government’s provision of grants to state governments to help pay for personal care in state mental hospitals and for the operation of the state’s public health agencies at the community level. The states, in turn, indirectly support local governmental public health activities by providing money for that purpose. Second, through grants and contracts to nongovernmental agencies (and, in certain cases, other government agencies), governments support other types of health-related programs, for example, in biomedical research and medical education. Third, and this is by far the major role of government in financing, under such programs as Medicare and Medicaid, governments pay providers for the delivery of care to patients. As will be discussed in greater detail in Chapter 6, federal, state, and local public funds accounted for about 45.2% of national health expenditures (NHE) in 2017, up from 43.4% in 2013, 35.5% in 2000, and 32.6% in 1990. Concomitantly, private business’ contribution to NHE dropped from 24.6% in 1990 to 20.9% in 2013 and 19.9% in 2017. The household contribution declined from 34.9% in 1990 to 28.2% in 2013 to 28% in 2017 (Centers for Medicare & Medicaid Services [CMS], 2017; National Center for Health Statistics [NCHS], 2015, Table 109).
THE FEDERAL GOVERNMENT’S ROLE IN HEALTH CARE Many federal agencies are involved in the health care system in ways big and small, among them provision of patient care, biomedical and health policy research, health workforce training, and financing health care. There is a particularly important role in developing data and methods for evaluating health care, which will be discussed in more detail in Chapter 7, Health Care System Performance. The U.S. Department of Health and Human Services (DHHS) is the most important federal actor in health and health care. There are two other federal agencies with major health services responsibilities: the VA and Department of Defense (DOD). Other federal agencies with significant health-related responsibilities include the Department of Agriculture (USDA; nutrition policy, meat and poultry inspection, food stamps), the Environmental Protection Agency (EPA), and the Department of Labor, which administers the Occupational Safety and Health Act (OSHA).
Department of Health and Human Services The central, though not only, federal agency responsible for health and health care in the United States is the DHHS. Its stated mission is “to enhance and protect the health and well-being of all Americans. We fulfill that mission by providing for effective health and
Goldsteen74024_05_CH05_149-168_03-18-20.indd 153
3/17/20 2:43 PM
154
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
human services and fostering advances in medicine, public health, and social services”(DHHS, 2019a). Through 11 operating divisions, the DHHS administers more than 115 health-related programs in a wide range of areas, including health and biomedical research, epidemiology and surveillance, disease prevention and immunization, food and drug safety, providing access to primary health care for certain populations, and bioterrorism response preparedness (DHHS, 2013). The DHHS directly employed the full-time equivalent (FTE) of approximately 80,027 people in 2018, and had a budget outlay of US$1.131 billion in 2018 (DHHS, 2018). Out of the 11 operating divisions within DHHS, eight are components of the U.S. Public Health Service. There are two staff offices within the Office of the Secretary, which are also designated components of the U.S. Public Health Service and which operate to coordinate the agency’s public health activities: the Office of the Assistant Secretary for Preparedness and Response and the Office of Global Affairs. These operating divisions and staff offices themselves each contain many subagencies and offices, administering hundreds of programs within the DHHS. Table 5.1 lists the DHHS operating divisions and their respective missions (DHHS, 2019b). As Table 5.1 indicates, the scope of activities and services undertaken by the DHHS is vast, and indeed, many of these agencies and offices have their own branches and divisions, each with its own mission and program responsibilities. A comprehensive discussion of the activities and programs of the DHHS agencies is far beyond what can be accomplished here. What follows should not, by any means, be considered an exhaustive description of the agencies discussed, but is rather intended to give an idea of some of the key programs and activities of the DHHS agencies and how they relate to the health care system in the United States. Collectively, the 11 operating divisions of the DHHS carry out a variety of functions: regulation, direct provision of personal and community health services, provision of financial support for a variety of health services through grants and contracts, direct biomedical research, and provision of the principal federal support of biomedical research in nongovernmental agencies. Although all divisions have relevance to the delivery of health care, some have a greater impact. A brief description of these divisions, in alphabetical order, follows.
Agency for Healthcare Research and Quality The Agency for Healthcare Research and Quality (AHRQ)“is the lead federal agency charged with improving the safety and quality of America’s health care system. AHRQ develops the knowledge, tools, and data needed to improve the health care system and help Americans, health care professionals, and policymakers make informed health decisions” (AHRQ, 2019, para 1). AHRQ supports research on health care quality and cost, access to health care, and effectiveness of health care treatments. The agency creates teaching materials and trains professionals to put research into practice. Further, it produces measures, data, and reports for providers, policy makers, and the public to improve of health care systems.
Centers for Disease Control and Prevention The Centers for Disease Control and Prevention (CDC) is the national public health agency primarily responsible for health promotion and disease and injury prevention efforts. Its programs are aimed at preventing and controlling disease and personal injury, directing foreign and interstate quarantine operations, developing programs for health education and health promotion, improving the performance of clinical laboratories, and developing the standards necessary to ensure safe and healthful working conditions for all working people. The CDC has an essential goal “to protect America from health, safety and security threats, both foreign and in the U.S. Whether diseases start at home or abroad, are chronic or acute, curable or preventable, human error or deliberate attack, CDC fights disease and supports communities and citizens to do the same” (CDC, 2019, p. 2).
Goldsteen74024_05_CH05_149-168_03-18-20.indd 154
3/17/20 2:43 PM
5
■
G o v e r n m e n t a n d t h e H e a l t h C a re S y s t e m
155
TABLE 5.1 Department of Health and Human Services Operating Divisions, Including Those Constituting the U.S. Public Health Service U.S. Public Health Service Agency for Healthcare Research and Quality
Mission: to produce evidence to make health care safer, higher quality, more accessible, equitable, and affordable; and to work within the U.S. Department of Health and Human Services and with other partners to make sure that the evidence is understood and used.
Agency for Toxic Substances and Disease Registry (ATSDR)
Mission: ATSDR protects communities from harmful health effects related to exposure to natural and man-made hazardous substances. We do this by responding to environmental health emergencies; investigating emerging environmental health threats; conducting research on the health impacts of hazardous waste sites; and building capabilities of and providing actionable guidance to state and local health partners.
Centers for Disease Control and Prevention
Mission: serves as the national focus for developing and applying disease prevention and control, environmental health, and health promotion and health education activities designed to improve the health of the people of the United States.
Food and Drug Administration (FDA)
Mission: The FDA is responsible for protecting the public health by ensuring the safety, efficacy, and security of human and veterinary drugs, biological products, and medical devices; and by ensuring the safety of our nation’s food supply, cosmetics, and products that emit radiation.
Health Resources and Services Administration
Mission: to improve health outcomes and address health disparities through access to quality services, a skilled health workforce, and innovative, high-value programs.
Indian Health Service
Mission: to raise the physical, mental, social, and spiritual health of American Indians and Alaska Natives to the highest level.
National Institutes of Health
Mission: to seek fundamental knowledge about the nature and behavior of living systems and the application of that knowledge to enhance health, lengthen life, and reduce illness and disability.
Substance Abuse and Mental Health Services Administration
Mission: to reduce the impact of substance abuse and mental illness on America’s communities.
Not U.S. Public Health Service Administration for Children and Families
Mission: to foster health and well-being by providing federal leadership, partnership, and resources for the compassionate and effective delivery of human services.
Administration for Community Living
Mission: to maximize the independence, well-being, and health of older adults, people with disabilities across the life span, and their families and caregivers.
Centers for Medicare & Medicaid Services
Mission: to ensure that the voices and needs of the populations we represent are present as the agency is developing, implementing, and evaluating its programs and policies.
SOURCE: U.S. Department of Health and Human Services. (2019b). HSS organizational chart. Retrieved from https://www.hhs.gov/about/ agencies/orgchart/index.html
The NCHS is a unit within the CDC. As the nation’s principal health statistics agency, the NCHS is a vital source of information about health in the United States. The NCHS compiles statistical information that can guide actions and policies to improve health in the United States. It is a “unique public resource for health information—a critical element of public health and health policy” (NCHS, 2019, p. 1). Through the NCHS, the CDC collects and publishes vital health and health services data that are critical to the health care system. This includes the birth, death, marriage, and divorce (vital) statistics, as well as data about
Goldsteen74024_05_CH05_149-168_03-18-20.indd 155
3/17/20 2:43 PM
156
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
population health, health behavior, and use of health services in the United States. The CDC maintains the nation’s reference laboratories and supports laboratory training programs.
Food and Drug Administration The FDA is responsible for protecting the public health by ensuring the safety, efficacy, and security of human and veterinary drugs, biological products, and medical devices; and by ensuring the safety of our nation’s food supply, cosmetics, and products that emit radiation. Thus, the FDA regulates prescription drugs and over-the-counter (OTC) medications, biological products, and human blood and its derivatives. The focus is on the assurance of the efficacy and safety of a product before marketing and on the assurance of continuing quality after approval. Medical devices are regulated in a similar manner. Radiological equipment is also regulated, the goals being to control radiation exposure to the public as well as to ensure efficacy (FDA, 2019). FDA also has responsibility for: • •
•
Regulating the manufacture, marketing, and distribution of tobacco products to protect the public health and to reduce tobacco use by minors Assisting to hasten innovations that make medical products more effective, safer, and more affordable and assisting the public get the accurate, science-based information they need to use medical products and foods to maintain and improve their health Aiding counterterrorism activities by ensuring food supply security and by fostering medical product developments that respond to deliberate and naturally emerging public health threats
The regulatory programs of the FDA, especially those focusing on the efficacy and safety of drugs and medical devices, are sometimes controversial. Industry spokespeople maintain that the entry of useful drugs to the market is at times unnecessarily delayed by a lengthy and expensive approval process. Supporters of that process recall, for example, the thalidomide disaster.
Health Resources and Services Administration The Health Resources and Services Administration (HRSA) provides health care to people who are geographically isolated and/or economically or medically vulnerable by funding health centers in underserved areas through its Bureau of Primary Health Care. This includes people living with HIV/AIDS, pregnant women, mothers and their families, and those otherwise unable to access high-quality health care. Through its Bureau of Health Workforce, HRSA also supports the training of health professionals and the distribution of providers to underserved areas. Using scholarships, loans, and loan repayment programs for health professionals, HRSA supports efforts to increase the number and diversity of health care professionals caring for the underserved and vulnerable. These include low-income populations, the uninsured, those with limited English proficiency, migrant and seasonal farmworkers, individuals and families experiencing homelessness, and those living in public housing. Millions of Americans obtain health care and other services from HRSA through over 90 programs and more than 3,000 grantees. HRSA highlights are (HRSA, 2019, p. 1): • •
More than 28 million people nationwide receive primary medical, dental, and/or behavioral health care from a HRSA-funded health center. More than half a million people with diagnosed HIV in the United States receive services through the Ryan White HIV/AIDS Program.
Goldsteen74024_05_CH05_149-168_03-18-20.indd 156
3/17/20 2:43 PM
5
• • •
• • • • •
■
G o v e r n m e n t a n d t h e H e a l t h C a re S y s t e m
157
More than 14,900 clinicians from the National Health Service Corps and Nurse Corps provide primary care services, including medical, dental, and mental health. HRSA workforce grants helped prepare more than 400,000 health profession trainees for practicing in primary care, rural, or underserved settings. An estimated 55 million individuals, including pregnant women, infants, children, including children with special health care needs, and their families in the United States benefited from a Title V service. This includes 91% of all pregnant women, 99% of infants, and 54% of children nationwide. Nearly 3.2 million miles in travel for care saved as patients were served More than 36,500 organ transplants were performed in the United States, a new alltime high. More than 6,100 bone marrow and cord blood transplants were performed. Of approximately 2.1 million human exposure calls to Poison Control Centers, 66% were treated at the site of exposure. Approximately 87% of Ryan White HIV/AIDS Program clients are virally suppressed, up from 70% in 2010, and exceeding the most recent national average of 63%.
National Institutes of Health Through its multiple institutes, such as the National Cancer Institute and the National Heart, Lung, and Blood Institute, the National Institutes of Health (NIH) is responsible for supporting and carrying out biomedical research. Its primary focus is basic biomedical research at the organ-system, tissue, cellular, and subcellular levels and expanding the knowledge base in these areas in order to enhance health and health care. The NIH invests nearly $39.2 billion annually in medical research for the American people. More than 80% of the NIH’s funding is awarded through almost 50,000 competitive grants to more than 300,000 researchers at more than 2,500 universities, medical schools, and other research institutions in every state and around the world. About 10% of the NIH’s budget supports projects conducted by nearly 6,000 scientists in its own laboratories, most of which are on the NIH campus in Bethesda, Maryland. (NIH, 2019, p. 1)
Substance Abuse and Mental Health Services Administration The Substance Abuse and Mental Health Services Administration (SAMHSA) is the lead agency within the DHHS to advance the behavioral health of the nation through public health efforts. Congress established the SAMHSA in 1992 to make substance use and mental disorder information, services, and research more accessible. The agency’s vision is “to provide leadership and resources—programs, policies, information and data, funding, and personnel—advance mental and substance use disorder prevention, treatment, and recovery services in order to improve individual, community, and public health” (SAMHSA, 2019). The SAMHSA supports educational programs for the general public and health care providers; improves substance abuse prevention and treatment services through the identification and dissemination of best practices; and conducts surveillance and monitoring of the prevalence and incidence of substance abuse.
Goldsteen74024_05_CH05_149-168_03-18-20.indd 157
3/17/20 2:43 PM
158
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Centers for Medicare & Medicaid Services The CMS administers Medicare, Medicaid, the Children’s Health Insurance Program (CHIP), and the Basic Health Program (BHP). These programs are fundamental to health care coverage for millions of Americans. •
• •
•
Medicare is a health insurance program for: • People age 65 or older, • People under age 65 with certain disabilities, and • People of all ages with end-stage renal disease (permanent kidney failure requiring dialysis or a kidney transplant). Medicaid provides health coverage to low-income people and is one of the largest payers for health care in the United States. It insures the young and old. CHIP provides states with federal matching funds to cover children in families with incomes too high to qualify for Medicaid, but not high enough to afford private health insurance. The BHP is an option for states to provide affordable coverage and better continuity of care for those whose income fluctuates above and below Medicaid and CHIP eligibility levels (CMS, 2019a).
Medicare spending was US$705.9 billion in 2017, or 20% of total NHE. Medicaid spending was US$581.9 billion in 2017, or 17% of total NHE (CMS, 2017). In 2017, the Medicare program served 58.5 million people each month, on average. Most beneficiaries were 65 and older (about 85%). The Medicaid program served over 73 million persons each month, on average, and CHIP enrollment was 6.7 million children (see Table 5.2).
Other Federal Departments Many other federal departments have some health services responsibilities, as previously noted. Several are discussed here.
Department of Veterans Affairs The VA provides many health services to veterans. After active duty military service, the U.S. veteran becomes entitled to a remarkably broad range of health services through a health care subsystem, the precise equivalent of which is not found in any other nation. This fact is doubtless related, on the one hand, to the lack of a national health insurance program for the general population, and on the other, to the political power of the veterans’ organizations. Coverage and access to services is based on factors such as service-connected disabilities and veterans’ income and assets. Certain other groups are covered as well, as are eligible survivors and caregivers. The specific rules covering health care eligibility for the many classes of veterans are complex. As of 2018, the veteran population was estimated at 19.6 million, of which 47.1% were age 65 or older. The total number of veterans enrolled in the VA health care system was 9.17 million (VA, 2019a). The VA is the second largest federal department, with a workforce of over 342,111 employees in 2017 (U.S. Office of Personnel Management, 2018). The VA operates the largest integrated health care delivery system in the United States and provides a wide range of primary and specialized medical care, as well as social services including primary care services, urgent care services, mental health services, geriatrics and extended care services,
Goldsteen74024_05_CH05_149-168_03-18-20.indd 158
3/17/20 2:43 PM
5
■
G o v e r n m e n t a n d t h e H e a l t h C a re S y s t e m
159
TABLE 5.2 Average Monthly Populationsa Served and Projected to Be Served by Medicare, Medicaid, and CHIP, 2017 to 2019 CY 2017
CY 2018b
CY 2019b
Parts A and/or B
58.5
60.0
60.8
Aged
49.7
51.3
52.2
Disabled
8.8
8.7
8.7
Original Medicare enrollment
38.7
38.7
38.2
19.8
21.3
22.7
FY 2017
FY 2018
FY 2019
Total
73.7
74.6
75.8
Aged
5.8
6.0
6.2
Blind/Disabled
10.6
10.7
10.9
Children
28.2
28.5
29.0
15.5
15.8
16.0
Expansion adult
12.2
12.2
12.4
CHIP (Average Monthly)c
6.7
7.0
7.2
Medicare (Average Monthly)
Medicare Advantage and other health plan enrollment c
Medicaid (Average Monthly)
Adults d
a
Populations are in millions and may not add due to rounding. Preliminary and subject to change. c Projected estimates. d Due to the Affordable Care Act’s (ACA) Medicaid expansion. CHIP, Children’s Health Insurance Program. SOURCE: Centers for Medicare & Medicaid Services. (2019b). CMS fast facts. Retrieved from https://www.cms.gov/Research-Statistics -Data-and-Systems/Statistics-Trends-and-Reports/CMS-Fast-Facts/index.html b
women’s health, rehabilitation services, VA care coordination, post deployment health services (PDHS), war-related illness and injury study centers (WRIISC), and pain management and opioid safety (VA, 2019a). Services and benefits are provided through a nationwide network of 1,255 health care facilities, including 170 medical centers and 1,074 outpatient facilities of varying complexity (VA, 2019b). There is a major shift underway from a primary focus on inpatient care to one on outpatient services, health promotion and disease prevention, and easier access to the system. In this regard, the VA is the largest integrated provider of health care education. The VA also trains physician residents and other health care trainees. The VA supports medical research in areas that most impact veterans and their dependents and other beneficiaries (VA, 2019a).
Department of Defense The DOD oversees the health services of the various branches of the military through the Military Health System. Each of the armed forces—the Army, Navy, Air Force, and Marines— has its own network of health facilities and civilian providers: hospitals, clinics, and field posts. All DOD health personnel are members of the military and salaried according to their military ranks (without relation to the specific services they render). The same basic structure prevails in times of war or peace. Health promotion and disease prevention are emphasized and integrated with the delivery of treatment services.
Goldsteen74024_05_CH05_149-168_03-18-20.indd 159
3/17/20 2:43 PM
160
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Through both its own facilities and contracting arrangements with civilian providers, the DOD provides health services to members of the armed forces, their dependents, surviving dependents of service people killed while on active duty, and military retirees and their dependents. Servicemen and women are eligible for retirement benefits after a minimum of 20 years of service. The health services component of that package is paid in addition to the VA benefits for which they may be eligible. There are currently 9.4 million persons covered by the Military Health System—active duty personnel, military retirees, and their families (Military Health System, 2019). An unusual aspect of military medical departments is that they are charged not only with providing a full range of direct health services, but also with providing for the environmental health and protection of their military communities. This unification of administrative responsibility for personal and community preventive and treatment services is rarely found elsewhere in the U.S. health care delivery system.
Department of Agriculture The USDA oversees the Food Safety Inspection Service (FSIS); the Food and Nutrition Service (FNS), which includes the Women, Infants, and Children (WIC) nutritional program and school breakfast and lunch programs, and the food stamp program, which helps poor people to buy food; the Center for Nutrition Policy and Promotion (CNPP), which, in cooperation with the DHHS, periodically issues dietary guidelines for the nation; the Animal and Plant Health Inspection Service (APHIS); and the Rural Utilities Service (RUS), which includes telemedicine programs. The USDA conducts research on the nutrient composition of foods, food consumption, and nutritional requirements. The FSIS and APHIS are operated in cooperation with the FDA (USDA, 2019).
Occupational Safety and Health Administration Focusing on preventive activities in the workplace, the Occupational Safety and Health Administration (OSHA) is part of the Department of Labor. OSHA uses criteria developed by the National Institute for Occupational Safety and Health (NIOSH), part of the CDC, to set national standards for occupational safety and health (Brock & Tyson, 1985). Since 1970, workplace fatalities have been reduced by more than 65% and occupational injury and illness rates have declined by 67%. At the same time, U.S. employment has almost doubled. Worker deaths in America are down—from about 38 worker deaths a day in 1970 to 12 a day in 2013. Worker injuries and illnesses are also down—from 10.9 incidents per 100 workers in 1972 to fewer than 3.3 per 100 in 2013 (OSHA, 2015). The Department of Labor also establishes national standards for workforce regulations, which applies to health care in such areas as minimum wage and overtime (for which health care is sometimes allowed exceptions not available to other industries). The major responsibilities of OSHA are to develop workplace health and safety standards, to enforce and gain compliance with the standards, to engage in education and training, to help the states in occupational safety and health matters (26 states have their own occupational safety and health programs), and to aid business in meeting OSHA requirements (OSHA, 2015). There are a few industries that are not covered by OSHA; for example, the health and safety of miners is the province of the Bureau of Mines in the Department of the Interior.
Environmental Protection Agency The EPA is an independent unit of the federal government created during the Nixon administration that was elevated to cabinet-level status during the Clinton administration (EPA, 2006). It has major responsibilities for the control of air and water quality and pollution,
Goldsteen74024_05_CH05_149-168_03-18-20.indd 160
3/17/20 2:43 PM
5
■
G o v e r n m e n t a n d t h e H e a l t h C a re S y s t e m
161
solid waste disposal, pesticide contamination, radiation hazards, and toxic substances (EPA, 2019). The EPA conducts research on air, water, and land pollution-control technology and the effects of pollution on humans; develops criteria and issues national standards for pollutants; and enforces compliance with these standards.
STATE GOVERNMENT’S ROLE IN HEALTH CARE At the state level, many different agencies and departments are involved in health care. States administer the Medicaid program in each state and provide some financing for low-income health care. Medicaid is often the largest state budget expense. States are often the major provider of mental health care. States have a role in developing and enforcing environmental, housing, and occupational health regulations, as well as insurance regulations. The state public health departments have much responsibility related to health care, including provision of preventive health services and policies. Since state and local governments vary substantially in priorities and resources, they can serve as laboratories for innovation in health care delivery—implementing new ideas on a small scale. A number of states—notably California, New York, Massachusetts, Minnesota, and Oregon—have developed policies that other states and the federal government have emulated.
Health Statistics Among the oldest of public health functions is the collection and analysis of vital and health statistics. Data on births, deaths, marriages, and divorces (the“vital”statistics) and incidence of the several reportable (primarily infectious) diseases are collected by the local health authorities and forwarded to the state level. There they are codified and analyzed, often by various demographic characteristics, such as age, gender, marital status, ethnicity, and geographic location. Each state then forwards its collected data to the NCHS of the CDC for further analysis and publication. Since the 1970s, the health statistics function has been enlarged from a focus on vital statistics and infectious disease. It now includes the social determinants of health and health care services—cost, quality, safety, and equity.
Licensing Licensing is a basic government function in health care. The licensing process for individual practitioners first establishes minimum standards for qualification. It then applies those standards to applicants to determine who may and who may not deliver what kinds of health services. Licensing of health care institutions sets minimum standards for each facility and their personnel as a group, applies the standards, and determines whether the institution may operate. The licensing authority is one of the most significant of the health powers residing with the states. The manner in which it is used is a major determinant of the character of the health care delivery system. The medical licensing system is particularly significant in that regard. Because no one can practice medicine without a license, the system has given physicians tight control over the central product of the health care delivery system, medical services. By exercising this control, physicians have largely determined the structure of the health care delivery system: how it is organized, the types and functions of the institutions, and the powers of the several categories of personnel who work in it. As noted earlier, it is interesting just how much government regulation of the health care system there is in the United States, well beyond that found in other countries. This is precisely because there is no national health system, so in order to provide some modicum of protection to the public in terms of finance and health care quality, the various players must be regulated.
Goldsteen74024_05_CH05_149-168_03-18-20.indd 161
3/17/20 2:43 PM
162
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
LOCAL GOVERNMENT’S ROLE IN HEALTH CARE A local health department (LHD) is a unit of either state or local government focusing exclusively on a “substate” geographic area, usually well-defined and considered by virtually any observer to be “local” in nature—a county, city, town, parish, or village. A current link to descriptions of LHDs nationally, as well as to descriptions of most of the major units, boards, and associations in health care, may be found at www.healthguideusa.org/local_health _departments.htm There is wide variation in the activities and services offered by LHDs (see Table 5.3). The availability of the services varies by the size of the population served. For example, fewer departments serving populations smaller than 25,000 people offer child immunization services, whereas almost all departments serving more than 500,000 people do so. That
TABLE 5.3 Clinical Programs and Services Provided Directly by Local Public Health Departments, 2016 Program/Service
%LHDs
Immunization
Program/Service
%LHDs
Treatment for Communicable Diseases
Program/Service
%LHDs
Other Clinical Services
Adult immunizations
90%
Tuberculosis
79%
Laboratory services
38%
Childhood immunizations
88%
Other STDs
63%
School-based clinics
34%
HIV/AIDS
35%
Oral health
28%
Asthma prevention and/or management
22%
Screening for Diseases/ Conditions Tuberculosis
84%
Maternal and Child Health Services
Other STDs
65%
Women, Infants, and Children
66%
Home health care
20%
HIV/AIDS
62%
Home visits
60%
Correctional health
13%
Blood lead
61%
Family planning
53%
Substance abuse
11%
High blood pressure
54%
Early and periodic screening, diagnosis, and treatment
38%
Comprehensive primary care
11%
Body mass index
53%
Well-child clinics
29%
Behavioral/mental health
10%
Diabetes
34%
Prenatal care
27%
Emergency medical services
Cancer
32%
Obstetrical care
Cardiovascular diseases
25%
4%
8%
LHD, local health department; STD, sexually transmitted disease. NOTE: n = 1,461 to 1.899. SOURCE: Reproduced with permission from the National Association of County and City Health Officials. (2016). 2016 national profile of local health departments. Retrieved from http://nacchoprofilestudy.org/chapter-7/
Goldsteen74024_05_CH05_149-168_03-18-20.indd 162
3/17/20 2:43 PM
5
■
G o v e r n m e n t a n d t h e H e a l t h C a re S y s t e m
163
the LHD does not provide a service either directly or through contract does not necessarily indicate that those services are not publicly available within a jurisdiction. In some cases, another local government agency, a state agency, or a nongovernmental organization (NGO) may provide the service (National Association of County and City Health Officials [NACCHO], 2009, 2010).
Public Health Contributions State and local public health services, and, indeed, federal services, face many problems. The current state of affairs is still best summarized by the Committee on the Future of Public Health, which published its report in 1988 (Institute of Medicine [IOM], 1988): Many of the major improvements in the health of the American people have been accomplished through public health measures …. But the public has come to take the success of public health for granted …. [T]his nation has lost sight of its public health goals and has allowed the system of public health activities to fall into disarray. Public health is what we, as a society, do collectively to assure the conditions in which people can be healthy …. [M]any problems demonstrate the need to protect the nation’s health through effective, organized, and sustained effort by the public sector …. The current state of our abilities for effective public health action … is cause for national concern …. [W]e have slackened our public health vigilance nationally, and the health of the public is unnecessarily threatened as a result …. Successes as great as those of the past are still possible, but not without public concern and concerted action to restore America’s public health capacity. This [report] envisions the future of public health, analyzes the current situation and how it developed, and presents a plan of action that will, in the committee’s judgment, provide a solid foundation for a strong public health capability throughout the nation. (pp. 1–2) The committee’s report is commended to those readers who are concerned with the future of public health in the United States. These observations are certainly still valid.
SUMMARY Although government is heavily involved in health and health care in the United States, its role is limited in order to maintain the public/private character of the health care system. Government provides the legal underpinning for the system through the licensing laws. It regulates the financial workings of the system and its quality of care. It also regulates the causes of potential environmental and occupational hazardous exposures and the possible responses to them. In addition, government is a direct financier and a direct provider of services for certain populations. It is preeminent in community health services and plays an important role in supporting health sciences education and research. Most health care providers of both the individual and corporate variety recognize (often grudgingly) the reality that government is essential in the health care system. As previously noted, they welcome participation in certain critical areas: licensing; care of the mentally ill, the tubercular, and the poor; community health services; health services and basic science research; and workforce education.
Goldsteen74024_05_CH05_149-168_03-18-20.indd 163
3/17/20 2:43 PM
164
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
DATA SOURCES Federal Government Each of the federal departments and agencies involved in health care provides detailed information on its website about its vision, mission, and goals; activities related to achieving its goals and their description; strategic plan; budget, staffing, and leadership; and organizational chart. You can explore each of the federal entities with health care responsibilities, beginning with the DHHS, at: www.hhs.gov
State and Local Governments •
Each state government office related to health care will provide information similar to that provided by the federal departments and agencies.
•
Another source of information about state and local health involvement in health care is the National Association of County and City Health Officials. “NACCHO is the only organization dedicated to serving every local health department in the nation. NACCHO serves 3,000 local health departments and is the leader in providing cutting-edge, skill-building, professional resources and programs, seeking health equity, and supporting effective local public health practice and systems” (NACCHO, 2019, p. 1). The place to begin exploring state and local efforts is: www.naccho.org
•
An additional source of information about state and local health initiatives is the Association of State and Territorial Health Officials (ASTHO). ASTHO is the national nonprofit organization representing public health agencies in the United States, the U.S. Territories, and the District of Columbia, and the over 100,000 public health professionals these agencies employ. ASTHO’s “primary function is to track, evaluate, and advise members on the impact and formation of public or private health policy which may affect them and to provide them with guidance and technical assistance on improving the nation’s health” (ASTHO, 2019, p. 1). Explore ASTHO at: www.astho.org
NOTE 1. The Public Health Law Manual by Grad (2005), Health and the Law by Christoffel (1982), and“The Legal Basis for Public Health”by Richards and Rathbun, Chapter 4 in Scutchfield and Keck’s Principles of Public Health Practice (1996), are valuable guides to the legal basis of governmental activity in health care and to the many legal procedures involved in the enforcement of public health law.
STUDY QUESTIONS 1. How has the U.S. Constitution affected the role of government in the health care system? 2. How would you describe the role of the Department of Health and Human Services in health care in the United States? 3. What are the major health care functions of state governments? 4. Considering the government’s role in the health care system, how would you define the private sector’s role?
Goldsteen74024_05_CH05_149-168_03-18-20.indd 164
3/17/20 2:43 PM
5
■
G o v e r n m e n t a n d t h e H e a l t h C a re S y s t e m
165
REFERENCES Agency for Healthcare Research and Quality. (2019). Agency for Healthcare Research and Quality: A profile. Retrieved from https://www.ahrq.gov/cpi/about/profile/index.html Association of State and Territorial Health Officials. (2019). About us. Retrieved from https:// www.astho.org/About/ Brock, W. E., & Tyson, P. R. (1985). All about OSHA. Washington, DC: U.S. Government Printing Office. Centers for Disease Control and Prevention. (2019). Official mission statements and organization charts. Retrieved from https://www.cdc.gov/maso/officialmissionstatementscharts .html Centers for Medicare & Medicaid Services. (2017). NHE fact sheet: Historical NHE, 2018. Centers for Medicare & Medicaid Services. (2019a). About CMS. Retrieved from https:// www.cms.gov/About-CMS/About-CMS.html Centers for Medicare & Medicaid Services. (2019b). CMS fast facts. Retrieved from https:// www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/ CMS-Fast-Facts/index.html Christoffel, T. (1982). Health and the law. New York, NY: Simon and Schuster. Environmental Protection Agency. (2006). About EPA. Retrieved from https://www.epa.gov/ aboutepa Environmental Protection Agency. (2019). About EPA. Retrieved from https://www.epa.gov/ aboutepa Food and Drug Administration. (2019). What we do. Retrieved from https://www.fda.gov/ about-fda/what-we-do Grad, F. (2005). The public health law manual (3rd ed.). Washington, DC: American Public Health Association. Health Resources and Services Administration. (2019). About HRSA. Retrieved from https:// www.hrsa.gov/about/index.html Institute of Medicine. (1988). The future of public health. Washington, DC: National Academies Press. Military Health System (Health.mil). (2019). About the military health system. Retrieved from https://www.health.mil/About-MHS Mustard, H. S. (1945). Government in public health. New York, NY: Commonwealth Fund. National Association of County and City Health Officials. (2009). 2008 national profile of local health departments. Washington, DC: Author. National Association of County and City Health Officials. (2010). The local health department workforce: Findings from the 2008 national profile of local health departments. Washington, DC: Author. National Association of County and City Health Officials. (2016). 2016 national profile of local health departments. Retrieved from http://nacchoprofilestudy.org/chapter-7/ National Association of County and City Health Officials. (2019). Our mission. Retrieved from https://www.naccho.org/about/our-mission
Goldsteen74024_05_CH05_149-168_03-18-20.indd 165
3/17/20 2:43 PM
166
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
National Center for Health Statistics. (2015). Health, United States, 2014: With special feature on adults aged 55–64 (Table 109). Hyattsville, MD: U.S. Department of Health and Human Services. Retrieved from http://www.cdc.gov/nchs/data/hus/2014/109.pdf National Center for Health Statistics. (2019). About the National Center for Health Statistics. Retrieved from https://www.cdc.gov/nchs/about/index.htm National Institutes of Health. (2019). Budget. Retrieved from https://www.nih.gov/about-nih/ what-we-do/budget Occupational Safety and Health Administration. (2015). Commonly used statistics. Retrieved from https://www.osha.gov/oshstats/commonstats.html Richards, E. P., & Rathbun, K. C. (1996). The legal basis of public health. In F. D. Scutchfield & C. W. Keck (Eds.), Principles of public health practice. Albany, NY: Delmar. Scutchfield, F. D., & Keck, C. W. (Eds.). (1996). Principles of public health practice. Albany, NY: Delmar. Stern, B. J. (1946). Medical services by government: Local, state and federal. New York, NY: Commonwealth Fund. Substance Abuse and Mental Health Services Administration. (2019). Who we are. Retrieved from https://www.samhsa.gov/about-us/who-we-are U.S. Department of Agriculture. (2019). About the U.S. Department of Agriculture. Retrieved from https://www.usda.gov/our-agency/about-usda U.S. Department of Health and Human Services. (2013). HHS programs and services. Retrieved from http://www.hhs.gov/about/programs/index.html U.S. Department of Health and Human Services. (2018). HHS FY 2018 budget in brief. Retrieved from https://www.hhs.gov/about/budget/fy2018/budget-in-brief/index.html U.S. Department of Health and Human Services. (2019a). About HHS. Retrieved from https:// www.hhs.gov/about/index.html U.S. Department of Health and Human Services. (2019b). HSS organizational chart. Retrieved from https://www.hhs.gov/about/agencies/orgchart/index.html U.S. Department of Veterans Affairs. (2019a). VA plans, budget, and performance. Retrieved from https://www.va.gov/performance/ U.S. Department of Veterans Affairs. (2019b). Veterans Health Administration. Retrieved from https://www.va.gov/health/aboutvha.asp U.S. Office of Personnel Management. (2018). Sizing up the executive branch, FY 2017. Retrieved from https://www.opm.gov/policy-data-oversight/data-analysis-documentation/federal -employment-reports/reports-publications/sizing-up-the-executive-branch-2016.pdf
FURTHER READING Assistant Secretary of Defense for Health Affairs. (1990, June). Report on the reorganization of military health care. Washington, DC: Author. Centers for Medicare & Medicaid Services. (2009). NHE data. Retrieved from http://www .cms.gov/NationalHealthExpendData/25_NHE_Fact_Sheet.asp#TopOfPage
Goldsteen74024_05_CH05_149-168_03-18-20.indd 166
3/17/20 2:43 PM
5
■
G o v e r n m e n t a n d t h e H e a l t h C a re S y s t e m
167
Centers for Medicare & Medicaid Services. (2015). NHE fact sheet: Historical NHE, 2018. Retrieved from http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics -Trends-and-Reports/NationalHealthExpendData/NHE-Fact-Sheet.html Dandoy, S. (1996). The state public health department. In F. D. Scutchfield & C. W. Keck (Eds.), Principles of public health practice. Albany, NY: Delmar. Environmental Protection Agency. (1988). Environmental progress and challenges: EPA’s update. Washington, DC: U.S. Government Printing Office. Environmental Protection Agency. (1989). Your guide to the United States Environmental Protection Agency. Washington, DC: EPA Office of Public Affairs. GovTrack.US. (2006). 109th U.S. Congress (2005–2006), S. 1956[109]: ACCESS act. GovTrack.US. (2011). 112th U.S. Congress (2011–2012), H.R. 3214: Food and Drug Administration Mission Reform Act of 2011. Indian Health Service. (2015a). A quick look. Retrieved from http://www.ihs.gov/newsroom/ includes/themes/newihstheme/display_objects/documents/factsheets/QuickLook.pdf Indian Health Service. (2015b). IHS year 2015 profile. Library of Congress. (2006). Food and Drug Administration Safety Act of 2005 (introduced in Senate). Retrieved from http://thomas.loc.gov MacPherson, P. (1996). The FDA just says yes. Hospitals and Health Networks, 70(10), 34–36, 38. Office of the Assistant Secretary of Defense for Health Affairs. (1996). Assistant Secretary of Defense for Health Affairs. Washington, DC: Author. Schmeckebier, L. F. (1923). The public health service. Baltimore, MD: Johns Hopkins University Press. U.S. Department of Agriculture. (2006). An overview. Retrieved from www.usda.gov U.S. Department of Health and Human Services. (2015a). About HHS. Retrieved from http:// www.hhs.gov/about/index.html U.S. Department of Health and Human Services. (2015b). Fiscal year 2016 budget in brief. Retrieved from http://www.hhs.gov/sites/default/files/budget/fy2016/fy-2016-budget -in-brief.pdf U.S. Department of Veterans Affairs. (2015a). FY 2014–2020 strategic plan. U.S. Department of Veterans Affairs. (2015b). National Center for Veterans Analysis and Statistics: Utilization. Retrieved from http://www.va.gov/vetdata/Utilization.asp Wilson, F. A., & Neuhauser, D. (1976). Health services in the United States. Cambridge, MA: Ballinger.
Goldsteen74024_05_CH05_149-168_03-18-20.indd 167
3/17/20 2:43 PM
Goldsteen74024_05_CH05_149-168_03-18-20.indd 168
3/17/20 2:43 PM
6 Financing the Health Care System
© CartoonStock Ltd. By Peter Steiner. www.CartoonStock.com.
LEARNING OBJECTIVES After completing this chapter, students will be able to: • Describe how U.S. health care expenditure as a percentage of gross domestic product (GDP) has changed since 1960. • Describe the differences between National Health Expenditures (NHE), Health Consumption Expenditures (HCE), and Personal Health Care Expenditures (PHCE). • Describe private health insurance and its contribution to paying the NHE and HCE. • Define “out-of-pocket expenditures” and describe the patient’s contribution to paying the NHE and HCE. • Discuss government spending on health care and how its percentage of the NHE has changed since 1960 for Medicare, Medicaid, the Children’s Health Insurance Program (CHIP), and other government-provided health care programs. • Explain the categories on which health care dollars are spent and what percentage is spent on each. • List and explain common modes of payment for health care services. • Discuss the need for third-party payers and their role in the health care system.
Goldsteen74024_06_CH06_169-214_03-18-20.indd 169
3/20/20 3:00 PM
170
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
INTRODUCTION Health care is like no other sector of the economy. In his seminal 1963 article, “Uncertainty and the Welfare Economics of Medical Care,” Kenneth Arrow (1963) identified these differences as uncertainty, asymmetries of information, and nonmarketability of risks inherent in medicine and medical practice. Even after a millennium of observation and study, our knowledge about the human body, disease, and medicine is very much incomplete. In addition, whereas the physician nearly always has more medical knowledge, patients generally know more about their own history, so there is usually a significant information asymmetry between patient and provider. Economists refer to situations in which an individual’s behavior changes when he or she is able to shift the risks of decisions to others as moral hazard (Arrow, 1963). If an accident costs a person US$2,000 but insurance pays US$1,500, the insured person has less incentive to avoid the accident than if the insurance paid only US$500. Although some may argue that this does not apply to one’s health, clearly people who defer medical treatment until they end up in an ED and programs that reward people for preventive and wellness activities are instances of people making decisions that are worse, both financially, and for their health when others bear the risk. Financing health care is a tension among the ethics and values we place on human life, the asymmetries of information, and uncertainty about care wrapped in nonmarketable risks. The implication is that the health care market would collapse if entirely governed by market forces, even though the health care sector exists within a general market economy. At some level, health care competes for resources (e.g., workers, supporting goods and services) against the production of food, the construction of homes, the creation of movies, and the seemingly infinite number of other goods and services that a nation of 300+ million people and associated businesses consume. At some level, providing resources for an additional surgeon to perform cardiac surgeries means that fewer houses can be constructed or that the quality or quantity of food produced will be diminished. Within the health care sector itself, trade-offs are also made: Money spent on an MRI machine is money not spent on additional doctors; money spent on research is money not spent on providing care; and money spent researching one disease is money not spent on another. In response to this, financing health care in the United States is a complex matter of workarounds, redundancies, and contradictions. Furthermore, because the United States lacks a single national health care payment system, how the money is paid to the providers of health care has become very complicated (Igelhart, 1999a), a situation that health care reform policies have not reduced. This chapter describes the basics of health care financing in the United States today: • • • •
How much money is spent on health care What the money is spent on How the money is paid to health care providers Where the money comes from
Source of Information About Health Care Financing Since 1964, the U.S. Department of Health and Human Services (DHHS) has published data annually on total health expenditures for the United States, called the National Health Expenditure Accounts (NHEA). The NHEA are the official estimates of health care spending in the United States. The goal for the NHEA is to measure spending on health care
Goldsteen74024_06_CH06_169-214_03-18-20.indd 170
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
171
consumption and health care investment in the medical sector. The NHEA have the following benefits for understanding the health care sector spending: First, the NHEA are comprehensive because they contain all of the main components of the health care system within a unified mutually exclusive and exhaustive structure. Second, the NHEA are multidimensional, encompassing not only expenditures for medical goods and services, but also the payers that finance these expenditures. Third, the NHEA are consistent because they apply a common set of definitions that allow comparisons among categories and over time. (Centers for Medicare & Medicaid Services [CMS], 2018b) The following terms will be mentioned frequently in our discussion of health care financing: •
•
•
National Health Expenditures (NHE). The NHE includes all health care consumption and investment in medical structures and equipment and noncommercial health services and biomedical research. The NHE includes Health Consumption Expenditures (HCE). The difference between NHE and HCE is the costs of investment in the medical sector. Health Consumption Expenditures. The HCE include all personal health care spending, government administration and net cost of private health insurance, and public health activities. “Government administration and the net cost of health insurance includes the administrative cost of running various government health care programs, and the difference between premiums earned by insurers and the claims or losses incurred for which insurers become liable (the net cost of private health insurance [PHI])” (CMS, 2018b, p. 6). The HCE includes Personal Health Care Expenditures (PHCE). Personal HealthCare (PHC). PHC includes all medical goods and services that are used to diagnose, treat, and prevent health problems in a specific person. “These include hospital care; professional services; other health, residential, and personal care; home health care; nursing care facilities and continuing care retirement communities; and the retail outlet sales of medical products” (CMS, 2018b, p. 6).
HOW MUCH IS SPENT? Health care spending has increased in the United States every year since 1960 in absolute and per capita terms, and, except for slight dips in 2013 and 2017, as a percentage of gross domestic product (GDP).1 In 2017, the NHE were approximately US$3.49 trillion, 17.9% of GDP, and US$10,739 per capita. Spending reached this level after decades of increases. For example, per capita spending on health care—not adjusted for inflation—was US$146 in 1960, compared to US$10,739 in 2017. The Bureau of Labor Statistics (BLS) estimates the buying power of US$146 in 1960 equates to about US$1,207 when adjusted by the Consumer Price Index (CPI; U.S. Department of Labor, BLS, 2019; see Table 6.1 and Figure 6.1). For the typical household, direct and indirect spending on health care—were it to be allocated evenly across the population—would be larger than any other household expense. In 2017, per capita income was US$31,177, median household income was US$57,652, and median rent or owner costs for housing were US$11,784 and US$18,180, respectively. With per capita NHE at US$10,739, health care expenditures would be more than one-third of per capita income. With per-household NHE at around US$29,000, health care expenditures
Goldsteen74024_06_CH06_169-214_03-18-20.indd 171
3/20/20 3:00 PM
172
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 6.1 National Health Expenditures: Aggregate and Per Capita Amounts, Annual Percentage Change, and Percentage Distribution: Selected Calendar Years, 1960 to 2017 Item
1960
1970
1980
1990
2000
2001
2002
2003
2004
2005
2006
Amount in Billions (US$) National Health Expenditures
27.2
74.6
255.3
721.4
1,369.2
1,486.2
1,628.7
1,767.6
1,895.8
2,023.8
2,156.3
24.7
67.0
235.5
674.1
1,285.9
1,398.8
1,531.9
1,663.9
1,784.4
1,904.1
2,031.1
Personal health care
23.3
63.1
217.0
615.3
1,161.5
1,261.4
1,367.1
1,477.2
1,587.5
1,695.7
1,804.3
Government administration and net cost of health insurance
1.1
2.6
12.1
38.7
81.3
90.6
112.6
132.5
142.0
151.1
165.9
Government public health activities
0.4
1.4
6.4
20.0
43.0
46.8
52.2
54.2
54.9
57.3
60.9
2.5
7.5
19.9
47.3
83.3
87.4
96.8
103.7
111.4
119.7
125.2
Health Consumption Expenditures
Investment
Average Annual Percentage Change from Previous Year Shown National Health Expenditures
10.6%
13.1%
10.9%
6.6%
8.5%
9.6%
8.5%
7.3%
6.8%
6.5%
10.5
13.4
11.1
6.7
8.8
9.5
8.6
7.2
6.7
6.7
Personal health care
10.5
13.2
11.0
6.6
8.6
8.4
8.1
7.5
6.8
6.4
Government administration and net cost of health insurance
9.4
16.4
12.4
7.7
11.5
24.2
17.7
7.2
6.4
9.8
Government public health activities
6.4
Health Consumption Expenditures
13.8
16.9
12.0
8.0
8.7
11.6
3.9
1.3
4.2
Investment
11.6
10.2
9.1
5.8
4.9
10.8
7.2
7.4
7.5
4.5
U.S. populationa
1.2
0.9
1.0
1.1
1.0
0.9
0.9
0.9
0.9
1.0
Gross domestic productb
7.1
10.3
7.6
5.6
3.2
3.4
4.8
6.6
6.7
6.0
282
285
287
290
293
295
298
5,218
5,666
6,097
6,479
6,854
7,232
10,252.3
10,581.8
10,936.4
11,458.2
12,213.7
13,036.6
13,814.6
13.4%
14.0%
14.9%
15.4%
15.5%
15.5%
15.6%
Millions U.S. populationa
186
210
230
National Health Expenditures
146
355
1,108
254
Per Capita Amount (US$) 2,843
4,855
Amount in Billions (US$) Gross domestic productb
542.4
1,073.3
2,857.3
5,963.1 Percentage
National Health Expenditures as a Percent of Gross Domestic Product
5.0%
6.9%
8.9%
12.1%
(continued)
Goldsteen74024_06_CH06_169-214_03-18-20.indd 172
3/20/20 3:00 PM
■
6
F i n a n c i n g t h e H e a l t h C a re S y s t e m
173
TABLE 6.1 National Health Expenditures: Aggregate and Per Capita Amounts, Annual Percentage Change, and Percentage Distribution: Selected Calendar Years, 1960 to 2017 (continued) Item
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
Amount in Billions (US$) National Health Expenditures
2,295.4
2,399.3
2,495.6
2,598.6
2,690.6
2,798.0
2,881.8
3,030.9
3,205.9
3,361.1
3,492.1
2,157.0
2,251.3
2,356.6
2,455.9
2,541.3
2,644.9
2,728.6
2,881.1
3,051.5
3,202.9
3,324.5
Personal health care
1,918.4
2,010.7
2,114.6
2,196.1
2,274.1
2,367.4
2,438.0
2,561.5
2,717.8
2,851.9
2,961.0
Government administration and net cost of health insurance
172.6
169.0
167.8
184.2
192.7
200.3
211.6
238.1
250.4
265.4
274.5
Health Consumption Expenditures
Government public health activities Investment
66.0
71.6
74.2
75.7
74.4
77.2
79.1
81.4
83.3
85.6
88.9
138.4
148.0
138.9
142.7
149.4
153.2
153.2
149.9
154.4
158.2
167.6
Average Annual Percentage Change from Previous Year Shown National Health Expenditures
6.5%
4.5%
4.0%
4.1%
3.5%
4.0%
3.0%
5.2%
5.8%
4.8%
3.9%
6.2
4.4
4.7
4.2
3.5
4.1
3.2
5.6
5.9
5.0
3.8
Personal health care
6.3
4.8
5.2
3.9
3.6
4.1
3.0
5.1
6.1
4.9
3.8
Government administration and net cost of health insurance
4.0
−2.1
−0.7
9.8
4.7
3.9
5.6
12.5
5.2
6.0
3.4 3.9
Health Consumption Expenditures
8.3
8.5
3.7
2.0
−1.7
3.7
2.4
3.0
2.3
2.7
Investment
Government public health activities
10.6
6.9
−6.1
2.7
4.7
2.5
0.0
−2.2
3.0
2.4
6.0
U.S. populationa
0.9
0.9
0.9
0.8
0.7
0.8
0.7
0.8
0.7
0.8
0.7
Gross domestic productb
4.6
1.8
−1.8
3.8
3.7
4.2
3.6
4.4
4.0
2.7
4.2
311
313
316
318
320
323
325
8,927
9,129
9,529
10,006
10,410
10,739
16,197.0
16,784.9
17,521.7
18,219.3
18,707.2
19,485.4
17.3%
17.2%
17.3%
17.6%
18.0%
17.9%
Millions U.S. populationa
301
304
306
National Health Expenditures
7,627
7,898
8,144
309
Per Capita Amount (US$) 8,411
8,649
Amount in Billions (US$) Gross domestic productb
14,451.9
14,712.8
14,448.9
14,992.1
15,542.6
Percentage National Health Expenditures as a Percent of Gross Domestic Product
15.9%
16.3%
17.3%
17.3%
17.3%
a
U.S. Bureau of the Census. Census resident-based population less armed forces overseas and population of outlying areas.
b
U.S. Department of Commerce, Bureau of Economic Analysis.
NOTE: Numbers and percentages may not add to totals because of rounding. Dollar amounts shown are in current dollars. Percentage changes are calculated from unrounded data. SOURCE: Centers for Medicare & Medicaid Services. (2018a). National Health Expenditures by type of service and source of funds, CY 1960-2017. Retrieved from https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsHistorical
Goldsteen74024_06_CH06_169-214_03-18-20.indd 173
3/20/20 3:00 PM
174
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
20.0% 18.0% 16.0% 14.0% 12.0% 10.0% 8.0% 6.0% 4.0%
National health expenditures as a percent of gross domestic product
2.0% 0.0% 1950
1960
1970
1980
1990
2000
2010
2020
FIGURE 6.1 National Health Expenditures as a percentage of gross domestic product, 1960 to 2017. Source: Data from Centers for Medicare & Medicaid Services. (2018a). National Health Expenditures by type of service and source of funds, CY 1960–2017. Retrieved from https://www.cms.gov/Research -Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/ NationalHealthAccountsHistorical
would be more than 50% of the median household income (U.S. Census Bureau, 2018). While health care consumption is not uniform across people nor throughout their lives, as will be discussed in the section“Where the Money Goes,”it is clear that the aggregate health care bill—that is, the NHE—is impractically large to allocate evenly across persons or their households. Although health care spending has increased continually since 1960, the increases in spending have not been uniform from year to year. Between 1960 and 1990, the average annual percent changes were double-digit increases except in 1985 to 1987. Beginning in 1991, the annual rate of increase in health care spending began to decline to single digits and continued in single digits through 2017. Actually, from 2008 to 2017, the annual rate of increase each year was below 6%. In 2017, spending grew only 3.9% from the previous year (see Table 6.1). The decline in 1991 corresponds to the advent of managed care and its downward pressure on both physician and hospital usage, which put a brake on health care cost increases, at least for several years. When trying to understand a sector of the economy that represents almost 20% of GDP, it will be helpful to remember the proceeding chapters describing key components of the health care system: health care facilities, workforce, medical supplies and equipment, and leadership and governance. While financing is a building block of the health care system in its own right (World Health Organization [WHO], 2015), it exists to fund the goods and services needed to provide health care. Additionally, the economist’s model of Cost = Price × Quantity can be helpful for analyzing the drivers of costs and their increases. The costs represented in the NHE are the sum of expenditures on billions of services and products consumed over the year at varying prices, but which can be grouped and analyzed across a limited number of categories. Within each category, it can be helpful to examine the quantity consumed, as well as the price paid for those goods or services. High or rising costs may be due to quantity, price, or in some cases, both. Finally, the maxim,“you get what you pay for” should remain an implicit consideration in understanding how different health care entities are currently incentivized, as well as why there are efforts under way to change how these entities are paid. Paying for costs tends
Goldsteen74024_06_CH06_169-214_03-18-20.indd 174
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
175
to produce higher costs. Paying for services tends to produce more services. In reaction to this basic fact, and after years of direct pressure on price and quantity through managed care contracting and utilization management (with much effort and modest success), new approaches to paying for health care are being introduced to focus on value. This change of emphasis and policy has significant implications for how health care is financed and health care providers are paid.
WHERE THE MONEY GOES Economists (and similarly, accountants with their own nomenclature) often separate expenses into current consumption and investment—those expenditures that create value in the future. These are represented in the NHE as HCE and Health Consumption Investments, respectively. As can be seen in Table 6.2, only a small portion of expenditures—ranging between 5% and 10% over the decades—go toward investments, a category comprised of Research and Structures and Equipment. * The vast majority of expenditures are in HCE, and most of these are for PHC, which includes hospitalization, physician services, prescription drugs, and other health care goods and services.† It should be noted that the NHE does not include expenditures for a much broader definition of health care that might include nonmedically supervised dieting and weight loss; health and fitness clubs; sporting goods and related recreation; and healthy foods. Regarding types of expenditures within the NHE, Table 6.2 provides an overview and Figure 6.2 highlights the trends over time. Hospital care accounted for the largest share of NHE, at about 33%, an amount that has remained relatively stable since at least 1960. Professional services had the second highest share of the NHE, at 26%, and most of this amount was for physician services, whose share of the total has also remained relatively constant. Retail prescription drugs accounted for the third highest share and was also a relatively stable expenditure over the past 50-plus years. What has increased as a share of the NHE was other health, residential, and personal care, which includes such services as ambulance providers and care delivered in residential care facilities, as well as nontraditional settings such as community centers and schools; net cost of private health insurance (which includes administrative costs of running plans, dividends, and retained earnings from plan profits/losses); and home health care (see Table 6.2). While they remain a small share of the total NHE, these expenditures have grown significantly, reflecting a policy shift to lower costs by providing health care in facilities outside the hospital (see Chapter 2, The Settings for Health Care Delivery). The increase in these types of expenditures also reflects an increasing use of private health insurance as a source of payment for health care consumption (see Table 6.3). Additionally, the increasing complexity and demands for sophistication and accountability of plans administered by private health insurance have increased over the years (Miller & Luft, 1994). Also, the expenditures for administration—including both government and *
In comparison with discussion of research and development (R&D) for medical products in Chapter 4, Medicines, Devices, and Technology, please note Table 6.2’s footnote “f,” which highlights the exclusion of R&D for medical products from this category (paralleling a general approach to calculating GDP that only counts goods and services in their final use rather than calculating intermediate activities which would double-count overall production). † For those interested, expenditures for complementary and alternative medicine (CAM) are included under other professional services and vitamin and mineral supplements are included under other medical products.
Goldsteen74024_06_CH06_169-214_03-18-20.indd 175
3/20/20 3:00 PM
176
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 6.2 National Health Expenditures; Aggregate, Annual Percentage Change, Percent Distribution, and Per Capita Amounts, by Type of Expenditure: Selected Calendar Years 1960 to 2017 Type of Expenditure
1960
1970
1980
1990
2000
2001
2002
2003
2004
2005
2006
Amount in Billions (US$) National Health Expenditures Health Consumption Expenditures
27.2
74.6
255.3
721.4
1,369.2
1,486.2
1,628.7
1,767.6
1,895.8
2,023.8
2,156.3
24.7
67.0
235.5
674.1
1,285.9
1,398.8
1,531.9
1,663.9
1,784.4
1,904.1
2,031.1
Personal health care
23.3
63.1
217.0
615.3
1,161.5
1,261.4
1,367.1
1,477.2
1,587.5
1,695.7
1,804.3
Hospital care
9.0
27.2
100.5
250.4
415.5
449.4
486.5
525.9
565.3
608.6
651.2
Professional services
7.9
19.8
64.5
207.3
387.0
420.7
454.6
487.1
521.8
553.0
581.8
Physician and clinical services
5.6
14.3
47.7
158.4
288.2
312.7
337.7
364.3
389.4
413.0
434.7
Other professional services
0.4
0.7
3.5
17.3
36.6
40.3
43.3
46.5
50.2
52.8
55.3
2.0
4.7
13.3
31.6
62.1
67.7
73.6
76.3
82.2
87.2
91.8
Other health, residential, and personal carea
Dental services
0.4
1.3
8.4
23.8
63.9
70.0
76.7
82.5
89.3
95.0
101.1
Home health careb
0.1
0.2
2.4
12.5
32.3
34.3
36.5
40.2
44.6
49.3
52.1
Nursing care facilities and continuing care retirement communitiesb,c
0.8
4.0
15.3
44.7
85.0
90.8
94.5
100.1
105.1
111.4
115.9
Retail outlet sales of medical products
5.0
10.6
25.9
76.5
177.8
196.4
218.3
241.4
261.3
278.3
302.3
Prescription drugs
2.7
5.5
12.0
40.3
121.0
139.0
157.9
176.7
192.8
205.2
224.1
Durable medical equipment
0.7
1.7
4.1
13.8
25.2
25.1
27.1
28.5
30.4
32.4
34.4
Other non-durable medical products Government administrationd
1.6
3.3
9.8
22.4
31.6
32.2
33.3
36.2
38.1
40.8
43.7
0.1
0.7
2.8
7.2
17.1
19.6
22.6
25.1
27.1
28.2
28.8 137.2
Net cost of health insurancee
1.0
1.9
9.3
31.6
64.2
71.0
90.0
107.3
114.9
122.9
Government public health activities
0.4
1.4
6.4
20.0
43.0
46.8
52.2
54.2
54.9
57.3
60.9
Investment
2.5
7.5
19.9
47.3
83.3
87.4
96.8
103.7
111.4
119.7
125.2
Researchf
0.7
2.0
5.4
12.7
25.5
28.5
32.0
34.8
38.6
40.3
41.2
Structures and equipment
1.8
5.6
14.4
34.6
57.8
58.9
64.8
68.9
72.8
79.4
84.0
Average Annual Percentage Change from Previous Year Shown National Health Expenditures
10.6%
13.1%
10.9%
6.6%
8.5%
9.6%
8.5%
7.3%
6.8%
6.5%
10.5
13.4
11.1
6.7
8.8
9.5
8.6
7.2
6.7
6.7
Personal health care
10.5
13.2
11.0
6.6
8.6
8.4
8.1
7.5
6.8
6.4
Hospital care
11.7
14.0
9.6
5.2
8.1
8.3
8.1
7.5
7.7
7.0
Professional services
9.6
12.6
12.4
6.4
8.7
8.1
7.1
7.1
6.0
5.2
9.9
12.8
12.7
6.2
8.5
8.0
7.9
6.9
6.1
5.3 4.7
Health Consumption Expenditures
Physician and clinical services Other professional services
6.3
17.0
17.4
7.8
9.9
7.6
7.3
7.9
5.1
Dental services
9.0
11.0
9.0
7.0
9.0
8.8
3.6
7.7
6.1
5.2
Other health, residential, and personal carea
11.5
20.5
11.0
10.4
9.4
9.6
7.6
8.3
6.4
6.4
Home health careb
14.5
26.9
18.1
9.9
6.1
6.4
10.2
11.1
10.5
5.5
Nursing care facilities and continuing care retirement communitiesb,c
17.4
14.2
11.4
6.6
6.7
4.1
5.9
5.0
6.0
4.0
Retail outlet sales of medical products
8.6
7.7
9.4
11.4
8.8
10.5
11.2
10.5
8.3
6.5
Prescription drugs
7.5
8.2
12.8
11.6
14.8
13.6
11.9
9.2
6.4
9.2
Durable medical equipment
9.0
8.8
13.0
6.2
−0.1
7.9
5.1
6.5
6.6
6.3
7.4
11.4
8.6
3.5
2.2
3.2
8.7
5.2
7.1
7.2
Government administrationd
Other nondurable medical products
30.0
14.1
10.0
9.0
14.7
15.1
11.4
7.6
4.3
1.9
Net cost of health insurancee
6.4
17.2
13.0
7.4
10.7
26.7
19.2
7.1
6.9
11.6 (continued)
Goldsteen74024_06_CH06_169-214_03-18-20.indd 176
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
177
TABLE 6.2 National Health Expenditures; Aggregate, Annual Percentage Change, Percent Distribution, and Per Capita Amounts, by Type of Expenditure: Selected Calendar Years 1960 to 2017 (continued) Type of Expenditure
1960
1970
1980
1990
2000
2001
2002
2003
2004
2005
2006
13.8
16.9
12.0
8.0
8.7
11.6
3.9
1.3
4.2
6.4
Investment
11.6
10.2
9.1
5.8
4.9
10.8
7.2
7.4
7.5
4.5
f
Research
10.9
10.8
8.9
7.2
11.9
12.3
8.8
10.7
4.5
2.1
Structures and equipment
11.9
10.0
9.2
5.3
1.8
10.0
6.4
5.7
9.1
5.8
Government public health activities
Percent Distribution National Health Expenditures Health Consumption Expenditures Personal health care
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
90.8
89.9
92.2
93.4
93.9
94.1
94.1
94.1
94.1
94.1
94.2
85.5
84.6
85.0
85.3
84.8
84.9
83.9
83.6
83.7
83.8
83.7
Hospital care
33.0
36.4
39.4
34.7
30.3
30.2
29.9
29.8
29.8
30.1
30.2
Professional services
29.1
26.5
25.3
28.7
28.3
28.3
27.9
27.6
27.5
27.3
27.0
20.4
19.2
18.7
22.0
21.0
21.0
20.7
20.6
20.5
20.4
20.2
Physician and clinical services Other professional services
1.4
1.0
1.4
2.4
2.7
2.7
2.7
2.6
2.6
2.6
2.6
Dental services
7.3
6.3
5.2
4.4
4.5
4.6
4.5
4.3
4.3
4.3
4.3
1.6
1.7
3.3
3.3
4.7
4.7
4.7
4.7
4.7
4.7
4.7
Home health care
0.2
0.3
0.9
1.7
2.4
2.3
2.2
2.3
2.4
2.4
2.4
Nursing care facilities and continuing care retirement communitiesb,c
3.0
5.4
6.0
6.2
6.2
6.1
5.8
5.7
5.5
5.5
5.4
Retail outlet sales of medical products
Other health, residential, and personal carea b
18.5
14.2
10.1
10.6
13.0
13.2
13.4
13.7
13.8
13.8
14.0
Prescription drugs
9.8
7.4
4.7
5.6
8.8
9.4
9.7
10.0
10.2
10.1
10.4
Durable medical equipment
2.7
2.3
1.6
1.9
1.8
1.7
1.7
1.6
1.6
1.6
1.6
6.0
4.5
3.8
3.1
2.3
2.2
2.0
2.0
2.0
2.0
2.0
Government administrationd
Other nondurable medical products
0.2
1.0
1.1
1.0
1.2
1.3
1.4
1.4
1.4
1.4
1.3
Net cost of health insurancee
3.7
2.5
3.6
4.4
4.7
4.8
5.5
6.1
6.1
6.1
6.4
Government public health activities
1.4
1.8
2.5
2.8
3.1
3.1
3.2
3.1
2.9
2.8
2.8
Investment
9.2
10.1
7.8
6.6
6.1
5.9
5.9
5.9
5.9
5.9
5.8
Researchf
2.6
2.6
2.1
1.8
1.9
1.9
2.0
2.0
2.0
2.0
1.9
Structures and equipment
6.7
7.5
5.7
4.8
4.2
4.0
4.0
3.9
3.8
3.9
3.9
a
Includes expenditures for residential care facilities (NAICS 623210 and 623220), ambulance providers (NAICS 621910), medical care delivered in nontraditional settings (such as community centers, senior citizens centers, schools, and military field stations), and expenditures for Home and Community Based Waiver programs under Medicaid. b Includes freestanding facilities only. Additional services of this type provided in hospital-based facilities are counted as hospital care. c Includes care provided in nursing care facilities (NAICS 6231), continuing care retirement communities (623311), state and local government nursing facilities, and nursing facilities operated by the Department of Veterans Affairs. d Includes all administrative costs (federal and state and local employees’ salaries, contracted employees including fiscal intermediaries, rent and building costs, computer systems and programs, other materials and supplies, and other miscellaneous expenses) associated with insuring individuals enrolled in the following health insurance programs: Medicare, Medicaid, Children’s Health Insurance Program, Department of Defense, Department of Veterans Affairs, Indian Health Service, workers’ compensation, maternal and child health, vocational rehabilitation, Substance Abuse and Mental Health Services Administration, and other federal programs. e Net cost of health insurance is calculated as the difference between CY-incurred premiums earned and benefits paid for private health insurance. This includes administrative costs, and, in some cases, additions to reserves, rate credits and dividends, premium taxes, and plan profits or losses. Also included in this category is the difference between premiums earned and benefits paid for the private health insurance companies that insure the enrollees of the following programs: Medicare, Medicaid, Children’s Health Insurance Program, and workers’ compensation (health portion only). f Research and development expenditures of drug companies and other manufacturers and providers of medical equipment and supplies are excluded from “research expenditures” but are included in the expenditure class in which the product falls. NOTE: Numbers may not add to totals due to rounding. Dollar amounts shown are in current dollars. Percent changes and percent distributions are calculated from unrounded data.
(continued)
Goldsteen74024_06_CH06_169-214_03-18-20.indd 177
3/20/20 3:00 PM
178
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 6.2 National Health Expenditures; Aggregate, Annual Percentage Change, Percent Distribution, and Per Capita Amounts, by Type of Expenditure: Selected Calendar Years 1960 to 2017 (continued) Type of Expenditure
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
Amount in Billions (US$) National Health Expenditures Health Consumption Expenditures
2,295.4
2,399.3
2,495.6
2,598.6
2,690.6
2,798.0
2,881.8
3,030.9
3,205.9
3,361.1
3,492.1 3,324.5
2,157.0
2,251.3
2,356.6
2,455.9
2,541.3
2,644.9
2,728.6
2,881.1
3,051.5
3,202.9
Personal health care
1,918.4
2,010.7
2,114.6
2,196.1
2,274.1
2,367.4
2,438.0
2,561.5
2,717.8
2,851.9
2,961.0
Hospital care
691.9
725.6
779.6
822.3
851.9
902.5
937.6
978.2
1,034.5
1,092.8
1,142.6
Professional services
615.3
649.1
667.8
688.3
716.6
743.2
759.4
792.5
838.0
884.0
920.0
Physician and clinical services
457.5
481.9
497.7
512.6
535.9
557.1
569.6
595.7
631.2
666.5
694.3
Other professional services
60.1
64.5
67.0
69.9
72.8
76.4
78.7
83.0
87.8
92.4
96.6
97.7
102.7
103.1
105.9
108.0
109.7
111.1
113.8
118.9
125.1
129.1
Other health, residential, and personal carea
Dental services
108.3
114.5
123.4
129.1
131.7
139.1
144.3
151.5
164.7
173.4
183.1
Home health careb
57.5
62.3
67.7
71.6
74.6
78.3
81.4
84.8
89.2
93.1
97.0
Nursing care facilities and continuing care retirement communitiesb,c
124.9
130.5
135.2
140.5
145.4
147.4
149.0
152.4
158.1
163.0
166.3
Retail outlet sales of medical products
320.5
328.6
340.9
344.3
353.9
356.8
366.3
402.1
433.3
445.6
451.9
Prescription drugs
235.7
241.5
252.7
253.1
258.8
259.2
265.2
297.9
324.5
332.0
333.4
Durable medical equipment
37.1
37.7
37.8
39.9
42.3
43.7
45.1
46.7
48.6
51.0
54.4
47.8
49.5
50.4
51.3
52.9
53.9
56.0
57.5
60.2
62.7
64.1
Government administrationd
Other non-durable medical products
29.2
29.3
29.6
30.2
32.9
34.2
37.4
42.1
42.7
44.7
45.0
Net cost of health insurancee
143.4
139.7
138.2
154.0
159.8
166.1
174.2
196.0
207.7
220.7
229.5
Government public health activities
66.0
71.6
74.2
75.7
74.4
77.2
79.1
81.4
83.3
85.6
88.9
Investment
138.4
148.0
138.9
142.7
149.4
153.2
153.2
149.9
154.4
158.2
167.6
Researchf
42.6
44.3
45.3
49.1
49.6
48.4
46.7
46.0
46.5
47.6
50.7
Structures and equipment
95.8
103.7
93.6
93.5
99.8
104.8
106.5
103.8
107.9
110.6
116.9
Average Annual Percentage Change from Previous Year Shown National Health Expenditures Health Consumption Expenditures Personal health care
6.5%
4.5%
4.0%
4.1%
3.5%
4.0%
3.0%
5.2%
5.8%
4.8%
3.9%
6.2
4.4
4.7
4.2
3.5
4.1
3.2
5.6
5.9
5.0
3.8
6.3
4.8
5.2
3.9
3.6
4.1
3.0
5.1
6.1
4.9
3.8
Hospital care
6.2
4.9
7.4
5.5
3.6
6.0
3.9
4.3
5.8
5.6
4.6
Professional services
5.8
5.5
2.9
3.1
4.1
3.7
2.2
4.4
5.7
5.5
4.1
5.2
5.3
3.3
3.0
4.5
4.0
2.2
4.6
6.0
5.6
4.2
Physician and clinical services Other professional services
8.7
7.4
4.0
4.3
4.2
5.0
3.0
5.4
5.9
5.1
4.6
Dental services
6.5
5.1
0.4
2.7
2.0
1.6
1.2
2.5
4.5
5.2
3.2
7.2
5.7
7.7
4.6
2.0
5.6
3.7
5.0
8.7
5.3
5.6
Other health, residential, and personal carea Home health care
b
10.4
8.5
8.6
5.7
4.2
4.9
3.9
4.2
5.3
4.3
4.3
Nursing care facilities and continuing care retirement communitiesb,c
7.8
4.4
3.6
3.9
3.5
1.4
1.1
2.3
3.8
3.1
2.0
Retail outlet sales of medical products
1.4
6.0
2.5
3.7
1.0
2.8
0.8
2.7
9.8
7.7
2.9
Prescription drugs
5.2
2.5
4.7
0.1
2.2
0.2
2.3
12.4
8.9
2.3
0.4
Durable medical equipment
7.7
1.6
0.4
5.6
5.8
3.4
3.2
3.6
4.1
4.9
6.8
9.2
3.6
1.8
1.8
3.1
2.0
3.9
2.7
4.7
4.1
2.2
Government administrationd
Other nondurable medical products
1.4
0.4
1.2
1.9
9.0
3.9
9.5
12.6
1.4
4.8
0.5
Net cost of health insurancee
4.6
−2.6
−1.1
11.4
3.8
3.9
4.8
12.5
6.0
6.2
4.0 (continued)
Goldsteen74024_06_CH06_169-214_03-18-20.indd 178
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
179
TABLE 6.2 National Health Expenditures; Aggregate, Annual Percentage Change, Percent Distribution, and Per Capita Amounts, by Type of Expenditure: Selected Calendar Years 1960 to 2017 (continued) Type of Expenditure
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
8.3
8.5
3.7
2.0
−1.7
3.7
2.4
3.0
2.3
2.7
3.9
10.6
6.9
−6.1
2.7
4.7
2.5
0.0
−2.2
3.0
2.4
6.0
Research
3.4
4.0
2.4
8.3
0.9
−2.4
−3.5
−1.3
1.1
2.3
6.5
Structures and equipment
14.1
8.3
−9.8
−0.1
6.7
5.0
1.6
−2.5
3.9
2.5
5.7
Government public health activities Investment f
Percent Distribution National Health Expenditures Health Consumption Expenditures Personal health care
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
100.0%
94.0
93.8
94.4
94.5
94.4
94.5
94.7
95.1
95.2
95.3
95.2
83.6
83.8
84.7
84.5
84.5
84.6
84.6
84.5
84.8
84.9
84.8
Hospital care
30.1
30.2
31.2
31.6
31.7
32.3
32.5
32.3
32.3
32.5
32.7
Professional services
26.8
27.1
26.8
26.5
26.6
26.6
26.4
26.1
26.1
26.3
26.3
19.9
20.1
19.9
19.7
19.9
19.9
19.8
19.7
19.7
19.8
19.9
Physician and clinical services Other professional services
2.6
2.7
2.7
2.7
2.7
2.7
2.7
2.7
2.7
2.7
2.8
Dental services
4.3
4.3
4.1
4.1
4.0
3.9
3.9
3.8
3.7
3.7
3.7
4.7
4.8
4.9
5.0
4.9
5.0
5.0
5.0
5.1
5.2
5.2
Home health care
2.5
2.6
2.7
2.8
2.8
2.8
2.8
2.8
2.8
2.8
2.8
Nursing care facilities and continuing care retirement communitiesb,c
5.4
5.4
5.4
5.4
5.4
5.3
5.2
5.0
4.9
4.9
4.8
Retail outlet sales of medical products
12.9
Other health, residential, and personal carea b
14.0
13.7
13.7
13.2
13.2
12.8
12.7
13.3
13.5
13.3
Prescription drugs
10.3
10.1
10.1
9.7
9.6
9.3
9.2
9.8
10.1
9.9
9.5
Durable medical equipment
1.6
1.6
1.5
1.5
1.6
1.6
1.6
1.5
1.5
1.5
1.6
2.1
2.1
2.0
2.0
2.0
1.9
1.9
1.9
1.9
1.9
1.8
Government administrationd
Other nondurable medical products
1.3
1.2
1.2
1.2
1.2
1.2
1.3
1.4
1.3
1.3
1.3
Net cost of health insurancee
6.2
5.8
5.5
5.9
5.9
5.9
6.0
6.5
6.5
6.6
6.6
Government public health activities
2.9
3.0
3.0
2.9
2.8
2.8
2.7
2.7
2.6
2.5
2.5
Investment
6.0
6.2
5.6
5.5
5.6
5.5
5.3
4.9
4.8
4.7
4.8
Researchf
1.9
1.8
1.8
1.9
1.8
1.7
1.6
1.5
1.5
1.4
1.5
Structures and equipment
4.2
4.3
3.8
3.6
3.7
3.7
3.7
3.4
3.4
3.3
3.3
a
Includes expenditures for residential care facilities (NAICS 623210 and 623220), ambulance providers (NAICS 621910), medical care delivered in nontraditional settings (such as community centers, senior citizens centers, schools, and military field stations), and expenditures for Home and Community Based Waiver programs under Medicaid. b Includes freestanding facilities only. Additional services of this type provided in hospital-based facilities are counted as hospital care. c Includes care provided in nursing care facilities (NAICS 6231), continuing care retirement communities (623311), state and local government nursing facilities, and nursing facilities operated by the Department of Veterans Affairs. d Includes all administrative costs (federal and state and local employees’ salaries, contracted employees including fiscal intermediaries, rent and building costs, computer systems and programs, other materials and supplies, and other miscellaneous expenses) associated with insuring individuals enrolled in the following health insurance programs: Medicare, Medicaid, Children’s Health Insurance Program, Department of Defense, Department of Veterans Affairs, Indian Health Service, workers’ compensation, maternal and child health, vocational rehabilitation, Substance Abuse and Mental Health Services Administration, and other federal programs. e Net cost of health insurance is calculated as the difference between CY-incurred premiums earned and benefits paid for private health insurance. This includes administrative costs, and, in some cases, additions to reserves, rate credits and dividends, premium taxes, and plan profits or losses. Also included in this category is the difference between premiums earned and benefits paid for the private health insurance companies that insure the enrollees of the following programs: Medicare, Medicaid, Children’s Health Insurance Program, and workers’ compensation (health portion only). f Research and development expenditures of drug companies and other manufacturers and providers of medical equipment and supplies are excluded from “research expenditures” but are included in the expenditure class in which the product falls. NOTE: Numbers may not add to totals due to rounding. Dollar amounts shown are in current dollars. Percent changes and percent distributions are calculated from unrounded data. SOURCE: Centers for Medicare & Medicaid Services. (2018a). National Health Expenditures by type of service and source of funds, CY 1960-2017. Retrieved from https://www.cms.gov/ Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsHistorical.
Goldsteen74024_06_CH06_169-214_03-18-20.indd 179
3/20/20 3:00 PM
180
I
■
100% 80% 60% 40% 20% 0% 1960
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
1970
1980
1990
2000
2010
Other health, residential, and personal care1
Hospital care
Net cost of health insurance5
Retail prescription drugs
Home health care2
Retail durable medical equipment
Nursing care facilities and continuing care retirement communities2,3 Government public health activities
Research6
Government administration4
2017
Professional services Structures and equipment Retail non-durable medical products
FIGURE 6.2 Share of National Health Expenditure by type of expenditure for selected calendar years 1960 to 2017. Source: Centers for Medicare & Medicaid Services. (2018a). National Health Expenditures by type of service and source of funds, CY 1960–2017. Retrieved from https://www.cms.gov/Research -Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/ NationalHealthAccountsHistorical
private insurance—are relatively high, at 8.3% of the NHE, using the Organisation for Economic Co-operation and Development (OECD) methodology. In comparison, the 10 largest OECD countries, as measured by GDP, had an average administrative cost of 3% in 2017. France had an administrative cost of 5.7%, which places the U.S. cost at 45% higher (OECD, 2019). How are the NHE allocated by health condition and characteristics of patients? Through its Medical Expenditure Panel Survey (MEPS) program, the Agency for Healthcare Research and Quality (AHRQ) maintains the most complete source of data on the cost and use of health care and health insurance coverage.2 Through large-scale surveys of families and individuals, their medical providers (doctors, hospitals, pharmacies, etc.), and employers across the United States, MEPS collects data on the specific health services that Americans use, how frequently they use them, the cost of these services, and how they pay for them, as well as data on the cost, scope, and breadth of health insurance held by and available to U.S. workers. A key difference between the NHE and MEPS data is that the NHEA attempts to capture all health care expenditures in the United States, while the MEPS attempts to provide more granular estimates of the health care utilization and expenditures of noninstitutionalized civilians (Bernard, Cowan, Selden, Lassman, & Catlin, 2018). According to the Centers for Disease Control (CDC, 2019a), “Chronic diseases are defined broadly as conditions that last 1 year or more and require ongoing medical attention or limit activities of daily living or both. Chronic diseases such as heart disease, cancer, and diabetes are the leading causes of death and disability in the United States.” (CDC, 2019a) Additionally, the CDC (2019b) notes that an estimated 90% of the NHE are for chronic and mental health diseases. Chronic conditions are also considered some of the most preventable of all health conditions (CDC, 2016). It should be no surprise, then, that most of the top 10 medical conditions by total expenditures in 2015 were chronic diseases (unfortunately, more recent totals are not available due to the conversion to ICD-10 in 2015). Trauma-related disorders are the notable exception and have the second-highest total expenditures of the conditions ranked. Also, the
Goldsteen74024_06_CH06_169-214_03-18-20.indd 180
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
181
appearance of infectious diseases is notable as an expenditure, for these were barely in the top 20 as of 2012 (AHRQ, 2019; see Table 6.4 and Figure 6.3). MEPS also provides insight into the concentration of health expenditures among noninstitutionalized civilians. As Figures 6.4 and 6.5 show, the lowest 70% of utilizers of health care account for less than 10% of expenditures, while the top 5% accounts for about half of the spending. Most of the services utilized among lowest 70% are ambulatory and dental services, with almost no inpatient hospital stays (Mitchell, 2019). This should not be surprising, as the cost of one hospital stay almost instantly puts a person in the top 50% of expenditures (see Figure 6.6). Finally, MEPS can be used to track persistence of health care utilization over time. In 2013, about 14% of patients who were in the top 1% of utilization were also in the top 1% of utilization for 2012. About 54% of patients who were in the top 20% for 2012 were also in the top 20% for 2013, and just under 75% of patients who were in the top 50% or bottom 50% for 2012 were in the same category for 2013 (see Figure 6.7). The implication is that most people who do not have significant health care usage in one year do not have it in the next, while those who are high utilizers continue to be so. However, about 25% of the population does switch between the bottom 50% and top 50% of utilization from year to year. Additionally, while 14% of patients in the top 1% of health care users in one year will remain in the top 1% the next, the vast majority of the top users are patients who had much lower utilization the previous year (Cohen, 2015b). Many of these outlier situations occur in the last year and even last six months of life, and while much attention has been given to better management of end-of-life care, Emanuel and Emanuel (1994) argue: Cost savings due to changes in practice at the end-of-life are not likely to be substantial. The amount that might be saved by reducing the use of aggressive life-sustaining interventions for dying patients is at most 3.3 percent of total national health care expenditures. (p. 543) They also assert that these savings “would not restrain the rate of growth in health care spending over time. Instead, this amount represents a fraction of the increase due to inflation in health care costs and less than (the amount) needed to cover the uninsured population” (p. 543). Accepting this, we cannot assume that less aggressive care at the end-of-life will solve the financial problems of the health care system. However, better palliative care has been shown to improve the quality of end-of-life care (and, ironically enough, the length of life) and therefore, to be highly worthwhile even if it does not significantly reduce health care expenditures (Cruz-Oliver, 2017).
INSURANCE, INTERMEDIARIES, AND OTHER THIRD PARTIES As noted earlier, whereas a significant number of people retain their health expenditure rank from year to year, a sizable number do not. While most people do not need very much health care in a given year, any significant health care incident is likely to be very expensive. Severe illness can easily cost tens of thousands of dollars, and heroic measures (e.g., trauma and organ transplants) can easily cost in the hundreds of thousands of dollars. Treatment of some rare conditions can even cost in the millions of dollars (Thomas, 2006; Zhang, 2006). A health care condition requiring US$500,000 in treatment would exceed the lifetime income of most people and would be financially devastating for all but a small percentage of the population.
Goldsteen74024_06_CH06_169-214_03-18-20.indd 181
3/20/20 3:00 PM
182
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 6.3 National Health Expenditures; Levels and Annual Percentage Change, by Source of Funds: Selected Calendar Years 1960 to 2017 Item
1960
1970
1980
1990
2000
2001
2002
2003
2004
2005
Amount in Billions (US$) National Health Expenditures Health Consumption Expenditures Out of pocket Health insurance
27.2
74.6
255.3
721.4
1,369.2
1,486.2
1,628.7
1,767.6
1,895.8
2,023.8
24.7
67.0
235.5
674.1
1,285.9
1,398.8
1,531.9
1,663.9
1,784.4
1,904.1
12.9
25.0
58.1
137.9
198.9
206.2
219.3
235.6
248.5
263.8
7.5
31.8
142.3
439.1
919.0
1,014.4
1,121.6
1,221.8
1,320.2
1,414.2
Private health insurance
5.8
15.5
69.2
233.9
458.0
502.0
561.0
615.1
658.3
701.2
Medicare
—
7.7
37.4
110.2
224.8
247.7
265.4
282.7
311.1
339.8
Medicaid
—
5.3
26.0
73.7
200.4
224.1
248.1
269.0
290.7
309.4
—
2.8
14.5
42.6
116.8
132.2
145.3
160.8
172.3
177.5 131.8
Federal State and local Other health insurance programsa Other third-party payers and programs and public health activityb Investment
—
2.4
11.5
31.1
83.5
91.9
102.8
108.2
118.4
1.7
3.3
9.7
21.4
35.8
40.7
47.1
55.0
60.0
63.9
4.3
10.3
35.0
97.1
168.0
178.2
191.1
206.5
215.8
226.1
2.5
7.5
19.9
47.3
83.3
87.4
96.8
103.7
111.4
119.7
Average Annual Percentage Change From Previous Year Shown National Health Expenditures Health Consumption Expenditures Out of pocket Health insurance
10.6%
13.1%
10.9%
6.6%
8.5%
9.6%
8.5%
7.3%
6.8%
10.5
13.4
11.1
6.7
8.8
9.5
8.6
7.2
6.7
6.8
8.8
9.0
3.7
3.7
6.3
7.5
5.5
6.2
15.5
16.2
11.9
7.7
10.4
10.6
8.9
8.0
7.1
10.3
16.1
12.9
7.0
9.6
11.8
9.7
7.0
6.5
Medicare
—
17.2
11.4
7.4
10.2
7.1
6.5
10.1
9.2
Medicaid
6.4
Private health insurance
—
17.3
11.0
10.5
11.9
10.7
8.4
8.1
Federal
—
17.7
11.4
10.6
13.1
9.9
10.7
7.2
3.0
State and local
—
16.7
10.4
10.4
10.0
11.9
5.2
9.5
11.3
7.0
11.4
8.2
5.3
13.6
15.9
16.8
9.0
6.4
9.3
13.0
10.7
5.6
6.1
7.2
8.1
4.5
4.8
11.6
10.2
9.1
5.8
4.9
10.8
7.2
7.4
7.5
Other health insurance programsa Other third-party payers and programs and public health activityb Investment
(continued)
Goldsteen74024_06_CH06_169-214_03-18-20.indd 182
3/20/20 3:00 PM
■
6
F i n a n c i n g t h e H e a l t h C a re S y s t e m
183
TABLE 6.3 National Health Expenditures; Levels and Annual Percentage Change, by Source of Funds: Selected Calendar Years 1960 to 2017 (continued) Item
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
Amount in Billions (US$) National Health Expenditures
2,156.3
2,295.4
2,399.3
2,495.6
2,598.6
2,690.6
2,798.0
2,881.8
3,030.9
3,205.9
3,361.1
3,492.1
2,031.1
2,157.0
2,251.3
2,356.6
2,455.9
2,541.3
2,644.9
2,728.6
2,881.1
3,051.5
3,202.9
3,324.5
Out of pocket
273.2
290.0
295.2
293.8
299.8
310.0
318.8
325.9
330.9
340.9
356.1
365.5
Health insurance
Health Consumption Expenditures
1,517.5
1,609.4
1,696.1
1,796.6
1,877.1
1,950.4
2,023.4
2,088.1
2,229.7
2,382.4
2,504.5
2,604.2
Private health insurance
737.2
776.2
802.9
832.9
864.3
898.5
929.6
947.1
1,000.7
1,069.8
1,136.4
1,183.9
Medicare
403.7
432.8
467.0
498.9
519.8
544.8
568.5
589.9
618.6
649.0
677.1
705.9
Medicaid
306.7
325.9
344.3
374.6
397.4
407.0
422.9
445.2
497.8
542.6
565.6
581.9
Federal
173.9
185.6
203.2
247.4
266.5
247.3
243.4
256.9
305.7
342.6
358.3
361.2
State and local
132.7
140.3
141.2
127.1
130.9
159.7
179.5
188.4
192.1
200.1
207.3
220.6
Other health insurance programsa
70.0
74.6
81.9
90.2
95.6
100.1
102.4
105.9
112.7
121.0
125.3
132.6
Other third-party payers and programs and public health activityb
240.4
257.7
260.0
266.3
279.1
280.9
302.7
314.7
320.4
328.2
342.4
354.8
138.4
148.0
138.9
142.7
149.4
153.2
153.2
149.9
154.4
158.2
167.6
Investment
125.2
Average Annual Percentage Change From Previous Year Shown National Health Expenditures Health Consumption Expenditures Out of pocket Health insurance
6.5%
6.5%
4.5%
4.0%
4.1%
3.5%
4.0%
3.0%
5.2%
5.8%
4.8%
3.9%
6.7
6.2
4.4
4.7
4.2
3.5
4.1
3.2
5.6
5.9
5.0
3.8
3.6
6.1
1.8
−0.5
2.0
3.4
2.8
2.2
1.5
3.0
4.4
2.6
7.3
6.1
5.4
5.9
4.5
3.9
3.7
3.2
6.8
6.8
5.1
4.0
Private health insurance
5.1
5.3
3.4
3.7
3.8
4.0
3.5
1.9
5.7
6.9
6.2
4.2
Medicare
18.8
7.2
7.9
6.8
4.2
4.8
4.3
3.8
4.9
4.9
4.3
4.2
Medicaid
2.9
−0.9
6.3
5.7
8.8
6.1
2.4
3.9
5.3
11.8
9.0
4.2
Federal
−2.0
6.7
9.5
21.8
7.7
−7.2
−1.6
5.5
19.0
12.1
4.6
0.8
State and local
0.7
5.7
0.6
−9.9
3.0
22.0
12.4
4.9
2.0
4.2
3.6
6.4
Other health insurance programsa
9.6
6.6
9.9
10.1
5.9
4.8
2.2
3.4
6.4
7.4
3.5
5.8
Other third-party payers and programs and public health activityb
6.3
7.2
0.9
2.4
4.8
0.6
7.8
4.0
1.8
2.4
4.3
3.6
4.5
10.6
6.9
−6.1
2.7
4.7
2.5
0.0
−2.2
3.0
2.4
6.0
Investment
—, not applicable. Medicare and Medicaid became effective July 1966. a
Includes Children’s Health Insurance Program (Titles XIX and XXI), Department of Defense, and Department of Veterans Affairs.
b
Includes worksite health care, other private revenues, Indian Health Service, workers’ compensation, general assistance, maternal and child health, vocational rehabilitation,
other federal programs, Substance Abuse and Mental Health Services Administration, other state and local programs, and school health. NOTE: Numbers may not add up to totals because of rounding. Dollar amounts shown are in current dollars. Percentage changes are calculated from unrounded data. SOURCE: Centers for Medicare & Medicaid Services. (2018a). National Health Expenditures by type of service and source of funds, CY 1960-2017. Retrieved from https://www.cms .gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsHistorical
Goldsteen74024_06_CH06_169-214_03-18-20.indd 183
3/20/20 3:00 PM
184
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 6.4 Total Expenditures in Millions by Condition, United States, 2011 to 2015 Condition
2011
2012
2013
2014
2015
Heart disease
116,308
100,996
96,454
105,412
113,438
Trauma-related disorders
81,778
92,137
98,109
100,171
102,672
Mental disorders
77,643
83,598
86,070
110,016
98,819
Diabetes mellitus
55,224
59,249
63,069
91,262
89,666
Osteoarthritis and other nontraumatic joint disorders
76,173
73,823
74,401
80,251
81,203
Cancer
88,668
87,538
74,847
87,818
80,249
COPD, asthma
75,183
75,907
71,504
82,392
78,557
Back problems
38,090
41,333
41,455
47,738
56,466
Infectious diseases
26,867
24,381
22,764
40,847
56,031
Hypertension
42,734
47,229
47,455
50,351
52,229
Systemic lupus and connective tissues disorders
36,178
36,458
37,731
38,465
51,110
Other CNS disorders
28,627
37,183
32,148
33,293
40,312
Normal birth/live born
39,381
39,287
44,170
35,557
39,439
Kidney disease
31,989
34,303
38,078
32,625
38,776
Residual codes
24,235
30,075
32,172
31,796
36,710
Hyperlipidemia
38,905
35,148
34,515
36,251
35,259
Skin disorders
23,889
35,589
26,358
25,671
33,225
Pneumonia
15,090
20,022
16,223
17,600
30,512
Other care and screening
15,405
18,234
21,889
22,926
28,515
Cerebrovascular disease
17,529
16,940
18,884
28,365
27,568
CNS, central nervous system; COPD, chronic obstructive pulmonary disease. SOURCE: Center for Financing, Access, and Cost Trends. (1996–2015). Agency for healthcare research and quality, medical expenditure panel survey.
Therefore, most people want some sort of insurance to protect themselves against wild swings in health care costs. As Glied (2001) pointed out, people do not buy health insurance to insure their health, but rather to insure their ability to pay for (and obtain) health care in the event that their health status changes. Thus, health insurers are termed “thirdparty payers”—neither patients nor providers. Historically, health insurance was intended to cover major medical events (Dranove & Millenson, 2006).
Matching Different Provider and Patient Payment Approaches Another motivation for having third-party payers is to bridge the gap between how people want to pay for health care and how providers want to be paid. Although there is little need for a third-party payer in a case where a person wants to pay a fixed monthly amount for
Goldsteen74024_06_CH06_169-214_03-18-20.indd 184
3/20/20 3:00 PM
Total Expenditure by Medical Condition, 2015 (in thousands) $120,000 $100,000 $80,000 $60,000 $40,000 $20,000
m el lit rn us o jo nin tr t d au is m or at de ic rs C an ce C O r PD ,a st hm Ba a ck pr ob In le fe m ct s io us di se as es H yp er te ns io n
rs de is or
es
ld
et ab
en O
st
eo
ar
th
rit
is
Tr
an
au
d
m
ot
he
Di
a-
re
M
la
H
te
ta
d
ea
rt
di
di
so r
se a
de
se
rs
$0
A Prevalence of Top 10 Medical Conditions by Total Expenditures, 2015 (in thousands) 70,000 60,000 50,000 40,000 30,000 20,000 10,000
m el es
ab et
O
st eo
ar th r
iti
s
Tr a
an
d
ot he
Di
M en
rn jo onin tr t d au is m or at de ic rs C an ce C O r PD ,a st hm Ba a ck pr ob In fe le m ct s io us di se as es H yp er te ns io n
lit us
rs or de
ta
ld is
di s
um
a-
re la t
H
ed
ea
rt di s
ea
or de
se
rs
0
B
FIGURE 6.3 Total expenditure by medical condition, 2015. Source: Data from the Center for Financing, Access, and Cost Trends. (1996–2015). Agency for healthcare research and quality, medical expenditure panel survey.
Goldsteen74024_06_CH06_169-214_03-18-20.indd 185
3/20/20 3:00 PM
Mean Expenditures of Top 10 Medical Conditions by Total Expenditure, 2015 $6,000 $5,000 $4,000 $3,000 $2,000 $1,000
es
m el lit rn us o jo nin tr t d au is m or at de ic rs C an ce C O r PD ,a st hm Ba a ck pr ob In fe le m ct s io us di se as es H yp er te ns io n
rs or de is ld ab
et
en ta O
st
eo
ar
th
rit
is
Tr a
an
d
um
ot
he
Di
M
a-
re l
at
H
ed
ea
rt
di
di
se
so rd e
as
e
rs
$0
C
FIGURE 6.3 (continued) 100%
$1,600
$1,400
80%
78.1 $1,200
70%
99% $1,000
60% 50.0
50% 40%
34.0
$800
95% $600
30% $400
17.8
20% 9.8 10% 0% 0%
0.0
0.1
10%
20%
0.4
1.3
2.8
$200
5.3
30% 40% 50% 60% 70% Cumulative percentage of population
Total expenditures (in billions)
Cumulative percentage of expenditures
90%
80%
90%
$0 100%
FIGURE 6.4 Concentration curve of health care expenditures, U.S. civilian noninstitutionalized population, 2016. Source: Mitchell, E. M. (2019). Concentration of health expenditures and selected characteristics of high spenders, U.S. civilian noninstitutionalized population, 2016 (AHRQ Statistical Brief #521). Retrieved from https://meps.ahrq.gov/data_files/publications/st521/stat521.pdf
Goldsteen74024_06_CH06_169-214_03-18-20.indd 186
3/20/20 3:00 PM
Average annual expenditure per person
$120,000
$110,003
$100,000 $80,000 $60,000
$50,077 $33,053
$40,000 $20,000 $5,006 $0
Overall
$15,057
$9,735 $276 Bottom 50%
Top Top Top 50% 30% 10% Percentile of spending distribution
Top 5%
Top 1%
FIGURE 6.5 Mean total expenditure per person by percentile of spending, 2016. Source: Mitchell, E. M. (2019). Concentration of health expenditures and selected characteristics of high spenders, U.S. civilian noninstitutionalized population, 2016 (AHRQ Statistical Brief #521). Retrieved from https://meps.ahrq.gov/data_files/publications/st521/stat521.pdf
100 90 80
8.2 5.4
7.6 5.6
8.5
36.1
40.3
30.2 26.4
25.7
70 Percentage
2.2
3.4
7.6
60 50 37.2
53.8
36.7
40
30.7
28.5
30 20 23.6 10 0
Overall
15.8 Bottom 50%*
23.8
22.2
Top 50%
Top 10%
20.5
Top 5%
Inpatient stays Dental and other Home health Ambulatory events Prescribed medicines
FIGURE 6.6 Type of service distribution by percentile of spending, 2016.‡ ‡
An interesting difference between the expenditures tracked under MEPS and the NHE is that prescribed medicines account for 23.6% of the former (Mitchell, 2019) and less than 10% of the latter. This may be due to measurement differences as well as a bias toward retail prescription usage among noninstitutionalized civilians. The population not sampled by MEPS (institutionalized persons) are unlikely to acquire their prescription drugs through a retail pharmacy. Then, while retail prescription drug costs may be only 10% of NHE, they may be a much larger proportion of the health expenditures of a typical household. *Home health and inpatient stays comprise 0.1% of the bottom 50%. Source: Mitchell, E. M. (2019). Concentration of health expenditures and selected characteristics of high spenders, U.S. civilian noninstitutionalized population, 2016 (AHRQ Statistical Brief #521). Retrieved from https://meps.ahrq.gov/data_files/publications/st521/stat521.pdf
Goldsteen74024_06_CH06_169-214_03-18-20.indd 187
3/20/20 3:00 PM
Percentage of population with same percentile rank in 2013
188
■
I
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
80
73.9
73.1
Top 50%
Lower 50%
63.2 53.8
60 42.7 33.7
40
20
0
14.0
Top 1%
Top 5%
Top 10%
Top 20%
Top 30%
Percentile rank by health care expenditures, 2012
FIGURE 6.7 Persistence in the level of health care expenditures, U.S. civilian noninstitutionalized population, 2012 to 2013. Source: Cohen, S. B. (2015). The concentration and persistence in the level of health expenditures over time: Estimates for the U.S. population, 2012–2013 (Statistical Brief No. 481). Rockville, MD: Agency for Healthcare Research and Quality.
health care to a provider who is paid on a capitation basis and offers the entire range of medical services, historically only a few providers (e.g., Kaiser Permanente) have offered this option. More often, people obtain their health care from a variety of providers that may be operating under different payments, and quite often an individual provider will offer services under multiple and differing charging models. A third-party payer adds value by converting a stream of monthly payments into a stream of service-driven or ailment-driven payments to providers.
Maintaining a Network of Providers Third-party payers typically maintain a network of providers with which they have negotiated contracts. These contracts detail which payment models will be used and what rates will be used, as well as other details common to commercial contracts.
Price and Provider Expertise Additionally, from their network of providers, payers inherently develop extensive databases of their patients’ experience with different providers over time. These databases are a wellspring of information for longitudinal studies and better understanding of treatment options. Third-party payers deal with an array of providers daily. They know the going rate for a wide variety of procedures and consultations across geographic regions and quality tiers. They can conduct quantitative quality studies more easily than any other organization. Therefore, it is third-party payers who have the best chance of predicting which providers will offer a good outcome. Many payers highlight their cost and quality experience with each of the providers in their network through some sort of star rating system, and these have become increasingly
Goldsteen74024_06_CH06_169-214_03-18-20.indd 188
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
189
important for patients as they search for “in-network” providers. While patients historically followed the referrals to specialists and hospitals from the primary care provider or similar, payers’ large databases of claims and outcomes allow them to measure performance more objectively (as will be discussed in Chapter 7, Health Care System Performance).
Provider Payment Approaches In general, there are six payment modes that people and organizations use to buy and sell services. These are: • • • • • •
Cost/cost-plus Hourly or time and materials Fee-for-service Fixed price Capitation Value
We discuss each in relationship to the provision of personal health care services.
Cost/Cost-Plus “Reimbursement” is how hospitals describe payment received for services they have already provided. Under a cost payment method, the organization providing the services tracks all costs associated with each customer and then asks to be paid that amount. This is similar to how an employee might be reimbursed for expenses incurred during a business trip. The employee would offer receipts for plane fare, hotel, food, and other allowable items and then expect to receive exactly that amount in return. An indemnity plan is one under which the covered party is reimbursed for all expenses he or she incurs. An organization is often paid on a cost-plus basis (so-called because a contract specifies that the organization will be reimbursed for actual costs plus an additional percentage of those costs). The cost-plus method provides an additional margin out of which the providing organization can generate profit after any nonproject expenses are paid. In practice, no independent entity can be paid in a cost-only manner. Of course, a profit-generating organization will never survive under a pure cost-only reimbursement model, but even nonprofits need more than cost reimbursement to survive. Under any contract there are nonreimbursable expenses, and every significant organization has expenses that are not specific to one project. The margin allowed on the cost-plus project is what an organization draws from to pay these expenses. Some people like cost-plus contracts because they provide high levels of transparency and seem to limit profits. However, there are drawbacks. These bills are often so detailed that the payer can understand only the bottom line.3 In practice, what is reimbursable, as well as ceilings and thresholds on the amounts, must be set. Accounting for utilization of shares of resources can be complicated, and approaches must be agreed on. In addition, cost-plus contracting does not reward the organization, in this case the health care provider, for either better quality or finding new ways to provide services more cheaply. In a true cost-plus system, the contract penalizes the providing organization for cutting costs.
Time and Materials The hourly payment method, common in service industries, is often referred to as “time and materials.”In this case, a provider would be charged a fixed hourly rate covering all the costs
Goldsteen74024_06_CH06_169-214_03-18-20.indd 189
3/20/20 3:00 PM
190
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
except agreed-on materials, which would be billed as incurred. For example, a residential electrician might pass along all costs for fixtures and breakers and charge US$85 per hour for his time, which then must cover his vehicle, all his tools, any assistants he might employ, and so forth. Time and materials tends to be the system of choice in cases where the scope of work is not clear to either party. Per diem (by the day) reimbursement remains a very common payment method for hospitals (Kaiser Family Foundation, 2002). Although such a system encourages the hospital to work hard to minimize overhead expenses, payers will always worry that the hospital is not looking for ways to increase efficiency.
The fee-for-service method is common when the scope of work is clear to both sides. It is the oldest form of payment for health services and the predominant system of paying physicians, dentists, and private providers in the “other professional services” category of the NHE. For example, a dentist will typically have a set price for a cleaning and checkup. If additional services are needed, those will be performed at essentially published prices. In such a system, the risk of inefficiency is borne by the provider and the risk of bad advice is borne by the customer. Whether a root canal requires 1 or 2 hours to perform and whether or not a root canal is the best use of the patient’s money, the dentist receives the same payment. The local market and the dentist’s reputation drive the rates he or she can charge. According to some observers (Jonas, 1978; Roemer, 1962), in the past, this piecework system was a major cause of many of the observed problems in the health care delivery system. Although the patient’s risk that he or she overpays for a service is reduced, such systems do not reward the provider for better-quality service. Nor do they reward the provider for steering the patient toward more efficient services. A frequent complaint is that preventive medicine is completely ignored (Lown, 1998; Medical Reform Group of Ontario, 1980).
© Randy Glasbergen
Fee-for-Service
Fixed Price A service is called “productized” when it can be marketed or sold as a commodity, which implies that a fixed price will buy a known quantity of that service. Critically, the known quantity is a customer-centric outcome (or in the case of health care, treatment of a disease or condition on a per-episode basis). This can be compared with the provider-centric fee-for-service system, which focuses on what the provider does, whereas a fixed-price, productized approach is nominally focused on the condition presented by the patient. As an example, Medicare (and many other payers) pay hospitals for their patients’ inpatient stays per-discharge based on the Diagnosis Related Group (DRG) assigned to that discharge. Different payers may use a different methodology to assign a DRG (the most common methodologies being the Medicare Severity Diagnosis Related Group [MS-DRG] used by CMS and the All Patient Refined Diagnosis Related Groups [APR-DRG] developed by 3M) and set the prices associated with the DRG. The CMS refers to this as a “prospective payment system” (PPS), since while the rates are set to reimburse providers for their costs,
Goldsteen74024_06_CH06_169-214_03-18-20.indd 190
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
191
they are established prospectively based on the expected utilization of resources for that DRG using an elaborate system of cost reports and historical claims data. The Acute Inpatient PPS was adopted for Medicare by the federal government in 1983 for Medicare Part A benefits (i.e., payments to hospitals) as a way to control costs. It can be seen as forcing productization on the hospitals—at least with respect to the patients covered by Medicare. CMS’s DRG system originally covered only acute care and only the hospital or facility-related charges (Cacace & Schmid, 2009; Mayes, 2006). Hospital outpatient services were moved to a PPS-type system effective August 2000 (Wynn, 2005). Charges from providers received pre- and postdischarge, even if related to the episode of care, have been billed separately. Recently there has been a movement to bundle patient and episode-of-care payments for the most well-understood treatments, such as joint replacements. In such a system the provider is rewarded for how efficiently the patient is treated. Quality is emphasized to the extent that it affects the efficiency of the treatments for the initial diagnosis. The negative side of this type of system is that it intrinsically rewards providers who exaggerate the reported severity of the diagnosis, because disease classification determines the amount of payment that will be received. Since patients are classified by the same organizations that treat them, there can be what is called “up-coding.”Also, providers are rewarded for attracting or seeking healthier patients (who otherwise tend to heal faster than sicker ones) and preventive medicine tends to remain a low priority. Finally, it should be noted that a true fixed price or productized solution would have a set price based solely on achieving the desired outcome, as compared to a fee-for-service system in which the prices for services are set though the services required varies (based on the decisions of medical professions in most cases). The current DRG systems are therefore in between, for while the rate is fixed based on the DRG regardless of the services used in providing care during the inpatient stay, there are different DRGs for different treatments and procedural options, and the DRG is not finalized until the discharge is fully coded. As an example, both the MS-DRG and APR-DRG have different DRGs for vaginal and cesarean delivery (CMS, 2019a; NYS-DOH, 2018a). The authors wonder if the U.S. C-section rate, which is roughly twice the rate that the WHO considers justifiable (Gibbons et al., 2010; NCHS, 2017a) and which some consider epidemic (Lancet, 2018), would trend lower if hospitals received the same rate regardless of the type of delivery.
Capitation Capitation is a fixed prepayment per person to the health care provider for an agreed-on array of services. The payment is the same no matter how many services or what type of services each patient actually gets. In theory, such a system encourages the selection of the least expensive treatments as well as promotes services likely to result in the lowest overall cost during the contract period. However, such a system has no reinforcement for promoting the long-term health of the patient. With capitation, providers are likely to be rewarded for enrolling patients least likely to consume many health services, that is, the healthy. One can also see “global budgeting” (a payment method common to government-run facilities) as a simplified form of capitation—one with only one payer. The provider receives a global budget, which must cover all costs of treatment needed by the eligible population. This is the common way of paying for Veterans Administration (VA) hospitals, state mental hospitals, and local health department clinics. In practice, a global-budget model tends to resemble the cost model, as the budgets are often negotiated starting with the previous year’s cost, and those in operational control are not usually rewarded for coming in under budget. In bureaucracies, coming in under budget is taken as a sign that the budget was set too high.
Goldsteen74024_06_CH06_169-214_03-18-20.indd 191
3/20/20 3:00 PM
192
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Value “Value-based compensation” is the payment model in which the performing organization is rewarded for the value delivered. Value-based systems are most often used when the value is easy to measure and indisputable. For example, personal injury lawyers often offer their services purely for a contingency fee because the value of the lawsuit proceeds is easy to measure. When first referenced in the 6th edition of this book, tying payments to value in health care was almost unheard of. It was only in 2006 that Michael Porter and Elizabeth Teisberg had brought the idea to the forefront in their book,“Redefining Health Care” (Porter & Teisberg, 2006). Nonetheless, initiatives such as MACRA, passed by Congress in 2015 (Shryock, 2019), and the New York State Delivery System Reform Incentive Program (DSRIP), finalized in 2014 after several years of negotiations between the State of New York and CMS, placed strong emphasis on shifting the delivery system to focus and ultimately reward value (NYS-DOH, n.d.). However, as recently as September 2019, it was noted in mainstream press that “Value-based care has created a conundrum: pretty much everyone in healthcare likes the idea of paying for outcomes, but no one is sure how to fairly implement it” (Shryock, 2019). While states like New York are continuing on their journey to a delivery system more focused on value after investing billions of dollars in system transformation, a review of their last roadmap suggests it is not simple and much work remains to be done (NYS-DOH, 2018b).
Risk Transfer and Good Intentions The different payment models can be arranged along a continuum representing the financial risk borne by the buyer and the risk borne by the provider. If the payment model with which the patient pays is different from the payment model under which the provider operates (as is possible in a system with third-party payers such as the current U.S. health system), then the possible combinations can be represented as a matrix (see Figure 6.8).
How provider wants to be paid (Risk from low to high)
How patient wants to pay (Risk from high to low)
Cost/Plus
T&M
FFS
PPS
Capitation
Value
Cost/Plus T&M FFS PPS Capitation Value The system requires a third-party payer. Third-party payer is not required. Not a valid combination.
FIGURE 6.8 Provider and patient risk matrix. T&M Time and Materials; FFS Fee-For-Service; PPS Prospective Payment System.
Goldsteen74024_06_CH06_169-214_03-18-20.indd 192
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
193
With each combination, any risk not borne by the provider or patient is borne by the third-party payer. One could expect a third-party payer to react to this risk by excluding people or conditions, rejecting charges, capping fees, or otherwise capping coverage and raising premiums. On the other hand, even when the payment methods match (e.g., the patient and the provider operate under a fee-for-service contract), either side may wish to use an intermediary. The introduction of health savings accounts (HSAs) created an opening for a different type of institution in health care that starts to resemble something like American Express as opposed to United Health. Initially banks—experts in low-risk, high-volume transactions such as managing payments for product purchases—entered the health care market. However, the regulatory requirements of managing HSAs was sufficiently different than traditional financial services that many traditional financial services firms exited the business over the past few years (Steyer, 2016). It should be noted that how we pay for health care has both short-term and long-term implications. The system of payment affects how the principals act in the system today, but also who and where the principals are tomorrow. There is no shortage of physicians in training who vie for residencies in dermatology or cosmetic surgery, but pediatrics is always in need. A simple capitation system will encourage physicians (and other providers) toward healthier patients. Similarly, a system rewarding outcomes may encourage physicians away from riskier cases. The challenge of rewarding for process consistency is that nearly all best practices are contraindicated in some populations.
WHERE THE MONEY COMES FROM WITHIN THE SYSTEM As Uwe Reinhardt wrote in Priced Out (2019),“Logically it must be true that all spending on the health system in any country originates 100 percent from the budgets of private households.” Nonetheless, as the schematic overview of funds flow in Figure 6.9 illustrates, in the United States the path from people to providers can be complicated. Depending on the person’s situation (e.g., see Reinhardt’s simplified overview of situations in Figure 6.10), the provider, any number of third-party payers that may be involved, the specific contracts that exist among them, and the specific services or care being sought, the cost of health care for that person will be paid by different combinations of them. With the passage of the Patient Protection and Affordable Care Act (ACA), patients typically don’t incur any direct costs at the point-of-care for preventive care services. In such cases, a provider might receive 100% of the payment for such services directly from a managed care plan. Or the provider may bear the incremental expense of providing those services as part of an overall capitation or value-based payment agreement. Even where a provider is paid under a traditional “fee-for-service” arrangement, one or more parties can come together to pay a bill. In such cases, money paid directly by the patient for health care costs is referred to as “out of pocket.”“Charity care” and “forgiven debts” are the terms providers use when they have borne the cost of providing care outside of a capitation or similar value-based payment arrangement. Anyone responsible for payment of a health care cost other than the patient (or the patient’s family) or the provider is a “third-party payer.”Third-party payers include the patient’s or his or her relatives’ employer(s), private insurance companies engaged by the patient or another party, charity organizations, and federal, state, and local governments. To use a typical situation as an example, a child might visit a pediatrician who would then receive a small“copay”from the mother (“out of pocket”) during the visit. Then the pediatrician’s office would bill a private insurance firm, which would pay some or the remainder of
Goldsteen74024_06_CH06_169-214_03-18-20.indd 193
3/20/20 3:00 PM
194
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Payments to providers as per each managed care company, provider, and patient’s product combination
Managed care with sponsorassumed risk
Wage cuts and payroll deductions Employers
Insurance premiums Managed care with risk assumption
Providers of Care
Private Households
Total of actual payments to employees’ provider plus administrative overhead
Government Taxes
Government Programs
Typically budget allocations
Direct payment to providers (e.g., traditional Medicare)
Self-pay and cost-sharing (deductibles, copayments, and coinsurance)
FIGURE 6.9 Funds flow from private households to providers of care. Source: Data from Reinhardt, U. (2019). Priced out: The economic and ethical costs of American health care. Princeton, NJ: Princeton University Press.
the bill. If the pediatrician is not fully reimbursed by the third-party payer, he or she would absorb the unpaid balance as charity care or forgiven debts. Very complicated relationships can enjoin three or more payers.
Private Health Insurance (or Managed Care) The salient feature of private insurance in the United States is that most people obtain it through their employer (or spouse’s or parent’s employer). Additionally, less than 2% of employers in 2017 offered traditional or“indemnity”health insurance plans, which covered 97% of plan participants nationally as of 1980 and 74% as of 1988. In their place, most employers now only offer one or more flavors of managed care plans (Briscoe, 2015; Kaiser Family Foundation, 2017), which includes “health maintenance organizations” (HMO), “preferred provider organizations” (PPO), “point-of-service” (POS), “exclusive provider organizations” (EPO), and perhaps all possible permutations (Fox & Kongstvedt, 2015). The distinguishing feature of managed care is management of the network of providers (Briscoe, 2015) with the implied ability to steer (or limit) members to preferred providers, negotiate rates, and manage utilization. Firms that provide these services (sometimes referred to as health coverage providers) are often referred to as managed care organizations (MCOs) and the largest in 2017 were UnitedHealth Group, with almost 50 million members and just over US$201 billion in revenue; Anthem, with just over 40 million members and about US$90 billion in revenue; and Aetna,§ with just over 22 million members and US$60 billion in revenue (Forbes, 2018). §
Note that Aetna merged with CVS as part of a plan for “transforming the consumer health care experience in America” (www.reuters.com/article/us-aetna-m-a-cvs/u-s-judge-approves-cvs-purchase -of-insurer-aetna-idUSKCN1VP2WO)
Goldsteen74024_06_CH06_169-214_03-18-20.indd 194
3/20/20 3:00 PM
6
The federal– state Medicaid program for certain of the poor, the blind, and the disabled.
SIMPLIFIED The millions of uninsured tend to be near poor.
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
The employed and their families are typically covered through their jobs, although many small employers do not provide coverage.
195
For the rich, “Disneyland” the-sky-is-the-limit policies without rationing of any sort (boutique medicine).
The young Near poor children may be temporarily covered by Medicaid and S-Chip, although 4 million are still uninsured.
Workingage people QUIMBIES SLIMBIES People age 65 and over
The very poor elderly are also covered by Medicaid.
QI2 The poor
The near poor
The broad middle class
The rich
Persons over age 65, who are covered by the federal Medicare program, but not for long-term care. Often the elderly have private supplemental MediGap insurance.
QI1 QDWI
FIGURE 6.10 Simplified categories of people in the U.S. health insurance system. Note: QI1, QI2, QDWI, QUIMBIES, SLIMBIES are the various categories of individuals who, collectively, are known as dual eligibles. Dual eligibles are individuals who are entitled to Medicare Part A and/or Part B and are eligible for some form of Medicaid benefit. Source: Reproduced with permission from Reinhardt, U. (2019). Priced out: The economic and ethical costs of American health care. Princeton, NJ: Princeton University Press.
It should be noted that insurance in the United States is generally governed by the states and this is almost true in health care. Health insurance where the MCO takes on the risk of the contract (i.e., the plan design and rate plans are determined by the MCO) must be approved for sale in each state with the associated regulatory requirements (along with some federal regulatory overlap). Most health insurance sold to individuals and small businesses fall into this category (Fox & Kongstvedt, 2015). Typically, larger employers are “self-insured” such that the employer ultimately pays the actual health care costs incurred by their employees while adhering to national rules governed by the Employee Retirement Income Security Act (ERISA). The employer accepts the financial risk, but contracts with an MCO to administer the plan (Fox & Kongstvedt, 2015). This allows the employer to control the plan design and contract nationally while still gaining the benefits that a third-party intermediary can provide as discussed previously in the section “Insurance, Intermediaries, and Other Third Parties.” Additionally, as the health care costs of their employees become one of their biggest expense, some employers have taken an active role in attempting to drive change in the delivery system as both a cost-savings measure and a benefit to their employees. The Leapfrog Group (2019) was an attempt to do this through coordinated action, while large national employers (e.g., Boeing and Walmart) created their own “centers of excellence programs” to contract and steer their employees to the best providers on a national rather than local basis (Blue Cross Blue Shield of Illinois, 2019; Walmart, 2019). Firms such as Pitney Bowes (2019) have become leaders in employee health and wellness programs.
Goldsteen74024_06_CH06_169-214_03-18-20.indd 195
3/20/20 3:00 PM
196
I
■
100% 80% 60% 40% 20% 0% 1960
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
1980
2000
2002
2004
2006
2008
2010
2012
2014
2016
Out of pocket
Private health insurance
Medicare
Medicaid—federal
Medicaid—state and local
Other health insurance programs1
Other third-party payers and programs and public health activity2
A 60%
50%
40%
30%
20%
10%
0% 1950
B
1960
1970
1980
Out of pocket Medicaid—federal Other third-party payers and programs and public health activity2
1990
2000
2010
2020
Private health insurance Medicaid—state and local Medicare Other health insurance programs1
FIGURE 6.11 Source of funds for Health Consumption Expenditures: selected calendar years 1960 to 2017. Source: National Center for Health Statistics. (2017). National health interview survey: Long-term trends in health insurance coverage, 1968-2017. Retrieved from https://www.cdc.gov/nchs/data/nhis/health _insurance/TrendHealthInsurance1968_2017.pdf
About 66% of people under the age of 65 are covered through private insurance (National Center for Health Statistics [NCHS], 2017b). Private health insurance paid about 36% of HCE in 2017, an amount that has been relatively constant since 1990 (see Table 6.3 and Figure 6.11). Additionally, it has become increasingly common for government programs to contract with an MCO to manage their members and pay providers on their behalf under plans that
Goldsteen74024_06_CH06_169-214_03-18-20.indd 196
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
197
meet minimum coverage requirements. The plans are often similar to individual or employer-sponsored plans (Jacobson, Freed, Damico, & Neuman, 2019), but the premiums are paid by the government agency. While privately administered, the source of funds for these programs is attributed to their government sponsor (e.g., Medicare or Medicaid in Table 6.3 and Figure 6.11). The history of insurance and the rise of managed care plans is discussed further in Chapter 8, Debates That Have Structured Health Care System Change.
Self-Pay and Out-of-Pocket Expenditures Providers often refer to uninsured patients as “self-pay” or “self-insured,” and such patients frequently bear the full cost of their provider’s services. Given the potentially extreme costs of some health care events discussed earlier, uninsured patients may be exposed to severe financial risk as they simultaneously deal with their health care crisis. In many cases, uninsured patients are asked to pay the full “list price” for health care services rather than the negotiated rates that large insurers can typically obtain (as discussed earlier; Martin, Hartman, Washington, Catlin, & The National Health Expenditure Accounts Team, 2018; Singer, Thode, & Pines, 2019). Not surprisingly, then, medical expenses remain a leading cause of bankruptcies in the United States (Himmelstein, Lawless, Thorne, Foohey, & Woolhandler, 2019). About 11% of people under the age of 65 were uninsured in 2017 (NCHS, 2017b). Even if insured, most people are responsible for at least some out-of-pocket expenditures for their health care. There are three kinds of expenses: (a) direct payments to providers for noncovered services; (b) extra payments to providers of insurance-covered services that bill at an amount higher than the insurance company pays for that service; and (c) deductibles and coinsurance required under the health insurance plan (Kaiser Family Foundation, 2017). A deductible is a flat amount; for example, US$200 per individual or US$500 per family that a health care beneficiary must pay out of pocket before the insurance company will begin paying for any health services received during some time period (usually a calendar year). Coinsurance is a share of the cost—for example, 20% of the payment for each service covered by insurance—for which the beneficiary is responsible. All are forms of cost-sharing designed to incentivize patients (or their responsible family member) to manage the cost of care. •
•
Copayments tend to decrease utilization and tiered copayment amounts tend to steer patients toward lower-cost products and services (e.g., it is now common to set the copayment amount for using an ED much higher than an urgent care or physician’s office). Coinsurance tries to steer patients toward providers with lower rates and/or less intense treatment (giving patients some “skin in the game”). Deductibles are common in casualty insurance to minimize claims for minor incidents where the expectation is that adverse events are rare and transaction costs are high. The concept of deductibles was carried through from these plans to managed care, though it is less clear if deductibles are applicable to the goal of managed care to help members better manage their care. About 81% of employer-sponsored plans have a deductible and the average amount across plans is about US$1,500 (Kaiser Family Foundation, 2017).
The ACA of 2010, also known as Obamacare, will be discussed in detail in Chapter 10, History of Change From 1900 to 2010: Comprehensive Reform. However, it can be noted here that the ACA implemented policies regarding deductibles and coinsurance. The average
Goldsteen74024_06_CH06_169-214_03-18-20.indd 197
3/20/20 3:00 PM
198
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
deductible across ACA Silver Plans on the health insurance exchanges created by the ACA was about US$4,000 in 2017 (Goodman, 2018). However, as many studies have found that consumers do not always make the most medically wise decisions about which health care services they should choose (Agarwal, Mazurenko, & Menachemi, 2017; Brook et al., 2006), the ACA also mandated that key preventive services be free to the patient regardless of the structure of copayment, coinsurance, and/or deductibles associated with the health insurance plan (Healthcare.gov, 2019). Overall, patients covered about 11% of HCE in 2017, a rate that remains historically low and has been declining over the decades (see Table 6.3 and Figure 6.11). The rate in 1960, which was prior to the advent of the Medicare and Medicaid programs, was about 52% and even in 1970 was 32%. Only after 2000 did out-of-pocket expenditures fall below 15% of HCE. While the greater than 50% rate for out-of-pocket expenses in 1960 seems impossibly high by current standards, note that per capita health care expenses were much lower then, even adjusting for inflation.
Government Spending on Health Care Government spending has accounted for an increasing proportion of the health care dollar since 1960 (see Table 6.3 and Figure 6.11). At that time, five years before Congress enacted the Medicare and Medicaid programs, the government’s share of HCE was about 23%. By 1970, it was 37% and by 1980 it was almost 42%. In 2017, local, state, and federal programs covered about 49% of national HCE. The vast majority (39%) is through the Medicare and Medicaid programs.
Medicare The first national social insurance program to finance medical care in the United States was established by Congress in 1965 as part of President Lyndon Johnson’s Great Society programs.3 Called “Medicare,” it is authorized by Title XVIII of the Social Security Act (Hoffman, Schoen, Rowland, & Davis 2001; Igelhart, 1999c; Moon, 2001). Originally, it provided payment for some health services for persons 65 years of age and older who were eligible for Social Security or Railroad Retirement benefits, whether they took them or not. In 1973, its coverage was broadened to include those permanently disabled workers and their dependents who were eligible for old age, survivors’ and disability insurance under Social Security, as well as persons with end-stage renal disease. Medicare administrative costs are remarkably low compared to those of the private health insurance sector, ranging from 1% to 2% (Hoffman, Klees, & Curtis, 2000, p. 11). Medicare has four programs: Hospital Insurance (Part A), which also covers skilled nursing facility care on a very limited basis, as well as hospice and home health care; Medical Insurance (Part B), which covers physician and certain other health professional services, hospital outpatient care, and certain other services; Medicare Advantage (Part C) in which members enroll with a plan administered by an MCO instead of Part A and B and optionally Part D; and Medicare Prescription Drug Coverage (Part D), which was designed to lower the costs of prescription medication for Medicare beneficiaries. Medicare Part A and Part B are called Original Medicare. Medicare Part A is funded primarily from Social Security taxes, whereas about two-thirds of Part B is funded from general revenues, with the balance coming from enrollee premium payments. Managed care plans sponsored under Medicare Advantage are sometimes referred to as “Managed Medicare” (CMS, 2019b). Medicare Part D, which was part of the Medicare Prescription Drug Improvement and Modernization Act (MMA) of 2003, began on Jan. 1, 2006, and provides eligible patients with prescription drug benefits designed to reduce the cost of medications. Stand-alone prescription drug plans (PDPs) may be purchased to complement those with Part A and B or
Goldsteen74024_06_CH06_169-214_03-18-20.indd 198
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
199
C coverage, or enrollees may choose a comprehensive Part C plan that covers Parts A, B, and D. Similar to Part B, the cost of the program is paid out of a combination of general revenues and enrollee premiums. Medicare was the source of funds for 21% of HCE or about US$706 billion in 2017 (see Table 6.3) and is the largest single payer for most providers if not the majority. Implicit in this is a substantial influence over the market and the ability to introduce plan participation requirements that other payers would be challenged to dictate to provide on a large scale. Estimated average cost per enrollee in Medicare was just over US$12,300 in 2017, the most of any of the major classes of payer.
Medicaid Along with Medicare, Congress created the Medicaid program in 1965, authorized by Title XIX of the Social Security Act (Hoffman et al., 2001; Igelhart, 1999b; Rosenbaum, 2002). Medicaid is a needs-based program that provides coverage for some health services for some of the poor on a means-tested basis. Therefore, to receive Medicaid coverage, unlike Medicare coverage, a person must apply for it. Also, in contrast to Medicare, the Medicaid program then applies a series of income-level determinations to each applicant, thus “testing their means.” Only those persons whose incomes and other assets fall below a certain level as specified by law or regulation (varying from state to state) are declared eligible for coverage. Medicaid covers people of all ages. In 2018, 77% of Medicaid enrollees were nonelderly adults and children, while 23% were disabled and elderly adults. Expenditures for these groups are reversed, with nonelderly adults and children accounting for 39% of Medicaid expenditures, and disabled and elderly adults accounting for 61% of Medicaid spending. Also, it should be noted that the ACA provided funds to states to expand Medicaid, and that expansion helped to reduce the number of uninsured in the 36 states that adopted expansion—from 13% in 2013 to 9% in 2016 (Kaiser Family Foundation, 2018). Medicaid is supported by federal and state tax levy funds and is administered by the states. Each state program is distinct and unique. Therefore, benefits and coverage vary widely from state to state. While states’ Medicaid programs historically paid providers on a fee-for-service basis,“Managed Medicaid” was introduced in the mid-1990s, and like Managed Medicare, allowed (or required) that beneficiaries obtain their coverage through private MCO who then collected premiums from the state. Each year the proportion of fee-for-service beneficiaries has been declining (CBO, 2018). Title XIX, as amended, requires a state to provide a set of 14 services in order to be eligible to receive federal funds for its program, with a very complicated set of requirements governing just who may be considered eligible for Medicaid and who may not. The 1996 Welfare Reform Act has had a major impact on Medicaid because of its elimination of the Aid to Families with Dependent Children (AFDC) program, the principal welfare program in the United States since the time of the New Deal. A combination of low-income eligibility requirements and low fees paid to providers (many of whom have therefore chosen not to participate) has led to very limited coverage in many states. A few of the wealthier states now provide Medicaid coverage for the“medically indigent.” These are persons in an income range deemed not to be low enough to qualify them by income, but low enough to make paying for health services a heavy burden. Medicaid programs totaled about 18% of HCE, or US$582 billion, in 2017 and about 62% of that came from the federal government, with the rest split among the 50 states. In 2017, the estimated average insurance cost per enrollee (i.e., excluding out-of-pocket expenses) was just over US$8,000 (see Table 6.5), though the average for each state varies considerably by each state’s rules. In 2014, average Medicaid spending per enrollee (full or partial benefit)
Goldsteen74024_06_CH06_169-214_03-18-20.indd 199
3/20/20 3:00 PM
200
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 6.5 Expenditures, Enrollment, and Per-Enrollee Expenditures on Health Insurance for Calendar Years 1987 to 2017 1987
1988
1989
1990
1991
1992
Expenditures
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
Amount in Billions (US$)
Total Private Health Insurance
149.2
175.8
204.8
233.9
255.1
274.7
295.3
308.2
325.3
343.7
359.6
384.7
417.1
458.0
502.0
561.0
Employer-sponsored private health insurance expenditures
127.2
151.6
178.8
205.4
224.2
241.5
258.2
269.7
288.5
308.2
323.9
346.7
376.1
414.6
455.5
507.5
11.5
13.1
14.0
15.7
17.0
18.3
20.1
20.7
20.8
20.7
21.7
22.4
24.1
25.8
27.3
30.5
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
— 11.8
Direct purchase Marketplace Medigap
—
—
—
—
—
—
—
—
—
—
—
—
—
—
11.2
Other direct purchase
—
—
—
—
—
—
—
—
—
—
—
—
—
—
16.1
18.7
Medicare
83.1
89.0
101.1
110.2
120.6
136.0
150.0
167.7
184.4
198.7
210.4
209.4
213.2
224.8
247.7
265.4
Medicaid
50.3
55.1
62.0
73.7
93.2
108.2
122.4
134.4
144.9
152.2
160.8
169.0
183.5
200.4
224.1
248.1
—
—
—
—
—
—
—
—
—
—
—
—
1.7
3.0
4.2
5.5
CHIP Enrollment
Amount in Millions
Total Private Health Insurance
177.8
177.8
180.4
179.2
178.5
177.8
178.6
180.9
183.8
187.0
188.5
191.3
193.5
197.9
198.0
198.3
Employer-sponsored private health insurance expenditures
149.0
155.1
158.2
158.1
158.6
154.5
156.1
158.7
163.0
165.4
168.1
171.9
178.2
182.0
180.2
180.1
23.2
23.2
23.2
23.0
23.0
23.5
23.2
23.3
21.9
21.6
20.3
19.0
18.1
18.0
19.9
20.4
Direct purchase Marketplace
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
Medigap
9.5
9.6
9.4
9.5
9.3
9.9
9.9
11.1
9.6
9.1
8.4
8.1
8.0
7.7
8.6
8.9
13.7
13.6
13.8
13.5
13.7
13.5
13.2
12.3
12.3
12.5
11.9
10.9
10.1
10.3
11.2
11.5
Medicare
Other direct purchase
31.7
32.3
32.9
33.5
34.2
34.9
35.6
36.2
36.8
37.3
37.6
38.0
38.3
38.8
39.1
39.6
Medicaid
20.0
20.0
20.8
22.8
25.9
28.5
30.5
31.7
32.3
32.2
31.8
31.4
32.2
34.1
36.8
40.4
—
—
—
—
—
—
—
—
—
—
—
—
1.7
2.3
3.2
3.9
CHIP Per-Enrollee Estimates of Health Insurance
Amount in Dollars (US$)
Total Private Health Insurance
839
989
1,135
1,305
1,429
1,546
1,653
1,704
1,770
1,838
1,907
2,011
2,155
2,314
2,535
2,829
Employer-sponsored private health insurance expenditures
854
977
1,131
1,299
1,414
1,564
1,654
1,700
1,770
1,863
1,927
2,016
2,111
2,278
2,527
2,818
Direct purchase
496
565
603
682
739
780
868
886
946
959
1,066
1,176
1,333
1,428
1,374
1,492
Marketplace
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
Medigap
—
—
—
—
—
—
—
—
—
—
—
—
—
—
1,298
1,324
Other direct purchase
—
—
—
—
—
—
—
—
—
—
—
—
—
—
1,432
1,621
Medicare
2,618
2,755
3,075
3,289
3,532
3,902
4,218
4,636
5,016
5,333
5,590
5,511
5,567
5,801
6,328
6,704
Medicaid
2,523
2,761
2,984
3,233
3,593
3,801
4,009
4,245
4,480
4,728
5,050
5,384
5,706
5,868
6,095
6,144
—
—
—
—
—
—
—
—
—
—
—
—
1,024
1,321
1,307
1,421
CHIP
(continued)
Goldsteen74024_06_CH06_169-214_03-18-20.indd 200
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
201
TABLE 6.5 Expenditures, Enrollment, and Per-Enrollee Expenditures on Health Insurance for Calendar Years 1987 to 2017 (continued) 1987
1988
1989
1990
1991
1992
1993
Growth rates:
1994
1995
1996
1997
1998
1999
2000
2001
2002
Percentage Change
Expenditures
Amount in Billions (US$)
Total Private Health Insurance
17.9%
16.5%
14.2%
9.1%
7.7%
7.5%
4.4%
5.6%
5.6%
4.6%
7.0%
8.4%
9.8%
9.6%
11.8%
Employer-sponsored private health insurance expenditures
19.2
18.0
14.9
9.2
7.7
6.9
4.5
7.0
6.8
5.1
7.0
8.5
10.3
9.9
11.4
Direct purchase
11.8
13.9
6.8
11.7
8.6
7.6
9.9
2.8
0.4
−0.3
4.7
3.4
7.8
6.8
5.9
Marketplace
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
Medigap
—
—
—
—
—
—
—
—
—
—
—
—
—
—
5.0 16.5
—
—
—
—
—
—
—
—
—
—
—
—
—
—
Medicare
Other direct purchase
7.1
13.7
8.9
9.5
12.8
10.3
11.8
10.0
7.8
5.8
−0.5
1.8
5.5
10.2
7.1
Medicaid
9.4
12.5
18.9
26.5
16.1
13.1
9.8
7.8
5.0
5.7
5.1
8.6
9.2
11.9
10.7
—
—
—
—
—
—
—
—
—
—
—
—
74.9
38.3
31.6
CHIP
—
Enrollment
Amount in Millions
Total Private Health Insurance
0.0%
1.4%
−0.7% −0.4% −0.4%
0.5%
1.3%
1.6%
1.7%
0.8%
1.5%
1.2%
2.3%
0.0%
0.2%
Employer-sponsored private health insurance expenditures
4.1
2.0
0.0
0.3
−2.6
1.1
1.7
2.7
1.5
1.6
2.3
3.6
2.1
−1.0
−0.1
Direct purchase
0.0
0.2
−1.2
0.3
1.9
−1.3
0.8
−6.0
−1.7
−5.8
−6.3
−4.9
−0.4
10.1
2.9
Marketplace
—
—
Medigap
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
2.9
Other direct purchase
—
—
—
—
—
—
—
—
—
—
—
—
—
—
2.9
Medicare Medicaid
1.8
1.8
1.9
2.0
2.0
2.0
1.7
1.6
1.4
1.0
1.0
0.8
1.2
1.0
1.1
0.0
4.0
9.8
13.8
9.7
7.2
3.7
2.1
−0.5
−1.0
−1.4
2.4
6.2
7.7
9.8
CHIP
—
—
—
—
—
—
—
—
—
—
—
—
35.5
39.7
21.1
Per Enrollee Estimates of Health Insurance
Amount in Dollars (US$)
Total Private Health Insurance
17.9%
14.8%
15.0%
9.5%
8.2%
7.0%
3.1%
3.9%
3.8%
3.8%
5.5%
7.2%
7.4%
9.6%
11.6%
Employer-sponsored private health insurance expenditures
14.5
15.7
14.9
8.8
10.6
5.8
2.8
4.1
5.3
3.4
4.6
4.7
7.9
10.9
11.5
Direct purchase
13.9
6.6
13.1
8.4
5.6
11.3
2.0
6.8
1.4
11.1
10.3
13.3
7.2
−3.8
8.6
Marketplace
—
—
—
—
—
—
—
—
—
—
—
—
—
—
—
Medigap
—
—
—
—
—
—
—
—
—
—
—
—
—
—
2.0
Other direct purchase
—
—
—
—
—
—
—
—
—
—
—
—
—
—
13.2
Medicare
5.2
11.6
7.0
7.4
10.5
8.1
9.9
8.2
6.3
4.8
−1.4
1.0
4.2
9.1
5.9
Medicaid
9.4
8.1
8.3
11.2
5.8
5.5
5.9
5.5
5.6
6.8
6.6
6.0
2.8
3.9
0.8
CHIP
—
—
—
—
—
—
—
—
—
—
—
—
29.0
−1.0
8.7
—, not applicable/not available.
(continued)
Goldsteen74024_06_CH06_169-214_03-18-20.indd 201
3/20/20 3:00 PM
202
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 6.5 Expenditures, Enrollment, and Per-Enrollee Expenditures on Health Insurance for Calendar Years 1987 to 2017 (continued) 2003
2004
2005
2006
2007
2008
Expenditures
2009
2010
2011
2012
2013
2014
2015
2016
2017
Amount in Billions (US$)
Total Private Health Insurance
615.1
658.3
701.2
737.2
776.2
802.9
832.9
864.3
898.5
929.6
947.1
1,000.7 1,069.8 1,136.4 1,183.9
Employer-sponsored private health insurance expenditures
555.0
594.9
636.9
672.8
714.1
741.3
766.4
793.1
824.3
852.2
866.6
896.7
33.4
35.4
35.8
35.0
34.3
35.3
38.8
42.7
45.8
48.3
50.1
71.6
—
—
—
—
—
—
—
—
—
—
—
24.0
Medigap
12.2
13.1
14.0
13.9
13.5
13.8
14.3
14.6
14.7
15.1
16.0
16.9
Other direct purchase
21.2
22.3
21.8
21.1
20.8
21.5
24.5
28.1
31.0
33.2
34.1
30.7
Medicare
282.7
311.1
339.8
403.7
432.8
467.0
498.9
519.8
544.8
568.5
589.9
Medicaid
269.0
290.7
309.4
306.7
325.9
344.3
374.6
397.4
407.0
422.9
6.3
7.2
7.6
8.4
9.1
10.2
11.1
11.5
12.0
12.6
Direct purchase Marketplace
CHIP Enrollment
947.4
1002.9
1043.5
88.6
96.0
100.8
40.1
47.2
55.1
17.6
18.9
20.1
30.8
30.0
25.6
618.6
649.0
677.1
705.9
445.2
497.8
542.6
565.6
581.9
13.5
13.2
14.7
16.8
18.2
Amount in Millions
Total Private Health Insurance
196.6
195.4
196.4
197.0
197.5
195.9
189.7
185.8
185.0
187.8
187.5
192.6
196.1
196.9
197.3
Employer-sponsored private health insurance expenditures
177.7
177.9
178.2
178.8
179.3
177.3
170.8
167.4
167.3
169.5
169.2
169.8
172.2
173.1
175.6
20.9
19.3
20.1
19.9
19.4
19.8
20.4
19.9
19.2
19.7
19.8
24.4
25.4
25.3
23.2
Direct purchase Marketplace
—
—
—
—
—
—
—
—
—
—
—
5.5
9.0
10.0
9.8
Medigap
9.1
8.7
9.0
8.5
8.2
8.1
7.5
7.2
7.1
7.0
7.0
7.0
7.1
7.7
7.7
11.8
10.6
11.1
11.4
11.2
11.7
13.0
12.7
12.1
12.7
12.8
11.9
9.3
7.6
5.7
Medicare
Other direct purchase
40.2
40.8
41.5
42.4
43.3
44.4
45.5
46.6
47.7
49.7
51.3
52.8
54.3
55.8
57.2
Medicaid
43.0
44.5
45.8
45.6
45.6
47.2
50.8
54.0
56.0
58.2
58.9
65.9
69.1
71.2
72.6
CHIP
4.2
4.3
4.4
4.6
4.9
5.0
5.3
5.5
5.6
5.8
6.0
5.9
6.0
6.5
6.8
Per-Enrollee Estimates of Health Insurance
Amount in Dollars (US$)
Total Private Health Insurance
3,129
3,368
3,570
3,741
3,931
4,099
4,390
4,653
4,857
4,951
5,052
5,195
5,454
5,771
6,001
Employer-sponsored private health insurance expenditures
3,123
3,344
3,574
3,764
3,983
4,182
4,488
4,738
4,927
5,026
5,122
5,282
5,502
5,794
5,942
Direct purchase
1,598
1,839
1,779
1,758
1,770
1,780
1,899
2,147
2,384
2,453
2,530
2,939
3,484
3,791
4,345
Marketplace
—
—
—
—
—
—
—
—
—
—
—
4,400
4,450
4,702
5,642
Medigap
1,351
1,506
1,561
1,633
1,648
1,702
1,916
2,030
2,072
2,155
2,281
2,400
2,491
2,449
2,608
Other direct purchase
1,788
2,113
1,955
1,851
1,860
1,834
1,889
2,214
2,567
2,617
2,666
2,587
3,304
3,946
4,470
Medicare
7,038
7,628
8,179
9,530
10,003
10,520
10,971
11,157
11,411
11,441
11,503
11,705
11,954
12,144
12,347
Medicaid
6,262
6,529
6,752
6,732
7,145
7,289
7,375
7,361
7,271
7,272
7,553
7,550
7,849
7,944
8,013
CHIP
1,501
1,658
1,722
1,831
1,871
2,023
2,086
2,117
2,131
2,186
2,259
2,239
2,455
2,592
2,686 (continued)
Goldsteen74024_06_CH06_169-214_03-18-20.indd 202
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
203
TABLE 6.5 Expenditures, Enrollment, and Per-Enrollee Expenditures on Health Insurance for Calendar Years 1987 to 2017 (continued) 2003
2004
2005
2006
2007
2008
Growth rates:
2009
2010
2011
2012
2013
2014
2015
2016
2017
Percentage Change
Expenditures
Amount in Billions (US$)
Total Private Health Insurance
9.7%
7.0%
6.5%
5.1%
5.3%
3.4%
3.7%
3.8%
4.0%
3.5%
1.9%
5.7%
6.9%
6.2%
4.2%
Employer-sponsored private health insurance expenditures
9.4
7.2
7.1
5.6
6.1
3.8
3.4
3.5
3.9
3.4
1.7
3.5
5.7
5.9
4.0
Direct purchase
9.6
6.0
1.0
−2.1
−2.2
2.9
9.9
10.1
7.2
5.7
3.6
43.0
23.7
8.4
5.0
Marketplace
—
—
—
—
—
—
—
—
—
—
—
—
66.9
17.7
16.8
Medigap
3.9
7.2
6.7
−0.9
−2.7
1.9
3.9
2.4
0.8
2.7
5.4
6.0
4.3
6.9
6.4
Other direct purchase
13.2
5.4
−2.3
−3.0
−1.9
3.5
13.8
14.7
10.6
7.1
2.8
−10.0
0.5
−2.9
−14.6
Medicare
6.5
10.1
9.2
18.8
7.2
7.9
6.8
4.2
4.8
4.3
3.8
4.9
4.9
4.3
4.2
Medicaid
8.4
8.1
6.4
−0.9
6.3
5.7
8.8
6.1
2.4
3.9
5.3
11.8
9.0
4.2
2.9
CHIP
14.8
13.8
5.6
10.6
9.0
12.0
8.8
3.9
3.9
5.3
6.9
−2.1
11.5
13.9
8.4
Enrollment
Amount in Millions
Total Private Health Insurance
−0.9%
−0.6%
0.5%
0.3%
0.2%
−0.8%
−3.1%
−2.1%
−0.4%
1.5%
−0.2%
2.8%
1.8%
0.4%
0.2%
Employer-sponsored private health insurance expenditures
−1.3
0.1
0.2
0.3
0.3
−1.1
−3.7
−2.0
0.0
1.3
−0.2
0.3
1.4
0.5
1.4
Direct purchase
2.3
−7.8
4.4
−0.9
−2.9
2.3
3.1
−2.6
−3.4
2.7
0.4
23.1
4.3
−0.4
−8.4 −2.7
Marketplace
—
—
—
—
—
—
—
—
—
—
—
—
65.1
11.4
Medigap
1.9
−3.9
3.0
−5.2
−3.6
−1.3
−7.7
−3.4
−1.3
−1.3
−0.4
0.7
0.5
8.7
0.0
Other direct purchase
2.6
−10.8
5.6
2.5
−2.3
5.0
10.5
−2.2
−4.6
5.0
0.9
−7.2
−21.4
−18.7
−24.6
Medicare
1.5
1.6
1.8
2.0
2.1
2.6
2.4
2.5
2.5
4.1
3.2
3.1
2.7
2.7
2.5
Medicaid
6.4
3.7
2.9
−0.6
0.1
3.6
7.5
6.3
3.7
3.9
1.3
11.9
4.9
3.0
2.0
CHIP
8.7
3.0
1.6
4.0
6.7
3.6
5.5
2.3
3.2
2.7
3.5
−1.3
1.7
7.9
4.6
Per Enrollee Estimates of Health Insurance
Amount in Dollars (US$)
Total Private Health Insurance
10.6%
7.7%
6.0%
4.8%
5.1%
4.3%
7.1%
6.0%
4.4%
1.9%
2.0%
2.8%
5.0%
5.8%
4.0%
Employer-sponsored private health insurance expenditures
10.8
7.1
6.9
5.3
5.8
5.0
7.3
5.6
4.0
2.0
1.9
3.1
4.2
5.3
2.6
Direct purchase
7.1
15.0
−3.2
−1.2
0.7
0.5
6.7
13.1
11.0
2.9
3.2
16.2
18.5
8.8
14.6
Marketplace
—
—
—
—
—
—
—
—
—
—
—
—
1.1
5.7
20.0
Medigap
2.0
11.5
3.6
4.6
1.0
3.3
12.6
5.9
2.1
4.0
5.8
5.2
3.8
−1.7
6.5
Other direct purchase
10.3
18.2
−7.5
−5.3
0.5
−1.4
3.0
17.2
16.0
1.9
1.9
−3.0
27.7
19.4
13.3
Medicare
5.0
8.4
7.2
16.5
5.0
5.2
4.3
1.7
2.3
0.3
0.5
1.7
2.1
1.6
1.7
Medicaid
1.9
4.3
3.4
−0.3
6.1
2.0
1.2
−0.2
−1.2
0.0
3.9
0.0
4.0
1.2
0.9
CHIP
5.6
10.5
3.9
6.4
2.2
8.1
3.1
1.5
0.6
2.6
3.3
−0.9
9.7
5.6
3.6
—, not applicable/not available. SOURCE: Centers for Medicare & Medicaid Services. (2018c). Expenditures, Enrollment and Per Enrollee Estimates of Health Insurance: United States, CY 1987-2017. Retrieved from https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/ NationalHealthExpendData/NationalHealthAccountsHistorical
Goldsteen74024_06_CH06_169-214_03-18-20.indd 203
3/20/20 3:00 PM
204
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
ranged from about US$3,700 in South Carolina to over US$10,000 in North Dakota (Kaiser Family Foundation, 2014).
Children’s Health Insurance Program Created as the State Children’s Health Insurance Program by the Clinton administration’s Balanced Budget Act (BBA) of 1997, CHIP provides health coverage for uninsured children who are not eligible for Medicaid. It is jointly financed by the federal and state governments and administered by the states. Within broad federal guidelines, each state determines the design of its program, eligibility groups, benefit packages, payment levels for coverage, and administrative and operating procedures. Federal payments to states are based on state expenditures under approved plans. CHIP provided a capped amount of funds to states on a matching basis for federal fiscal years (FYs) 1998 to 2007. The expansion continued under the ACA, and 9.5 million children were enrolled in CHIP at some point since it began through federal FY 2017 (CMS, 2017), and 6.8 million were still enrolled during calendar year 2017 (Medicaid.gov, 2019). The estimated average insurance cost per enrollee was under US$2,700 in 2017 (see Table 6.5) and the program total was US$18.2 billion.
Other Government Programs Among other major government health programs are, at the federal level, those offered through the Department of Defense (DOD) and the Veterans Affairs (VA). At the state level, they include the state public health and mental hospital services and, at the local level, the local public general hospitals and local public health services. These government programs are paid primarily with broad-based tax levy funds. Together, they consume a relatively small proportion of the NHE. For example, in 2017, Other Health Insurance Programs—which include the DOD and VA health programs—were 4% of national HCE. Moreover, they had accounted for 4% of HCE every year since 2008, and before that for 3% since 1990. Their highest level was in 1960, when they accounted for 7% of HCE (see Table 6.3).
GoFundMe Campaigns One curious artifact of the modern U.S. health care system is the rise of GoFundMe campaigns to pay for individuals’ health care needs. As Kaiser Health Network noted in its interview with GoFundMe’s CEO Rob Solomon, the “prominence of the medical category is the symptom of a broken system” (Bluth, 2019). And summarizes the author of a New Yorker article, the “advantages in crowdfunding still go to the people who arrive with the most powerful connections and the best networks. After that, there is competition, with perverse incentives: whoever has the most heartrending story wins” (Heller, 2019).
PRICES A considerable part of the constant upward trend in health care spending in the United States has been caused by factors other than simple utilization, such as the ever-intensifying use of expensive technology-based diagnostic and procedural interventions, especially at the beginning and the end of life (Franks, Clancy, & Nutting, 1992; Meier & Morrison, 2002). In “The Growth in Cost Per Case Explains Far More of U.S. Health Spending Increases Than Rising Disease Prevalence,” Roehrig and Rousseau (2011) show that three quarters of the increase in real per capita health spending was attributable to growth in cost per case. Thus,
Goldsteen74024_06_CH06_169-214_03-18-20.indd 204
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
205
it remains to be seen how long the increase in expenditure rate will remain at a relatively modest level (although still above the general rate of inflation), or whether it will return to its previously astronomical (double-digit) levels, as in the 1970s and 1980s.
SUMMARY The United States spends more on health care than any other country in the world, both on a gross basis and on a per capita basis. Further, the United States has a uniquely complex financing and payment system (as demonstrated by the information in this chapter). As some have assessed, we creakily crank dollars through the system, which requires an enormous amount of eligibility determination, benefit checking, coinsurance/deductible calculation, billing and collection effort, preutilization authorization, utilization review, and so on (Himmelstein & Woolhandler, 2001). Mountains of paperwork are created, astronomical voice and fax/telephone costs are incurred, and untold amounts of computer time and space are used. Huge numbers of staff are required to carry out these activities. In addition to the high cost of administration, the U.S. health care system still leaves many people without health insurance despite the passage of the ACA. The ACA led to historic gains in health insurance coverage by extending Medicaid coverage to many low-income individuals and providing Marketplace subsidies for individuals below 400% of poverty. The number of uninsured nonelderly Americans decreased from over 44 million in 2013 (the year before the major coverage provisions went into effect) to just below 27 million in 2016. However, in 2017, the number of uninsured people increased by nearly 700,000 people, the first increase since implementation of the ACA. (Kaiser Family Foundation, 2018) This lack of health insurance has many negative consequences, ranging from personal anxiety and increased use of EDs (often meaning that care was deferred past the point where it might have been routine—and cheaper—to where it was complex and expensive, with the delay leading to avoidable complications), to growing personal bankruptcy rates (Hoffman et al., 2001). Reforming the U.S. health care delivery system to respond to its cost and access problems will be discussed in more detail in Chapter 10, History of Change From 1900 to 2010: Comprehensive Reform, with a review of the ACA to date. In the next chapter, we discuss the current performance—quality, equity, and efficiency— of the complex system that we have developed for providing health care in the United States. This is followed by chapters on the history of attempts to reform the health care system and projections about the future.
DATA SOURCES The following are authoritative sources of data and reports related to health care financing in the United States. •
National Health Expenditure Accounts. The NHEA is an activity of the CMS that produces “the official estimates of total health care spending in the United States. Dating back to 1960, the NHEA measures annual U.S. expenditures for health care goods and services, public health activities, government administration, the net cost of health insurance, and investment related to health care. The data are presented by type of service, sources of funding, and type of sponsor.”The historical data can be found in Excel form in NHE Tables [ZIP], as well as in reports and
Goldsteen74024_06_CH06_169-214_03-18-20.indd 205
3/20/20 3:00 PM
206
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
tables. Begin exploring at: www.cms.gov/Research-Statistics-Data-and-Systems/ Statistics-Trends-and-Reports/ NationalHealthExpendData/NationalHealth AccountsHistorical.html •
Medical Expenditure Panel Survey. MEPS is an activity of the AHRQ. MEPS is a “set of large-scale surveys of families and individuals, their medical providers, and employers across the United States. MEPS is the most complete source of data on the cost and use of health care and health insurance MEPS is the source of information about numerous health care financing topics including access to health care, children’s insurance coverage, health insurance, Medicare/Medicaid/CHIP, and projected data/expenditures. As an example, within the area of health care costs/ expenditures, there are tables available in an interactive format on the Household Component Summary Tables platform. There is also a query tool—MEPSnet/HC— that can be used to generate your own estimates for health care expenditures. Begin exploring here: www.meps.ahrq.gov/mepsweb
•
Kaiser Family Foundation (KFF). KFF is a private, nonprofit organization dedicated to providing information on national health issues. KFF is the source of a multitude of reports based on its own polling and research. Among KFF’s topics related to health care financing are health costs, health reform, Medicaid, Medicare, private insurance, and the uninsured. Start here to begin an exploration of KFF’s resources: www.kff.org
STUDY QUESTIONS 1. Define National Health Expenditures (NHE), Health Consumption Expenditures (HCE), and Personal HealthCare Expenditures (PHC), and describe a question or situation when each would be used. 2. What are the key government programs that finance health care in the United States and what persons do they cover? 3. What percentage of HCE is paid by government programs? How has government spending on health care changed since 1960? 4. What are the nongovernmental sources of health care financing? 5. What percentage of HCE is paid by nongovernmental sources? How has nongovernmental spending on health care changed since 1960? 6. Explain the categories on which health care dollars are spent and what percentage is spent on each. 7. Compare and contrast the six payment modes that are used to buy and sell health services.
NOTES 1. Like all elements of the GDP, unpaid work is not counted. This is particularly significant in health care because most medical symptoms are self-diagnosed and treated (Dean, 1981). Additionally, it is very common for people to receive care from family and loved ones in the course of mild illness. When people stay home from work because of illness, the GDP is reduced. On the other hand, if those same people were taken care of by a paid caregiver, the GDP would increase. 2. The expenditures included in the MEPS survey are a subset of those included in the personal health care component of the NHE. Although the sample of U.S. civilian noninstitutionalized population surveyed in the household component of MEPS represents 98% of the U.S. population, the nature of the population excluded from the MEPS
Goldsteen74024_06_CH06_169-214_03-18-20.indd 206
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
207
sample is such that they are likely to have very different health care expenditures. In addition, the NHE includes expenditures on nonpatient services (gift shops, cafeterias, etc.) as well as other expenditures not counted by MEPS (e.g., nonprescription nondurable goods, as well as CAM services). In 1996, the expenditures of MEPS household component made up about 60% of the personal health care component of NHEs, and in 2003, MEPS accounted for US$895.5 billion or slightly less than 62% of the estimated US$1,446 billion spent on personal health care. The authors strongly recommend that anyone planning to use either NHE or MEPS data for analysis or decision making should supplement their understanding of the inclusions, exclusions, and limitations of such data with the article “Reconciling Medical Expenditure Estimates From the MEPS and the NHA,” by Selden et al. (2001). 3. In health care, a cottage industry has formed around the interpretation of medical bills. For fees ranging between US$50 and US$250 per hour, “claims assistance” professionals or“health care advocates”will decipher bills, challenge errors, and negotiate discounts (Francis, 2006; Whitehouse, 2006).
REFERENCES Agarwal, R., Mazurenko, O., & Menachemi, N. (2017). High-deductible health plans reduce health care cost and utilization, including use of needed preventive services. Health Affairs, 36(10), 1762–1768. doi:10.1377/hlthaff.2017.0610 Agency for Healthcare Research and Quality. (2016). Total expenses and percent distribution for selected conditions by type of service: United States, 2013. Medical Expenditure Panel Survey Household Component Data. Retrieved from https://meps.ahrq.gov/data_stats/ tables_compendia_hh_interactive.jsp?_SERVICE=MEPSSocket0&_PROGRAM=MEP SPGM.TC.SAS&File=HCFY2013&Table=HCFY2013%5FCNDXP%5FC&_Debug= Agency for Healthcare Research and Quality. (2019). MEPS summary tables: Medical conditions. Retrieved from https://meps.ahrq.gov/mepstrends/hc_cond/ Arrow, K. J. (1963). Uncertainty and the welfare economics of medical care. American Economic Review, 53(5), 941–973. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/ articles/PMC2585909/ Bernard, D. M., Cowan, C., Selden, T. M., Lassman, D., & Catlin, A. (2018). Reconciling medical expenditure estimates from the MEPS and NHEA, 2012. Rockville, Maryland: Agency for Healthcare Research and Quality. Retrieved from https://meps.ahrq.gov/data_files/ publications/workingpapers/wp_17003.pdf Blue Cross Blue Shield of Illinois. (2019). Boeing Centers of Excellence (COE). Retrieved from https://www.bcbsil.com/boeing/find-a-doctor-or-hospital/centers-of-excellence.html Bluth, R. (2019, January 16). GoFundMe CEO: ‘Gigantic Gaps’ in health system showing up in crowdfunding. Kaiser Health News. Retrieved from https://khn.org/news/ gofundme-ceo-gigantic-gaps-in-health-system-showing-up-in-crowdfunding/ Briscoe, B. (2015). Understanding health plan types: What’s in a name? Beyond the Numbers, 4(2). Retrieved from https://www.bls.gov/opub/btn/volume-4/understanding_health _plan_types.htm Brook, R. H., Keeler, E. B., Lohr, K. N., Newhouse, J. P., Ware, J. E., Rogers, W. H., … Reboussin, D. (2006). The Health Insurance Experiment: A classic RAND study speaks to the current health care reform debate. Santa Monica, CA: RAND Corporation. Retrieved from https:// www.rand.org/pubs/research_briefs/RB9174.html
Goldsteen74024_06_CH06_169-214_03-18-20.indd 207
3/20/20 3:00 PM
208
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Cacace, M., & Schmid, A. (2009). The role of diagnosis related groups (DRGs) in healthcare system convergence. BMC Health Services Research, 9(Suppl. 1), A5. doi:10.1186/1472-6963-9-S1-A5 Center for Financing, Access, and Cost Trends. (2008). Total expenses for conditions by site of service: United States, 2003: Medical expenditure panel survey component data. Rockville, MD: Agency for Healthcare Research and Quality. Centers for Disease Control and Prevention. (2016). Chronic disease prevention and health promotion. Retrieved from http://www.cdc.gov/chronicdisease/ Centers for Disease Control and Prevention. (2019a). National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP): About chronic diseases. Retrieved from https:// www.cdc.gov/chronicdisease/about/index.htm Centers for Disease Control and Prevention. (2019b). National Center for Chronic Disease Prevention and Health Promotion (NCCDPHP): Health and economic costs of chronic diseases. Retrieved from https://www.cdc.gov/chronicdisease/about/costs/index.htm Centers for Medicare & Medicaid Services. (2017). Unduplicated number of children ever enrolled in CHIP and Medicaid. Retrieved from https://www.medicaid.gov/chip/down loads/fy-2017-childrens-enrollment-report.pdf Centers for Medicare & Medicaid Services. (2018a). National Health Expenditures by type of service and source of funds, CY 1960-2017. Retrieved from https://www.cms.gov/Research -Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpend Data/NationalHealthAccountsHistorical Centers for Medicare & Medicaid Services. (2018b). National health expenditure accounts: Methodology paper. Retrieved from https://www.cms.gov/Research-Statistics-Data -and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/ DSM-17.pdf Centers for Medicare & Medicaid Services. (2018c). Expenditures, Enrollment and Per Enrollee Estimates of Health Insurance: United States, CY 1987-2017. Retrieved from https://www .cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/ NationalHealthExpendData/NationalHealthAccountsHistorical Centers for Medicare & Medicaid Services. (2019a). ICD-10-CM/PCS MS-DRG v35.0 definitions manual. Retrieved from https://www.cms.gov/Medicare/Medicare-Fee-for -Service-Payment/AcuteInpatientPPS/MS-DRG-Classifications-and-Software Centers for Medicare & Medicaid Services. (2019b). What’s a Medicare advantage plan? Retrieved from https://www.medicare.gov/Pubs/pdf/12026-Understanding-Medicare -Advantage-Plans.pdf Cohen, S. B. (2015b). The concentration and persistence in the level of health expenditures over time: Estimates for the U.S. population, 2012–2013 (Statistical Brief No. 481). Rockville, MD: Agency for Healthcare Research and Quality. Cruz-Oliver, D. M. (2017). Palliative care: An update. Missouri Medicine, 114(2), 110–115. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6140030/ Dean, K. (1981). Self-care responses to illness: A selected review. Social Science and Medicine: Part A, 15(5), 673–687. doi:10.1016/0271-7123(81)90091-2 Dranove, D., & Millenson, M. L. (2006). Medical bankruptcy: Myth versus fact. Health Affairs, 25(2), w74–w83. doi:10.1377/hlthaff.25.w74
Goldsteen74024_06_CH06_169-214_03-18-20.indd 208
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
209
Emanuel, E. J., & Emanuel, L. L. (1994). The economics of dying. The illusion of cost savings at the end-of-life. New England Journal of Medicine, 330(8), 540–544. doi:10.1056/ NEJM199402243300806 Forbes. (2018). Aetna. Forbes Magazine. Retrieved from https://www.forbes.com/ pictures/5a8c601ca7ea43169013eb91/3-aetna/#45e7a4b213e2 Fox, P. D., & Kongstvedt, P. R. (2015). A history of managed health care and health insurance in the United States. Burlington, MA: Jones & Bartlett Learning. Francis, T. (2006, March 20). Escape from claims hell. The Wall Street Journal. Retrieved fromhttp://www.wsj.com/articles/SB114235173505397791#:TBzgjSylQxCkUA Franks, P., Clancy, C. M., & Nutting, P. A. (1992). Gatekeeping revisited: Protecting patients from overtreatment. New England Journal of Medicine, 327(6), 424–429. doi:10.1056/ NEJM199208063270613 Gibbons, L., Belizan, J. M., Lauer, J. A., Betran, A. P., Merialdi, M., & Althabe, F. (2010). The global numbers and costs of additionally needed and unnecessary caesarean sections performed per year: Overuse as a barrier to universal coverage. World Health Report (Background Paper 30). Retrieved from https://www.who.int/healthsystems/topics/ financing/healthreport/30C-sectioncosts.pdf Glied, S. A. (2001). Health insurance and market failure since Arrow. Journal of Health Politics, Policy and Law, 26(5), 957–965. doi:10.1215/03616878-26-5-957 Goodman, J. (2018, May 11). High-deductible health insurance: The good, the bad and the ugly. Forbes. Retrieved from https://www.forbes.com/sites/johngoodman/2018/05/11/ high-deductible-health-insurance-the-good-the-bad-and-the-ugly/#5b0c2c957b18 HealthCare.gov. (2019). Health benefits & coverage: Preventive health services. Retrieved from https://www.healthcare.gov/coverage/preventive-care-benefits/ Heller, N. (2019, July 1). The hidden cost of gofundme health care. The New Yorker. Retrieved from https://www.newyorker.com/magazine/2019/07/01/the-perverse-logic-of-gofund me-health-care Himmelstein, D. U., Lawless, R. M., Thorne, D., Foohey, P., & Woolhandler, S. (2019). Medical bankruptcy: Still common despite the Affordable Care Act. American Journal of Public Health, 109(3), 431. doi:10.2105/AJPH.2018.304901 Himmelstein, D. U., & Woolhandler, S. (2001). Bleeding the patient: The consequences of corporate health care. Monroe, ME: Common Courage Press. Hoffman, C., Schoen, C., Rowland, D., & Davis, K. (2001). Gaps in health coverage among working-age Americans and the consequences. Journal of Health Care for the Poor and Underserved, 12(3), 272–289. doi:10.1353/hpu.2010.0739 Hoffman, E. D., Klees, B. S., & Curtis, C. A. (2000). Overview of the Medicare and Medicaid Programs. Health care financing review. Medicare and Medicaid Statistical Supplement, 22(1), 1–348. Retrieved from https://europepmc.org/backend/ptpmcrender .fcgi?accid=PMC4194683&blobtype=pdf Igelhart, J. K. (1999a). The American health care system: Expenditures. New England Journal of Medicine, 340(1), 70–76. doi:10.1056/NEJM199901073400122 Igelhart, J. K. (1999b). The American health care system: Medicaid. New England Journal of Medicine, 340(5), 403–408. doi:10.1056/NEJM199902043400525
Goldsteen74024_06_CH06_169-214_03-18-20.indd 209
3/20/20 3:00 PM
210
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Igelhart, J. K. (1999c). The American health care system: Medicare. New England Journal of Medicine, 340(4), 327–332. doi:10.1056/NEJM199901283400424 Jacobson, G., Freed, M., Damico, A., & Neuman, T. (2019). A dozen facts about Medicare advantage in 2019. Retrieved from https://www.kff.org/medicare/ issue-brief/a-dozen-facts-about-medicare-advantage-in-2019/ Jonas, S. (1978). Medical mystery: The training of doctors in the United States. New York, NY: W. W. Norton. Kaiser Family Foundation. (2002). Section 6: Trends in health plan and provider relationships. In Trends and indicators in the changing health care marketplace. Menlo Park, CA: Author. Retrieved from https://www.kff.org/health-costs/report/ trends-and-indicators-in-the-changing-health-3/ Kaiser Family Foundation. (2014). Medicaid spending per enrollee (full or partial benefit). State Health Facts. Retrieved from https://www.kff.org/medicaid/state-indicator/ medicaid-spending-per-enrollee/ Kaiser Family Foundation. (2017). 2017 employer health benefits survey. Retrieved from https:// www.kff.org/report-section/ehbs-2017-section-4-types-of-plans-offered/ Kaiser Family Foundation. (2018). Key facts about the uninsured population. Retrieved from https://www.kff.org/uninsured/fact-sheet/key-facts-about-the-uninsured-population/ Lancet. (2018, October 13). Editorial: Stemming the global caesarean section epidemic. The Lancet, 392(10155), 1279. doi:10.1016/S0140-6736(18)32394-8 Leapfrog Group. (2019). Raising the bar for safer health care. Retrieved from https://www .leapfroggroup.org/about Lown, B. (1998). Physicians need to fight the business model of medicine. Hippocrates, 12(5), 25–28. Retrieved from http://graham.main.nc.us/~bhammel/MED/mcare00.txt Martin, A. B., Hartman, M., Washington, B., Catlin, A., & The National Health Expenditure Accounts Team. (2018). National health care spending in 2017: Growth slows to post-great recession rates; share of GDP stabilizes. Health Affairs, 38(1). doi:10.1377/ hlthaff.2018.05085 Mayes, R. (2006). The origins, development, and passage of Medicare’s revolutionary prospective payment system. Journal of the History of Medicine and Allied Sciences, 62(1), 21–55. doi:10.1093/jhmas/jrj038 Medicaid.gov. (2019). Children’s Health Insurance Program (CHIP). Retrieved from https:// www.medicaid.gov/chip/index.html Medical Reform Group of Ontario. (1980). The crisis in health care. Toronto, Canada: Author. Meier, D. E., & Morrison, R. S. (2002). Autonomy reconsidered. New England Journal of Medicine, 346(14), 1061–1066. doi:10.1056/NEJM200204043461413 Miller, R. H., & Luft, H. S. (1994). Managed care plans: Characteristics, growth, and premium performance. Annual Review of Public Health, 15, 437–459. doi:10.1146/annurev .pu.15.050194.002253 Mitchell, E. M. (2019). Concentration of health expenditures and selected characteristics of high spenders, U.S. civilian noninstitutionalized population, 2016 (AHRQ Statistical Brief #521). Retrieved from https://meps.ahrq.gov/data_files/publications/st521/stat521.pdf Moon, M. (2001). Health policy 2001: Medicare. New England Journal of Medicine, 344(12), 928–931. doi:10.1056/NEJM200103223441211
Goldsteen74024_06_CH06_169-214_03-18-20.indd 210
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
211
National Center for Health Statistics. (2017a). Births: Methods of delivery. Retrieved from https://www.cdc.gov/nchs/fastats/delivery.htm National Center for Health Statistics. (2017b). National health interview survey: Long-term trends in health insurance coverage, 1968-2017. Retrieved from https://www.cdc.gov/nchs/ data/nhis/health_insurance/TrendHealthInsurance1968_2017.pdf New York State, Department of Health. (2018a). Final APR-DRG weights effective July 1, 2018 (v34). Retrieved from https://www.health.ny.gov/facilities/hospital/reimbursement/apr -drg/weights/2018-07-01_final_weights.htm New York State, Department of Health. (2018b). A path toward value based payment: Annual update. Retrieved from https://www.health.ny.gov/health_care/medicaid/redesign/dsrip/ vbp_library/2018/docs/2018-06_final_vbp_roadmap.pdf New York State Department of Health. (n.d.). Redesigning New York’s Medicaid Program. Retrieved from https://www.health.ny.gov/health_care/medicaid/redesign/ Organisation for Economic Co-operation and Development. (2019). Health expenditure and financing. Retrieved from https://stats.oecd.org/Index.aspx?DataSetCode=SHA Pitney Bowes. (2019). Health and wellness. Retrieved from https://www.pitneybowes.com/us/ our-company/corporate-responsibility/health-and-wellness.html Porter, M. E., & Teisberg, E. O. (2006). Redefining health care: Creating value-based competition on results. Retrieved from https://store.hbr.org/product/redefining-health-care-creating -value-based-competition-on-results/7782?sku=7782-HBK-ENG Reinhardt, U. (2019). Priced out: The economic and ethical costs of American health care. Princeton, NJ: Princeton University Press. Roehrig, C. S., & Rousseau, D. M. (2011). The growth in cost per case explains far more of U.S. health spending increases than rising disease prevalence. Health Affairs, 3(9), 1657–1663. doi:10.1377/hlthaff.2010.0644 Roemer, M. I. (1962, Spring). On paying the doctor and the implications of different methods. Journal of Health and Human Behavior, 3(1), 4–14. doi:10.2307/2948736 Rosenbaum, S. (2002). Health policy report: Medicaid. New England Journal of Medicine, 346(8), 635–640. doi:10.1056/NEJM200202213460825 Schroeder, S. A. (2001). Prospects for expanding health insurance coverage. New England Journal of Medicine, 344(11), 847–852. doi:10.1056/NEJM200103153441113 Selden, T. M., Levit, K. R., Cohen, J. W., Zuvekas, S. H., Moeller, J. F., McKusick, D., & Arnett, A. H. (2001). Reconciling medical expenditure estimates from the MEPS and the NHA, 1996. Health Care Financing Review, 23(1), 161–178. Retrieved from https://www.ncbi .nlm.nih.gov/pmc/articles/PMC4194726/ Shryock, T. (2019). Does value-based pay have a future? Medical Economics, 96(18). Retrieved from https://www.medicaleconomics.com/news/does-value-based-pay-have-future Singer, A. J., Thode, H. C ., & Pines, J. M. (2019). US emergency department visits and hospital discharges among uninsured patients before and after implementation of the Affordable Care Act. JAMA Network, 2(4), e192662. doi:10.1001/jamanetworkopen .2019.2662 Steyer, R. (2016, June 13). Big players dropping HSA business despite growth potential. Pensions&Investments. Retrieved from https://www.pionline.com/article/20160613/ PRINT/306139985/big-players-dropping-hsa-business-despite-growth-potential
Goldsteen74024_06_CH06_169-214_03-18-20.indd 211
3/20/20 3:00 PM
212
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Thomas, R. (2006, November 23). Million dollar man: Life slowly returning to normal after struggle with tick bite. Decatur Daily. Retrieved from http://legacy.decaturdaily.com/de caturdaily/news/061123/million.shtml U.S. Census Bureau. (2018). QuickFacts: United States. Retrieved from https://www.census .gov/quickfacts/fact/table/US/PST045218# U.S. Congressional Budget Office. (2018). Exploring the growth of Medicaid managed care. Retrieved from https://www.cbo.gov/publication/54235 U.S. Department of Labor, Bureau of Labor Statistics. (2019). CPI inflation calculator. Retrieved from https://data.bls.gov/cgi-bin/cpicalc.pl?cost1=146.00&year1=196007&year2=201707 Walmart. (2019). Centers of excellence: World-class treatment for the most serious conditions. Retrieved from https://one.walmart.com/content/uswire/en_us/me/health/health-pro grams/centers-of-excellence.html Whitehouse, K. (2006, January 1). How to fight overcharges. The Wall Street Journal. Retrieved from https://www.wsj.com/articles/SB113607079996735555 World Health Organization. (2015). Health systems. Retrieved from http://www.who.int/ topics/health_systems/en/ Wynn, B. O. (2005). Medicare payment for hospital outpatient services: A historical review of policy options. Santa Monica, CA: RAND Corporation. Retrieved from https://www.rand .org/pubs/working_papers/WR267.html Zhang, J. (2006, December 5). Amid fight for life, a victim of lupus fights for insurance. The Wall Street Journal. Retrieved from http://www.wsj.com/articles/SB116528580686740743#: sBAMZZF3uhCkUA
FURTHER READING Agency for Healthcare Research and Quality. (2012). Medical expenditure panel survey background. Retrieved from http://meps.ahrq.gov/mepsweb/about_meps/survey_back.jsp Blue Cross Blue Shield Association. (2012). About the Blue Cross and Blue Shield Association. Blue Cross Blue Shield Association. (2015). About the Blue Cross and Blue Shield Association. Burns, B., Glaun, K., & Lipschutz, D. (2005). Consumers face inadequate protections concerning Medicare Part D. Enrollment and/or disenrollment problems. California Health Advocates. Carper, K., & Stagnitti, M. N. (2014). National health care expenses per person in the U.S. civilian noninstitutionalized population, 2012 (MEPS Statistical Brief #457). Retrieved from http:// meps.ahrq.gov/mepsweb/data_files/publications/st457/stat457.shtml Centers for Medicare & Medicaid Services. (2014). NHE web tables. Retrieved from http:// www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/ NationalHealthExpendData/Downloads/DSM-17.pdf Cohen, S. B. (2015a). Differentials in the concentration of health expenditures across population subgroups in the U.S., 2013 (Statistical Brief No. 480). Rockville, MD: Agency for Healthcare Research and Quality. Cunningham, R., & Sherlock, D. B. (2002). Bounceback: Blues thrive as markets cool toward HMOs. Health Affairs, 21(1), 24–38. doi:10.1377/hlthaff.21.1.24 Frakt, A. (2019, August 26). Why doctors still offer treatments that May not help. New York Times. Retrieved from https://www.nytimes.com/2019/08/26/upshot/why-doctors-still -offer-treatments-that-may-not-help.html?searchResultPosition=19
Goldsteen74024_06_CH06_169-214_03-18-20.indd 212
3/20/20 3:00 PM
6
■
F i n a n c i n g t h e H e a l t h C a re S y s t e m
213
Kaiser Family Foundation. (2019). Medicaid in the United States. Retrieved from http://files .kff.org/attachment/fact-sheet-medicaid-state-US Kaiser Family Foundation and Health Research Educational Trust. (2017). 2017 employer health benefits survey. Retrieved from https://www.kff.org/health-costs/ report/2017-employer-health-benefits-survey/ Kenney, G. M., & Pelletier, J. (2010). How will the Patient Protection and Affordable Care Act of 2010 affect children? Washington, DC: Urban Institute. Retrieved from www.urban.org/ uploadedpdf/412129-PPACA-affect-children.pdf Klees, B. S., & Wolfe, C. J. (2013). Brief summaries of Medicare & Medicaid. Office of the Actuary Centers for Medicare & Medicaid Services. Retrieved from https://www.cms.gov/ Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/MedicarePro gramRatesStats/Downloads/MedicareMedicaidSummaries2013.pdf National Center for Health Statistics. (2011). Health, United States, 2010: With special feature on death and dying. Hyattsville, MD: U.S. Department of Health and Human Services. National Center for Health Statistics. (2015). Health, United States, 2014: With special feature on adults aged 55–64. Hyattsville, MD: U.S. Department of Health and Human Services. Retrieved from http://www.cdc.gov/nchs/data/hus/hus14.pdf Organisation for Economic Cooperation and Development. (2011). OECD health data 2011. Retrieved from www.oecd.org/document/16/0,3343,en_2649_34631_2085200_1_1_1_1,00. html Organisation for Economic Cooperation and Development. (2015). How does health spending in the United States compare?: OECD health statistics 2015. Stanton, M. W., & Rutherford, M. K. (2006). The high concentration of U.S. health care expenditures (Research in Action, Issue 19). Rockville, MD: Agency for Healthcare Research and Quality. Urban Institute. (2010). State Children’s Health Insurance Program (SCHIP). U.S. Bureau of Economic Analysis. (2011). Table 2.5.5. Personal consumption expenditures by function. Retrieved from https://apps.bea.gov/iTable/iTable.cfm?reqid=19&step=2 U.S. Census Bureau. (2011). Statistical abstract of the United States: 2012. Retrieved from https://www.census.gov/library/publications/2011/compendia/statab/131ed.html U.S. Department of Labor, Bureau of Labor Statistics. (2006). Health care (NAICS 62, except 624). In Career guide to industries: 2006–07 edition (pp. 231–237). Washington, DC: Author. U.S. Department of Labor, Bureau of Labor Statistics. (2010). Current population survey: Employment and earnings, 2010. Retrieved from http://www.bls.gov/cps/cpsa2010.pdf U.S. Department of Labor, Bureau of Labor Statistics. (2011). Healthcare. In Career guide to industries, 2010–2011 edition. Washington, DC: Author. Retrieved from www.bls.gov/ oco/cg/cgs035.htm U.S. Department of Labor, Bureau of Labor Statistics. (2014). Current population survey: Employment and earnings, 2014. Retrieved from http://www.bls.gov/cps/cpsa2014.pdf Zarabozo, C., Taylor, C., & Hicks, J. (1996). Medicaid managed care: Numbers and trends. Health Care Financing Review, 17(3), 243–246.
Goldsteen74024_06_CH06_169-214_03-18-20.indd 213
3/20/20 3:00 PM
Goldsteen74024_06_CH06_169-214_03-18-20.indd 214
3/20/20 3:00 PM
7 Health Care System Performance
© Artizans Entertainment Inc. By Chris Wildt.
LEARNING OBJECTIVES After completing this chapter, students will be able to: • Define and explain quality, equity, and efficiency in terms of health care. • Identify and describe key population health outcomes. • Discuss how the United States has fared in measures of health outcomes in recent years. • Identify common clinical outcomes used to evaluate quality of health care. • Define and explain clinical effectiveness and patient safety. • Define healthcare-associated infections and describe their prevalence and methods to prevent them. • Identify organizations that have a major influence on health care quality and explain their functions. • Describe the role of data and information technology in assessing the performance of health care systems.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 215
3/19/20 10:54 AM
216
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
INTRODUCTION Satisfactory performance is critical to health care organizations and to the health care system as a whole. It is the basis of the confidence and support they need from individuals and institutions to survive and succeed. Thus, assessing health system performance is a vital function. And although health care performance has always been informally evaluated, the Flexner Report of 1910 (Duffy, 2011) started medicine and the health care field on the path toward rigorous scientific assessments. However, it was the widespread availability of electronic computing capacity in the 1970s that allowed health systems assessments to move from small, time-consuming studies with limited findings to current evaluations based on “big health data.” Today’s performance assessments, supported by electronic data capture and powerful computing capabilities, are comprehensive and timely compared with the past. As a result of the importance of health systems performance, it is essential for health care professionals to understand the assessment process. First, they increasingly contribute—in big or small ways—to the process of assessing and improving system performance. Second, they are greatly affected by the results of assessing health system performance. Whether they provide direct care to patients as a nurse, therapist, physician, or other clinician, or contribute to management of a health care organization—be it a hospital, nursing home, clinic, or other—their careers will be influenced by the assessment process. Over time, the insights gained from evaluating health systems performance drive change in professional roles, practice, and training. There are numerous frameworks for evaluating health care system performance, and, as discussed in Chapter 1, Introduction, this book uses the work of Aday et al., which identifies three evaluation criteria for health care systems: (a) quality, (b) equity, and (c) efficiency (Aday, Begley, Lairson, & Balkrishnan, 2004; Aday, Begley, Lairson, & Slater, 1993). Health care system performance may be assessed at the microlevel—for organizations including hospitals, physician practices, long-term care facilities, and other health care settings—or the macrolevel—for regions, states, nations, and other large population groups. At the microlevel, performance assessment is conducted with identifiable health care providers, organizations, and treatments. For example, we may be interested in the quality of care received by cataract patients in an ambulatory surgery center as indicated by the rate of postsurgical complications. Or if we are focused on health care efficiency, we might examine medical care costs for cataract surgery in that ambulatory center. If our interest is equity, we could ask if cataract patients with private health insurance have fewer postsurgical complications than those with Medicaid, in that ambulatory center. At the macro level of regions, states, and nations, the picture is more complex. Many health care providers and organizations are assessed simultaneously using global measures of health outcomes such as life expectancy and mortality rates. For example, we might be interested in how the health care system, as a whole, performs for seniors in a particular region. To evaluate the quality of care delivered by the health system in this region, we might use chronic disease mortality rates for people over 65. Or if our interest is equity, we might compare the chronic disease mortality rates of seniors with supplemental health insurance to those with Medicare only to determine whether mortality is higher in the Medicare-only group. In the case of efficiency, we could examine global costs for hospitalization among seniors in the region. In all cases, the quality, equity, and efficiency of the health care system for seniors is inferred from global measures that aggregate many health care providers and organizations. We actually do not know how many seniors received health care and, if they did, what treatments were received, how often, and by what health care providers and organizations. These details underlie the results but are obscured because the data are not available.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 216
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
217
However, it should be noted that the capacity to collect and process “big health data” continues to increase and, as a result, macrolevel information is becoming better and better. This topic is discussed in the last section of the chapter. Regardless of whether evaluation occurs at the microlevel or macrolevel, the process requires a comparison to be useful. Referents are either a: • •
“Gold standard”—a recognized “best” performance, or a “Benchmark”—a starting point from which to begin the comparison
An entity’s own performance may be the“benchmark.”Here, the question asked is whether the entity—ambulatory practice, hospital, region, nation, or other—has improved over its own past performance. Or the “benchmark” may be the performance of another entity— ambulatory practice, region, nation, or other. The question, then, is whether the entity is performing as well as or better than a peer, perhaps one that is recognized for high performance. In this chapter, we discuss each criterion for assessing health systems performance—quality, equity, and efficiency—including common indicators and measures for each. We emphasize the quality criterion, describing the process for assessing quality in health care systems and providing an example of a quality assessment and improvement initiative. The major organizations that influence health systems’ performance are identified. The chapter concludes with the role of data and information systems in assessment of health systems performance.
HEALTH CARE QUALITY Using the model originally developed by Donabedian, health care quality is assessed in terms of structure, process, and outcomes (Donabedian, 1980–1985).“Structure ... is meant to designate the conditions under which care is provided”(Donabedian, 2003, p. 46). It includes material resources, such as facilities and equipment; human resources, such as number and qualities of professional and support personnel providing health care; and organizational characteristics, such as (for individual facilities such as hospitals) nonprofit status, academic affiliation, and governing structure. Examples of structure-oriented questions are as follows: What is the nurse-to-patient ratio on a hospital floor? What is the age of the facility? What proportion of a hospital’s patients do not have insurance, are receiving Medicaid, or are covered by Medicare? Are the physicians in a practice salaried employees or paid on a fee-for-service basis? Process “is taken to mean the activities that constitute health care—including diagnosis, treatment, rehabilitation, prevention, and patient education—usually carried out by professional personnel, but also including other contributions to care, particularly by patients and their families” (Donabedian, 2003, p. 46). For example, a study of health care process might ask the following questions: Is infection control policy followed by the hospital staff? How long does it take for the primary care physician to receive the test results needed for diagnosis? How does the treating physician transmit information about a drug’s side effects to the patient? What is the waiting time in the emergency room? How much time does a physician spend with a patient, on average, for an annual physical? What is the standard practice among the physician staff for treating a particular health condition, such as acute myocardial infarction or stroke? Structure and process influence the outcomes of health care. For example, each of the structure- and process-oriented issues just mentioned may lead to poor health care outcomes, but they are not outcomes in themselves. Outcomes “are taken to mean changes (desirable or undesirable) in the health of individuals and populations that can be attributed to health care” (Donabedian, 2003, p. 46).
Goldsteen74024_07_CH07_215-272_03-18-20.indd 217
3/19/20 10:54 AM
218
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Ultimately, our interest is in outcomes, and we ask: Have the structures and processes of the health care system resulted in the desired outcome: quality, equitable, and efficient health care? Generally speaking, there are two types of outcomes used to assess the quality of health care systems: • •
Population health outcomes Clinical (or healthcare-associated) outcomes
Population health outcomes are generalized outcomes that are not attributed to a specific medical intervention. They include, for example, life expectancy and mortality rates for populations with a varied history of health problems and medical care. The age-adjusted mortality rate for all people living in a geographic region is an example. Clinical outcomes result from medical interventions for particular health conditions. They are directly attributable to health care processes. The age-adjusted mortality rate for patients who have undergone open-heart surgery is an example. We begin with population health outcomes and then consider clinical (healthcare-associated) outcomes.
Population Health Outcomes Health outcomes can be measured at the population level and used to evaluate the quality of care provided by a health care system (Kindig, 1997). Population health outcomes include population mortality and morbidity rates, and they are used in macrolevel performance evaluations of regions, states, and nations. The impact of health care on these rates is presumed even though there is no explicit measure of health care interventions among the population considered. If, for example, a disease-specific mortality rate is higher in one region than another, we assume that the health care system is not optimal for that disease in the region with the higher mortality rate. There is an inferred, not explicit, connection between the health care system and the population health outcome. Historically, population health outcomes that have been used to assess the quality of health systems are life expectancy, premature death rate, time lost to premature death, age-adjusted death rates, disease-specific death rates, and infant mortality rate. The World Health Organization (WHO) also emphasizes maternal mortality and the under-5 mortality rate. The most common are defined as follows: •
•
•
Life expectancy is defined as the number of years of life that individuals in a population can be expected to live, on average. Life expectancy at birth is commonly reported. It is defined as the average number of years that a newborn can expect to live, if he or she were to be exposed throughout life to the conditions prevailing at the time of his or her birth. Using life expectancy, premature death can be calculated. Premature death is defined as death before the expected age of death for an individual’s population. The time lost to premature death, also called years of potential life lost (YPLL), is based on the difference between the actual age at death and the expected age at death. Deaths at a younger age are weighted more heavily in the YPLL, providing an indicator of the severity of premature death’s impact on the population. It is expressed as years lost per 100,000 population. Mortality (or death) rates are measures of the frequency of death in a defined population during a given time period, often a year. Mortality rates are usually expressed
Goldsteen74024_07_CH07_215-272_03-18-20.indd 218
3/19/20 10:54 AM
7
• •
•
•
•
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
219
as the number of deaths per 100,000 population. There are a number of commonly used death rates. The crude death rate is the number of deaths from all causes for a population during a defined time period, often a year, and usually expressed as 100,000 per population. The cause-specific death rate is the number of deaths from a particular health condition (e.g., stroke) for a given population during a defined time period, often a year, and usually expressed as 100,000 per population. The age-specific death rate is the number of deaths among individuals in a specific age group (e.g., adults ages 39–64) in the population of that age during a defined time period, often a year, and usually expressed as 100,000 per population. The age-adjusted death rate takes into account the population’s age distribution when calculating mortality rate. Using a statistical method that “standardizes” the target population to a reference population, this measure is commonly used when comparing mortality rates across different populations. The infant mortality rate is the number of deaths among infants between birth and exactly 1 year of age per all births in the population during a defined time period, often a year. This rate is expressed per 1,000 live births.
A more recent population health concept takes into account quality of life. Healthy life expectancy (HALE) at birth is defined by WHO as the “average number of years that a person can expect to live in ‘full health’ by taking into account years lived in less than full health due to disease and/or injury” (WHO, 2012, p. 1). HALE is a measure that combines length and quality of life into a single estimate that indicates years of life that can be expected in a specified state of health (Kindig, 1997, p. 45). Other health-adjusted life expectancy measures are quality-adjusted life years (QALYs), which emphasize the individual’s perceived health status as the indicator of quality of life; disability-adjusted life years (DALYs), which combine mortality and disability measures; and years of healthy life (YHL), which combine perceived health and disability activity limitation measures from the National Health Interview Survey (Kindig, 1997). Next, we briefly consider the performance of the U.S. health care system, based on several population health indicators. This section relies on data from WHO, the Organisation for Economic Co-operation and Development (OECD), and the National Center for Health Statistics (NCHS), a component of the Centers for Disease Control and Prevention (CDC).
United States Compared With Other Countries In this discussion, we examine life expectancy, infant mortality, and years of potential life lost— comparing the United States with all OECD member countries (see Table 7.1). As all OECD members are democratic countries with market economies, this is an interesting comparison. The OECD member countries include wealthy, developed nations such as the United States, Germany, Japan, and Australia, as well as those less developed but with similar democratic values and economic goals, such as Poland, Mexico, Turkey, and Estonia. Unfortunately, the United States’ performance on these indicators is near the bottom, along with countries that are far less developed and have far fewer resources. First, we consider life expectancy. In 2016, the life expectancy of women in the 35 OECD member countries varied widely—from 77.8 years in Mexico to 87.1 years in Japan, with an average of 83.4 years. The United States was 30th at 81.1 years. Only the Slovak Republic (80.7), Turkey (80.7), Hungary (79.7), Latvia (79.6), and Mexico (77.8) had a lower life expectancy for women than the United States. For men, there are similar results. In 2016, life expectancy for men in the 35 OECD member countries ranged from 69.8 years in Latvia to 81.7 years in Switzerland, with an average life expectancy of 78.1 years. The life expectancy for men in the United States was 76.1 years, as in the
Goldsteen74024_07_CH07_215-272_03-18-20.indd 219
3/19/20 10:54 AM
220
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Czech Republic. Only seven of the 35 countries had a lower male life expectancy than did the United States—Latvia, Mexico, Estonia, Poland, Slovakia, Hungary, and Turkey (see Table 7.1). Comparison of infant mortality rates in the United States with the other OECD countries also indicates a problem in the United States. In 2016, the U.S. IMR was 5.9 per 1,000 live births. Although this rate is low, there are only three countries among the OECD member states with a higher IMR—Chile (6.9), Turkey (10.0), and Mexico (12.1). The lowest IMR was 0.7/1,000 live births in Finland. The OECD average IMR was 3.9 (see Table 7.1). Finally, a review of years of potential life lost among the OECD member countries confirms a problem in the United States. The following figures are per 100,000 men or women, 0-69 years old. In 2016, the YPLL among men in OECD member states ranged from 2,782 years in Norway to 9,570 years in Latvia. The average for all OECD member countries was 4,296 years. The U.S. YPLL was 5,909 years, significantly higher than the OECD average. In only six OECD member countries was the YPLL higher than in the United States: Latvia, Mexico, Estonia, Poland, Hungary, and the Slovak Republic. The YPLL for women in the United States was 3,523 years, which was higher than that in all other countries except Mexico, where it was 4,604 years. The average for all OECD member countries for women was 2,247 years (see Table 7.1).
TABLE 7.1 Population Health Outcomes in OECD Member Countries, 2016 Women
Men
Infant Mortalitya
Life Expectancy at Birth (2016 or Nearest Year)
Potential Years of Life Lost, All Causesb
Life Expectancy at Birth (2016 or Nearest Year)
Potential Years of Life Lost, All Causesc
Australia
3.1
84.6
2,013.3
80.4
3,420.9
Austria
3.1
84.1
1,913.8
79.3
3,401.7
Belgium
3.2
84.0
2,266.8
79.0
3,732.1
Canada
4.7
83.9
2,368.7
79.8
3,669.8
Chile
6.9
82.7
2,815.4
77.1
5,098.5
Czech Republic
2.8
82.1
2,235.7
76.1
4,469.8
Denmark
3.1
82.8
2,140.8
79.0
3,319.0
Estonia
2.3
82.2
2,686.9
73.3
6,932.5
Finland
1.9
84.4
1,785.8
78.6
3,788.6
France
3.7
85.5
2,039.4
79.2
4,019.2
Germany
3.4
83.5
2,129.7
78.6
3,758.3
Greece
4.2
84.0
2,061.1
78.9
4,257.9
Hungary
3.9
79.7
3,135.5
72.6
6,595.0
Iceland
0.7
84.1
1,486.6
80.4
2,876.0
Ireland
3.0
83.6
1,975.8
79.9
3,404.2
Israel
3.1
84.2
1,744.0
80.7
3,072.0
OECD Member Country
(continued)
Goldsteen74024_07_CH07_215-272_03-18-20.indd 220
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
221
TABLE 7.1 Population Health Outcomes in OECD Member Countries, 2016 (continued) Italy
2.8
85.6
1,689.5
81.0
2,965.3
Japan
2.0
87.1
1,600.9
81.0
2,923.2
Korea
2.8
85.4
1,681.8
79.3
3,488.4
Latvia
3.7
79.6
3,471.3
69.8
9,570.8
Luxembourg
3.8
85.4
1,255.4
80.1
2,880.8
Mexico
12.1
77.8
4,604.3
72.6
8,297.2
Netherlands
3.5
83.2
2,140.0
80.0
2,846.4
New Zealand
5.7
83.4
2,429.4
80.0
3,756.2
Norway
2.2
84.2
1,711.0
80.7
2,782.3
Poland
4.0
82.0
2,685.0
73.9
6,749.1
Portugal
3.2
84.3
1,889.7
78.1
4,295.9
Slovak Republic
5.4
80.7
2,855.4
73.8
6,397.4
Slovenia
2.0
84.3
1,826.8
78.2
3,993.7
Spain
2.7
86.3
1,619.8
80.5
3,111.9
Sweden
2.5
84.1
1,775.3
80.6
2,856.4
Switzerland
3.6
85.6
1,777.1
81.7
3,047.3
Turkey
10.0
80.7
2,985.0
75.3
5,012.8
United Kingdom
3.8
83.0
2,323.6
79.4
3,676.7
United States
5.9
81.1
3,523.7
76.1
5,909.1
OECD Average
3.9
83.4
2,247.0
78.1
4,296.5
a
Deaths per 1,000 live births, no minimum threshold of gestation period or birth weight. Years lost/100,000 women, aged 0 to 69 years. c Years lost/100,000 men, aged 0 to 69 years. SOURCE: Data from Organisation for Economic Co-operation and Development. (2019). OECD health statistics 2018—Frequently requested data. Retrieved from http://www.oecd.org/health/health-statistics.htm b
Quality-of-Life Adjusted Measures The WHO (2015) comparisons of the United States with a subset of the most developed OECD member countries indicate, once again, that the U.S. population is not as healthy as one would expect given its wealth, as well as the enormous amount spent on health care. In 2013, HALE at birth for males was 68 years in the United States, the lowest ranked country of the 13 (Finland and United States were at the bottom, with 68 years). Japan was ranked first (72 years). For HALE at birth for females, the United States and Denmark were ranked at the bottom in 2013, with 71 years. In 2012, the age-standardized DALY per 100,000 population for all causes of death was higher in the United States than in any of its 12 peer countries (22,775/100,000 population). The next highest DALY was 20,376/100,000 population in the United Kingdom.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 221
3/19/20 10:54 AM
222
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Limitations of Population Health Outcomes for Assessing Health Care Systems Although population health outcome measures such as life expectancy, mortality rates, and others reflect on a region’s health care system, it is also recognized that many factors outside the health care system affect these measures. For example, the difference in life expectancy and mortality rates between Whites and African Americans is thought to reflect in part differences in standard of living as well as access to health services (Geiger, 1996; Institute of Medicine [IOM], 2003; Schwartz, Kofie, Rivo, & Tuckson, 1990). As Levitt, Claxton, Cox, Gonzales, and Kamal (2014) summarize: Complicating any assessment of health system performance is the problem of distinguishing health system impacts from those that stem from other societal drivers. Many factors outside of the health system—such as poverty, diet, exercise, substance use, environmental factors, and social policies—not only contribute directly to health status, but also affect access to medical care. Even when potentially informative measures can be identified, consistent trend data may not always be available at the health system level for the U.S. and other countries. Historically, more emphasis has been placed on cost than on health system outcomes. However, industry leaders and policymakers cannot make good judgments about spending without understanding how well the system is working for patients. To put it simply, we need to better understand how much we are spending, what is driving growth, and what we are getting for what we spend. This means tracking how well the health system is performing at keeping people healthy and treating them when they get sick. Are we getting better health outcomes for our increased spending? If we are successful at reducing growth in spending, is there a sacrifice in terms of health? At the broadest level, we can think of a dual focus on health system spending and outcomes as assessing the efficiency of the health system. (Levitt et al., 2014, paras 4 and 5) Now we turn from population health outcomes to a discussion of clinical outcomes.
Clinical (or Healthcare-Associated) Outcomes Clinical outcomes (which will be used synonymously with healthcare-associated outcomes) are the consequences of health care interventions that are specific to persons who have received care. Unlike the quality assessment based on population health outcomes, the clinical outcomes assessment begins with the provider–patient interaction and its subsequent clinical processes and outcomes. For example, clinical outcomes for pancreatic cancer treatment may be 5-year survival and 30-day hospital readmission. For hip replacement surgery, clinical outcomes may be the absence of long-term pain and discomfort and patient satisfaction with changes in mobility after the surgery. Studies of clinical interventions and their outcomes are essential for evaluating and maintaining the quality of the health care system. Conducted with scientifically valid methods, clinical outcomes studies indicate the quality of the health care received by patients— answering these questions: • • •
Was the health care intervention implemented correctly? (the process) Was the health care intervention effective? That is, did it produce the desired or intended results? (an outcome) Did the health care intervention have adverse consequences for patients? (an outcome)
Goldsteen74024_07_CH07_215-272_03-18-20.indd 222
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
223
Increasingly, the patient’s point of view about treatment outcomes contributes to the determination of success or failure—whether the intervention was effective and whether it had adverse consequences for patients. Health care providers and patients have been found to differ in their assessment. For example, a 2010 study of adverse events in hospitals found that “The patient’s concept of adverse events was different from that of the physician. ... Patients emphasized emotional consequences of the adverse events” (Masso Guijarro, Aranaz, Mira, Perdiguero, & Aibar, 2010, p. 144). Clinical outcomes studies are the basis of evidence-based medicine, which has famously been defined in the British Medical Journal as: Evidence-based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence-based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research. (Sackett, Rosenberg, Gray, Haynes, & Richardson, 1996, p. 71) Clinical outcomes studies ensure that scientifically valid, empirical research provides the basis for assessing the effectiveness, or quality, of health care at the microlevel of physician practices, hospitals, and other health care settings. An example of a clinical outcomes study is Association Between Adverse Clinical Outcomes After Coronary Artery Bypass Grafting and Perioperative Blood Transfusions. The abstract is reprinted in Exhibit 7.1. EXHIBIT 7.1 Association Between Adverse Clinical Outcomes After Coronary Artery Bypass Grafting and Perioperative Blood Background: Bleeding is a serious complication of coronary artery bypass grafting that often leads to blood transfusion. Approximately 50% of patients who have the surgery receive blood products, and blood transfusions play a role in adverse outcomes after the surgery. Objective: To examine the association between perioperative blood transfusion and postoperative adverse outcomes in patients undergoing coronary artery bypass grafting. Methods: A systematic review of the literature, via the matrix method of quality evaluation, was conducted. PubMed, CINAHL, and Science Direct databases for 2000 through 2016 were searched. Inclusion criteria were articles published in English and original research related to clinical outcomes of blood transfusion after coronary artery bypass grafting. Seventeen articles were included in the review. Results: Mortality, both short- and long-term, was significantly higher in transfusion patients than in nontransfusion patients. Patients with transfusion of red blood cells had higher resource utilization and more complications, including infection, pneumonia, renal failure, graft occlusion, and atrial fibrillation, than did nontransfusion patients. Conclusion: An association exists between red blood cell transfusions and adverse clinical outcomes for patients undergoing coronary artery bypass grafting. Transfusion of red blood cells is sometimes unnecessary, may be injurious, and should be used cautiously. Even a single-unit increase in perioperative red blood cell transfusions can have a significant adverse impact on outcomes. Individual benefits and risks should be weighed before transfusion to avoid adverse outcomes. Transfusion guidelines should be reviewed to include the latest evidence to guarantee the most appropriate use of blood products (p. 26). Source: Reproduced with permission from Mirzaei, S., Hershberger, P. E., & DeVon, H. A. (2019). Association between adverse clinical outcomes after coronary artery bypass grafting and perioperative blood transfusions. Critical Care Nurse, 39(1), 26–35. doi:10.4037/ccn2019589
Goldsteen74024_07_CH07_215-272_03-18-20.indd 223
3/19/20 10:54 AM
224
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Designing and conducting clinical outcomes studies are the first explicit steps in the process of evaluating health care quality—in a facility, by a provider, or by a health care system. In a fully developed quality-improvement process, they are followed by systematic reviews, development of clinical practice guidelines, and their implementation in health care settings.
Systematic Reviews and Clinical Practice Guidelines Experts in a clinical field synthesize many clinical outcomes studies in systematic reviews. “A systematic review attempts to identify, appraise and synthesize all the empirical evidence that meets pre-specified eligibility criteria to answer a specific research question. Researchers conducting systematic reviews use explicit, systematic methods that are selected with a view aimed at minimizing bias, to produce more reliable findings to inform decision making” (Cochrane Collaboration, 2019a, para 1). Using many studies to determine the clinical efficacy of a set of clinical practices overcomes the limitations of a single study. Systematic reviews can be used to develop clinical practice guidelines (or clinical practice protocols). In 2011, the IOM redefined clinical practice guidelines as follows: “Clinical practice guidelines are statements that include recommendations intended to optimize patient care that are informed by a systematic review of evidence and an assessment of the benefit and harms of alternative care options” (IOM, 2011, p. 4). Developing clinical practice guidelines is a collaborative activity between experts in the focus area, including health professionals, health care researchers, and policy makers. Each set of clinical practice guidelines is the result of the distillation of the evidence provided by hundreds of studies through systematic reviews. The result is evidence-based “best practices” focused on the quality of care in clinical settings—hospitals, ambulatory care centers, and nursing homes—for all categories of health conditions—for instance, heart disease, infectious diseases, diabetes, or asthma. Because concrete recommendations for clinical practice by physicians, nurses, technicians, and other health professionals result from developing guidelines, it is a weighty endeavor. The process of developing guidelines is outlined by Shekelle, Woolf, Eccles, and Grimshaw (1999) as follows: • • • • •
Identifying and refining the subject area is the first step in developing a guideline. Convening and running guideline development groups is the next step. On the basis of systematic reviews, the group assesses the evidence about the clinical question or condition. This evidence is then translated into a recommendation within a clinical practice guideline. The last step in guideline development is external review of the guideline. (p. 593)
An example of a systematic review of clinical outcomes studies is provided by Carson, McDonagh, and Peterson (2006; see Exhibit 7.2, for researchers’ conclusions). The review compares the effectiveness of different atypical antipsychotic drugs for people with dementia. This review demonstrates the difficulty of developing clinical practice guidelines. The reviewers were unable to recommend practice guidelines because the results of the review, although suggestive, were inconclusive. Therefore, at the time of this systematic review, more studies and another review would be needed to develop consensus around practice guidelines for treatment of dementia with these drugs. The preceding systematic review of atypical antipsychotic drugs for people with dementia illustrates the very important point that health care interventions are “works in progress.”At any given time,
Goldsteen74024_07_CH07_215-272_03-18-20.indd 224
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
225
EXHIBIT 7.2 A Systematic Review of the Efficacy and Safety of Atypical Antipsychotics in Patients With Psychological and Behavioral Symptoms of Dementia Although the Food and Drug Administration (FDA) has not approved atypical antipsychotics for use in patients with dementia, they are commonly prescribed in this population. Recent concerns about increased risk of cerebrovascular events and mortality have led to warnings. A systematic review was conducted to assess the benefits and harms of atypical antipsychotics when used in patients with behavioral and psychological symptoms of dementia. Electronic searches (through March 2005) of the Cochrane Library, Medline, Embase, and PsycINFO were supplemented with hand searches of reference lists, dossiers submitted by pharmaceutical companies, and a review of the FDA website and industry-sponsored results database. Using predetermined criteria, each study was assessed for inclusion, and data about study design, population, interventions, and outcomes were abstracted. An overall quality rating (good, fair, or poor) was assigned based on internal validity. The evidence for olanzapine and risperidone supports their effectiveness compared with placebo. Short-term adverse events were similar to placebo. Risperidone had no advantage over haloperidol on efficacy measures in the better-quality studies. Risperidone had an advantage over haloperidol on some measures of extrapyramidal symptoms. Evidence for the other atypical antipsychotics is too limited to assess efficacy and safety. Trials were short term and conducted in highly selected populations. The potential for increased risk of cerebrovascular adverse events and mortality is a serious concern. To make judgments about when the benefits of atypical antipsychotics outweigh the potential harms, clinicians need more information. Additional data from existing trials and more complete reporting of trial results could provide this information (p. 354). Source: Reproduced with permission from Carson, S., McDonagh, M., & Peterson, K. (2006). A systematic review of the efficacy and safety of atypical antipsychotics in patients with psychological and behavioral symptoms of dementia. Journal of the American Geriatric Society, 54(2), 354–361. doi:10.1111/j.1532-5415.2005.00566.x
• •
there may be insufficient scientific evidence to develop clinical practice guidelines existing clinical practice guidelines may change as science advances
Moreover, when scientific evidence is absent or inconclusive, clinical practices are developed by consensus of experienced clinicians and other experts. Although clinical practice guidelines are sometimes derisively referred to as “cookbook medicine,” they are proliferating and increasingly used by insurers and other payers to evaluate the quality of health care provided to patients.
Health Care Quality Standards and Their Implementation Clinical outcomes research, systematic reviews, and clinical practice guidelines lay the foundation for assessing health care quality. From this evidence-based underpinning, the next phase of the assessment process is developed. The next phase requires creating quality standards for each health care setting—hospital, ambulatory, long-term care, and others; developing measures for these quality standards; and then identifying and collecting the data needed for the measures. Organizations that monitor and enforce the quality standards must be identified or established. Training that prepares people to participate in the assessment process is needed. Finally, and perhaps most importantly, consensus among stakeholders—health care providers, administrators, payers, policy makers, and others—that the assessment process
Goldsteen74024_07_CH07_215-272_03-18-20.indd 225
3/19/20 10:54 AM
226
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
is adequate and fair must be built. This is no small task, as there are scientific, political, and economic ramifications at each step in the process. Particularly now, as value-based payment of providers is gathering momentum, it is critical that measures of health care outcomes are valid indicators of health care quality. Baker and Chassin (2017) proposed four criteria for all outcome measures used to hold providers accountable for care: • • • •
Strong evidence should exist that good medical care leads to improvement in the outcome within the time period for the measure; The outcome should be measurable with a high degree of precision; The risk-adjustment methodology should include and accurately measure the risk factors most strongly associated with the outcome; and Implementation of the outcome measure must have little chance of inducing unintended adverse consequences.
They state: “Although the goal of medicine is to improve health outcomes for patients, using outcome measures for accountability requires extreme care. We must approach this task as rigorously as has been done for process measures if we are going to identify and reward providers who achieve the best outcomes and use measurement to drive quality improvement” (Baker & Chassin, 2017, p. 422). Next, we discuss the major organizations that participate in the assessment of health care quality and their roles.
Organizations With Major Influence on Health Care Quality The job of assessing health care system quality in the United States is distributed among many organizations. This section describes the efforts of the many public and private organizations that play a role in improving the quality of health care. These are the organizations that together • • • • • • • •
fund clinical outcomes research, which provides evidence for quality assessment produce clinical outcomes research conduct systematic reviews produce clinical practice guidelines develop quality-of-care standards and measures collect quality-of-care data monitor and enforce quality standards train people to participate in the quality assessment process
Efforts to improve health care quality are increasingly collaborative and can include federal and state agencies; provider, payer, educational, and accreditation organizations; and businesses. It is difficult to say which organizations are the most influential. Clearly, The Joint Commission, as the country’s largest health care accrediting organization, and the CMS, as one of the largest payers of health care services in the country, are extremely important. However, other private and public organizations have very significant roles. The discrete impact of each organization is difficult to assess, but their joint influence is profound. The list of organizations described in this section is not all-inclusive, but contains major actors and the roles they play. The list illustrates the public/private nature of the U.S. health care system. See Table 7.2.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 226
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
227
TABLE 7.2 Organizations With Major Roles in Health care Quality Improvement, 2019 Role in Health care Quality Improvementa Organization 1
2
3
4
5
6
7
8
X
X
X
X
Federal Agencies Centers for Medicare & Medicaid Services (CMS) Agency for Healthcare Research and Quality
X
X
X
X
X
X
Centers for Disease Control and Prevention
X
X
X
X
X
X
National Institutes of Health
X
X
X X
X
X
X
X
X
X
X
Health Care Accrediting Organizations (Private, Nonprofit) The Joint Commission
X
National Committee for Quality Assurance
X
Other CMS-Approved Accrediting Organizations
X
X
Other Private, Nonprofit Organizations National Quality Forum
X
X
Leapfrog Group
X
X
X
X
X
Institute for Healthcare Improvement Cochrane Collaboration Patient-Centered Outcomes Research Institute
X X
X
X
X
Healthcare Professional Associations
X
X
Medical Specialty Organizations
X
X
X
X
Universities and Research Institutes
X
X
X
X
a
Key to roles: 1. Fund clinical outcomes research, which provides evidence for quality assessment 2. Produce clinical outcomes research 3. Conduct systematic reviews 4. Produce clinical practice guidelines 5. Develop quality-of-care standards and measures 6. Collect quality-of-care data 7. Monitor and/or enforce quality standards 8. Train people to participate in the quality assessment process
Federal Agencies The major federal government agencies that focus on ensuring and improving the quality of health care in the United States are described next. Each agency has been discussed previously in Chapter 5, Government and the Health Care System, or Chapter 6, Financing the Health Care System, but the following section focuses on their roles in assessing health care quality. The influence of federal agencies on health care quality cannot be overestimated.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 227
3/19/20 10:54 AM
228
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Centers for Medicare and Medicaid Services CMS (formerly the Healthcare Financing Administration, or HCFA) is located in the U.S. Department of Health and Human Services (DHHS). CMS pays for the covered health care services of Medicare and Medicaid beneficiaries in hospitals, nursing homes, home health agencies, end-stage renal disease (ESRD), hospices, and other facilities serving these beneficiaries. Health care quality improvement is a CMS core function. The CMS final report on physician quality reporting programs articulates and expands on the CMS position on quality: Driving health care quality improvement is a core function of the Centers for Medicare & Medicaid Services (CMS). As the largest health care payer in the United States, with over 100 million Medicare beneficiaries and Medicaid enrollees, CMS facilitates the delivery of high quality health care and continuously seeks ways to improve quality. CMS also supports the U.S. Department of Health and Human Services’ (HHS) efforts to drive towards a system that delivers better care, is smarter about how health care dollars are spent, and that keeps the population healthy. These efforts center around improving health care delivery, improving how providers are paid, and improving the way information is distributed. (CMS, 2015, p. 2) As the largest payer of health care services in the country—with over 100 million beneficiaries—CMS influences quality throughout the health care system. Using its power as the largest payer, CMS attempts to drive quality higher and costs lower. Every health care provider and facility is affected by CMS policies and practices, directly or indirectly. For example, other insurance companies will use CMS quality measures to evaluate the health services they pay, rather than developing their own measures. The practice of harmonizing with CMS also impacts providers by reducing the number of quality measures they must collect and report. CMS quality goals and objectives are set forth in the CMS Quality Strategy, which aligns with the National Quality Strategy. The CMS Quality Strategy 2016 (Box 7.1; CMS, 2019a)
BOX 7.1 CMS Quality Strategy 2016 Three Aims 1. Better Care: Improve the overall quality of care by making healthcare more person-centered, reliable, accessible, and safe. 2. Healthier People, Healthier Communities: Improve the health of Americans by supporting proven interventions to address behavioral, social, and environmental determinants of health, and deliver higher-quality care. 3. Smarter Spending: Reduce the cost of quality healthcare for individuals, families, employers, government, and communities.
Six Goals 1. 2. 3. 4. 5. 6.
Make care safer by reducing harm caused in the delivery of care. Strengthen person and family engagement as partners in their care. Promote effective communication and coordination of care. Promote effective prevention and treatment of chronic disease. Work with communities to promote best practices of healthy living. Make care affordable.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 228
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
229
has three overarching aims and six goals for quality improvement (Box 7.1). The CMS Quality Strategy also identifies policy levers and drivers to meet these goals. For example, a policy lever for quality is“measuring and publicly reporting providers’ quality performance.”Finally, note the expansive view of quality to include prevention of disease and disability and improved communications between providers and patients. The CMS Quality Strategy is not limited to improving health care interventions and their cost. To implement its Quality Strategy, CMS activities include Quality Initiatives (QIs) and Quality Measures (QMs). The overall goal of the QIs is to improve the quality of services for Medicare and Medicaid recipients through provider accountability and public disclosure (CMS, 2019b). The QIs were launched nationally in 2002 with the Nursing Home QI (NHQI) and expanded in 2003 with the Home Health QI (HHQI) and the Hospital QI (HQI). In 2004, the Physician Focused QI, which includes the Doctor’s Office Quality Project, was developed. In 2004, the QIs were expanded to include kidney dialysis facilities. The ESRD QI promotes ongoing CMS strategies to improve the quality of care provided to ESRD patients. In 2006, CMS launched the Physician Voluntary Reporting Program (CMS, 2007). In 2009, CMS estimated that almost all settings covered by Medicare were covered by QMs (CMS, 2009). Quality Measures are developed and used in QIs. They are “tools that help us measure or quantify health care processes, outcomes, patient perceptions, and organizational structure and/or systems that are associated with the ability to provide high-quality health care and/ or that relate to one or more quality goals for health care” (CMS, 2019c, para 2). The CMS Quality Measures Inventory compiles the measures used by CMS in various programs. “The Inventory lists each measure by program, reporting measure specifications including, but not limited to, numerator, denominator, exclusion criteria, National Quality Strategy (NQS) domain, measure type, and National Quality Forum (NQF) endorsement status” (CMS, 2019d, para 1). An example of a measure in the CMS Quality Measures Inventory is “Acute Care Hospitalization: Unplanned Hospitalization during First 60 days of Home Health,” which is an outcome measure used in Home Health Quality Reporting and Home Health Value-Based Purchasing. Each measure in the Quality Measures Inventory contains standardized information, as available. See Table 7.3 for an example. TABLE 7.3 Acute Care Hospitalization: Unplanned Hospitalization During First 60 Days of Home Health, CMS Quality Measure, 2019 Info as of
Not available
Description
Percentage of home health stays in which patients were admitted to an acute care hospital during the 60 days following the start of the home health stay.
Numerator
Number of home health stays for patients who have a Medicare claim for an admission to an acute care hospital in the 60 days following the start of the home health stay.
Denominator
Number of home health stays that begin during the 12-month observation period. A home health stay is a sequence of home health payment episodes separated from other home health payment episodes by at least 60 days.
Denominator Exclusions
Home health stays that begin with a Low Utilization Payment Adjustment claim. Home health stays in which the patient receives service from multiple agencies during the first 60 days. Home health stays for patients who are not continuously enrolled in fee-for-service Medicare for the 6 months prior to and the 60 days following the start of the home health stay or until death.
Rationale
Not available
Evidence
Not available
SOURCE: Centers for Medicare & Medicaid Services. (2019). Quality measures inventory. Retrieved from https://www.cms.gov/Medicare/ Quality-Initiatives-Patient-Assessment-Instruments/MMS/Quality-Measures-Inventory.html
Goldsteen74024_07_CH07_215-272_03-18-20.indd 229
3/19/20 10:54 AM
230
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
In 2017, CMS instituted the “Meaningful Measures” initiative, which advances QMs by identifying the highest priorities for quality measurement and improvement. “It involves only assessing those core issues that are the most critical to providing high-quality care and improving individual outcomes” (CMS, 2019e, para 1). CMS uses QMs to monitor compliance with Medicare standards in the laboratories, hospitals, nursing homes, home health agencies, ESRD facilities, hospices, and other facilities serving Medicare and Medicaid beneficiaries. The results of oversight are made available to beneficiaries, providers/suppliers, researchers, state agencies, and other stakeholders with the goal of improving health care purchasing of services by providing information about health care quality (CMS, 2019c). Two units within CMS are responsible for most of its quality activities—Center for Clinical Standards and Quality (CCSQ), the older unit, and CMS Innovation Center, established in 2010 by the Affordable Care Act (ACA). The CCSQ coordinates quality-related activities with outside organizations, monitors the quality of Medicare and Medicaid programs, and evaluates the success of interventions (CMS, 2019f). The Center for Medicare Innovation (CMI) (same as the Center for Medicare and Medicaid Innovation [CMMI]) has a greater focus on the role of payment models to improve quality than CCSQ. “The purpose of the CMI is to test innovative payment and service delivery models to reduce program expenditures ... while preserving or enhancing the quality of care furnished to individuals” (CMS, 2019g, para 2). In selecting models, CMS gives preference to models that also improve the coordination, quality, and efficiency of health care services furnished. The Medicare Health Outcomes Survey (HOS) is another important CMS quality activity. CMS, in collaboration with the National Committee for Quality Assurance (NCQA), launched the HOS in 1998 to study the outcomes of Medicare-managed care. The Medicare Health Outcomes Survey (HOS) is the first patient-reported outcomes measure used in Medicare managed care. The goal of the Medicare HOS is to gather valid, reliable, and clinically meaningful health status data from the Medicare Advantage (MA) program to use in quality improvement activities, pay for performance, program oversight, public reporting, and to improve health. All managed care organizations with Medicare contracts must participate. (CMS, 2019h, para 1)
Agency for Healthcare Research and Quality The Agency for Healthcare Research and Quality (AHRQ) is located in the DHHS. It is the designated federal agency for improving the safety and quality of the U.S. health care system. The AHRQ develops the knowledge, tools, and data to improve the health care system and help consumers, policy makers, and health care professionals make informed health decisions. The AHRQ mission is“to produce evidence to make health care safer, higher quality, more accessible, equitable, and affordable, and to work within the U.S. Department of Health and Human Services and with other partners to make sure that the evidence is understood and used” (AHRQ, 2019a, para 5). The AHRQ leads the National Quality Strategy, which is a“national effort to align public- and private-sector stakeholders to achieve better health and health care for all Americans” (AHRQ, 2019b, para 1). The AHRQ also produces the annual National Healthcare Quality Report and the National Healthcare Disparities Report, each mandated by Congress and, since 2014, integrated into a single document. The results of these reports can be queried online (AHRQ, 2019c). AHRQ is responsible for three major health care data systems that aid in examining health care quality: •
Medical Expenditure Panel Survey (MEPS) MEPS is a set of large-scale surveys of families and individuals, their medical providers, and employers across the United States. MEPS is the most complete source of data on the cost and use of health care and health insurance coverage.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 230
3/19/20 10:54 AM
7
•
•
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
231
Consumer Assessment of Healthcare Providers and Systems (CAHPS) CAHPS supports research on the patient experience with health care and assists organizations to improve the quality of care. Healthcare Cost and Utilization Project (HCUP) HCUP is a family of health care databases that includes the largest collection of longitudinal hospital care data in the United States, with all-payer, encounter-level information beginning in 1988. These databases enable research on a broad range of health policy issues, including cost and quality of health services, access to health care, and health care outcomes in national, state, and local markets.
The AHRQ is charged with disseminating scientific findings about clinical practice guidelines and facilitating public access to information on the quality of health care. AHRQ research provides evidence-based information on health care outcomes; quality; and health care cost, use, and access. The information helps health care decision makers—patients and clinicians, health system leaders, purchasers, and policy makers—make more informed decisions and improves the quality of health care services. Beginning in 2005, the AHRQ’s research agenda reflected an emphasis on translation of research into practice. The AHRQ developed the Systematic Review Data Repository, an open-access repository of data abstracted from primary studies included in systematic reviews, which is currently administered by Brown University (AHRQ, 2019a). The AHRQ awards grants and contracts to researchers at universities and other research institutions across the country. Researchers are funded to conduct systematic, comprehensive analyses and syntheses of the scientific literature and to develop reports and technology assessments based on the research-supported evidence (i.e., clinical practice guidelines). To ensure that report findings are translated into improvements in clinical practice, the AHRQ enlists partners, such as specialty societies and health systems, which use the findings of evidence-based practice centers to develop tools and materials that will improve the quality of care. The AHRQ also funds training and education. It provides free continuing education events in the areas of comparative effectiveness, quality and patient safety, and prevention/ care management (AHRQ, 2019a).
Centers for Disease Control and Prevention The CDC, located in the DHHS, is the nation’s primary government agency for developing disease prevention and control initiatives and health promotion and educational activities. In terms of health care quality, it has a particularly important role in the control of health care-associated infection through the Division of Healthcare Quality Promotion (DHQP). The DHQP is charged with protecting patients and health care personnel and promoting safety, quality, and value in the health care system. Among the DHQP priorities are the following: •
•
• •
Measuring, validating, interpreting, and responding to data relevant to patient safety, including healthcare-associated infections (HAIs); antimicrobial resistance; adverse drug events; blood, organ and tissue safety; immunization safety; and other related adverse events or medical errors in health care affecting patients and health care personnel Investigating and responding to outbreaks and emerging antimicrobial-resistant pathogens and infections among patients or associated with the health care environment Identifying and evaluating the efficacy of interventions designed to prevent HAIs or antimicrobial resistance, related adverse events, and medical errors Promoting clinical microbiology laboratory quality (CDC, 2019a)
Goldsteen74024_07_CH07_215-272_03-18-20.indd 231
3/19/20 10:54 AM
232
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
The DHQP provides extensive information on infection control guidelines, infectious disease outbreak management, antimicrobial resistance, laboratory practice, sterilization and disinfection, and surveillance. The CDC further offers advice and consultation to health care providers or regional health departments on matters relating to infection control. It also operates a free rapid notification system through which time-sensitive email messages about important health care events (e.g., outbreaks, product recalls) and publications (e.g., new health care guidelines) are sent to persons active in the prevention of HAIs and antimicrobial resistance (CDC, 2019a). The DHQP’s Healthcare Infection Control Practices Advisory Committee (HICPAC) is a federal advisory committee made up of 14 external infection control experts who provide advice and guidance to the CDC in regard to the practice of health care infection control, strategies for surveillance, and prevention and control of HAIs in U.S. health care facilities. One of the primary functions of the committee is to issue recommendations for preventing and controlling HAIs in the form of practice guidelines, resolutions, and informal communications (CDC, 2019b).
National Institutes of Health The National Institutes of Health (NIH, 2019) is a primary source of funding for medical and behavioral research in the United States. NIH, within the DHHS, funds a broad array of extramural projects, grants, contracts, and cooperative agreements conducted primarily by universities, hospitals, and other research institutions. Much of the patient-oriented research includes studies on the development of new technologies, human disease mechanisms, therapeutic interventions, and clinical trials. Other clinical research includes epidemiological and behavioral studies, outcomes research, and health services research. The NIH is the source of much funding for clinical outcomes studies that are used for evidence-based medicine and clinical practice guidelines.
Health Care Accrediting Organizations (Private, Nonprofit) By setting and monitoring quality standards for health care organizations, the accrediting organizations have a great deal of influence on quality assurance and improvement in health care. This is particularly true because of the relationship between the CMS certification process and accreditation by a CMS-approved organization such as The Joint Commission. CMS has Conditions of Participation (CoPs), which are federal regulations that health care organizations must be certified as meeting. CMS certification can be established directly through a survey conducted for CMS by a state agency. Or, more commonly, CMS certification may be granted by accrediting organizations such as The Joint Commission or DNV GL Health care that have CMS “deemed status” and can “deem” that a health care organization meets CMS requirements (American Society for Healthcare Engineering of the American Hospital Association, 2019). The CoPs and Conditions for Coverage (CfCs) set by CMS are standards that CMS considers essential for improving quality and protecting the health and safety of Medicare and Medicaid beneficiaries (CMS, 2012). The health care accrediting organizations such as The Joint Commission aid CMS in maintaining these standards. Through its approval process, CMS tries to ensure that the standards of approved accrediting organizations meet or exceed the Medicare standards set forth in the CoPs and the CfCs (CMS, 2012).
The Joint Commission The Joint Commission (formerly The Joint Commission on Accreditation of Healthcare Organizations or JCAHO) is the oldest and largest health care accrediting organization in the country, accrediting nearly 21,000 health care organizations in the United States, including general, pediatric, psychiatric, rehabilitation and critical access hospitals; home
Goldsteen74024_07_CH07_215-272_03-18-20.indd 232
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
233
care organizations; nursing homes and rehabilitation centers; behavioral health care organizations; ambulatory care providers; and independent or freestanding clinical laboratories. It accredits about 77% of all U.S. hospitals and about 88% of accredited hospitals. The Joint Commission is governed by a 21-member board of commissioners, which includes physicians, administrators, nurses, employers, quality and innovation experts, and educators. • •
Joint Commission state-of-the-art standards are the basis of an objective evaluation process and can help organizations measure, assess and improve performance. The standards focus on important patient, individual, or resident care and organization functions that are essential to providing safe, high-quality care.
The Joint Commission standards are developed with input from health care professionals, providers, subject matter experts, consumers, and government agencies (including the CMS). They are informed by scientific literature and expert consensus. New standards are added only if they relate to patient safety or quality of care, have a positive impact on health outcomes, meet or surpass law and regulation, and can be accurately and readily measured (Joint Commission, 2019a). The Joint Commission aims to provide standards for quality that ensure both patient and staff safety. Accreditation is designed to ensure quality care, maintain infection control, and help reduce the occurrence of medical errors. The performance measurement tools used by The Joint Commission have developed over the years. For example, in 1986, The Joint Commission (then JCAHO) developed the Indicator Measurement System (IMS). It had six sets of performance measures, for perioperative care, obstetrical care, trauma care, oncology care, infection control, and medication use. This system was not implemented, but it set the stage for the current ORYX initiative, which is based on multiple measurement systems. As described by The Joint Commission, the ORYX system: • • •
The Joint Commission’s ORYX initiative integrates performance measurement data into the accreditation process. ORYX measurement requirements support Joint Commission-accredited organizations in their quality improvement efforts. The Joint Commission continues to align measures as closely as possible with the Centers for Medicare & Medicaid Services (CMS). (The Joint Commission, 2019b, para 1)
The Joint Commission has been engaged with CMS since 2003 to align each organization’s QMs. The result is one common set of measures in the Specifications Manual for National Hospital Inpatient Quality Measures (now in version 5.6). The goal is to minimize data collection efforts for hospitals and focus efforts on the use of data to improve health care delivery and quality (The Joint Commission, 2019c).
National Committee for Quality Assurance Founded in 1990, NCQA accredits health plans (mainly health insurance companies) and helps government and private-sector clients measure and improve quality. The NCQA mission is “to improve the quality of health care” by applying evidence-based standards of care to health plans and the doctors who provide health services for their beneficiaries. Its accreditation is a “rigorous assessment of health plans’ structure and process, clinical quality and patient satisfaction. More than 173 million people are enrolled in NCQA-accredited health plans” (NCQA, 2019a, para 3). NCQA’s slogan is “the right care, at the right time, every time.”
Goldsteen74024_07_CH07_215-272_03-18-20.indd 233
3/19/20 10:54 AM
234
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
The NCQA creates standards and guidelines to measure performance and shares these with stakeholders, including the public. It summarizes these activities as follows: Measure. Analyze. Improve. Repeat: This is the heart of our work. We make measures and standards that health care professionals use to identify areas they can improve. Public reporting of performance against our measures and standards becomes the focus for groups we evaluate and for their customers. Releasing results to the public helps everyone set higher goals and continue improving. (NCQA, 2019a, para 4) The NCQA has developed the Healthcare Effectiveness Data and Information Set (HEDIS) to measure health plan performance. HEDIS has more than 90 measures across six domains of care: • • • • • •
Effectiveness of care Access/availability of care Experience of care Utilization and risk-adjusted utilization Health plan descriptive information Measures collected using electronic clinical data systems
HEDIS obtains data from administrative records, medical records, and surveys of health plan members. Some HEDIS measures are collected through the Medicare HOS and through CAHPS. About 190 million people are enrolled in plans that report HEDIS results (NCQA, 2019b).
Other CMS-Approved Accrediting Organizations Other CMS-approved, but much smaller, accrediting bodies for hospitals are the American Osteopathic Association’s Healthcare Facilities Accreditation Program (HFAP); the Center for Improvement in Healthcare Quality (CIHQ); and DNV GL (DNV GL Health Care, 2019). The Accreditation Association for Ambulatory Health Care, the American Association for Accreditation of Ambulatory Surgery Facilities, the Community Health Accreditation Partner, Institute for Medical Quality, National Dialysis Accreditation Commission, The Compliance Team, and the Accreditation Commission for Health Care are CMS approved for nonhospital health care settings, including ambulatory surgery centers, dialysis centers, and hospices (CMS, 2019b).
Other Private Organizations There are also a number of private, nonprofit organizations providing health care performance information to consumers and purchasers. Both the consumers and the purchasers of hospital services, such as insurance companies, employers, and the Medicare program, have a vital interest in the quality of those services. However, until fairly recently, consumers and purchasers had very limited ability to evaluate the quality of a hospital’s performance on any aspect of care. In the late 1990s, three organizations—the National Quality Forum (NQF), the Leapfrog Group, and the Institute for Healthcare Improvement (IHI)— focused on rectifying this problem by developing standard measures of hospital quality and disseminating information about hospital performance to purchasers and consumers. Since then, transparency through publicly available reports has become a national standard in all organizations related to health care quality, including CMS, AHRQ, The Joint Commission, and CDC.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 234
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
235
National Quality Forum The NQF is a nonprofit organization created to improve the quality of American health care by building consensus on national priorities and goals for performance improvement, endorsing national consensus standards for measuring and publicly reporting on performance, and promoting the attainment of national goals through education and outreach programs (NQF, 2012). Established in 1999 as a partnership between public and private stakeholders, the NQF aims to promote health care quality improvement by developing the intellectual framework for nationally standardized performance measures and quality data reporting so that individual hospitals and health systems can be compared. NQF shares the goal of increasing the value of health care—including improving patient safety and quality and lowering health care costs—with many other organizations. However, NQF has developed two distinct, but complementary, roles in this endeavor: •
•
Standardized performance measures developed through evidence-based research and input from a broad array of stakeholders. This work is recognized by the Office of Management and Budget (OMB); Building consensus among public and private health care leaders and providing proactive advice about the first National Quality Strategy (NQF, 2019a, para 2).
The NQF encourages the use of standardized measures by consumers and stakeholders within the health care system. However, it should be noted that the NQF has no authority to implement its standards, although payers of hospital services, such as insurance companies and the Medicare program, can demand compliance with their standards. Other groups, including the NCQA and the American Medical Association/Physician Consortium for Performance Improvement (PCP) develop the performance measures endorsed by NQF. Other groups, including The Joint Commission and CMS, must require reporting of NQF-endorsed performance measures. Other groups, such as the Quality Improvement Organizations (QIOs) and physician specialty societies, must provide technical assistance to health systems and medical practices that seek to use NQF performance measures to guide their improvement efforts (NQF, 2019a). The NQF enjoys broad participation from health care consumer advocacy groups, public and private purchasers, health care professionals, employers, provider organizations, health plans, accrediting bodies, organized labor, and organizations involved in health care research and quality improvement. The organization is governed by a board of directors representing consumers, purchasers, providers, insurers, health services experts, and representatives from CMS, AHRQ, CDC, and the Health Resources and Services Administration (HRSA). Currently, there are more than 400 member organizations and 5,000 individual members (NQF, 2019b). The NQF seeks not only to promote new guidelines, standards, and QMs to rectify serious and pervasive quality deficiencies, but also to reconcile the redundant and often incompatible guidelines, standards, and reporting measures offered by various organizations and agencies dedicated to health care quality improvement. The NQF consensus process was developed pursuant to and in accordance with the National Technology Transfer Act of 1995 (U.S. OMB Circular A-119). This means that NQF endorsement of hospital performance measures and standards confers on them the special legal status of voluntary consensus standards. This status makes NQF-endorsed recommendations more easily adopted for use by Medicare, Medicaid, and other federally funded health care programs; that is, federal health care programs can require hospitals to adopt NQF recommendations in order to qualify for federal insurance programs (NQF, 2019a).
Goldsteen74024_07_CH07_215-272_03-18-20.indd 235
3/19/20 10:54 AM
236
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
The NQF has issued reports endorsing a set of QMs and patient safety practices. The measures are designed to provide consumers, providers, purchasers, and quality-improvement professionals the tools to evaluate and compare the quality of care in hospitals across the nation using a standard set of measures. The goal is to make data on these performance measures publicly available and thus enable performance-based decisions about hospital selection, create incentives for hospital performance improvement, enhance value-based purchasing, and generally stimulate the improvement of health care (NQF, 2019a).
The Leapfrog Group The Leapfrog Group is a member-supported, nonprofit organization founded in 2000 with the aim of mobilizing employer purchasing power to alert America’s health industry that big leaps in health care safety, quality, and customer value will be recognized and rewarded. In its own words, Leapfrog is a “nonprofit watchdog organization that serves as a voice for health care purchasers, using their collective influence to foster positive change in U.S. health care” (Leapfrog Group, 2019a, para 4). Its stated mission today is “[t]o trigger giant leaps forward in the safety, quality and affordability of U.S. health care by using transparency to support informed health care decisions and promote high-value care”(Leapfrog Group, 2019b, para 5). Leapfrog was founded by the Business Roundtable, and its funding comes from its members. Its 2019 Partners Advisory Committee includes Anthem, WebMD, Allied BioScience, HealthNet, Aetna, UCLA Health, Nemours Children’s Health System, UCLA Health, United Health care, Merck, and Castlight. It has four major programs (Leapfrog Group, 2019): •
•
•
•
Leapfrog Hospital Survey A voluntary survey completed by more than 2,000 hospitals each year providing information on safety, quality, and resource use Leapfrog Hospital Safety Grade A publicly available (www.hospitalsafetygrade.org) letter grade given biannually to all general hospitals (about 2,600) based on their record of safety, including errors, injuries, infections, and accidents. Data are obtained from the Leapfrog Hospital Survey or from CMS, if a hospital does not complete the Leapfrog Hospital Survey. Leapfrog Value-Based Purchasing Program A program, based on the Leapfrog Hospital Survey, that advises health plans, employers, and other large health care purchasers how to choose the highest-value hospitals in individual markets. Data are obtained from the Leapfrog Hospital Survey. Leapfrog Ambulatory Surgery Center Survey A voluntary survey of ambulatory surgery centers to provide information on safety and quality of care
Institute for Healthcare Improvement The IHI is a nonprofit organization, founded in 1991, with a mission “to improve health and health care worldwide” (IHI, 2019a, para 1). It is an explicitly values-driven organization, promoting courage, love, equity, and trust. The IHI developed the Triple Aim framework for optimizing health system performance: improving the patient experience of care, improving the health of populations, and reducing the per capita cost of health care. It has also developed an associated improvement process to solve health care problems: The science of improvement is an applied science that emphasizes innovation, rapid-cycle testing in the field, and spread in order to generate learning about what changes, in which contexts, produce improvements. It is characterized by the combination of expert subject knowledge with improvement methods and tools. It is
Goldsteen74024_07_CH07_215-272_03-18-20.indd 236
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
237
multidisciplinary—drawing on clinical science, systems theory, psychology, statistics, and other fields. (IHI, 2019b, para 2) One of the IHI’s most well-known projects is the 100,000 Lives Campaign. This was a nationwide, 18-month initiative in 2005 to decrease morbidity and mortality in U.S. hospitals by encouraging the adoption of six safety practices: • • • • • •
Deploy rapid response teams ... at the first sign of patient decline. Deliver reliable, evidence-based care for acute myocardial infarction ... to prevent deaths from heart attack. Prevent adverse drug events (ADEs) ... by implementing medication reconciliation. Prevent central line infections ... by implementing a series of interdependent, scientifically grounded steps called the “central line bundle” Prevent surgical site infections ... by reliably delivering the correct perioperative antibiotics at the proper time. Prevent ventilator-associated pneumonia ... by implementing a series of interdependent, scientifically grounded steps including the“ventilator bundle.”(IHI, 2019c, para 4)
After its 100,000 Lives Campaign, the IHI ran the 5 Million Lives Campaign in 2006. The IHI has continued to develop initiatives based on its improvement models and aimed at improving health care quality in facilities and, more recently, in the health care system as a whole. The IHI also has an educational program. The IHI Open School is an online curriculum and community that trains health care professionals and others to participate in the health care improvement process.
Cochrane Collaboration The Cochrane Collaboration is a nonprofit organization based in the United Kingdom and working worldwide. It is dedicated to producing evidence that improves health care quality through the development of systematic reviews and other synthesized research evidence. Its mission “is to promote evidence-informed health decision-making by producing high-quality, relevant, accessible systematic reviews and other synthesized research evidence” (Cochrane Collaboration, 2019b, para 3). With review groups in 43 countries, there are currently over 7,500 Cochrane Systematic Reviews in the Cochrane Library. In order to make the evidence widely accessible, the Cochrane Collaboration translates the plain-language summaries into 14 languages (Cochrane Collaboration, 2019b).
Patient-Centered Outcomes Research Institute Patient-Centered Outcomes Research Institute (PCORI) is a nonprofit corporation authorized under the Affordable Care Act of 2010. PCORI is funded by the Patient-Centered Outcomes Research Trust Fund, which receives income from three sources: appropriations from the general fund of the U.S. Treasury, transfers from CMS trust funds, and a fee assessed on private insurance and self-insured health plans (the PCOR fee). PCORI’s mission is to help people make informed health care decisions, and improve health care delivery and outcomes, “by producing and promoting high-integrity, evidence-based information that comes from research guided by patients, caregivers, and the broader health care community” (PCORI, 2019, para 3). PCORI’s 21-member governing board represents a wide range of perspectives and expertise in clinical health sciences research, including epidemiology, decisions sciences, health economics, and statistics.
Health Care Professional Associations The health care professional associations, particularly the American Medical Association, the American Hospital Association (AHA), and the American Nurses Association, continue
Goldsteen74024_07_CH07_215-272_03-18-20.indd 237
3/19/20 10:54 AM
238
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
to be at the heart of quality improvement. The organizations contribute especially to the development of clinical practice guidelines and quality of care standards.
Advocacy Organizations Organizations such as the American Heart Association, the American Diabetes Association, the Asthma and Allergy Foundation of America, and the American Cancer Society play a role in the development of clinical practice guidelines and quality of care standards. We now take a closer look at one important health care quality problem and the efforts to improve performance in this area—healthcare-associated infections.
Health Care-Associated Infections: An Example of Health Care Quality Improvement Patient Safety and the Patient Safety Movement Health care interventions can have adverse, as well as beneficial, effects. Some adverse effects are patient safety issues, which include errors, injuries, and infections, and can occur in any health care setting—hospitals, clinics, nursing homes, and others. Patient safety problems affect a substantial number of patients. In 2019, it was estimated that in the United States • • •
440,000 people die every year from hospital errors, injuries, accidents, and infections. Each year, one out of every 25 hospital patients develops a preventable infection. A hospitalized Medicare patient has a one in four chance of experiencing injury, harm, or death (Leapfrog Hospital Safety Grade, 2019).
The patient safety movement of the 1990s led to a great deal of interest in improving the quality of health care delivery by reducing errors, injuries, and infections. Quality assessment and quality improvement related to patient safety respond to the question: Did the health care intervention have an adverse effect on the patient? The patient safety movement applied methods borrowed from other industries and pioneered by W. Edwards Deming. Deming, an American statistician, was considered the father of the modern quality assurance movement. He developed his system following the end of World War II. Unable to get a hearing in this country, he went to Japan. His methods, designated Statistical Process Control (SPC) and Total Quality Management (TQM), strongly influenced the rebirth and eventual massive expansion of Japanese industry post–World War II. Patient safety has been defined by the IOM (2000) as“freedom from accidental injury; ensuring patient safety involves the establishment of operational systems and processes that minimize the likelihood of errors and maximize the likelihood of intercepting them when they occur” (p. 211). Therefore, patient safety encompasses all events and situations that result in accidental harm to patients, including medication errors, surgical mistakes, falls, improper use of medical devices, and health care-associated (nosocomial) infections. The IOM report To Err Is Human (2000) has played a major role in bringing the issue of patient safety to national attention. The Report converted an issue of gradually growing professional awareness over a great deal of time to one of substantial public concern in a manner and pace unprecedented in modern experience with matters of health care quality. The epidemiologic finding that more than one million injuries and nearly 100,000 deaths occur in the United States annually as a result of mistakes in medical care came from studies nearly a decade old. But this was new information for the public, and it resonated strongly. (Leape, Berwick, & Bates, 2002, p. 501)
Goldsteen74024_07_CH07_215-272_03-18-20.indd 238
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
239
To Err Is Human brought a new perspective to health care quality assurance by supporting the importation of industrial quality-improvement practices into health care settings. Modeled on Charles Perrow’s analysis of the Three Mile Island accident (Perrow, 1984), the report advocates a systems approach to health care improvement in order to understand and modify the conditions that contribute to errors. The authors conclude: The application of human factors in other industries has successfully reduced errors. Health care has to look at medical error not as a special case of medicine, but as a special case of error, and to apply the theory and approaches already used in other fields to reduce errors and improve reliability. (IOM, 2000, p. 66) Next, we examine an example of the adverse consequences that may result from health care interventions: healthcare-associated infections. HAIs have been the focus of immense concern and the target of remarkable prevention efforts.
Healthcare-Associated Infections HAIs are infections caused by bacteria, fungi, viruses, or other, less common, pathogens, and acquired by patients receiving care for another condition. Also called nosocomial infections, these are infections that were not present or incubating in the patient at the time of admission to the health care facility. Patients may acquire HAIs in hospitals, ambulatory surgical centers, ESRD facilities, and long-term care facilities. HAIs are a substantial health problem in the United States. Although there is no infection rate that is held up as the “gold standard,” other industries would not accept the failure rates that health care facilities accept in terms of infections. In other industries, the goal for errors that are as costly as HAIs and that can be fatal or disabling would be close to zero. The DHHS summarizes the magnitude of the issue: HAIs are a significant cause of illness and death—and they can have devastating emotional, financial, and medical consequences. At any given time, about one in 25 inpatients have an infection related to hospital care. These infections lead to the loss of tens of thousands of lives and cost the U.S. health care system billions of dollars each year. (DHHS, Office of Disease Prevention and Health Promotion, 2019, para 2)
Challenges to the Prevention and Control of HAIs It is an understatement to say that preventing the occurrence of HAIs is challenging. The microorganisms that cause infection are ubiquitous in health care settings. Patients are often immunocompromised to begin with and, while in the health care setting, are often undergoing invasive medical processes that provide pathways for microorganisms to enter—including placement of catheters and ventilators and intravenous procedures. Health care staff members may inadvertently assist infective microorganisms as they go from patient to patient. Every staff member—maintenance, cleaning, and food service; laboratory, imaging, and other technician; nurse, aide, physician, and resident—is a possible carrier. In the course of performing their jobs, health care staff members move from patient to patient, potentially exposing them to pathogens acquired from prior contact with contaminated persons, surfaces, and equipment. A single lapse in infection control protocol on a single day by just one of the many people who come into contact with a patient during a hospitalization may result in exposure of that patient to an infective agent. The increasing rate of antimicrobial resistance among the major infective organisms compounds the problem of HAI control, should a patient develop an infection. Bacteria,
Goldsteen74024_07_CH07_215-272_03-18-20.indd 239
3/19/20 10:54 AM
240
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
fungi, and even viruses can become resistant to drugs, leaving fewer and fewer options for treatment if an infection occurs. The development of antimicrobial resistance is largely associated with antibiotic overuse or misuse through the prescription of the wrong drug or the wrong dose or the wrong duration (U.S. Congress, Office of Technology Assessment, 1995). For these reasons, it is easy to conclude that health professionals seeking to prevent and control infection are at a disadvantage compared with their microscopic companions causing infection.
Brief History of HAI Prevention and Control in the United States As with other clinical quality-improvement efforts, the story of HAI prevention and control includes: • • • • •
Conducting clinical research studies and synthesizing their results in systematic reviews Developing HAI practice guidelines from the systematic reviews Developing support within the health care community to implement the HAI practice guidelines Training and developing professionals to implement and monitor practice guidelines Reinforcing implementation of HAI practice guidelines through monitoring and feedback
Infection-control programs are the foundation of efforts to prevent HAIs. They have their origin in the nosocomial Staphylococcus aureus infection outbreaks of the 1950s and the subsequent recommendation of the AHA to include infection surveillance as a regular hospital function (Haley et al., 1985). In the 1950s, events such as epidemic penicillin-resistant S. aureus outbreaks, especially in hospital nurseries, had raised concern about HAIs, and by the 1960s CDC epidemiologists and hospital-based clinicians were developing techniques to identify and prevent HAIs, but with a limited number of hospitals. Two notable projects, begun in the 1960s, laid the evidence-based foundation for HAI prevention and control: •
•
A national network of hospitals volunteered to conduct HAI surveillance using CDC methods and to report monthly to the CDC. This was the National Nosocomial Infection Surveillance Program (later changed to the National Healthcare Safety Network). The Comprehensive Hospital Infections Project was located in eight community hospitals that served as laboratories for CDC HAI control activities. Hospital staff worked closely with the CDC to investigate how infections developed and what clinical practices could prevent infection (Dixon, 2011).
By 1970, these two projects had begun to provide evidence that HAIs could be prevented by changing clinical practice patterns. However,“CDC determined that a rigorous scientific assessment of the effectiveness of infection control programs would be necessary to propel widespread adoption of hospital-based programs. That decision led to the Study on the Effectiveness of Nosocomial Infection Control (SENIC), a rigorous assessment of infection control effectiveness that compared outcomes in hospitals with and without CDC-style infection control programs” (Dixon, 2011, p. 60). In the early 1970s, SENIC was implemented with 338 randomly selected U.S. hospitals that were stratified by geography, inpatient bed capacity, and teaching status. About half of the hospitals had infection surveillance and control programs. The study found that
Goldsteen74024_07_CH07_215-272_03-18-20.indd 240
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
241
infection rates were reduced by about 32% among hospitals with a strong commitment to infection control, which included a full-time infection-control practitioner per 250 beds and a trained hospital epidemiologist (Hospital Infections Program, National Center for Infectious Diseases, CDC, 1992). These results led to a broad acceptance of infection-control guidelines and to The Joint Commission’s mandate for hospitals to have an infection control program: When (SENIC) showed that hospitals with infection control programs had significantly lower rates of HAIs than did hospitals without such programs, expectations for hospital programs changed. With strong scientific evidence supporting the value of such programs, accrediting organizations such as the Joint Commission on Accreditation of Hospitals (now The Joint Commission) mandated that accredited hospitals have infection control programs similar to those recommended by CDC and the professional organizations of hospital epidemiologists and infection control practitioners. The Joint Commission made this an accreditation requirement in 1976. (Dixon, 2011, pp. 60–61) The interest in preventing HAIs after the success of SENIC led to the continued development of HAI practice guidelines and efforts to implement them universally in health care settings.
HAI Prevention and Control Today Today, as in the past, the CDC has led efforts in the United States to prevent and control HAIs, largely through the units listed in Box 7.2.
Box 7.2 CDC Units With Major Roles in Preventing and Controlling HealthcareAssociated Infections, 2019 •
•
• •
National Healthcare Safety Network (NHSN; formerly, the National Nosocomial Infections Surveillance System or NNISS) The nation’s most widely used HAI tracking system to monitor progress in prevention and control of prevailing HAIs. In 2017, most U.S. health care facilities were required to report HAI data to NHSN in order to participate in various Quality Reporting Programs for CMS. Emerging Infections Program (EIP) A network for surveillance, prevention, and control of emerging infectious diseases that includes 10 state and local health departments, academic institutions, public health and clinical laboratories, infection control professionals, and health care providers (Division of Preparedness and Emerging Infections, 2019). Healthcare Infection Control Practices Advisory Committee (HICPAC) An advisory group of HAI experts, appointed from outside the federal government. Division of Healthcare Quality Promotion (DHQP) A division within the National Center for Emerging and Zoonotic Infectious Diseases focused on HAIs and other health care safety issues affecting patients and workers. DHQP includes NHSN, EIP, and HICPAC.
HAI, healthcare-associated infections.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 241
3/19/20 10:54 AM
242
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Through the units listed in Box 7.2, the CDC has supported the prevention and control of HAIs in the following ways:
Conducting HAI Clinical Research That Is Synthesized in Systematic Reviews The CDC funds research to prevent and eliminate HAIs through DHQP’s Safety and Healthcare Epidemiology Prevention Research Development (SHEPheRD) Program. The DHQP also has the Prevention Epicenters Program, in which DHQP researchers collaborate with academic investigators to conduct innovative HAI studies (CDC, 2019c).
Developing HAI Practice Guidelines From the Systematic Reviews The CDC assists with guideline development through HICPAC, a federal advisory committee whose members provide advice and guidance to DHHS and CDC regarding HAI practice guidelines, as well as HAI surveillance, prevention, and control. Appointed by the Secretary of DHHS, HICPAC has 14 voting members who are experts in HAI-related areas but are not federal employees (CDC, 2019b). HICPAC and DHQP work with the professional infection-control organizations, particularly the Association for Professionals in Infection Control and Epidemiology (APIC), the Society for Healthcare Epidemiology of America (SHEA), and the Surgical Infection Society (SIS), to continually generate, update, and publish infection control guidelines based on expert review, assessment, and synthesis of current research and integration of new findings. Thus, the infection-control guidelines are evidence-based, having been distilled from the research on each infection-control area. The guidelines reflect the current state of knowledge about infective agents—detection, prevention of their transmission, and treatment—derived from research in the basic and clinical sciences. The guidelines are based on evidence from thousands of scientific studies.
Training and Developing Professionals to Implement and Monitor HAI Practice Guidelines The CDC has developed and made available a plethora of training resources for health care facilities, including State-based HAI Prevention Activities, Prevention Toolkits, Infection Control Assessment Tools, and Laboratory Resources (CDC, 2019d). Also, the DHQP administers the HAI Guidelines Library, which contains the most recent practice guidelines as well as guidelines that have been“retired.”These are publicly available through the Guidelines Library portal (CDC, 2019e).
Reinforcing Implementation of HAI Practice Guidelines Through Monitoring and Feedback Two complementary HAI surveillance systems—the NHSN and the EIP—provide data for reports that track HAI progress and problems: CDC’s NHSN is the nation’s most widely used HAI tracking system. NHSN provides facilities, states, regions, and the nation with data needed to identify problem areas, measure progress of prevention efforts, and ultimately eliminate HAIs. In addition, NHSN allows health care facilities to track antimicrobial use and resistance, blood safety errors and important health care process measures such as health care personnel influenza vaccine status and infection control adherence rates. (CDC, 2019f, para 1) Using these data, the NHSN produces annual and special reports on HAI infection rates and their trends in acute care hospitals, critical access hospitals, inpatient rehabilitation facilities, and long-term acute care hospitals (CDC, 2019f). The rates for each health care facility are reported back to that facility to assist in its HAI quality-improvement initiatives and accreditation requirements. These reports are intended to document the status of HAI prevention and control—nationwide, in the states, and in health care facilities—and to motivate continued improvement.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 242
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
243
The NHSN also provides the data for the online, consumer-oriented Hospital Compare, which permits public scrutiny of the HAI issue. The site provides hospital-level information on HAIs and other quality indicators for over 4,000 Medicare-certified hospitals (Medicare. gov, 2019). Hospital Compare makes it possible for the public to compare hospital infection rates and encourages improvements in individual facilities and the system, as a whole, through public oversight.
Developing Support Within the Health Care Community to Implement HAI Practice Guidelines A hallmark of the effort to prevent and control HAIs is cooperation and coordination among the CDC and other federal agencies, health care facilities, voluntary professional organizations, and state and local public health departments. At the federal level, the CDC develops HAI tools, recommendations, and programs in collaboration with CMS, AHRQ, and the Office of the Assistant Secretary for Health (OASH) (CDC, 2019c). In addition, the DHHS Steering Committee for the Prevention of Healthcare-Associated Infections, established in July 2008, developed the HHS Action Plan to Prevent Healthcare-Associated Infections, a “roadmap for HAI prevention in acute care hospitals” (DHHS, 2019, para 1). CDC collaborators outside the federal government include the AHA, The Joint Commission, Leapfrog, the IHI, NQF, universities, and state and local public health departments. The success of collaboration is reflected in the number of health care facilities that participate in CDC’s HAI monitoring activities. More than 25,000 health care facilities are tracking HAIs through the NHSN system. They include acute care, long-term care, psychiatric, and rehabilitation hospitals; outpatient dialysis centers; ambulatory surgery centers, and nursing homes (CDC, 2019g).
How Successful Have HAI Prevention Efforts Been? The NHSN produces an annual HAI progress report for states and the nation. The 2017 National and State Healthcare-Associated Infections (HAI) Progress Report provides a summary of select HAIs in the four health care settings in which data are obtained: acute care hospitals, critical access hospitals, inpatient rehabilitation facilities, and long-term acute care hospitals. For each of the four health care settings, the report consists of national factsheets and detailed technical tables. The factsheets provide a high-level view of HAIs at a national level, while the technical tables include additional statistics about HAIs, reporting mandates, and data validation efforts in each state and select US territories (CDC, 2019h). The report covers the following HAIs and the progress in prevention that has been made since 2016, using 2015 baseline and risk-adjustment models. Practice guidelines for each of these HAIs can be found in the CDC’s Guidelines Library (CDC, 2019e). • • • • • • •
Central Line-Associated Bloodstream Infections (CLABSI) Surgical Site Infection (SSI) From Colon Surgery SSI From Abdominal Hysterectomy Catheter-Associated Urinary Tract Infection (CAUTI) Ventilator-Associated Events (VAE) Clostridium difficile Events (C. diff) Methicillin-resistant Staphylococcus aureus bacteremia (MRSA)
Table 7.4 presents the findings from the 2017 Progress Report for acute care hospitals, which are the largest group of health care facilities monitored by the NHSN. The 2017 report and previous reports indicate that progress is being made in preventing and controlling HAIs. In
Goldsteen74024_07_CH07_215-272_03-18-20.indd 243
3/19/20 10:54 AM
244
■
I
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
2017, compared with 2016, there was a decline in all HAIs except SSIs for colon surgery and abdominal hysterectomies. Other highlights of the 2017 Progress Report are as follows: • • • • • •
An approximately 9% statistically significant decrease in CLABSI between 2016 and 2017 An approximately 5% statistically significant decrease in CAUTI between 2016 and 2017 An approximately 3% statistically significant decrease in VAE between 2016 and 2017 An approximately 1% statistically significant decrease in SSI related to the 10 select procedures tracked in the report between 2016 and 2017 An approximately 8% statistically significant decrease in MRSA bacteremia between 2016 and 2017 An approximately 13% statistically significant decrease in C. diff infections between 2016 and 2017 (CDC, 2019h)
The NHSN data used in the National and State Healthcare-Associated Infections (HAI) Progress Report are also available by hospital online at Hospital Compare, a CMS website (Medicare.gov, 2019). This is a public site that produces information about QMs for individual hospitals in many areas, including HAIs. See Table 7.5 for an example. Three hospitals in a region were entered into Hospital Compare and then the site was queried for a report on ICU CLABSI infections in those hospitals.
TABLE 7.4 National Trends in HAIs for Acute Care Hospitals, 2017
HAI Type
# of Facilities That Reported Data to CDC’s NHSN, 2017
2017 National SIR vs. 2016 National SIR
2017 National SIR vs. National Baseline
2017 National SIR
CAUTI
3,679
↓–5%
↓–12%
0.88
C. diff events
3,669
↓–13%
↓–20%
0.80
CLABSI
3,576
↓–9%
↓–19%
0.81
SSI: Colon surgery
3,158
3% no difference
↓–9%
0.91
SSI: Abdominal hysterectomy
2,970
2% no difference
↓–11%
0.89
MRSA bacteremia
3,662
↓–8%
↓–14%
0.86
VAEs
2,046
↓–3%
↓–5%
0.95
CAUTI, catheter-associated urinary tract infection; CLABSI, central line-associated bloodstream infections; HAI, healthcare-associated infections; NHSN, National Healthcare Safety Network; MRSA, methicillin-resistant Staphylococcus aureus; SIR, standardized infection ratio; SSI, surgical site infection, VAE, ventilator-associated events. NOTE: HAIs are infections patients can get while receiving medical treatment in a health care facility. Working toward the elimination of HAIs is a CDC priority. The standardized infection ratio (SIR) is a summary statistic that can be used to track HAI prevention progress over time; lower SIRs are better. The infection data are reported the NHSN. HAI data for nearly all U.S. hospitals are published on the Hospital Compare (n.d.) website . This report is based on 2017 data, published in 2019 and uses the 2015 baseline and risk-adjusted models. SOURCE: Centers for Disease Control and Prevention. (2019e). 2018 National and state healthcare-associated infections progress report. Retrieved from https://www.cdc.gov/hai/data/portal/progress-report.html#anchor_1552573635018
Goldsteen74024_07_CH07_215-272_03-18-20.indd 244
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
245
TABLE 7.5 CLABSI in ICUs and Select Wards, Acute Care Hospitals, 2017 # of Infections Reported (A)
Central Line Days
Predicted # of Infections (B)
SIR (A/B)
Evaluation
Hospital A
0.000
1,830
1.704
0.000
No different than national benchmark
Hospital B
1.000
7,159
6.774
0.148
Better than the national benchmark
Hospital C
13.000
23,405
24.972
0.521
Better than the national benchmark
SIR national benchmark = 1. Lower SIRs are better. A score of (0)—meaning no CLABSIs—is best. CLABSI, central line–associated bloodstream infections; SIR, standardized infection ratio. SOURCE: Medicare.gov. (2019). Hospital compare: Complications & death, infections. Retrieved from https://www.medicare.gov/ hospitalcompare/search.html
Future of HAI Prevention and Control A great deal of progress in reducing HAIs has been made since the SENIC study in the 1970s. This is undoubtedly the result of the prevention and control initiatives put in place by the CDC and its collaborators, which have moved HAI prevention beyond a small group of facilities to the health care system, as a whole. There are “more eyes on the problem” now. There is more formal oversight. All Joint Commission and CMS-accredited health care facilities must report HAIs to the NHSN in order to maintain accreditation. And these data are publicly available for inspection by other stakeholders, including payers and policy makers. In addition, consumers can compare HAI rates among hospitals, a measure that creates informal oversight. Finally, training and supportive resources from the CDC are readily available to health care facilities, including quality-improvement expertise to individual hospitals. Despite these achievements, however, the HAI rate is still not near zero. There are two major explanations: • •
Infection-control guidelines are not fully implemented in all health care facilities; and Some HAIs may not be 100% preventable with our current knowledge.
Each issue is briefly discussed next. Research suggests that when hospitals fully implement the infection-control guidelines, the rate of HAI falls dramatically, in some cases to almost zero, as desired. We know that the infection-control guidelines have dramatically reduced nosocomial infection rates when they have been fully implemented, for instance within individual hospitals and in some European countries (e.g., IHI, 2012; Muto et al., 2003). Therefore, improving compliance with the guidelines should be remarkably effective in reducing HAIs in U.S. hospitals. Yet this is not necessarily easy. Although a great deal has been done to develop HAI practice guidelines and train infection-control professionals, the more difficult task is to ensure that infection-control guidelines are implemented, fully and appropriately, in each U.S. hospital (e.g., Goldsteen, Goldsteen, Gladwin, & Jefferson, 2004). Within hospitals, competing priorities, declining budgets, and entrenched behaviors and beliefs about infection control inhibit the implementation of practices that research has shown prevent HAIs. However, hospitals that have attempted to reduce their HAI rates have demonstrated that two key programmatic elements are necessary: (a) application of quality-improvement methods borrowed from other industries and (b) institutional will. These ingredients must be present for sustained infection control.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 245
3/19/20 10:54 AM
246
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
In addition to ensuring that infection-control guidelines are fully implemented, clinical and technological breakthroughs are needed to improve the guidelines. A recent study was conducted by Umscheid and his colleagues to estimate the proportion of HAIs that are“reasonably preventable” (Umscheid et al., 2011). They found that: As many as 65%–70% of cases of CABSI and CAUTI and 55% of cases of VAP and SSI may be preventable with current evidence-based strategies. CAUTI may be the most preventable HAI. CABSI has the highest number of preventable deaths, followed by VAP. CABSI also has the highest cost impact; costs due to preventable cases of ventilator-associated pneumonia (VAP), CAUTI, and SSI are likely less. (p. 101) The authors concluded that“100% prevention of HAIs may not be attainable with current evidence-based prevention strategies”(although implementing current guidelines still saves tens of thousands of lives and billions of dollars; Umscheid et al., 2011, p. 101). However, new technologies and new discoveries in the basic sciences of genetics, microbiology, biochemistry, and so forth will undoubtedly have a tremendous impact on our ability to detect and prevent transmission of infectious disease organisms in health care settings. They will be used to improve the infection control guidelines and increase the proportion of HAIs that are considered “preventable.” Next, we turn to a short discussion of equity, the second criterion for evaluating health system performance.
EQUITY IN HEALTH CARE Equity is the second criterion used to evaluate the performance of health care systems. Equity or distributive justice is concerned with the fair allocation of benefits and burdens among those who are deserving of care and those who are in a position to pay for it—the two groups may or may not be the same (Aday et al., 1993, p. 120). We are concerned about inequities in access to health care, as well as inequities in the quality of health care—as measured and evaluated by standards established for structure, process, and outcomes. We use disparities in access and quality of health care to indicate inequities.
Equity in Health Care Quality and Access Before the Affordable Care Act Prior to the Affordable Care Act (ACA), the factors consistently associated with inequities in health care access and quality were socioeconomic status (SES), race and ethnicity, and geographic location. Study after study found that people with low income, low education, and low-status occupations; people belonging to minority racial and ethnic groups, particularly African Americans, Native Americans, and Hispanics; and people who lived in rural areas or inner cities were more likely to have poor access to care and poor-quality health care (IOM, 2003).
Equity and the Quality of Health Care Was the distribution of quality health care equitable in the United States? An examination of disparities in quality of care suggests that it was not (Fiscella, Franks, Gold, & Clancy, 2000). For example, lower SES was associated with receiving fewer Pap tests, mammograms, childhood and adult influenza immunizations, and diabetic eye exams. Lower SES was also associated with late enrollment in prenatal care and lower-quality ambulatory and
Goldsteen74024_07_CH07_215-272_03-18-20.indd 246
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
247
hospital care. Racial and ethnic status was linked to quality of care received. Elderly African Americans received fewer preventive medicine procedures when compared with elderly Whites. African Americans, in general, received less intensive hospital care, and Hispanic women received fewer medical procedures and preventive measures as compared with Whites. African Americans were also found to have higher rates of end-stage diabetic conditions, such as amputations, indicating poor-quality ambulatory care. However, a study by the RAND Corp. (Asch et al., 2006) suggests that inequities in health care quality may not be as important as deficiencies in the overall level of quality in the United States. In the RAND study, health care quality differed little between people in different socioeconomic, racial, ethnic, and geographic groups. Rather, the researchers found that health care was mediocre for all groups, equally. The study suggests that disparities in quality of care may be closing but that the overall quality of health care for all Americans needs much improvement. The discrepancy between the RAND study findings and those of previous research had not been resolved at the time this book was written, but it is an important issue that should generate a great deal of research in the future.
Equity and Access to Health Care Was access to health care equitable in the United States prior to the ACA? Here, the evidence is quite clear. People without health insurance (or with poor health insurance) had much less access to health care. As we have discussed, the United States finances health care through a mixed system, based largely on employer-based health insurance and the public insurance programs for the elderly and disabled (Medicare) and the poor (Medicaid). This patchwork system left millions of people without health insurance (Kaiser Family Foundation, 2015). Millions more were underinsured, that is, they did not have comprehensive coverage. This could mean high deductibles and copays and limited coverage for a variety of health care services, including mental health services, medical equipment, and preventive care (Lee & Tollen, 2002). The health care access problems of the uninsured were well documented. The uninsured were much less likely to have a “usual place to go” for medical care. If they had a usual place for health care, they were less likely than insured persons to have a physician’s office as their site of care. Uninsured adults were more likely to use “safety net” providers, such as community health centers, EDs, and public health or free clinics as their usual place for health care. They were less likely than the insured persons to see the same health care provider each time they obtained health care. They were more likely to report not getting needed health care, and they had fewer ambulatory care visits. Research showed that uninsured persons were significantly more likely to delay seeking health care. Lack of health insurance was found to be significantly related to the failure to fill a recommended prescription, and it was found that medications, even when filled, were less likely to be taken as directed, but saved or spread out over a longer than prescribed period of time to save money (Kaiser Family Foundation, 2002). Not all Americans had the same probability of being uninsured. National surveys consistently found that age, SES, race, and ethnicity were predictors of being uninsured or underinsured. The majority of the uninsured and underinsured were employed. People who had no more than high school education were more likely to be uninsured. A higher percentage of Hispanics and African Americans were uninsured compared with non-Hispanic Whites. Foreign-born noncitizens showed the highest rate of being uninsured (Jonas & Kovner, 2005; Kaiser Family Foundation, 2006, 2015). Another factor leading to inequities in access to health care was geographic location. People who lived in rural America and those who lived in inner cities had reduced access to health care, even if they had health insurance. These areas often lacked health care resources, including physicians and other health care providers and facilities, particularly
Goldsteen74024_07_CH07_215-272_03-18-20.indd 247
3/19/20 10:54 AM
248
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
easy-to-reach, comprehensive hospitals. Rural residents generally faced a greater financial burden for obtaining care than urban and suburban residents, and mental health services were especially scarce (Reschovsky & Staiti, 2005). Rural areas tended to attract fewer doctors than urban areas. Even though 20% of Americans lived in rural areas, only 9% of U.S. physicians practiced in rural areas (AHRQ, 2005). This was the situation that prompted the passage in 2010 of the ACA, whose primary goal was to address the inequities in health care. The problem of equity, in both access to and quality of health care, was well known, and there had been efforts to remedy the problem starting early in the 20th century, when reformers began to focus on securing universal health care coverage in the United States. The history of the efforts to correct the inequities in the U.S. health care system prior to the ACA is described at length in Chapter 8, Debates That Have Structured Health Care System Change.
Equity in Health Care Quality and Access After the ACA The ACA extended and enlarged former reform efforts through policies that included the following: • •
•
Changing Medicaid eligibility criteria so that more people qualified for coverage and subsidizing state Medicaid programs to encourage states to expand Medicaid. Setting minimum standards for private health insurance policies, including coverage of preexisting conditions, so that people could not purchase “junk” insurance and find themselves without coverage when they needed it. Mandating that everyone purchase health insurance and providing subsidies for those with low incomes (“individual mandate”).
Has equity in access and quality of health care improved since the ACA? We must remember that the major provisions of the ACA were not implemented until 2014, and since 2016, the Trump administration has chipped away at essential components of the legislation, weakening its policies. The individual mandate is no longer in effect. Private insurance companies have been allowed to provide health insurance policies that do not meet the original minimum standards. Also, many states did not expand Medicaid, which played a vital role in insuring the uninsured under the ACA. Nevertheless, the ACA resulted in a great many people obtaining health insurance. By 2018, “an estimated 20 million people (had) become newly insured, and approximately 24 million people (had) gained access to subsidized or free care through marketplace tax credits and Medicaid expansion”(Eibner, 2018, para 2). Furthermore, the disparities in health insurance coverage between racial and ethnic groups narrowed after implementation of the ACA, although they did not disappear. The Kaiser Family Foundation (2019, para 5) reports that: Since implementation of the major ACA health coverage expansions in 2014, people of color have experienced large coverage gains that helped narrow the longstanding racial and ethnic disparities in coverage. These gains reflected increases in both Medicaid and private coverage. Hispanics experienced the largest coverage gain. ... Asians, American Indian/Alaska Native (AIANs) and Blacks also experienced larger coverage gains compared to Whites. These coverage gains helped to narrow racial and ethnic disparities in coverage. However, people of color remained more likely to be uninsured, with AIANs and Hispanics at the highest risk of lacking coverage. See Figure 7.1, which visualizes the decline in the uninsured by racial and ethnic groups between 2013 and 2017.Figure 7.1 Uninsured rates among nonelderly individuals by race and ethnicity, 2013 to 2017.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 248
3/19/20 10:54 AM
■
7
H e a l t h C a re S y s t e m P e r f o r m a n c e
249
100 90 80 70
22% 19%
60 50 23% 40
21%
30 20
11%
11% 7%
12% 30%
10%
8%
8%
30% 19%
10
7%
18%
16%
12%
0 AIAN
Hispanic
Black 2013
NHOPI 2015
Asian
White
2017
FIGURE 7.1 Uninsured rates among nonelderly individuals by race and ethnicity, 2013 to 2017. Source: Data from Kaiser Family Foundation. (2019). Changes in health coverage by race and ethnicity since implementation of the ACA, 2013-2017. Retrieved from https://www.kff.org/disparities-policy/issue-brief/ changes-in-health-coverage-by-race-and-ethnicity-since-implementation-of-the-aca-2013-2017/
Another study found that the ACA had a beneficial effect on health coverage among low-income households, decreasing the disparities between high- and low-income families: In its first two years of full implementation, the ACA improved health care access for Americans in low-income households, people who were not college graduates, and the unemployed. The law’s Medicaid expansion was responsible for about half of these gains. The ACA was associated with a substantial (but incomplete) narrowing of socioeconomic disparities in access, particularly in states that expanded Medicaid. (Griffith, Evans, & Bor, 2017, p. 1509) Thus, there is evidence that the ACA improved health care equity by decreasing ethnic, racial, and economic disparities in health insurance coverage. It can be assumed that health insurance coverage also increased in rural areas. Next, we turn to a brief discussion of efficiency, the third criterion for evaluating health system performance.
HEALTH CARE EFFICIENCY Efficiency is the third criterion for judging a health care system.“Efficiency requires that we produce the combination of goods and services with the highest attainable total value, given our limited resources and technology” (Aday et al., 1993, p. 73). Efficiency is either allocative
Goldsteen74024_07_CH07_215-272_03-18-20.indd 249
3/19/20 10:54 AM
250
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
or production. Allocative efficiency concerns attaining the most valued mix of health care services. Production efficiency refers to producing a given level of health care services at minimum cost. For example, an allocative efficiency issue is how much to invest in preventive versus curative medical services, whereas a production efficiency issue might concern whether and when to substitute relatively low-cost nurses for higher cost physicians in the provision of health care services.
Microlevel Health Care Efficiency At the microlevel of physician practices, hospitals, and other health care settings, efficiency is assessed using (a) production functions and (b) cost-effectiveness, cost-benefit, and related cost-utility analysis (Aday et al., 1993). These analyses are used to determine, for example, which of two equally effective treatments should be recommended to clinicians. If both are effective, the goal of efficiency suggests that the less expensive treatment is preferable. These kinds of decisions are increasingly made by health care payers. For example, the Commonwealth Fund Newsletter reports: Washington State’s Health Care Authority, which coordinates the Prescription Drug Program for the state’s Medicaid, public employee, and worker compensation programs, is using an integrated approach to value-based pharmaceutical purchasing. The evidence-based drug review process involves a thorough analysis of quality and effectiveness before applying cost considerations. The process, which includes an evidence-based preferred drug list and supplemental rebates from pharmaceutical manufacturers, is producing savings of about $20 million each year to the state—over 5 percent of its Medicaid fee-for-service drug spending—and about $40 million in combined state–federal spending. (2006, p. 1)
Macrolevel Health Care Efficiency At the macrolevel, efficiency analysis is based on comparisons between regions, states, and nations. Often, we use international comparisons of health care systems (Aday et al., 1993). The Commonwealth Fund’s Mirror, Mirror on the Wall reports (2010, 2014, 2017) contrast the United States with 10 peer nations—Australia, Canada, France, Germany, New Zealand, Norway, the Netherlands, Switzerland, Sweden, and the United Kingdom—on numerous indicators of cost and available health care resources. In 2010 and 2014, the United States ranked first in the proportion of its gross domestic product (GDP) spent on health services (17.7%) and also in per capita total expenditures on health care. At the average exchange rate in U.S. dollars, per capita expenditure in 2014 was US$8,508 in the United States, compared with US$3,405 in the United Kingdom (Davis, Schoen, & Stremikis, 2010; Davis, Stremikis, Schoen, & Squires, 2014). The United States ranked second to last in the number of physicians per 1,000 population and last in the number of physician visits per capita. The United States recorded the lowest percentage of those who believed, if they became seriously ill, they would be confident they could afford the care they needed. Overall, the United States ranked last on mortality amenable to health care, last on infant mortality, and second to last on healthy life expectancy at age 60. Primary care physician survey data also suggested the United States was lagging in the adoption of national policies that promote primary care, quality improvement, and information technology. The United States was spending more per capita on health care and providing fewer basic health care resources relative to other countries. Further, the U.S. rankings on various
Goldsteen74024_07_CH07_215-272_03-18-20.indd 250
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
251
measures of mortality discussed previously in this chapter (see “Population Health Outcomes”) suggested that the U.S. health care system was not efficient, because our rankings on life expectancy, quality-of-life adjusted life expectancy, infant mortality, and other mortality rates were consistently lower than those of peer nations spending less on health care. The Commonwealth Fund’s 2017 Mirror, Mirror on the Wall report showed no improvement over earlier reports. Among the 11 peer countries, the health system performance of the United States was rated worst in nearly every respect: overall performance; care process, including preventive care, safe care, coordinated care, and engagement and patient preferences; access, including affordability and timeliness; administrative efficiency; equity; and health care outcomes (Schneider, Sarnak, Squires, Shah, & Doty, 2017). See Table 7.6. Negative scores indicate the country is below the 11-country average. The greater the negative score, the greater the distance from the average score, and the worse the score. After the enactment of the ACA, health insurance coverage in the United States was higher than in 2014, but still lower than in the peer countries, where at least 99% of people were covered. Another Commonwealth Fund report focused on health care spending in the 11 peer nations in 2016 (Papanicolas, Woskie, & Jha, 2018). The authors found that health care spending
TABLE 7.6 Eleven-Country Summary Scores on Health System Performance, The Commonwealth Fund, 2016 AUS
CAN
FRA
GER
NETH
NZ
NOR
SWE
SWIZ
UK
US
Overall Performance Score
–0.26
–0.45
0.07
0.27
0.13
0.13
0.08
0.08
0.37
–0.75
–0.26
Care process
0.38
0.15
–0.42
–0.12
0.29
0.36
–0.60
–0.82
–0.03
0.56
0.23
Preventive care
0.57
–0.38
–0.96
0.43
0.11
–0.34
–0.20
–0.07
0.46
0.25
0.57
Self-care
0.89
0.03
–0.38
0.08
0.18
0.29
–1.08
–0.82
–0.49
1.03
0.29
–0.11
–0.23
–0.22
0.37
0.06
0.64
–0.11
–1.07
0.41
0.30
–0.04
Engagement and patient preferences
0.69
0.22
–0.71
0.04
0.49
0.40
–0.86
–1.17
0.04
0.45
0.42
Access
0.19
–0.77
–0.14
0.58
0.70
0.02
0.14
0.06
–0.11
0.39
–1.07
Affordability
0.06
–0.31
–0.59
0.67
0.28
0.15
0.46
0.69
–0.52
0.97
–1.87
Timeliness
0.32
–1.23
0.31
0.48
1.13
–0.10
–0.18
–0.56
0.31
–0.19
–0.27
Administrative efficiency
0.74
0.08
–1.41
0.08
–0.15
0.60
0.54
0.26
–0.12
0.59
–1.21
–0.14
–0.39
–0.53
0.01
0.46
–0.24
0.14
0.37
0.34
0.93
–0.94
0.62
–0.35
0.23
–0.18
0.03
–0.12
0.42
0.55
0.32
–0.63
–0.76
Coordinated care
Equity Health care outcomes
NOTE: “Performance Score” is based on the distance from the 11-country average, measured in standard deviations. SOURCE: Schneider, E. C., Sarnak, D. O., Squires, D., Shah, A., & Doty, M. M. (2017). Mirror, mirror 2017: International comparison reflects flaws and opportunities for better U.S. health care. The Commonwealth Fund. Retrieved from http://www.commonwealthfund.org/ interactives/2017/july/mirror-mirror/
Goldsteen74024_07_CH07_215-272_03-18-20.indd 251
3/19/20 10:54 AM
252
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
as a percentage of GDP remained the highest in the United States—17.8% compared with the 11.5% average for the comparable countries. In addition, they found that higher U.S. costs were driven by higher spending on pharmaceuticals, physician salaries, and administrative costs, rather than by higher utilization for treatment: •
•
Except for diagnostic tests, the U.S. uses health care services at rates similar to those of other countries. Numbers of hospital visits and surgeries performed in the U.S. are similar to those in other countries. However, the U.S. performs 118 MRI scans per 1,000 people, compared to an average of 82 MRIs per 1,000 people among all high-income countries. The U.S. also performs a higher rate of CT scans: 245 per 1,000 people, compared to 151 per 1,000 people among all high-income countries. The U.S. pays more for . . . • Doctors. The average salary for a general practitioner in the U.S. is $218,173, nearly double the average salary across all high-income countries. Specialists and nurses in the U.S. also earn significantly more than elsewhere. • Pharmaceuticals. The U.S. spends $1,443 per person on pharmaceuticals, compared to the average of $749. • Health care administration. The U.S. spends 8 percent of total national health expenditures on activities related to planning, regulating, and managing health systems and services, compared to an average 3 percent spent among all high-income countries. (Papanicolas et al., 2018, para 3)
Similarly to the case in 2014, in 2016 there was still little or no evidence that the U.S. health care system was efficient given its poor performance and high cost relative to those of its peer nations.
A NATIONAL SCORECARD The Commonwealth Fund evaluates the performance of the U.S. health care system comprehensively, rather than piece by piece, in the National Scorecard on U.S. Health System Performance. The National Scorecard is an ongoing initiative since 2006. The 2019 National Scorecard rates health system performance in each state using 47 indicators grouped into four dimensions: •
•
•
•
Access and Affordability Seven indicators, including insurance coverage for children and adults, out-ofpocket expenses for health insurance and medical care, cost-related barriers to receiving care, and receiving dental care. Prevention and Treatment Fifteen indicators, including quality of ambulatory, hospital, postacute, and longterm care settings, and receiving preventive and needed mental health care Potentially Avoidable Hospital Use and Cost Thirteen indicators, including avoidable hospital and ED use, per person spending among Medicare beneficiaries and working-age adults with employer-sponsored insurance Healthy Lives Twelve indicators, including premature death; health status; health risk behaviors, including smoking and obesity; and tooth loss (Radley, Collins, & Hayes, 2019)
Goldsteen74024_07_CH07_215-272_03-18-20.indd 252
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
253
TABLE 7.7 2019 National Scorecard on State Health System Performance: Lowest- and Highest-Performing States, Overall Highest-Ranking States
Lowest-Ranking States
Hawaii
West Virginia
Massachusetts
Arkansas
Minnesota
Nevada
Washington
Texas
Connecticut
Oklahoma
Vermont
Mississippi
SOURCE: Radley, D. C., Collins, S. R., & Hayes, S. L. (2019). 2019 scorecard on state health system performance. The Commonwealth Fund. Retrieved from https://www.commonwealthfund.org/publications/fund-reports/2019/jun/2019-scorecard-state-health-system-performance-deaths-suicide
Using publicly available data, the authors of the National Scorecard calculate scores for states on each of these indicators and then rank states relative to each other. In any one year, there is no absolute or“gold standard”benchmark for each indicator. When the data are available, states are also compared with their own prior performance to assess improvement or decline in performance. For example, in 2016, Minnesota was ranked No. 1 (or best) on the indicator “diabetic adults without an annual hemoglobin A1c test.” Only 5.6% of diabetics in Minnesota did not receive this important test in 2016. The range for all states on this indicator was 5.6% to 22.5% in that year. Minnesota was also compared with its own performance in 2015 on the hemoglobin A1c test and found to have improved; in 2015, 11% of diabetics had not received the A1c test in Minnesota. The 2019 National Scorecard reports the overall state rankings, as well as rankings on individual indicators. Overall performance is a summary of all indicators. The six highest- and lowest-ranking states, overall, are displayed in Table 7.7. The scorecard also identifies states that made the largest gains over their past performance. The 2019 National Scorecard reports that California made the largest improvement in rankings, up 12 spots. New York and Washington rose 10 spots in the rankings, and Rhode Island went up nine places. Importantly, the authors of the 2019 National Scorecard estimated the improvements that could be made if every state achieved the top performance on every indicator. These improvements include: • • • •
10 million more children would receive recommended annual medical and dental visits 296,000 fewer hospital readmissions 6.7 million fewer emergency room visits for nonemergency care or conditions treatable with primary care 90,000 fewer deaths before age 75 from treatable diseases. (Radley et al., 2019, p. 15)
DATA AND INFORMATION TECHNOLOGY Every major organization with an interest in health care performance recognizes the need for better data in order to benchmark the current situation and then determine whether improvements have occurred in quality, access and equity, and cost and efficiency. It is
Goldsteen74024_07_CH07_215-272_03-18-20.indd 253
3/19/20 10:54 AM
254
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
generally agreed, as Hanrahan and his colleagues have written, that“[p]roper functioning of health care systems requires an advanced health information network that supports clinical care, personal health management, population health, and research. But this infrastructure does not yet exist in the United States” (Hanrahan, Foldy, Barthell, & Wood, 2006, p. 16). Although advances have been made since 2006, there is still no single, national health information network. The organizations that need data include the payers of health care, such as the Medicaid and Medicare programs and private health insurance companies; providers of health care, including hospitals and ambulatory clinics; private foundations, such as the Commonwealth Fund, that focus on health policy; private organizations such as the NQF, whose goal is to improve the health care system; the accreditation organizations such as The Joint Commission; and many consumer groups. Data are used to: • • • •
Conduct clinical outcomes studies; Measure population health outcomes, such as morbidity and mortality rates for regions, states, and the nation; Design and evaluate interventions to improve clinical practice; and Increase access, equity, and efficiency of the health care system.
Health information technology (HIT) makes it possible to manipulate health data to create the information needed. HIT is defined as “the application of information processing involving both computer hardware and software that deals with the storage, retrieval, sharing, and use of health care information, data, and knowledge for communication and decision making” (HealthIT.gov, 2019a, para 8).
Where Are the Health Data? The data currently used for assessing health systems performance are scattered throughout the health care system in provider records, health insurance forms, and surveys conducted by providers, payers, and the government, particularly the CDC. They include administrative records, medical records, and surveys.
Administrative Records Billing Claim Forms The Uniform Billing Form (UB-04 or CMS 1450) is used by health care institutions, including hospitals, nursing homes, and other facilities, to submit bills to health insurance companies for payment of health care services provided. The HCFA-1500 (CMS 1500) is the claim form used by individual providers, including physicians, nurses, therapists, chiropractors, and other health care professionals. The forms are standardized by CMS and are the basis for paper forms required by most payers when needed. More generally, HIPAA required standardizing the claims format for electronic exchange among all payers as part of its administration simplification section. However, payers may have their nuances and extensions necessitating that providers adjust outgoing claims for some payers to some extent. These forms all include basic patient information, including age, sex, and insurance, as well as the diagnoses associated with treatment provided and the treatment (procedure) codes. Despite being originally developed to facilitate billing, billing (or claims) data are becoming increasingly important for quality measurement and population analytics due to its near universality and highly structured format. Additionally, CPT Category II and similar extensions enable certain quality information to be transferred over the existing, extensive infrastructure already developed to support claims transmittal and processing.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 254
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
255
Enrollment Files Enrollment files are kept by health care facilities about their patients and by health insurance companies about their beneficiaries. They exist in each facility and organization in which the individual is or has been a patient or beneficiary. They contain basic personal information, including age, sex, health insurance, residence, and contact information.
Medical Records Medical records originate and are maintained in the health provider organization in which care was received—hospital, ambulatory clinic, physician office, nursing home, or other facility. The purpose of medical records is to document past and guide future health care. Therefore, they contain detailed information about treatment and diagnosis, which billing forms do not. This includes the patient’s medical history, diagnoses, medications, treatment plans, immunization dates, allergies, radiology images, and laboratory and test results. Although some medical records are still recorded and stored on paper, they are increasingly computerized. There are two types: the Electronic Medical Record and the Electronic Health Record.
Electronic Medical Record Electronic medical records (EMRs) are a digital version of the paper charts in the clinician’s office. An EMR contains the medical and treatment history of the patients in one practice. EMRs have advantages over paper records. For example, EMRs allow clinicians to: • • • •
Track data over time Easily identify which patients are due for preventive screenings or checkups Check how their patients are doing on certain parameters—such as blood pressure readings or vaccinations Monitor and improve overall quality of care within the practice. (HealthIT.gov, 2019b)
Electronic Health Record Electronic health records (EHRs) contain everything in the EMR and more.“EHRs focus on the total health of the patient—going beyond standard clinical data collected in the provider’s office and inclusive of a broader view on a patient’s care. EHRs are designed to reach out beyond the health organization that originally collects and compiles the information. They are built to share information with other health care providers, such as laboratories and specialists, so they contain information from all the clinicians involved in the patient’s care” (HealthIT.gov, 2019b, para 4).
Health Surveys Whereas administrative and medical records contain health data on all persons who have received care, surveys are samples, not a universe. They elicit information that is not contained in administrative records or the medical record but that is valuable to assess health system performance. For example, a patient’s satisfaction, including perceptions of quality of care and respectful treatment by staff following a medical procedure, is not collected on the billing form or even the medical record. Some of the most useful surveys for evaluating health system performance have been identified in this chapter and/or are described below.
Hospital Consumer Assessment of Healthcare Providers and Systems Survey Hospital Consumer Assessment of Healthcare Providers and Systems Survey (HCAHPS) is a 27-question survey developed by CMS in partnership with AHRQ to obtain patient perceptions about their hospital experience relating to communication with doctors, communication with nurses, responsiveness of hospital staff, cleanliness of the hospital
Goldsteen74024_07_CH07_215-272_03-18-20.indd 255
3/19/20 10:54 AM
256
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
environment, quietness of the hospital environment, communication about pain, communication about medicines, discharge information, overall rating of hospital, and recommendation of hospital. The purpose of the survey is to provide a standardized instrument and method for collecting patient satisfaction information that can be used to compare hospitals locally, regionally, and nationally. Hospitals sample recently discharged patients and provide the survey results to CMS. The results of the survey, in which most hospitals participate, are available by individual hospital at CMS Hospital Compare (visit: www. medicare.gov/hospitalcompare/search.html). CMS believes that HCAHPS provides health care consumers with “objective and meaningful comparisons of hospitals,” which will incentivize hospitals to improve quality and promote accountability (CMS, 2019i, para 2).
Other Relevant Health Surveys Relevant surveys conducted by AHRQ are: • • •
Health care Cost and Utilization Project Medical Expenditure Panel Survey Home Health CAHPS (HHCAHPS)
Relevant surveys conducted by CMS are: • •
CAHPS Hospice Survey Medicare Health Outcomes Survey
Relevant surveys conducted by the CDC are: • • • • •
National Health Interview Survey (NHIS) National Ambulatory Medical Care survey (NAMCS) National Health and Nutrition Examination Survey (NHANES) National Hospital Ambulatory Medical Care Survey (NHAMCS) Behavioral Risk Factor Surveillance System (BRFSS)
Relevant Leapfrog surveys are: • •
Leapfrog Hospital Survey Leapfrog Ambulatory Surgery Center Survey
For each of these surveys, a description of the purpose, sample, questionnaire, and data collection process can be obtained electronically on the host website. Summary results are usually provided, as well. In some cases, such as the BRFSS, data may also be obtained online.
Other Relevant Administrative Data National Vital Statistics System The National Vital Statistics System (NVSS) is one of the most important sources of information for evaluating health systems performance, especially at the macrolevel. The NVSS contains the Linked Birth and Infant Death Data (NVSS-L), the Mortality Data (NVSS-M), and the Natality Data (NVSS-N). These data sources are required for indicators including life expectancy and mortality rates. The NVSS is an initiative of the NCHS (2019).
National Program of Cancer Registries The National Program of Cancer Registries collects data on all cancer occurrences and their initial treatment and outcomes of treatment. Records include type, extent, and location of
Goldsteen74024_07_CH07_215-272_03-18-20.indd 256
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
257
cancer. The cancer registries were established by Congress in 1992 and are administered by the CDC (2019i).
Health Information Exchange: The HIT Dream The dream is for patients, providers, and payers to have electronic access to a patient’s health information in all sites of care and by all providers involved in the patient’s care. The sites would include laboratories, specialists, medical imaging facilities, pharmacies, and school and workplace clinics, in addition to hospitals and primary care physician offices. The information would include the patient’s medical history, diagnoses, medications, treatment plans, immunization dates, allergies, radiology images, and laboratory and test results. Ideally, the information would be gathered from the EHR so as to contain relevant patient facts such as smoking, physical activity, and nutrition. An electronic health information network or health information exchange (HIE) would gather together and share patient information beyond the health organization that originally collected and compiled it. Essentially, the information would move with the patient: to the specialist, the hospital, the nursing home—wherever the patient sought care. It would be accessible to the patient and the patient’s providers and payers. The information exchange would occur in real time and would protect patient privacy and confidentiality. Although a nationwide HIE is desired, current activities have focused on developing regional health information organizations (RHIOs). “RHIOs are thought to have a greater likelihood of success than other strategies, given that they are locally based, and they may be linked together in the future to enable national exchange. Efforts to reap the benefits of clinical data exchange are widely embraced and remarkably nonpartisan” (Adler-Milstein, McAfee, Bates, & Jha, 2017, W60-61). Since 2004, the Office of the National Coordinator for Health Information Technology (ONC) has led the effort to develop HIE. Located in the DHHS, it is responsible for “support[ing] the adoption of health information technology and the promotion of nationwide health information exchange to improve health care. ... ONC is the principal federal entity charged with coordination of nationwide efforts to implement and use the most advanced health information technology and the electronic exchange of health information”(ONC, 2019, para 1). The ONC efforts to advance HIE include a great deal of private-sector reliance on developing communication standards, software, hardware, and training for those who will use the system. With regard to assisting health care organizations to adopt electronic records, Karen DeSalvo, the national coordinator, wrote in the Federal Health IT Strategic Plan 2015–2020: Implementation of the prior Plan created a strong foundation for achieving this Plan’s goals and objectives. Over 450,000 eligible professionals and 4,800 eligible hospitals received an incentive payment for participation in the Medicare and Medicaid Electronic Health Record (EHR) Incentive Programs. This incredible achievement was not easy. Hospitals and health care providers have invested capital, time, and hard work to convert their patient medical records from paper systems to EHRs, and to adapt workflow and culture to deliver care in this electronic environment. This has created a strong demand for the seamless sharing of information across technology systems, information platforms, location, provider, or other boundaries. (ONC, 2015, para 2) As a result of these and other efforts, there has been substantial progress since 2004, when the ONC was established in the number of health care organizations that have implemented some stage of the process. See Table 7.8. Another indicator of partnership and progress is the awarding of NCQA’s eMeasure Certification to the Nebraska Health Information Initiative (NHII), the first exchange organization to earn this certification. The NEHII submitted its electronic clinical quality measure
Goldsteen74024_07_CH07_215-272_03-18-20.indd 257
3/19/20 10:54 AM
258
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
TABLE 7.8 Status of Electronic Medical Records, 2018 Provider Group Percentage of office-based physicians and nonfederal acute care hospitals that:
Office-based physicians (2015)
Nonfederal acute care hospitals (2017)
are electronically sending or receiving (exchanging) patient health information with any health care providers outside their organization
48%
90%
can electronically find patient health information from sources outside their health system
34%
61%
can integrate (e.g., without manual entry) health information received electronically into their health IT
31%
53%
had necessary patient health information electronically available from health care providers or sources outside their systems at the point of care
36%
51%
SOURCE: Office of the National Coordinator for Health Information Technology. (2018). 2018 report to Congress: Annual update on the adoption of a nationwide system for the electronic use and exchange of health information. Washington, DC: Department of Health and Human Services. Retrieved from https://www.healthit.gov/topic/about-onc/health-it-strategic-planning
(eCQM) to NCQA, and, after testing, NCQA concluded that the software’s results were accurate and reliable. As an ONC-Authorized Testing Lab, NCQA can test QMs as part of the ONC Health IT Certification program. At this time, NCQA is the only approved alternative to ONC’s electronic quality measure testing process (NCQA, 2019c).
Barriers to Achieving the HIT Dream Information is not easily exchanged between providers and payers who may have been using different hardware, software, processes, and definitions. The ONC’s 2018 Report to Congress provides the most recent description of progress so far:
Current State of HIE The increase in adoption of health IT means most Americans receiving health care services now have their health data recorded electronically. However, this information is not always accessible across systems and by all end users—such as patients, health care providers, and payers—in the market in productive ways. For example: •
•
•
Despite the individual right to access health information about themselves established by the HIPAA Privacy Rule, patients often lack access to their own health information, which hinders their ability to manage their health and shop for medical care at lower prices; Health care providers often lack access to patient data at the point of care, particularly when multiple health care providers maintain different pieces of data, own different systems, or use health IT solutions purchased from different developers; and Payers often lack access to clinical data on groups of covered individuals to assess the value of services provided to their customers.
Lack of data standardization undermines the ability to share data easily so that longitudinal data trending can be based on all patient interactions with all their providers. While
Goldsteen74024_07_CH07_215-272_03-18-20.indd 258
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
259
privacy protections and controls are critical to widespread trust in such a system, consent rules can also be restrictive and cumbersome placing a significant burden on the patient and every treating provider to ensure that every provider that the patient wants to have access to their medical records actually has access to their records. Fully using modern computing tools is critical to advancing health care. Patients should be able to easily and securely access their medical data through their smartphones. Currently, patients electronically access their health information through patient portals that prevent them from easily pulling from multiple sources or health care providers. Patient access to their electronic health information also requires repeated use of logins and manual data updates. For health care providers and payers, interoperable access and exchange of health records is focused on accessing one record at a time. Payers cannot effectively represent their members if they lack computational visibility into which health care providers offer the highest quality care at the lowest cost. Without the capability to access multiple records across a population of patients, health care providers and payers will not benefit from the value of using modern computing solutions—such as machine learning and artificial intelligence— to inform care decisions and identify trends. In addition, payers and employer group health plans which purchase health care have little information on health outcomes. ... Outcome data will allow payers to apply machine learning and artificial intelligence to have better insight into the value of the care they purchase. (ONC, 2018, pp. 4–5)
Current HIE Barriers Over the past year, HHS heard from stakeholders that barriers to interoperable access to health information remain, including technical, financial, trust, and business practice barriers. These barriers impede the movement of health information to where it is needed across the care continuum. In addition, burden arising from quality reporting, documentation, administrative, and billing requirements that prescribe how health IT systems are designed also hamper the innovative usability of health IT. (ONC, 2018, p. 6) ONC plans to address the problems of HIE, as identified earlier, by: • • • •
Providing certified health IT to health care provider needs, including upgrades that support interoperability; Supporting development use of upgraded HIT capabilities; Encouraging data sharing including through open application programming interfaces (APIs); and Reducing the administrative burden of HIT (ONC, 2018).
The ONC is particularly focusing on open APIs.“Open APIs are technology that allow one software program to access the services provided by another software program and can improve access and exchange of health information”(ONC, 2018, p. 6). Open APIs will support patient access to information through devices such as smartphones and mobile applications. They will permit payers to view information without having to access one record at a time.
A Health Information Example: National Healthcare Safety Network The CDC developed an Internet-based data collection and information retrieval system called the National Healthcare Safety Network (NHSN) that became available in 2005. This network is an expansion and enhancement of current surveillance and monitoring capabilities,
Goldsteen74024_07_CH07_215-272_03-18-20.indd 259
3/19/20 10:54 AM
260
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
and once implemented will replace three existing CDC surveillance systems: NNIS, the National Surveillance System for Healthcare Workers, and the Dialysis Surveillance Network. The goal is to create a common interface web-based system for accumulating, exchanging, and integrating relevant information and resources among stakeholders in an effort to support local efforts to promote patient safety. The two main aspects of the network are reporting of adverse events—including nosocomial infections—and disseminating information on preventing such events. Ultimately, the CDC aims to work with other public health agencies to create a national system integrating data from a variety of surveillance systems into a national aggregate data repository through which health care providers and federal, state, and private stakeholders can exchange data and retrieve information. In the beginning, however, the system will be restricted to providers submitting data in the areas currently covered by the three systems identified earlier, with the CDC acting as the central repository (CDC, 2019f).
Participation A major benefit of the proposed system will be the collection of data that essentially have been unavailable, as CDC surveillance systems have been focused on a limited number of facilities and procedures. In the current NNIS system, membership is restricted to only approximately 315 hospitals. Participating hospitals must also meet certain thresholds of bed number and size of infection-control staff. Under the NHSN, all bona fide health care delivery entities (participants in the CMS, members of the AHA, and Veterans Administration [VA] stations) whose practice generates relevant data will be encouraged to participate. Nationwide implementation of the system will be phased in, first being available to existing CDC surveillance participants, then to their affiliates, and finally to all health care entities. Nationwide availability of the system was expected sometime in 2006.
Surveillance and Data Collection The system will be divided into various adverse event modules, including device-associated adverse events, procedure-associated adverse events, and medication-associated adverse events. The infection data collected will be similar to that collected through the NNIS, but with important differences.
Device-Associated Module Currently, in the intensive care unit and high-risk nursery (HRN) components of the NNIS system, data are collected on incidence rates and distributions for infections at all sites. In the NHSN system, infection data will initially be collected only for CLABSIs, CAUTIs, ventilator-associated pneumonia, and infections related to dialysis treatments. Although data on fewer infection sites will be collected under the new system, surveillance will not be limited to the ICU and HRN. Facilities may also choose to collect and report device-associated infection data for specialty care units, other wards, long-term care facilities, and home therapy. This will provide further flexibility in selecting the event and population under surveillance so that facilities may better tailor surveillance activities to their particular needs.
Procedure-Associated Module Data will be collected on in- and outpatients undergoing NHSN-defined operative procedures. Under the NHSN, seven more categories of procedure are covered than under the NNIS, and whereas in the NNIS system information only on SSIs is collected, under the NHSN information on other surgical complications will also be collected. Further, the data collection protocols being designed for the NHSN will allow for more robust information on infections in surgical patients, including the ability to link bloodstream infections,
Goldsteen74024_07_CH07_215-272_03-18-20.indd 260
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
261
pneumonia, and urinary tract infections occurring after an operative procedure to the procedure and the ability to monitor—by type of operation—procedure-associated pneumonia regardless of whether a ventilator is used.
Medication-Associated Module Antimicrobial resistance and antibiotic prescription monitoring will remain essentially unchanged in the transition from current surveillance activities to the NHSN.
Data Analysis and Feedback The web-based system and central data repository being designed for the NSHN will allow participants to share data in a timely manner between users and public health agencies as well as among users (e.g., a multihospital system). The system will include data analysis wizards and statistical calculators, which will allow facilities (or groups of facilities) to generate custom reports, line lists, tables, graphs, and control charts easily. The ready availability of customizable internal and comparative analysis of infection rates is designed to facilitate the ability of health care providers to engage in continuous performance improvement. The system will also include a repository of prevention tools, lessons learned, and best practices. It is also designed to provide automatic feedback, including alerts for selected adverse events or near misses, identifying sentinel events that require an immediate response and need for root cause analysis, and identifying unusual events that might signal a preventable threat to patient safety.
SUMMARY We have discussed health care system performance from the perspective of three recognized criteria: (a) quality of health care, (b) equity of health care, and (c) efficiency of health care. Of the three, we have spent the most time on the quality of health care, mainly because over the past 20 years an increasingly large effort has developed to measure and improve quality at the microlevel. Evaluations of clinical effectiveness and patient safety are based on empirical studies that provide evidence about best practices and are the foundation of clinical practice guidelines. These studies have been well funded, and the practice guidelines that have resulted are increasingly used to evaluate the performance of health care providers—individual providers and organizations. Public as well as private organizations are involved in this effort. Equity in access to and quality of health care, although not a major focus of this chapter, is a major concern to policy makers in the United States. Our history is replete with attempts to make our system equitable by extending health care coverage to all Americans. This history is detailed in the final chapter, but no attempts have been completely successful. The efficiency of the health care system is another area that, although important, has received less attention in this chapter. However, many of the QIs are driven by an equal interest: making our system more efficient. Finally, we have briefly touched on the importance of data for evaluating health system performance. In the area of HIT, there is tremendous activity, partially driven by improvements in the technological capability to computerize information. The EMR and even EHR are becoming standard for all health care providers—individual and institutional. Again, this development is having a significant impact on the way care is delivered and how easily it can be evaluated. Thus, health information systems, too, will affect the work and future of all health professionals.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 261
3/19/20 10:54 AM
262
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
DATA SOURCES Population Health Outcomes Two international organizations are especially important sources of data on population health outcomes in the United States and other countries. These are the WHO and the OECD. As previously discussed, the NCHS is also a source for population health outcomes data in the U.S. •
The World Health Organization. The WHO is one of the most authoritative source of information about world health statistics through its worldwide data collection systems in 193 member countries (WHO, 2019a), which make information available through the Global Health Observatory (WHO, 2019b). Start here to explore statistics: www.who.int/healthinfo/statistics/en
•
The Organisation for Economic Co-operation and Development. The OECD is a “forum where the governments of 35 democracies with market economies work with each other, as well as with more than 70 non-member economies to promote economic growth, prosperity, and sustainable development”(OECD, 2019a, para 1). Start here to explore: www.oecd.org/health/health-statistics.htm
Clinical (Health care-Associated) Outcomes The section “Where Are the Health Data?” in this chapter discusses the data that are available for clinical (health care-associated) outcomes studies. These health data sources are found in administrative records, medical records, and surveys conducted by government agencies such as NCHS, health care providers and payers, and nonprofit organizations such as Leapfrog. Many of these data sources are available online and can be queried for results. Some of these are:
Centers for Medicare and Medicaid Services •
Hospital Consumer Assessment of Healthcare Providers and Systems Survey. The results of this survey are available by individual hospital at CMS Hospital Compare (visit: www.medicare.gov/hospitalcompare/search.html).
Agency for Healthcare Research and Quality •
Medical Expenditure Panel Survey. Data are available in summary form and in interactive query tools. Start here: www.meps.ahrq.gov/mepsweb/data_stats/data_overview.jsp
•
Healthcare Cost and Utilization Project. HCUPnet is an online query system based on data from HCUP. It contains statistics and information for hospital inpatient, ED, and ambulatory settings as well as population-based health care data on counties. Start here: hcupnet.ahrq.gov/#setup
Centers for Disease Control and Prevention •
Web-based Injury Statistics Query and Reporting system (WISQARS). WISQARS is an interactive, online database that provides fatal and nonfatal injury, violent death, and cost of injury data from a variety of trusted sources. Start here: www.cdc.gov/ injury/wisqars/index.html
Goldsteen74024_07_CH07_215-272_03-18-20.indd 262
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
263
•
National Vital Statistics System. The NVSS can be queried online to investigate underlying and multiple causes of death, by age, sex, race and ethnicity, region, state, county and more, from 1999 to 2017. Start here for underlying cause of death: https://wonder.cdc.gov/ucd-icd10.html
•
Other CDC interactive database systems provide information on health topics including birth defects, child and adolescent health, chronic disease, diabetes, disabilities, and environmental health. Start here for a list of these databases and their links: www.cdc.gov/surveillancepractice/data.html
STUDY QUESTIONS 1. What are key population health outcomes? 2. What are some common clinical outcomes used to evaluate health care quality? 3. How are clinical effectiveness and patient safety improved? 4. What are the major organizations that influence health care quality? 5. What is the role of data and information technology in assessing health care system performance?
REFERENCES Aday, L. A., Begley, C. E., Lairson, D. R., & Balkrishnan, R. (2004). Evaluating the healthcare system: Effectiveness, efficiency, and equity. Chicago. IL: Health Administration Press. Aday, L. A., Begley, C. E., Lairson, D. R., & Slater, C. H. (1993). Evaluating the medical care system: Effectiveness, efficiency, and equity. Ann Arbor, MI: Health Administration Press. Adler-Milstein, J., McAfee, A. P., Bates, D. W., & Jha, A. K. (2017). The state of regional health information organizations: Current activities and financing. Health Affairs, 26(2), w60–w69. doi: 10.1377/hlthaff.27.1.w60 Agency for Healthcare Research and Quality. (2005). Health care disparities in rural areas: Selected findings from the 2004 national healthcare disparities report. Retrieved from http:// archive.ahrq.gov/research/ruraldisp/ruraldispar.htm Agency for Healthcare Research and Quality. (2019a). Agency for Healthcare Research and Quality: A profile. Retrieved from https://www.ahrq.gov/cpi/about/profile/index.html Agency for Healthcare Research and Quality. (2019b). Programs. Retrieved from https:// www.ahrq.gov/programs/index.html Agency for Healthcare Research and Quality. (2019c). National Healthcare Quality and Disparities reports. Retrieved from https://nhqrnet.ahrq.gov/inhqrdr/reports/qdr American Society for Healthcare Engineering of the American Hospital Association. (2019). Centers for Medicare & Medicaid Services. Retrieved from http://www.ashe.org/advocacy/ orgs/cms.shtml Asch, S. M., Kerr, E. A., Keesey, J., Adams, J. L., Setodji, C. M., Malik, S., & McGlynn, E. A. (2006). Who is at greatest risk for receiving poor-quality health care? New England Journal of Medicine, 354(11), 1147–1156. doi: 10.1056/NEJMsa044464 Baker, D. W., & Chassin, M. R. (2017). Holding providers accountable for health care outcomes. Annals of Internal Medicine, 167, 418–423. doi: 10.7326/M17-0691
Goldsteen74024_07_CH07_215-272_03-18-20.indd 263
3/19/20 10:54 AM
264
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Carson, S., McDonagh, M., & Peterson, K. (2006). A systematic review of the efficacy and safety of atypical antipsychotics in patients with psychological and behavioral symptoms of dementia. Journal of the American Geriatric Society, 54(2), 354–361. doi: 10.1111/j.1532-5415.2005.00566.x Centers for Disease Control and Prevention. (2019a). Division of Healthcare Quality Promotion (DHQP). Retrieved from https://www.cdc.gov/ncezid/dhqp/index.html Centers for Disease Control and Prevention. (2019b). About HICPAC. Retrieved from https:// www.cdc.gov/hicpac/about.html Centers for Disease Control and Prevention. (2019c). Innovative research to support safe healthcare. Retrieved from https://www.cdc.gov/hai/research/research.html Centers for Disease Control and Prevention. (2019d). HAI data. Retrieved from https://www .cdc.gov/hai/data/index.html Centers for Disease Control and Prevention. (2019e). Guidelines & guidance library. Retrieved from https://www.cdc.gov/infectioncontrol/guidelines/index.html Centers for Disease Control and Prevention. (2019f). About NHSN. Retrieved from https:// www.cdc.gov/nhsn/about-nhsn/index.html Centers for Disease Control and Prevention. (2019g). HAI data archive. Retrieved from https://www.cdc.gov/hai/data/archive/archive.html Centers for Disease Control and Prevention. (2019h). 2018 National and state healthcareassociated infections progress report. Retrieved from https://www.cdc.gov/hai/data/portal/ progress-report.html#anchor_1552573635018 Centers for Disease Control and Prevention. (2019i). National Program of Cancer Registries. Retrieved from https://www.cdc.gov/cancer/npcr/index.htm Centers for Medicare & Medicaid Services. (2007). Quality initiatives: General information. Retrieved from www.cms.hhs.gov/QualityInitiativesGenInfo Centers for Medicare & Medicaid Services. (2009). Roadmap for quality measurement in the traditional Medicare fee-for-service program. Retrieved from https://www.cms.gov/Medicare/ Quality-Initiatives-Patient-Assessment-Instruments/QualityInitiativesGenInfo/ Downloads/QualityMeasurementRoadmap_OEA1-16_508.pdf Centers for Medicare & Medicaid Services. (2012). Conditions for coverage (Cfcs) & conditions of participations (CoPs). Retrieved from www.cms.gov/Regulations-and-Guidance/ Legislation/CFCsAndCoPs/index.html Centers for Medicare & Medicaid Services. (2015). CMS physician quality reporting programs strategic vision. Retrieved from https://www.cms.gov/Medicare/Quality-Initiatives -Patient-Assessment-Instruments/PQRS/Downloads/Physician_Quality_Reporting _Programs_Strategic_Vision_Document.pdf Centers for Medicare & Medicaid Services. (2019a). CMS quality strategy. Retrieved from https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/ QualityInitiativesGenInfo/Legacy-Quality-Strategy.html Centers for Medicare & Medicaid Services. (2019b). Quality initiatives—General information. Retrieved from https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment -Instruments/QualityInitiativesGenInfo/index.html
Goldsteen74024_07_CH07_215-272_03-18-20.indd 264
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
265
Centers for Medicare & Medicaid Services. (2019c). Quality measures. Retrieved from https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/ qualitymeasures/index.html Centers for Medicare & Medicaid Services. (2019d). Quality measures inventory. Retrieved from https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instru ments/MMS/Quality-Measures-Inventory.html Centers for Medicare & Medicaid Services. (2019e). Meaningful measures hub. Retrieved from https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/ QualityInitiativesGenInfo/MMF/General-info-Sub-Page.html Centers for Medicare & Medicaid Services. (2019f). Center for Clinical Standards and Quality. Retrieved from https://www.cms.gov/About-CMS/Leadership/ocsq/index.html Centers for Medicare & Medicaid Services. (2019g). About the CMS innovation center. Retrieved from https://innovation.cms.gov/About/ Centers for Medicare & Medicaid Services. (2019h). Health outcomes survey (HOS). Retrieved from https://www.cms.gov/Research-Statistics-Data-and-Systems/Research/HOS/ Centers for Medicare & Medicaid Services. (2019i). HCAHPS: Patients’ perspectives of care survey. Retrieved from https://www.cms.gov/medicare/quality-initiatives-patient -assessment-instruments/hospitalqualityinits/hospitalhcahps.html Cochrane Collaboration. (2019a). What is a systematic review? Retrieved from https://www .cochranelibrary.com/about/about-cochrane-reviews Cochrane Collaboration. (2019b). About us. Retrieved from https://www.cochrane.org/about-us The Commonwealth Fund. (2006, March). Washington state: An integrated approach to evidence-based drug purchasing. New York, NY: Author. Retrieved from https:// www.commonwealthfund.org/publications/newsletter-article/washington-state -integrated-approach-evidence-based-drug-purchasing Davis, K., Schoen, C., & Stremikis, K. (2010). Mirror, mirror on the wall: How the performance of the U.S. health care system compares internationally. The Commonwealth Fund. Retrieved from https://www.commonwealthfund.org/publications/fund-reports/2010/ jun/mirror-mirror-wall-how-performance-us-health-care-system Davis, K., Schoen, C., Stremikis, K., & Squires, D. (2014). Mirror, mirror on the wall: How the U.S. health care system compares internationally. The Commonwealth Fund. Retrieved from https://www.commonwealthfund.org/publications/fund-reports/2014/jun/mirrormirror-wall-2014-update-how-us-health-care-system Division of Preparedness and Emerging Infections, Centers for Disease Control and Prevention. (2019). About EIP. Retrieved from https://www.cdc.gov/ncezid/dpei/eip/eip-about.html Dixon, R. E. (2011). Control of health-care—Associated infections, 1961–2011. Morbidity and Mortality Weekly Report Supplements, 60(4), 58–63. Retrieved from https://www.cdc.gov/ mmwr/preview/mmwrhtml/su6004a10.htm?s_cid=su6004a10_w DNV GL Healthcare. (2019). Healthcare accreditation and certification. Retrieved from https:// www.dnvgl.us/assurance/healthcare/index.html Donabedian, A. (1980–1985). Explorations in quality assessment and monitoring. Vol. I: The definition of quality and approaches to its measurement; Vol. II: The criteria and standards of
Goldsteen74024_07_CH07_215-272_03-18-20.indd 265
3/19/20 10:54 AM
266
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
quality; Vol. III: The methods and findings of quality assessment and monitoring—An illustrated analysis. Ann Arbor, MI: Health Administration Press. Donabedian, A. (2003). An introduction to quality assurance in health care. Oxford, UK: Oxford University Press. Duffy, T. P. (2011). The Flexner report—100 years later. Yale Journal of Biology and Medicine, 84(3), 269–276. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC3178858/ Eibner, C. (2018). The future of U.S. health care: Replace or revise the affordable care act? Rand Health Care. Retrieved from https://www.rand.org/health-care/key-topics/ health-policy/in-depth.html Fiscella, K., Franks, P., Gold, M. R., & Clancy, C. M. (2000). Inequality in quality: Addressing socioeconomic, racial, and ethnic disparities in health care. Journal of the American Medical Association, 283(19), 2579–2584. doi: 10.1001/jama.283.19.2579 Geiger, J. (1996). Race and health care—An American dilemma? New England Journal of Medicine, 335(11), 815–816. doi: 10.1056/NEJM199609123351110 Goldsteen, K., Goldsteen, R. L., Gladwin, C. J., & Jefferson, J. A. (2004). Saving lives by eliminating hospital-acquired infections. Jericho, NY: Long Island Community Foundation. Griffith, K., Evans, L., & Bor, J. (2017). The affordable care act reduced socioeconomic disparities in health care access. Health Affairs, 36(8), 1503–1510. doi: 10.1377/hlthaff.2017.0083 Haley, R. W., Culver, D. H., White, J. W., Morgan, W. M., Emori, T. G., Munn, V. P., & Hooton, T. M. (1985). The efficacy of infection surveillance and control programs in preventing nosocomial infections in U.S. hospitals. American Journal of Epidemiology, 121(2), 182–205. doi: 10.1093/oxfordjournals.aje.a113990 Hanrahan, L. P., Foldy, S., Barthell, E. N., & Wood, S. (2006). Medical informatics in population health: Building Wisconsin’s strategic framework for health information technology. Wisconsin Medical Journal, 105(1), 16–20. Retrieved from http://www.wisconsinmedical society.org HealthIT.gov. (2019a). Glossary: Health IT terms. Retrieved from https://www.healthit.gov/ topic/health-it-basics/glossary HealthIT.gov. (2019b). What is an electronic health record (EHR)? Retrieved from https://www .healthit.gov/faq/what-electronic-health-record-ehr Hospital Compare. (n.d.). Retrieved from https://www.medicare.gov/hospitalcompare Hospital Infections Program, National Center for Infectious Diseases, CDC. (1992). Public health focus: Surveillance, prevention, and control of nosocomial infections. Morbidity and Mortality Weekly Review, 41(42), 783–787. Retrieved from https://www.cdc.gov/ mmwr/preview/mmwrhtml/00017800.htm Institute for Healthcare Improvement. (2019a). About us. Retrieved from http://www.ihi.org/ about/Pages/default.aspx Institute for Healthcare Improvement. (2019b). Science of improvement. Retrieved from http:// www.ihi.org/about/Pages/ScienceofImprovement.aspx Institute for Healthcare Improvement. (2019c). Innovations. Retrieved from http://www.ihi .org/about/Pages/innovationscontributions.aspx Institute of Medicine. (2000). To err is human: Building a safer health system. Washington, DC: National Academies Press.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 266
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
267
Institute of Medicine. (2003). Unequal treatment: Confronting racial and ethnic disparities in health care. Washington, DC: National Academies Press. Institute of Medicine. (2011). Clinical practice guidelines we can trust. Washington, DC: The National Academies Press. The Joint Commission. (2019a). Facts about the Joint Commission. Retrieved from https:// www.jointcommission.org/facts_about_the_joint_commission/ The Joint Commission. (2019b). Facts about ORYX for Hospitals. Retrieved from https://www. jointcommission.org/measurement/reporting/accreditation-oryx/ The Joint Commission. (2019c). Specifications manual for national hospital inpatient quality measures. Retrieved from https://www.jointcommission.org/specifications_manual_for _national_hospital_inpatient_quality_measures.aspx Jonas, S., & Kovner, A. R. (2005). Health care delivery in the United States (8th ed.). New York, NY: Springer Publishing Company. Kaiser Family Foundation. (2002, May). Sicker and poorer: The consequences of being uninsured. Retrieved from https://www.kff.org/uninsured/report/sicker-and-poorer -the-consequences-of-being/ Kaiser Family Foundation. (2006, August). Medicaid and the uninsured: Who are the uninsured? A consistent profile among national surveys. Retrieved from www.kff.org/uninsured/ upload/7553.pdf Kaiser Family Foundation. (2015). Key facts about the uninsured population. Retrieved from http://kff.org/uninsured/fact-sheet/key-facts-about-the-uninsured-population/ Kaiser Family Foundation. (2019). Changes in health coverage by race and ethnicity since implementation of the ACA, 2013-2017. Retrieved from https://www.kff.org/disparities-policy/issue-brief/changes-in-health-coverage-by-race-and-ethnicity-since-implementation-of-the-aca-2013-2017/ Kindig, D. A. (1997). Purchasing population health: Paying for results. Ann Arbor: University of Michigan Press. Leape, L. L., Berwick, D. M., & Bates, D. W. (2002). What practices will most improve safety? Journal of the American Medical Association, 288(4), 501–507. doi: 10.1001/jama.288.4.501 Leapfrog Group. (2019a). About us. Retrieved from https://www.leapfroggroup.org/about Leapfrog Group. (2019b). Mission and vision. Retrieved from https://www.leapfroggroup .org/about/mission-and-vision Leapfrog Hospital Safety Grade. (2019). What is patient safety? Retrieved from https://www .hospitalsafetygrade.org/what-is-patient-safety_m#errors Lee, J. S., & Tollen, L. (2002). How low can you go? The impact of reduced benefits and increased cost sharing. Health Affairs, 21(1), w229–w241. doi: 10.1377/hlthaff.w2.229 Levitt, L., Claxton, G., Cox, C., Gonzales, S., & Kamal, R. (2014). Assessing the performance of the U.S. health system. Kaiser Family Foundation Health System Tracker. Retrieved from https://www.healthsystemtracker.org/brief/assessing-the-cost-and -performance-of-the-u-s-health-system/#item-start Masso Guijarro, P., Aranaz, J. M., Mira, J. J., Perdiguero, E., & Aibar, C. (2010). Adverse events in hospitals: The patient’s point of view. Quality & Safety in Health Care, 19(2), 144–147. doi: 10.1136/qshc.2007.025585
Goldsteen74024_07_CH07_215-272_03-18-20.indd 267
3/19/20 10:54 AM
268
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Medicare.gov. (2019). Hospital compare complications & death: Infections. Retrieved from https://www.medicare.gov/hospitalcompare/search.html Mirzaei, S., Hershberger, P. E., & DeVon, H. A. (2019). Association between adverse clinical outcomes after coronary artery bypass grafting and perioperative blood transfusions. Critical Care Nurse, 39(1), 26–35. doi: 10.4037/ccn2019589 Muto, C. A., Jernigan, J. A., Ostrowsky, B. E., Richet, H. M., Jarvis, W. R., Boyce, J. M., & Farr, B. M. (2003). SHEA guideline for preventing nosocomial transmission of multidrugresistant strains of Staphylococcus aureus and Enterococcus. Infection Control and Hospital Epidemiology, 24(5), 362–386. doi: 10.1086/502213 National Center for Health Statistics. (2019). National Vital Statistics System. Retrieved from: https://www.cdc.gov/nchs/nvss/index.htm National Committee for Quality Assurance. (2019a). About NCQA. Retrieved from https:// www.ncqa.org/about-ncqa/ National Committee for Quality Assurance. (2019b). HEDIS and performance measurement. Retrieved from https://www.ncqa.org/hedis/ National Committee on Quality Assurance. (2019c). Health information exchange earns emeasures certification. Retrieved from https://www.ncqa.org/news/health-information -exchange-earns-emeasures-certification/ National Institutes of Health. (2019). What we do. Retrieved from https://www.nih.gov/ about-nih/what-we-do National Quality Forum. (2012). About NQF. Retrieved from www.qualityforum.org/About _NQF/About_NQF.aspx National Quality Forum. (2019a). NQF frequently asked questions. Retrieved from https:// www.qualityforum.org/Field_Guide/NQF_FAQs.aspx National Quality Forum. (2019b). NQF members: Leading the quality community. Retrieved from https://www.qualityforum.org/membership/ Office of the National Coordinator for Health Information Technology. (2015). Federal IT strategic plan. Retrieved from https://www.healthit.gov/sites/default/files/9-5-federal healthitstratplanfinal_0.pdf Office of the National Coordinator for Health Information Technology. (2018). 2018 report to Congress: Annual update on the adoption of a nationwide system for the electronic use and exchange of health information. Retrieved from https://www.healthit.gov/sites/default/files/ page/2018-12/2018-HITECH-report-to-congress.pdf Office of the National Coordinator for Health Information Technology. (2019). About ONC. Retrieved from https://www.healthit.gov/topic/about-onc Organization for Economic Cooperation and Development. (2019a). What is the OECD? Retrieved from https://usoecd.usmission.gov/our-relationship/about-the-oecd/what -is-the-oecd/ Organization for Economic Cooperation and Development. (2019b). OECD health statistics 2018—Frequently requested data. Retrieved from http://www.oecd.org/health/health -statistics.htm Papanicolas, I., Woskie, L. R., & Jha, A. (2018). Health care spending in the United States and other high-income countries. The Commonwealth Fund. Retrieved from https://www.commonwealthfund.org/publications/journal-article/2018/mar/ health-care-spending-united-states-and-other-high-income
Goldsteen74024_07_CH07_215-272_03-18-20.indd 268
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
269
Patient-Centered Outcomes Research Center. (2019). About us. Retrieved from https://www .pcori.org/about-us Perrow, C. (1984). Normal accidents. New York, NY: Basic Books. Radley, D. C., Collins, S. R., & Hayes, S. L. (2019). 2019 Scorecard on state health system performance. The Commonwealth Fund. Retrieved from https://www.commonwealthfund .org/publications/fund-reports/2019/jun/2019-scorecard-state-health-system-perfor mance-deaths-suicide Reschovsky, J. D., & Staiti, A. B. (2005). Access and quality: Does rural America lag behind? Health Affairs, 24(4), 1128–1139. doi: 10.1377/hlthaff.24.4.1128 Sackett, D. L., Rosenberg, W. M. C., Gray, J. A. M., Haynes, R. B., & Richardson, W. S. (1996). Evidence-based medicine: What it is and what it isn’t. British Medical Journal, 312(7023), 71–72. doi: 10.1136/bmj.312.7023.71 Schneider, E. C., Sarnak, D. O., Squires, D., Shah, A., & Doty, M. M. (2017). Mirror, mirror 2017: International comparison reflects flaws and opportunities for better U.S. health care. The Commonwealth Fund. Retrieved from http://www.commonwealthfund.org/ interactives/2017/july/mirror-mirror/ Schwartz, E., Kofie, V. Y., Rivo, M., & Tuckson, R. V. (1990). Black/White comparisons of deaths preventable by medical interventions. International Journal of Epidemiology, 19(3), 591–598. doi: 10.1093/ije/19.3.591 Shekelle, P. G., Woolf, S. H., Eccles, M., & Grimshaw, J. (1999). Developing guidelines. British Medical Journal, 318(7183), 593–596. doi: 10.1136/bmj.318.7183.593 Umscheid, C. A., Mitchell, M. D., Doshi, J. A., Agarwal, R., Williams, K., & Brennan, P. J. (2011). Estimating the proportion of healthcare-associated infections that are reasonably preventable and the related mortality and costs. Infection Control & Hospital Epidemiology, 32(2), 101–114. doi: 10.1086/657912 U.S. Congress, Office of Technology Assessment. (1995). Impacts of antibiotic-resistant bacteria (OTA-H-269). Washington, DC: U.S. Government Printing Office. U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. (2019). Overview: Health care-associated infections. Retrieved from https:// health.gov/hcq/prevent-hai.asp World Health Organization. (2012). Health status statistics: Mortality. Retrieved from http:// www.who.int/healthinfo/statistics/indhale/en/ World Health Organization. (2015). Global health observatory (GHO) data. Mortality and Global Health Estimates. Retrieved from http://who.int/gho/mortality_burden_disease/ en/ World Health Organization. (2019a). Health statistics and information systems. Retrieved from https://www.who.int/healthinfo/statistics/en/ World Health Organization. (2019b). Global health observatory (GHO). Retrieved from https:// www.who.int/gho/en/
FURTHER READING Adler, N. E., Boyce, T., Chesney, M. A., Folkman, S., & Syme, S. L. (1993). Socioeconomic inequalities in health: No easy solution. Journal of the American Medical Association, 269(24), 3140–3145. doi: 10.1001/jama.1993.03500240084031
Goldsteen74024_07_CH07_215-272_03-18-20.indd 269
3/19/20 10:54 AM
270
I
■
U. S. H e a l t h C a re S y s t e m : P re s e n t S t a t e
Adler, N. E., & Rehkopf, D. H. (2008). U.S. disparities in health: Descriptions, causes, and mechanisms. Annual Review of Public Health, 29, 235–252. doi: 10.1146/annurev. publhealth.29.020907.090852 Berwick, D. M., Gladfrey, A. B., & Roessner, J. (1990). Curing health care: New strategies for quality improvement. San Francisco, CA: Jossey-Bass. Braithwaite, J., Hibbert, P., Blakely, B., Plumb, J., Hannaford, N., Long, J. C., & Marks, D. (2017). Health system frameworks and performance indicators in eight countries: A comparative international analysis. SAGE Open Medicine, 5, 1–10. doi: 10.1177/2050312116686516 The Commonwealth Fund. (2011, October). Why not the best? The national scorecard on U.S. health system performance, 2011. Retrieved from https://www.commonwealthfund .org/sites/default/files/documents/___media_files_publications_fund_report_2011 _oct_1500_wntb_natl_scorecard_2011_web_v2.pdf Dlugacz, Y. D., Restifo, A., & Greenwood, A. (2004). The quality handbook for health care organizations. San Francisco, CA: Jossey-Bass. Field, M. J., & Lohr, K. N. (Eds.). (1992). Guidelines for clinical practice: From development to use. Washington, DC: National Academies Press. Garner, J. S. (1996). Guideline for isolation precautions in hospitals. American Journal of Infection Control, 24(1), 24–52. doi: 10.1016/S0196-6553(96)90050-4 Grove, R. D., & Hetzel, A. M. (1968). Vital statistics rates in the United States: 1940–1960. Washington, DC: National Center for Health Statistics. Healthcare Quality Improvement Partnership. (2015). A guide to quality improvement methods. Moorfields, UK: Author. Institute for Healthcare Improvement. (2012). About us. Retrieved from www.ihi.org/ihi/about The Joint Commission. (2012). Facts about the Joint Commission. Retrieved from www.jointcommission.org/facts_about_the_joint_commission National Center for Health Statistics. (2018). Health, United States, 2017: With special feature on mortality. Hyattsville, MD: U.S. Department of Health and Human Services. Retrieved from http://www.cdc.gov/nchs/data/hus/hus17.pdf National Center for Health Statistics. (2019). About the National Center for Health Statistics. Retrieved from https://www.cdc.gov/nchs/about/index.htm Pappas, G., Queen, S., Hadden, W., & Fisher, G. (1993). The increasing disparity in mortality between socioeconomic groups in the United States, 1960 and 1986. New England Journal of Medicine, 329(15), 1139. doi: 10.1056/NEJM199310073291524 Ransom, E. R., Joshi, M. S., Nash, D. B., Ransom, S. B. (2008). The healthcare quality book: Vision, strategy, and tools (2nd ed.). Chicago: Health Administration Press. United Nations International Children’s Emergency Fund. (2006). Definitions: Basic indicators. Retrieved from www.unicef.org/infobycountry/stats_popup1.html U.S. Department of Health and Human Services. (2019). HHS action plan to prevent healthcare-associated infections. Retrieved from https://www.cdc.gov/hai/prevent/prevention .html U.S. Department of Health and Human Services, Office of the National Coordinator for Health Information Technology. (2006). Goals of strategic framework.
Goldsteen74024_07_CH07_215-272_03-18-20.indd 270
3/19/20 10:54 AM
7
■
H e a l t h C a re S y s t e m P e r f o r m a n c e
271
Van Den Heuvel, J., Bogers, A. J. J., Does, R. J. M. M., van Dijk, S. F., & Berg, M. (2006). Quality management: Does it pay off? Quality Management in Health Care, 15(3), 137–149. doi: 10.1097/00019514-200607000-00003 World Health Organization, Regional Office for Europe. (2012). Health systems performance assessment: A tool for health governance in the 21st century. Retrieved from http://www .euro.who.int/__data/assets/pdf_file/0019/160813/HSPA_A-tool-for-health-gover nance-in-the-21st-century.pdf
Goldsteen74024_07_CH07_215-272_03-18-20.indd 271
3/19/20 10:54 AM
Goldsteen74024_07_CH07_215-272_03-18-20.indd 272
3/19/20 10:54 AM
II U.S. Health Care System in Transition: How We Got Here and Where We Are Going
Goldsteen74024_08_CH08_273-296_03-18-20.indd 273
3/20/20 1:02 PM
Goldsteen74024_08_CH08_273-296_03-18-20.indd 274
3/20/20 1:02 PM
8 Debates That Have Structured Health Care System Change
© Cagel Cartoons, Inc. By R.J. Matson.
LEARNING OBJECTIVES After completing this chapter, students will be able to: • Identify the major reports that have been issued since 1900 outlining problems with the U.S. health care system, as well as their eras and authors. • Describe the problems identified in each report and the continuities across reports. • Discuss health care as a public good and a private good and the implications of each perspective for the health care system. • Describe the mixed public/private U.S. health care system. • Discuss the role of ideology in producing the mixed public/private U.S. health care system. • Acquire the ability to identify and understand the underlying orientation of the proponents and opponents of a specific health policy.
Goldsteen74024_08_CH08_273-296_03-18-20.indd 275
3/20/20 1:02 PM
276
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
INTRODUCTION Problems with the performance of the U.S. health care system—quality, equity, and efficiency—are not new and have not gone unnoticed. Throughout the 20th century and into our own, they have been recognized. As far back as 1932, the findings of the first comprehensive study of health care in the United States were summarized in these terms: The problem of providing satisfactory medical service to all the people of the United States at costs which they can meet is a pressing one. At the present time, many persons do not receive service which is adequate either in quantity or quality, and the costs of service are inequably distributed. The result is a tremendous amount of preventable physical pain and mental anguish, needless deaths, economic inefficiency, and social waste. Furthermore, these conditions are … largely unnecessary. The United States has the economic resources, the organizing ability, and the technical experience to solve this problem. (Committee on the Costs of Medical Care [CCMC], 1932/1970, p. 2) The committee, chaired by Ray Lyman Wilbur, a past president of the American Medical Association, had been created in 1927 to look into the problems of the health care system. Strikingly, some would say tragically, the foregoing statement is entirely applicable today. In the 1960s and 1970s, observers of the U.S. health care system, of different political persuasions, often spoke of the“crisis”in health care. Indeed, there have been numerous critical reports and studies going back many years. For a bibliography of such reports, see “Data Sources” at the end of this chapter. For a timeline of U.S. health care events, see “Appendix” also at the end of this chapter. In 1970, the editors of Fortune magazine, echoing the CCMC’s 1932 report, wrote: American medicine, the pride of the nation for many years, stands now on the brink of chaos. To be sure, our medical practitioners have their great moments of drama and triumph. But much of the U.S. medical care, particularly the everyday business of preventing and treating routine illnesses, is inferior in quality, wastefully dispensed, and inequitably financed. Medical manpower and facilities are so maldistributed that large segments of the population, especially the urban poor and those in rural areas, get virtually no care at all even though their illnesses are most numerous and, in a medical sense, often easy to cure. (Editors of Fortune magazine, 1970, p. 9) Also echoing the CCMC’s final report, and eerily presaging the problems of our own time, none other than President Richard M. Nixon (1994) in 1971 said: For a growing number of Americans, the cost of care is becoming prohibitive. Even those who can afford most care may find themselves impoverished by a catastrophic medical expenditure. The quality of medicine varies widely with geography and income. Because we pay so little attention to preventing disease and treating it early, too many people get sick and need intensive treatment. Costs have skyrocketed but values have not kept pace. We are investing more of our nation’s resources in the health of our people, but we are not getting a full return on our investment. (p. 11) In 1973, the Committee for Economic Development, with a board composed of representatives of many of the leading American corporations and banks, came to the following conclusions concerning the health care system:
Goldsteen74024_08_CH08_273-296_03-18-20.indd 276
3/20/20 1:02 PM
8
■
D e b a t e s Th a t H a v e S t r u c t u re d H e a l t h C a re S y s t e m C h a n g e
277
First, faulty allocation of resources is a major cause of inadequacies and inequalities in U.S. health services that result today in poor or substandard care for large segments of the population. Second, the task of assuring all people the ability to cope financially with the costs of health care has been made realizable by the substantial base of coverage now provided by both private and public insurance plans. Third, unless step-by-step alterations are made in the means of delivering services and paying providers, closing the gaps in financing would overburden an inadequate system and offer little prospect of materially improving the quality and quantity of medical services of the health of the American people. (Committee for Economic Development, 1973, p. 17) In 1990, perhaps the most prominent of a spate of reports and program proposals for health care reform issued that year had this to say (U.S. Bipartisan Commission on Comprehensive Health Care, 1990): The American health care system is approaching a breaking point. Rapidly rising medical costs are increasing the numbers of people without health coverage and straining the system’s capacity to provide care for those who cannot pay. The gap is widening between the majority of Americans, who can take advantage of the best medical services in the world, and the rest, who find it hard to get even basic needed care. As the gap increases, the weight of financing care for those without adequate coverage is undermining the stability of our health care facilities. Even for the majority, the explosive growth in health care costs is steadily eroding the private insurance system—the bulwark they count on as their defense against financial risk in case of illness. (p. 2) Marking the advent of the 21st century, with many old themes still resonating, the Committee on Quality of Health Care in America of the National Academy of Sciences’ prestigious Institute of Medicine (IOM, 2001) came to the following conclusions: The American health care delivery system is in need of fundamental change. Many patients, doctors, nurses, and health care leaders are concerned that the care delivered is not, essentially, the care we should receive. The frustration levels of both patients and clinicians have never been higher …. Health care today harms too frequently and routinely fails to deliver its potential benefits. Americans should be able to count on receiving care that meets their needs and is based on the best scientific knowledge. Yet there is strong evidence that this is frequently not the case …. Between the health care we have and the health care we could have lies a chasm …. At no time in the history of medicine has the growth in knowledge and technologies been so profound …. As medical science and technology have advanced at a rapid pace, however, the health care delivery system has floundered in its ability to provide consistently high-quality care to all Americans …. The health care system as currently structured does not, as a whole, make the best use of its resources …. What is perhaps most disturbing is the absence of real progress toward restructuring health care systems to address both quality and cost concerns, or toward applying advances in information technology to improve administrative and clinical processes …. It is not surprising, then, that studies of patient experience document that the health system for some is a “nightmare” to navigate. (pp. 1–4)
Goldsteen74024_08_CH08_273-296_03-18-20.indd 277
3/20/20 1:02 PM
278
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
The remainder of this book deals with the history of change in the U.S. health care system. Throughout the 20th and 21st centuries, we have responded to the identified problems of the health care system, but within the American context. In this chapter, we discuss the values and beliefs that structure change in the United States. In Chapter 9, History of Change From 1900 to 2010: Incrementalism, we describe the specific incremental changes that have been made in order to address issues of performance—quality, efficiency, and equity—within the American value system. In Chapter 10, History of Change From 1900 to 2010: Comprehensive Reform, we describe the various attempts to achieve comprehensive change since 1900, all of which failed until the passage of the Obama administration’s Patient Protection and Affordable Care Act (ACA) in 2010. Finally, in Chapter 11, The Affordable Care Act: Achievements, Limitations, and Opposition, we discuss trends in health care today and what may be expected over the next several years.
IDEOLOGY AND THE HEALTH CARE SYSTEM The U.S. health care system exists within a framework bounded by two ideological opposites: health care is a public good and health care is a private good. These two concepts— private good and public good—are defined as follows. The key term relevant to health care is excludability. Public good, in economics, (is) a product or service that is non-excludable and nondepletable (or“non-rivalrous”). A good is non-excludable if one cannot exclude individuals from enjoying its benefits when the good is provided. A good is nondepletable if one individual’s enjoyment of the good does not diminish the amount of the good available to others. For example, clean air is (for all practical purposes) a public good, because its use by one individual does not (for all practical purposes) deplete the stock available to other individuals, and there is no way to exclude an individual from consuming it, if it exists. (Ingham, 2019, para 1) Private good (is) a product or service produced by a privately owned business and purchased to increase the utility, or satisfaction, of the buyer. The majority of the goods and services consumed in a market economy are private goods, and their prices are determined to some degree by the market forces of supply and demand. Pure private goods are both excludable and rivalrous, where excludability means that producers can prevent some people from consuming the good or service based on their ability or willingness to pay and rivalrous indicates that one person’s consumption of a product reduces the amount available for consumption by another. In practice, private goods exist along a continuum of excludability and rivalry and can even exhibit only one of these characteristics. (Summary & Henry, 2019, para 1)
Health Care as a Public Good The position of those on one side of the ideological spectrum is that health, and therefore, health care, are human rights. One expression of this belief, but certainly not the only, is the 1948 United Nations Declaration of Human Rights, Article 25, which states: Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services …. The Universal Declaration makes additional accommodations for security in case of physical debilitation or disability, and makes special
Goldsteen74024_08_CH08_273-296_03-18-20.indd 278
3/20/20 1:02 PM
8
■
D e b a t e s Th a t H a v e S t r u c t u re d H e a l t h C a re S y s t e m C h a n g e
279
mention of care given to those in motherhood or childhood fundamental human rights to be universally protected. (U.N., 1948, Article 25) Acceptance of this view identifies health care as a public good—a product or service that is nonexcludable. When the good or service is provided, individuals cannot be excluded from enjoying or using it. It is a right, not a commodity that only some can have. Karsten (1995) advances this view in a review of the writings of philosophers including Rawls, Donaldson, and Adam Smith. Pellegrino (1999) provides a representative discussion of health care as a human right and not a commodity. He argues that health care is fundamentally about healing, and is necessarily a public good, not a commodity: Treating health care as a commodity is injurious to the ethics of patient care and a society has an obligation to protect health care from the “market ethos.” Understanding health care to be a commodity takes one down one arm of a bifurcating pathway to the ethic of the marketplace and instrumental resolution of injustices. Taking health care as a human good takes us down a divergent pathway to the resolution of injustice through a moral ordering of societal and individual priorities …. If health care is a commodity, it is for sale, and the physician is, indeed, a money -maker; if it is a human good, it cannot be for sale and the physician is a healer. [There is] only one ethically defensible answer. (p. 262)
Health Care as a Private Good On the other side of the ideological spectrum is the view that health care is not a public good. Rather, it is a private good, from which individuals can be excluded. It is a commodity, not a right. One expression of this belief is provided by Michael Tanner, a senior fellow at the Cato Institute, a conservative think tank. He provides a representative discussion of health care as a private good—a commodity—in a plea to Republicans to replace the ACA with a market-based health care system after Donald Trump took office in 2016. First, Tanner asserts that health care is not a right, but a business: But whoever eventually comes up with a replacement for the ACA should keep a few hard truths in mind. •
Health care is neither a right nor a privilege; it’s a commodity. Worse, it’s a finite commodity. There are only so many doctors, so many hospitals, and so much money, and there are limits to how much these things can be expanded. That’s why no health-care system, outside Bernie Sanders’s fantasies, provides unlimited care to everyone.
Every health-care system in the world rations care in some way, either through bureaucratic fiat (Scandinavia, the U.K.), waiting lists (Canada), or price (that’s us). One can argue about which of these rationing mechanisms is fairest or most efficient, but let’s not pretend that it won’t occur. Republicans would be well advised to stop trying to win a popularity contest and simply do what’s right. •
The uninsurable are uninsurable. Let us remember that the definition of “pre-existing condition” is: someone who is already sick. It’s a little like driving your car into a tree and then trying to retroactively buy auto insurance. It won’t work. Insurance is the business of spreading risk. But for someone who, say, has cancer, there’s no risk to spread, just cost. That’s not insurance, it’s paying for health care. (Tanner, 2017, paras 2, 3, 7)
Goldsteen74024_08_CH08_273-296_03-18-20.indd 279
3/20/20 1:02 PM
280
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Second, Tanner argues that health care before and after passage of the ACA has not been a free-market system, but that the free-market ideology should guide the health care system: •
No, we didn’t have a “free market” health-care system before Obamacare. Suggest free-market reforms to our health-care system and critics will inevitably suggest that you want to go back to the flawed system we had before Obamacare. But that system had little to do with a free market. Nearly all health care was subsidized in some way, either directly or indirectly. … This thirdparty and even fourth-party payment mechanism insulated consumers from the cost of their health-care choices and drove up both spending and prices.
At the same time, provider cartels, both insurers and medical professionals, used regulatory and licensing barriers to protect themselves from competition and inflate prices. Other markets in goods and services routinely produce lower prices and better quality. Health care has always been different precisely because free-market competition and consumer choice have been missing. •
Americans want widely contradictory things from health-care reform. They want the highest-quality care for everyone, with no wait, from the doctor of their choice. And they want it as cheap as possible, preferably for free. At the same time doctors, trial lawyers, hospitals, insurers, pharmaceutical companies, and government bureaucrats are all trying to protect their fiefdoms, hold onto their gains, and shift costs to others. There is simply no way to satisfy all these special interests and produce a health-care plan that will be hugely popular.
Given this reality, Republicans would be well advised to stop trying to win a popularity contest and simply do what’s right. They need to repeal Obamacare down to the last comma and semicolon, then replace it with true market-based reforms. (Tanner, 2017, paras 13, 14, 16, 17)
Health Care: Public or Private Enterprise? Should health care be a public or private enterprise? There is a tendency for those who believe that health care is a public good to believe that it should also be a public enterprise. If health care is a right and cannot be reduced to a commodity, then a public sector system seems the natural choice to provide it. As a right, health care must be provided to all, even those who cannot afford it, and government has an obligation to provide for and protect people’s rights, which the private sector does not. Those who view health care as a private good tend to favor a private health care system. The United States was founded on the principle of a constitutionally limited government, and this remains a strong value in the United States today. America’s founders believed that governmental power should be limited and constrained by our Constitution. For those on this side of the spectrum, health care delivery belongs to the free-market economy, which made America an economic superpower and provided generations of Americans with opportunities and higher standards of living. The markets and private enterprise are best suited to deliver the health care that people want. Indeed, among those who believe that health care is a private good, some have argued that having government provide social services such as health care is actually unjust. MacLean (2017) describes how James Buchanan, an influential conservative thinker, approached this issue. She wrote that Buchanan was deeply opposed to:
Goldsteen74024_08_CH08_273-296_03-18-20.indd 280
3/20/20 1:02 PM
8
■
D e b a t e s Th a t H a v e S t r u c t u re d H e a l t h C a re S y s t e m C h a n g e
281
the seemingly unfettered ability of an increasingly more powerful federal government to force individuals with wealth to pay for a growing number of public goods and social programs they had had no personal say in approving. Better schools, newer textbooks, and more courses for Black students might help the children, for example, but whose responsibility was it to pay for these improvements? The parents of these students? Others who wished voluntarily to help out? Or people like himself, compelled through increasing taxation to contribute to projects they did not wish to support? To Buchanan, what others described as taxation to advance social justice or the common good was nothing more than a modern version of mob attempts to take by force what the takers had no moral right to: the fruits of another person’s efforts. In his mind, to protect wealth was to protect the individual against a form of legally sanctioned gangsterism. (p. xxiv) The view that taxation to pay for social welfare needs such as health care is unjust stands in sharp contrast to the perspective of those who believe health care is a public good. For them, providing health care for all is also a matter of justice—often expressed as social justice. As stated by the American Public Health Association (2019): “Social justice is the view that everyone deserves equal rights and opportunities—this includes the right to good health.” The tension between identifying health care as a private or public good is remarkably salient in the United States today. Further, it is ironic that one justification for each perspective is justice.
A MIXED HEALTH CARE SYSTEM With two opposing views about health care framing the public debate, it is not surprising that the U.S. health care system is a“mixed enterprise,”one in which there is a strong private sector wielding enormous power, as well as a large and influential public sector (Rosenberg, 2006). Neither viewpoint has prevailed. Through the years, policy makers have compromised and cooperated to create the system we have today, which is influenced by both perspectives. Key reasons for the mix of public and private sectors in the health care system have to do with historical precedent, pragmatism, and preference for checks and balances on power, which are briefly discussed next.
Historical Roots The “mixed enterprise” has historical roots that transcend health care. As Rosenberg (2006) explains: There is nothing more fundamental in the history of American health care than the mixture of public and private. In this regard, American distinctiveness lies not in some unique devotion to the market and individualism, but in a widespread inattention to a more complex reality. From the canal and railroad land grants in antebellum America to support for the aircraft industry in the twentieth century, from tariff policy to the creation of the corporation in the nineteenth century to today’s outsourcing of military functions, the interactive and mutually constitutive mixture of public and private has been so ubiquitous in American history as to be almost invisible; it is as true for medicine as it is and has been for transportation or the military-industrial complex…. It is a tradition with roots older than the nation itself. (pp. 14–15)
Goldsteen74024_08_CH08_273-296_03-18-20.indd 281
3/20/20 1:02 PM
282
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Thus, government and the private sector have a long history of shared engagement in the health care system. Prior to the mid-1960s, government was involved mainly in only four areas: providing money to train physicians and other health care workers; funding medical research, primarily through the National Institutes of Health (NIH); funding public health activities such as epidemic control at the federal, state, and local levels; and providing medical services to special populations, principally the military, both active and retired, and the mentally ill. Consistent with Rosenberg’s (2006) assertions, these governmental activities included the private sector, as well. Government research laboratories, universities, nonprofit research organizations, and commercial enterprises have long undertaken research with government and nonprofit funds or with profit expectations. Typically, the more basic research is government funded, whereas for-profit pharmaceutical and medical device manufacturers undertake development and commercialization. Furthermore, training of the workforce, especially physicians, is typically provided by private, nonprofit (and some for-profit), and state universities and colleges with substantial government support and oversight. Licensing of medical professionals is often required by state regulations, but the exams may be designed by nonprofit professional organizations and/or administered by for-profit testing services. After the mid-1960s, government involvement increased markedly because of the passage of the Medicaid and Medicare legislation in 1965 and, later, the Children’s Health Insurance Program (CHIP). However, the private sector maintained a vital role in the health care system, and the joint provision and administration of health care services continued and evolved.
Pragmatism A major reason for government’s presence in the health care system, especially today, is cost. Most people cannot afford the full costs of their health care, and the private sector has no incentive or obligation to subsidize them. The mixed enterprise system addresses this financing problem—government assumes responsibility for those who are not profitable for the private sector. The national healthcare expenditure (NHE) per household illustrates the problem. In 2017, the per household cost of health care was US$29,000, compared to the median household income of US$60,336 for the same time period. And at US$29,000, the per household cost of health care was also much greater than the median rent or owner costs for housing— US$12,276 and US$18,696, respectively (U.S. Census Bureau, 2018a, 2018b). However, we must look beyond aggregate statistics to understand fully the problem of financing health care for individuals and families. First, health problems are not uniformly distributed in any society, nor are they predictable except statistically. Older people are more likely to have a chronic health condition than younger people, but not every older person will need exceptional levels of medical care and not every young person will be free from illness. Injuries occur more frequently among the very young than among middle-aged adults, but a particular middle-age individual cannot count on not needing treatment for an injury. The need for medical care is a probability, and some people have higher probabilities than others, but there is no certainty that a particular individual will require or not require medical treatment. The uncertainty of need is compounded by the variability in cost and ability to pay. The price of medical care ranges from inexpensive—like a course of antibiotics for a bacterial infection—to hugely expensive, like cancer treatment, which can cost hundreds of thousands of dollars. In addition, the ability to pay for health care is not equally distributed among people. Few persons can expect to afford all needed medical care without insurance. Most cannot. Nor can the average person, even the most resourceful, budget for health care costs because of uncertainty. How much medical care will any individual need during his
Goldsteen74024_08_CH08_273-296_03-18-20.indd 282
3/20/20 1:02 PM
8
■
D e b a t e s Th a t H a v e S t r u c t u re d H e a l t h C a re S y s t e m C h a n g e
283
or her life? This question cannot be answered with certainty. The health care scenario that a particular person will face in the course of his or her lifetime is unknown and unknowable. Engaging in healthy behaviors and taking other actions to promote health can reduce risk, but does not eliminate uncertainty. Even with health insurance, medical expenses can overwhelm individuals. For example, a study in 2015 found that roughly 25% of Americans 18 to 64 years old had problems paying medical bills, and about 45% of these reported major consequences for their lives, including cutting back on food and other essentials, mortgaging a house, and taking a second job. There were insured and uninsured among the persons studied (Kaiser Family Foundation, 2018). The private sector has no incentive or obligation to subsidize people who cannot afford their health care. The mixed enterprise system provides a solution to this problem by having the public sector pay.
Preference for Checks and Balances The health care system fits quite well with the American preference for a system that constrains power and encourages compromise and cooperation. The system is driven by an interplay of competing forces—public and private—that seek to have their interests represented. Different levels of government vie with one another for influence, as they have since the founding of the republic. This system of checks and balances makes it less likely that any one level, federal or state, will become too powerful, and ensures that the overall system will receive input from each. The regulatory structure is an example of public–private partnership. Private organizations, such as The Joint Commission and medical specialty boards, which are composed of professionals who actually work in the field, inject technical expertise. These organizations are balanced by government agencies, which provide a more disinterested external perspective that is presumably less subject to economic self-interest. In essence, the system benefits by receiving regulatory input from varying perspectives. State and local agencies are often closest to the actual provision of health care and the most sensitive to regional needs. Federal oversight is usually necessary to provide national coordination, for example, to prevent physicians who have been disciplined by a medical board from gaining licensure in another state. Private organizations offer the deepest expertise in the clinical aspects of care (Field, 2008).
Mixed-Enterprise Trade-Offs Our mixed-enterprise health care system—based on history, pragmatism, and preference for constraining power through checks and balances—works. It gives voice to those all along the ideological spectrum and, in the past, has facilitated compromise and cooperation. It is also uniquely American, which we like. However, this mixed-enterprise system has costs. So far, the system has not achieved peak performance goals—quality, equity, and efficiency. About 10% of Americans do not have health insurance. Care is provided inefficiently compared to our peers. The United States has worse health outcomes than similar countries. There have been trade-offs.
MAKING POLICY AND BRINGING CHANGE The history of the U.S. health care system has been one of pragmatic, incremental change, typically focused on requiring the least possible modification to address a striking problem that has entered the public’s consciousness. Change has favored private-sector inclusion,
Goldsteen74024_08_CH08_273-296_03-18-20.indd 283
3/20/20 1:02 PM
284
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
and major government intervention and regulation has been avoided if possible. When the market has failed or, worse, vulnerable populations have been injured, the government has stepped in but almost always with the minimum protections needed to “stop the bleeding.” Policy debates are contested along ideological lines, and then resolved, usually through compromise. A simplification of health policy debates is that those favoring the public goods perspective emphasize access to health care. They tend toward concern for decreasing the number of uninsured and reducing other access issues such as lack of resources in medically underserved communities. They are more likely to sacrifice efficiency for equity. Those arguing from the private goods perspective tend toward concern for the cost of health care and the effect of increasing costs on the overall economy. They are more likely to sacrifice quality and equity for efficiency. Compromise is commonly led by moderates, who look for common ground and eschew rigid ideological approaches. They seek needed change that is “something everyone can live with.”For them, there are shades of gray, not black and white. An expression of this thinking is found in Atul Gawande’s exploration: Is Health Care a Right? One of the people he interviewed held this nuanced view, after experiencing serious health problems himself: He (Mark) no longer opposed the requirement that people get insurance coverage. Fire insurance wouldn’t work if people paid for it only when their house was on fire, and health insurance wouldn’t work if people bought it only when they needed it. He was no longer interested in repealing protections for people like him …. “But that doesn’t mean I have to sign on for full-blown socialism—cradle-to-grave everything,” Mark said.“It’s a balance.” (Gawande, 2017, paras 60–63) Gawande concludes: Our willingness to trust in efforts like health reform can be built on experience, as happened with Mark, though we must recognize how tenuous that trust remains. Two sets of values are in tension. We want to reward work, ingenuity, self-reliance. And we want to protect the weak and the vulnerable—not least because, over time, we all become the weak and vulnerable, unable to get by without the help of others. Finding the balance is not a matter of achieving policy perfection; whatever program we devise, some people will put in more and some will take out more. Progress ultimately depends on whether we can build and sustain the belief that collective action genuinely results in collective benefit. No policy will be possible otherwise. (2017, paras 63 and 64) Of course, even when there is agreement on overall goals, there is often disagreement on how to reach them, which opens the door for further discussion, compromise, and cooperation. In recent times, for example, there was a fair amount of agreement among health policy makers and stakeholders that health care quality could be improved through utilization management, care management, and evidence-based medicine (Kindig, 1997; Shortell, Gillies, Anderson, Erickson, & Mitchell, 2000). How these concepts might be implemented, by whom, in what time frame, and at what cost were other matters entirely.
Future of the Mixed Enterprise Recently, the intensity of health policy debates has increased, taking a toll on the policymaking process. Intensification may be related to the marked growth of the health care system— both public and private—since 1960. As discussed in Chapter 6, Financing the Health Care System, the health care system has grown dramatically since then in expenditures and
Goldsteen74024_08_CH08_273-296_03-18-20.indd 284
3/20/20 1:02 PM
8
■
D e b a t e s Th a t H a v e S t r u c t u re d H e a l t h C a re S y s t e m C h a n g e
285
percentage of the gross national product. For those who view health care as a private good, these changes have been worrisome because much of the growth was in the public sector. Prior to the mid-1960s, medical care delivery was primarily a “cottage industry” made up of individual or small groups of providers paid for their services directly by patients, or their employer-based insurance, on a fee-for-service basis. Medicare and Medicaid brought about a momentous shift in public-sector involvement in the health care system, moving it beyond its traditional purview of medical research, workforce training, public health, and provision of medical care for certain special populations. By funding medical care for the elderly (Medicare) and the poor (Medicaid), these programs brought the public sector into the business of actually providing and funding medical care directly and for large sections of the general population. Moreover, both programs have grown steadily in size of expenditures, number of people served, and influence on hospitals, physicians, and other providers since their inception. For those who believe health care is a public good, the changes began at about the same time. As the public sector was increasing, the private sector, particularly the for-profit sector, was developing too. There was tremendous growth among for-profit health care companies in traditional service areas such as supply of therapeutics, including pharmaceuticals, medical supplies, and medical devices; and new service areas such as supply of information technology. In addition, for-profit insurance companies, such as Prudential and Aetna, entered the health insurance market, changing it from a mainly private, nonprofit arena based on community rating to a for-profit one, based on experience rating.1 Finally, companies such as UnitedHealth Group, Tenet, Triad, and Humana were developed to provide direct medical care through integrated systems of care from ambulatory, hospital, rehabilitation, home health, to nursing home. These for-profit corporations stand in sharp contrast to the “cottage industry” providers of the past. Much as local banks have been replaced by large national and international banking corporations, United Health Care, Tenet, and others with Wall Street money exemplify the same trend in the direct provision of medical care. The growing private-sector presence has concerned those who believe health care is a public good. Preference for health care as private or public good has more and more been along political party lines. As discussed in Chapter 10, History of Change From 1900 to 2010: Comprehensive Reform, passage of the ACA was a hard-fought battle mostly by Democrats, who tend to favor the public goods view and thus focused the ACA on achieving universal access to health care. Since its passage in 2010, the ACA has been relentlessly undermined by Republicans, who tend to favor the private-goods perspective. By the fall of 2019, the pressure from Republicans to repeal and replace the ACA remained strong, although no replacement was on the table. Democrats are equally motivated to save the ACA or replace it with a program even more rooted in the public sector.
U.S. HEALTH CARE SYSTEM COMPARED TO PEER COUNTRIES When thinking about private versus public involvement in the health care system, one should consider that no modern health care system is 100% private, as even “public health” systems depend on an economy of private suppliers and, very likely, at least some option for private physicians, hospitals, and other services. And although the debate about the U.S. health care system is often posed as “government-run health care” or a “socialist health care system” versus a “free-market model,” these two extremes do not really exist, at least among peer countries in the Organisation for Economic Co-operation and Development (OECD). The reality across all modern economies is that health care systems depend on a mix of private enterprise and public involvement.
Goldsteen74024_08_CH08_273-296_03-18-20.indd 285
3/20/20 1:02 PM
286
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Virtually every government takes responsibility for public health, but countries have made different choices about the aspects of medical care they defer to the private sector and those that the government operates directly. Even among the OECD countries with the highest share of government funding, such as Norway, depend on private physicians and hospitals to deliver care. Although 66% of France’s inpatient beds are in public hospitals, 25% are in for-profit hospitals, a higher percentage than the United States (Commonwealth Fund, 2015; OECD, 2015). However, all OECD countries have primarily public systems, whereby the government ensures health care for all residents through direct provision of services (e.g., United Kingdom), universal health insurance (e.g., Canada), or a mix of these. The U.S. health care system is unique. Although there is a public/private mix, we have one of the lowest rates of government funding for health care among OECD countries (48% across all states and multiple federal executive departments), which results in limited ability to affect fundamental change in the system (OECD, 2015). Furthermore, the U.S. health care financing system is much more complex than those of other countries. There is no primary payer of health care. Rather, funding flows from patients, myriad private payers, and multiple government programs to the thousands of providers of care.
FRAMEWORK FOR ANALYZING HEALTH CARE POLICY In the following chapters, we will discuss health policies that have been considered in the United States since 1900. Some of these were enacted; most were not. While reading about these policies, readers will benefit by thinking about each in terms of the following framework. This will provide insight into the orientation of the proponents and opponents of each policy and their motivations for support or opposition.
What Information Is Needed to Understand Specific Health Policy Proposals The key questions that need to be answered about health care policy proposals are: • •
• •
•
What problems with the status quo motivate the desire for change? • What are the system performance goals of the proposed change? How does the new policy propose to achieve these system performance goals? • How would one or more of the building blocks of the health care system be changed? • What are the likely indirect impacts on other building blocks from the proposed changes? What stakeholders of the health care system are affected by the proposed changes? • Are the changes negative or positive for each affected stakeholder? What are the factors affecting support or opposition to the new policy? • How does self-interest affect support for policy changes? • How does ideology affect support? • How do political ties affect support? For policies that are implemented, what have been the results? • What worked as planned? • What did not work?
Goldsteen74024_08_CH08_273-296_03-18-20.indd 286
3/20/20 1:02 PM
8
■
D e b a t e s Th a t H a v e S t r u c t u re d H e a l t h C a re S y s t e m C h a n g e
287
Context of Health Care Policy Debates As discussed in Chapter 7, Health Care System Performance, assessment of a health care system’s performance drives change and the desire for change. Is the system generally seen as performing well or poorly? This assessment is based on performance criteria, and performance of all health care systems can be evaluated on three criteria: equity, efficiency, and quality (or effectiveness) of health care. These criteria can be measured at the organizational level and the population level—groups, communities, and societies. When we are dealing with national health policy, our measures are mostly at the population, rather than organizational, level. Efficiency, for instance, concerns what combination of inputs produces the greatest health improvements in a population, given the available resources (Aday et al., 2004). Quality concerns whether the system achieves improvements in population health. However, just because health care systems are evaluated on the same criteria does not mean that they organize, manage, and finance their system’s building blocks in the same way. Quite the opposite. Different health care systems throughout the world attempt to achieve equity, efficiency, and quality in different ways. Thus, the organization and interaction among the common building blocks of a health care system vary tremendously. In addition, health care systems can place different emphases on the three criteria. For example, some countries emphasize quality over efficiency; others prioritize equity.
Factors Affecting How a Health Care System Is Organized to Achieve Equity, Efficiency, and Quality Factors that affect how a health care system is organized include resources, history, and the amount and kind of population health needs. Another important factor is societal values. In this regard, a crucial distinction between health care systems is the amount and kind of public- and private-sector involvement. There is a range extending from almost completely public to almost completely private. A country’s preference for private- or public-sector action has a huge impact on how its health care system is organized, managed, and financed to achieve equity, efficiency, and quality.
How Preference for Private or Public Involvement Impacts the U.S. Health Care System Along the continuum of private to public involvement, the U.S. health care system lies between the two extremes. It is a complex mix of public and private activities that reflects America’s continuing debate over the appropriate roles for private enterprise and the public sector. This debate has led to our complex health care system, in which both private and public sectors play important roles. Indeed, throughout our history, the public versus private debate has been adjudicated by policy makers whenever they considered whether and how to change the health care system—as will be discussed in Chapter 9, History of Change From 1900 to 2010: Incrementalism; Chapter 10, History of Change From 1900 to 2010: Comprehensive Reform; and Chapter 11, The Affordable Care Act: Achievements, Limitations, and Opposition. Thus, regardless of the stated goals of U.S. health care system reform—reduced cost, increased access to health care, better-quality health care—policy options have varied according to their proponents’ beliefs about the appropriate roles for public and private action. Furthermore, changes often reflect pendulum swings between public and private policy solutions when a convincing case is made that we have gone too far in one direction or the other.
Goldsteen74024_08_CH08_273-296_03-18-20.indd 287
3/20/20 1:02 PM
288
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
How Economic Principles Apply to Health Care Economics in the United States In economics, the three fundamental questions that need to be answered are: • • •
What to produce? How to produce? For whom to produce?
A fourth economics question comes up—perhaps unique to health care economics— which is, Who bears the cost? In a pure market economy, these questions would be determined by market forces— health care products and services would be produced to meet the demand of those who had money to afford them, and producers would determine the most efficient organizations and processes to do this efficiently. Challenges for achieving efficiency in a health care system with market solutions: •
•
•
•
Efficient markets depend on rational individuals who are the best judge of their own welfare, have sufficient information to make good choices, and can accurately predict the results of their consumption decisions. • Aside from challenges with the increasing complexity of medicine, where much remains unknown and even what is known remains unevenly distributed among doctors, most individuals don’t have the knowledge or expertise to make rational decisions about health care. • This becomes a form of the agency problem (e.g., patients often do not know what they are buying and at what price and they pay what doctors bill). • More complicated are those individuals who are decidedly not rational—those with mental and behavioral health problems, as well as those unconscious or similarly incompetent. Market efficiency may be limited when firms have market power and/or there are barriers to firms entering a market. • The vast majority of health care utilization in the United States is local—from routine visits to a physician to emergency care—and great health care at great prices 500 miles away is unlikely to divert people from local options except in the case of planned and significant procedures (e.g., total hip replacement surgery) or needs that local providers cannot meet. • Some markets simply do not have the scale to support multiple competing providers with the scale to offer efficiency with present standards of care. • Outside of major cities, the market for acute care is likely a monopoly or oligopoly, and with the need for vertical integration, coordination of care, and even cooperation for admitting privileges, even ambulatory care, may more closely resemble an oligopoly if not a monopoly. In the case of infectious diseases, those who can afford health care may still be at risk from those who cannot afford it. • Providing health care outside the market to ensure surveillance and other public health activities may be justified, similar to government activities for the common defense. In extreme cases, health care services can have infinite value to the consumer. • In traditional microeconomics, goods and services have a high but finite decreasing value relative to quantity consumed.
Goldsteen74024_08_CH08_273-296_03-18-20.indd 288
3/20/20 1:02 PM
8
■
D e b a t e s Th a t H a v e S t r u c t u re d H e a l t h C a re S y s t e m C h a n g e
289
•
•
When the next-best alternative to not accessing health care is death, the market clearing price for services can be unbounded—arguably patients would be better off paying all the money they have or could get if it meant living rather than dying. • Since death is irreversible, warranties and similar types of guarantees used in other markets are less likely to mitigate these issues. Last, a market economy does not distribute goods and services evenly or even according to objective need, but many people are challenged to see their fellow citizens dying or suffering for lack of access to health care.
While efficiency, quality, and equity are the common criteria that we use to evaluate a health care system, the high-level inputs to its design include answers to the following questions: • • • •
For whom and at what cost are different health care products and services available? How are these health care products and services produced? How much will be spent on each of the building blocks? Who bears the cost of these expenditures?
Additional critical design inputs include how are funds allocated, how do they flow through the system, and what are the drivers of payment?
SUMMARY The tension between those claiming health care as a private good or public good is remarkably salient in the United States today. In his preface to the landmark report of the IOM’s Committee on the Future of Public Health, Remington (IOM, 1988) summarized the issues concerning public and private involvement in terms that, for better or worse, still apply: But what is the most appropriate nature of that governmental presence? How should government’s role relate to that of the private sector? How should governmental responsibility for public health be apportioned among local, state, and federal levels? Should government be the health care provider of last resort or does it have a greater responsibility? Should public health consist only of a necessary residuum of activities not met by private providers? How should governmental activities directed toward the maintenance of an environment conducive to health be apportioned among various agencies? But above all, just what is public health? What does it include and what does it exclude? Based on an appropriate definition, what kinds of programs and agencies should be constructed to meet the needs and demands of the public, which is often resistant to an increasing role, or at least an increasing cost, of government? (pp. v–vi) These questions have yet to be answered for the United States. To the question of what kind of change might result from the present and future periods of discontent, we need to assess the power of each sector—public and private—and their interest in promoting certain directions in reform, and the likelihood that one will be more successful than the other. Will the mixed system prevail, or will one sector become dominant?
Goldsteen74024_08_CH08_273-296_03-18-20.indd 289
3/20/20 1:02 PM
290
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
DATA SOURCES Chapters 8 through 11 largely concern policy and legislation related to the U.S. health care system. Following are authoritative sources of information for these topics. They include government websites and past reports from a variety of organizations that have influenced policy and legislation.
Government Sources •
U.S. Congress. The U.S. Congress hosts a website that contains legislation from the Senate and the House of Representatives and all related actions beginning with introduction of each bill. For health care legislation, the site begins with the 1973–1974 congressional session. For each bill, the site includes a summary, the title and text, actions taken, amendments, sponsors and cosponsors, committees that reviewed the legislation, and any related bills. This site also contains links to websites for each state’s legislature for information on state legislation, including bill tracking. Start here to explore information about health care legislation, policy reports, and executive actions: www.congress.gov
•
Federal Register. The Federal Register is the official source for federal agency regulations, proposed rules and notices of interest to the public, as well as executive orders and other presidential documents. It is published daily by the Office of the Federal Register, National Archives and Records Administration (NARA). It was first published in 1936. The information in the Federal Register became available electronically in 2014, although print copies can be obtained for a fee. Start here to explore information in the Federal Register: www.federalregister.gov
•
White House. The White House hosts a site that contains information about the president’s briefings, statements, and actions, including executive orders. Start here to explore information on this site: www.whitehouse.gov
Influential Reports on the U.S. Health Care System, 1927–2005 In a review of the Ehrenreich and Ehrenreich (1971) book, The American Health Empire: Power, Profits, and Politics, which appeared in the International Journal of Health Services (1972), Dr. Milton Roemer listed a series of other reports going back many more years: Every few years, more recently in the last decade, there appears a book analyzing the serious defects of health care in America. In 1927, Harry H. Moore produced American Medicine and the People’s Health, in the 1930s were the magnificent 27 volumes of the Committee on the Costs of Medical Care, in 1939 there was James Rorty’s American Medicine Mobilizes, and in 1940 Hugh Cabot’s The Patient Dilemma. After World War II, Carl Malmberg wrote 140 Million Patients in 1947, Michael Davis wrote Medical Care for Tomorrow in 1955, and Richard Carter wrote The Doctor Business in 1958. In 1965, there was Selig Greenberg’s excellent The Troubled Calling: Crisis in the Medical Establishment. The year after Medicare, 1966, saw two critical outputs: The American Health Scandal by Raul Tunley and The Doctors by Martin L. Gross. In 1967, there was Fred J. Cook’s Plot Against the Patient and in 1970 Ed Cray’s In Failing Health. (p. 119) It is fascinating that, allowing for changes in magnitude, many of these analyses and the recommendations they make are similar in so many ways. It is also fascinating that three
Goldsteen74024_08_CH08_273-296_03-18-20.indd 290
3/20/20 1:02 PM
8
■
D e b a t e s Th a t H a v e S t r u c t u re d H e a l t h C a re S y s t e m C h a n g e
291
quarters of a century after Dr. Moore’s book appeared, such books, referred to and cited in the text (e.g., the IOM’s Crossing the Quality Chasm, Himmelstein and Woolhandler’s Bleeding the Patient, and Kleinke’s Oxymorons), are still being written. This is the case because not only do many of the problems of cost, distribution, coverage, and quality that past works highlight remain with us, but because of the changes in their magnitude over time—they are only getting worse. Additional reports from 1960 through 2005 include the following: Aday, L. A. (2001). At risk in America: The health and health care needs of vulnerable populations in the United States. San Francisco, CA: Jossey-Bass. Citizens’ Board of Inquiry into Health Services for Americans. (1971). Heal yourself [Report]. Washington, DC: Author. The crisis in American medicine. (1960, October). Harper’s Magazine, p. 123. Ehrenreich, B., & Ehrenreich, J. (1971). The American health empire: Power, profits, and politics. New York, NY: Vintage Books. Health Task Force of the Urban Coalition. (1969). Rx for action [Report]. Washington, DC: Author. Himmelstein, D., & Woolhandler, S. (2001). Bleeding the patient: The consequences of corporate health care. Monroe, ME: Common Courage Press. Institute of Medicine. (2000). To err is human: Building a safer health system. Washington, DC: National Academies Press. Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academies Press. Institute of Medicine. (2003). Unequal treatment: Confronting racial and ethnic disparities in health care. Washington, DC: National Academies Press. Institute of Medicine. (2004). Patient safety. Achieving a new standard for care. Washington, DC: National Academies Press. Jonas, S. (1978). Medical mystery: The training of doctors in the United States. New York, NY: W. W. Norton. Kennedy, E. M. (1972). In critical condition: The crisis in America’s health care. New York, NY: Simon & Schuster. Kleinke, J. D. (2001). Oxymorons: The myth of a U.S. health care system. San Francisco, CA: Jossey-Bass. Knowles, J. H. (Ed.). (1977). Doing better and feeling worse. New York, NY: W. W. Norton. Moskin, J. R. (1964, November 3). The challenge to our doctors. Look, p. 26. National Commission on Community Health Services. (1966). Health is a community affair. Cambridge, MA: Harvard University Press. Ribicoff, A., & Danaceau, P. (1972). The American medical machine. New York, NY: Saturday Review Press. Schorr, D. (1970). Don’t get sick in America. Nashville, TN: Aurora Publishers. Silver, G. A. (1976). A spy in the house of medicine. Germantown, MD: Aspen Press. Somers, A. R., & Somers, H. M. (1977). Health and health care. Germantown, MD: Aspen Press.
Goldsteen74024_08_CH08_273-296_03-18-20.indd 291
3/20/20 1:02 PM
292
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
STUDY QUESTIONS 1. What are private goods and public goods? 2. Why would one view health care as a private good? What are some implications of doing so? 3. Why would one view health care as a public good? What are some implications of doing so? 4. How has the tension between the two perspectives—health care as a private good versus health care as a public good—been resolved in the U.S. health care system? 5. What recent changes in the U.S. health care system concern people who favor health care as a private good? 6. What recent changes in the U.S. health care system concern people who favor health care as a public good?
NOTE 1. Community rating means that the cost of a health insurance premium is the same for everyone regardless of differences in health status, prior utilization of health care, or other factors that increase the risk of requiring health care in the future. With experience rating, people pay different amounts based on these factors, with people at low risk paying less than people at high risk.
REFERENCES Aday, L. A., Begley, C. E., Lairson, D. R., & Balkrishnan, R. (2004). Evaluating the healthcare system: effectiveness, efficiency, and equity. Chicago, IL: Health Administration Press. American Public Health Association. (2019). Social justice and health. Retrieved from https://www.apha.org/what-is-public-health/generation-public-health/our-work/ social-justice Centers for Disease Control and Prevention. (1999). Achievements in public health, 1900– 1999. Mortality and Morbidity Weekly Review, 48(38), 849–858. Retrieved from https:// www.cdc.gov/mmwr/preview/mmwrhtml/mm4838a2.htm#fig1 Committee on the Costs of Medical Care. (1970). Medical care for the American people (Original work published 1932 by University of Chicago Press). Washington, DC: U.S. Department of Health, Education, and Welfare. Committee for Economic Development. (1973). Building a national health-care system: A statement on national policy. New York, NY: Author. Commonwealth Fund. (2015). International profiles of health care systems, 2014. Retrieved from https://www.commonwealthfund.org/publications/fund-reports/2015/jan/international -profiles-health-care-systems-2014-australia-canada Editors of Fortune Magazine. (1970). Our ailing medical system: It’s time to operate. New York, NY: Harper & Row. Field, R. I. (2008). Why is health care regulation so complex? Pharmacy and Therapeutics, 33(10), 607–608. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2730786/ Gawande, A. (2017, September 25). Is health care a right? The New Yorker. Retrieved from https://www.newyorker.com/magazine/2017/10/02/is-health-care-a-right Ingham, S. (2019). Public good. Encyclopedia Britannica. Retrieved from https://www.britan nica.com/topic/public-good-economics
Goldsteen74024_08_CH08_273-296_03-18-20.indd 292
3/20/20 1:02 PM
8
■
D e b a t e s Th a t H a v e S t r u c t u re d H e a l t h C a re S y s t e m C h a n g e
293
Institute of Medicine. (1988). The future of public health. Washington, DC: National Academies Press. Kaiser Family Foundation. (2018). 5 charts about Americans and medical bills. Retrieved from https://www.kff.org/slideshow/5-charts-americans-medical-bills/ Karsten, S. G. (1995). Health care: Private good vs. public good. American Journal of Economics and Sociology, 54(2), 129–143. doi:10.1111/j.1536-7150.1995.tb02684.x Kindig, D. A. (1997). Purchasing population health: Paying for results. Ann Arbor: The University of Michigan Press. MacLean, N. (2017). Democracy in chains. New York, NY: Viking Press. Nixon, R. M. (1994, September 19–26). Health care now. Excerpts from speech given by Nixon to Congress on 2/18/1971. The New Republic, p. 11. Organisation for Economic Co-operation and Development. (2015). Health at a glance 2015, OECD indicators. Retrieved from http://www.keepeek.com/Digital -Asset-Management/oecd/social-issues-migration-health/health-at-a-glance -2015_health_glance-2015-en#page173 Pellegrino, E. D. (1999). The commodification of medical and health care: The moral consequences of a paradigm shift from a professional to a market ethic. Journal of Medicine and Philosophy, 24(3), 243–266. doi:10.1076/jmep.24.3.243.2523 Rosenberg, C. E. (2006). Anticipated consequences: Historians, history, and health policy. In R. A. Stevens, C. E. Rosenberg, & L. R. Burns (Eds.), History and health policy in the United States: Putting the past back in (pp. 13–31). New Brunswick, NJ: Rutgers University Press. Shortell, S. M., Gillies, R. R., Anderson, D. A., Erickson, K. M., & Mitchell, J. B. (2000). Remaking health care in America: The evolution of organized delivery systems (2nd ed.). San Francisco, CA: Jossey-Bass. Summary, R., & Henry, E. G. (2019). Private good. Encyclopedia Britannica. Retrieved from https://www.britannica.com/topic/private-good Tanner, M. C. (2017, April 5). Hard truths about health care. National Review (Online). Retrieved from https://www.cato.org/publications/commentary/hard-truths-about-health-care United Nations. (1948). Universal declaration of Human Rights. Retrieved from https://www .un.org/en/universal-declaration-human-rights/ U.S. Bipartisan Commission on Comprehensive Health Care. (1990, September). A call for action. Washington, DC: U.S. Government Printing Office. U.S. Census Bureau. (2018a). Household Income: 2017. Retrieved from https://www.census .gov/library/publications/2018/acs/acsbr17-01.html U.S. Census Bureau. (2018b). QuickFacts, United States. Retrieved from https://www.census .gov/quickfacts/fact/table/US/PST045218
FURTHER READING Goldsteen, R. L., Goldsteen, K., Kronenfeld, J. J., & Hann, N. (1997). Anti-government sentiment and support for public health goals: Are they compatible? American Journal of Public Health, 87(1), 25–28. doi:10.2105/AJPH.87.1.25 Kaveny, M. C. (1999). Commodifying the polyvalent good of health care. Journal of Medicine and Philosophy, 24(3), 207–223. doi:10.1076/jmep.24.3.207.2528
Goldsteen74024_08_CH08_273-296_03-18-20.indd 293
3/20/20 1:02 PM
294
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
APPENDIX Timeline: Development of the U.S. Health Care System, 1763 to 2015 1763: 1798: 1798:
Physicians petition to allow doctors to found societies with licensing powers. Edward Jenner publishes his work on developing a vaccine against smallpox. The Act for the Relief of Sick and Disabled Seamen is signed into law under Present John Adams and later extended to every sailor and officer in the U.S. Navy. It led to creation of marine hospitals and then to the Commission Corps of the U.S. Public Health Service. 1811: Federal government authorizes the first domiciliary and medical facility for veterans. 1813: U.S. Vaccine Agency is established, and the U.S. Post Office is required to carry smallpox vaccine material for free. 1847: The American Medical Association (AMA) is founded. 1854: President Franklin Pierce vetoed a national mental health bill on the basis that it would be unconstitutional to regard health as anything but a private matter in which government should not become involved. 1861–65: The U.S. mobilizes a“support army”to care for the Civil War wounded, advancing the practice of surgery, nursing, and emergency medicine while establishing new legitimacy for physicians. 1877: Louis Pasteur proposed the germ theory of disease. 1895: X-rays are discovered and almost immediately put into use for medical research and diagnostics. 1900: About 100 infants died per 1,000 births. About 850 women died in childbirth per 100,000 births. In some cities, up to 30% of infants died before their first year. 1900: Bertillon or International List of Causes of Death is adopted (predecessor of International Classification of Diseases [ICD]). 1902: The Biologics Control Act is passed to ensure purity and safety of serums, vaccines, and similar products used to prevent or treat diseases in humans. 1906: Pure Food and Drug Act is passed prohibiting interstate commerce in adulterated and misbranded food and drugs, establishing the forerunner of the Food and Drug Administration (FDA). 1910: Flexner Report facilitates new standards for medical schools, essentially endorsing AMA standards and practices as standards for medicine. 1920: AMA opposes compulsory health insurance through a resolution by its house of delegates. 1929: Blue Cross Plans are established to provide “pre-paid” hospital care. 1930: Blue Shield Plans begin providing reimbursement for physician services. 1930: NIH is established for the purpose of discovering the causes, prevention, and cure of disease. 1935: Social Security Act is approved. It does not include compulsory health insurance, as a result of AMA influence. 1938: The Federal Food, Drug, and Cosmetic (FDC) Act of 1938 establishes the FDA to oversee the safety of food, drugs, and cosmetics. 1943: Penicillin is mass produced for the first time. 1940–44: U.S. businesses begin to offer health benefits as they compete for workers during World War II, giving rise to the employer-based systems in place today. 1946: Communicable Disease Center (CDC) is founded by visionary leader in public health, Dr. Joseph Mountin.
Goldsteen74024_08_CH08_273-296_03-18-20.indd 294
3/20/20 1:02 PM
8
1948: 1951: 1955: 1956:
1962: 1965: 1973: 1983: 1986:
1989: 1994: 1996:
1997:
2000: 2001:
2006: 2010:
2015:
2015:
■
D e b a t e s Th a t H a v e S t r u c t u re d H e a l t h C a re S y s t e m C h a n g e
295
AMA launches a campaign against President Truman’s plan for national health insurance; the plan is subsequently defeated. Durham–Humphrey Amendment establishes a system prohibiting sales of many drugs except under prescription from a physician. Health insurance coverage grows to nearly 70% from 10% in 1940. Dependents Medical Care Act of 1956 is passed, beginning the development of the Military Health System of today, which provides health care to active duty and retired military personnel and their dependents. Kefauver–Harris Drug Amendments require drug manufacturers to prove scientifically that a medication is not only safe, but effective prior to marketing. Medicaid and Medicare programs are created to ensure access to health care for the poor and elderly. The Health Maintenance Organization (HMO) Act is signed into law to encourage the development of competition in the health care market. Medicare’s Prospective Payment System (PPS) replaces the generally “cost-plus” reimbursement model that threatened Medicare’s solvency. The Emergency Medical Treatment and Labor Act (EMTALA) requires hospitals to provide appropriate medical screening and stabilizing treatment to anyone who presents for care. New Medicare physician fee schedule replaces previous “customary and usual” rate schedules, while Stark Law limits self-referrals. The Health Security Act of 1993, President Clinton’s plan for health care reform, fails. The Health Insurance Portability and Accountability Act (HIPAA) establishes that the data within the medical record belong to the patient, provides for continuity or “portability” of coverage during changes in health insurance, and gives mental health the same status as physical health. The Children’s Health Insurance Program (CHIP) is signed into law under President Clinton, providing health insurance for children in families that cannot afford insurance but have incomes too high to qualify for Medicaid. U.S. infant mortality rate is 6.9 per 1,000 live births, a nearly 95% decrease since 1900 (Centers for Disease Control and Prevention, 1999). The Human Genome Project consortium publishes a 90% complete sequence of all 3 billion base pairs in the human genome. It is understood to be the blueprint for life. Massachusetts implements plan to provide health care coverage for nearly all state residents, which becomes the model for the ACA under President Obama. Passage of the ACA, which aims to (a) increase access; (b) increase quality; and (c) decrease cost of health care through new regulations and taxes on physicians, hospitals, insurers/payers, drug and medical device companies, and establishes national and state-based health insurance marketplaces modeled after Massachusetts’ program. International Classification of Diseases, Tenth Revision, Clinical Modification (ICD10-CM) is implemented approximately 21 years after the World Health Organization (WHO) developed ICD-10 and 18 years after the CDC’s, National Center for Health Statistics (NCHS) began the first round of testing. The Medicare Access and Children’s Health Insurance Program Reauthorization Act shifts physicians to alternative payment models designed to encourage quality and efficiency.
Goldsteen74024_08_CH08_273-296_03-18-20.indd 295
3/20/20 1:02 PM
Goldsteen74024_08_CH08_273-296_03-18-20.indd 296
3/20/20 1:02 PM
9 History of Change From 1900 to 2010: Incrementalism
© Randy Glasbergen.
LEARNING OBJECTIVES After completing this chapter, students will be able to: • Describe the major developments of the 19th century that laid the foundation for the current health care system. • Describe the incremental changes made to the U.S. health care system during the 20th century to provide access to health care. • Describe the incremental financing and organizational changes made to the U.S. health care system during the 20th century and how they addressed cost and efficiency problems. • Define major organizational developments of the 20th century including health maintenance organizations (HMOs), managed care organizations, and integrated delivery systems (IDSs).
Goldsteen74024_09_CH09_297-318_03-18-20.indd 297
3/19/20 3:04 PM
298
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
INTRODUCTION At the beginning of the 20th century, health care in the United States was predominantly a cottage industry, engaged in by physicians and their assistants, largely students. When the 20th century opened, doctors were mostly solo practitioners; hospitals were single, independent entities; long-term care for the elderly was largely home-based; and pharmaceutical and medical device manufacturing was small business. Health care was a minor part of the economy. However, numerous developments during the 19th century laid the foundation for the complex health care system that emerged during the 20th century, including: •
•
• • •
• •
Founding of the American Medical Association (AMA) in 1847 at the Academy of Natural Sciences in Philadelphia, which established standards for preliminary medical education for the degree of MD and a code of medical ethics; recommended use of anesthetic agents for surgery and obstetrics; noting the dangers of secret remedies and patent medicines; and recommending that state governments register births, marriages, and deaths (AMA, 2019). Improvements in surgery made during the Civil War and application to medicine of advances in bacteriology by scientists such as Louis Pasteur. The latter affected the physician’s ability to control infectious diseases—the leading causes of death at that time. Both advances made the practice of medicine more successful in treating health problems. Demand for therapeutics fueled by the Civil War, which provided the start for some of the largest names in the modern pharmaceutical industry: Wyeth, Pfizer, and Squibb. Founding of the U.S. Nursing Corps in 1861, and with it the idea of professional nursing and its importance to medical care. Development of the Ambulance Corps during the Civil War, creating the ambulance-to-ED system we know today and establishing a hierarchy of treatment stations and hospital facilities (National Museum of Civil War Medicine, 2016). Founding of the Association of Hospital Superintendents in 1899, which became the American Hospital Association (AHA). Adoption of the Bertillon or International List of Causes of Death in 1900, predecessor of the International Classification of Diseases (ICD; WHO, 2016).
These developments and others led to the modern health care system, which includes a professionalized health care workforce working in specialized institutions to deliver health care services, a health care research sector that advances diagnosis and treatment, an industry that provides health care supplies and therapeutics, and a classification and data-collection system to evaluate health care performance. However, as discussed in Chapter 8, Debates That Have Structured Health Care System Change, the U.S. health care system that evolved differs from that of most other developed nations because of how we organized and financed these components. Our values and beliefs determined our response to the need for change and growth. This chapter describes the uniquely American health care system that had resulted by 2010, and the incremental approach that was taken to get there.
ACCESS TO HEALTH CARE As the 20th century began, the value of medical care was increasingly evident. In the medical “tool box” were vaccines and antitoxins, which prevented childhood illnesses; medicines, such as insulin, which saved and extended life; and surgery, which could cure dozens of
Goldsteen74024_09_CH09_297-318_03-18-20.indd 298
3/19/20 3:04 PM
9
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : I n c re m e n t a l i s m
299
conditions, aided by effective anesthesia and the protection of aseptic techniques. International comparisons in rates of illness and death, which became possible with the standardization of vital statistics reporting, emphasized the dramatic differences in both overall death rates and deaths from specific causes as a result of public health improvements and medical care (Center for Medical Humanities, Compassionate Care, and Bioethics, 2012). With medicine’s improved ability to cure disease and treat chronic conditions, the demand for care increased, as did its cost. In response, a major focus of health policy since the early 20th century has been assuring access to health care. Broadly speaking, this effort has been twofold: • •
Provide health insurance in order that patients can afford care and providers are compensated for their services; and Build facilities, particularly hospitals, needed to provide health care.
Both efforts developed in ways that reflect the American preference for private/public policy solutions (see Chapter 8, Debates That Have Structured Health Care System Change). Both public and private sectors were involved in providing health care coverage and building the American health care infrastructure. As a result, health care access varied for people in different groups, ranging from insufficient to luxurious.
Providing Health Insurance Effective drug therapies and safer surgery motivated reformers to extend the reach of professional medical attention to the entire population for the first time. Paying for health care services and therapeutics was a major issue. Only the well-to-do could afford the benefits of improved medical care. This was a problem for both patients and providers, since hospitals and physicians needed paying patients. However, unlike peer countries such as Germany and England, the United States did not develop a government policy that provided universal health care coverage. Rather, the American solution was a mixed public/private sector one that covered many, but not all, people. Access to health care for members of the military and their families, as well as veterans, had become a public-sector initiative. The federal government continued to build a military health care system that was begun in 1811 when the first home and medical facility for veterans was authorized. Later in the 19th century, the nation’s veterans’ assistance was expanded to include benefits and pensions for veterans as well as their widows and dependents. The military system continued to grow and develop during the 20th century and is a major provider of health care today (U.S. Department of Veterans Affairs [VA], 2015).
Developing Employer-Based Health Insurance Meanwhile, the private sector extended health care coverage to a large, but distinct group— the employed. Thus, the United States created a system of employer-based health insurance for nonmilitary workers and their families. In 1910, early forerunners of health insurance plans (HIPs) appeared as“prepaid”group practices. Plan members paid a monthly premium and received a wide range of medical services through an exclusive group of providers. The American system of health insurance developed from there. The leading employer-based HIPs were Blue Cross and Blue Shield. In 1929, Blue Cross plans were established to provide “prepaid” hospital care to workers in the Dallas public school system. Baylor University Hospital came forward with the plan, which provided teachers with hospital care at Baylor in exchange for small monthly payments of 50 cents.
Goldsteen74024_09_CH09_297-318_03-18-20.indd 299
3/19/20 3:04 PM
300
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
The plan was inspired by the observation of a Baylor Hospital official that Americans were spending less on medical care than on cosmetics. He made the assumption that some of the Dallas teachers’ discretionary spending could be used to insure their medical costs (Blumberg & Davidson, 2009). Later, in 1939, Blue Shield plans began providing reimbursement for physician services in additional to hospital expenses. After the United States entered World War II, caps on wages fostered employer-based health insurance as it was used to attract scarce workers. Subsequently, Blue Cross and Blue Shield plans developed nationwide and grew rapidly. They began to unify as one company in the 1940s when together they served 24 million members and included 81 hospital plans and 44 medical plans. By the 1960s, Blue Cross had 52 million members and Blue Shield had 40 million members. Blue Cross and Blue Shield covered 33% of federal employees. The Blue Cross and Blue Shield logos had become “ubiquitous icons in both homes and medical offices across America” (Lichtenstein, 2014, para 10). It is important to note that the Blue Cross and Blue Shield plans were offered by voluntary, nonprofit companies established as charitable and benevolent organizations. As voluntary, nonprofit companies, Blue Cross and Blue Shield could generate profit, but any profit was required to support the mission of the organization. Profits could not be distributed to owners or directors. This model was established from the start with the Baylor Hospital plan and maintained until 1994. The Baylor prepaid hospital plan was created to be distinct from traditional commercial insurance. As a nonprofit plan, one of its earliest brochures boasted that,“Baylor uses no sales agency or middlemen, but prefers to deal directly with each group so that all group hospitalization fees paid may be used only for hospital care of members and not for any personal profit.” (Cunningham & Cunningham, 1997) Consistent with their charitable mission, Blue Cross and Blue Shield plans used community rating, not experience rating, to set prices for their products. Community rating refers to insurance pricing whereby everyone in the same geographic area pays the same premium, regardless of their health status, age, gender, family composition, occupation, health behaviors such as smoking, or claims history. In contrast, experience rating tailors policies and premiums to a particular group or individual. With experience rating, premiums are based on the insured person’s prior claims, health status, and risk of future claims as indicated by his or her age, gender, health behaviors, and so forth.
Extending Health Insurance to the Unemployed By the mid-20th century, it was clear that inconsistent access to health care was a problem that needed attention. As care grew more and more expensive as a result of new diagnostic and treatment methods, the gaps in coverage were increasingly untenable for patients and providers. The unemployed and their families were not covered. Although there were charitable and municipal health care providers, these increasingly failed to meet the needs of the unemployed, including the growing elderly population removed from the workforce by retirement. As a result, between 1965 and 1999, Congress passed legislation that provided health insurance to three groups not covered by employer-based insurance: • • •
Medicare for people 65 and older; Medicaid for uninsured, low-income people; and Children’s Health Insurance Program (CHIP) for uninsured, moderate-income children.
Goldsteen74024_09_CH09_297-318_03-18-20.indd 300
3/19/20 3:04 PM
9
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : I n c re m e n t a l i s m
301
The campaign for Medicare was long and arduous (Harris, 1966a, 1966b; Stevens, 1971). Legislation creating it and its afterthought companion, Medicaid (Friedman, 1995), was passed by Congress in 1965 (Committee on Finance, 1979; Goldfield, 2000, Chapter 8, Debates That Have Structured Health Care System Change). Both had their historical antecedents. For example, the earliest American Association of Labor Legislation (AALL) proposals contained the concept of beginning with partial coverage, aimed at the working poor. (In contrast, Medicaid covers primarily the nonworking poor.) Medicaid-like proposals had appeared in a bill authored by Sen. Robert Wagner, D-N.Y., before World War II. Determination of an eligible population by age as in Medicare was a relatively new twist, going back only to 1950. However, in a failure to follow the example of the world’s other industrialized countries, since 1965 the progression from some sort of partial coverage to comprehensive coverage, or close to it, did not take place in the United States because of the strength of the political and health care system opposition to such change. In 1997, approximately 10 million children were without health insurance. The Children’s Health Insurance Program (CHIP) was passed to address this problem for uninsured children in families with incomes too low to qualify for Medicaid. The CHIP was included in the Balanced Budget Act of 1997, which was sponsored by Senrs. Edward Kennedy D-Mass., and Orrin Hatch, R-Utah.
Filling Gaps in Health Care Coverage: EMTALA and HIPAA After the passages of Medicare and Medicaid, two federal health policies were enacted in the latter years of the 20th century to solve problems related to health care coverage: • •
the Emergency Medical Treatment and Labor Act (EMTALA); and the Health Insurance Portability and Accountability Act (HIPAA).
The complex system of private and public health insurance, with many people covered through employment, created gaps in coverage. For example, people who changed jobs or lost jobs were vulnerable if they experienced a serious health event before coverage could be reestablished. The EMTALA of 1986 required Medicare-participating hospitals with active EDs to provide appropriate medical screening and stabilizing treatment. “Dumping”—the denial or limitation of medical services to a patient for economic reasons and referral of the patient to another facility—had been identified as a problem despite its prohibition by The Joint Commission on Accreditation of Healthcare Organizations (JCAHO, now The Joint Commission) and the American College of Emergency Physicians. The EMTALA was passed after several highly publicized reports of “dumping.” The act is now considered one of the most important laws guaranteeing nondiscriminatory access to emergency medical care and the health care system in general. Through interpretations by the Centers for Medicare & Medicaid Services (CMS) and the courts, the EMTALA potentially applies to virtually all aspects of patient care in the hospital setting (Zibulewsky, 2001). The HIPAA of 1996 brought about a number of significant improvements in access to health coverage. It mandated continuity or “portability” of coverage in the large group, small group, and individual health insurance markets. It also mandated that health insurance cover at least a two-day hospital stay for women who give birth vaginally and four days for cesarean deliveries (C-sections). Mental health was given the same status as physical health by the HIPAA legislation. Furthermore, privacy standards related to personal health information were established under HIPAA. The act established that the data within the medical record belong to the patient, whereas the physical form the data take belongs to the entity responsible for maintaining the record. Patients have the right to ensure that the
Goldsteen74024_09_CH09_297-318_03-18-20.indd 301
3/19/20 3:04 PM
302
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
information contained in their record is accurate, and can petition their health care provider to amend factually incorrect information in their records. Finally, HIPAA created national standards for certain electronic health care transactions to improve efficiency and privacy (U.S. Department of Health and Human Services [DHHS], 2013). The latter privacy provisions were especially important for individuals who might be discriminated against because of their health status, as was a concern for persons with chronic conditions such as AIDS before HIPAA.
Building Hospitals The hospital developed as the heart of the health care delivery system in the 20th century, and as a result, building hospitals was a major effort. Sick people needed to be diagnosed and treated by providers employing the latest medical methods and medicines. The hospital became the place that brought patients and providers together for this purpose. Similar to health insurance, the hospital sector grew through the mid-20th century in ways that reflected the American preference for private/public policy solutions.
Public Hospitals From the early 1900s through the mid-20th century, hospital development was similar to that of health insurance in its public/private character and emphasis, by the private sector, on voluntary, nonprofit investments for the “public good.” Public hospitals, particularly at the municipal level, were developed to provide care for the poor.“Rooted in this tradition of charity, the public hospital traces its ancestry to the development of cities and community efforts to shelter and care for the chronically ill, deprived, and disabled”(America’s Essential Hospitals, 2005, para 1). Bellevue Hospital in New York City, the oldest public hospital in the United States, is an example of a public hospital that survives today. The public hospital sector was augmented by the federal government’s Marine Hospital Service (later the Public Health Service). The Marine Hospital Service was developed to serve seamen in the 19th century and later was “expanded greatly beyond the medical relief of the sick seamen to include the supervision of national quarantine (ship inspection and disinfection), the medical inspection of immigrants, the prevention of interstate spread of disease, and general investigations in the field of public health, such as that of yellow fever epidemics” (Kondratas, 2012, p. 3).
Voluntary, Nonprofit Hospitals The private sector produced the voluntary, nonprofit hospital—private hospitals developed as charitable institutions for the “public good.”They often had a religious affiliation—such as Catholic, Lutheran, Jewish, or Methodist. They were tax-exempt and could not distribute any profits to directors or investors. Examples of religiously affiliated hospitals that survive today are Mount Sinai Health System in New York City and Methodist Health System in Dallas. Voluntary, nonprofits made up most of the hospitals in the early years, as they still do. As discussed in Chapter 2, The Settings for Health Care Delivery, the voluntary, nonprofit hospital is still the most common hospital in the United States, accounting for 2,968 of the 5,262 community hospitals in 2019. However, Stevens (1982) points out that, from the start, these private hospitals were often subsidized with public funds. Stevens quotes a leading hospital administrator speaking to the AHA in 1909 who “called his listeners’ attention to the ‘distinctively American practice of appropriating public funds for the support of hospitals managed by private benevolent corporations’”(p. 555). Not surprisingly, this subsidization of private health care institutions by the public sector continues today in a number of different forms.
Goldsteen74024_09_CH09_297-318_03-18-20.indd 302
3/19/20 3:04 PM
9
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : I n c re m e n t a l i s m
303
Government-Funded Community Hospitals The 1946 Hill–Burton Act funded hospital construction in underserved areas throughout the United States. It was actually aimed at preventing government from taking a larger role in the provision of medical care for the general population: Supported by the medical establishment and guided through the Senate by Senator Robert Taft, [the Hill–Burton Act] deflected President Truman’s proposal for a comprehensive health plan by limiting the government’s role to the subsidy of voluntary nonprofit hospitals. (Lipscomb, 2002, p. 109) Despite this legislative intent, many hospitals were built as a result of Hill–Burton. The act eventually helped to finance 9,200 new hospitals and other facilities, assisting in financing almost one-third of all hospital projects in the nation. The Hill–Burton Act improved access to medical care remarkably, particularly in rural areas.
ORGANIZATION AND FINANCING OF HEALTH CARE In the latter half of the 20th century, solo physician practices and single hospitals, like smalltown banks and grocery stores, were becoming obsolete. The demand for health care services was growing. The population had exploded from 76.2 million in 1900 to 180.7 million in 1960. More and more people had health insurance and could afford health care. And a large portion of the uninsured were about to receive coverage through Medicare or Medicaid. Health care costs were also surging. They accounted for about 0.3% of the gross domestic product (GDP) from 1900 through 1930, when they rose steeply to 1.3% GDP in 1960 and 4.1% by 1980 (Ortiz-Ospina & Roser, 2019). In this growth environment, the financing and organization of the health care system underwent several important, incremental changes: • • •
Expansion of capitation and the rise of managed care Growth of vertical and horizontal integration of health care organizations Increase in for-profit health care organizations
Each of these changes is discussed next.
Expansion of Capitation and the Rise of Managed Care Capitation and indemnity health insurance are two contrasting ways to pay health care providers for their services. At the heart of their differences is who assumes the risk for cost of the care—the health care provider or the health care payer. This is how they work. •
•
Capitation is the practice of paying a flat fee to a health care provider in exchange for a stipulated range of services for an individual during a given time period, usually a year. The flat fee guarantees medical coverage for that person regardless of how much or how little care the individual needs or uses. Indemnity health insurance reimburses an individual for fees paid for medical services after they are performed. Payments may be made to the patient or directly to the provider, on a retrospective, fee-for-service basis.
Under indemnity plans, the providers of care are not employed by, contracted to, or owned by the payer (insurer). The insurer simply pays the freight, according to some agreed-to
Goldsteen74024_09_CH09_297-318_03-18-20.indd 303
3/19/20 3:04 PM
304
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
schedule; the financial responsibility (or risk) for the cost of health care provided is borne by the insurer. Under the indemnity system, beneficiaries (in most cases, the beneficiaries’ employers) pay sums (usually called premiums) to the insurance companies, which in turn pay the providers for the care used by the beneficiaries. Under indemnity insurance, payment is made on a fee-for-service or item-of-service basis, after the fact (or “retrospectively”). There are usually some personal payments (deductibles and coinsurance) that the beneficiaries must make themselves, as well as specified limits in dollars and units/types of service that are covered by the insurance package. The increase in capitation occurred concurrently with organizational changes that departed from the solo physician practice financed primarily by indemnity insurance. These changes began with development of prepaid group medical practices, later with health maintenance organizations (HMOs), and then with managed care organizations. Efficiency, cost containment, and improved quality of care motivated these changes, and capitation was seen as a tool needed to achieve these goals.
Prepaid Group Medical Practice Indemnity insurance was the traditional type of insurance provided by both Blue Cross Blue Shield and the commercial insurance companies before the mid-century. However, capitation first appeared on a very limited basis in the 1890s in the form of prepaid group medical practice (MacColl, 1966; Mayer & Mayer, 1985). During the first half of the 20th century, physicians were joining to form group medical practices, which have been defined as: The provision of health care services by three or more physicians who are formally organized as a legal entity in which business and clinical facilities, records, and personnel are shared. Income from medical services provided by the group are [sic] treated as receipts of the group and distributed according to some prearranged plan. (Austrin, 1999, p. 90) Some of these group medical practices were prepaid, and they were the forerunners of organizational forms with capitation as their base—prepaid group medical practices. The two principal modern organizational pioneers of prepaid group medical practice were the HIP of New York City and Kaiser Permanente on the West Coast (MacColl, 1966; Smits, 2002). Both were founded during the Great Depression of the 1930s. They entered periods of significant growth after World War II. As had their much smaller, much poorer predecessors in the early 20th century, prepaid group medical practices encountered much resistance from“organized medicine,”that is, the AMA and the state and county medical societies. The resistance to prepaid group practice was based primarily on an antipathy to the ways in which physicians were paid, which were antithetical to the fee-for-service, piecework system that they would replace. There are two major forms of prepaid group practice. In the staff model, physicians work directly for the prepaid group practice organization on a salaried basis. HIP was an early example. In the group model, physicians join together to form their own company. It, in turn, contracts to provide medical services with the financing and administrative entity that, in turn, sells the prepaid health care coverage package to beneficiaries or their employers. In this case, the physicians’ group company pays its individual members, either on a salary or on a capitation basis. Kaiser Permanente was an early example. Organized medicine also did not like the idea of providing medical care under contracts negotiated between groups of physicians and groups of patients. Organized medicine always claimed that its opposition to capitation and contracts had nothing to do with money, but with principle. It “distorted incentives,”“made the doctor a wage slave,”“interfered with
Goldsteen74024_09_CH09_297-318_03-18-20.indd 304
3/19/20 3:04 PM
9
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : I n c re m e n t a l i s m
305
medical judgment,”“put a corporation between the physician and the patient,” and “removed the symbol (the private fee) of the special relationship between doctor and patient.” (It would do well to remember the old adage, “When they say ‘it’s not the money,’ it’s the money.”) As Silver (1963) and MacColl (1966) noted in the 1960s, there are many advantages of group practices for physicians—which accrue to prepaid group practices, as well. They include the opportunity to share knowledge and responsibility; the establishment of a rational division of labor between generalist and specialist; regularly allotted time for continuing medical education; a regular work schedule; guaranteed (although not necessarily high) income; a fringe benefit package, including malpractice insurance; and better access to ancillary personnel and services. Prepaid group practices have advantages for patients, as well. They include no or low charges at time of service; one-stop shopping for 24-hour, seven-day service; continuity of care; and protection against unnecessary hospitalization and surgery. The primary disadvantages for patients center around the possible development of a clinic atmosphere, loss of choice of physician and hospital, delays in receiving service, locational inconvenience, and impersonality.
Health Maintenance Organizations Under President Richard Nixon, the federal Health Maintenance Organization Act was passed in 1973. President Nixon was interested in the idea because it had been shown that the HMO’s predecessor—the prepaid group medical practice—could save significant amounts of money, primarily by reducing hospitalization rates (Roemer & Shonick, 1973). Today, the National Center for Health Statistics (NCHS) defines HMOs as follows: An HMO is a health care system that assumes or shares both the financial risks and the delivery risks associated with providing comprehensive medical services to a voluntarily enrolled population in a particular geographic area, usually in return for a fixed, prepaid fee. Pure HMO enrollees use only the prepaid capitated health services of the HMO panel of medical care providers. Open-ended HMO enrollees use the prepaid HMO health services but, in addition, may receive medical care from providers who are not part of the HMO panel. There is usually a substantial deductible, copayment, or coinsurance associated with use of nonpanel providers. (NCHS, 2007, p. 505) HMOs are not homogenous, however. The NCHS identifies the following types of HMOs, based on their staffing and ownership models (NCHS, 2007): •
•
•
•
Staff Model.“A type of closed-panel HMO (where patients can receive services only through a limited number of providers) in which physicians are employees of the HMO. The providers see members in the HMO’s own facilities.” Group Model.“An HMO that contracts with a single multi-specialty medical group to provide care to the HMO’s membership. The group practice may work exclusively with the HMO, or it may provide services to non-HMO patients as well. The HMO pays the medical group a negotiated per capita rate, which the group distributes among its physicians, usually on a salaried basis.” Network Model.“An HMO model that contracts with multiple physician groups to provide services to HMO members; may involve large single and multi-specialty groups.” Mixed Model.“An HMO that combines features of more than one HMO model.”
Goldsteen74024_09_CH09_297-318_03-18-20.indd 305
3/19/20 3:04 PM
306
II
•
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Independent Physician Association (IPA). “A type of health care provider organization composed of a group of independent practicing physicians who maintain their own offices and band together for the purpose of contracting their services to HMOs, Preferred Provider Organizations (PPO), and insurance companies. An IPA may contract with and provide services to both HMO and non-HMO plan participants” (NCHS, 2007, p. 505). The physicians remain in their offices, which they own and in which they see HMO enrollees. There is no group practice at any level of abstraction and no pooling of either medical or ancillary service resources. The physicians may be paid on either a capitation or fee-for-service basis by the IPA central organization.
A major difference between group and staff model HMOs, on the one hand, and IPAs, on the other, is that the former have“closed”medical staffs; that is, the HMO or medical group has full control over its members, whereas, in most cases, any physician who can meet the (usually minimal) membership qualifications can join an IPA, at his or her option. It should be noted that, although for the most part any physician can join any IPA, the IPA medical manager usually has the power to“deselect”any physician who does not abide by the IPA’s rules and procedures. Just as there are limitations in using and applying the original definition of an HMO, by the end of the 1990s, there were some still newer organizational forms that the earlier HMO typology did not cover (Barton, 1999, Table 2.1). One of these was the introduction of Point of Service (POS) plans, allowing HMO members to use nonplan providers by paying an additional fee. The POS plan “allows members to choose to receive services from a participating or nonparticipating network provider, usually with a financial disincentive for going outside the network” (NCHS, 2007, p. 505).
Managed Care Although health insurance had traditionally been a major payer of health care costs, the enactment of the HMO Act of 1973 brought about a major change in how health insurance pays for health care, called managed care. Managed care plans are a type of health insurance. They have contracts with health care providers and medical facilities to provide care for members at reduced costs. These providers make up the plan’s network. How much of your care the plan will pay for depends on the network’s rules. Plans that restrict your choices usually cost you less. If you want a flexible plan, it will probably cost more. There are three types of managed care plans: •
• •
Health Maintenance Organizations (HMO) usually pay for care only within the network. You choose a primary care doctor who coordinates most of your care. Preferred Provider Organizations (PPO) usually pay more if you get care within the network, but they still pay a portion if you go outside. Point of Service (POS) plans let you choose between an HMO or a PPO each time you need care. (MedlinePlus, 2018, paras 1 and 2)
Managed care organizations enter into contracts with hospitals, physicians, and other providers to deliver health care to their enrollees (or beneficiaries) at what the managed care organizations believe will be a favorable rate per enrollee for their care (capitated). Key attributes of managed care plans are: •
Selecting providers who will then deliver a comprehensive range of services to enrollees at the agreed upon rate;
Goldsteen74024_09_CH09_297-318_03-18-20.indd 306
3/19/20 3:04 PM
9
• •
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : I n c re m e n t a l i s m
307
Giving economic incentives to providers to choose less costly care; and Reviewing providers’ utilization and quality of care, formally and regularly, through data mining claims data and chart review.
Typically, the primary care provider is the “gatekeeper” who must approve the use of specialists. There are controls on inpatient hospital care and length of stay; and disease management, case management, wellness incentives, and patient education are used to control costs and quality. This matter-of-fact description of managed care disguises the transformational change that it brought about in the U.S. health care system. Managed care organizations shifted the balance of power from providers to payers. Payers entered“the treatment room”with providers, influencing their treatment patterns through reimbursement rates that affect patient flow; through provider incentives that favor certain tests and procedures over others; and through utilization and quality reviews that further constrain provider autonomy in decision-making. Managed care has been a very controversial practice from the start. Critics say it restricts needed access to health care and adversely affects health care quality. The use of economic incentives to providers for limiting certain kinds of health care and the restraint on their fees concern detractors. Proponents argue that managed care reduces inefficiencies and, thereby, costs of the health care system without affecting quality or access. However, two factors make it difficult to evaluate the effects of managed care on cost, quality, and access. •
•
Managed care is almost invisible now because it is so pervasive. All payers— for-profit, nonprofit, and government—have adopted managed care principles and practices to some extent. As an example, the health care reform legislation passed under President Obama in 2010—the Affordable Care Act (ACA)—put managed care principles and practices into place by its focus on effectiveness and efficiency. Managed care plans are so varied that it is difficult to generalize about their effects on cost, quality, and access. The criteria for selection of providers, the limitations on covered services, the reimbursement rates negotiated with providers, and the ways that utilization and quality reviews are used differ widely across plans. Thus, we should expect that the actual quality of care received and the costs of that care will differ, as well. These factors—reimbursement rates, favored services, and utilization review criteria—may be more predictive of quality and cost of health care than whether or not the care was “managed.”
Nevertheless, we refer to managed care as an entity because of its singular influence on the way health care is delivered today in the United States, although its influence on costs, quality, and access appears “not” to be uniform. In the mid-1990s, a longtime observer of the managed care scene laid out a list of what he thought would and should happen under managed care over the next 10 years (Dennis L. Kodner, personal communication with Jonas, autumn 1996): • • • • • •
An increase in the practice of population-based care An increase in the use of physician/nonphysician team care The development of highly sophisticated medical, health, and management information systems The return of physician control Increased public-sector enrollment: Medicare/Medicaid “Carve-outs” (health services sectors set outside the managed care system), for example, mental health, substance abuse, and high-cost subspecialty care
Goldsteen74024_09_CH09_297-318_03-18-20.indd 307
3/19/20 3:04 PM
308
II
• • • •
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Increased insurance company ownership of managed care organizations and decline in insurance company involvement in indemnity insurance Decline of both group and staff model plans with a concomitant rise in other forms, such as the integrated delivery system (IDS) Competition among managed care organizations on the basis of quality Going from managed cost to managed care
A similar list was developed by Barton (1999), who also added rationalization of resource use, greater accountability, more disease prevention and health maintenance, and improved quality. The list by Shortell, Gillies, Anderson, Erickson, and Mitchell (1999) is also similar. However, 20 years later, we see that the emphasis on quality and population health has not occurred as completely as predicted. Luft (2003) has described the problem of defining managed care, and therefore, of evaluating managed care organizations on quality, access, and cost: The collection of health plans commonly referred to as “managed care” has come to include an astonishing variety of forms. Although a few are tightly integrated prepaid group practices, a much larger number reflect the complex mixes of associations of clinicians and institutions into provider groups and insurers that face myriad, sometimes conflicting, incentives and employ widely disparate information systems. Managed care plans also differ in the mix of prepaid and fee-for-service patients they enroll and the associated payor sources with which they must interact. Given this heterogeneity, it is difficult to meaningfully compare the quality of managed care plans as a group to fee-for-service plans or to assess the relative performance among types of managed care plans. (p. 1373) As a result, the controversy that has followed the rise of managed care regarding its ability to meet our health care goals continues today and opinion is mostly unfavorable. For example, we still question the effect of managed care on the doctor–patient relationship. Does managed care affect the relationship between physician and patient? There is evidence brought to bear on both sides of the argument (e.g., Alexander & Lantos, 2006; Light, 2006). Further research may resolve this issue and others related to the desirability of managed care. However, the continual change of managed care organizations in response to critics—both patients and providers—poses difficulties for obtaining convincing answers. Managed care has changed dramatically in response to its critics. For example, the RAND Corp. (Marquis, Rogowski, & Escarce, 2005) put forward two nearly polar opposite explanations for the failure of HMO enrollment to drop in the late 1990s and early 2000s following much reported consumer disfavor with managed care: • •
Many consumers were more satisfied with their HMOs than had been thought; and Many HMOs relaxed their cost-containment restrictions in order to avoid losing market share.
Growth of Vertical and Horizontal Integration of Health Care Organizations Increasingly, individual hospitals needed to affiliate with other hospitals to form systems if they are to remain financially viable. For example, in New York City in 2010, there were 43 general hospitals. Of these, only 17 were independent, and the remaining 26 were members
Goldsteen74024_09_CH09_297-318_03-18-20.indd 308
3/19/20 3:04 PM
9
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : I n c re m e n t a l i s m
309
of just five hospital systems (AHA, 2011). This was not unique to New York, and it is a trend that has been going on since the 1970s, as discussed by Prybil in 1982: The growth of multiunit hospital systems (organizations that include two or more acute-care hospitals owned, leased, or managed by a single corporate entity) and their impact on health care are described. In 1970, there were fewer than 50 nongovernmental multiunit hospital systems in the United States. By 1981, this figure increased to 256; 53% of the systems included only two or three hospital units, whereas 13% included 11 or more units. Approximately one third of all nongovernmental hospitals in 1981 were included in multiunit systems. About 12% of the systems, which included 39% of the hospitals, were owned or operated by investor-owned firms. Multiunit hospital systems can improve the hospital industry’s overall effectiveness and efficiency by achieving economies of scale and by developing hospital performance criteria and standards. In the future, the number and size of U.S. multiunit hospital systems most likely will continue to increase. The nation’s multiunit hospital systems vary enormously in size and composition, as well as in their mission, goals, values, and approaches to governance and management. (1982, p. 1888) In addition, hospitals are increasingly seeking affiliations with nonhospital medical providers in order to coordinate care better across sectors—ambulatory care, home care, and long-term care—and achieve better outcomes. For example, a still-valid definition of the IDS was offered by Kongstvedt, Plocher, and Stanford (2001): “IDSs may be described as falling into three broad categories: systems in which only the physicians are integrated, systems in which the physicians are integrated with facilities (hospitals and ancillary sites), and systems that include the insurance functions” (p. 46). In the past, according to Kodner (personal communication with Jonas, autumn 1996), “Hospitals had doctors; doctors had patients.” Now, increasingly, as the various forms of managed care spread throughout the health care delivery system, it is the payers or the insurance, risk-assuming side of the managed care organizations that has the patients, with both the doctors and the hospitals providing the health care services for the managed care organization—and its patients. Presenting in part a normative definition, that is, what they would have liked IDSs to be, not necessarily what they all are, Shortell, Gillies, and Anderson (1994) defined the IDS as “[a] network of health care organizations that provides and/or arranges a coordinated continuum of care to a defined population, and is willing to be held clinically and fiscally responsible for the outcomes and health status of that population” (p. 46). In the view expressed by Shortell et al. (1999), the IDS would be an essential element in creating their “ideal health care system” (p. 8), having, in summary, the following features: • • • • • • • • •
Serves a defined population Provides a defined set of services/benefits Integrates services, administratively and clinically, and has an integrated information system covering all of the services offered Pays providers, for the most part, on a capitated basis Has hospital beds and one or more long-term care services, such as a skilled nursing facility or a home health agency Pools funds coming in from several sources Shares a mission, philosophy, and vision Has centralized and joint planning and management Provides an organized continuum of care, through health care teams
Goldsteen74024_09_CH09_297-318_03-18-20.indd 309
3/19/20 3:04 PM
310
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
In short, the ideal IDS would provide the type of coordinated, continuous, comprehensive, available, acceptable, and accessible care that was envisioned in the landmark Dawson Report—which was issued in the United Kingdom in 1920 (Sidel & Sidel, 1983) and described in the final report of the U.S. Committee on the Costs of Medical Care in 1932. The question in the United States remains: Can this sort of care be provided in a system that has a primary focus on either physician or corporate incomes/profit accumulation?
Increase in For-Profit Health Care Organizations In the first half of the 20th century, private-sector health care organizations were predominantly nonprofit. At mid-century, Blue Cross Blue Shield was the largest private health insurer, and all of its affiliates were obligated to adhere to a voluntary, nonprofit status. Most, if not all, private hospitals were also voluntary, nonprofit organizations. That has since changed. It is difficult to pinpoint the beginnings of profit-making in the health care system. However, we can say that in the early 1990s, profit-making had a clear foothold. An indication is Blue Cross Blue Shield Association’s decision in 1994 to permit its affiliates to switch to for-profit status, which many did. By 2007, 15 of the 64 Blue Cross Blue Shield affiliates were profit-making. Much of the controversy surrounding health care delivery reorganizations, such as introduction of managed care, and the creation of large, integrated health systems concerns profit-making and its compatibility with the provision of quality, efficient, and accessible health care. For example, a prediction of the effects of managed care as it has evolved made by health policy analyst Fuchs (2002) was rather grim: The announcement that most of the nation’s biggest insurers—Aetna, CIGNA, Humana, the United Health Group, and WellPoint Health Network—will be introducing a new kind of health plan during the next year or two signals the beginning of a new era in health insurance in the United States. These plans feature a complicated menu of premiums, co-payments, and deductibles that will add impetus to the trend of employers offering a defined [monetary] contribution for health benefits …. One of their major effects will be to shift the burden of health care costs from employees who use little care to those who use more. Thus, the new plans will be another nail in the coffin of health insurance as a form of social insurance. (p. 1822) As Randel, Pearson, Sabin, Hyams, and Emanuel (2001) put it, in terms that still apply: The growth of managed care in the United States has been paralleled by a rising tide of anti–managed care sentiment. The “managed care problem” is understood generally as the need to protect individuals against large companies that care more about their bottom line than about people. (p. 44) And as Koop (1996; certainly no radical reformer) maintained, it is the question of for-profit versus not-for-profit health care, not just managed care. It is the question of whether having the health care delivery system become a major profit center for corporate America (the insurance industry) is healthy (in a variety of senses) for America and Americans. It is the issue at the center of virtually every other health care issue related not only to managed care but to the future of the health care delivery system as a whole. The question is not a moral one. It is a functional one. Can a profit-making system and the free market solve the myriad problems of the U.S. health care delivery system? Because
Goldsteen74024_09_CH09_297-318_03-18-20.indd 310
3/19/20 3:04 PM
9
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : I n c re m e n t a l i s m
311
the focus of a for-profit system must be on profits, by definition, and because the solution of so many of the problems not only cannot generate profits but also would cost considerable sums of money, the answer would appear to be no.
SUMMARY During the 20th century, the health care delivery system changed dramatically, but incrementally, through efforts of both the public and the private sectors—in the American tradition. Some changes were intended to improve access to health care. Others changed organizational structure and financing mechanisms to contain health care costs and improve efficiency. In the early years of the century, changes focused on providing access to health care. The private sector tended to develop voluntary, nonprofit health care initiatives. Health insurance was provided to nonmilitary persons by private-sector insurance companies, which at first covered the employed and their families. Until mid-century, the largest of these insurance companies was Blue Cross Blue Shield, which created voluntary, nonprofit companies nationwide. Public-sector efforts at this time were primarily for the military, military families, and veterans. Hospitals were built by the private sector as voluntary, nonprofit institutions, often by religious groups, and by government, particularly for the military. Throughout the latter part of the 20th century and into the 21st, complex organizational arrangements developed including HMOs and managed care organizations. Both of these were premised largely on paying for health services through capitation, rather than indemnity insurance. This practice transferred the risk to health care providers from health care payers (insurers). Also, for-profit initiatives developed in both health insurance and health care delivery organizations. Blue Cross Blue Shield affiliates were permitted to become for-profit entities in 1994. Beginning in 1965, federal programs provided health insurance to low-income (Medicaid) and retired persons (Medicare), and later still to uninsured children (CHIP), leaving the private sector to continue serving the employed population and a small number of individuals.
DATA SOURCES Following are authoritative sources of information concerning policy and legislation related to the U.S. health care system. They include government websites and past reports from a variety of organizations that have influenced policy and legislation.
Government Sources •
U.S. Congress. Congress hosts a website that contains legislation from the Senate and House of Representatives and all related actions beginning with introduction of each bill. For health care legislation, the site begins with the 1973–1974 congressional session. For each bill, the site includes a summary, the title and text, actions taken, amendments, sponsors and cosponsors, committees that reviewed the legislation, and any related bills. This site also contains links to each state’s legislature websites for information on state legislation including bill tracking. Start here to explore information about health care legislation, policy reports, and executive actions: www.congress.gov
Goldsteen74024_09_CH09_297-318_03-18-20.indd 311
3/19/20 3:04 PM
312
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
•
Federal Register. The Federal Register is the official source for federal agency regulations, proposed rules and notices of interest to the public, as well as executive orders and other presidential documents. It is published daily by the Office of the Federal Register, National Archives and Records Administration (NARA). It was first published in 1936. The information in the Federal Register became available electronically in 2014, although print copies can be obtained for a fee. Start here to explore information in the Federal Register: www.federalregister.gov
•
White House. The White House hosts a site that contains information about the president’s briefings, statements, and actions, including executive orders. Start here to explore information on this site: www.whitehouse.gov
Influential Reports on the U.S. Health Care System, 1927 to 2005 In a review of the Ehrenreich and Ehrenreich (1971) book, The American Health Empire: Power, Profits, and Politics, which appeared in the International Journal of Health Services (1972), Dr. Milton Roemer listed a series of other reports going back many more years. He wrote: Every few years, more recently in the last decade, there appears a book analyzing the serious defects of health care in America. In 1927, Harry H. Moore produced American Medicine and the People’s Health, in the 1930s were the magnificent 27 volumes of the Committee on the Costs of Medical Care, in 1939 there was James Rorty’s American Medicine Mobilizes, and in 1940 Hugh Cabot’s The Patient Dilemma. After World War II, Carl Malmberg wrote 140 Million Patients in 1947, Michael Davis wrote Medical Care for Tomorrow in 1955, and Richard Carter wrote The Doctor Business in 1958. In 1965, there was Selig Greenberg’s excellent The Troubled Calling: Crisis in the Medical Establishment. The year after Medicare, 1966, saw two critical outputs: The American Health Scandal by Raul Tunley and The Doctors by Martin L. Gross. In 1967, there was Fred J. Cook’s Plot Against the Patient and in 1970 Ed Cray’s In Failing Health. (p. 119) It is fascinating that, allowing for changes in magnitude, many of these analyses and the recommendations they make are similar in so many ways. It is also fascinating that three quarters of a century after Dr. Moore’s book appeared, such books, referred to and cited in the text (e.g., the IOM’s Crossing the Quality Chasm, Himmelstein and Woolhandler’s Bleeding the Patient, and Kleinke’s Oxymorons), are still being written. This is the case because not only do many of the problems of cost, distribution, coverage, and quality that past works highlight remain with us, but because of the changes in their magnitude over time—they are only getting worse. Additional reports from 1960 through 2005 include the following: Aday, L. A. (2001). At risk in America: The health and health care needs of vulnerable populations in the United States. San Francisco, CA: Jossey-Bass. Citizens’ Board of Inquiry into Health Services for Americans. (1971). Heal yourself [Report]. Washington, DC: Author. The crisis in American medicine. (1960, October). Harper’s Magazine, p. 123. Ehrenreich, B., & Ehrenreich, J. (1971). The American health empire: Power, profits, and politics. New York, NY: Vintage Books. Health Task Force of the Urban Coalition. (1969). Rx for action [Report]. Washington, DC: Author.
Goldsteen74024_09_CH09_297-318_03-18-20.indd 312
3/19/20 3:04 PM
9
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : I n c re m e n t a l i s m
313
Himmelstein, D., & Woolhandler, S. (2001). Bleeding the patient: The consequences of corporate health care. Monroe, ME: Common Courage Press. Institute of Medicine. (2000). To err is human: Building a safer health system. Washington, DC: National Academies Press. Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academies Press. Institute of Medicine. (2003). Unequal treatment: Confronting racial and ethnic disparities in health care. Washington, DC: National Academies Press. Institute of Medicine. (2004). Patient safety. Achieving a new standard for care. Washington, DC: National Academies Press. Jonas, S. (1978). Medical mystery: The training of doctors in the United States. New York, NY: W. W. Norton. Kennedy, E. M. (1972). In critical condition: The crisis in America’s health care. New York, NY: Simon & Schuster. Kleinke, J. D. (2001). Oxymorons: The myth of a U.S. health care system. San Francisco, CA: Jossey-Bass. Knowles, J. H. (Ed.). (1977). Doing better and feeling worse. New York, NY: W. W. Norton. Moskin, J. R. (1964, November 3). The challenge to our doctors. Look, p. 26. National Commission on Community Health Services. (1966). Health is a community affair. Cambridge, MA: Harvard University Press. Ribicoff, A., & Danaceau, P. (1972). The American medical machine. New York, NY: Saturday Review Press. Schorr, D. (1970). Don’t get sick in America. Nashville, TN: Aurora Publishers. Silver, G. A. (1976). A spy in the house of medicine. Germantown, MD: Aspen Press. Somers, A. R., & Somers, H. M. (1977). Health and health care. Germantown, MD: Aspen Press.
STUDY QUESTIONS 1. What foundations of the modern health care system evolved from the Civil War? 2. What is employer-based health insurance, and how does it differ from health insurance in other countries? 3. How is capitation different from indemnity health insurance? 4. What are the characteristics of HMOs and managed care organizations, and how are they similar? 5. What is an example of a for-profit health care organization? 6. What is a horizontally integrated health care organization? 7. How did the incremental changes to the U.S. health care system conform to the American preference for public/private policy solutions?
Goldsteen74024_09_CH09_297-318_03-18-20.indd 313
3/19/20 3:04 PM
314
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
REFERENCES Alexander, G. C., & Lantos, J. D. (2006). The doctor–patient relationship in the post–managed care era. American Journal of Bioethics, 6(1), 29–33. doi:10.1080/15265160500394556 America’s Essential Hospitals. (2005). History of public hospitals in the United States. Retrieved from https://essentialhospitals.org/about-americas-essential-hospitals/ history-of-public-hospitals-in-the-united-states/ American Hospital Association. (2011). AHA guide 2010. Chicago, IL: Health Forum. American Medical Association. (2019). AMA history. Retrieved from https://www.ama-assn .org/about/ama-history/ama-history Austrin, M. S. (1999). Managed health care simplified: A glossary of terms. Albany, NY: Delmar. Barton, P. L. (1999). The health services delivery system: Managed care. In J. A. Russell (Ed.), Managed care essentials: A book of readings. Chicago, IL: Health Administration Press. Blumberg, A., & Davidson, A. (2009). Accidents of history created U.S. health system. Retrieved from http://www.npr.org/templates/story/story.php?storyId=114045132 Center for Medical Humanities, Compassionate Care, and Bioethics. (2012). History of medicine. Retrieved from https://www.stonybrook.edu/commcms/bioethics/events/history .php#RegionalResource Cunningham, R. III, & Cunningham, R. M. (1997). The blues: A history of Blue Cross and Blue Shield. DeKalb, IL: Northern Illinois Press. Ehrenreich, B., & Ehrenreich, J. (1971). The American health empire: Power, profits, and politics. New York, NY: Vintage Books. Friedman, E. (1995). The Compromise and the Afterthought: Medicare and Medicaid After 30 Years. JAMA. 274(3):278–282. doi:10.1001/jama.1995.03530030098045. Retrieved from https://jamanetwork.com/journals/jama/article-abstract/389250 Fuchs, V. R. (2002). Sounding board: What’s ahead for health insurance in the United States? New England Journal of Medicine, 346(23), 1822–1824. doi:10.1056/NEJM200206063462314 Goldfield, N. I. (2000). National health reform American style: Lessons from the past. Tampa, FL: American College of Physician Executives. Harris, R. (1966a, July 9). Annals of legislation: Medicare III—We do not compromise. The New Yorker, pp. 40–62. Harris, R. (1966b, July 16). Annals of legislation: Medicare IV—A sacred trust. The New Yorker, pp. 35–56. Kondratas, R. (2012). Images from the history of the public health service: Two centuries of health promotion. Bethesda, MD: U.S. National Library of Medicine. Retrieved from https://www.nlm.nih.gov/exhibition/phs_history/intro.html Kongstvedt, P. R., Plocher, D. W., & Stanford, J. C. (2001). Integrated health care delivery systems. In P. R. Kongstvedt (Ed.), The managed health care handbook (pp. 42–72). Gaithersburg, MD: Aspen. Koop, C. E. (1996, Fall). Manage with care [Special issue]. Time, p. 69. Lichtenstein, M. (2014). Health insurance from invention to innovation: A history of the blue cross and blue shield companies. Blue Cross and Blue Shield Association. Retrieved from https://web.archive.org/web/20140523225053/
Goldsteen74024_09_CH09_297-318_03-18-20.indd 314
3/19/20 3:04 PM
9
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : I n c re m e n t a l i s m
315
Light, D. W. (2006). Be clear about managed care to get clear about doctor–patient relations. American Journal of Bioethics, 6(1), 38–41. doi:10.1080/15265160500394747 Lipscomb, C. E. (2002). Lister Hill and his influence. Journal of the Medical Library Association, 90(1), 109–110. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC64768/ Luft, H. S. (2003). Measuring quality in modern managed care. Health Services Research, 38(6, Pt. 1), 1373–1378. doi:10.1111/j.1475-6773.2003.00183.x MacColl, W. A. (1966). Group practice and the prepayment of medical care. Washington, DC: Public Affairs Press. Marquis, M. S., Rogowski, J., & Escarce, J. J. (2005). The managed care backlash: Did consumers vote with their feet? Santa Monica, CA: RAND Corporation. Retrieved from http://www .rand.org/pubs/research_briefs/RB9121.html Mayer, T. R., & Mayer, G. G. (1985). HMOs: Origins and development. New England Journal of Medicine, 312(9), 590–594. doi:10.1056/NEJM198502283120926 MedlinePlus. (2018). Managed care: summary. Retrieved from https://medlineplus.gov/managedcare.html National Center for Health Statistics. (2007). Health, United States, 2007: With chartbook on trends in the health of Americans. Hyattsville, MD: U.S. Department of Health and Human Services. National Museum of Civil War Medicine. (2016). Dr. Jonathan Letterman: Father of modern emergency medicine. Retrieved from http://www.civilwarmed.org/letterman-award/ letterman-father-of-battlefield-medicine/ Ortiz-Ospina, E., & Roser, M. (2019). Our world in data: Financing healthcare. Retrieved from https://ourworldindata.org/financing-healthcare Prybil, L. D. (1982). Growth and impact of multiunit hospital systems. American Journal of Hospital Pharmacy, 39(11), 1888–1891. doi:10.1093/ajhp/39.11.1888 Randel, L., Pearson, S. D., Sabin, J. E., Hyams, T., & Emanuel, E. J. (2001). How managed care can be ethical. Health Affairs, 20(4), 435–436. doi:10.1377/hlthaff.20.4.43 Roemer, M. I., & Shonick, W. (1973). HMO performance: The recent evidence. Milbank Memorial Fund Quarterly, Health and Society, 51(3), 271–317. doi:10.2307/3349556 Shortell, S. M., Gillies, R. M., & Anderson, D. A. (1994). The new world of managed care: Creating organized delivery systems. Health Affairs, 13(5), 46–64. doi:10.1377/hlthaff.13.5.46 Shortell, S. M., Gillies, R. M., Anderson, D. A., Erickson, K. M., & Mitchell, J. B. (1999). Working toward an ideal system. In J. A. Russell (Ed.), Managed care essentials: A book of readings. Chicago, IL: Health Administration Press. Sidel, V. W., & Sidel, R. (1983). A healthy state (Rev. ed.). New York, NY: Pantheon Books. Silver, G. A. (1963). Group practice: What it is. Medical Care, 1, 94. doi:10.1097/00005650 -196304000-00010 Smits, H. L. (2002). Managed care. In A. R. Kovner & S. Jonas (Eds.), Health care delivery in the United States (7th ed., pp. 289–314). New York, NY: Springer Publishing Company. Stevens, R. (1971). American medicine and the public interest. New Haven, CT: Yale University Press. Stevens, R. (1982). A poor sort of memory: Voluntary hospitals and government before the depression. Milbank Memorial Fund, 60(4), 551–584. doi:10.2307/3349691
Goldsteen74024_09_CH09_297-318_03-18-20.indd 315
3/19/20 3:04 PM
316
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
U.S. Department of Health and Human Services. (2013). HIPAA: Combined regulation text of all rules. Retrieved from http://www.hhs.gov/hipaa/for-professionals/privacy/laws-reg ulations/combined-regulation-text/index.html U.S. Department of Veterans Affairs. (2015). About VA—VA history. Retrieved from http:// www.va.gov/about_va/vahistory.asp U.S. Senate, Committee on Finance. (1979). Comparison of major features of health insurance proposals. Washington, DC: U.S. Government Printing Office. World Health Organization. (2016). International classification of diseases. Retrieved from http://www.who.int/classifications/icd/en/HistoryOfICD.pdf Zibulewsky, J. (2001). The emergency medical treatment and active labor act: What it is and what it means for physicians. Baylor University Medical Center Proceedings, 14(4), 339– 346. doi:10.1080/08998280.2001.11927785
FURTHER READING American Medical Association. (1996). Medical groups in the U.S.: A survey of practice characteristics. Chicago, IL: Author. Bureau of Labor Statistics, U.S. Department of Labor. (2018). May 2018 national occupational employment and wage estimates. Retrieved from https://www.bls.gov/oes/current/ oes_nat.htm#29-0000 Commonwealth Fund. (2006, March). Newsletter. Retrieved from http://www.common wealthfund.org/publications/newsletters/states-in-action/2006/mar/march-2006 Dudley, R. A., & Luft, H. S. (2001). Health policy, 2001: Managed care in transition. New England Journal of Medicine, 344(14), 1087–1092. doi:10.1056/NEJM200104053441410 Field, R. I. (2008). Why is health care regulation so complex? Pharmacy and Therapeutics, 33(10), 607–608. Fox, P. D. (1990). Foreword: Overview of managed care trends. In National Health Lawyers Association (Ed.), The insider’s guide to managed care (pp. 1–12). Washington, DC: National Health Lawyers Association. Fox, P. D. (2001). An overview of managed care. In P. R. Kongstvedt (Ed.), The managed health care handbook (pp. 3–16). Gaithersburg, MD: Aspen. Freudenheim, M. (1994, June 30). Blue Cross lets plans sell stock. The New York Times. Retrieved from https://www.nytimes.com/1994/06/30/business/blue-cross-lets-plans-sell -stock.html Geiger, H. J. (1997). Doctoring: The nature of primary care medicine [Book review]. New England Journal of Medicine, 337(22), 1637. doi:10.1056/NEJM199711273372221 Goldman, D. P., & McGlynn, E. A. (2005). U.S. health care: Facts about cost, access, and quality. Santa Monica, CA: RAND Corp. HealthInsurance.org. (2019). What is community rating? Retrieved from https://www.health insurance.org/glossary/community-rating/ Hunt, W. C. (1904). 1900 Census special reports: Occupations at the twelfth census. Washington, DC: Department of Commerce and Labor, Bureau of the Census. Retrieved from https:// www.census.gov/library/publications/1904/dec/occupations.html
Goldsteen74024_09_CH09_297-318_03-18-20.indd 316
3/19/20 3:04 PM
9
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : I n c re m e n t a l i s m
317
Igel, L. (2008, May–June). The history of health care as a campaign issue. Politics and the Physician Executive, pp. 12–15. Internal Revenue Service. (2012). Pharmaceutical industry overview: Trends. Retrieved from www.irs.gov/businesses/article/0,id=169580,00.html Kaiser Family Foundation. (2006). Employer health benefits, 2006 annual survey. Menlo Park, CA: Author. Kaiser Family Foundation/Harvard School of Public Health. (2001). National survey on consumer experience with and attitudes toward health plans. Kleinke, J. D. (2001). Oxymorons: The myth of a U.S. health care system. San Francisco, CA: Jossey-Bass. Koplan, J. P., & Harris, J. R. (2000). Not-so-strange bedfellows: Public health and managed care. American Journal of Public Health, 90(12), 1824–1826. doi:10.2105/AJPH.90.12.1824 Levi, J. (2000). Managed care and public health. American Journal of Public Health, 90(12), 1823–1824. doi:10.2105/AJPH.90.12.1823 Luft, H. S. (1980). Assessing the evidence on HMO performance. Milbank Memorial Fund Quarterly, Health and Society, 58(4), 5015–5036. doi:10.2307/3349805 National Center for Health Statistics. (2011). Health, United States, 2010: With special feature on death and dying. Hyattsville, MD: U.S. Department of Health and Human Services. Shouldice, R. G. (1991). Introduction to managed care. Arlington, VA: Information Resources Press. Stevenson, D., Grabowski, D., & Bramson, J. (2009). Nursing home ownership trends and their impact on quality of care. Washington, DC: U.S. Department of Health and Human Services. Tufts Health Care Institute. (2006). Managed care glossary. U.S. Government Accountability Office. (2010). Nursing homes: Complexity of private investment purchases demonstrates need for CMS to improve the usability and completeness of ownership data. Retrieved from www.gao.gov/assets/320/310573.pdf Weinerman, E. R. (1968). Problems and perspectives of group practice. Bulletin of the New York Academy of Medicine (2nd Series), 44, 1423.
Goldsteen74024_09_CH09_297-318_03-18-20.indd 317
3/19/20 3:04 PM
Goldsteen74024_09_CH09_297-318_03-18-20.indd 318
3/19/20 3:04 PM
10 History of Change From 1900 to 2010: Comprehensive Reform
© Randy Glasbergen.
LEARNING OBJECTIVES After completing this chapter, students will be able to: • Describe National Health Insurance (NHI) and differentiate it from the current U.S. health care system. • Identify the attempts to legislate comprehensive health care reform during the 20th century. • Describe the elements of the Clinton health plan to bring about comprehensive reform of the U.S. health care system. • Describe some of the arguments against the Clinton health plan.
INTRODUCTION As mentioned in Chapter 8, Debates That Have Structured Health Care System Change, the problems with the U.S. health care system, particularly cost and access, are long-standing
Goldsteen74024_10_CH10_319-340_03-18-20.indd 319
3/19/20 3:04 PM
320
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
and have not gone unnoticed. As far back as 1932, the findings of the first comprehensive study of health care in the United States were summarized in these terms: The problem of providing satisfactory medical service to all the people of the United States at costs which they can meet is a pressing one. At the present time, many persons do not receive service which is adequate either in quantity or quality, and the costs of service are inequably distributed. The result is a tremendous amount of preventable physical pain and mental anguish, needless deaths, economic inefficiency, and social waste. Furthermore, these conditions are … largely unnecessary. The United States has the economic resources, the organizing ability, and the technical experience to solve this problem. (Committee on the Costs of Medical Care, 1932/1970, p. 2) The committee, chaired by Ray Lyman Wilbur, a past president of the American Medical Association (AMA), had been created in 1927 to look into the problems of the health care system. Strikingly, some would say tragically, the foregoing statement is entirely applicable today. In Chapter 9, History of Change From 1900 to 2010: Incrementalism, we described the incremental changes made from 1900 to 2010 to address the problems identified with the U.S. health care system in the report of Ray Wilbur. In this chapter, we describe the attempts during the same period to address these problems in a comprehensive way. Most attempts until the 1990s were related to achieving National Health Insurance (NHI),1 which usually describes a single, countrywide health care financing system run by the government at one or more jurisdictional levels. With varying prominence over time, proposals to create an NHI system have been on the national political agenda of the United States since Theodore Roosevelt made it one of the planks of his Bull Moose Party platform in the presidential election of 1912. Other proposals have been considered to reform the system comprehensively. Nevertheless, the central problems of the U.S. health care delivery system that any comprehensive program would address—from its high cost, to the maldistribution of personnel and facilities, to the lack of financial access for many people, to its lack of attention to health promotion and disease prevention, to its heavy emphasis on the use of expensive pharmaceuticals and medical/surgical procedures—remained unaddressed through the George W. Bush administration. The fragmented, privately operated health care delivery system was unable to address most of the major problems on the list because dealing successfully with most of them required a comprehensive, coordinated, planned, national approach. In this chapter, we will discuss all of the major initiatives to develop a comprehensive health plan in the United States through 2010, when comprehensive reform came about under the Obama administration.
NATIONAL HEALTH INSURANCE One of the major emphases of health care reformers seeking a comprehensive solution to the problems of the U.S. health care system has been to secure universal health coverage. In this section, we detail the history of this effort, beginning with a description of the world historical context in which the U.S. efforts have existed.
NHI: World Historical Background The first NHI program appeared on the world stage in the 1880s. (Some readers may be distressed to learn that both the content and form of the arguments for and against NHI have
Goldsteen74024_10_CH10_319-340_03-18-20.indd 320
3/19/20 3:04 PM
10
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : C o m p re h e n s i v e R e f o r m
321
remained largely fixed since that time [Boas, 1958; Falk, 1973; McKittrick, 1940/1958; Schwartz, 1972]. This has been the case regardless of changed circumstances or new information.) It was introduced by Otto von Bismarck, the “Iron Chancellor” of Prussia and, after 1871, of the unified German state. Shortly after the bourgeois revolution of 1848 in Europe, he had said: “The social insecurity of the worker is the real cause of their being a peril to the state”(Roemer, 1960, p. 127). In 1881, the German Kaiser, Wilhelm I, in a speech written by Bismarck, said, “The healing of social evils cannot be sought in the repression of social democratic excesses exclusively but must equally be sought in the positive promotion of the workers’ welfare” (Roemer, 1960, p. 129). In other words,“The workers are revolting; let’s do something for them.” From the 1830s onward, various fragmented accident, workers’ compensation, and sickness insurance schemes, both compulsory and voluntary, had come into existence in the several German states. Building on them, in 1883, Bismarck succeeded in ushering through the German Reichstag (Parliament) a Sickness Insurance Act (Roemer, 1960). Bismarck had wanted a uniform, national system, excluding those of the existing “sickness societies” that were for profit, retaining only the not-for-profit ones. Understandably, the former objected to the prospect of being put out of business. (In this regard, they had much in common with the present U.S. health insurance companies. Understandably as well, the insurers protest strongly against any proposed U.S. NHI plan that has no, or a limited, role for them.) Bismarck settled for a plan that used the then-existing network of sickness societies, both for- and not-for-profit. Nevertheless, it was a national program that certain categories of workers paid for medical care and provided cash support during periods of sickness and accidental injury. Two thirds of the premiums were paid by the employees and one third by the employers. Thus, it came to pass that the world’s first NHI scheme was created, not by a progressive democratic or socialist government, but by a conservative constitutional monarchy. By the 1920s, most of the European industrialized countries, as well as Japan, had some kind of NHI system. In each it usually began as a partial or voluntary system, generally progressing to a comprehensive and compulsory one (Douglas-Wilson & McLachlan, 1973; Fry & Farndale, 1972; Glaser, 1978; Roemer, 1985). After World War II, the industrialized countries of the British Commonwealth gradually followed suit (Fry & Farndale, 1972; Lynch & Raphael, 1963; Roemer, 1985, 1991). As the new millennium began, the United States remained the only major industrialized country in the world not to have some sort of NHI system, but it was not for a lack of trying.
NHI in the United States Early 20th-Century NHI Proposals2 The first campaign for an NHI program in the United States was undertaken by the American Association for Labor Legislation (AALL), a middle-class, liberal, reform-minded group founded in 1906 (Anderson, 1968; Burrow, 1963, 1977; Goldfield, 2000). As noted, proposals for a broad social insurance plan were part of Teddy Roosevelt’s third-party Bull Moose platform in 1912 (Burrow, 1963). In 1916, proposing that the several states each adopt the program independently, the AALL put forward a standard bill for compulsory medical care and sickness benefits insurance. Its program would have covered persons earning below a certain income and would have used existing insurance carriers. Employers, employees, and the states would have shared the costs (Anderson, 1968; Burrow, 1963). At first, support was widespread, extending to the AMA and even the National Association of Manufacturers (Burrow, 1963). Beginning in 1917, however, when the U.S. entry into World War I generally deflated the reform movement of the time, opposition began to surface from several quarters. Among the opponents were the American Federation of Labor and the commercial insurance industry (Anderson, 1968; Burrow, 1977).
Goldsteen74024_10_CH10_319-340_03-18-20.indd 321
3/19/20 3:04 PM
322
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
A battle ensued over the issue within the AMA (Anderson, 1968; Burrow, 1963). As part of an overall shift of power from the academic wing of the medical profession to the practitioner wing that was going on at the time, the latter, conservative, faction won out (Harris, 1966a, 1966b).3 In 1920, the AMA House of Delegates passed the following resolution: Resolved, that the American Medical Association declares its opposition to the institution of any plan embodying the system of compulsory contributory insurance against illness, or any other plan of compulsory insurance which provides for medical service to be rendered contributors or their dependents, provided, controlled, or regulated by any state or the Federal government. (Burrow, 1963, p. 150) In toto, that remained the AMA’s position until the late 1960s (Harris, 1966a, 1966b). Even in the mid-1970s, by which time the AMA had adopted an NHI proposal of its own that ran counter to the bulk of the 1920 resolution, the noncompulsory principle was retained (Committee on Ways and Means, U.S. House of Representatives, 1974). It was not until 1990 that the AMA had dropped the noncompulsory principle as well (AMA, 1990).
The New Deal and Postwar NHI Proposals Serious consideration was next given to NHI during the development of the Social Security Act of 1935. This consideration was stimulated in part by the final report of the Committee on the Costs of Medical Care (CCMC, 1932; see also Anderson, 1968; Stevens, 1971). In 1934, President Franklin Roosevelt created the Committee on Economic Security to consider the whole question of social insurance. NHI was on the agenda; it did not stay there long (Goldfield, 2000). The principal opposition again came from the AMA (Burrow, 1963). Economic Security Committee Executive Director E. E. Witte wrote: When in 1934 the Committee on Economic Security announced that it was studying health insurance, it was at once subjected to misrepresentation and vilification. In the original social security bill there was one line to the effect that the Social Security Board should study the problem and make a report thereon to Congress. That little line was responsible for so many telegrams to the members of Congress that the entire social security program seemed endangered until the Ways and Means Committee unanimously struck it out of the bill. (Anderson, 1968, p. 108) President Roosevelt wanted to ensure that the basic Social Security Act, conceived as one of the cornerstones of the New Deal, became law. It was eventually passed by Congress with no reference to NHI. Sen. Robert Wagner, D-N.Y., initiated the next major legislative foray on behalf of NHI in the United States.4 The landmark National Labor Relations Act of 1935 (referred to as the “Wagner Act”) established the right to collective bargaining for all nonpublic employees in the United States. Then in 1939, Wagner introduced a bill to provide for the general welfare by enabling the several states to make more adequate provision for public health, prevention and control of disease, maternal and child health services, construction, and maintenance of needed hospitals and health centers, care of the sick, disability insurance, and training of personnel (Roemer, 1960). The bill, S-1620, proposed to subsidize state public health programs (this later became federal policy through a series of separate acts), the construction of hospitals (enacted in 1946 as the Hill–Burton Act), and state programs for medical care for the poor (eventually enacted in part in 1960 as Kerr–Mills Medical Assistance for the Aged, then expanded as
Goldsteen74024_10_CH10_319-340_03-18-20.indd 322
3/19/20 3:04 PM
10
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : C o m p re h e n s i v e R e f o r m
323
the federal/state Medicaid program in 1965). S-1620 also proposed to provide cash sickness benefits (a standard feature of the European/Japanese approach to NHI that has never made headway in the United States). Additionally, there was to be a program of federal subsidies to those states enacting comprehensive health insurance programs. The bill died in committee, after being vigorously attacked by the AMA (Harris, 1966a, 1966b; Roemer, 1960). Wagner tried again in 1943, this time in concert with Sen. James Murray, D-Mont., and Rep. John Dingell, D-Mich. Their bill, S. 1161, advocated for a federal health insurance system that would provide comprehensive health care benefits and would be financed by payroll taxes (Stevens, 1971). This was the first major legislative proposal for a federal rather than a state-based system. Once again, the AMA responded negatively, with vigor (Harris, 1966a). The bill never got very far, although it was reintroduced in several successive Congresses (Anderson, 1968). In 1947, Sen. Robert Taft, R-Ohio, introduced a proposal for federal subsidies to the states to pay for medical care for the poor. The proposal was similar to Wagner’s 1939 package and would eventually see the light of day as the Medicaid program (Stevens, 1971). Though sponsored by a conservative Republican, it also got nowhere in 1947. In 1949, Harry Truman was reelected president with Democratic majorities in both houses of Congress (Goldfield, 2000). He decided to make enactment of NHI a major goal of his administration. He proposed a national, compulsory system, to be paid for by a combination of Social Security and general taxation, similar in many ways to the Wagner–Murray–Dingell bill of 1943. It was in 1945, just after he succeeded to the presidency following Roosevelt’s death in April of that year and the end of World War II, that Truman had first enunciated the principles on which the proposed system would be based: Everyone should have ready access to all necessary medical, hospital, and related services …. A system of required prepayment would not only spread the costs of medical care, it would also prevent much serious disease. … Such a system of prepayment should cover medical, hospital, nursing, and laboratory services. It should cover dental care [as far as] resources of the system permit. … [T]he nation-wide system must be highly decentralized in administration. … Subject to national standards, methods and rates of paying doctors and hospitals should be adjusted locally. … People should remain free to choose their own physicians and hospitals. … Likewise physicians should remain free to accept or reject patients. … Our voluntary hospitals and our city, county, and state general hospitals, in the same way, must be free to participate in the system to whatever extent they wish. … [W]hat I am recommending is not socialized medicine. Socialized medicine means that all doctors work as employees of government. … No such system is proposed. (Truman, 1958, pp. 629–630) The AMA mounted a furious attack on the plan, based primarily on the claim that it was indeed “socialized medicine” (Harris, 1966a). The AMA used a major public relations firm and a war chest of over US$2 million, a very substantial sum in those days. With allies from the drug and insurance industries (Stevens, 1971), it was once again successful in defeating an NHI plan in Congress. With the election of a Republican government in 1952, the AMA was able to breathe easily (Burrow, 1963). In the post–World War II climate of domestic and foreign anticommunism (Freeland, 1975), it was difficult for Truman to win support at home for a program consistently attacked as“communist”or“socialist,”but in any case“Red.”Thus, in 1951, on the recommendation of Oscar Ewing, the federal Social Security administrator, the Truman administration withdrew its support for NHI and began the campaign that eventually led to the passage of Medicare in 1965 (Goldfield, 2000; Harris, 1966a, 1966b; Stevens, 1971).
Goldsteen74024_10_CH10_319-340_03-18-20.indd 323
3/19/20 3:04 PM
324
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
NHI Proposals in the 1960s and 1970s Once Congress had passed Medicare and Medicaid, beginning in the late 1960s many new legislative proposals for NHI were made (Burns, 1971; Eilers, 1971a, 1971b; Falk, 1973, 1977; Goldfield, 2000; Hastings, 1972). In the 1970s, they were summarized by the House Ways and Means Committee (Committee on Ways and Means, U.S. House of Representatives, 1974), the Committee for Economic Development (1973), and the Senate Finance Committee (Committee on Finance, 1970, 1979; see also Davis, 1975). In the wide-ranging debate on NHI, the basic arguments of the several sides had changed little over time. As of 1975, a time when the passage of some sort of NHI seemed imminent to many observers, there were four major proposals before Congress. The constituencies represented were organized labor, the American Hospital Association (AHA, McMahon, 1975), the Health Insurance Association of America, and, notably, the AMA itself. Because all of the major actors were on stage, it was believed that surely one of these proposals or some compromise among them would find its way through Congress (Editors of Fortune, 1970; Friedman, 1977a, 1977b, 1977c, 1977d; Friedman & Wendorf, 1977). One predicts the passage of NHI in the United States at one’s peril, however. For example, in 1974, an observer wrote: The United States of America is the only major country in the developed, capitalist world without some form of national health insurance programme. The struggle for national health insurance in the U.S., a long and bitter one, has been well described. It now appears as if there will be some form of national health insurance legislation in the U.S. before the Presidential elections of 1976. (Jonas, 1974, p. 143) There wasn’t. In the 1976 presidential campaign, Democratic candidate Jimmy Carter said, in his only speech on health policy: We must have a comprehensive program of national health insurance. ... The coverage must be universal and mandatory. We must lower the present barriers, in insurance coverage and otherwise, to preventive and primary care and thus reduce the need for hospitalization. We must have strong cost and quality controls, and … rates … should be set in advance. … We must phase in the program as rapidly as revenues permit, helping first those who need help, and achieving a comprehensive program well defined in the end. (quoted in Cavalier, 1979, p. 7) The Carter administration never submitted such a proposal to Congress.
NHI Proposals in the 1980s In 1979, the Congressional Research Service of the Library of Congress (Cavalier, 1979) stated that the major policy issues to be addressed in designing an NHI program were as follows: • • • • •
Rising costs of health care Gaps in present health insurance coverage, in terms of both services and populations Geographic maldistribution of personnel and facilities Access to health care service by ability to pay, social class, age group, and geography Impact, or lack thereof, of NHI on the population’s health status
Goldsteen74024_10_CH10_319-340_03-18-20.indd 324
3/19/20 3:04 PM
10
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : C o m p re h e n s i v e R e f o r m
325
Once again, this list, published more than 30 years ago, has a familiar sound to it. In 1980, the same major NHI-proposal players were still on the field (Committee on Finance, 1979; Jonas, 1981; Shabecoff, 1979). Many policy makers and observers argued the case of the Canadian health service as a model and pointed out the health care cost, quality, and access disparities between the United States and its northern neighbor (Evans et al., 1989; Fuchs & Hahn, 1990; Igelhart, 1986a, 1986b, 1986c, 1990; Starr, 1982; Woolhandler & Himmelstein, 1991). However, with the election of Ronald Reagan in 1980, the whole movement to develop NHI ran out of gas. A measure of the enormous loss of energy suffered by the pro-NHI forces in the 1980s can be found in the contents of bills introduced by Sen. Edward Kennedy, D-Mass. Health care was a major interest of Kennedy and he introduced many bills in the 1980s that proposed changes to the existing health care system, but not comprehensive reform. In 1985, he introduced 10 bills, including the Health Care Improved Access Act of 1985, the Access to Health Care Act of 1986, the Medicare Solvency and Health Care Financing Reform Act of 1985, and the State Comprehensive Mental Health Services Plan Act of 1986. These Kennedy-sponsored bills proposed measures such as: • • • •
Reducing the number of persons uninsured for health care costs by requiring employers to make health insurance available to former employees at group rates Reducing or eliminating “patient dumping” by hospitals Restraining increases in Medicare Part A premium costs Holding down Medicare payments to hospitals
Only one of the 10 bills became law—the State Comprehensive Mental Health Services Plan Act of 1986 (Congress.gov, 1985–1986). This was a far cry from the sweeping changes proposed by Kennedy in several major bills he offered in the 1970s. That weak cry of 1985 had an echo in 1996 with the eventual passage of a bill sponsored by Kennedy and Sen. Nancy Kassebaum, R-Kan. providing that certain elements of portability from job to job become required for employer-provided health insurance (Goldfield, 2000; Hoppszallern & Arges, 2002; Kuttner, 1997). See Chapter 9, History of Change From 1900 to 2010: Incrementalism for more information about this bill—the Health Insurance Portability and Accountability Act (HIPAA).
NHI by Contract, or the Personal Health Care System In the early 1980s, a proposal was published that was designed to deal with the problem list set out by the Congressional Research Service as well as many others (Jonas, 1980). First designated “NHI by contract,” it was later called the personal health care system (PHCS). By 2002, it had yet to be put into legislative language per se, although some of its central concepts appeared as essential elements of President Bill Clinton’s health plan—the comprehensive reform proposal that came next.
COMPREHENSIVE HEALTH CARE REFORM UNDER THE CLINTON ADMINISTRATION The last comprehensive health care reform proposal before the Obama administration (2008–2016) was developed in the 1990s—the Health Security Act by the Clinton administration. The Clinton proposal retained elements of the existing health care system, including a mix of private and public health insurance and other elements designed to appeal to the
Goldsteen74024_10_CH10_319-340_03-18-20.indd 325
3/19/20 3:04 PM
326
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
uniquely American preferences that have constrained health care reform since at least 1900. We will discuss the Health Security Act next.
Political Context of the Health Security Act For a variety of reasons—primarily continually escalating costs, a growing pool of uninsured persons, and declining health for certain portions of the population—in the early 1990s, NHI reappeared with prominence on the national political agenda. Once again, there were a whole series of proposals placed on the table, from such disparate groups as Senator Kennedy’s Committee on Labor and Human Resources (1988), the National Association of Manufacturers (1989), the Heritage Foundation (1989), the National Leadership Commission on Health Care (1989; cochaired by former Presidents Richard Nixon, Gerald Ford, and Jimmy Carter), the Oil, Chemical, and Atomic Workers (1989), the Committee for National Health Insurance (1989; affiliated with the AFL-CIO), the AMA (1990), the U.S. Bipartisan Commission on Comprehensive Health Care of the U.S. Congress (1990; also known as the Pepper Commission), and the Physicians for a National Health Program’s “Single-Payor” System (Grumbach, Bodenheimer, Himmelstein, & Woolhandler, 1991; Himmelstein & Woolhandler, 1989). In 1994, the year that the Clinton administration’s Health Security Act was debated and defeated in Congress (Blumenthal, 1995; Goldfield, 2000; Skocpol, 1995), some form of managed care was already the reality for an increasing number of Americans— providers and patients alike (Freudenheim, 1994). Many of the changes that concerned providers the most, including being forced into some form of organized practice and seeing significant declines in their incomes, were happening whether the Health Security Act or any of the other proposals then on the table were to be enacted. Many managed care–induced changes affecting patients, such as limiting their choices of plans and providers, were also already a reality. Many changes affecting both patients and providers, such as having insurance/managed care company representatives at the other end of an 800 telephone line making treatment choices, were already a reality, too. See Chapter 9, History of Change From 1900 to 2010: Incrementalism for more information on managed care. One real choice facing the country as a whole at the time of the debate of the Health Security Act was whether this process would occur in a haphazard, unplanned way or be accomplished in a rational manner. In the latter case, the aim would be to achieve stated goals related to the health and health care of the people, not arising from the narrow interests of the insurance and managed-care companies, many of them for-profit, and the provider networks. Another real choice was whether a system heavily dependent on public funds for its operations, such as the health care delivery system, should have a strong public voice in determining its policies and practices. A highly political debate on the Health Security Act ensued (Hacker, 1996), which aired these questions.
Introduction of the Health Security Act When President Bill Clinton introduced his ill-fated Health Security Act in 1993, his words eerily sounded like those uttered by President Nixon (1994) when he presented his own NHI plan in 1971. Ironically, the Nixon plan was introduced in the Senate by none other than Robert Dole, R-Kan., who, in 1994, led the fight in Congress to kill the Health Security Act. Clinton had this to say when he offered his bill to the Congress:
Goldsteen74024_10_CH10_319-340_03-18-20.indd 326
3/19/20 3:04 PM
10
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : C o m p re h e n s i v e R e f o r m
327
Americans are blessed with the world’s finest doctors and nurses, the best hospitals, the most advanced medical technology, and the most promising research on the face of the earth. We cherish—and we will never surrender—our right to choose who treats us and how we get our care. But today our health care system is badly broken. Insurance has become a contest of finding only the healthiest people to cover. Millions of Americans are just a pink slip away from losing their health coverage, one serious illness away from losing their savings. Millions more are locked into jobs for fear of losing their benefits. And small-business owners throughout our nation want to provide health care for their employees and families but can’t get it or can’t afford it. Next year we will spend more than one trillion dollars on health care—and still leave 37 million Americans without health insurance, and 25 million more with inadequate coverage. … In short, all the things that are wrong with our health care system threaten everything that’s right. (White House Domestic Policy Council, 1993, p. iii) Sounds familiar? Perhaps there has been only one speech writer for every speech of this type from the time of the final report of the CCMC in 1932 to the present. If there is, surely he or she has a better health care plan than most Americans did throughout the 20th century. Clinton’s proposed Health Security Act had five primary features: guaranteed private insurance for everyone, choice of physician and health plan, elimination of unfair insurance practices, preservation of Medicare, and health benefits guaranteed through the work site (Goldfield, 2000; White House Domestic Policy Council, 1993). The act was based on six basic principles: security, savings, simplicity, choice, quality, and responsibility (White House Domestic Policy Council, 1993). Senator Paul Wellstone, D-Minn., was a supporter of the Health Security Act. In fact, he introduced the bill in the Senate in 1993. He extolled the following features of the legislation: • • • • • •
Administrative simplicity, as it was a single-payer plan Cost control Universal coverage Comprehensive benefits Quality assurance Equitable financing
He wrote that“Every other industrialized nation has been able to use the power of a public authority to provide a secure and dependable environment for the healing arts. In every other industrialized nation people are far more satisfied with the health care system than we are in the United States, and by every measure of public health they are in better condition. … Surely with all our technology, creativity, and good will, Americans can borrow from their experience and do equally well” (Wellstone & Shaffer, 1993, pp. 1492–1493).
The Health Security Act Plan Under the proposed Health Security Act, a new series of agencies, called “health care alliances,” would have been established by the states. Among other things, they would collect all of the money used to support health services from all sources. They would then contract with provider networks and groups in their region to provide a package of health care services for all persons enrolled—much like the approach of the PHCS (Redlener, 1993).
Goldsteen74024_10_CH10_319-340_03-18-20.indd 327
3/19/20 3:04 PM
328
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
The alliances would have oversight for all quality-assurance activities. This system would presumably simplify both money flow and paperwork. It would guarantee a choice of plan and a system of quality assurance for the beneficiaries. For the providers, it would reunify authority and responsibility by putting medical decision-making back in the hands of provider groups, along with fiscal responsibility for the viability of the plan. A comprehensive benefit package was laid out, to be subject to fine-tuning and modification over time by the National Health Board (White House Domestic Policy Council, 1993). Its description took up 92 pages in the text of the Health Security Act bill submitted to Congress. It included virtually all inpatient, outpatient, short- and long-term, institutional and home-based, preventive, diagnostic, treatment, rehabilitative, and follow-up services. The Health Security Act called for each person to be able to choose from among three types of coverage: • •
•
A health maintenance organization (HMO), with no deductible and a copayment of no more than US$10 for each doctor visit A preferred provider organization (PPO), with no deductible and a US$10 copayment if the patient were to use network providers, and deductibles and higher copayments for the use of physicians outside the PPO (which would be permitted) A fee-for-service system, allowing completely free choice of doctor, with significant deductibles and copayments. Under the PPO option, there would be a fee schedule for the physicians, and no balance billing would be allowed (White House Domestic Policy Council, 1993).
For most businesses, large and small, participation would have been mandatory, which was a major bone of contention. Because employers would have no say in plan choice by their employees, change from plan to plan would be only at the individual’s option—unless a plan went out of business. Coverage would be portable from job to job and from job to no job. Finally, the Health Security Act would have linked payment and planning, under public rather than private control, the desideratum so eloquently set forth by Rashi Fein (Institute of Medicine [IOM], 1981). This would have enabled—although not guaranteed—significant health care delivery system reform. This was, perhaps, what the opponents of the Health Security Act were most against.
Opposition to the Health Security Act The Republican intellectual William Kristol—former chief of staff to Vice President Dan Quayle and editor of The Weekly Standard, published by Rupert Murdoch, from its founding in 1995 until it ceased publication in December 2018—was an early leader of the opposition to the Health Security Act. In the first of the soon-to-be-famous “Kristol Memos,” he wrote: The Clinton proposal is a serious political threat to the Republican Party. Republicans must therefore clearly understand the political strategy implicit in the Clinton plan—and then adopt an aggressive and uncompromising counterstrategy designed to delegitimize the proposal and defeat its partisan purpose. (Kristol, 1993, p. 2) On the provider and payer sides, most of the medical, hospital, and insurance industry groups were arrayed against the Health Security Act for a variety of reasons, ranging from an antagonism to “government regulation” to a concern with potential limitations on profit-making.
Goldsteen74024_10_CH10_319-340_03-18-20.indd 328
3/19/20 3:04 PM
10
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : C o m p re h e n s i v e R e f o r m
329
On the public side, the “single-payer” forces were also arrayed against it; at least their leadership was (Navarro, 1994). They felt that it did not go far enough, that it left too many players in“big health care”in place. They assumed that if the Health Security Act went down to defeat, their approach would be next on the health care agenda. Unfortunately, on that point, history proved them wrong. Finally, there was “big business.” Represented by such groups as the U.S. Chamber of Commerce and the National Association of Manufacturers, it had originally been thought to be a major supporter of the Health Security Act, at least by the Clinton administration. They were wrong. Industry groups, by and large, eventually came out in opposition (Hacker, 1996). Another factor in the defeat of the Health Security Act was the fact that, although it appeared to be well thought out and adapted to the American political and health care delivery system realities, there was no comprehensive marketing plan prepared by the forces supporting it (Hacker, 1996). Thus, under a lengthy and expensive onslaught, the Health Security Act went down to defeat in the summer of 1994 (Goldfield, 2000; Skocpol, 1995). An infamous, nationwide marketing campaign was developed during this period, which was influential in turning public opinion and policy makers against the act. The campaign—”Harry and Louise”—undermined the proposal by acknowledging problems in the health care system, but then gradually sowing seeds of doubt about the effect of change. Would change be worse than the current system? This marketing strategy was highly effective and has become a template for other efforts to undermine large public-policy initiatives (Goldsteen, Goldsteen, Swan, & Clemenã, 2001).
After Defeat of the Health Security Act: 1994 to 2010 The period after the Health Security Act was defeated, and before the Patient Protection and Affordable Care Act (ACA) was enacted in 2010 under President Barack Obama, was one of continued dissatisfaction and unrest among health care providers, patients and their advocates, and health policy makers. The problem list for the financing, distribution, and delivery of services had changed little since the time of the publication in 1932 of the CCMC final report—except that the costs were incredibly higher. Indeed, certain problems considered important by the CCMC that were still pressing originated in our country and those of our European forebears well before the CCMC’s time, in the 17th, 18th, and 19th centuries (Freymann, 1974). This was the case even though the advances in the science and technology of medicine had gone well beyond the wildest dreams of anyone giving thought to possibilities in 1932. The American health care system was continually evaluated and found lacking and even dangerous to the health of the many who lacked access to quality medical care (Angell, 1999; Blumenthal, 1999; Himmelstein, Woolhandler, & Hellander, 2001; Katz, Cardiff, Pascali, Barer, & Evans, 2002; Koplan & Fleming, 2000; Krugman, 2002; Rothman, 2001; Woolhandler & Himmelstein, 1997). Broaddus and Park (2007) warned of reversing gains in children’s health coverage because of proposed cuts in the early 2000s in the Children’s Health Insurance Program (CHIP). Alternate proposals were frequently put forward by those on both sides of the ideological divide (Blevins, 1997; Dickey & McMenamin, 1999; Himmelstein & Woolhandler, 2002; Tuohy, 2002). Dissatisfaction with the health care system was growing again (Helman & Fronstin, 2006). Lack of health insurance was linked to personal bankruptcy for people with high medical bills (Himmelstein, Warren, Thorne, & Woolhandler, 2005). The number of uninsured was increasing (Institute of Medicine, 2009). Interestingly enough, the one segment of the health care industry that seemed to be doing very well in this period was the for-profit hospital/HMO sector. For example, a headline
Goldsteen74024_10_CH10_319-340_03-18-20.indd 329
3/19/20 3:04 PM
330
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
in the February 2002 issue of the AHA’s journal Hospitals and Health Networks read,“Hospital Stocks Prove Health on Wall Street” (Carpenter, 2002). The popular companies were Tenet Health Care, Triad Hospitals, and Humana. An article published on the aol.smartmoney.com website in April 2002 was headlined “What Health Care Crisis?” It reported that Lehman Brothers had noted that managed-care stocks, which earlier were considered in “intensive care,” had “popped 76% in the last year and 48% in 2002” (Bradford, 2002). In addition, the pharmaceutical companies had been highly profitable. As reported in the British Medical Journal in 2002, “Pharmaceuticals again ranked as the most profitable sector in the United States, topping the annual Fortune 500 ranking of America’s top industries, released this month” (Gottlieb, 2002, p. 1054). A story in The New York Times about pharmaceutical profits in 2006 stated:“Drug makers continued to post strong profit gains yesterday, led by Pfizer, the world’s biggest pharmaceutical company, which reported that its third-quarter earnings had more than doubled from a year earlier” (Berenson, 2006, p. C2). WellCare, a health care provider company, saw earnings double in the fourth quarter of 2006 and membership increase by 1.4 million, whereas Cynosure, the maker of cosmetic surgery systems, reported a 75% surge in earnings in the same quarter (“Business Briefs,” 2007). Triad reported that, in the first nine months of 2006, patient revenue per adjusted admission increased 7.7%, patient revenues increased 9.8%, and revenues increased 9.5%, compared to the same period in 2005 (“Triad Reports,” 2006). Humana reported that earnings for the third quarter of 2006 were up 64% over the same period in 2005. The company was projecting significant growth for 2007 (Humana, 2006). Nevertheless, looking at the larger picture, there was a fundamental conundrum facing health policy analysts, political leaders who would like to change things, and, above all, the American people. Unfortunately, this conundrum went unaddressed. To do so, one might have asked the following questions: •
•
•
Why was it that the plea of the IOM made after it offered its litany of problems, for “all health care constituencies … [to] commit to a national statement of purpose for the health care system as a whole and to a shared agenda for improvement” (IOM, 2000, p. 5) was likely to go entirely unheeded for the foreseeable future? Why was it that the findings and recommendations of a major report on health care issued in 1932 and echoed strongly in many, many similar efforts offered since had never been acted on? Why indeed, when it came to issues such as coverage, distribution, the organization of health services, planning, quality assurance, and prevention, hadn’t things changed?
Or as Schiff and Young (2001) put it at the end of a friendly critique of the 2001 IOM report quoted earlier: We indeed have a chasm to cross. With the current emphasis on incrementalism, many reformers believe they can succeed by first attending to quality and then reforming finance and delivery. Unfortunately, you cannot bridge a chasm in two jumps—health system reform must be pursued at the same time as quality reform. And you cannot bridge the gap between Black and White or rich and poor health care by creating separate or stratified programs (which both Republicans and Democrats are proposing) based on ability to pay. Instead, we need a universal financing system that includes everyone, spreading the costs and the benefits in a fair and efficient way. (p. 401)
Goldsteen74024_10_CH10_319-340_03-18-20.indd 330
3/19/20 3:04 PM
10
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : C o m p re h e n s i v e R e f o r m
331
SUMMARY Efforts to reform the U.S. health care system comprehensively continued throughout the 20th century. Most of these were efforts to provide NHI. None was successful. It is fascinating that, for the most part, problems identified with the health care system were not the result of a technical or scientific inability to deal with diseases or other health deficits. Nor were the problems caused by a lack of money, as is the case in so many other countries. In the United States, the principal problems, as determined by major system studies done since the 1930s, were as follows: • •
• • • •
• • • •
As a nation, we spent too much on health care, not too little. The rate of increase in health care costs, which moderated somewhat in the late 1990s before gaining momentum again in the early 2000s, had been unaffected by any interventions tried to date. The geographic and demographic distribution of health services was highly variable. Much that could be done to prevent disease and promote health using available knowledge and techniques was not done. Health care was widely misallocated and fragmented. Many health care needs were under-met (e.g., not enough home health care for the infirm elderly), whereas others were over-met (e.g., too many hospital beds, too much surgery, too much diagnostic testing). Many people had no health care cost coverage of any kind. There was an increasing focus on high-tech, increasingly expensive interventions that benefit a relatively small number of people. Rationing of access, especially by income, was widespread. There were serious problems with the quality of health care.
In short, the problems were not the result of a lack of resources, but rather the misuse and misallocation of resources.
DATA SOURCES Following are authoritative sources of information concerning policy and legislation related to the U.S. health care system. They include government websites and past reports from a variety of organizations that have influenced policy and legislation.
Government Sources •
U.S. Congress. Congress hosts a website that contains legislation from the Senate and House of Representatives and all related actions beginning with introduction of each bill. For health care legislation, the site begins with the 1973–1974 congressional session. For each bill, the site includes a summary, the title and text, actions taken, amendments, sponsors and cosponsors, committees that reviewed the legislation, and any related bills. This site also contains links to each state’s legislature websites for information on state legislation including bill tracking. Start here to explore information about health care legislation, policy reports, and executive actions: www.congress.gov
Goldsteen74024_10_CH10_319-340_03-18-20.indd 331
3/19/20 3:04 PM
332
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
•
Federal Register. The Federal Register is the official source for federal agency regulations, proposed rules and notices of interest to the public, as well as executive orders and other presidential documents. It is published daily by the Office of the Federal Register, National Archives and Records Administration (NARA). It was first published in 1936. The information in the Federal Register became available electronically in 2014, although print copies can be obtained for a fee. Start here to explore information in the Federal Register: www.federalregister.gov
•
White House. The White House hosts a site that contains information about the president’s briefings, statements, and actions, including executive orders. Start here to explore information on this site: www.whitehouse.gov
Influential Reports on the U.S. Health Care System, 1927 to 2005 In a review of the Ehrenreich and Ehrenreich (1971) book, The American Health Empire: Power, Profits, and Politics, which appeared in the International Journal of Health Services (1972), Dr. Milton Roemer listed a series of other reports going back many more years. He wrote: Every few years, more recently in the last decade, there appears a book analyzing the serious defects of health care in America. In 1927, Harry H. Moore produced American Medicine and the People’s Health, in the 1930s were the magnificent 27 volumes of the Committee on the Costs of Medical Care, in 1939 there was James Rorty’s American Medicine Mobilizes, and in 1940 Hugh Cabot’s The Patient Dilemma. After World War II, Carl Malmberg wrote 140 Million Patients in 1947, Michael Davis wrote Medical Care for Tomorrow in 1955, and Richard Carter wrote The Doctor Business in 1958. In 1965, there was Selig Greenberg’s excellent The Troubled Calling: Crisis in the Medical Establishment. The year after Medicare, 1966, saw two critical outputs: The American Health Scandal by Raul Tunley and The Doctors by Martin L. Gross. In 1967, there was Fred J. Cook’s Plot Against the Patient and in 1970 Ed Cray’s In Failing Health. (p. 119) It is fascinating that, allowing for changes in magnitude, many of these analyses and the recommendations they make are similar in so many ways. It is also fascinating that three quarters of a century after Dr. Moore’s book appeared, such books, referred to and cited in the text (e.g., the IOM’s Crossing the Quality Chasm, Himmelstein and Woolhandler’s Bleeding the Patient, and Kleinke’s Oxymorons), are still being written. This is the case because not only do many of the problems of cost, distribution, coverage, and quality that past works highlight remain with us, but because of the changes in their magnitude over time—they are only getting worse. Additional reports from 1960 through 2005 include the following: Aday, L. A. (2001). At risk in America: The health and health care needs of vulnerable populations in the United States. San Francisco, CA: Jossey-Bass. Citizens’ Board of Inquiry into Health Services for Americans. (1971). Heal yourself [Report]. Washington, DC: Author. The crisis in American medicine. (1960, October). Harper’s Magazine, p. 123. Ehrenreich, B., & Ehrenreich, J. (1971). The American health empire: Power, profits, and politics. New York, NY: Vintage Books. Health Task Force of the Urban Coalition. (1969). Rx for action [Report]. Washington, DC: Author.
Goldsteen74024_10_CH10_319-340_03-18-20.indd 332
3/19/20 3:04 PM
10
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : C o m p re h e n s i v e R e f o r m
333
Himmelstein, D., & Woolhandler, S. (2001). Bleeding the patient: The consequences of corporate health care. Monroe, ME: Common Courage Press. Institute of Medicine. (2000). To err is human: Building a safer health system. Washington, DC: National Academies Press. Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academies Press. Institute of Medicine. (2003). Unequal treatment: Confronting racial and ethnic disparities in health care. Washington, DC: National Academies Press. Institute of Medicine. (2004). Patient safety. Achieving a new standard for care. Washington, DC: National Academies Press. Jonas, S. (1978). Medical mystery: The training of doctors in the United States. New York, NY: W. W. Norton. Kennedy, E. M. (1972). In critical condition: The crisis in America’s health care. New York, NY: Simon & Schuster. Kleinke, J. D. (2001). Oxymorons: The myth of a U.S. health care system. San Francisco, CA: Jossey-Bass. Knowles, J. H. (Ed.). (1977). Doing better and feeling worse. New York, NY: W. W. Norton. Moskin, J. R. (1964, November 3). The challenge to our doctors. Look, p. 26. National Commission on Community Health Services. (1966). Health is a community affair. Cambridge, MA: Harvard University Press. Ribicoff, A., & Danaceau, P. (1972). The American medical machine. New York, NY: Saturday Review Press. Schorr, D. (1970). Don’t get sick in America. Nashville, TN: Aurora Publishers. Silver, G. A. (1976). A spy in the house of medicine. Germantown, MD: Aspen Press. Somers, A. R., & Somers, H. M. (1977). Health and health care. Germantown, MD: Aspen Press.
STUDY QUESTIONS 1. What is National Health Insurance (NHI)? 2. What were the main differences between health care systems with NHI and the U.S. system during the 20th century? 3. How was the Clinton Administration’s Health Security Act different from previous U.S. proposals? 4. How did the Health Security Act address the conflict over public and private solutions to health care system problems, as outlined in Chapter 8?
Goldsteen74024_10_CH10_319-340_03-18-20.indd 333
3/19/20 3:04 PM
334
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
NOTES 1. The term health insurance is a misnomer. Generically, insurance is a system that provides for the periodic collection of relatively small sums of money from large numbers of people to protect each of them against the financial consequences of a relatively rare negative event. However, over the course of a lifetime, for most people, using health services is not a “relatively rare event.”Thus, health insurance is not insurance in the conventional sense. Rather, it is a system for the collective, long-term prepayment for the costs of health services that each member of the group of people covered will, on average, use during the time period for which he or she is covered. Furthermore, the term is a misnomer in the sense that not much “health insurance” money actually pays for the maintenance and promotion of health. Rather, most of it goes to cover the costs of care during sickness. Nevertheless, the term as it is commonly used will be employed in this chapter. 2. Most of the references used in this section were published some time ago. They provide a great deal of detail about the events described here, some from quite a close-up perspective, and remain valid and useful. For a recently published overview of the history of comprehensive U.S. health care reform efforts, from the time of the Wilson presidency (1913–1921) to the present, see Goldfield (2000). 3. Both Burrow’s book and the Harris articles contain detailed histories and analyses of the AMA’s involvement in legislative battles over NHI. The Burrow (1963) book detailed those battles through the 1950s. The Harris (1966a, 1966b) articles covered the Medicare struggles. An excellent overall historical perspective was provided by Falk (1977), a man who had been at the center of the reform battles from the time he was staff director of the CCMC until the push for NHI was dropped at the end of the Truman administration. 4. The details of all major NHI proposals made between 1935 and 1957 are summarized in Brewster (1958).
REFERENCES American Medical Association. (1990, March). Health access America. Chicago, IL: Author. Anderson, O. W. (1968). The uneasy equilibrium: Private and public financing of health services in the United States, 1875–1965. New Haven, CT: Yale University Press. Angell, M. (1999). The American health care system revisited: A new series. New England Journal of Medicine, 340(1), 481. doi:10.1056/NEJM199901073400108 Berenson, A. (2006, October 20). Pfizer and other drug makers report higher profits. The New York Times, p. C2. Blevins, S. A. (1997, December 12). Restoring health freedom: The case for a universal tax credit for health insurance. Policy Analysis (The Cato Institute), No. 290. Blumenthal, D. (1995). Health care reform—past and future. New England Journal of Medicine, 332, 465. doi:10.1056/NEJM199502163320711 Blumenthal, D. (1999). Health care reform at the close of the 20th century. New England Journal of Medicine, 340(24), 1916–1920. doi:10.1056/NEJM199906173402412 Boas, F. P. (1958). Why do we need national health insurance? In Committee on Medical Care Teaching of the Association of Teachers of Preventive Medicine (Ed.), Readings in
Goldsteen74024_10_CH10_319-340_03-18-20.indd 334
3/19/20 3:04 PM
10
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : C o m p re h e n s i v e R e f o r m
335
medical care. Chapel Hill: University of North Carolina Press. (Original work published 1945 by Society for Ethical Culture) Bradford, S. L. (2002). Stock watch: What health-care crisis? Retrieved from www.aol.smart money.com Brewster, A. W. (1958). Health insurance and related proposals for financing personal health services. Washington, DC: U.S. Government Printing Office. Broaddus, M., & Park, E. (2007). Freezing SCHIP funding in coming years would reverse recent gains in children’s health coverage. Center on Budget and Policy Priorities. Retrieved from http:// www.cbpp.org/research/freezing-schip-funding-in-coming-years-would-reverse -recent-gains-in-childrens-health Burns, E. M. (1971). Health insurance: Not if, or when, but what kind? American Journal of Public Health, 61(11), 2164–2175. doi:10.2105/AJPH.61.11.2164 Burrow, J. G. (1963). AMA: Voice of American medicine. Baltimore, MD: Johns Hopkins University Press. Burrow, J. G. (1977). Organized medicine in the progressive era. Baltimore, MD: Johns Hopkins University Press. Business Briefs (Medical). (2007, February 14). Investor’s Business Daily, p. A02. Carpenter, D. (2002). For-profit health care: Hospital stocks prove health on Wall Street. Hospitals and Health Networks, 76(2), 22, 24. Cavalier, K. (1979). National health insurance. Washington, DC: Congressional Research Service, Library of Congress. Committee for Economic Development. (1973, April). Building a national health-care system: A statement on national policy by the research and policy committee of the committee for economic development. New York, NY: Author. Committee for National Health Insurance. (1989). The health security partnership. Washington, DC: Author. Committee on Finance, U.S. Senate. (1970). Medicare and Medicaid: Problems, issues and alternatives. Washington, DC: U.S. Government Printing Office. Committee on Finance, U.S. Senate. (1979). Comparison of major features of health insurance proposals. Washington, DC: U.S. Government Printing Office. Committee on Labor and Human Resources, U.S. Senate. (1988, April 29). Background information on S. 1265: The minimum health benefits for all workers act of 1988. Washington, DC: U.S. Government Printing Office. Committee on the Costs of Medical Care. (1970). Medical care for the American people. Washington, DC: U.S. Department of Health, Education, and Welfare. (Original work published 1932 by University of Chicago Press) Committee on Ways and Means, U.S. House of Representatives. (1974). National health insurance resource book. Washington, DC: U.S. Government Printing Office. Congress.gov. (1985a). S. 1615: Health Care Improved Access Act of 1985. Retrieved from https://www.congress.gov/bill/99th-congress/senate-bill/1615?s=5&r=7 Congess.gov. (1985b). S. 1346: Medicare Solvency and Health Care Financing Reform Act of 1985. Retrieved from https://www.congress.gov/bill/99th-congress/senate-bill/1346?s=5&r=8
Goldsteen74024_10_CH10_319-340_03-18-20.indd 335
3/19/20 3:04 PM
336
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Congress.gov. (1986a). S. 2402: Access to Health Care Act of 1986. Retrieved from https://www .congress.gov/bill/99th-congress/senate-bill/2402?s=5&r=2 Congress.gov. (1986b). S. 1744: State Comprehensive Mental Health Services Plan Act of 1986. Retrieved from https://www.congress.gov/bill/99th-congress/senate-bill/1744?s=5&r=6 Davis, K. (1975). National health insurance: Benefits, costs, and consequences. Washington, DC: Brookings Institution. Dickey, N. W., & McMenamin, P. (1999). Putting power into patient choice. New England Journal of Medicine, 341(17), 1305–1308. doi:10.1056/NEJM199910213411711 Douglas-Wilson, I., & McLachlan, G. (1973). Health service prospects: An international survey. Boston, MA: Little, Brown. Editors of Fortune. (1970). Our ailing medical system: It’s time to operate. New York, NY: Harper & Row. Ehrenreich, B., & Ehrenreich, J. (1971). The American health empire: Power, profits, and politics. New York, NY: Vintage Books. Eilers, R. D. (1971a). National health insurance: What kind and how much?—Part 1. New England Journal of Medicine, 284(16), 881–886. doi:10.1056/NEJM197104222841605 Eilers, R. D. (1971b). National health insurance: What kind and how much?—Part 2. New England Journal of Medicine, 284(17), 945–954. doi:10.1056/NEJM197104292841705 Evans, R. G., Lomas, J., Barer, M. L., Labelle, R. J., Fooks, C., Stoddart, G. L.,… Tholl, W. G. (1989). Controlling health expenditures: The Canadian reality. New England Journal of Medicine, 320(9), 571–577. doi:10.1056/NEJM198903023200906 Falk, I. S. (1973). Medical care in the USA, 1932–1972: Problems, proposals and programs from the Committee on the Costs of Medical Care to the Committee for National Health Insurance. Milbank Memorial Fund Quarterly, Health and Society, 51(1), 1–32. doi:10.2307/3349608 Falk, I. S. (1977). Proposals for national health insurance in the USA: Origins and evolution, and some perceptions for the future. Milbank Memorial Fund Quarterly, Health and Society, 55(2), 161–191. doi:10.2307/3349642 Freeland, R. M. (1975). The Truman doctrine and the origins of McCarthyism. New York, NY: Alfred Knopf. Freudenheim, M. (1994, June 27). Health industry is changing itself ahead of reform. The New York Times, p. 1. Freymann, J. G. (1974). The American health care system: Its genesis and trajectory. New York, NY: Medcom. Friedman, E. (1977a). Medicaid: The primrose path (first of series). Hospitals, 51(16), 51–56. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/330377 Friedman, E. (1977b). Medicaid: Crop of nettles (third of series). Hospitals, 51(18), 73–80. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/330379 Friedman, E. (1977c). Medicaid: One seed for the crow (fourth of series). Hospitals, 51(19), 61–66. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/332611 Friedman, E. (1977d). Medicaid: Uncertain harvest (fifth of series). Hospitals, 51(21), 77–83. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/332615
Goldsteen74024_10_CH10_319-340_03-18-20.indd 336
3/19/20 3:04 PM
10
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : C o m p re h e n s i v e R e f o r m
337
Friedman, E., & Wendorf, C. (1977). Medicaid: A garden sown with dragon’s teeth (second of series). Hospitals, 51(17), 59–64. Retrieved from https://www.ncbi.nlm.nih.gov/ pubmed/334668 Fry, J., & Farndale, W. A. J. (Eds.). (1972). International medical care. Oxford, UK: Medical & Technical Publishing Company. Fuchs, V. R., & Hahn, J. S. (1990). How does Canada do it? A comparison of expenditures for physicians’ services in the United States and Canada. New England Journal of Medicine, 323(13), 884–890. doi:10.1056/NEJM199009273231306 Glaser, W. A. (1978). Health insurance bargaining. New York, NY: Gardner. Goldfield, N. I. (2000). National health reform American style: Lessons from the past. Tampa, FL: American College of Physician Executives. Goldsteen, R. L., Goldsteen, K., Swan, J. A., & Clemenã, W. (2001). Harry & Louise & health care reform: Romancing public opinion. Journal of Health Politics, Policy and Law, 26(6), 1325–1352. doi:10.1215/03616878-26-6-1325 Gottlieb, S. (2002). Drug companies maintain “astounding” profits [News]. British Medical Journal, 324(7345), 1054. doi:10.1136/bmj.324.7345.1054/b Grumbach, K., Bodenheimer, T., Himmelstein, D. U., & Woolhandler, S. (1991). Liberal benefits, conservative spending: The physicians for a National Health Program proposal. Journal of the American Medical Association, 265(19), 2549–2554. doi:10.1001/ jama.1991.03460190127034 Hacker, J. S. (1996, Winter). National health care reform: An idea whose time came and went. Journal of Health Politics, Policy and Law, 21(4), 647–696. doi:10.1215/03616878-21-4-647 Harris, R. (1966a, July 9). Annals of legislation: Medicare III—We do not compromise. The New Yorker, pp. 40–62. Harris, R. (1966b, July 16). Annals of legislation: Medicare IV—A sacred trust. The New Yorker, pp. 35–56. Hastings, J. E. (1972). Toward a national health program: Canadian experience. Bulletin of the New York Academy of Medicine, 48(1), 58–65. Retrieved from bullnyacadmed00191-0068 .pdf Helman, R., & Fronstin, P. (2006). 2006 Health Confidence Survey: Dissatisfaction with health care system doubles since 1998. EBRI Notes, 27(11), 2–10. Retrieved from https:// www.ebri.org/crawler/view/2006-health-confidence-survey-dissatisfaction-with -health-care-system-doubles-since-1998-3758 Heritage Foundation. (1989). Critical issues: A National Health System for America. Washington, DC: Author. Himmelstein, D. U., Warren, E., Thorne, D., & Woolhandler, S. (2005). Illness and injury as contributors to bankruptcy. Health Affairs, 24, W5-63–W5-73. doi:10.1377/hlthaff.w5.63 Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/15689369 Himmelstein, D. U., & Woolhandler, S. (1989). A national health program for the United States. A physicians’ proposal. New England Journal of Medicine, 320(2), 102–108. doi:10.1056/NEJM198901123200206 Himmelstein, D. U., & Woolhandler, S. (2002). Liberal benefits, conservative spending. Archives of Internal Medicine, 162(9), 973–975. doi:10.1001/archinte.162.9.973
Goldsteen74024_10_CH10_319-340_03-18-20.indd 337
3/19/20 3:04 PM
338
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Himmelstein, D. U., & Woolhandler, S., & Hellander, I.. (2001). Bleeding the patient: The consequences of corporate health care. Monroe, ME: Common Coverale Press. Hoppszallern, S., & Arges, G. (2002). Leveraging the cost of HIPAA. Hospitals and Health Networks, 76(1), 57–62. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/11912975 Humana. (2006, October 30). Humana Inc. reports third quarter 2006 financial results including earnings per share of $0.95. Business Wire. Retrieved from https://www .businesswire.com/news/home/20061030005322/en/1369312/Humana-Reports -Quarter-2006-Financial-Results-including Igelhart, J. K. (1986a). Canada’s health care system: Part 1. New England Journal of Medicine, 315(3), 202–208. doi:10.1056/NEJM198607173150330 Igelhart, J. K. (1986b). Canada’s health care system: Part 2. New England Journal of Medicine, 315(12), 778–784. doi:10.1056/NEJM198609183151238 Igelhart, J. K. (1986c). Canada’s health care system: Part 3. New England Journal of Medicine, 315(25), 1623–1628. doi:10.1056/NEJM198612183152531 Igelhart, J. K. (1990). Canada’s health care system faces its problems. New England Journal of Medicine, 322(8), 562–568. doi:10.1056/NEJM199002223220827 Institute of Medicine. (2000). To err is human: Building a safer health system. Washington, DC: National Academies Press. Institute of Medicine. (2009). America’s uninsured crisis: Consequences for health and health care. Report Brief. Retrieved from http://www.nationalacademies.org/hmd/Reports/ 2009/Americas-Uninsured-Crisis-Consequences-for-Health-and-Health-Care.aspx Institute of Medicine, Committee on health planning goals and standards. (1981). Health planning in the United States: Selected policy issues (Vol. 2). Washington, DC: National Academies Press. Jonas, S. (1974). Issues in national health insurance in the United States of America. Lancet, 2(7873), 143–146. doi:10.1016/S0140-6736(74)91567-0 Jonas, S. (1980). Planning for national health insurance by objective: The contract mechanism. Journal of Policy Studies, 9(2), 250–260. doi:10.1111/j.1541-0072.1980.tb02201.x Jonas, S. (1981). National health insurance. In S. Jonas (Ed.), Health care delivery in the United States (2nd ed., pp. 438–470). New York, NY: Springer Publishing Company. Katz, S. J., Cardiff, K., Pascali, M., Barer, M. L., & Evans, R. G. (2002). Phantoms in the snow: Canadians’ use of health care services in the United States. Health Affairs, 21(3), 19–31. doi:10.1377/hlthaff.21.3.19 Koplan, J. P., & Fleming, D. W. (2000). Current and future public health challenges. Journal of the American Medical Association, 284(13), 1696–1698. doi:10.1001/jama.284.13.1696 Kristol, W. (1993, December 2). Defeating president Clinton’s health care proposal [memo]. Retrieved from https://www.scribd.com/doc/12926608/William-Kristol-s-1993-Memo -Defeating-President-Clinton-s-Health-Care-Proposal Krugman, P. (2002, March 19). Bad medicine. The New York Times, p. A23. Kuttner, R. (1997). The Kassebaum-Kennedy bill—The limits of incrementalism. New England Journal of Medicine, 337(1), 64–67. doi:10.1056/NEJM199707033370123 Lynch, M. J., & Raphael, S. S. (1963). Medicine and the state. Springfield, IL: Charles C Thomas.
Goldsteen74024_10_CH10_319-340_03-18-20.indd 338
3/19/20 3:04 PM
10
■
H i s t o r y o f C h a n g e Fro m 1 9 0 0 t o 2 0 1 0 : C o m p re h e n s i v e R e f o r m
339
McKittrick, L. S. (1958). Medical care for the American people: Is compulsory health insurance the solution? In Committee on Medical Care Teaching of the Association of Teachers of Preventive Medicine(Ed.), Readings in medical care. Chapel Hill: University of North Carolina Press. (Original work published 1940 in the New England Journal of Medicine, 240, 998) McMahon, J. A. (1975, November 10). Statement of the American Hospital Association on National Health Insurance before the health subcommittee of the house committee on ways and means. Washington, DC: American Hospital Association. National Association of Manufacturers. (1989). Meeting the health care crisis. Washington, DC: Author. National Leadership Commission on Health Care. (1989). For the health of a nation: A shared responsibility. Ann Arbor, MI: Health Administration Press Perspectives. Navarro, V. (1994). The need to mobilize support for the Wellstone-McDermott-Conyers single-payer proposal. American Journal of Public Health, 84(2), 178–179. doi:10.2105/ AJPH.84.2.178 Nixon, R. M. (1994, September 19–26). Health care now. Excerpts from speech given by Richard Nixon to Congress on 2/18/1971. The New Republic, p. 11. Oil, Chemical, and Atomic Workers. (1989). National health care: Pass it on! Lakewood, CO: Author. Redlener, I. (1993, November 10). Presentation: Rockland County Democratic Forum. New City, NY. Roemer, M. I. (Ed.). (1960). Henry E. Sigerist on the sociology of medicine. New York, NY: MD Publications. Roemer, M. I. (1985). I. S. Falk, the Committee on the Costs of Medical Care, and the drive for national health insurance. American Journal of Public Health, 75(8), 841–848. doi:10.2105/ AJPH.75.8.841 Roemer, M. I. (1991). National health systems of the world: The countries (Vol. 1). New York, NY: Oxford University Press. Rothman, D. (2001). Severed trust: Why American medicine hasn’t been fixed [Book review]. Journal of the American Medical Association, 286(20), 2604–2605. doi:10.1001/ jama.286.20.2604-JBK1128-3-1 Schiff, G. D., & Young, Q. D. (2001). You can’t leap a chasm in two jumps: The Institute of medicine health care quality report [Book review]. Public Health Reports, 116(5), 396–403. doi:10.1016/S0033-3549(04)50067-5 Schwartz, H. (1972). The case for American medicine: A realistic look at our health care system. New York, NY: David McKay. Shabecoff, P. (1979, May 15). Kennedy offers broad health plan and challenges Carter to support it. The New York Times. Retrieved from https://www.nytimes.com/1979/05/15/ archives/kennedy-offers-broad-health-plan-and-challenges-carter-to-support.html Skocpol, T. (1995). The rise and resounding demise of the Clinton plan. Health Affairs, 14(1), 66–85. doi:10.1377/hlthaff.14.1.66 Starr, P. (1982). The social transformation of American medicine: The rise of a sovereign profession and the making of a vast industry. New York, NY: Basic Books.
Goldsteen74024_10_CH10_319-340_03-18-20.indd 339
3/19/20 3:04 PM
340
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Stevens, R. (1971). American medicine and the public interest. New Haven, CT: Yale University Press. Triad reports third quarter results. (2006, October 30). Business Wire. Truman, H. S. (1958). Message from the president of the United States. In Committee on Medical Care Teaching of the Association of Teachers of Preventive Medicine (Ed.), Readings in medical care. Chapel Hill: University of North Carolina Press. (Original work published 79th Congress, 1st Session, 1945, Washington, DC: U.S. Government Printing Office) Tuohy, C. H. (2002, May–June). The costs of constraint and prospects for health care reform in Canada. Health Affairs, 21(3), 32–46. doi:10.1377/hlthaff.21.3.32 U.S. Bipartisan Commission on Comprehensive Health Care. (1990, September). A call for action. Washington, DC: U.S. Government Printing Office. Wellstone, P. D., & Shaffer, E. R. (1993). The American Health Security Act – A singlepayer proposal. New England Journal of Medicine, 328, 1489–1493. doi:10.1056/ NEJM199305203282013 White House Domestic Policy Council. (1993). Health security: The president’s report to the American people. Washington, DC: The White House. Woolhandler, S., & Himmelstein, D. U. (1991). The deteriorating administrative efficiency of the U.S. health care system. New England Journal of Medicine, 324(18), 1253–1258. doi:10.1056/NEJM199105023241805 Woolhandler, S., & Himmelstein, D. U. (1997). Costs of care and administration at for-profit and other hospitals in the United States. New England Journal of Medicine, 336(11), 769–774. doi:10.1056/NEJM199703133361106
FURTHER READING Jonas, S. (1977). Quality-control of ambulatory care. New York, NY: Springer Publishing Company. Jonas, S. (1984). The personal health care system. New York State Journal of Medicine, 84(4), 187–189. Stark, Kennedy to propose health reforms. (1985, June 17). Washington Report on Medicine and Health.
Goldsteen74024_10_CH10_319-340_03-18-20.indd 340
3/19/20 3:04 PM
11 The Affordable Care Act: Achievements, Limitations, and Opposition
© Cagel Cartoons, Inc. By Jimmy Margulies.
LEARNING OBJECTIVES After completing this chapter, students will be able to: • Describe the major components of the Affordable Care Act (ACA), which was passed during the Obama administration. • Identify the cost-saving measures in the ACA. • Identify measures in the ACA to address equity and quality problems in the U.S. health care system. • Describe the limitations of the ACA. • Describe the executive, legislative, and legal actions taken by the Trump administration to modify the ACA. • Describe the House and Senate health care bills that were proposed, but not passed, during the Trump administration.
Goldsteen74024_11_CH11_341-368_03-18-20.indd 341
3/19/20 10:55 AM
342
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
INTRODUCTION After the defeat of the Clinton health plan, the health care system continued to grow more expensive and to show major defects in both quality and efficiency (Institute of Medicine [IOM], 2000). When Barack Obama was elected president in 2008, he was determined to seek a national solution to the health care problems of the country, but without a National Health Service or National Health Insurance (NHI). He was open to a plan that was consistent with the private-sector involvement in health care that had evolved during the 20th century, which, not surprisingly, was the kind of plan enacted. Nevertheless, the battle for passage of a bill was hard-fought for nearly two years. The bill that resulted, the Patient Protection and Affordable Care Act (PPACA), or simply the ACA, was passed in March 2010 by the Democrats with no Republican votes. The final legislation was in every way a compromise that kept a place at the table for the complex mix of public and private stakeholders in the existing system. Many of its important and needed benefits were planned to be phased in over several years, including prohibiting discrimination against persons with preexisting health conditions and eliminating annual limits on insurance coverage, both of which did not go into effect until 2014. Other provisions were scheduled to be implemented by 2020 (DHHS, 2012). Yet, the ACA is a national plan that affected all Americans, and it addressed many of the shortcomings of the old health care delivery system. It represented a huge step toward solving some of the egregious problems of the old system. In this chapter, the ACA is explained, including its achievements, limitations, and major oppositions to the legislation.
HEALTH CARE REFORM UNDER THE OBAMA ADMINISTRATION Problems That Motivated Change When President Obama took office in January 2009, he and his administration faced an intricate tapestry of public and private health care payers, as well as a sizeable, but differentiated, population of uninsured persons: •
•
Insured population’s health care payers • Employer-sponsored insurance (ESI) • Private health insurance not related to employment • Medicare • Medicaid • The Children’s Health Insurance Program (CHIP) • Military and veteran’s health insurance Uninsured population’s makeup • Unemployed, who could not afford insurance on the individual market • Employed with no ESI and who could not afford the individual market • Employed, especially the young, who did not take ESI that was available to them
This existing system of public and private payers was the springboard from which any new policies had to emerge, and it was widely considered a problem. At the societal level, costs were escalating, and health care expenditures were accounting for a greater and greater portion of the gross domestic product (GDP). Health expenditures as percentage of GDP
Goldsteen74024_11_CH11_341-368_03-18-20.indd 342
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
343
TABLE 11.1 Trends in Health Care Costs, 1960 to 2009 1960
1970
1975
1980
1990
2000
2009
% National health expenditures of GDP
5.0
6.9
7.9
8.9
12.1
13.3
17.3
Per capita health expenditures (in US$)
146
355
605
1,108
2,843
4,857
8,141
% of health consumption expenditures spent on administrative costs
3.9
3.5
3.7
4.7
5.4
5.9
6.7
Gross domestic product (GDP), national health expenditures, per capita amounts, percentage distribution, and average annual percent change: United States, selected years 1960 to 2015. SOURCE: Data from National Center for Health Statistics. (2017). Health, United States, 2016: With chartbook on long-term trends in health (Table 93). Hyattsville, MD: Author.
had steadily increased, from 13.3% in 2000 to 17.3% in 2009. Per capita expenditures for health care had gone from US$4,857 in 2000 to US$8,141 in 2009 (see Table 11.1). Meanwhile, other developed countries were paying much less for their health care systems. For example, see Figure 11.1 for a comparison of the United States to the developed countries of the Organisation for Economic Co-operation and Development (OECD). At 17.4% of GDP in 2009, U.S. health spending was one and a half times more than the next most expensive health care, in the Netherlands, and 1.8% higher than the OECD average. In addition, per capita costs were higher in the United States than in any other OECD country (see Figure 11.2). Also, administrative costs were very high compared to systems in other industrialized countries, particularly single-payer systems. For example, administrative costs were 1.2% of GDP in the United States in 2009 compared to 0.7% of GDP in France, the country with the next highest administrative costs (OECD, 2010). Finally, the U.S. health care system had poorer health outcomes compared to other countries, particularly when life expectancy and healthy life expectancy were compared. In 2007, the United States had a life expectancy of 78 and a health-adjusted life expectancy (HALE) of 70. The maximum life expectancy in that year was 83 and the maximum HALE was 76 (World Health Organization [WHO], 2010), both in Japan. Most of our peer industrialized countries do better. Furthermore, within the United States, there were disparities in these health outcomes, particularly by socioeconomic status and race and ethnicity, with life expectancies lower than 78 and HALEs lower than 70. Equity was a huge problem, as well, both in terms of having health insurance and the quality of that insurance. “The percentage of adults aged 18–64 who were uninsured increased from 11.9% in 1978 to over 18% by the mid 1990s before climbing to more than 20% in the early years of the 2010 decade” (NCHS, 2017, p. 7). Inequitable access to health care was also indicated by the wide variation in covered benefits, “junk coverage,” lack of coverage for preexisting conditions, and other characteristics of health insurance policies that affected the equity of health care coverage. Private- and employer-sponsored health plans could and did offer inexpensive plans, but at a price. Poor health insurance policies were characterized by highly restricted benefits and high out-of-pocket expenses for deductibles, premiums, and copayments, as well as lifetime and annual caps on payments. The number of uninsured and poorly insured patients had serious cost implications for the health care system. Uninsured and poorly insured persons increased the amount of uncompensated care for providers, distorting pricing as providers shifted these costs to patients with better health insurance. In addition, the uninsured and poorly insured had a greater tendency to postpone health care until their condition required ED or hospital treatment. Deferred health care exacerbates health problems and makes them more costly to treat.
Goldsteen74024_11_CH11_341-368_03-18-20.indd 343
3/19/20 10:55 AM
344
■
II
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Public
Private United States Netherlands France Germany Denmark Canada Switzerland Austria Belgium New Zealand Portugal Sweden United Kingdom Iceland Greece Norway OECD Ireland Italy Spain Slovenia Finland Slovak Rep. Brazil Australia Japan South Africa Chile Czech Rep. Israel Luxembourg Hungary Poland Estonia Korea Mexico Turkey Russian Fed. China India Indonesia
10
8
6 4 % of GDP
2
0
0
1
2
4
6
8
10
% of GDP
FIGURE 11.1 Total health expenditure as a share of gross domestic product (GDP), 2009 (or nearest year). Source: Data from Organization for Economic Co-operation and Development. (2011). Health at a glance 2011: OECD indicators. Paris, France: OECD Publishing. doi:10.1787/health_glance-2011-en
From the perspective of the individual, the health care system was also a problem: •
•
People with health insurance feared losing it, especially those with preexisting conditions. For Medicaid recipients, eligibility could be lost as a result of a small increase in income. Persons with ESI might lose health insurance through job loss or job change. Children lost coverage on their parent’s health insurance, often before they were able to afford their own or obtain a job with ESI. The tendency of insurance companies not to cover people with preexisting conditions exacerbated these fears. Out-of-pocket costs were increasing, including deductibles, co-insurance, and premiums (Schoen, Lippa, Collins, & Radley, 2012).
Goldsteen74024_11_CH11_341-368_03-18-20.indd 344
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
Public Expenditure on Health
345
Private Expenditure on Health United States Norway Switzerland Netherlands Luxembourg Canada Denmark Austria Germany France Belgium Ireland Sweden Iceland United Kingdom Australia OECD Finland Italy Spain New Zealand Japan Greece Slovenia Portugal Israel Czech Republic Slovak Republic Korea Hungary Poland Estonia Chile Russian Fed. Brazil Mexico Turkey South Africa China India Indonesia
5000
4000
3000 2000 USD PPP
1000
0
0
1000
2000
3000
4000
5000
USD PPP
FIGURE 11.2 Total health expenditure per capita, public and private, 2009 (or nearest year). Source: Data from Organization for Economic Co-operation and Development. (2011). Health at a glance 2011: OECD indicators. Paris, France: OECD Publishing. doi:10.1787/ health_glance-2011-en
•
•
Fewer and fewer employers were offering ESI. Adults under age 65 years had to purchase usually more expensive health insurance on their own or go without (Planalp, Sonier, & Fried, 2015). Even though an individual had health insurance, a health condition might not be covered or covered sufficiently to afford care. A major health problem—for example, serious injury, cancer, or stroke—could result in health care bills that exceeded an individual’s ability to pay for care.
The perception of policy makers and the public that we needed to respond to these health care system problems in a significant way propelled President Obama and the Democratic-controlled Congress to focus their attention on health care reform as a signature
Goldsteen74024_11_CH11_341-368_03-18-20.indd 345
3/19/20 10:55 AM
346
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
achievement of the administration. The Obama administration’s goals were comprehensive: to bend the cost curve downward, achieve greater equity in insurance coverage, and improve the quality of health care (i.e., Aday et al., 1999).
How the Obama Administration Planned to Achieve Its Goals It was apparent early on that reform eliminating any of the existing payers in the U.S. health care system—Medicare, Medicaid, CHIP, ESI, private health insurance, veterans and military health insurance—would not have sufficient support for passage. Each had its own set of stakeholders with vested interests in continuing their role in the health care system. This fact precluded a popular, but not sufficiently popular, option, the single-payer plan. Thus, the Obama administration and its supporters in Congress decided that the reform would have to maintain our patchwork system of public and private payers. To address the cost, equity, and quality problems of the health care system, myriad policy changes were needed to “fix” many of the major system problems that were leading to high costs, uninsurance, and disparities in health care quality, while maintaining the existing payers in the system. An underlying assumption was that cost, quality, and equity are linked, and access to health care is a prerequisite for assuring equity and controlling cost (efficiency). Thus, insuring most, if not all people, was imperative. Access to health care for all, or most, would: • • •
Reduce the use of expensive care (hospital, ED, and urgent care) that results from delaying needed care because of cost. Reduce costly exacerbation of health conditions that result when patients delay seeking needed care because of cost. Reduce uncertainty and uncompensated care for providers.
To do this within the complex system of private and public payers and the varied ability of patients to pay for health insurance, existing government health insurance plans were relatively unchanged: • • •
Medicare and health insurance for veterans and the military were retained. Traditional Medicaid was retained and could be expanded to 138% of the federal poverty level (FPL) as a state option. CHIP was extended.
Rather, changes to the private health insurance market were at the heart of the ACA, and these were aimed at insurance coverage (equity). In order to extend basic coverage to people who were uninsured or underinsured, the ACA: •
•
• •
Mandated that private health insurance plans meet minimum standards. There are 10 essential health benefits (EHB) that must be included, as well as no-cost preventive benefits with limited cost sharing. Mandated that plans cannot discriminate against people with preexisting conditions (guaranteed issue), cannot impose lifetime and annual limits on coverage, and must extend dependent coverage to age 26. Created state-based health insurance exchanges for individuals and small businesses to compare plans, apply for financial assistance, and purchase coverage. Created the Small Business Health Options Program (SHOP) to help firms with 50 or fewer employees cover their workers.
Goldsteen74024_11_CH11_341-368_03-18-20.indd 346
3/19/20 10:55 AM
11
•
•
•
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
347
Mandated that most citizens and legal residents have health insurance—the individual mandate. The private health insurance market is intended to cover everyone not already insured—those without ESI or government insurance and the uninsured. By mandating that everyone have health insurance, the ACA distributes health care costs over people in poor health and good health (community rating), not according to individuals’ risk of using health care. Provided subsidies for low-income enrollees between 100% and 250% of the FPL to reduce patient cost sharing (e.g., deductibles and copays). The federal government then makes payments to insurance companies directly to cover these reductions (cost-sharing reduction or CSR payments). Provided refundable premium tax credits, based on income and cost of coverage, for individuals and families with income between 100% and 400% of the FPL.
The individual mandate was critical to the success of the ACA as its purpose was to stabilize the private health care marketplace by distributing costs across both healthy and unhealthy people. In doing so, the drafters of the ACA were attempting to avoid what the insurance industry calls a “death spiral.”This term refers to the situation in which more individuals with high health care costs enroll in a particular plan and drive the insurer’s costs, and therefore premiums, higher. As a result, healthier people disenroll in the plan, in favor of less expensive coverage. The sicker individuals who remain in the original plan drive the insurer’s costs even higher, creating a cycle leading to collapse. By mandating that everyone—healthy and sick—have health insurance and that all health insurance plans meet a minimum requirement for coverage, the ACA aimed to prevent this situation. The ACA provided other aids to stabilize the private insurance markets, including tax benefits and subsidies for lower income people (Eibner and Nowak, 2018). In addition, the ACA put in place three organizations intended to lower health care costs and improve quality over the long term: •
•
Independent Payment Advisory Board The Independent Payment Advisory Board, as described by the White House in 2011, as follows: “outlined a framework for reducing our deficits and debt that is based on the values of shared responsibility and shared prosperity. We know we can’t reduce our deficit without reducing the growth of health care spending. But we also cannot bring down health care cost growth by simply raising costs for seniors and States and ending Medicare as we know it. That’s why the President opposes any plan that would simply place the burden of deficit reduction on seniors and undermine Medicare.” The President’s framework instead builds on the improvements made by the Affordable Care Act. It tackles Medicare fraud and excessive payments for prescription drugs, proposes a stronger Federal-State partnership in Medicaid, and includes a series of health care reforms that would save $340 billion by 2021, $480 billion by 2023 and at least an additional $1 trillion in the following decade. (Deparle, 2011, paras 1 and 2) Centers for Medicare & Medicaid Innovation The Centers for Medicare & Medicaid Innovation was established to develop cost savings through health services research, which evaluates the effectiveness and efficiency of health care treatments. “The CMS Innovation Center has a growing portfolio testing various payment and service delivery models that aim to achieve better care for patients, better health for our communities, and lower costs through improvement for our health care system” (Centers for Medicare & Medicaid Services [CMS], 2017, para 2).
Goldsteen74024_11_CH11_341-368_03-18-20.indd 347
3/19/20 10:55 AM
348
II
•
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Prevention and Public Health Fund Preventing health problems is another way to decrease demand for health care and thus its costs. If fewer people had, for example, diabetes, the cost of care to the health care system would be lower. This was the aim of the Prevention and Public Health Fund. “The Affordable Care Act established the Prevention and Public Health Fund to provide expanded and sustained national investments in prevention and public health, to improve health outcomes, and to enhance health care quality. To date, the Fund has invested in a broad range of evidence-based activities including community and clinical prevention initiatives; research, surveillance and tracking; public health infrastructure; immunizations and screenings; tobacco prevention; and public health workforce and training”(U.S. Department of Health and Human Services [DHHS], 2017, para 2).
How the ACA Was Financed A report by the Congressional Budget Office (CBO) in 2012 identified how the ACA was expected to obtain the money needed for implementation. There were two sources: cutting government spending and raising revenue (CBO, 2012). Cuts to government spending were estimated at US$741 billion, mostly in government changes to payments to doctors and hospitals that provide care to Medicaid and Medicare patients (see Figure 11.3).
450
415
400 350 300 250 200
156
150
114
100
56
50 0
Cuts in Medicare Cuts in Medicare payment rates Advantage payments
Cuts in disproportionate share payments
Other cuts
Cuts (in billions) The Congressional Budget Office
FIGURE 11.3 Affordable Care Act spending cuts, 2013 to 2022.
Goldsteen74024_11_CH11_341-368_03-18-20.indd 348
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
349
In addition, new revenue was expected from various provisions of the ACA. These include a tax penalty for those who do not purchase coverage, which was expected to generate US$55 billion over a decade. A tax on the most expensive, so-called “Cadillac,” insurance plans would result in US$111 billion. The CBO expected US$216 billion to be saved from the positive side effects of expanding insurance, like reduction in uncompensated care. Another US$318 billion was expected to be generated by having those who earn a gross income over US$200,000 pay 3.8% of investment income toward Medicare’s hospital insurance. There are also taxes on drug and medical device makers and insurance companies based on their market share and other factors.
Supreme Court Challenges to the ACA During the Obama Administration Supreme Court decisions were handed down in 2012 and 2015 as a result of Republican efforts to turn back the ACA. The 2012 decision had enormous impact on the ACA and the efforts to provide all Americans with health insurance. The attorneys general of 26 states and the National Federation of Independent Businesses had asked the Supreme Court to hear a case against the ACA, particularly the individual mandate and Medicaid expansion. The individual mandate was crucial to the law’s success. For its supporters, the main purpose of the ACA was to provide all Americans with health insurance. However, the expense of providing health insurance for all would increase an already expensive system unless the legislation had cost-containment provisions. If costs could not be controlled, any health care legislation would be unsustainable. Because other options for insuring every American were not supported by conservative legislators, the ACA addressed this problem in three ways: (a) to spread the costs of health care over all people by requiring all persons to have health insurance through the individual mandate and Medicaid expansion, (b) to seek efficiencies in the system of delivering care, and (c) to promote prevention and thereby reduce the demand for this costly service. The case brought before the Supreme Court sought to cripple the ACA’s ability to moderate price by striking down the individual mandate and Medicaid expansion (Kaiser Family Foundation, 2010; Liptak, 2011; Mears, 2011). The Obama administration defended the individual mandate as permissible under the Commerce Clause. In March 2012, a 5-4 decision by the court upheld the constitutionality of the ACA. However, in a surprise to most observers, the court did not justify its ruling with the Commerce Clause. Rather, the authority of the federal government to impose taxes was the basis of the court’s ruling, and the chief justice, a highly conservative justice known for favoring limited government, wrote the decision. Chief Justice John Roberts wrote in a split-the-difference decision, “The federal government does not have the power to order people to buy health insurance. The federal government does have the power to impose a tax on those without health insurance” (Cuccinelli & Gottstein, 2013, pp. 140–142). Roberts sided with Justices Ruth Bader Ginsburg, Stephen Breyer, Sonia Sotomayor, and Elena Kagan to form the majority opinion. As a result of the Supreme Court decision, the ACA continued to be implemented. The decision was another episode in the curious, complicated, and long tale of America’s attempt to achieve universal access to health care, as all developed nations of the world have done. However, the Supreme Court victory for the ACA was not the end of the story. The elections in November 2012 threatened to deliver a Republican president who would repeal the ACA. Republican presidential candidate Mitt Romney pledged to overturn it if elected, as did most leaders of the Republican Party, even though the ACA is virtually the same as the legislation that Romney enacted as governor of Massachusetts and the Heritage Foundation recommended as a means of keeping government out of health care. Indeed, the Supreme
Goldsteen74024_11_CH11_341-368_03-18-20.indd 349
3/19/20 10:55 AM
350
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Court decision of 2012 galvanized conservative political action to prevent reelection of President Obama, maintain a Republican majority in the House of Representatives, and create a Republican majority in the Senate. Further, the Supreme Court decision, although it allows the survival of the ACA on the basis of the federal government’s taxing authority, may have established legal precedent for future threats to federal programs that have been justified by the Commerce Clause. Upholding the individual mandate on the basis of the government’s ability to tax weakens the future ability of government in the area of economic and social justice legislation (Karlan, 2012). In 2015, another key feature of the ACA was considered by the Supreme Court, which upheld the provision that health insurance subsidies can be given to all qualifying Americans. As reported in The New York Times,“The Supreme Court ruled on Thursday that President Obama’s health care law allows the federal government to provide nationwide tax subsidies to help poor and middle-class people buy health insurance, a sweeping vindication that endorsed the larger purpose of Obama’s signature legislative achievement” (Liptak, 2015, para 1).
Status of the ACA at the End of the Obama Administration Achievements of ACA That Have Led to Its Support Among Citizens By and large, people insured under Medicare, Medicaid, CHIP, large-employer ESI, or veterans and military insurance saw little change in their coverage and costs under the ACA. And many people benefited from the specific ACA policies aimed at reducing the number of uninsured and addressing the instability of health care coverage faced by people prior to the ACA’s passage. For example, provisions of the ACA including mandated coverage for preexisting conditions, mandated minimum benefit plans, and subsidies for low- and moderate-income individuals were helpful to many. Also, the guaranteed issue policy helped people in transition: “The Affordable Care Act has enabled many of those workers to get transitional coverage that provides a bridge to the next phase of their lives—a stopgap to get health insurance if they leave a job, are laid off, start a business or retire early” (Abelson, 2017, para 2). Although access to health care and an uninsured population remained, the ACA led to decreased numbers of persons without health insurance. A report by Martinez, Zammitti, and Cohen (2017) confirmed: •
•
• •
In the first 9 months of 2016, 28.2 million (8.8%) persons of all ages were uninsured at the time of interview—20.4 million fewer persons than in 2010 and 0.4 million fewer persons than in 2015 (a statistically nonsignificant difference). In the first 9 months of 2016, among adults aged 18–64, 12.3% were uninsured at the time of interview, 20.3% had public coverage, and 69.0% had private health insurance coverage. In the first 9 months of 2016, among children aged 0–17 years, 5.0% were uninsured, 43.4% had public coverage, and 53.5% had private coverage. The rates of uninsurance at the time of interview remained relatively stable from 2010 through 2013 for all age groups except adults aged 18–24. Among adults aged 18–24, the percentage of those uninsured decreased, from 31.5% in 2010 to 25.9% in 2011, and then remained stable through 2013. (Martinez, Zammitti, & Cohen, 2017)
Reduction of Uncompensated Care The ACA also had a positive impact on uncompensated care, which the ACA counted on to reduce overall health care costs and stabilize provider costs. Using Medicare Hospital Cost
Goldsteen74024_11_CH11_341-368_03-18-20.indd 350
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
351
Reports from 2011 to 2015, the Commonwealth Fund (2017) found economically meaningful declines in uncompensated care associated with the Medicaid expansion: Uncompensated care burdens fell sharply in expansion states between 2013 and 2015, from 3.9 percent to 2.3 percent of operating costs. Estimated savings across all hospitals in Medicaid expansion states totaled $6.2 billion. The largest reductions in uncompensated care were found for hospitals in expansion states that care for the highest proportion of low-income and uninsured patients. Legislation that scales back or eliminates Medicaid expansion is likely to expose these safety-net hospitals to large cost increases. Conversely, if the 19 states that chose not to expand Medicaid were to adopt expansion, their uncompensated care costs also would decrease by an estimated $6.2 billion. (Commonwealth Fund, 2017, para 1)
Limitations of the ACA However, despite these improvements, Obamacare was never overwhelmingly supported by the public during the Obama administration. This lack of support was due mainly to problems within the private health insurance market, which is how the ACA intended to provide health insurance for those who did not have Medicare, Medicaid, CHIP, veterans and military insurance, or ESI. Historically, persons served by the private health insurance market have been the self-employed, small-business owners, employed persons whose employers do not offer ESI, or unemployed persons with the means to purchase their own health insurance coverage. Under Obamacare, many people who were already in the private health insurance market faced higher costs because the law eliminated lower-quality, cheaper health insurance plans. Therefore, an often-heard complaint about the ACA was that people could not keep their old insurance policy, as had been promised. To address this problem during implementation of the ACA, short-term waivers were given for those who wanted to keep policies that did not meet the minimum standards of the ACA. In addition, people who moved into private insurance markets and did not qualify for subsidies or tax credits under the ACA because they exceeded the qualifying FPL were particularly affected by the cost of health insurance. Recall that subsidies are provided up to 250% of the FPL, which, for a family of four in 2017, was US$61,500 annual income—a moderate, not opulent amount. Subsidies ended for individuals earning more than US$30,150 annually. Tax credits are then provided to individuals and families over 250% FPL and up to 400% FPL, which, in 2017, ended for individuals at US$48,240 and for families of four at US$98,400 (see Table 11.2). These problems continued into 2017. Health care costs had been rising since the ACA was fully implemented, and individuals and families who exceeded the FPL for subsidies or tax credit faced higher premiums in the private market: Health insurance premiums on the Affordable Care Act’s marketplaces (also called exchanges) are expected to increase faster in 2017 than in previous years due to a combination of factors, including substantial losses experienced by many insurers in this market and the phasing out of the ACA’s reinsurance program. (Dox et al., 2016, para 1) The increases between 2016 and 2017 for people who did not qualify for subsidies or tax credits ranged from 9% or lower in 18 states: Arkansas, California, Indiana, Iowa, Kentucky, Massachusetts, Michigan, Missouri, Nevada, New Hampshire, New Jersey, North Dakota, Ohio, Rhode Island, Vermont, Virginia, Washington, and Wyoming. Other states, however, saw larger increases, with five states over 50%: Alabama, Arizona, Minnesota, Oklahoma, and Pennsylvania. Each state was different, but the reader should refer to Table 11.1 in the Kaiser Family Foundation publication (Dox et al., 2016) for the monthly premium costs for 2016 and 2017, in each state, before and after tax credits.
Goldsteen74024_11_CH11_341-368_03-18-20.indd 351
3/19/20 10:55 AM
352
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
TABLE 11.2 Federal Poverty Guidelines, 2017 Household Size
100% FPL (US$)
133% FPL (US$)
150% FPL (US$)
200% FPL (US$)
250% FPL (US$)
300% FPL (US$)
400% FPL (US$)
1
12,060
16,040
18,090
24,120
30,150
36,180
48,240
2
16,240
21,599
24,360
32,480
40,600
48,720
64,960
3
20,420
27,159
30,630
40,840
51,050
61,260
81,680
4
24,600
32,718
36,900
49,200
61,500
73,800
98,400
5
28,780
38,277
43,170
57,560
71,950
86,340
115,120
6
32,960
43,837
49,440
65,920
82,400
98,880
131,840
7
37,140
49,396
55,710
74,280
92,850
111,420
148,560
8
41,320
54,956
61,980
82,640
103,300
123,960
165,280
FPL, federal poverty level.
Furthermore, the reader is directed to the website: www.healthcare.gov. The costs of various health care plans and eligibility for subsidies and tax credits are provided for each state. By the end of the Obama administration, even supporters of the ACA acknowledged that the private health insurance market needed attention and revision. The variation in health policy premiums by state and their increasing costs was a concern. There was a growing consensus that the private market needed to be stabilized and premium costs needed to be affordable for all. A notable effort to improve the quality and cost of health care during the Obama administration (but after passage of the ACA) was the bipartisan Medicare Access and CHIP Reauthorization Act of 2015 (MACRA). This bill increases payments to clinicians while encouraging transition to a value-based payment system from fee-for-service. It promotes this transition by implementing alternative payment options, including the Merit-Based Incentive Payment System (MIPS) that holds providers accountable for the cost and quality of care received by Medicare patients (American College of Cardiology, 2015). However, some ACA supporters went so far as to say that the ACA tweaking of our mixed private and public health care system was not enough and that a single-payer system, based on Medicare, would be preferable (Medicare for All). This is the context in which the Trump administration and the Republican majority in Congress began their health care deliberations in 2017.
“REPEAL AND REPLACE” EFFORTS BY REPUBLICANS Republican Objections to the ACA The 2016 election brought a Republican president and Republican majority in both the House of Representatives and the Senate. Prior to 2016, Republicans in the House and Senate had been voting to repeal the ACA since they gained a majority in the 2010 midterm elections, although they knew that President Obama would veto any bill that reached him. However, the election of 2016 altered that situation. The Republicans now had the opportunity to bring about change in the health care system by repealing and replacing the ACA.
Goldsteen74024_11_CH11_341-368_03-18-20.indd 352
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
353
The Republican opposition to the ACA is motivated by a central belief that the problems of cost, quality, and equity in the health care system could be solved more effectively by the private sector—a case of the goals being similar, but the means different. Competition in the private market would lead to greater efficiency and quality and eventually equity, according to the Republicans. They also believe that government regulations hamper the private sector’s ability to achieve these goals. As a result, Republican opposition to the ACA has focused on aspects of the law that increased government’s involvement in both spending and oversight. Related to spending, they oppose the Medicaid expansion and federal government subsidies for low-income individuals and families. Related to oversight, the regulatory mandates on the private health insurance market and the individual mandate to purchase health insurance are opposed. And the three organizations intended to lower health care costs and improve quality over the long term—Independent Payment Advisory Board, Centers for Medicare & Medicaid Innovation, and the Prevention and Public Health Fund—are opposed on both fronts. Indeed, a view expressed by many Republican opponents is that the ACA is a springboard to a single-payer system—a total government system—a plan they dislike even more than the ACA. Funding of the ACA is another point of contention. Many Republicans view the tax sources of new revenue as unfair transfers of wealth from the rich to the poor, the young to the old, and the healthy to the unhealthy.
American Healthcare Act: House of Representatives Bill The House of Representatives, with a majority of Republicans, passed a bill in May 2017 that was a complicated mix of changes to the ACA, not a repeal and replace of the ACA. The American Healthcare Act (AHCA) left Medicare, military and veterans insurance, and ESI relatively untouched. The biggest changes would have occurred in the private insurance market and to Medicaid and CHIP. The bill would have: • • •
• • • • • • • • • •
Repealed the individual mandate (in 2016) Repealed premium and cost-sharing subsidies for the private market plans (in 2020) Retained the private market rules for policies sold on the exchanges (e.g., no preexisting condition exclusions), but increased the ability of private insurers to sell policies outside the exchanges, which do not have to meet the minimum benefit mandates Modified the ACA tax credits so that younger people get more credit and older people get less credit Retained health insurance marketplaces and enrollment periods Encouraged the use of health savings accounts Maintained the Medicaid expansion for those states that had adopted it, but phased it out by 2020 Converted Medicaid funding to a per capita allotment and limited growth in 2020. This would end Medicaid as an entitlement program. Created the Patient and State Stability Fund to provide money to states for multiple purposes, such as high-risk pools and cost-sharing subsidies Added a state option to require work as a condition of eligibility for able Medicaid adults Repealed the Medicare high-income tax increase and other ACA revenue provisions Defunded the Prevention and Public Health Fund (Kaiser Family Foundation, 2017) Defunded Planned Parenthood
Goldsteen74024_11_CH11_341-368_03-18-20.indd 353
3/19/20 10:55 AM
354
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Better Care Reconciliation Act: Senate Bill The last Senate bill developed before Congress recessed in July 2017—the Better Care Reconciliation Act (BCRA)—was another complicated mix of changes to the ACA, not a repeal-and-replace bill. There were a number of revisions to the Senate bill, but the BCRA never received the 50 votes from Republican senators needed to pass. No Democrats voted for it. The June 2017 version of the bill provides insight into the kinds of changes considered by the Senate. There is actually little difference between the AHCA and the BCRA in their fundamental components: • • • • • • • • • • • •
Repeal the individual mandate (in 2016). Repeal premium and cost-sharing subsidies (in 2020). Modify tax credits to benefit younger people. Encourage health savings accounts. Retain the private market rules for policies sold on the exchanges (e.g., no preexisting condition exclusions). Maintain the Medicaid expansion for those states that had adopted it, but phase it out by 2024. Convert Medicaid to a per capita allotment. Create a fund to provide money to states for multiple purposes, such as high-risk pools and cost-sharing subsidies—the State Stability and Innovation Program. Add a state option to require work as a condition of eligibility for able Medicaid adults. Repeal the Medicare high-income tax increase and other ACA revenue provisions. Defund Planned Parenthood. Defund the Prevention and Public Health Fund (Kaiser Family Foundation, 2017).
Both the AHCA and BCRA proposals sought less federal government funding and regulation by converting Medicaid to a per capita allotment and ending the program as an entitlement, eliminating the Medicaid expansion, ending the individual mandate, weakening regulation of the private health insurance market through waivers and other means to allow insurers to offer products that are less regulated, and giving money to states that they could spend on their own priorities including high-risk pools and cost-sharing subsidies. It should be noted that none of the plans—ACA, AHCA, or BCRA—tackled a certain set of problems that have enormous influence on cost and access to health care. These include drug and medical-device pricing and the maldistribution of health care providers, which leaves many rural and urban areas underserved. The factors affecting where health care providers are located, which determine how much access even people with health insurance have, are complex and difficult to address.
End of ACA “Repeal and Replace”? In July 2017, the Republican Congress failed to repeal and replace the ACA. However, its opponents have utilized various means to undermine the law during the Trump administration, perhaps hoping that public opinion will turn against the ACA if it fails to work as promised. These oppositional actions have resulted in higher health premium costs for many people and a reduction in the number of Americans with health insurance (Kaiser Family Foundation, 2018, 2019).
Goldsteen74024_11_CH11_341-368_03-18-20.indd 354
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
355
As we have discussed, the ACA left government health insurance plans, including Medicare, health plans for the military and veterans, CHIP, and Medicaid, relatively unchanged. Rather, the ACA focused mainly on transforming the private health insurance market, requiring private insurers to: • • • •
Provide a minimum benefit package (EHB) Cover persons with preexisting conditions Extend coverage to dependents up to age 26 End lifetime and annual limits on coverage
These criteria were intended to ensure that all persons had quality health insurance by ending the availability of “junk” insurance—insurance policies with high deductibles and limited benefits. Under the ACA, the government would assist private health insurers by: • • • • •
Providing CSRs to them Giving tax credits to low-income enrollees, which assist them in paying the insurance premiums Implementing state-based health insurance exchanges Creating the SHOP Implementing and enforcing the individual mandate
Thus, another avenue for ACA opponents during the Trumpa Administration has been to undermine the law by weakening its requirements on the private health insurance market. Opponents also targeted the Medicaid expansion and the vitally important individual mandate, both of which were aimed at expanding the number of people insured. The means to weaken the ACA’s private market provisions have included: (a) executive actions; (b) federal legislation; and (c) legal actions. Next, we will discuss each of these actions.
ACA-Related Executive Actions Taken During the Trump Administration Executive actions do not require congressional approval and, therefore, have been a means to weaken fundamental provisions of the ACA during the Trump administration.
ACA Exchanges and Medicaid Expansion Some executive actions taken to undermine the ACA began early in the Trump presidency. These actions were aimed at reducing the number of people enrolling in private health insurance, as well as Medicaid. As Thompson, Gusmano, and Shohara (2018) wrote, The executive branch was a major arena in repeal-and-replace politics in 2017 and early 2018. The Trump administration pursued an array of executive initiatives to undercut the ACA. It attempted to hamper the operation of the ACA’s exchanges by discontinuing certain insurance industry subsidies, reducing advertising and outreach, shortening the enrollment period. … As for Medicaid, the Trump administration opened the door to state demonstration waivers that would impose work requirements, drug testing, time limits, lock-out periods, and greater cost sharing on enrollees (para 6).
Goldsteen74024_11_CH11_341-368_03-18-20.indd 355
3/19/20 10:55 AM
356
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
In 2019, The Wall Street Journal reported that the Medicaid work requirement instituted in Arkansas had been costly to administer while not producing much employment. The state estimated implementing the work mandate at a cost of US$26.1 million, which did not include the costs of notifying enrollees of the change. Meanwhile, studies did not find that this mandate improved the unemployment status of beneficiaries (Campo-Flores & Armour, 2019).
Quality of Health Plans Very importantly, the Trump administration brought back “junk” health insurance policies via the Presidential Executive Order Promoting Healthcare Choice and Competition Across the United States, signed by the president on Oct. 12, 2017 (Trump, 2017). This executive order exempted short-term, limited duration insurance (STLDI) plans from the “onerous and expensive insurance mandates and regulations” included in the ACA and expanded “the availability of and access to alternatives to expensive, mandate-laden (ACA) insurance” (Trump, 2017, Section 1, bii and ci). The executive order allowed people to purchase these STLDIs for up to 12 months and to renew them after that. As a result, this executive order ended the requirement that health insurers must offer only plans that cover the ACA’s EHB, cover preexisting conditions, cover dependents up to the age of 26, and end lifetime and annual limits on coverage. Health insurers can now offer these cheaper health plans to siphon off healthy enrollees and subvert community rating. A report by Sullivan in The Hill summarizes the Democratic view toward Trump’s executive order. The new rules permitted states to use Obamacare subsidies for the purchase of “short-term” health insurance plans—the cheaper, more limited policies—rather than the comprehensive plans required by the ACA. These short-term policies allow insurance companies to disallow people with pre-existing conditions or charge them more, thereby undermining the ACA’s intent to provide coverage for all (Sullivan, 2018).
Cost-Sharing Reductions CSRs were aimed at helping health insurers by reimbursing them for the copays and deductibles that low-income enrollees were not being charged. CSRs were abandoned under the Trump administration when Attorney General Jeff Sessions determined that there were no funds appropriated to pay them (Hargan, 2017). This was a blow to health insurers, since CSRs had been paid to them by the government for the copays and deductibles of low-income people. This action has resulted in higher health insurance premiums as health insurers attempt to recoup the lost CSR revenue.
ACA-Related Federal Legislation Passed During the Trump Administration In addition to executive orders, the Trump administration passed the Tax Cuts and Jobs Act of 2017 (U.S. Congress, 2017, 2018). The administration used the law, which was a major overhaul of the tax code, to repeal the ACA’s individual mandate penalty beginning in 2019. As a cornerstone of the ACA, repeal of the individual mandate penalty was another severe blow to the law. Glied (2018) summarized the consequences for the public’s health. Between 2018 and 2027, she reported that the law will reduce total federal revenue by about 4%. Moreover, the law’s repeal of the ACA’s individual mandate penalties will result in increased rates of uninsurance, with likely consequences being increased uncompensated care. Overall, she predicts the law will have a negative impact on prevention and public health: In addition, the law is expected to lead to substantial increases in the federal debt and, consequently, to calls for reductions in spending on entitlement programs, particularly Medicare, and on discretionary programs, including public health.
Goldsteen74024_11_CH11_341-368_03-18-20.indd 356
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
357
Many other provisions of the law could also have second-order effects on public health. (Glied, 2018, p. 734)
ACA-Related Legal Actions Taken During the Trump Administration Legal Challenge to the ACA During the Trump administration, a major lawsuit to nullify the ACA was undertaken by the attorneys general of 20 states headed by Republican administrations—Texas v. United States. The plaintiffs asserted that the ACA was invalidated when the Tax Cuts and Jobs Act of 2017 removed the penalty for failing to have health insurance (individual mandate) because the individual mandate could no longer be considered a tax. Plaintiffs made this argument based on the Supreme Court’s 2012 ruling that upheld the ACA. In that case, the chief justice wrote that the individual mandate penalty is constitutional because Congress has the power “to impose a tax on those without health insurance.” Without the penalty, the individual mandate could not be considered a tax. Therefore, the plaintiffs argued that“repeal of the individual mandate penalty has rendered the mandate unconstitutional. Because the mandate is an essential, nonseverable feature of the ACA, the states assert, the rest of the law must be struck down too” (Corlette, Kona, & Giovannelli, 2018, para 3). On Dec. 14, 2018, federal Judge Reed O’Connor, who heard the case, found that the ACA’s individual mandate “can no longer be sustained as an exercise of Congress’s tax power.” He ruled the mandate to be unconstitutional and, therefore, the remaining provisions invalid (Fernandez, 2018). California and 16 other states defending the ACA have appealed the ruling to the U.S. Court of Appeals for the Fifth Circuit. O’Connor later issued a stay that will keep the law in effect while the ruling is appealed (Inserro, 2019). In March 2019, the House of Representatives was approved to join the appeal.
Legal Actions in Support of the ACA In response to Texas v. United States and other threats to the ACA, two additional lawsuits seeking to uphold the ACA were initiated. 1. Association for Community Affiliated Plans et al. v. United States A coalition of consumer advocates and safety net health plans filed a lawsuit on Sept. 14, 2018, against the Department of Treasury, Department of Labor, and the DHHS that challenged the rules related to STLDI plans in President Trump’s executive order. Plaintiffs included the Association for Community Affiliated Plans, the National Alliance on Mental Illness, Mental Health America, the American Psychiatric Association, AIDS United, the National Partnership for Women and Families, and the Little Lobbyists. Keith (2018), in a summary of the plaintiff’s issues, observed that STLDI plans would not conform to the ACA’s reforms. Companies that offer these plans would be able to: • Charge higher premiums based on health status • Exclude people with preexisting conditions • Enforce annual or lifetime limits on coverage • Exclude benefit categories, such as substance abuse or pregnancy • Refuse coverage altogether These plans would be much less expensive than ACA-approved plans, since shortterm coverage is generally available only to people who can pass medical underwriting. Therefore, those who enroll would tend to be younger and healthier. Keith (2018) concluded that “The sale of these plans will thus result in adverse selection against the ACA individual market, as healthier consumers exit the ACA market to enroll in
Goldsteen74024_11_CH11_341-368_03-18-20.indd 357
3/19/20 10:55 AM
358
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
short-term coverage. This will raise premiums for those with health needs or who otherwise need or want access to comprehensive coverage” (para 12). 2. State of Maryland v. United States On Sept. 13, 2018, a lawsuit was initiated by Maryland Attorney General Brian Frosh against the Trump administration for undermining the ACA and supporting invalidation of major ACA components. The suit included the Department of Justice, DHHS, and the Internal Revenue Service. The complaint alleged that the uncertainty caused by the Trump administration about the constitutionality of the ACA directly damages Maryland. The suit seeks to have the court declare that the ACA is constitutional and enforceable (Attorney General, State of Maryland, 2018).
Health Care Reform Going Forward In our increasingly divided political culture, Republicans and Democrats still differ dramatically in their solutions to problems of the health care system. Republicans continue to favor repeal of the ACA and its replacement by a more market-based system. However, they have not offered a comprehensive replacement plan since the failure of both the AHCA and the BCRA. Rather, the Trump administration put forward a number of executive actions in 2019 that address certain problems of access and cost within the health care system, while maintaining the altered ACA. Each of them has a market-based orientation. These executive orders are: • Improving Price and Quality Transparency in American Healthcare to Put Patients First (Trump, 2019a). This executive order assumes that price transparency will bring about lower health care costs by providing price information to consumers, payers, and providers.“The goal of the executive order is to help consumers know the prices and quality of a good or service and to make informed decisions about their health care. The executive order is consistent with recent rules to, for instance, require drug manufacturers to disclose list prices in their advertisements or require hospitals to publish list prices on their websites” (Keith, 2019, para 1). • Advancing American Kidney Health (Trump, 2019b). This executive order aims to expand options for persons with kidney disease. It has three goals: “fewer patients developing kidney failure, fewer Americans receiving dialysis in dialysis centers, and more kidneys available for transplant”(DHHS, 2019, para 1). It includes provider payment models to incentivize preventive kidney care and home kidney dialysis. • Protecting and Improving Medicare for Our Nation’s Seniors (Trump, 2019c). This executive order is aimed at revising the Medicare Advantage (MA) plan, which is administered by private insurance companies under the oversight of the CMS. MA is the alternative to traditional Medicare, a government-administered program through the CMS. This executive order permits MA plans to compete with traditional Medicare for beneficiaries by offering greater flexibility in choice of providers and expanded benefits, such as dental care, optical care, and others, which they were unable to offer in the past. It would: i. encourage innovative MA benefit structures and plan designs, including through changes in regulations and guidance that reduce barriers to obtaining Medicare Medical Savings Accounts and that promote innovations in supplemental benefits and telehealth services;
Goldsteen74024_11_CH11_341-368_03-18-20.indd 358
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
359
ii. include a payment model that adjusts supplemental MA benefits to allow Medicare beneficiaries to share more directly in the savings from the program, including through cash or monetary rebates, thus creating more incentives to seek high-value care; and iii. ensure that, to the extent permitted by law, FFS [fee-for-service] Medicare is not advantaged or promoted over MA with respect to its administration. (Trump, 2019c, Section 3, i, ii, iii) The 2018 midterm elections brought about a Democratic majority in the House of Representatives and in many statehouses. Availability and affordability of health care was a major issue for winning candidates. The new speaker of the House, Nancy Pelosi, promised to review the Trump administration’s actions related to the ACA and consideration of Medicare for All. The availability, quality, and affordability of health care is a key issue for Democratic candidates seeking the presidency in 2020. The importance placed on health care by most Americans, as well as its cost, guarantee continued debate of new policy proposals as Americans seek a health care system that provides quality care for all. Basically, Democrats are considering two paths to improving the health care system. Both reflect a public-good orientation. They are: • •
Improving the ACA Replacing the ACA with a completely public system—Medicare for All
Improving the ACA could mean simply restoring the features of the legislation that have been lost or weakened under the Trump administration, including restoration of the individual mandate; the EHB for all insurance policies; and the subsidies for low-income people to afford health insurance premiums, copays, and deductibles. In addition, improvement could mean addressing some of the original ACA’s weaknesses, such as the failure to address high prescription drug prices and rising middle-class costs (Collins, Radley, & Baumgartner, 2019). Allowing people to buy into Medicare, for example, has been discussed as a solution. This would be a voluntary decision. In contrast, some Democrats favor replacing the ACA with a public system, which is often called Medicare for All. Under such a policy, the Medicare program would provide health care for all Americans and the private health insurance system would be abandoned. This plan would align the United States more closely with other developed countries. Despite Republican opposition, public favorability toward the ACA continues to increase (Kirzinger, Munana, & Brodie, 2018), and improving the ACA is considered by many Democrats a viable policy. Medicare for All is widely debated—with very strong advocates, as well as detractors.
SUMMARY When Barack Obama became president in 2008, the U.S. health care system had been the object of intense scrutiny and criticism for some time. The Obama administration responded with passage of the ACA in 2010. The ACA brought about comprehensive change that addressed many of the health care system’s problems. The Commonwealth Fund found that the ACA delivered on President Obama’s three goals for the legislation: • • •
“Expand access to affordable health insurance for those without coverage. Improve the affordability of insurance for those who already have it. Slow the rise in health care costs for individuals, families, and employers while not adding to the federal budget deficit” (Davis, 2010, p. 5).
Goldsteen74024_11_CH11_341-368_03-18-20.indd 359
3/19/20 10:55 AM
360
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
The ACA was a huge step forward in providing access to health care, particularly for low-income families. As Davis wrote, A majority of Americans stand to gain under health reform. Primary beneficiaries include the uninsured and intermittently insured, the underinsured, those who cannot afford their out-of-pocket costs or health insurance premiums, small businesses and their employees, young adults who will be able to stay on their parents’ policies until they find a job with health benefits, and those who are denied coverage because they have preexisting conditions or major health problems. … Most Americans fall into one of these categories and have personally experienced the shortcomings of our current system. (2010, p. 7) Despite these improvements in the health care system, the ACA has been opposed since its inception. The fault line is along political party lines. From the beginning, the ACA was generally hailed by Democrats, while most Republicans were critical. In fact, a major effort of the Republican Party during the Obama administration was to “repeal and replace” the ACA (or Obamacare), bills that passed the House many times, but not the Democrat-controlled Senate. Once Republicans gained majority control of the Senate in 2015 after the 2014 election, another attempt was made to repeal the ACA, and this legislation was vetoed by President Obama. Also during this time, conservative Republicans challenged the ACA by bringing it to the Supreme Court in 2012 and 2015, where it was upheld. The 2016 election of Donald Trump as president and Republican majorities in both houses of Congress provided Republicans with their opportunity to overturn the ACA. However, the Republican majorities were unable to pass an alternative to the ACA. Instead, the Trump administration threats to the ACA came in the form of executive actions, federal legislation, and legal actions. As of the writing of this book, the ACA has been weakened by these actions, but not overturned.
DATA SOURCES Following are authoritative sources of information concerning policy and legislation related to the U.S. health care system. They include government websites and past reports from a variety of organizations that have influenced policy and legislation.
Government Sources •
U.S. Congress. Congress hosts a website that contains legislation from the Senate and House of Representatives and all related actions beginning with introduction of each bill. For health care legislation, the site begins with the 1973–1974 congressional session. For each bill, the site includes a summary, the title and text, actions taken, amendments, sponsors and cosponsors, committees that reviewed the legislation, and any related bills. This site also contains links to each state’s legislature websites for information on state legislation including bill tracking. Start here to explore information about health care legislation, policy reports, and executive actions: www.congress.gov
•
Federal Register. The Federal Register is the official source for federal agency regulations, proposed rules and notices of interest to the public, as well as executive orders and other presidential documents. It is published daily by the Office of the
Goldsteen74024_11_CH11_341-368_03-18-20.indd 360
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
361
Federal Register, National Archives and Records Administration (NARA). It was first published in 1936. The information in the Federal Register became available electronically in 2014, although print copies can be obtained for a fee. Start here to explore information in the Federal Register: www.federalregister.gov •
White House. The White House hosts a site that contains information about the president’s briefings, statements, and actions, including executive orders. Start here to explore information on this site: www.whitehouse.gov
Influential Reports on the U.S. Health Care System, 1927–2005 In a review of the Ehrenreich and Ehrenreich (1971) book, The American Health Empire: Power, Profits, and Politics, which appeared in the International Journal of Health Services (1972), Dr. Milton Roemer listed a series of other reports going back many more years. He wrote, Every few years, more recently in the last decade, there appears a book analyzing the serious defects of health care in America. In 1927, Harry H. Moore produced American Medicine and the People’s Health, in the 1930s were the magnificent 27 volumes of the Committee on the Costs of Medical Care, in 1939 there was James Rorty’s American Medicine Mobilizes, and in 1940 Hugh Cabot’s The Patient Dilemma. After World War II, Carl Malmberg wrote 140 Million Patients in 1947, Michael Davis wrote Medical Care for Tomorrow in 1955, and Richard Carter wrote The Doctor Business in 1958. In 1965, there was Selig Greenberg’s excellent The Troubled Calling: Crisis in the Medical Establishment. The year after Medicare, 1966, saw two critical outputs: The American Health Scandal by Raul Tunley and The Doctors by Martin L. Gross. In 1967, there was Fred J. Cook’s Plot Against the Patient and in 1970 Ed Cray’s In Failing Health. (p. 119) It is fascinating that, allowing for changes in magnitude, many of these analyses and the recommendations they make are similar in so many ways. It is also fascinating that three-quarters of a century after Dr. Moore’s book appeared, such books, referred to and cited in the text (e.g., the IOM’s Crossing the Quality Chasm, Himmelstein and Woolhandler’s Bleeding the Patient, and Kleinke’s Oxymorons), are still being written. This is the case because not only do many of the problems of cost, distribution, coverage, and quality that past works highlight remain with us, but because of the changes in their magnitude over time—they are only getting worse. Additional reports from 1960 through 2005 include the following: Aday, L. A. (2001). At risk in America: The health and health care needs of vulnerable populations in the United States. San Francisco, CA: Jossey-Bass. Citizens’ Board of Inquiry into Health Services for Americans. (1971). Heal yourself [Report]. Washington, DC: Author. The crisis in American medicine. (1960, October). Harper’s Magazine, p. 123. Ehrenreich, B., & Ehrenreich, J. (1971). The American health empire: Power, profits, and politics. New York, NY: Vintage Books. Health Task Force of the Urban Coalition. (1969). Rx for action [Report]. Washington, DC: Author. Himmelstein, D., & Woolhandler, S. (2001). Bleeding the patient: The consequences of corporate health care. Monroe, ME: Common Courage Press.
Goldsteen74024_11_CH11_341-368_03-18-20.indd 361
3/19/20 10:55 AM
362
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Institute of Medicine. (2000). To err is human: Building a safer health system. Washington, DC: National Academies Press. Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academies Press. Institute of Medicine. (2003). Unequal treatment: Confronting racial and ethnic disparities in health care. Washington, DC: National Academies Press. Institute of Medicine. (2004). Patient safety. Achieving a new standard for care. Washington, DC: National Academies Press. Jonas, S. (1978). Medical mystery: The training of doctors in the United States. New York, NY: W. W. Norton. Kennedy, E. M. (1972). In critical condition: The crisis in America’s health care. New York, NY: Simon & Schuster. Kleinke, J. D. (2001). Oxymorons: The myth of a U.S. health care system. San Francisco, CA: Jossey-Bass. Knowles, J. H. (Ed.). (1977). Doing better and feeling worse. New York, NY: W. W. Norton. Moskin, J. R. (1964, November 3). The challenge to our doctors. Look, p. 26. National Commission on Community Health Services. (1966). Health is a community affair. Cambridge, MA: Harvard University Press. Ribicoff, A., & Danaceau, P. (1972). The American medical machine. New York, NY: Saturday Review Press. Schorr, D. (1970). Don’t get sick in America. Nashville, TN: Aurora Publishers. Silver, G. A. (1976). A spy in the house of medicine. Germantown, MD: Aspen Press. Somers, A. R., & Somers, H. M. (1977). Health and health care. Germantown, MD: Aspen Press.
STUDY QUESTIONS 1. What were the major goals and strategies of the ACA? 2. What were the major goals and strategies of the BCRA? 3. How does the ACA address the conflict over public or private solutions to health care system problems, as outlined in Chapter 8? 4. What steps has the Trump administration taken to alter the health care system?
REFERENCES Abelson, R. (2017, June 11). Flexibility that A.C.A. lent to work force is threatened by G.O.P. plan. The New York Times. Retrieved from https://www.nytimes.com/2017/06/11/health/ health- insurance-transitional-coverage.html Aday, L. A., Begley, C. E., Lairson, D. R., Slater, C. H., Richard, A. J., & Montoya, I. D. (1999). A framework for assessing the effectiveness, efficiency, and equity of behavioral healthcare. American Journal of Managed Care, 5, SP25–SP44. Retrieved from https://www .ajmc.com
Goldsteen74024_11_CH11_341-368_03-18-20.indd 362
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
363
American College of Cardiology. (2015). Medicare access and CHIP reauthorization act of 2015: What you need to know. Retrieved from https://www.acc.org/latest-in-cardiology/arti cles/2015/04/28/15/59/medicare-access-and-chip-reauthorization-act-of-2015-what -you-need-to-know Attorney General, State of Maryland. (2018, September 13). State of Maryland v. United States. Retrieved from www.marylandattorneygeneral.gov/news%20documents/Marylandv .United%20StatesACA.pdf Campo-Flores, A., & Armour, S. (2019, October 13). The Medicaid experiment in Arkansas: Thousands lost coverage, few gained jobs. The Wall Street Journal. Retrieved from https:// www.wsj.com/articles/the-medicaid-experiment-in-arkansas-thousands-lost-coverag e-few-gained-jobs-11570964402?mod=mhp&ns=prod/accounts-wsj Centers for Medicare & Medicaid Services. (2017). The CMS Innovation Center. Retrieved from https://innovation.cms.gov Collins, S. R., Radley, D. C., & Baumgartner, J. C. (2019). Trends in employer health care coverage, 2008–2018: Higher costs for workers and their families. The Commonwealth Fund. Retrieved from https://www.commonwealthfund.org/publications/2019/nov/ trends-employer-health-care-coverage-2008-2018 The Commonwealth Fund. (2017). The impact of the ACA’s Medicaid expansion on hospitals’ uncompensated care burden and the potential effects of repeal. Retrieved from http:// www.commonwealthfund.org/publications/issue-briefs/2017/may/aca-medicaid -expansion-hospital-uncompensated-care Congressional Budget Office. (2012). Report to Honorable John Boehner. Retrieved from https:// www.cbo.gov/sites/default/files/43471-hr6079_0.pdf Corlette, S., Kona, M., & Giovannelli, J. (2018, August 29). Lawsuit threatens Affordable Care Act preexisting condition protections but impact will depend on where you live. To the Point (blog), The Commonwealth Fund. Retrieved from https://www.commonwealthfund .org/blog/2018/lawsuit-ACA-preexisting-condition-protections-where-you-live Cuccinelli, K., & Gottstein, B. (2013). The last line of defense: The new fight for American liberty. New York, NY: Crown Forum. Davis, K. (2010). A new era in American health care: Realizing the potential of reform. New York, NY: The Commonwealth Fund. Deparle, N. A. (2011). The facts about the independent payment advisory board. Retrieved from https://obamawhitehouse.archives.gov/blog/2011/04/20/facts-about-independent -payment-advisory-board Dox, C., Long, M., Semanskee, A., Kamal, R., Claxton, G., & Levitt, L. (2016). 2017 premium changes and insurer participation in the Affordable Care Act’s health insurance marketplaces. Kaiser Family Foundation. Retrieved from http://www.kff.org/health -reform/issue-brief/2017-premium-changes-and-insurer-participation-in-the -affordable-care-acts-health-insurance-marketplaces/ Eibner, C. & Nowak, S. (2018). The effect of eliminating the individual mandate penalty and the role of behavioral factors. The Commonwealth Fund. Retrieved from https://www. commonwealthfund.org/publications/fund-reports/2018/jul/eliminating-individual -mandate-penalty-behavioral-factors Fernandez, M. (2018, December 15). In weaponized courts, judge who halted Affordable Care Act is a conservative favorite. The New York Times. Retrieved from https://www .nytimes.com/2018/12/15/us/judge-obamacare-reed-oconnor.html
Goldsteen74024_11_CH11_341-368_03-18-20.indd 363
3/19/20 10:55 AM
364
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Glied, S. (2018, June). Implications of the 2017 Tax Cuts and Jobs Act for public health. American Journal of Public Health, 108(6), 734–736. doi: 10.2105/AJPH.2018.304388 Hargan, E. (2017, October 12). Payments to issuers for cost-sharing reductions (CSRs). [Letter to Seema Verma, Administrator, Centers for Medicare and Medicaid Services]. Retrieved from https://www.hhs.gov/sites/default/files/csr-payment-memo.pdf Inserro, A. (2019, January 3). Federal ACA ruling to be appealed by coalition of California, democratic-led states. American Journal of Managed Care Newsroom. Retrieved from https://www .ajmc.com/newsroom/federal-aca-ruling-appealed-by-coalition-of-california -democraticled-states Institute of Medicine. (2000). To err is human: Building a safer health system. Washington, DC: National Academies Press. Kaiser Family Foundation. (2010). The Republican ‘pledge’ on health care. Kaiser Health News. Retrieved from https://khn.org/news/text-republican-health-care-document/ Kaiser Family Foundation. (2017). Compare proposals to replace the Affordable Care Act. Retrieved from http://www.kff.org/interactive/proposals-to-replace-the-affordable-care -act Kaiser Family Foundation. (2018, December 10). The number of uninsured people rose in 2017, reversing some of the coverage gains under the Affordable Care Act. Retrieved from https:// www.kff.org/uninsured/press-release/the-number-of-uninsured-people-rose-in-2017 -reversing-some-of-the-coverage-gains-under-the-affordable-care-act/ Kaiser Family Foundation. (2019, January). Health costs. Retrieved from https://www.kff.org/ health-costs/ Karlan, P. S. (2012, June 30). No respite for liberals. The New York Times: Sunday Review, Opinion. Retrieved from http://www.nytimes.com/2012/07/01/opinion/sunday/no -respite-for-liberals.html?_r=0 Keith, K. (2018, September 17). Two new lawsuits challenge Trump Administration actions on health reform. Health Affairs Blog. Retrieved from https://www.healthaffairs.org/ do/10.1377/hblog20180917.479910/full/ Keith, K. (2019, June 25). Unpacking the executive order on health care price transparency and quality. Health Affairs Blog. Retrieved from https://www.healthaffairs.org/ do/10.1377/hblog20190625.974595/full/ Kirzinger, A., Munana, C., & Brodie, M. (2018, December 19). 6 Charts about public opinion on the Affordable Care Act. Kaiser Family Foundation, Polling. Retrieved from https:// www.kff.org/health-reform/poll-finding/6-charts-about-public-opinion-on-the -affordable-care-act/ Liptak, A. (2011, November 15). Justices to hear health care case as race heats up. The New York Times, p. A1. Liptak, A. (2015, June 25). Supreme Court allows nationwide health care subsidies. The New York Times. Retrieved from http://www.nytimes.com/2015/06/26/us/obamacare -supreme-court.html Martinez, M. E., Zammitti, E. P., & Cohen, R. A. (2017). Health insurance coverage: Early release of estimates from the National Health Interview Survey, January–September 2016. National Center for Health Statistics. Retrieved from https://www.cdc.gov/nchs/data/nhis/ earlyrelease/insur201702.pdf
Goldsteen74024_11_CH11_341-368_03-18-20.indd 364
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
365
Mears, B. (2011, November 14). Supreme Court takes up challenge to health care reform law. CNN Politics. Retrieved from https://edition.cnn.com/2011/11/14/politics/health -care/index.html National Center for Health Statistics. (2017). Health, United States, 2016: With chartbook on long-term trends in health (Table 93). Hyattsville, MD: Author. Retrieved from https:// www.cdc.gov/nchs/data/hus/hus16.pdf Organization for Economic Co-operation and Development. (2010). Health expenditure and financing: Governance and health system and financing administration as share of GDP, 2010. Retrieved from https://stats.oecd.org/Index.aspx?DataSetCode=SHA Organization for Economic Co-operation and Development. (2011). Health at a glance 2011: OECD indicators. Paris, France: OECD Publishing. doi:10.1787/health_glance-2011-en Planalp, C., Sonier, J., & Fried, B. (2015). State-level trends in employer-sponsored health insurance: A state-by-state analysis. Minneapolis, MN: State Health Access Data Assistance Center. Schoen, C., Lippa, J., Collins, S., & Radley, D. (2012). State trends in premiums and deductibles, 2003–2011: Eroding protection and rising costs underscore need for action. The Commonwealth Fund. Retrieved from https://www.commonwealthfund.org/publications/ issue-briefs/2012/dec/state-trends-premiums-and-deductibles-2003-2011-eroding Sullivan, P. (2018, October 22). Dems blast Trump rule changes on Obamacare. The Hill. Retrieved from https://thehill.com/policy/healthcare/412586-dems-blast -trump-rule-changes-on-obamacare Thompson, F. J., Gusmano, M. K., & Shinohara, S. (2018, July). Trump and the affordable care act: Congressional repeal efforts, executive federalism, and program durability. Publius: The Journal of Federalism, 48(3), 396–424. doi: 10.1093/publius/pjy007 Trump, D. J. (2017, October). Presidential executive order: Promoting healthcare choice and competition across the United States. Retrieved from https://www.whitehouse.gov/pres idential-actions/presidential-executive-order-promoting-healthcare-choice-competi tion-across-united-states/ Trump, D. J. (2019a, June). Executive order on improving price and quality transparency in American healthcare to put patients first. Retrieved from https://www.whitehouse.gov/ presidential-actions/executive-order-improving-price-quality-transparency-american -healthcare-put-patients-first/ Trump, D. J. (2019b, July). Executive order on advancing American kidney health. Retrieved from https://www.whitehouse.gov/presidential-actions/executive-order-advancing-ame rican-kidney-health/ Trump, D. J. (2019c, October). Executive order on protecting and improving Medicare for our nation’s seniors. Retrieved from https://www.whitehouse.gov/presidential-actions/ executive-order-protecting-improving-medicare-nations-seniors/ U.S. Congress. (2017). Tax Cuts and Jobs Act of 2017 (P.L. 115-97). Retrieved from https:// www.congress.gov/115/plaws/publ97/PLAW-115publ97.htm U.S. Congress, Joint Committee on Taxation. (2018, December). General explanation of public law 115-97. Washington, DC: U.S. Government Publishing Office. Retrieved from https://www.jct.gov/publications.html?func=startdown&id=5152
Goldsteen74024_11_CH11_341-368_03-18-20.indd 365
3/19/20 10:55 AM
366
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
U.S. Department of Health and Human Services. (2012). About the Affordable Care Act. Retrieved from https://www.hhs.gov/healthcare/about-the-aca/index.html U.S. Department of Health and Human Services. (2017). Prevention and public health fund. Retrieved from https://www.hhs.gov/open/prevention/index.html U.S. Department of Health and Human Services. (2019, July 10). HHS launches President Trump’s ‘Advancing American Kidney Health’ initiative [Press Release]. Retrieved from https://www.hhs.gov/about/news/2019/07/10/hhs-launches-president-trump-advanc ing-american-kidney-health-initiative.html World Health Organization. (2010). World health statistics 2010. Retrieved from http://www .who.int/whosis/whostat/2010/en/
FURTHER READING American Medical Association. (2017). Independent Payment Advisory Board. Retrieved from https://www.ama-assn.org/practice-management/independent-payment-advisory -board Consumer Reports. (2012). Junk health insurance: Stingy plans may be worse than no insurance at all. Retrieved from http://www.consumerreports.org/cro/magazine/2012/03/ junk-health-insurance/index.htm Eibner, C. (2017, January 11). Repeal-and-delay would make budget neutrality for the ACA replacement difficult. To the Point: The Commonwealth Fund. Retrieved from http://www.commonwealthfund.org/publications/blog/2017/jan/repeal-and-delay -budget-neutrality-aca-replacement Energy and Commerce Committee, U.S. House of Representatives. (2017). The AHCA: The Patient State and Stability Fund. HealthCare.gov (A federal government website managed by the U.S. Department of Health and Human Services). (2012). Provisions of the Affordable Care Act, by year. Health Reform Tracker. (2017a). The ACA’s “Impending Implosion”: Fact or fiction? Health Reform Tracker. (2017b). Summary of stakeholder views. Hellmann, J., Weixel, N., & Sullivan, P. (2019, January 3). Overnight health care: Dem states take first step to appeal Obama Care ruling | Pelosi backs hearings on ‘Medicare for all’ | Maine governor signs order for Medicaid expansion. The Hill. Retrieved from https://thehill.com/policy/healthcare/overnights/423794-overnight-health-care-dem -states-take-first-step-in-appealing Kaiser Family Foundation. (2017a). State action on the Medicaid expansion decision, January 2017. Retrieved from http:// www.kff.org/health-reform/state-indicator/state-activity-around -expanding-medicaid-under-the-affordable-care-act/?currentTimeframe=0&sortMod el=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D Kaiser Family Foundation. (2017b). Total monthly Medicaid and CHIP enrollment, January 2017. Retrieved from http://www.kff.org/health-reform/state-indicator/total-monthly -medicaid-and-chip-enrollment/?currentTimeframe=0&sortModel=%7B%22colId %22:%22Total%20Monthly%20Medicaid%2FCHIP%20 Enrollment%22,%22sort%22: %22desc%22%7D
Goldsteen74024_11_CH11_341-368_03-18-20.indd 366
3/19/20 10:55 AM
11
■
Th e A f f o r d a b l e C a re A c t : A c h i e v e m e n t s , L i m i t a t i o n s , a n d O p p o s i t i o n
367
Lassman, D., Sisko, A. M., Catlin, A., Barron, M. C., Benson, J., Cuckler, G. A., … Whittle, L. (2017). Health spending by state 1991–2014: Measuring per capita spending by payers and pro-grams. Health Affairs, 36(7), 1318–1327. doi: 10.1377/hlthaff.2017.0416 Levey, N. N. & Kim, K. (2017, June 28). A side-by-side comparison of Obamacare and the GOP’s replacement plans. Los Angeles Times. Retrieved from http://www.latimes.com/ projects/la-na-pol-obamacare-repeal/ Medicaid.gov. (2019). September 2019 Medicaid and CHIP enrollment data highlights. Retrieved from https://www.medicaid.gov/medicaid/program-information/medicaid-and -chip-enrollment-data/report-highlights/index.html Republican Governors Association. (2017). Our governors. Retrieved from https://www.rga .org Rudd, R. A., Seth, P., David, F., & Scholl, L. (2016). Increases in drug and opioid-involved overdose deaths—United States, 2010–2015. Morbidity and Mortality Weekly Report, 65(50/51): 1445–1452. doi: 10.15585/mmwr.mm655051e1 Silver, N. (2017, March 7). Why it’s so hard for the GOP to agree on health care. FiveThirtyEight. Retrieved from https://fivethirtyeight.com/features/why-its-so-hard-for-the -gop-to-agree-on-health-care/ Tanner, M. (2017, April 5). Hard truths about health care. National Review. Retrieved from http:// www.nationalreview.com/article/446439/health-care-basic-facts-and-hard-truths U.S. Census Bureau. (2017). Annual estimates of the resident population for the United States, regions, states, and Puerto Rico: April 1, 2010 to July 1, 2016. Retrieved from https://www .census.gov/data/tables/time-series/demo/popest/2010s-state-total.html U.S. Senate. (2017). Senators by state. Retrieved from https://www.senate.gov
Goldsteen74024_11_CH11_341-368_03-18-20.indd 367
3/19/20 10:55 AM
Goldsteen74024_11_CH11_341-368_03-18-20.indd 368
3/19/20 10:55 AM
12 Trends in the U.S. Health Care System
© Randy Glasbergen.
LEARNING OBJECTIVES After completing this chapter, students will be able to: • Discuss the status of the Affordable Care Act (ACA) and changes that have been made to it during the Obama and Trump administrations. • Describe trends in the role of the private and public sectors in the U.S. health care system. • Describe trends in consolidation in health care. • Describe trends in use of technological advances in health care and their impacts.
CURRENT STATE OF U.S. HEALTH POLICY With enactment of the Patient Protection and Affordable Care Act (ACA) of 2010 under President Obama, we saw comprehensive reform in the U.S. health care system for the first time.Yet, consistent with the American context discussed in Chapter 8, Debates That Have Structured
Goldsteen74024_12_CH12_369-380_03-18-20.indd 369
3/19/20 3:03 PM
370
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Health Care System Change, the overhaul of the health care system maintained the mixed public and private system. All previous private-sector participants in health care delivery remained, even though governmental involvement had been expanded through mandates on individuals; employers; health insurance companies; health care providers, including physicians, hospitals, and long-term care facilities; as well as pharmaceutical companies. An example of the reach of the bill’s mandates is the overall approach to expanding access to health care coverage: Require most U.S. citizens and legal residents to have health insurance. Create state-based American Health Benefit Exchanges through which individuals can purchase coverage, with premium and cost sharing credits available to individuals/ families with income between 133–400% of the federal poverty level (the poverty level is $18,310 for a family of three in 2009) and create separate Exchanges through which small businesses can purchase coverage. Require employers to pay penalties for employees who receive tax credits for health insurance through an Exchange, with exceptions for small employers. Impose new regulations on health plans in the Exchanges and in the individual and small group markets. Expand Medicaid to 133% of the federal poverty level. (Kaiser Family Foundation, 2013, para 2) In addition, there had been an expansion of the public programs—Medicaid and the Children’s Health Insurance Program (CHIP)—under the ACA, as well as creation of state-based health insurance exchanges—American Health Benefit Exchanges and Small Business Health Options Program (SHOP) Exchanges—that were to be“administered by a government agency or nonprofit organization and (through) which individuals and small businesses with up to 100 employees could purchase qualified coverage” (Kaiser Family Foundation, 2013, para 17). Therefore, we can say that under the original ACA, public-sector involvement in the health care delivery system was substantial, although the private sector was very involved as well.
Zigzag Theory of U.S. Health Care Reform However, as discussed in Chapter 11, The Affordable Care Act: Achievements, Limitations and Opposition, passage of the ACA was not the end of the story. The drama of health care reform has continued, following a familiar zigzag pattern. Increased public-sector involvement in the health care system under the ACA brought about a reaction to turn back or moderate this outcome. Policy took a zig toward increased public involvement with the ACA and then a zag back toward asserting more private-sector engagement. Beginning in the period after the ACA was enacted and through the Trump administration that followed, the rhetoric of Americans who wish to limit government has been perhaps more explicit and strident than at any time in memory, and antigovernment sentiment has appeared more widespread and powerful. The rise of the Tea Party as the most influential representative of conservative America has been a hallmark of this period. The mission and core principles of the Tea Party movement, in its own words, are: At its root the American Dream is about freedom. Freedom to work hard and the freedom to keep the fruits of your labor to use as you see fit without harming others and without hindering their freedom. Very simply, three guiding principles give rise to the freedom necessary to pursue and live the American Dream (Tea Party Patriots, 2020, para 1): • • •
Personal Freedom Economic Freedom Debt-Free Future
The ideas of the Tea Party Patriots were not new. Indeed, they arose from a concerted effort since the 1980s of a few extremely wealthy families—including the Koch brothers, the
Goldsteen74024_12_CH12_369-380_03-18-20.indd 370
3/19/20 3:03 PM
12
■
Tre n d s i n t h e U. S. H e a l t h C a re S y s t e m
371
Coors brewing family, the DeVos family that founded Amway, and others—to change the direction of American policy, including health policy: They challenged the widely accepted post-World War II consensus that an activist government was a force for public good. Instead they argued for “limited government,” drastically lower personal and corporate taxes, minimal social services for the needy, and much less oversight of industry, particularly in the environmental arena. (Mayer, 2016, p. 7) Republican politicians and the Republican Party were their means to success through the large political donations they received from these affluent donors. Thus, it is not surprising that, after the ACA was passed and for the remainder of the Obama administration, Republicans in Congress repeatedly attempted to repeal the legislation. They explained themselves in the“Pledge”on Health Care:“Because the new health care law kills jobs, raises taxes, and increases the cost of health care, we will immediately take action to repeal this law”(Kaiser Family Foundation, 2010, para 11). This assertion was without basis in fact, but was part of the“calculus of deceit”practiced by radical opponents of the ACA. Mayer (2016) describes a campaign developed by the Koch brothers and their allies, which illustrates this practice: Rather than respectfully debating Obama’s health care plan as a policy issue, the Kochs and their allied donors poured cash into a dark-money group call the Center to Protect Patient Rights, which mounted a guerrilla war of fearmongering and vitriol. Television ads sponsored by the group featured the false claims that Obama’s plan was “a government takeover” of health care, which PolitiFact named “the Lie of the Year” in 2010. Meanwhile, a spinoff of Americans for Prosperity organized anti-Obamacare rallies at which protesters unfurled banners depicting corpses from Dachau, implying that Obama’s policies would result in mass murder. (Mayer, 2016, p. xx) When repeal of the ACA was unsuccessful, opponents found ways to weaken the legislation in the remaining years of the Obama administration. Republicans in Congress found bipartisan support to delay important provisions of the ACA, including the tax on generous health plans and a separate tax on health insurance providers. The excise tax on manufacturers of medical devices, which took effect in 2013, was suspended through 2017. The White House and many economists defended the “Cadillac tax” on high-cost employer-sponsored health plans as a way to reduce health costs and make the health care system more efficient (Herszenhorn & Pear, 2015). The Commonwealth Fund explains, A last-minute deal in Congress delayed or suspended some of the taxes included in the ACA—one on medical devices, one on health insurers, and one on high-cost health plans. Estimated cost: $35.8 billion in lost revenue. To be clear, most of the ACA’s funding comes from general revenue, and so isn’t directly impacted by these taxes. (Blumenthal & Squires, 2015, para 5) In addition, many states rejected the Medicaid expansion, which is a feature of the ACA whereby the income eligibility criteria are expanded to include more people and the costs of adding health care for a greater number of people is paid by the federal government at first. This was a blow for the goal of attaining full health care coverage. Another disappointment concerning the ACA was the performance of the Consumer Operated and Oriented Plan Program (CO-OP). “The Affordable Care Act calls for the establishment of the Consumer Operated and Oriented Plan (CO-OP) Program, which will foster the creation of qualified nonprofit health insurance issuers to offer competitive health plans in the individual and small group markets”(Centers for Medicare & Medicaid Services
Goldsteen74024_12_CH12_369-380_03-18-20.indd 371
3/19/20 3:03 PM
372
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
[CMS], 2015, para 1). However, the Commonwealth Fund assessment was that this would not be a major defeat for ACA exchanges: Underfunding for risk corridor programs designed to stabilize premiums, unmanageable deadlines, restrictions on marketing, the difficulty of setting up brand new insurance companies—there are many culprits behind the collapse of 12 of the 23 ACA-funded CO-OPs (Consumer Operated and Oriented Plans). But evidence that the folding CO-OPs are a harbinger of a broader collapse of the ACA exchanges remains scant. Rather, the CO-OPs’ struggles have highlighted the substantial barriers to injecting competition into insurance markets—and how both economics and politics can get in the way. (Blumenthal & Squires, 2015, para 7) The zag toward strengthening private-sector involvement in the health care system has continued, and even accelerated, since President Trump took office in January 2016. The 2016 election brought Republican majorities in both houses of Congress and provided Republicans with the opportunity to overturn the ACA. However, the Republican majorities were unable to pass an alternative to the ACA. Instead, executive actions by the president, federal legislation, and legal actions have been used during the Trump administration to weaken the ACA and its provisions to increase public involvement in health care. These are described in Chapter 11, The Affordable Care Act: Achievements, Limitations and Opposition. Medicare provides a summary example of the zigzag in U.S. health care reform. After the original Medicare legislation was enacted in 1965, each of the subsequent modifications expanded private-sector participation in the program (Patel & Guterman, 2017). •
•
•
•
1965—Medicare was passed to provide health care for people aged 65 years and older. This legislation designated the CMS to administer the Medicare program and pay health care providers directly on a fee-for-service basis. This plan is called traditional or original Medicare, and it has two parts: Part A (hospital insurance) and Part B (other medical insurance including provider services and outpatient care). Prior to this legislation, there were no government health care programs for seniors. 1997—Medicare+Choice (also referred to as Part C and currently called Medicare Advantage) was passed to develop a managed care option within the Medicare program aimed at lowering its costs. This legislation—the Medicare Balanced Budget Act (BBA) of 1997—created Medicare+Choice as an alternative to traditional Medicare. Unlike traditional Medicare, CMS provides funds to private companies, which then administer the Medicare+Choice plans. Traditional Medicare (Parts A and B) remained a choice for Medicare-eligible seniors. 2003—The Medicare Prescription Drug, Improvement, and Modernization Act (MMA) of 2003 (also referred to as Part D) was passed to assist seniors with the rising cost of drug therapies, which were not covered by the Medicare plans at that time. Part D followed the design of Medicare+Choice: CMS provided funds to private companies, which then administered the program. 2019—Executive Order on Protecting and Improving Medicare for Our Nation’s Seniors was issued on October 3 to expand the Medicare Advantage Plan (formerly Medicare+Choice), which is contracted to private companies, and make it more attractive than traditional Medicare for Medicare beneficiaries (Lipschutz, 2019).
U.S. HEALTH CARE SYSTEM TRENDS The ACA has provided a comprehensive framework for health care delivery, but this does not mean that it has halted change. Because the U.S. health care system remains a decentralized
Goldsteen74024_12_CH12_369-380_03-18-20.indd 372
3/19/20 3:03 PM
12
■
Tre n d s i n t h e U. S. H e a l t h C a re S y s t e m
373
mix of public and private stakeholders—payers, providers, employers, researchers, pharmaceutical and medical equipment suppliers, policy makers, and others—innovation continues in what might be called “creative chaos.”Trends in consolidation, consumerism, technological advancement, and payment reform are among the areas that are changing health care delivery, and they are affecting the system, regardless of the ACA or with its help. Much is being done to improve the quality and efficiency of health care and provide value to patients within and outside the ACA framework. Even if the ACA is overturned, many of its policies will remain, as they represent trends that were underway before passage of the bill and have much support in all sectors of the health care system. Following is a brief description of major trends in the U.S. health care system at this time.
Consolidation in the Health Care System Consolidation will be an ongoing theme, continuing the trend of the past 20 years. As the 2015 Commonwealth Fund report notes, It seemed like every week in 2015 brought news of a mega-merger between two drug companies, hospital systems, or health insurers. This arms race in market size has attracted scrutiny from regulators and calls for greater antitrust enforcement. Such calls are likely to grow louder in light of new evidence linking high regional private health spending to market concentration, and indications that competition in insurance markets lowers premiums. (Blumenthal & Squires, 2015, para 6) This is as true today as in 2015. Consolidation continues to take place across three dimensions: • • •
Vertical with payers and providers Horizontal with the creation of larger systems of providers such as hospitals Continuum of care from primary care through postacute care
In consolidation, national payer chains dominate, including United, Aetna, and Blue Cross Blue Shield. Also, national health care delivery chains dominate, including Community Health Systems (CHS), HCA Healthcare, and Tenet Healthcare. State- and regional-based organizations are not the dominant players. Federal regulations rather than state regulations are tending to predominate; as a result, the trend is toward nationalization of payers and providers.
Big Data and Health Information Access to more and better data, with the ability to manage and analyze it, will continue to transform the health care system: •
•
•
Complete, longitudinal electronic health records will allow a previously inconceivable level of data mining, enabling new levels of understanding about how genomics/biome, environment, and behavior affect health and medical care. Access to data will increase the emphasis on quality reporting and pay for performance, which will bring about improvements in quality of care, some improvements in costs, and eventually improvements in outcomes. Evaluations of medical procedure effectiveness, and resulting protocols, will continue to improve as a result of new data systems.
Goldsteen74024_12_CH12_369-380_03-18-20.indd 373
3/19/20 3:03 PM
374
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
Prevention and Mental Health • •
•
Mental health, behavioral health, and physical health will be more tightly linked in diagnosis and treatment. There will be continuing interest in prevention in order to control health care costs. This trend also links primary care and public health, in order to foster prevention and to diagnose early. The health care systems will become more oriented toward promoting health in populations (population health).
Cost of Prescription Drugs Under Scrutiny The “correct pricing” of pharmaceuticals will become a bigger issue in order to control cost, including inpatient care, resulting from, for example, coronary events (e.g., Lipitor) and liver failure (e.g., new hepatitis cures, although expensive, are cheaper than transplants).
Impact of New Technology The continual pursuit of improved quality and efficiency in the health care system will drive application of technological innovations and policy changes. Technological improvements will continue to address cost or cost and quality. •
•
• • •
•
Automation will start to take hold—starting with eliminating lower-level jobs like phlebotomists and coders while accelerating/supplementing higher-level jobs like RNs and physicians, for example, through computer-assisted diagnosis, computer-assisted documentation, and continuous patient assessments. Genomics and proteomics will lead to increasingly personalized treatments and protocols in the short term and begin to revolutionize the approach to medicine and health in general over longer time periods. We will start growing what we used to manufacture. This is already happening with knee implants. We will start injecting stem cells, nanobots, or other biologics to regrow new body parts and replace surgery. Medical devices and drugs will become so personalized that they will need to be evaluated like a medical procedure—effectiveness of an approach rather than a particular chemical compound or manufactured device. Shorter term new technology and understanding will allow more “site of service” optimization: hospital → outpatient → home care → telemedicine.
Hospital Versus Ambulatory Care There will continue to be widespread use of ambulatory, home, and community care in place of traditional inpatient services and expanded use of new communication and monitoring techniques. Medical devices have become more portable and sophisticated, making it possible to treat and monitor chronic conditions outside the hospital. A significant number of devices including infusion pumps, ventilators and wound care therapies are now
Goldsteen74024_12_CH12_369-380_03-18-20.indd 374
3/19/20 3:03 PM
12
■
Tre n d s i n t h e U. S. H e a l t h C a re S y s t e m
375
being used for home care. Given the growing number of home medical devices, the Food and Drug Administration plans on developing procedures for makers of home-care equipment. Procedures will include post-marketing follow-up and other things that will encourage the safe use of these devices. (American Hospital Association, 2011, para 3)
Consumerism People have historically been their own first line of defense against disease, and “self care” remains most people’s care the majority of the time. Given that much of most people’s health is tied to nonmedical factors and, conversely, control over one’s health may feel synonymous with control over one’s body and life, patient empowerment and consumerism have strong appeal.
Choosing Complementary Medicine A tremendous amount of out-of-pocket money is being spent by Americans each year on complementary or alternative medical care, that is, nonallopathic medicine. A growing trend in hospitals is to add complementary medical therapies to their offerings. These include acupuncture, massage therapy, guided imagery for stress reduction, pet therapy, and music/art therapy. The National Center for Complementary and Integrative Health (NCCIH) and the Centers for Disease Control and Prevention (CDC) reported that in 2012, Americans spent: •
•
US$14.7 billion out-of-pocket on visits to alternative health providers, including chiropractors, acupuncturists, and massage therapists. This amount was about 30% of what was spent out-of-pocket for conventional physicians. US$12.8 billion out-of-pocket on natural product supplements. This amount was about one-quarter of what was spent out-of-pocket on prescription drugs (Nahin, Barnes, & Stussman, 2016).
Andrews (2011) observed that “As hospitals elbow one another to attract patients, increasingly they’re hoping to tap into Americans’ interest in—and willingness to spend money on—complementary and alternative therapies such as acupuncture and massage. … [H]ospitals aren’t blind to the opportunity these therapies present to attract patients and perhaps make some money” (Andrews, 2011, para 2). One explanation for the rise of complementary and alternative medicine (CAM) is the perceived empowerment and open relationships between consumers and CAM practitioners (Emmerton, Fejzic, & Tett, 2012). Additionally, consumerism can be seen as people often seek alternatives to traditional or conventional medical care after experiences with conventional medical care that fall short of meeting their needs and expectations (Sirois & Purc-Stephenson, 2008).
Patient Access to Medical Records Through the Health Insurance Portability and Accountability Act (HIPAA) of 1996 and, later, the Health Information Technology for Economic and Clinical Health (HITECH) Act, which was part of the American Recovery and Reinvestment Act of 2009, a patient’s right to view, download, transmit, and otherwise gain access to their medical records was solidified into law and promulgated in regulations that followed (e.g., Department of Health and Human Services [DHHS], 2000, 2017).
Goldsteen74024_12_CH12_369-380_03-18-20.indd 375
3/19/20 3:03 PM
376
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
The impact of these pieces of legislation was slow to be perceptible for reasons not the least of which were the relatively small amount of health care data in digital form and relatively low benefits for providers to share these data easily in 1996. However, they have the potential to empower patients to control their health care journey and bring their data with them as never before. Additionally, they create the potential for consumer-oriented third parties to assist patients in new ways or provide new insights into their health (or even enable research that was not practical before; Blumenthal & Chopra, 2018; Christensen, Waldeck, & Fogg, 2017; Sullivan, 2018). It should be noted that to the extent that devices (e.g., smartphones) empowered with patients’ data qualify as medical devices (as outlined in Chapter 4, Medicines, Devices, and Technology), they would still be subject to regulation as such by the Food and Drug Administration (FDA).
ZIGZAG OR A PRIVATE SYSTEM? The strong, historical incentives to maintain a mixed health care system have prevented the United States from following our peer countries. All of them have primarily public systems, whereby the government ensures health care for all residents through direct provision of services (e.g., United Kingdom), universal health insurance (e.g., Canada), or a mix of these. However, there are signs that the United States may be on the threshold of developing a nonmixed health care delivery enterprise (Pellegrino, 1999). Playing to a strong current of antigovernment sentiment in the United States since the 1980s, conservative stakeholders have pressed toward privatization of public functions. Although antigovernment sentiment among Americans is not uncritical or necessarily a primary motivation (Goldsteen, Goldsteen, Kronenfeld, & Hann, 1997), it has been a useful political device for ideologues to promote a private sector–only agenda. The “framing” of issues in antigovernment terms has succeeded in limiting public-sector involvement in health care, as well as other areas. This “crafted approach” is working to move health care and other public activities away from the mixed enterprise system. We are in an era in which privatization of public-sector functions is widespread. There is “privatization creep” in health care as well as other sectors. For example, private companies have been given long-term leases for public roads in Northern Virginia on the Dulles Greenway, in Indiana on the East–West Toll Road, and on a 157-mile highway running east from Chicago to the Ohio border. The idea has been considered in New Jersey, Illinois, Ohio, Texas, and other locales. Commodification of water is occurring throughout the world, including the United States. Many municipalities are looking to private corporations for long-term leasing of water supplies. The transnational private water corporations, including Suez, Vivendi, and Nestle/Perrier, have annual revenues of over US$1 trillion and have privatized many formerly public water sources. As water shortages and conflicts increase, water is more and more being transformed from a public good to a privately owned commodity that is sold and traded for profit. It is an increasingly alluring idea to municipalities faced with expensive infrastructure costs. Major functions of the military have been privatized in recent years. There are advocates for privatizing military maintenance and other functions traditionally performed by the military itself. Blackwater USA, by its own statement in 2007, “the most comprehensive professional military, law enforcement, security, peacekeeping, and stability operations company in the world”(Blackwater USA, 2007, para 1; since 2009, Xe Services, doing business as
Goldsteen74024_12_CH12_369-380_03-18-20.indd 376
3/19/20 3:03 PM
12
■
Tre n d s i n t h e U. S. H e a l t h C a re S y s t e m
377
Academi), was used heavily in the Iraq War and other military conflicts. A review of privatizing military training by Avant (2005, p. 1) summarizes the current situation: • • •
Private military companies (PMCs), performing an array of security tasks for a variety of clients, have proliferated. In pursuing its war on terrorism, the Pentagon is increasingly relying on the services of PMCs, as overseas training programs expand. Although PMCs have long performed covert and unsavory tasks, today’s PMCs are seeking to polish their image as legitimate firms.
In the realm of health care delivery, changes to the Medicare program over the years are examples of privatization creep into this originally public plan. This is discussed earlier in the chapter as the zigzag between public and private control of health care programs. Indeed, the motivation for the Medicare Advantage plans was clearly not fiscal restraint, but the desire to move health care delivery to the private, for-profit sector, as evidenced by its excess cost, as reported by Krugman (2007). A study by the Medicare Payment Advisory Commission, an independent federal body that advises Congress on Medicare issues, found that the cost of Medicare Advantage was 11% more per beneficiary than traditional Medicare. “According to the Commonwealth Fund, which has a similar estimate of the excess cost, the subsidy to private HMOs cost Medicare $5.4 billion in 2005” (Krugman, 2007, para 6). It seems likely that the private sector will continue in traditional service areas, such as supply of therapeutics and equipment, and provide new services such as information technology. There is also little doubt that the public sector will continue supporting medical research, health workforce training, and public health functions such as epidemic control because of their high cost and lack of profitability. At issue is whether the mixed system will prevail in the direct provision of health care—ambulatory, hospital, long-term care, and so forth. The balance between private and public for the delivery of direct services to the general population may be shifting in favor of the private, for-profit sector. Although we could address the problems of quality, equity, and efficiency by expanding the highly successful Medicare program to all Americans, we may be moving instead toward a totally integrated delivery system owned by a few large companies, such as Humana, Triad, and UnitedHealth Group, and a small public sector to serve those deemed“unaffordable”by the private-sector companies. Employer-based health insurance, the private health insurance market, and public programs for special groups, such as the poor, elderly, and veterans, would be eliminated. Thus, health care delivery might be integrated and “single payer,” but the provider would be a for-profit corporation rather than a public or nonprofit entity. As a result of the extreme schism between Americans with a strong antigovernment orientation and those who desire a strong role for the public sector in health care and other endeavors, we are unable to say how the health care system will change in this regard. At this time, a case could be made that the ACA will be repealed, or at least seriously weakened, and replaced by the previous health care delivery system or one with a smaller, even nonexistent, governmental role. Much depends upon the 2020 elections, which will determine the next president of the United States and the majority party in Congress. Should a Republican president be elected, the new legislation is surely endangered. The road to health care reform remains full of potholes, and its destination is still uncertain. Health policy in the United States is still pulled taut between those who want government to take an active role in assuring equal rights and opportunities for Americans and those who believe that equalities will occur naturally, with little governmental action, as an offshoot of private enterprise.
Goldsteen74024_12_CH12_369-380_03-18-20.indd 377
3/19/20 3:03 PM
378
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
STUDY QUESTIONS 1. What events suggest that the current roles of the private and public sectors in the U.S. health care system may be changing? 2. How are technological advances being used in the health care system and what are their impacts? 3. What are the trends in consolidation in the health care system, including the role of for-profit organizations?
REFERENCES American Hospital Association. (2011). AHA environmental scan 2011. Retrieved from http:// www.thefreelibrary.com/AHA+environmental+scan+2011.-a0238750180 American Recovery and Reinvestment Act. (2009). Retrieved from http://en.wikipedia.org/ wiki/American_Recovery_and_Reinvestment_Act_of_2009 Andrews, M. (2011). Hospitals offering complementary medical therapies. Kaiser Health News. Retrieved from https://khn.org/news/michelle-andrews-on-hospitals-offering -complementary-medical-therapies/ Avant, D. (2005). Privatizing military training. Foreign Policy in Focus, 7(6), 1–4. Retrieved from https://fpif.org/privatizing_military_training/ Blackwater USA. (2007). Blackwater. Retrieved from www.blackwaterusa.com Blumenthal, D., & Chopra, A. (2018). Apple’s pact with 13 health care systems might actually disrupt the industry. Harvard Business Review. Retrieved from https://hbr.org/2018/03/ apples-pact-with-13-health-care-systems-might-actually-disrupt-the-industry Blumenthal, D., & Squires, D. (2015). 2015: The health care year in review. The Commonwealth Fund Blog. Retrieved from http://www.commonwealthfund.org/publications/ blog/2015/dec/2015-health-care-in-review Centers for Medicare & Medicaid Services. (2015). Consumer operated and oriented plan program. Retrieved from https://www.cms.gov/CCIIO/Programs-and-Initiatives/Insurance -Programs/Consumer-Operated-and-Oriented-Plan-Program.html Christensen, C. M., Waldeck, A., & Fogg, R. (2017). The innovation health care really needs: Help people manage their own health. Harvard Business Review. Retrieved from https:// hbr.org/2017/10/the-innovation-health-care-really-needs-help-people-manage-their -own-health Emmerton, L., Fejzic, J., & Tett, S. E. (2012). Consumers’ experiences and values in conventional and alternative medicine paradigms: A problem detection study (PDS). BMC Complementary and Alternative Medicine. Retrieved from https://www.ncbi.nlm.nih.gov/ pmc/articles/PMC3349512/ Goldsteen, R. L., Goldsteen, K., Kronenfeld, J. J., & Hann, N. (1997). Anti-government sentiment and support for public health goals: Are they compatible? American Journal of Public Health, 87(1), 25–28. doi: 10.2105/ajph.87.1.25 Herszenhorn, D. M., & Pear, R. (2015, December 15). House reaches accord on spending and tax cuts. The New York Times, Politics. Retrieved from http://www.nytimes .com/2015/12/16/us/politics/congress-9-11-emergency-workers-zadroga-act.html Kaiser Family Foundation. (2010). The Republican ‘pledge’ on health care. Kaiser Health News. Retrieved from https://khn.org/news/text-republican-health-care-document/
Goldsteen74024_12_CH12_369-380_03-18-20.indd 378
3/19/20 3:03 PM
12
■
Tre n d s i n t h e U. S. H e a l t h C a re S y s t e m
379
Kaiser Family Foundation. (2013, April 25). Summary of the Affordable Care Act. Retrieved from https://www.kff.org/health-reform/fact-sheet/summary-of-the-affordable-care-act/ Krugman, P. (2007, January 5). First, do less harm. The New York Times, Opinion pages. Retrieved from http://www.nytimes.com/2007/01/05/opinion/05krugman.html Lipschutz, D. (2019, October 10). Analysis of President Trumps Medicare executive order: Among vague language and proposals, real harm to Medicare beneficiaries. Center for Medicare Advocacy. Retrieved from https://www.medicareadvocacy.org/ analysis-of-president-trumps-medicare-executive-order/ Mayer, J. (2016). Dark money. New York, NY: Anchor Books. Nahin, R. L., Barnes, P. M., & Stussman, B. J. (2016). Expenditures on complementary health approaches: United States, 2012 (National Health Statistics Reports). Hyattsville, MD: National Center for Health Statistics. Retrieved from https://www.ncbi.nlm.nih.gov/ pubmed/27352222 Patel, Y. M., & Guterman, S. (2017). The evolution of private plans in Medicare. The Commonwealth Fund. Retrieved from https://www.commonwealthfund.org/publications/ issue-briefs/2017/dec/evolution-private-plans-medicare Pellegrino, E. D. (1999). The commodification of medical and health care: The moral consequences of a paradigm shift from a professional to a market ethic. Journal of Medicine and Philosophy, 24(3), 243–266. doi: 10.1076/jmep.24.3.243.2523 Sirois, F. M., & Purc-Stephenson, R. J. (2008). Personality and consultations with complementary and alternative medicine practitioners: A five-factor model investigation of the degree of use and motives. Journal of Alternative and Complementary Medicine, 14(9), 1151–1158. doi: 10.1089/acm.2007.0801 Sullivan, T. (2018). Apple health exec says hospitals are at a convergence point. Healthcare IT News. Retrieved from https://www.healthcareitnews.com/news/apple-health -exec-says-hospitals-are-convergence-point Tea Party Patriots. (2020). Our core principles. Retrieved from https://www.teapartypatriots .org/ourvision/ U.S. Department of Health and Human Services. (2017, November). Individuals’ right under HIPAA to access their health information 45 CFR § 164.524. Retrieved from https://www.hhs .gov/hipaa/for-professionals/privacy/guidance/access/index.html#newlyreleasedfaqs U.S. Department of Health and Human Services. (2000, December). Summary of the HIPAA privacy rule. Retrieved from https://www.hhs.gov/hipaa/for-professionals/privacy/laws -regulations/index.html
FURTHER READING Kaveny, M. C. (1999). Commodifying the polyvalent good of health care. Journal of Medicine and Philosophy, 24(3), 207–223. doi: 10.1076/jmep.24.3.207.2528 Kim, M. (2011). The effect of hospital price transparency in health care markets (Dissertation, University of Pennsylvania). Retrieved from https://repository.upenn.edu/dissertations/ AAI3475926/ LaPointe, J. (2018). CMS finalizes hospital price transparency rules, 3% payment boost. Revcycle Intelligence: xtelligent Healthcare Media. Retrieved from https://revcycleintelligence .com/news/cms-finalizes-hospital-price-transparency-rules-3-payment-boost
Goldsteen74024_12_CH12_369-380_03-18-20.indd 379
3/19/20 3:03 PM
380
II
■
U. S. H e a l t h C a re S y s t e m i n Tra n s i t i o n : H o w We G o t H e re a n d W h e re We A re G o i n g
McAneny, B. L. (2019, May 8). AMA: Trump administration requiring pricing information in TV drug ads. AMA Statements. Retrieved from https://www.ama-assn.org/presscenter/ama-statements/ama-trump-administration-requiring-pricing-information-tv -drug-ads Trump, D. J. (2017). Presidential executive order promoting healthcare choice and competition across the United States. Retrieved from https://www.whitehouse.gov/presidential-actions/ presidential-executive-order-promoting-healthcare-choice-competition-across-united -states/ Trump, D. J. (2019). Executive order on improving price and quality transparency in American healthcare to put patients first. Retrieved from https://www.whitehouse.gov/presidential -actions/executive-order-improving-price-quality-transparency-american-healthcare -put-patients-first/
Goldsteen74024_12_CH12_369-380_03-18-20.indd 380
3/19/20 3:03 PM
Index AACN. See American Association of Colleges of Nursing AALL. See American Association for Labor Legislation AAMC. See Association of American Medical Colleges Abbreviated New Drug Application (ANDA), 130, 135 ABFM. See American Board of Family Medicine ABIM. See American Board of Internal Medicine ABP. See American Board of Pediatrics ACA. See Affordable Care Act Accreditation Council for Graduate Medical Education (ACGME), 89–90, 115 ACEP. See American College of Emergency Physicians ACGME. See Accreditation Council for Graduate Medical Education ACS. See American Community Survey active pharmaceutical ingredient (API), 126 ADEs. See adverse drug events adverse drug events (ADEs), 231, 237 AFDC. See Aid to Families with Dependent Children Affordable Care Act (ACA), 25, 41–42, 50, 193, 197–199, 205, 230, 246–249, 251, 278, 329 data sources, 360–362 federal poverty guidelines, 2017, 352 finance, 348–349 goals, 346–348 government sources, 360–361 gross domestic product (GDP), 344, 345 health care costs, 1960 to 2009, 343 limitations, 351–352 Obama administration, 342–352 overview, 342 problems that motivated change, 342–343 reduction of uncompensated care, 350–351 “repeal and replace” efforts by Republicans, 352–359 American Health Care Act, 353 Better Care Reconciliation Act, 354
Goldsteen74024_13_IDX_381-390_03-18-20.indd 381
cost-sharing reductions, 356 end of ACA, 354–355 exchanges and Medicaid expansion, 355–356 executive actions, Trump Administration, 355–356 federal legislation, Trump Administration, 356–358 Health Care Reform Going Forward, 358–359 legal actions and challenges, 357–358 objections to the ACA, 352–353 quality of health plans, 356 spending cuts, 2013 to 2022, 348 status at the end of the Obama administration, 350 support among citizens, 350 Supreme Court challenges, 349–350 U.S. Health Care System, 1927–2005, 361–362 Agency for Healthcare Research and Quality (AHRQ), 60–61, 180, 230–231, 235, 243, 248, 255–256 AHA. See American Hospital Association AHCA. See American Health Care Act AHRQ. See Agency for Healthcare Research and Quality Aid to Families with Dependent Children (AFDC), 199 allopathic physician (MD), 88, 89 AMA. See American Medical Association ambulatory care, 36–37 emergency department, 38–44 industrial and other workplace health clinics, 50–51 neighborhood and community health centers, 49–50 outpatient departments, hospital, 45–48 physician home visits, 51 physician offices, 37–38 public health clinics, 48–49 retail pharmacies, 51–52 school health clinics, 51
3/19/20 8:48 AM
382
Index
ambulatory care (cont.) surgery centers, 52–53 telehealth/telemedicine, 51 ambulatory surgery centers (ASCs), 33, 37, 52–53 American Academy of Physician Assistants (AAPA), 108 PA definition, 109 American Association for Labor Legislation (AALL), 301, 319 American Association of Colleges of Nursing (AACN), 103, 107–108, 115 American Board of Family Medicine (ABFM), 94 American Board of Internal Medicine (ABIM), 94 American Board of Pediatrics (ABP), 94 American College of Emergency Physicians (ACEP), 41 American Community Survey (ACS), 26 American Health Care Act (AHCA), 353–354, 358, 362 American Heart Association, 21 American Hospital Association (AHA), 54, 56, 107, 298, 302, 309 classification of hospitals, 55 American Housing Survey, 26 American Lung Association, 8 American Medical Association (AMA), 21, 86, 298, 304, 320–326, 329, 334 Physician Practice Benchmark Survey, 91 Principles of Medical Ethics, 80 American Nurses Association (ANA), 21, 101, 115 nursing, definition, 100–101 American Osteopathic Association (AOA), 88, 115 American Public Health Association (APHA), 21 ANA. See American Nurses Association ANDA. See Abbreviated New Drug Application AOA. See American Osteopathic Association APHA. See American Public Health Association APIC. See Association for Professionals in Infection Control and Epidemiology associates degree in nursing (ADN), 102 Association for Professionals in Infection Control and Epidemiology (APIC), 242 Association of American Medical Colleges (AAMC), 22, 85–86, 115
bachelor’s degree in nursing (BSN), 102 Balanced Budget Act (BBA), 97, 204 BBA. See Balanced Budget Act BCRA. See Better Care Reconciliation Act of 2017 Behavioral Risk Factor Surveillance System (BRFSS), 25, 256 Better Care Reconciliation Act of 2017 (BCRA), 354, 358, 362
Goldsteen74024_13_IDX_381-390_03-18-20.indd 382
BHPr. See Bureau of Health Professions (BHPr) biologics license application (BLA), 129 Biologics Price Competition and Innovation Act of 2009, 128, 130 BLA. See biologics license application BRFSS. See Behavioral Risk Factor Surveillance System BSN. See bachelor’s degree in nursing Bureau of Health Professions (BHPr), 97 Bureau of Labor Statistics (BLS), 81 categories of health care workers, 81
CAHPS. See Consumer Assessment of Healthcare Providers and Systems CAM. See complementary and alternative medicine Catheter-Associated Urinary Tract Infection (CAUTI), 243–246 CAUTI. See Catheter-Associated Urinary Tract Infection CBO. See Congressional Budget Office CCMC. See Committee on the Costs of Medical Care CCRCs. See Continuing Care Retirement Communities CCS. See Clinical Classification Software CCSQ. See Center for Clinical Standards and Quality CDC. See Centers for Disease Control and Prevention Center for Clinical Standards and Quality (CCSQ), 230 Center for Improvement in Healthcare Quality (CIHQ), 234 Center for Medicare Innovation (CMI), 230 Centers for Disease Control and Prevention (CDC), 180, 219, 231–232, 234–235, 240–245, 254, 256, 259–260, 263, 295 Centers for Medicare & Medicaid Services (CMS), 94, 131–132, 226–237, 241–245, 254–256, 262, 301, 347, 358, 371–372 major provider types, 34 Central Line-associated Bloodstream Infections (CLABSI), 243–245 CfCs. See Conditions for Coverage CHCs. See community health centers Children’s Health Insurance Program (CHIP), 37, 42–43, 46, 199, 282, 300–301, 311, 329, 342, 346, 350–351, 355, 370 CHIP. See Children’s Health Insurance Program CHS. See Community Health Systems CIHQ. See Center for Improvement in Healthcare Quality
3/19/20 8:48 AM
Index
CLABSI. See Central Line-associated Bloodstream Infections Clinical Classification Software (CCS), 61, 63 CMI. See Center for Medicare Innovation CMS. See Centers for Medicare & Medicaid Services Commission on Collegiate Nursing Education (CCNE), 103 Committee on the Costs of Medical Care (CCMC), 276, 322, 327, 329 community-based care ambulatory care, 36–37 community hospitals, 57–58 health conditions treatment, 60–64 hospital structure, 64 inpatient acute care, hospitals, 53–57 medical staff organization, 64–65 most common diseases, 61–64 organization of hospitals, 64 other divisions, 65 public general hospitals, 59–60 rural hospital, 59 self-care, 35–36 teaching hospitals, 59 community health centers (CHCs), 33–34, 49–50, 53 Community Health Systems (CHS), 373 community-oriented primary care (COPC), 111 complementary and alternative medicine (CAM), 375 Comprehensive Hospital Infections Project, 240 comprehensive reform 1900 to 2010 Clinton administration, 325–330 data sources, 331–333 from 1927 to 2005, 332–333 government sources, 331–332 Health Security Act, 326–330 National Health Insurance, 320–325 contract, or the personal health care system, 325 New Deal and post-war proposals, 322–323 proposals in the 1980s, 324–325 proposals in the 1960s and 1970s, 324 Opposition to the Health Security Act, 328–329 overview, 319–320 Political Context of the Health Security Act, 326 Conditions for Coverage (CfCs), 232 Conditions of Participation (CoPs), 232 Congressional Budget Office (CBO), 348–349 Consumer Assessment of Healthcare Providers and Systems (CAHPS), 231, 234, 256 Consumer Operated and Oriented Plan Program (CO-OP), 371–372
Goldsteen74024_13_IDX_381-390_03-18-20.indd 383
383
Consumer Operated and Oriented Plans (CO-OPs), 371–372 Continuing Care Retirement Communities (CCRCs), 67 Controlled Substance Act (CSA), 129 CO-OP. See Consumer Operated and Oriented Plan Program Co-operation and Development (OECD), 180 CO-OPs. See Consumer Operated and Oriented Plans COPC. See community-oriented primary care CoPs. See Conditions of Participation CSA. See Controlled Substance Act
DALYs. See disability-adjusted life years delivery system. See also community-based care categories of settings, 33–34 hospital emergency departments, 38–44 vertical and horizontal integration, 34–35 Department of Health and Human Services (HHS), 357–358 DHQP. See Division of Healthcare Quality Promotion diagnosis related group (DRG), 190–191 disability-adjusted life years (DALYs), 219 Division of Healthcare Quality Promotion (DHQP), 232, 241–242 Doctor of Medicine (MD), 90 Doctor of Osteopathy (DO), 90 DO. See Doctor of Osteopathy DRG. See diagnosis related group
eCQM. See electronic clinical quality measure EHB. See essential health benefits EHRs. See electronic health records EIP. See Emerging Infections Program electronic clinical quality measure (eCQM), 257–258 electronic health records (EHRs), 255, 257, 261 emergency departments (EDs), 36, 38–44 Emergency Medical Treatment and Labor Act (EMTALA), 301–302 Emergency Nurses Association (ENA), 41 emerging biopharma (EBP), 133–134 Emerging Infections Program (EIP), 241–242 Employee Retirement Income Security Act (ERISA), 195 employer-sponsored insurance (ESI), 342–347, 351, 353 EMTALA. See Emergency Medical Treatment and Labor Act ENA. See Emergency Nurses Association
3/19/20 8:48 AM
384
Index
end-stage renal disease (ESRD), 228–230, 239 Environmental Protection Agency (EPA), 6, 21 EPA. See Environmental Protection Agency ESI. See employer-sponsored insurance ESRD. See end-stage renal disease essential health benefits (EHB), 346, 355–356, 359
FDA. See Food and Drug Administration FDC Act, 129 Federally Qualified Health Centers (FQHC), 19 federal poverty level (FPL), 346–347, 351–352 finance basics, 170 capitation, 191 Children’s Health Insurance Program (CHIP or CHIP), 204 consumption and investment, 175–181 cost/cost-plus, 189 fee-for-service, 190 fixed price, 190–191 GoFundMe campaigns, 204 increase in expenditure, reasons for, 204–205 information sources, 170–171 insurance, 181–184 intermediaries, 181–184 managed care, 194–197 Medicaid, 198–204 Medicare, 198–199 network of providers, 188 other government programs, 204 payment modes, 189–192 price and provider expertise, 188–189 private household budget, 193–194 provider and patient payment approaches, 184–188 risk transfer, 192–193 self-pay and out-of-pocket expenditures, 197–198 spending, 171–175 third parties, 181–184 time and materials, 189–190 value-based compensation, 192 Food & Drug Administration (FDA), 126–127, 225, 376 combination products, 141 Current Good Manufacturing Practice (CGMP) regulations, 134 New Drug Application (NDA), 127–130 FPL. See federal poverty level FQHC. See Federally Qualified Health Centers full-time equivalent (FTE) physicians, 97
Goldsteen74024_13_IDX_381-390_03-18-20.indd 384
GDP. See gross domestic product generally regarded as safe and effective (GRAS/E or GRASE), 127–128 governmental authority. See also specific authorities Agency for Healthcare Research and Quality (AHRQ), 154 Animal and Plant Health Inspection Service (APHIS), 160 Centers for Disease Control and Prevention (CDC), 154–156 Centers for Medicare & Medicaid Services (CMS), 158 Children’s Health Insurance Program (CHIP), 158 community health services, 152–153 constitutional basis, 150–151 Department of Health and Human Services (DHSS), 153–154 Department of Veterans Affairs (VA), 158–159 Environmental Protection Agency, 160–161 executive branch, 152 federal agencies, 153–161 Food and Drug Administration (FDA), 156 Food and Nutrition Service (FNS), 160 Food Safety Inspection Service (FSIS), 160 health care financing, 153 Health Resources and Services Administration (HRSA), 156–157 health statistics, 161 judiciary, 152 legislative branch, 150–151 licensing, 161 local health department (LHD), 162–163 National Institute for Occupational Safety and Health (NIOSH), 160 National Institutes of Health (NIH), 157 Occupational Safety and Health Administration (OSHA), 160 personal health services, 152 public health contributions, 163 Rural Utilities Service (RUS), 160 Substance Abuse and Mental Health Services Administration (SAMHSA), 157 U.S. Department of Agriculture (USDA), 160 Women, Infants, and Children (WIC), 160 Graduate Medical Education (GME), 88–90 gross domestic product (GDP), 252, 303, 342–344 group purchasing organization [GPO], 132, 139
HAIs. See healthcare-associated infections HALE. See health-adjusted life expectancy
3/19/20 8:48 AM
Index
HCAHPS. See Hospital Consumer Assessment of Healthcare Providers and Systems Survey HCE. See health consumption expenditures HCFA. See Health Care Financing Administration HCUP. See Healthcare Cost and Utilization Project health-adjusted life expectancy (HALE), 343 health behaviors, 14 health care, categories, 9–10 healthcare-associated infections (HAIs), 215, 231, 238–239, 241–246 Healthcare Cost and Utilization Project (HCUP), 60, 231, 256, 264 Healthcare Effectiveness Data and Information Set (HEDIS), 234 Healthcare Facilities Accreditation Program (HFAP), 234 Healthcare Financing Administration, (HCFA), 228, 254 Healthcare Infection Control Practices Advisory Committee (HICPAC), 232, 241–242 healthcare issues age structures, 17 diabetes, 16 heart disease and cancer, 15 income disparities, 17 obesity, 17 prevalence of functional limitation, 13 health care providers complexity, 86–87 demographic characteristics, 84–86 physicians, 87–99 practice settings, 80, 84 practitioner and technical occupations, 81–82 wages, 82–84 health care systems. See also specific systems efficiency, 23 equity, 23 facilities, 19 financing, 22 government’s role, 20–21 key components, 18 medical products, 19–20 nongovernmental organizations’ role, 21–22 primary, secondary, and tertiary, 24 quality, 23–24 special populations and diseases, 24–25 workforce, 19 health consumption expenditures (HCE), 171, 175 health, determinants, 5–8 behavioral determinants, 9, 14 genetic inheritance, 6
Goldsteen74024_13_IDX_381-390_03-18-20.indd 385
385
health care as, 8 physical environment, 6 social environment, 6–7 health information exchange (HIE), 257–259 Health Information Technology for Economic and Clinical Health (HITECH), 375 health information technology (HIT), 254, 257– 258, 259, 261 health insurance plans (HIPs), 299 Health Insurance Portability and Accountability Act (HIPAA), 301–302, 375 Health Maintenance Organization Act (HMO), 305–306, 308 health maintenance organizations (HMOs), 39, 65, 297, 305–306, 308, 311, 313 Health Outcomes Survey (HOS), 230, 234 health professional shortage areas (HPSAs), 90, 98 Health Resources and Services Administration (HRSA), 235 health savings accounts (HSAs), 193 health services, types, 23–25 healthy life expectancy (HALE), 219, 221, 263 HEDIS. See Healthcare Effectiveness Data and Information Set HFAP. See Healthcare Facilities Accreditation Program HHCAHPS. See Home Health CAHPS HHQI. See Home Health QI HHS. See Department of Health and Human Services HHS. See U.S. Department of Health and Human Services HICPAC. See Healthcare Infection Control Practices Advisory Committee HICPAC. See Healthcare Infection Control Practices Advisory Committee HIE. See health information exchange HIPAA. See health Insurance Portability and Accountability Act HIPs. See health insurance plans HIT. See Health information technology HITECH. See Health Information Technology for Economic and Clinical Health HMO. See Health Maintenance Organization Act HMOs. See health maintenance organizations Home Health CAHPS (HHCAHPS), 256 Home Health QI (HHQI), 229 HOS. See Health Outcomes Survey Hospital Consumer Assessment of Healthcare Providers and Systems Survey (HCAHPS), 255–256, 262 Hospital QI (HQI), 229 HQI. See Hospital QI
3/19/20 8:48 AM
386
Index
HRSA. See Health Resources and Services Administration HSS. See U.S. Department of Health and Human Services
ICD. See International Classification of Diseases IDSs. See integrated delivery systems IHI. See Institute for Healthcare Improvement implantable medical device (IMD), 138 IMS. See Indicator Measurement System incrementalism 1900 to 2010 building hospitals, 302 capitation and rise of managed care, 303–308 health maintenance organizations, 305–306 managed care, 306–308 prepaid group medical practice, 304–305 data sources, 311–313 employer-based health insurance, 299–300 EMTALA and HIPAA, 301–302 from 1927 to 2005, 312–313 government-funded community hospitals, 303 government sources, 311–312 health care access, 298–303 health care organizations for-profit, 310–311 vertical and horizontal integration, 308–310 health insurance to the unemployed, 300–301 organization and financing, 303–311 overview, 298 providing health insurance, 299 public hospitals, 302 voluntary, nonprofit hospitals, 302 Independent Physician Association (IPA), 306 indicator measurement system (IMS), 233 inpatient acute care, hospitals historical background, 53–54 modern settings, 54–57 Institute for Healthcare Improvement (IHI), 234, 236–237, 245 Institute of Medicine (IOM), 102, 137, 222, 224, 238–239, 246, 328, 330, 332 integrated delivery systems (IDSs), 297, 309 International Classification of Diseases (ICD), 298 ICD-10, 180 IOM. See Institute of Medicine IPA. See Independent Physician Association IQVIA, 134, 142
JCAHO. See Joint Commission on Accreditation of Healthcare Organizations Joint Commission on Accreditation of Healthcare Organizations (JCAHO), 232–233, 301
Goldsteen74024_13_IDX_381-390_03-18-20.indd 386
Kaiser Family Foundation (KFF), 206 KFF. See Kaiser Family Foundation LCME. See Liaison Committee on Medical Education length of stay (LOS), 55, 57–58 LHDs. See local health departments Liaison Committee on Medical Education (LCME), 88–89, 115 Linked Birth and Infant Death Data (NVSS-L), 256 local health departments (LHDs), 48–49 long-term care acute hospitals (LTCAHs), 66 LOS. See length of stay LTCAHs. See long-term care acute hospitals MA. See Medicare Advantage MACRA. See Medicare Access and CHIP Reauthorization Act of 2015 major in nursing (MA), 103 managed care organizations (MCOs), 65, 111, 194, 198 master of nursing degree (MN), 103 master’s degree in nursing (MSN), 103 Medicaid, 34 exchanges and expansion, 355–356 finance, 198, 204 medical degree (MD or DO), 97 medical devices apps ad, 141 buyers, 138–139 categories, 136 challenges, 141 company/market structure, 140–141 components, 126 MedPAC, 139 regulatory process, 135–137 Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), 352 Medical Expenditure Panel Survey (MEPS), 230, 256, 262 Medicare, 34 Medicare Advantage (MA), 230, 358–359 Medicare Payment Advisory Commission (MedPAC), 135–136, 142 Medicare Prescription Drug, Improvement, and Modernization Act (MMA), 198, 372 Medicare Severity Diagnosis Related Group (MS-DRG), 190–191 Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), 352 MEPS. See Medical Expenditure Panel Survey Merit-Based Incentive Payment System (MIPS), 352
3/19/20 8:48 AM
Index
methicillin-resistant Staphylococcus aureus bacteremia (MRSA), 243–244 MIPS. See Merit-Based Incentive Payment System MMA. See Medicare Prescription Drug, Improvement, and Modernization Act morbidity, 13–14 mortality, 10–13 Mortality Data (NVSS-M), 256 MRSA. See methicillin-resistant Staphylococcus aureus bacteremia
NAMCS. See National Ambulatory Medical Care survey NARA. See National Archives and Records Administration Natality Data (NVSS-N), 256 National Ambulatory Medical Care survey (NAMCS), 71, 256 National Archives and Records Administration (NARA), 290, 332, 361 National Center for Complementary and Integrative Health (NCCIH), 375 National Center for Health Statistics (NCHS), 97, 219, 256, 262, 295, 305–306 National Committee for Quality Assurance (NCQA), 230, 233–235, 257–258 National Evaluation System for health Technology (NEST), 137 National Health and Nutrition Examination Survey (NHANES), 16–17, 26, 256 national healthcare expenditure (NHE), 282 National Healthcare Safety Network (NHSN), 241–245, 259–261 National Health Expenditure Accounts (NHEA), 170–171 National Health Expenditure (NHE), 22 National Health Insurance (NHI), 319, 322–326, 331, 333–334 National Health Interview Survey (NHIS), 26 National Hospital Ambulatory Medical Care Survey (NHAMCS), 256 National Institutes of Health (NIH), 232, 282, 294 National League of Nursing Accrediting Commission (NLNAC), 103 National Nosocomial Infections Surveillance System (NNISS), 241 National Quality Forum (NQF), 229, 234–236, 243, 254 National Quality Strategy (NQS), 229 National Study of Long-Term Care Providers (NSLCP), 71 National Vital Statistics System (NVSS), 25, 256, 263
Goldsteen74024_13_IDX_381-390_03-18-20.indd 387
387
NCCIH. See National Center for Complementary and Integrative Health NCHS. See National Center for Health Statistics NCQA. See National Committee for Quality Assurance Nebraska Health Information Initiative (NHII), 257–258 neighborhood health center (NHC), 36, 49–50 NEST. See National Evaluation System for health Technology NHAMCS. See National Hospital Ambulatory Medical Care Survey NHANES. See National Health and Nutrition Examination Survey NHE. See national healthcare expenditure NHI. See National Health Insurance NHII. See Nebraska Health Information Initiative NHIS. See National Health Interview Survey NHQI. See Nursing Home QI NHSN. See National Healthcare Safety Network NIH. See National Institutes of Health NLNAC. See National League of Nursing Accrediting Commission NNISS. See National Nosocomial Infections Surveillance System nonprescription or “over-the-counter” (OTC) medicines, 36 NQF. See National Quality Forum NQS. See National Quality Strategy NSLCP. See National Study of Long-Term Care Providers nurses advanced degree nurses, 103 advanced practice degree nurses, 103–104 challenges, 105–106 demography, 98 education, 102 historical background, 99–100 practice settings, 104–105 registered nurses (RN), 102–103 roles and responsibilities, 100–102 supply model, 106–108 Nursing Home QI (NHQI), 229 Nursing Practice Act of New York State, 100 NVSS. See National Vital Statistics System NVSS-L. See Linked Birth and Infant Death Data NVSS-M. See Mortality Data NVSS-N. See Natality Data
OASH. See Office of the Assistant Secretary for Health Occupational Employment Statistics (OES), 81
3/19/20 8:48 AM
388
Index
Occupational Safety and Health Administration (OSHA), 21 OECD. See Organization for Economic Cooperation and Development OES. See Occupational Employment Statistics Office of Economic Opportunity (OEO), 49 Office of the Assistant Secretary for Health (OASH), 243 Organization for Economic Co-operation and Development (OECD), 180, 219–221, 262, 285–286, 343–345 OSHA. See Occupational Safety and Health Administration over-the-counter (OTC) drugs, 126–129, 131, 133
Patient-Centered Outcomes Research Institute (PCORI), 237 Patient Protection and Affordable Care Act (PPACA), 342 PBMs. See Pharmacy Benefit Managers PCORI. See Patient-Centered Outcomes Research Institute PCPI. See Physician Consortium for Performance Improvement PDPs. See prescription drug plans performance acute care hospitalization, 229, 245 administrative data, 256 administrative records, 254–255 adverse clinical outcomes, 223 advocacy organizations, 238 Agency for Healthcare Research and Quality, 230–231, 262 billing claim forms, 254 CDC units, 231–232, 241, 262–263 Centers for Medicare & Medicaid Services, 228–229, 234, 262 clinical outcomes, 222–224, 262 consumer assessment, 255–256 data and information technology, 253–263 device-associated module, 260 electronic health record (EHR), 255, 257 enrollment files, 255 equity in health care, 246–249 access, 247–248 before and after the ACA, 246, 248 quality, 246–247 uninsured rates nonelderly individuals by race and ethnicity, 2013 to 2017, 249 federal agencies, 227 healthcare-associated infections (HAIs), 232, 238–246 health care efficiency, 249–252
Goldsteen74024_13_IDX_381-390_03-18-20.indd 388
Commonwealth Fund, 2016, 251 macro and micro level, 250–252 Healthcare Professional Associations, 237–238 quality improvement, 2019, 225–227 Health Information Example, 261 health information exchange (HIE), 257–259 health surveys, 255–256 Institute for Healthcare Improvement, 236–237 Joint Commission, 232–233 limitations of population health outcomes, 222 medical records, 255 medication-associated module, 260 National Committee for Quality Assurance, 233–234 National Healthcare Safety Network, 259–261 National Institutes of Health, 232 National Program of Cancer Registries, 256–257 National Quality Forum, 235–236 national scorecard, 252–253 National Vital Statistics System, 256 overview, 216–217 participation, 260 Patient-Centered Outcomes Research Institute, 237 patient safety movement, 238–239 Population Health Outcomes, 218–221, 262 private organizations, 234 procedure-associated module, 260 quality-of-life adjusted measures, 221 surveillance and data collection, 260 systematic review, 224–225 United States compared with other countries, 219–220 personal health care system (PHCS), 171, 175, 325, 327 pharmaceuticals biological products, 126–127 innovative and generics companies, 134–135 OTC drugs, 131 regulatory process, 127–131 retail setting, 132 U.S. market, 132–134 Pharmacy Benefit Managers (PBMs), 131–132 PHCS. See personal health care system PHO. See physician–hospital organization PHS Act. See Public Health Service (PHS) Act physician assistants, 108–109 Physician Consortium for Performance Improvement (PCPI), 235 physician–hospital organization (PHO), 65 physician preference items (PPI), 139
3/19/20 8:48 AM
Index
physicians demography, 87 graduate, 89–90 historical background, 87–88 hospitalist, 93–94 influencing factors, 95 licensure, 90 medical education, 88 ownership or salaried position, 91 practice issue, 94 primary care or other specialty, 92–93 solo or group practice, 91–92 supply model, 97–99 undergraduate, 88–89 workforce projections, 95–97 Physician Supply Model (PSM), 97 PMCs. See private military companies Point of Service (POS), 306 POS. See Point of Service post-acute care, 66 long-term, 66–70 PPACA. See Patient Protection and Affordable Care Act PPGP. See prepaid group practice PPI. See physician preference items PPO. See preferred provider organizations preferred provider organizations (PPO), 306 prepaid group practice (PPGP), 49 prescription drug plans (PDPs), 198 primary care providers, 109–111 delivery system, 113–114 functions, 111–112 historical background, 112 workforce, 113 private military companies (PMCs), 377 Public Health Service (PHS) Act, 128–129 QALYs. See quality-adjusted life years QIOs. See quality improvement organizations QIs. See quality initiatives QMs. See quality measures quality-adjusted life years (QALYs), 219 Quality Improvement Organizations (QIOs), 235 quality initiatives (QIs), 229, 261 quality measures (QMs), 229–230, 233, 236, 244, 257–258 R&D. See research and development Red Cross, The, 21 redefining health care, 192 regional health information organizations (RHIOs), 257 registered nursing (RN), 108 research and development (R&D), 133, 135
Goldsteen74024_13_IDX_381-390_03-18-20.indd 389
389
RHIOs. See regional health information organizations Robert Wood Johnson Foundation, 21
Safety and Healthcare Epidemiology Prevention Research Development (SHEPheRD), 242 SENIC. See Study on the Effectiveness of Nosocomial Infection Control SES. See socioeconomic status SHEA. See Society for Healthcare Epidemiology of America SHEPheRD. See Safety and Healthcare Epidemiology Prevention Research Development SHOP. See Small Business Health Options Program short-term, limited duration insurance (STLDI), 356–357 SIS. See Surgical Infection Society Small Business Health Options Program (SHOP), 346, 355, 370 Social Security Act, 198 Society for Healthcare Epidemiology of America (SHEA), 242 Society of Hospital Medicine, 94 socioeconomic status (SES), 246–247 SPC. See Statistical Process Control SSI. See Surgical Site Infection Statistical Process Control (SPC), 238 STLDI. See short-term, limited duration insurance structure, 290–291 affecting factors, 287 checks and balances, 283 context, 287 debates, 275–295 economic principles, 288–289 government sources, 290 historical roots, 281–282 ideology, 278–281 mixed and, 281–283 mixed enterprise, 284–285 overview, 276–278 policy making, 283–285, 286–289 pragmatism, 282–283 private good, 278, 279–280 private or public involvement, 287 public good, 278–279 public or private enterprise?, 280–281 specific proposals, 286 trade-offs, 283 U.S. from 1763 to 2015, 294–295 U.S. from 1927–2005, 290–291 U.S. compared to peer countries, 285–286
3/19/20 8:48 AM
390
Index
Study on the Effectiveness of Nosocomial Infection Control (SENIC), 240–245 Surgical Infection Society (SIS), 242 Surgical Site Infection (SSI), 243–246
total quality management (TQM), 238 TQM. See total quality management
UN. See United Nations United Nations (UN), 278–279 U.S. Department of Health and Human Services (DHHS), 170, 231–232, 239, 243, 257 U.S. Health Care System. See also comprehensive reform 1900 to 2010 Big Data and health information, 373 comparison to other nations, 5 complementary medicine, 375 consolidation, 373 consumerism, 375 cost of prescription drugs under scrutiny, 374 current state of policy, 369–372 from 1927–2005, 361–362 hospital versus ambulatory care, 374–375 incrementalism 1900 to 2010, 298–313 new technology, 374 patient access to medical records, 375–376 prevention and mental health, 374 trends, 371–376 zigzag theory, 370–372, 376–377
Goldsteen74024_13_IDX_381-390_03-18-20.indd 390
U.S. International Trade Association (ITA), 132 U.S. population, 10 health needs, 18 racial diversities, 16 special care programs, 24
VAE. See Ventilator-Associated Events Ventilator-Associated Events (VAE), 243–244 Veterans Affairs (VA), 204
Web-based Injury Statistics Query and Reporting System (WISQARS), 262 Welfare Reform Act, 199 WHO. See World Health Organization WISQARS. See Web-based Injury Statistics Query and Reporting System World Health Organization (WHO), 37, 218–219, 221, 262, 295 definition, health, 5
years of healthy life (YHL), 219 years of potential life lost (YPLL), 219–220 YHL. See years of healthy life YPLL. See years of potential life lost
zigzag theory, 370–372, 376–377
3/19/20 8:48 AM