Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II (Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application) 9819955017, 9789819955015
This book continues the discussion from Volume I on the risks organizations face in order to succeed with a special focu
158 29 6MB
English Pages 268 [256] Year 2023
Acknowledgments
ISBN
Contents
Editor and Contributors
List of Figures
List of Charts
List of Tables
Part I Introduction Chapter
1 Introduction: “Sectoral Fraud Tree” for Better Understanding Fraud Science—Trial Fraud Tree for Health Sector
1.1 Introduction
1.2 New Recommendation for Fraud Prevention: Sectoral Fraud Tree
1.3 Discussion
References
Part II Managerial Issues in Health Sector
2 Marketing in the Health Sector
2.1 Introduction
2.2 Services
2.2.1 Definition and Context
2.2.2 Characteristics of Services
2.3 Health Services Marketing
2.3.1 The Marketing Mix of the Health Services
2.4 Conclusion
References
3 A Model Proposal for Solutions to the Problems Faced by Small and Mediums in the COVID-19 Process
3.1 Introduction
3.2 SME Definition
3.2.1 SMEs in the World and Turkey
3.2.2 COVID-19 Pandemic
3.2.3 Pandemic Concept
3.3 Announcement of COVID-19 Pandemic Process and WHO’s Targets
3.4 Effects of the Pandemic on SMEs
3.5 Research Method, Findings, and Model Proposal
3.5.1 Research Type
3.5.2 Research Purpose
3.5.3 Research Importance
3.5.4 Research Population and Sample
3.5.5 Research Questions
3.5.6 Aggregation of Research Data
3.5.7 Analyzing Research Data
3.5.8 Results
3.6 Model Proposal
3.7 Conclusion and Recommendations
References
4 Taxation of Healthcare Sector in India
4.1 Introduction to the Healthcare Sector in India
4.2 Taxation of Healthcare Sector in India
4.2.1 Individuals Income Tax Rates: Individuals & HUF
4.2.2 Corporate Income Tax Rates
4.3 Income Tax Deduction Available Towards Healthcare
4.3.1 Section 80D: Deduction for Premium Payment Towards Healthcare Insurance Policy When Parents Are Senior Citizen
4.3.2 Deduction in Respect of Payment Towards Preventive Healthcare Check-Up
4.3.3 Deduction in Respect of Expenses Towards Medical Treatment
4.3.4 Deduction for Medical Treatment of a Dependent Person with Disability
4.3.5 Section 80G: Deduction for Donation and Contribution Made
4.3.6 Section 80GGA: Donations Towards Scientific Research or Rural Development
4.4 Indirect Tax—GST—Goods & Services Tax Act 2017
4.4.1 Chargeability of GST on Healthcare Sector
4.5 GST Exemption Available Towards Healthcare Services.
4.6 Tax Incentives and Deductions Available Towards Healthcare Under Income Tax Act 1961
4.7 Conclusions
References
5 Sustainability Based Medical Waste Logistics in Healthcare Enterprises: A University Hospital Application
5.1 Introduction
5.2 Logistics
5.3 Reverse Logistics
5.4 Concept of Waste and Management
5.4.1 Medical Waste Concept and Its Qualities
5.5 Reverse Logistics Process Related to Medical Wastes
5.6 Medical Waste Collection and Disposal Process
5.7 Cost of Medical Waste
5.7.1 Transportation of Medical Wastes in the Health Institution
5.7.2 Temporary Storage of Medical Waste in a Healthcare Organization
5.7.3 Transport of Medical Waste to Processing Facilities
5.8 Medical Wastes Disposal Methods
5.9 Regulations on Management of Medical Wastes
5.10 Duties and Responsibilities
5.10.1 Authority and Duties of the Ministry
5.10.2 Duties and Authorities of Provincial Directorates
5.10.3 Obligations of Municipalities
5.10.4 Obligations of Health Institutions
5.11 Case Study
References
6 Evaluating Working Conditions in Healthcare During COVID-19 Crisis
6.1 Introduction
6.2 Methodology
6.3 Control Variables
6.4 Evaluation of Working Conditions During COVID-19
6.5 Conclusion
References
Part III Economic Issues in Health Sector
7 Fighting Against COVID-19: The Role of Consolidated Fiscal Policies and Transparency in Data Sharing
7.1 Introduction
7.2 Theoretical Background
7.2.1 Budget Transparency
7.2.2 Budgets During Crisis
7.3 Data and Methodology
7.4 Results
7.5 Conclusion
References
8 Investigation of Dyspnea and Quality of Life in Patients with Heart Failure
8.1 Introduction
8.2 Aim
8.2.1 Materials and Method
8.3 Results
8.4 Discussion
8.5 Conclusion
References
9 Ranking eHealth Efforts of Countries to Fight Coronavirus Pandemic via Grey Systems Theory: Evidence from National COVID-19 Mobile Apps
9.1 Introduction
9.2 Conceptual Background
9.3 Materials and Methods
9.3.1 Grey Systems Theory
9.3.2 Grey Relational Analysis
9.3.3 Ranking of COVID-19 Mobile Apps Using Grey Relational Analysis
9.4 Results
9.5 Discussions and Implications
9.6 Conclusion, Limitations, and Future Research
References
10 Informal Health Payments in the SARS-CoV-2 Era: Options from Greece
10.1 Introduction
10.2 Corruption in Healthcare
10.3 Informal Payments in Healthcare
10.4 Informal Payments in Greek Healthcare System
10.5 Conclusions
References
11 Health and Human Welfare: Issues and Challenges Faced and Defeated
11.1 Introduction
11.2 Assessment of Human Development
11.3 Improving the Way Our Welfare System Works
11.4 Challenges in Our Existing Welfare System
11.5 Alternate Models: Overcoming These Challenges
11.6 Improving Health for People in Rural and Regional Areas
11.7 Conclusion
References
12 Evaluation of Pain in the Critical Care Unit Patients Who Had Intubated and Sedated
12.1 Introduction
12.2 Study Design, Settings, and Participants
12.3 Ethical Approval
12.4 Data Collection
12.5 Data Analysis
12.6 Results
12.7 Discussion
12.8 Conclusion
References
13 Corruption in the Health Sector: Case Study of Kosovo
13.1 Introduction
13.2 Corruption in Kosovo
13.3 Corruption in Health Sector
13.4 Methodology and Findings
13.4.1 Demographic Profile of Respondents
13.4.2 Health Services Questions
13.4.3 Perceived Level of Corruption in Health Sector
13.4.4 Reported Level of Corruption
13.5 Results and Recommendations
References
Index
Recommend Papers










- Author / Uploaded
- Kıymet Tunca Çalıyurt (editor)
File loading please wait...
Citation preview
Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application
Kıymet Tunca Çalıyurt Editor
Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II
Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application Series Editor Kıymet Tunca Çalıyurt, Centre for Forensic Accounting Research and Enterprise, School of Finance and Management, SOAS University of London, London, UK
This Scopus indexed series acts as a forum for book publications on current research arising from debates about key topics that have emerged from global economic crises during the past several years. The importance of governance and the will to deal with corruption, fraud, and bad practice, are themes featured in volumes published in the series. These topics are not only of concern to businesses and their investors, but also to governments and supranational organizations, such as the United Nations and the European Union. Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application takes on a distinctive perspective to explore crucial issues that currently have little or no coverage. Thus the series integrates both theoretical developments and practical experiences to feature themes that are topical, or are deemed to become topical within a short time. The series welcomes interdisciplinary research covering the topics of accounting, auditing, governance, and fraud.
Kıymet Tunca Çalıyurt Editor
Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II
Editor Kıymet Tunca Çalıyurt Centre for Forensic Accounting Research and Enterprise, School of Finance and Management SOAS University of London London, UK
ISSN 2509-7873 ISSN 2509-7881 (electronic) Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application ISBN 978-981-99-5501-5 ISBN 978-981-99-5502-2 (eBook) https://doi.org/10.1007/978-981-99-5502-2 © The Editor(s) (if applicable) and The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd. 2023 This work is subject to copyright. All rights are solely and exclusively licensed by the Publisher, whether the whole or part of the material is concerned, specifically the rights of reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. The publisher, the authors, and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, expressed or implied, with respect to the material contained herein or for any errors or omissions that may have been made. The publisher remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. This Springer imprint is published by the registered company Springer Nature Singapore Pte Ltd. The registered company address is: 152 Beach Road, #21-01/04 Gateway East, Singapore 189721, Singapore
Acknowledgments
Some academics are fighting to prevent fraud in the health sector and train new warriors. One of these academics is Prof. Dr. Taryn Vian. I had the opportunity to visit her office in 2016 while she was working at the Boston University School of Public Health; since then, we have been discussing the prevention of cheating in the health sector. Her and co-authors’ book titled Anticorruption in the Health Sector: Strategies for Transparency and Accountability is a reference book for CFEs and students in health and management science. I got three books in my office and at home.
v
vi
Acknowledgments
Acknowledgments
vii
I am fortunate to have Taryn as a friend, and thanks for her special note for me while presenting me in her office at Boston University. I hope she has a long, healthy, and happy life with her family and students. We are looking forward to reading her new research and publications. Prof. Dr. Kıymet Tunca Çalıyurt Book Series Editor Founding President, International Group of Governance Fraud Ethics and ESG June 2023
viii
Acknowledgments
Acknowledgments
ix
As the editorial board of the book series and International Conference on Governance Fraud Ethics and CSR, we would like to dedicate this book to Prof. Dr. Taryn Vian and would like to share her CV. We would like to thank her for fighting against fraud in the health sector. Prof. Dr. Taryn Vian University of San Francisco School of Nursing and Health Professionals https://www.usfca.edu/faculty/taryn-vian
Biography Dr. Taryn Vian is a public health scholar and academic leader whose work is guided by the belief that all people have the right to access quality healthcare without having to experience financial hardship. She is dedicated to practice-based teaching and the development of emerging public health leaders eager to work with communities to address the underlying social determinants of health. Through her research and scholarly work, she has furthered efforts to control corruption in the health sector, advance health systems and access to medicines, and evaluate public-private partnerships and community health initiatives. She has published over 140 articles, book chapters, and professional reports and has served on international technical committees, and advised the World Health Organization, Council of Europe, World Bank, Bill and Melinda Gates Foundation, and other clients.
x
Acknowledgments
Her passion for education inspires her efforts to reform curriculum and pedagogy for health professionals, including initiatives to motivate and engage students in the classroom, collaborate with partner organizations in practice-based teaching, and enhance intentional communities of scholar-teachers through peer review. She is a returned Peace Corps Volunteer from Cameroon and has a Ph.D. in Public Policy and Global Health from Boston University, an M.S. in Health Policy and Management from the Harvard School of Public Health, and a B.A. in Philosophy from Colgate University. Follow her on Twitter @TarynVian.
Expertise • • • •
Global health Public-private partnerships Anti-corruption Health policy and management
Research Areas • Corruption in the health sector • Transparency and good governance • Health systems strengthening
Appointments • Acting Director, Health Policy Leadership Concentration • Co-Director, Community Public Health Practice Concentration • Research Fellow, World Health Organization (WHO) Collaborating Centre for Governance, Accountability and Transparency in the Pharmaceutical Sector. Leslie Dan Faculty of Pharmacy, University of Toronto (January 2020–present) • Clinical Professor of Global Health, Boston University School of Public Health (2016–2019) • Associate Chair, Department of Global Health, Boston University School of Public Health (2015–2018)
Acknowledgments
xi
Education • Ph.D., Public Policy and Global Health, University Professors Program, Boston University • SM, Health Policy and Management, Harvard School of Public Health, Boston • B.A. Colgate University, Philosophy, Hamilton, NY
Awards & Distinctions • Norman A. Scotch Award for Excellence in Teaching, Boston University. 2011 • Alumni Award for Outstanding Doctoral Dissertation, University Professors Program, Boston University. 2010 • Awards for Excellence in Teaching, IH757 Fighting Corruption Through Transparency and Accountability, Boston University School of Public Health, and IH773 Financial Management for Health Programs. 2014 • Best Abstract Award (with co-author Travis DiJoseph), John McCahan Medical Campus Education Day, Boston University. “Pilot test of the General Observation and Reflection Platform (GORP) for measuring the level of activity in classrooms.” 2016
Selected Publications • Vian T, Agnew B., & McInnes DK. (2022). Whistleblowing as an anti-corruption strategy in health and pharmaceutical organizations: A scoping review protocol. Global Health Action, 15(1), Article 2140494. • Scott NA, Kaiser JL, Jack BW, Nkholongo EL, Nash T, Alade M, Vian T. (2022). Observational study of the clinical performance of a Public-Private Partnership national referral hospital network in Lesotho: Do improvements last over time? PLOS ONE, 17(9), e0272568. • Vian T, Kaiser JL, Ngoma T, Juntunen A, Mataka KK, Bwalya M, Sakanga V, Rockers PC, Hamer DH, Biemba G, Scott NA. (2022). Planning for maternity waiting home bed capacity: Lessons from rural Zambia. Annals of Global Health, 88(1), Article 37. • Vian T, Fong R, Kaiser JL, Sakanga V, Mwansa M, Chastain P, Ngoma T, Scott NA. (2020). Using open public meetings and elections to promote inward transparency and accountability: lessons from Zambia. International Journal of Health Policy and Management. • Vian T. (2020). Anti-corruption, transparency and accountability in health: Concepts, frameworks, and approaches. Global Health Action, 13(sup1). Article 1694744.
ISBN
This Is the Official Book Series for the International Group on Governance Fraud Ethics and CSR.
xiii
Contents
Part I 1
Introduction Chapter
Introduction: “Sectoral Fraud Tree” for Better Understanding Fraud Science—Trial Fraud Tree for Health Sector . . . . . . . . . . . . . . Kıymet Tunca Çalıyurt
Part II
Managerial Issues in Health Sector
2
Marketing in the Health Sector . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Esra Demirba¸s
3
A Model Proposal for Solutions to the Problems Faced by Small and Mediums in the COVID-19 Process . . . . . . . . . . . . . . . . . Ahmet Konak and Agah Sinan Ünsar
4
Taxation of Healthcare Sector in India . . . . . . . . . . . . . . . . . . . . . . . . . . Jagbir Singh Kadyan
5
Sustainability Based Medical Waste Logistics in Healthcare Enterprises: A University Hospital Application . . . . . . . . . . . . . . . . . . Kadir Kaan Göncü
6
3
17
37 55
83
Evaluating Working Conditions in Healthcare During COVID-19 Crisis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101 Jamil Kobrossi and Walid Dagher
Part III Economic Issues in Health Sector 7
Fighting Against COVID-19: The Role of Consolidated Fiscal Policies and Transparency in Data Sharing . . . . . . . . . . . . . . . . . . . . . . 115 Görkem Sariyer and Ece Acar
8
Investigation of Dyspnea and Quality of Life in Patients with Heart Failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 129 Eda Ertu˘grul and Serap Ünsar xv
xvi
9
Contents
Ranking eHealth Efforts of Countries to Fight Coronavirus Pandemic via Grey Systems Theory: Evidence from National COVID-19 Mobile Apps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 143 Eyüp Çetin and Hilal Özen
10 Informal Health Payments in the SARS-CoV-2 Era: Options from Greece . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 179 Paraskevi Koufopoulou, Athanassios Vozikis, Kyriakos Souliotis, and Andreas Koutoupis 11 Health and Human Welfare: Issues and Challenges Faced and Defeated . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 191 Usha Pathak 12 Evaluation of Pain in the Critical Care Unit Patients Who Had Intubated and Sedated . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 201 Fatma Güçlü and Serap Ünsar 13 Corruption in the Health Sector: Case Study of Kosovo . . . . . . . . . . . 217 Luan Vardari, Berk Arapi, and Qëndresa Kukaj Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 239
Editor and Contributors
About the Editor Prof. Dr. Kıymet Tunca Çalıyurt (CPA, CFE) graduated from the Faculty of Business Administration at Marmara University, Istanbul, Turkey. Her Master’s and Ph.D. degrees are in Accounting and Finance Programme from the Social Graduate School, Marmara University. She has worked as an auditor at Horwath Auditing Company, a manager at Mcdonald’s, and finance staff at Singapore Airlines before positioning herself in academia. After vast private sector experience, she started working at Trakya University as a Lecturer in 1999. She was a Visiting Researcher at Concordia University, Canada (2001), Amherst Business School, Massachusetts University, USA (2014), and UNWE, Sofia, in 2019. In 2009, she founded the International Group on Governance, Fraud, Ethics and Social Responsibility (IGonGFE&SR) and International Women and Business Group (IWBG), which organizes a global annual conference. She published articles in Web of Science journals like Managerial Auditing Journal, International Journal on Law and Management, Risks and Sustainability. Her book chapters and books nationally and internationally on fraud, social responsibility, and ethics in accounting/finance/aviation disciplines are in Springer and Routledge. She is a book series editor for; – Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application (Springer Nature indexed by Scopus) – Women and Sustainable Business (Routledge) She is acting as an associate or editorial board member in the following titles; – – – –
Journal of Financial Crime (ESCI) International Journal on Law and Management (ESCI) Journal of Money Laundering Control (ESCI) International Journal of Climate Change Strategies and Management (SSCI)
xvii
xviii
Editor and Contributors
She is the founding Chief-in-Editor for the Accounting Finance Auditing: An International Journal. She is an invited speaker at the International Economic Crime Symposium at Jesus College, Cambridge University, and partner of Herme Consulting in Trakya University Technopark.
Contributors Ece Acar Department of Business Administration, Faculty of Business, Yasar University, Izmir, Turkey Berk Arapi Faculty of Medicine, Istanbul University Cerrahpa¸sa, Istanbul, Turkey Kıymet Tunca Çalıyurt Business Administration Department, Faculty of Business Sciences and Economics, Trakya University, Edirne Merkez, Turkey Eyüp Çetin Laboratory for Industrial and Applied Mathematics, York University, Toronto, ON, Canada; New York Business Global, Silver Spring, MD, USA Walid Dagher Issam Fares Faculty of Technology, University of Balamand-Kelhat, El Koura, Lebanon Esra Demirba¸s Istanbul Yeni Yuzyil University, ˙Istanbul, Turkey Eda Ertu˘grul Prof. Dr. Cemil Ta¸sçıo˘glu City Hospital Adult Emergency Clinic, Istanbul, Türkiye Kadir Kaan Göncü Social Vocational College, Trakya Üniversitesi, Edirne Merkez, Turkey Fatma Güçlü Murat State Hospital, Edirne, Türkiye Jagbir Singh Kadyan Swami Shraddhanand College, University of Delhi, New Delhi, India Jamil Kobrossi Faculty of Business Management, University of Balamand-Kelhat, El Koura, Lebanon Ahmet Konak Faculty of Economics and Administrative Sciences, Trakya University, Edirne, Turkey Paraskevi Koufopoulou Department of Pharmacy, Sector of Pharmacognosy and Natural Products Chemistry, School of Health Sciences, National and Kapodistrian University of Athens, Athens, Greece Andreas Koutoupis Department of Accounting and Finance, School of Economics and Administrative Sciences, University of Thessaly, Larissa, Greece Qëndresa Kukaj Faculty of Business and Management, “Universum” College, Lipjan, Kosovo
Editor and Contributors
xix
Hilal Özen Department of Business Administration, Faculty of Economics and Administrative Sciences, Trakya University, Edirne, Turkey Usha Pathak Department of Teacher Education, D.A.V. (P.G.) College, Dehradun, Uttarakhand, India Görkem Sariyer Department of Business Administration, Faculty of Business, Yasar University, Izmir, Turkey Kyriakos Souliotis Department of Social and Educational Policy, School of Social and Political Studies, University of Peloponnese, Corinth, Greece Agah Sinan Ünsar Faculty of Economics and Administrative Sciences, Trakya University, Edirne, Turkey Serap Ünsar Medical Nursing Department, Trakya University, Edirne, Türkiye; Faculty of Health Sciences, Internal Nursing Department, Trakya University, Edirne, Türkiye Luan Vardari Faculty of Economic, University “UKSHIN HOTI” Prizren, Prizren, Kosovo Athanassios Vozikis Laboratory of Health Economics and Management, Department of Economics, School of Economics, Business and International Studies, University of Piraeus, Piraeus, Greece
List of Figures
Fig. 1.1 Fig. 1.2 Fig. 1.3 Fig. 1.4 Fig. 3.1 Fig. 5.1
Fig. 6.1 Fig. 6.2 Fig. 6.3 Fig. 6.4 Fig. 6.5 Fig. 6.6 Fig. 6.7 Fig. 6.8 Fig. 6.9 Fig. 6.10 Fig. 6.11 Fig. 7.1
Fig. 7.2
How does occupational fraud affect organizations in health sector? Source ACFE (2022) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Fraud schemes and methods in health sector . . . . . . . . . . . . . . . . Methods of Medicare and Medicaid Fraud by Paul and Townsend (1997). Source Ford (1992) . . . . . . . . . . . . . . . . . . Fraud tree for health sector . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Model proposal . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Medical waste emblem (D˙IKKAT! TIBBI ATIK [ATTENTION! MEDICAL WASTE]. Resource: Official Gazette, Republic of Turkey, January 25, 2017) . . . . . . . . . . . . . . Dysfunctions caused by the physicians . . . . . . . . . . . . . . . . . . . . . Ill processes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Poor records keeping . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Inaccurate data entry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Delays in deliveries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Lack of training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Lack of operations control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Poor processes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Lack of workspace and poor circulation . . . . . . . . . . . . . . . . . . . . Lack of leadership . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Lack of strategic planning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Sub-total and health sector measures (as % of GDP) for G20: advanced economies for the three announcement periods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Sub-total and health sector measures (as % of GDP) for G20: emerging markets for the three announcement periods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4 5 6 12 48
91 105 106 106 107 107 108 108 109 109 110 110
124
125
xxi
List of Charts
Chart 4.1
Chart 4.2
Chart 4.3
Chart 4.4
Chart 4.5
Chart 4.6
Chart 4.7
Budgetary allocation of Ministry of Health and Family Welfare (in | crore) (Note BE—Budget Estimate; RE—Revised Estimates. Sources Expenditure Budget 2021–22; PRS) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Allocation of funds towards healthcare by MoHFW (Note During the year 2021 RE, |23,860 under the head “Others” includes | 14,217 crore towards COVID-19 emergency response and vaccination of healthcare and frontline worker. Source Ministry of Health and Family welfare, Govt. of India. https://www.mohfw.gov.in/) . . . . . . . . . . . . . . . . . Actual utilization of Budget by Department of Healthcare and Family Welfare (2010–11 to 2020–21) (Source https:// prsindia.org/budgets/parliament/demand-for-grants-202021-analysis-health-and-family-welfare) . . . . . . . . . . . . . . . . . . . . Growing Trends of India’s Healthcare Sector (US$) (Note F-Forecast. Source Frost and Sullivan, LSI Financial Services, Deloitte) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Government Healthcare Expenditure as a Percentage of GDP (Note BE-Budgeted Estimate, RE-Revised Estimate. Source World Bank, Economic Survey 2020) . . . . . . . Direct Jobs in India’s Healthcare Sector. 2017–2022 (Note The 2022 estimates for nurses and midwives may be high given the limited capacity to train and deploy an additional 1.9 million nurses and midwives in a 5-year period. Source Ministry of Skill Development & Entrepreneurship) . . . . . . . . . . Major out-of-pocket healthcare expenditures (Source Economic Survey Report 2020–21) . . . . . . . . . . . . . . . . . . . . . . .
58
59
60
61
61
62 62
xxiii
List of Tables
Table 3.1 Table 3.2 Table 3.3 Table 3.4 Table 3.5 Table 3.6 Table 3.7 Table 3.8 Table 3.9 Table 3.10 Table 3.11 Table 3.12 Table 3.13 Table 4.1 Table 4.2 Table 4.3
Table 4.4
Table 4.5 Table 5.1 Table 5.2 Table 5.3
Gender distribution of participants . . . . . . . . . . . . . . . . . . . . . . Distribution of participants by age . . . . . . . . . . . . . . . . . . . . . . Distribution of participants by educational status . . . . . . . . . . Operating period of the companies owned by the participants in years . . . . . . . . . . . . . . . . . . . . . . . . . . . . Monthly total family income distribution of participants . . . . Distribution of settlement areas where participants stayed the most in the age of growth . . . . . . . . . . . . . . . . . . . . . Negative feelings code frequencies . . . . . . . . . . . . . . . . . . . . . . Financial problems code frequencies . . . . . . . . . . . . . . . . . . . . Technical issues code frequencies . . . . . . . . . . . . . . . . . . . . . . . Current solution suggestions code frequencies . . . . . . . . . . . . . Capital and finance solutions code frequencies . . . . . . . . . . . . Solution suggestions for customers code frequencies . . . . . . . Code frequencies based on government solutions . . . . . . . . . . Taxation in India . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Income tax slab rate applicable for New Tax regime – FY 2020–21 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Income tax rates applicable in case of domestic companies for assessment year 2021–22 and 2022–23 are as follows: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Special income tax rates applicable in case of domestic companies for assessment year 2021–22 and 2022–23 are as follows: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Income tax rates applicable to foreign companies for assessment years 2021–22 & 2022–23 . . . . . . . . . . . . . . . . Classification of wastes from health institutions (T.C. Resmi Gazete, 25 Ocak 2017) . . . . . . . . . . . . . . . . . . . . . . . . . . Medical waste producers (T.C. Resmi Gazete, 25 Ocak 2017) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Trakya University 2021 Waste Declaration Form . . . . . . . . . .
44 44 44 45 45 45 46 47 47 49 49 50 51 64 65
66
67 67 88 90 95 xxv
xxvi
Table 7.1 Table 7.2 Table 7.3 Table 8.1 Table 8.2 Table 8.3 Table 8.4 Table 8.5 Table 9.1 Table 9.2 Table 9.3 Table 9.4 Table 9.5 Table 9.6 Table 12.1 Table 12.2 Table 12.3 Table 12.4
Table 12.5
Table 12.6 Table 13.1 Table 13.2 Table 13.3 Table 13.4 Table 13.5 Table 13.6 Table 13.7
List of Tables
List of countries with no-announcements . . . . . . . . . . . . . . . . . Minimum, maximum, and average statistics of fiscal measures (% of GDP) of the countries in each category . . . . . List of countries with (almost) no additional spending or foregone revenues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Personal and disease-related characteristics of the patients (n=143) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Information regarding LVD-36 and BDI . . . . . . . . . . . . . . . . . . Comparison of patient characteristics and mean LVD-36 scores . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Comparison of patient characteristics and mean BDI scores . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Correlation between the LVD-36 and BDI scores of the patients and age, BMI, EF, and number of drugs . . . . . . The raw data for the national apps by attributes . . . . . . . . . . . . Quantified data for the national apps by attributes . . . . . . . . . . Grey relational generating . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Grey Relational Coefficient . . . . . . . . . . . . . . . . . . . . . . . . . . . . Grey relational grades . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . The ranking of COVID-19 national mobile apps . . . . . . . . . . . Intubated and sedated intensive care unit patients descriptive characteristics (n = 91) . . . . . . . . . . . . . . . . . . . . . . Critical Care Pain Observation Tool (CPOT) aspiration and position measurements (n = 91) . . . . . . . . . . . . . . . . . . . . . Critical Care Pain Observation Tool (CPOT) aspiration and position scores comparison (n = 91) . . . . . . . . . . . . . . . . . Critical Care Pain Observation Tool (CPOT) aspiration and position measurements number and percentage results (n = 91) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . According to some physiological variables of intubated and sedated intensive care unit patients’ comparison of aspiration and position measurements (n = 91) . . . . . . . . . . Correlation results of the measurement scores of the CPOT and RSS (n = 91) . . . . . . . . . . . . . . . . . . . . . . . . . Areas that are vulnerable to corruption in the health sector of Kosovo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Gender percent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Age percent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Ethnicity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Residence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Region . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Which of the healthcare institutions have you most frequently visited during the years 2000–2020? . . . . . . . . . . . .
121 122 123 135 136 137 138 139 153 156 164 166 168 169 205 205 206
207
208 210 222 224 224 225 225 225 226
List of Tables
Table 13.8
Table 13.9 Table 13.10 Table 13.11
Table 13.12 Table 13.13
Table 13.14
Table 13.15
Table 13.16
Table 13.17
Table 13.18
Table 13.19
Table 13.20
Table 13.21
xxvii
What is the level of satisfaction of the health services for the following institutions? (University Clinical Center of Kosovo (UCCK)) . . . . . . . . . . . . . . . . . . . . . . . . . . . . What is the level of satisfaction of the health services for the following institutions? (Regional hospitals) . . . . . . . . . What is the level of satisfaction of the health services for the following institutions? (Family Medicine Center) . . . . What is the perception on the level of corruption in public healthcare institutions? (University Clinical Center of Kosovo) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . What is the perception on the level of corruption in public healthcare institutions? (Regional hospitals) . . . . . . . What is the perception on the level of corruption in public healthcare institutions? (Family Medicine Centers) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . What are the perceptions on the change in the level of corruption in the public health system in last two years? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . What are your perceptions on the implementation of effective anti-corruption policies or measures in health system by local public authorities? . . . . . . . . . . . . . . How often did you encounter the situation when you were supposed to go to private health institution due to the lack of services in public institutions? . . . . . . . . . . . . . . Do you agree or disagree with the following statement about the public health system in Kosovo (1–5)? (Doctors refer patients to their private surgeries or the private hospitals/clinics where they are employed) . . . . Do you agree or disagree with the following statement about the public health system in Kosovo (1–5)? (Doctors in public healthcare institutions do not respect working hours) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Do you agree or disagree with the following statement about the public health system in Kosovo (1–5)? (Doctors refer patients to certain pharmacies for drugs purchase) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Do you agree or disagree with the following statement about the public health system in Kosovo (1–5)? (Doctors misuse the medical equipment of public health institutions for personal benefits) . . . . . . . . . . . . . . . . . . . . . . . Do you agree or disagree with the following statement about the public health system in Kosovo (1–5)? (Doctors misuse drugs found in the essential drug list (free drugs) for personal benefits) . . . . . . . . . . . . . . . . . . . . . . .
226 227 227
227 228
228
229
229
230
230
231
231
231
232
xxviii
Table 13.22
Table 13.23
Table 13.24
Table 13.25
Table 13.26
Table 13.27
Table 13.28 Table 13.29 Table 13.30 Table 13.31
Table 13.32
List of Tables
Do you agree or disagree with the following statement about the public health system in Kosovo? (Doctors are offered informal payments in order to (in exchange to) receive better health services) . . . . . . . . . . . . . . . . . . . . . . . . . . Do you agree or disagree with the following statement about the public health system in Kosovo? (Doctors are offered material goods (non-monetary/gifts) in order to receive better health services) . . . . . . . . . . . . . . . . . . . . . . . . Do you agree or disagree with the following statement about the public health system in Kosovo? (Nurses are offered informal payments in order to receive better health services) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Do you agree or disagree with the following statement about the public health system in Kosovo? (Technical staff (laboratory technicians, radiologists, etc.) are offered informal payments in order to receive better health services) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Do you agree or disagree with the following statement about the public health system in Kosovo? (Technical staff (laboratory technicians, radiologists, etc.) are offered material (non-monetary) goods in order to receive better health services) . . . . . . . . . . . . . . . . . . . . . . . . Do you agree or disagree with the following statement about the public health system in Kosovo? (Nurses are offered material (non-monetary) goods in order to receive better health services) . . . . . . . . . . . . . . . . . . . . . . . . Do you think personally, or family connections should be used to receive better health services? . . . . . . . . . . . . . . . . . Have you donated money or other non-monetary goods to receive better health services in the last 12 months? . . . . . . What were the reasons for giving money or material goods? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Which of the medical services did you most often give money or material goods in public healthcare institutions? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Have you filed (experienced) cases of corruption before official authorities/institutions? . . . . . . . . . . . . . . . . . . .
232
233
233
233
234
234 234 235 235
236 236
Part I
Introduction Chapter
Chapter 1
Introduction: “Sectoral Fraud Tree” for Better Understanding Fraud Science—Trial Fraud Tree for Health Sector Kıymet Tunca Çalıyurt
Abstract To understand the types of fraud in the business world, we refer to Fraud Tree, published by the Association of Certified Fraud Examiners (ACFE). However, we encountered many new different schemes of fraud, especially after the pandemic and digitalization period. The fraudster, victims, material and moral consequences of each scam, and the relevant penal code differ. Therefore, our need for Certified Fraud Examiners, and lecturers who teach fraud prevention in the “sectoral fraud tree”, is clear. In this chapter, we started a trial study for sectoral fraud trees in the health sector. Keywords Sectoral fraud tree · Fraud Tree for Health Sector
1.1 Introduction Fraud ‘... crimes against the health care system..., last year cost the country $100 billion’. (National Underwriter, August 1994 cited from Robert Paul & James Towsend, 1997)
Robert J. Paul and James B. Townsend have mentioned about fraud problem in the health system in their paper published in 1997. They said that healthcare fraud and abuse have become epidemic in the USA, accounting for almost ten percent of all healthcare costs (Cox 1993; Stuart 1995) or about $100 billion per year (Hofmann 1994). In fact, this fraud has emerged as the Number 2 priority of the Federal Bureau of Investigation after violent crime (Wechsler 1995). To deal with
K. T. Çalıyurt (B) Centre for Forensic Accounting Research and Enterprise, School of Finance and Management, SOAS University of London, London, UK e-mail: [email protected] © The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd. 2023 K. T. Çalıyurt (ed.), Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II, Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application, https://doi.org/10.1007/978-981-99-5502-2_1
3
4
K. T. Çalıyurt
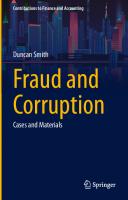
Fig. 1.1 How does occupational fraud affect organizations in health sector? Source ACFE (2022)
the growing evidence of waste and abuse, the FBI 1 has established healthcare fraud squads in its largest field offices (cited from Paul and Townsend 1997) (Fig. 1.1). Unfortunately, even the world’s most regulated countries are struggling to find solutions to fraud in the health sector. The world is getting smaller as e-trade increases; however, unpredictable crises, cultural differences, lack of standardization in trade codes, taxation codes, globalization, and ambitious leaders make it impossible to prevent fraud in the business world. According to the Report to the Nations published by ACFE (2022), the most critical fraud scheme is corruption in the health sector (Fig. 1.2). What is a fraud scheme in the health sector? Each sector has its own specific fraud schemes so health sector does. Inevitably, schemes help the CFEs2 get to the fraudster faster by solving fraud schemes which always consist of successive steps. Consequently, criminals who take roles in the schemes act same as the fraudster who committed crime in previous frauds in the same scheme. For example, let’s look at pharmacy fraud. In his 1992 Ford article, he presented a typical fraud scheme in the healthcare industry. It showed that a drug costing $16 was billed to the insurance company by the pharmacy for $164 (Fig. 1.3). Corruption concerning the development, evaluation, and distribution of pharmaceuticals, and in the health sector more broadly, is a significant problem. This corruption and the system of laws, regulations, and opportunities for profit that shapes and sustains it bring serious harm, including high prices, lack of availability of certain essential medicines, and a distorted medical knowledge base. The profit motive and power of the drug companies make reining in this corruption and the harm and injustice that results very difficult. Progress here will plausibly require a multipronged approach (Gifford 2020).
1 2
Federal Bureau Investigation. Certified Fraud Examiners.
1 Introduction: “Sectoral Fraud Tree” for Better Understanding Fraud …
5
Fig. 1.2 Fraud schemes and methods in health sector
What are the most common types of fraud in the health sector? Medicare fraud has been defined by the Centers for Medicare and Medicaid Services (CMS) as submitted or caused to have been submitted false acquisitions or misrepresentations of facts that have obtained federal healthcare payment for which no entitlement would have otherwise existed (Centers for Medicare and Medicaid Services). Upcoding: Upcoding is a type of fraud where healthcare providers submit inaccurate billing codes to insurance companies to receive inflated reimbursements. These false “current procedural technology” (CPT) submissions indicate that doctors provided patients with treatments that were more complex, costly, and time-consuming than what they actually received. This unlawful scheme is a violation of the False Claims Act (FCA)3 because it defrauds federal programs including Medicare, Medicaid, 3
The 1863 False Claims Act (FCA) is a federal law that allows whistleblowers to report companies or individuals that are defrauding the US government. A lawsuit filed under this statute, known as a Qui Tam case, is submitted directly to the federal court system; the whistleblower, known as
6
K. T. Çalıyurt
Fig. 1.3 Methods of Medicare4 and Medicaid Fraud by Paul and Townsend (1997). Source Ford (1992)
and Tricare (whistleblowerinternational 2023). Upcoding has been one of the most expensive and pervasive examples of healthcare fraud. Between 2002 and 2012, it was one of the costliest publicly funded medical assistance programs with an estimated $11 billion. These are not victimless crimes, as they place unnecessary strain on a social safety net that many millions of individuals rely on for their essential medical needs (Coustasse 2021). Phantom Billing: Phantom billing is the act of submitting bills for the payment of services, treatments, procedures, or prescription drugs that were never performed or necessary. This is identified as a specific form of medical fraud and is prosecuted under the False Claims Act (FCA) (https://www.lawsuitlegal.com/false-cla ims-act.php). Medical practitioners use fraudulent billing to make hundreds of thousands of dollars without any expense because the patients never existed and treatments never occurred. Phantom invoicing for non-existent treatments is an unethical medical billing practice and is the most common form of fraud because it is so simple to commit. Only one or two people need to be involved to accomplish this fraudulent act. This is one reason it is difficult to stop and easy to carry out. Patients and staff members can be totally unaware of the illicit activities since medical procedures the relator, is effectively suing the fraudulent company or individual on behalf of the Department of Justice. The government has the option of joining the plaintiff’s case against the fraudulent corporation or individual or decline to do so, leaving the relators free to proceed with the case in court on their own. 4 Medicare is health insurance for people 65 or older.
1 Introduction: “Sectoral Fraud Tree” for Better Understanding Fraud …
7
never actually happened. Patients can also be part of the scam. A healthcare provider will offer monetary compensation to patients, in exchange for the patient cooperation (Lawsuitlegal 2023). Billing for Unnecessary Services: Unnecessary medical billing can take many forms. In some cases, a physician will bill for a service never provided or upcode a service as a more expensive test or procedure in order to obtain further compensation. In other cases, the healthcare provider will intentionally misdiagnose a patient, knowing this diagnosis will enable them to bill for costlier tests and procedures the patient never needed. Another example of unnecessary medical billing occurs when a patient is provided a service or supply they never needed because the healthcare provider is hoping to receive additional funds. All unnecessary medical billing is wrong, but not all unnecessary medical billing falls under the False Claims Act. This law was specifically created to allow for prosecution of entities which are misusing government funds. This means, any unnecessary medical billing being paid by Medicare or Medicaid will fall under the law. The False Claims Act allow for citizens to act on behalf of the US government by filing a complaint. This is compared to cases where a private insurance company is being billed unnecessarily. This type of insurance fraud is not covered under the False Claims Act, but it is illegal. The private insurance company will need to seek out an attorney who can work with them to file a lawsuit on their behalf (Bothwell 2015). Double Billing: This practice occurs when healthcare providers bill both insurance companies and Medicare for the same procedure or treatment. For instance, a homehealthcare agency billed both Medicare and Medicaid $1 million for the same service (Taylor 1992). Medicare reports that double billing is often done by billing at the beginning of the month and again at the end of the month for the same service. Unbundling: Another form of improper medical coding and fraud is unbundling, also referred to as “fragmentation”. This fraudulent activity most commonly occurs in bills submitted to Medicare and Medicaid because the federal insurers often provide lower reimbursement rates for specific types of medical procedures that tend to be performed together. For example, incisions and closures related to surgical procedures will be bundled or combined with the procedure itself—or multiple blood tests from a single specimen will be bundled at a specific billing amount. Typically, the total reimbursement rate will be lower than it would have been for the procedures billed separately. Unbundling in medical coding occurs when a healthcare provider fragments or unbundles billing codes to receive a higher reimbursement amount. Providers may utilize electronic health records (EHR) software to falsify treatment notes or alter the displayed codes, thus justifying the unbundled billing at a higher rate (HalunenLaw 2022). Kickbacks: Here, medical providers, home-healthcare providers Robert J. Paul and James B. Townsend, 23, and others receive kickback payments for recommending particular home-healthcare or pharmaceutical services. In most of these cases, the cost of the kickback is integrated into the cost of the procedures and billed to Medicare or Medicaid, private workers’ compensation insurers, or the patients themselves (Paul and Townsend 1997).
8
K. T. Çalıyurt
From the FBI’s website, the most common types of fraud related to the health sector are listed as follows. Fraud Committed by Medical Providers • • • •
Double billing: Submitting multiple claims for the same service. Phantom billing: Billing for a service visit or supplies the patient never received. Unbundling: Submitting multiple bills for the same service. Upcoding: Billing for a more expensive service than the patient actually received.
Fraud Committed by Patients and Other Individuals • Bogus marketing: Convincing people to provide their health insurance identification number and other personal information to bill for non-rendered services, steal their identity, or enroll them in a fake benefit plan. • Identity theft/identity swapping: Using another person’s health insurance or allowing another person to use your insurance. • Impersonating a healthcare professional: Providing or billing for health services or equipment without a license. Fraud Involving Prescriptions • Forgery: Creating or using forged prescriptions. • Diversion: Diverting legal prescriptions for illegal uses, such as selling your prescription medication. • Doctor shopping: Visiting multiple providers to get prescriptions for controlled substances or getting prescriptions from medical offices that engage in unethical practices (FBI 2023). What are the patterns of fraud in the health sector in crises times? FBI (2020) warned the public of the following potential indicators of fraudulent activity: • Advertisements or offers for early access to a vaccine upon payment of a deposit or fee. • Requests asking you to pay out of pocket to obtain the vaccine or to put your name on a COVID-19 vaccine waiting list. • Offers to undergo additional medical testing or procedures when obtaining a vaccine. • Marketers offering to sell and/or ship doses of a vaccine, domestically or internationally, in exchange for payment of a deposit or fee. • Unsolicited emails, telephone calls, or personal contact from someone claiming to be from a medical office, insurance company, or COVID-19 vaccine center requesting personal and/or medical information to determine recipients’ eligibility to participate in clinical vaccine trials or obtain the vaccine. • Claims of FDA approval for a vaccine that cannot be verified. • Advertisements for vaccines through social media platforms, email, telephone calls, online, or from unsolicited/unknown sources.
1 Introduction: “Sectoral Fraud Tree” for Better Understanding Fraud …
9
• Individuals contacting you in person, by phone, or by email to tell you the government or government officials require you to receive a COVID-19 vaccine. Tips to avoid COVID-19 vaccine-related fraud: • Consult your state’s health department website for up-to-date information about authorized vaccine distribution channels and only obtaining a vaccine through such channels. • Check the FDA’s website (fda.gov) for current information about vaccine emergency use authorizations. • Consult your primary care physician before undergoing any vaccination. • Don’t share your personal or health information with anyone other than known and trusted medical professionals. • Check your medical bills and insurance explanation of benefits (EOBs) for any suspicious claims and promptly report any errors to your health insurance provider. • Follow guidance and recommendations from the US Centers for Disease Control and Prevention (CDC) and other trusted medical professionals. General online/cyber fraud prevention techniques: • Verify the spelling of web addresses, websites, and email addresses that look trustworthy but may be imitations of legitimate websites. • Ensure operating systems and applications are updated to the most current versions. • Update anti-malware and anti-virus software and conduct regular network scans. • Do not enable macros on documents downloaded from an email unless necessary and after ensuring the file is not malicious. • Do not communicate with or open emails, attachments, or links from unknown individuals. • Never provide personal information via email; be aware that many emails requesting your personal information may appear legitimate. • Use strong two-factor authentication if possible, using biometrics, hardware tokens, or authentication apps. • Disable or remove unneeded software applications (FBI 2020). Risks of fraud and corruption increase considerably during a crisis situation and even more so during an extended global crisis, which is characterized by chaos, fear, and uncertainty. Crises are breeding grounds for fraud and corruption as business models are challenged, supply chains are disrupted, the focus is more on operations than on compliance, and there are lack of suitable controls and a shortage of budget and resources (Mahanti and Neogi 2022). The COVID-19 pandemic has created a perfect storm for fraudsters. The healthcare system is under strain, and there is a lot of money flowing through it. Fraudsters are taking advantage of this by exploiting the system in various ways. This group should be classified as a separate type of fraud, as never before seen fraud patterns emerge in the healthcare industry during the crisis.
10
K. T. Çalıyurt
1.2 New Recommendation for Fraud Prevention: Sectoral Fraud Tree Some of the most common fraud schemes in the health sector during the COVID-19 pandemic include: • Telemedicine fraud: Fraudsters are billing for telemedicine services that were never provided. • Test kit fraud: Fraudsters sell fake or counterfeit COVID-19 test kits. • Vaccine fraud: Fraudsters are selling fake or counterfeit COVID-19 vaccines. • Insurance fraud: Fraudsters submit false claims to insurance companies for COVID-19-related expenses. • Medicare fraud: Fraudsters submit false claims to Medicare for COVID-19-related expenses. These fraud schemes are costing taxpayers billions of dollars. They are also putting patients at risk by providing them with fake or counterfeit medical products and services. It is important to be aware of these fraud schemes to protect yourself and your loved ones. If you suspect you have been a victim of fraud, you should report it to the authorities (Bard.Google).
1.3 Discussion If we want to stop paying to fraud, we should think economy as a whole system, nationally and internationally, institutionally and individually that Vian, Savedoff, and Mathisen mentioned in their study (2010) that: – institutional or system-level: monopoly, discretion, accountability, citizen voice, transparency, detection and enforcement, incentives; – individual level (perspectives of officials and citizens): attitudes, social and ethical norms, self-efficacy are main factors to discuss in fraud prevention. Fighting corruption requires strategies like these, which are grounded in theory, informed by evidence, guided by experience, and adapted to the context. Development agencies are promoting the “mainstreaming” of anticorruption, that is, incorporating anticorruption approaches in all sectors and at all intervention levels to achieve sustainable development results. But how do we adapt anticorruption principles to the particular context of the health system? (Vian et al., 2010). No matter what kind of precautions you take, if the politicians and the government in the country do not adopt the ethical rules. If the public-independent-internal auditors do not work by the criteria of independence and if the international standards of transparency, trade, accountability, reporting, and judicial system do not work in any sector, it cannot be prevented. In summary, “ethics in politics” is the first and unchangeable rule.
1 Introduction: “Sectoral Fraud Tree” for Better Understanding Fraud …
11
It is essential to classify business frauds, which show an increase during the pandemic and digitalization period. For example, the “knife money” type of bribery, which is still very common, is specific to the healthcare field. Selling the olive oil we buy by mixing other oils is a trick specific to the oil industry. Accurate classification of fraud in the business world is important in terms of detecting, examining, investigating, reporting, preventing, and anti-fraud training. A single fraud tree containing all sectors is insufficient for this fraud classification after the pandemic and digitalization period. In our new series titled “Integrity, Transparency, and Corruption in Healthcare & Research on Health”, we propose a health sector-specific fraud live map. We will renew and update this tree in every volume. We plan to focus and research sample cases of each type of health fraud. I would like to share the significant result of the study done by Amponsah et al. (2022). They have mentioned that blockchain’s disruptive nature in providing contemporary solutions cannot be over-emphasized. Considering the annual cumulative funds lost to fraud, the need for a novel approach to processing health insurance claims is momentous and requires the most excellent attention. By developing and testing a blockchain-based system that uses machine learning and domain data to judge the fraudulent nature of health insurance claims, this work has proposed a novel claims submission and processing system that is secured and makes datadriven decisions. The machine learning experiments imply that the proposed system accurately classified the claims data with an accuracy of about 98%. In a similar light, future claims will be classified with an error rate of about 2%. Although there is a cost ramification in adopting the proposed system, the long-term benefits make it a necessary cost compared to the worldwide annual amounts lost to fraud. Transitioning from the centralized approach to the decentralized blockchain-based system will ensure security, efficiency, and high data integrity in claims processing and also tremendously increase the efforts against fraud. CFEs should include blockchain and related issues in their agenda immediately. If they don’t know how to use blockchain in their controls and fraud examination activities, they can read newly published books and articles. Demirel (2022) has mentioned in his book that giant help company Novartis which works with the “PharmaLedger” project runs the blockchain platform to measure the supply chain, clinical trials, and health data accurately and transparently within the pharmaceutical sector. The blockchain project ensures that patients can access the information correctly by scanning the drug codes and that the real-time manufacturers know this information. It aims to ensure that drug manufacturers and the proper medications are transported to suitable patients and that the entire patient–drug relationship is followed in a network. These configurations are technological developments that will provide the infrastructure for personalized health services. It aims to ensure the control and transparency of the drug produced only for you within the network associated with your information. The solution to ethical problems in the healthcare industry is using blockchain and related technologies by the CFE, CPA, and other auditors (Fig. 1.4).
Fig. 1.4 Fraud tree for health sector
12 K. T. Çalıyurt
1 Introduction: “Sectoral Fraud Tree” for Better Understanding Fraud …
13
References ACFE (2022) Occupational fraud 2022: a report to the nations. https://acfepublic.s3.us-west-2.ama zonaws.com/2022+Report+to+the+Nations.pdf Amponsah AA, Adekoya AF, Weyori BA (2022) A novel fraud detection and prevention method for healthcare claim processing using machine learning and blockchain technology. Decis Analytics J 4. Bothwell M (2015, November 24) Bothwell law group, does unnecessary medical billing fall under the false claims act? https://whistleblowerlaw.com/unnecessary-medical-billing/. Accessed on June 13, 2023 Centers for Medicare and Medicaid Services (2017) Medicare Fraud & Abuse: Prevention, Detection, and Reporting. https://www.cms.gov/Outreach-and-Education/Medicare-LearningNetwork-MLN/MLNProducts/Downloads/Fraud-Abuse-MLN4649244.pdf Coustasse A (2021) Upcoding medicare: is healthcare fraud and abuse increasing? Perspect Health Inf Manag 18(4, Fall):1f. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8649706/#B36 Cox B (1993, February 8) Computers: a key weapon in healthcare fraud battle. National Underwriter Co. Property & Casualty/Risk & Benefits Management Ed. (Paul and Townsend, 1997) Demirel E (2022) Blockchain business projects. Amazon. ISBN-13:979-8370806681 FBI (2020) Federal agencies warn of emerging fraud schemes related to COVID-19 vaccines. https://www.fbi.gov/news/press-releases/federal-agencies-warn-of-emerging-fraudschemes-related-to-covid-19-vaccines. Published on Dec 21, 2020, Accessed on June 5, 2023 FBI (2023) Health care fraud. https://www.fbi.gov/investigate/white-collar-crime/health-care-fraud Ford JL (1992) Health care fraud the silent bandit. ISSN 0014-5688, USPS 383-310. https://www. ojp.gov/pdffiles1/Digitization/139191NCJRS.pdf Gifford F (2020) The health impact fund and the problem of corruption in the global pharmaceutical sector. In: Caliyurt KC (ed) Book: Integrity, transparency, and corruption in healthcare & research on health, volume I, Book Series: Accounting, finance, sustainability, governance & fraud: theory and application. Springer Nature, Singapore HalunenLaw (2022, Febraury 3) Upcoding, and unbundling are common types of healthcare fraud. https://www.halunenlaw.com/upcoding-and-unbundling-types-of-healthcare-fraud/. Accessed on June 15 2023 Hofmann M (1994) Antifraud groups praise senate report. Business Insurance 28(29):90 (cited from Paul and Townsend, 1997) Lawsuitlegal (2023) What is phantom billing? https://www.lawsuitlegal.com/phantom-billing.php. Accessed on June 15 2023 Mahanti R, Neogi MS (2022) Covıd-19, fraud, and compliance. EDPACS, The EDP Audit, Control, and Security Newsletter 65(5):17–26. https://doi.org/10.1080/07366981.2022.2038897 Paul R, Townsend JB (1997) Some legal and managerial strategies for managing healthcare fraud. Health Mark Q 14(3):19–33. https://doi.org/10.1300/J026v14n03_03 Stuart P (1995) HR attracts healthcare fraud. Personnel Journal 74(3):28–33 (cited from Paul and Townsend, 1997) Taylor, Jim (1992) Medicaid Fraud Control, FBI Law Enforcement Bulletin, October 1992, Volume 61, Number 10. https://www.ojp.gov/pdffiles1/Digitization/139194NCJRS.pdf Vian T, Savedoff WD, Mathisen H (2010) Anticorruption in the health sector, strategies for transparency and accountability. Kumarian Press, Sterling, USA Wechsler J (1995) Fraud Anach creates problems for MCOS. Managed Healthcare 5(6):17–18 (cited from Paul and Townsend, 1997) Whistleblowersinternational (2023) https://www.whistleblowersinternational.com/types-of-fraud/ healthcare/upcoding/. Accessed on June 30, 2023
14
K. T. Çalıyurt
Prof. Dr. Kıymet Tunca Çalıyurt (CPA, CFE) graduated from the Faculty of Business Administration at Marmara University, Istanbul, Turkey. Her Master’s and Ph.D. degrees are in Accounting and Finance Programme from the Social Graduate School, Marmara University. She has worked as an auditor at Horwath Auditing Company, a manager at Mcdonald’s, and finance staff at Singapore Airlines before positioning herself in academia. After vast private sector experience, she started working at Trakya University as a Lecturer in 1999. She was a Visiting Researcher at Concordia University, Canada (2001), Amherst Business School, Massachusetts University, USA (2014), and UNWE, Sofia, in 2019. In 2009, she founded the International Group on Governance, Fraud, Ethics and Social Responsibility (IGonGFE&SR) and International Women and Business Group (IWBG), which organizes a global annual conference. She published articles in Web of Science journals like Managerial Auditing Journal, International Journal on Law and Management, Risks and Sustainability. Her book chapters and books nationally and internationally on fraud, social responsibility, and ethics in accounting/finance/aviation disciplines are in Springer and Routledge. She is a book series editor for: – Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application (Springer Nature indexed by Scopus) – Women and Sustainable Business (Routledge) She is acting as an associate or editorial board member in the following titles; – – – –
Journal of Financial Crime (ESCI) International Journal on Law and Management (ESCI) Journal of Money Laundering Control (ESCI) International Journal of Climate Change Strategies and Management (SSCI)
She is the founding Chief-in-Editor for the “Accounting Finance Auditing: An International Journal” and “International Journal on Governance, Fraud, Ethics and ESG” which will take a start in 2023. She is an invited speaker at the International Economic Crime Symposium at Jesus College, Cambridge University, and partner of Herme Consulting in Trakya University Technopark.
Part II
Managerial Issues in Health Sector
Chapter 2
Marketing in the Health Sector Esra Demirba¸s
Abstract During the pandemic, healthcare services have become more important than ever. The strategic composition of the marketing mix for healthcare services has become critical and the strategic management and the usage of both health staff and medical resources have become vital for the health sector. The marketing mix of services differentiates due to the special features and due to nature of services. Difficulties faced in the pandemic have revealed the fact that the marketing mix composition and the service quality features of the health sector should be questioned and reviewed to bring the sector to be ready to successfully answer extraordinary and/ or unexpected problems and demands such as combatting and handling infectious diseases that affect the whole world. In this conceptual study, specific characteristics of services and the marketing mix of services will be reviewed considering healthcare services. Moreover, perceived service quality including five gaps encountered during the service performance will be discussed. Keywords Service specifications · Services marketing · Marketing mix of health services · Perceived service quality · GAPs in services
2.1 Introduction A service is an act or performance that is offered and obtained mutually between two parties that is essentially intangible and results in the ownership of nothing, instead offering solutions to answer customers’ needs (Kotler and Keller 2012; Grönroos et al. 2000; Grönroos 1998; Berry 1987; Berry et al. 1985). In services marketing, the focus point should be the management of resources and execution of the system and of the process to produce a result or a value for customers rather than producing and managing physical products (Grönroos 2001). E. Demirba¸s (B) Istanbul Yeni Yuzyil University, ˙Istanbul, Turkey e-mail: [email protected] © The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd. 2023 K. T. Çalıyurt (ed.), Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II, Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application, https://doi.org/10.1007/978-981-99-5502-2_2
17
18
E. Demirba¸s
Accordingly, healthcare service could be described as a process of providing solutions first to patients’ health problems and complaints and patients’ relative’s needs. Specific characteristics of services such as intangibility, heterogeneity (being also called “variability” by Kotler and Keller [2012, p. 381]), inseparability, and perishability differentiate them from goods and affect the composition of the marketing mix. During the pandemic period, healthcare services have become more important than ever. The strategic composition of the marketing mix for healthcare services has been critical, and the strategic management and the direction of both health staff and medical resources have become vital for both the public and private health sectors. Difficulties faced in the pandemic have revealed the fact that the service quality features and relatedly the marketing mix composition of the health sector should be questioned and reviewed to bring the sector to be ready to successfully answer extraordinary and/or unexpected problems and demands such as combatting and handling infectious diseases that affect the whole world. In this conceptual study, the specific characteristics and seven components of the marketing mix of services, and the customers’ service quality perception as a measure of satisfaction, will be reviewed considering healthcare services to be remembered and to be evaluated upon the pandemic conditions, to look forward much more in detail, and to be able to successfully combat with unexpected difficulties. Furthermore, Parasuraman et al.’s (1985) SERVQUAL model including five GAPs to determine the difference between customers’ expectation and their received service performance will be reviewed in this work considering healthcare services.
2.2 Services 2.2.1 Definition and Context Berry (1980) described services as tangible or intangible “deed, act or performance” (p. 25) and pointed out (1987) the difference between good and services as “good business sell things and service businesses sell performance” (p. 5). According to Grönroos (1998), a service company is mainly differentiated from a manufacturer in terms of offerings: A manufacturer produces products, whereas a service company offers solutions to answer customers’ needs. Moreover, the “process that leads to an outcome during partly simultaneous production”, and “the interactions between the customer and the quality-generating resources controlled by the service provider” compose the “heart of services marketing” (Grönroos 2001, p. 150). Kotler et al. (2012) extended Berry’s (1980) description by defining service as “any act or performance one party can offer to another that is essentially intangible and does not result in the ownership of anything. Its production may or may not be tied to a physical product” (p. 378).
2 Marketing in the Health Sector
19
Lovelock (1983) classified services as the following categories by underlining the fact that each service industry may be different (p. 10): i. Tangible actions to people’s bodies, such as airline transportation, haircutting, and surgery, ii. Tangible actions to goods and other physical possessions, such as lawn mowing, and janitorial services, iii. Intangibles actions directed at people’s minds, such as broadcasting and education, iv. Intangible actions are directed at people’s intangible assets, such as insurance, investment banking, and consulting. Health services fall into Lovelock’s all above categories upon the kind of healthcare received. Meanwhile, Tengilimo˘glu (2012) made another grouping that health services are belonged to: “public services, primary emergency/compulsory services, services delivered by a human, both profitable (private sector) and non-profitable services(public) and finally services that are requested qualified workforce (doctors, nurses, technicians)” (p. 52).
2.2.2 Characteristics of Services Characteristics that differ services from goods are intangibility, heterogeneity (being called “variability” by Kotler et al. [2012, p. 381]), Inseparability, and perishability. These characteristics are also called “IHIP” in the literature (Lovelock and Gummesson 2004, p. 22). Pride and Ferrell (2003) added two more characteristics as “client-based relationships and customer contact” (p. 325) to “IHIP”. Intangibility Unlike physical goods, services could not be touched, seen, tasted, felt, heard, or smelled before they are consumed, and these specifications lead service providers to present their service quality in the form of physical evidence or to transform intangible services into concrete benefits and a good experience. Following Bateson’s (1979) physical and mental intangibility classification, Laroche et al. (2001) grouped intangibility into three dimensions as follows: mental one explaining “the fact that physical tangibility does not ensure a clear, mentally tangible representation of an object, especially in case of unavailability of an evaluator to present the experience with that object” (p. 29); physical one meaning “inaccessibility to the senses” (p. 28); and generality referring to “how general/specific a consumer perceives a particular product (Laroche et al. 2003, p. 124). Lovelock and Gummesson (2004) stated that “even though pure goods and pure services are situated at the extremities, most other items are presented as containing a mix of tangible and intangible elements” (p. 26).
20
E. Demirba¸s
Heterogeneity Dependence on providers’ and/or consumers’ characteristics, and on time and/or place of service offerings make services, especially labor-intensive ones, heterogeneous or variable. This feature may be interpreted as not always receiving the same performance in services as it is in the mass production of goods. However, different studies and strategies have been developed in the services field to obtain uniformity in its production for a long time, such as Levitt’s (1972) attempt on the industrialization of service operation. Casati and Shan (2001) emphasized that a service should be “ideally able to be transparently adopted due to changes in the environment and to consumers’ needs with minimal touches or no user intervention” (p. 143). This will lead companies to be competent in satisfying individualistic needs in an increasingly competitive environment. Pilioura and Tsalgatidou (2001) also underlined the critical importance of rapid adaptation to the unique needs and continuous evolution of a dynamic business environment with changing requirements. According to Lovelock et al. (2004), replacement of human inputs by automation and rigorous application of quality improvement procedures causes a reduction in variability of output in numerous service industries. Kotler et al. (2012) proposed three steps to minimize the negative effects of variability feature such as “investing in good hiring and training procedures, standardizing the service-performance process throughout the organization (development and application of a service-blue print) and monitoring customer satisfaction” (p. 382) to get high qualified performance. In health services, to minimize the variability, there are written protocols that should be followed by people who touch patients and controlled by the administrator. On the other hand, health staff has a really hard time during the pandemic due to changeable indications of the virus from person to person. Hence, the protection rules could be standardized but, in the treatment, variable methods have been applied. Inseparability There is no possibility to produce services prior and to stock up then to deliver services to consumers. Contrarily, services are produced and consumed simultaneously. Not only the provider but also the client is part of the services process. This provider-client interaction was defined as “a special future of services marketing-insuperability” by Kotler et al. (2012, p. 381). Zeithaml (1981) claimed that intangibility, inseparability, and no standardization specifications of services create more difficulty than goods in the evaluation step. She also emphasized that besides goods that could be easily determined and evaluated before the purchase, “other goods and many services are high in experience qualities because their attributes could not be known or assessed until they have been purchased and are being consumed” (p. 187). According to Berry (1986), the human factor is the driving force in services marketing, and services firms should not only concentrate on external customers’ needs but also internal customers’ requests that are called internal marketing. Satisfied employees will bring satisfied consumers. The internal marketing issue has become more important than ever for the health sector in which the staff had really
2 Marketing in the Health Sector
21
hard times in the unexpected pandemic period when they served 7*24 h without physically contacting their families and relatives and any social contact. Perishability “Not to be stored” is the perishability characteristic of services. Kotler et al. (2012) proposed “the yield management” (p. 383) to overcome the perishability problem. They explained yield management as providing “the right services to the rights customers, at the right places, at the right times and at the right prices to maximize profitability” (p. 383). Successful demand management is also critical for a service organization. The length of demand fluctuation (wide or narrow) should be determined well and be strategically managed. During the pandemic, the fluctuated health demand that brought unexpected and not encountered workloads before in the health sector and health people extraordinary efforts to handle those workloads and unexpected cases, are stunning examples for the perishability feature of the health services. Pride and Ferrell (2003) mentioned two more characteristics additional to “IHIP” as “client-based relationships” and “customer contact” (p. 325). A congruent classification to the subject of this study has been offered by Chase (1978), categorizing services as” high contact” and “low contact”. The high-contact category includes “a large group of services involving delivery of tangible actions to customers”. The low-contact category is also subgrouped as “e-services” and “separable services”. Health services fall in the high contact category and hence should be managed with the relationship marketing concept and should always be customer oriented.
2.3 Health Services Marketing 2.3.1 The Marketing Mix of the Health Services 2.3.1.1
The Product/Service and the Product Mix of the Health Services
The product component of the health services is the combination of the intangible (treatment, hosting, pension, medical operation, catering, insurance coverage) services and the tangible (medicines, medical devices, prothesis, etc.) services (Tengilimo˘glu 2012). Service Levels Services can be described with three main service levels such as the core service, the basic service, and the augmented service. Meanwhile, Kotler (2000) clustered five product levels as follows: “core benefit, basic product, expected product, augmented product, and potential product” (p. 395). The core product of health services is the treatment of diseases. Meanwhile, hospital buildings, information desks, patient rooms, examination rooms, operating rooms, surgery rooms, delivery rooms, policlinics, labs, doctors, nurses, secretaries, medicines, medical devices, and operation
22
E. Demirba¸s
devices compose the basic product to be able to diagnose and treat diseases. At the expected level, a set of services normally patients and their relatives expect when they buy health services such as patient reservation office, cleaning and catering services, security, sufficient waiting area, and the name of the hospital. Extended pension services for both patients and patient relatives, private patients’ rooms, even suite patient rooms, catering for relatives, food and beverage shops, barbershop, parking, ATMs, etc., construct the augmented product level for health services (Kotler and Armstrong 2010). Although the core product is vital for health services, the quality and the successful management of the basic, expected, and augmented levels are highly influential in clients’ repurchase intentions for healthcare institutions (AlDoghaither et al. 2003; Choi et al. 2005). Considering Kotler’s (2000) expectation of the transformation of augmented benefits into expected ones, especially in the private health sector, it found more meaningful to group health services as core, basic, and augmented levels in which augmented level includes both expected and augmented levels features. Product/Service Hierarchy for the Health Services Kotler (2000) explained a product mix as “the set of all product lines and items that a particular seller offers for the sale, to buyers” (p. 396) and explained a product/ service line as “a group of products/services that are closely related because they function similarly, and sold to the same customer groups, are marketed through these same types of outlets, fall within given price range” (p. 396). A broad service mix length would bring the opportunity of treatments of several diseases. As wide as the service mix length means as much as holistic service offered, in a healthcare institution. Furthermore, the depth of a line would answer different health complaints. For example, emergency, surgery, mother and infant, oncology, radiology, and dermatology compose the length of the service line in a hospital while infant health, pediatrics, delivery, gynecology, newborn room, and newborn intensive care unit construct the depth of a service line (Tengilimo˘glu 2012). Continues studies on various health subjects would contribute to the length of the depth of a service line. However, because of the unexpected situation of the pandemic, some health institutions have obliged to constitute new COVID-19 departments and additional intensive care units for hooking up positive patients to an oxygen tube in both public and private hospitals. Moreover, new hospitals were constructed to answer the tremendous treatment demand of the public due to positives. Furthermore, the research laboratories have focused on developing a new vaccine to handle the virus to save the life of the world population. Of course, there is no possibility to develop medicine or a vaccine from zero in a short time, but continuous research on the appeared previous virus and on cancer diseases supported the scientists to offer a few kinds of vaccines within one year after the first appearance of the virus. Masque, respiration tubes, alcohol, sterile waters, and plastic gloves are the high consuming products during the pandemic period.
2 Marketing in the Health Sector
2.3.1.2
23
Pricing in the Health Services
Price is the marketing mix component that is determined at a level in which a customer agrees to buy, and a provider agrees to sell. Holistic marketers should consider many factors during pricing such as “the company, the customers, the competition and the marketing environment”. Lovelock and Wirtz (2012) defined the pricing tripod with the following three legs (p. 181): i. The cost the firms need to recover sets the minimum of floor price which is “the cost of the services” and “below that there is no profit” (Mucuk 2014). ii. The customer’s perceived value of the offering sets a maximum or ceiling price above which there would be no demand for the service (Mucuk 2014). iii. The price charged for competing services determines where, within the floorto-ceiling range, the price can be set. Mucuk (2014) posited that the price should be set taking into consideration of “internal and external factors” such as “the marketing policy of the service provider, the structure of the market and the demand, the competitors’ policies and prices” (p. 160). The main purpose of health services is to answer different health services demands of the society with the lowest price whenever and at which quality standards they request. However, successive technological developments, increasing costs and differentiation in diseases and viruses, even unexpected ones as COVID-19, and increasing quality expectation level have made the structure of the marketing mix of health services, much more complicated (Papatya et al. 2012). A well-known and/or a well-experienced brand is important factors in people’s choice of health service provider. Even more, customers think that healthcare institutions, including these two specifications, are more expensive (Tüfekçi et al. 2016). Wu (2011) also stated that brand image, service quality, and confidence play an effective role in the repurchase intention of the healthcare services. There are four types of pricing methods in the health sector (Gümü¸s and Kaya 2018). These are (i) cost-based pricing, (ii) competitive-based pricing, (iii) demandbased pricing, and (iv) authority-based (the ministry or the related professional institution about the public health) pricing (p. 68). Waters and Hussey (2004) stated that from a public perspective, the essential objectives in pricing health services are to ensure: “a. providers are fairly reimbursed for their work, b. prices accurately reflect the costs of correctly provided services and promote system sustainability, c. pricing structure supports the practice of appropriate medicine and rewards care that leads to good health outcomes” (pp. 1–2).
24
2.3.1.3
E. Demirba¸s
Promotion in the Health Services
Activities of a company to inform the target market about its product(s) or service(s), to convince people to buy them, and to frequently remind itself and its product(s) or service(s) are called the promotion component of the marketing mix. Convincing action has two different objectives in the promotion: (a) to inform permanent customers to enhance their repurchase intention throughout the company and (b) to convince non-users to become customers of that company (Mucuk 2014). “The traditional communication process which depicts the flow of messages from senders to receivers via elements such as encoding, media, and decoding” (Lasswell 1948, cited in Madhavaram et al. 2005, p. 69). The integrated marketing communication (IMC) approach has become the critical issue of promotion since the end of the last century, especially in the service sector. Vargo and Lusch (2004) argued that marketing is evolving towards a service-centered that is a dynamic and evolutionary process, and accordingly, institutions should act with the integrated marketing communication concept (IMC) instead of limitedfocus promotional tools and use the brand management for initiating and maintaining mutual relationships with the customers. For Kitchen et al. (2004), IMC will be a strategic weapon to “move forward in the highly competitive world of the twentyfirst century” (p. 28). For Keller (2001), “IMC represents the voice of a brand and how companies can establish a dialogue with consumers concerning their product offerings” (p. 823). Mucuk (2014) explained IMC as “not only integration of promotion activities” (p. 175) but also considering the multiplier effects of other marketing mix components besides the promotion, raising communication power of the company. Therefore, “all marketing mix components should be in coherence to give the same messages to customers, not contradict each other, and should always take into consideration other components” (Winer 2000, p. 181). “The synergy between the elements of the marketing mix and the promotion mix” (Odaba¸si 1995, p. 49) should be considered as a key factor of the IMC. Meanwhile, in many countries in the world including Turkey, “direct advertising activities of the health institutions and health products are prohibited and other promotional activities are limited due to the probability of misdirection of the target segment, of unfair competition, of the patients’ abuse and the redundant supply” (Gümü¸s and Kaya 2018, p. 72) and also due to misuse and overconsumption of different health products and also to a contradiction of them with the customs of the society with laws, regulations, and statutes (Tengilimo˘glu 2012, pp. 234–241). Accordingly, those institutions prefer more indirect promotion and public relations activities. Patients and relatives who receive satisfying services are the highly effective promotional agents in the health sector. Sharing the opinion verbally or digitally which is called word of mouth (WOM and e-WOM) plays a critical role in the service sector, especially in healthcare. WOM is “an informal communication way occurring between consumers about a product, a service or an organization to pass their opinion, mostly their delight or dissatisfaction through other people” (Demirba¸s
2 Marketing in the Health Sector
25
2018, p. 16). Positive recommendations will motivate people to contact that wellperformed center whereas complaints discourage them to go to poorly performed places. Hence “patients ‘satisfaction, brand management, and public relations are highly preferred promotional activities by the health institutions”. Technological and digital developments are also important promotional tools for healthcare institutions. Automatically, information access, online appointment, online data access, information gathering via social media tools, and a well-designed webpage are good opportunities for clients and to keep positive opinions about a health institution. Some promotional activities that are used by healthcare institutions could be summarized as follows: clients’/patients’ satisfaction, internal customers’ (staff) satisfaction, sponsorship, celebrated patients, field(s) specialization, awards/ certificates, agreements that allow patients to come for treatments, membership programs, special campaigns, social responsibility projects, scientific meetings, media declarations, competition organization, scholarship-granting (Gümü¸s and Kaya 2018), well-designed and updated webpages, effective social media accounts, well-educated employees, celebrated doctors, leaflets, publications in the journals, affiliation with a medical faculty of a well-known university, and providing facilities for patients that have difficulties to reach the health institutions by themselves. The corporate public relation has been critical in the pandemic. “Hygienic and contactless life with a masque” and “there is a life at home” and “staying at home saves the life” are the popular slogans of the pandemic period and have been used in the different channels to be emphasized, even in the emojis of the social media. Moreover, the health and education ministers always tried and successfully performed, to inform and orient the society to handle the virus and the pandemic via the mass and social media channels, including their private accounts.
2.3.1.4
Distribution and Distribution Channels in the Health Services
Distribution is the effective delivery action of goods/services to the target market (Tengilimo˘glu 2012). Effective delivery means whenever, whatever, how, and where clients could easily purchase the requested goods and services. Lovelock and Wirtz (2012) clustered service delivery into three groups based on the “nature of the interaction between customer and service organization; i. customer goes to a service organization, ii. service organization goes to customers, iii. customer and service organization transact remotely (mail or electronic communications)” (p. 134). Distribution channels are grouped as direct and indirect channels due to the interaction of channel members. Delivery of the service from a provider to customers is direct distribution whereas, an indirect one, there is an intermediary(ies) between the service provider and consumers. If a patient directly goes to a doctor’s office or a cottage hospital or a hospital, a direct distribution occurs. If a patient goes to a physical therapist and the therapist request MR and the patient goes to radiology, this interaction occurs as indirect distribution.
26
E. Demirba¸s
Physical structure, accessibility to healthcare providers, the usefulness of the received service, professionalism of the staff, specialization in the service, correct and effective usage of equipment and other sources during the service delivery, effective information, and quick referral systems compose dimensions of the distribution component in the health services. Strong cooperation with other healthcare institutions and an effective referral system are required especially for the specialized subjects (Tengilimo˘glu 2012, p. 279). Since patients go to a health institution, the service center should be convenient for both customers and the service provider. Easy and economic access to the health facility is very important for patients and their relatives (Karafakio˘glu 1998). Tengilimo˘glu (2012) pointed out that the distance from the hospital deters the patient from getting healthcare. Time spending by consumers to benefit from the service also plays an important role in consumers’ provider preferences, “quick and adequate service delivered in time maximizes a consumer’s satisfaction” (Odaba¸sı 1994, p. 64). In addition, easily getting appointment and examination whenever it is requested without a long wait, availability of digital access to the healthcare database, and of online communication bring both time and place saving to the mutual parts as a distribution function (Gümü¸s and Kaya 2018). Some hospitals may follow a widespread distribution policy as having different centers in where there are potential clients such as Presbyterian Hospitals in the USA and Acıbadem Hospitals in Turkey. Some healthcare services request a deep specialization on a subject that operates with a selective distribution choice such as Massachusetts the Joselin Clinic, Ankara Cancer Hospital, MD Anderson Children’s Cancer Hospital in Houston, Texas, Ko¸suyolu Heart Hospital, and Zeynep Kamil Maternity Hospital in ˙Istanbul. In Turkey, the widespread distribution policy is followed by the government. Different “city hospitals” have been launched upon the potential patient volume. Meanwhile, some state hospitals have been appointed as the pandemic hospitals during the pandemic to treat patients upon COVID-19 protocols and to keep the pandemic under control for the health of the society. High-quality service delivered healthcare centers also follow the selective distribution policy as VK Foundation American Hospital in Turkey, Mayo, and Cleveland Clinics in the USA. Receiving the COVID-19 test and the COVID-19 vaccination at home has been the golden service of the pandemic period in terms of the distribution.
2.3.1.5
Physical Evidence in the Health Services
The environment in which a service provider offers its products and services to consumers, the equipment and tools are used during service production, and the staff’s uniform, attitudes, and other material used to compose the physical evidence component of the marketing mix (Karahan 2000). Since the services are intangible, the physical evidence helps to bring a tangible dimension to the service to make
2 Marketing in the Health Sector
27
consumers able to evaluate the service received. Moreover, the physical evidence could be used as an effective tool in the brand and image management and the customers’ satisfaction by the management of a service company (Tengilimo˘glu 2012). There is no doubt that the physical evidence is an important component for the health services marketing mix due to patients who apply to any health center with an expectation of feeling better because of feeling already themselves uncomfortable (Tengilimo˘glu et al. 2015). There are two kinds of physical evidence those are called “the substantial evidence which cannot be owned by consumers” such as patient rooms, waiting rooms, and patients’ bed and “the complimentary evidence that is received with the service, a part of it” (Tengilimo˘glu 2012, pp. 294–295) such as drainage massage after surgery, surgical stocking, or delicious foods offering to patients (Tengilimo˘glu 2012, pp. 294–295). All offers should be focused on consumers’ comfortability, appreciation, and satisfaction in the health services from the waiting room seats or lights to the decoration of patient’s rooms and the diagnosis technics and the equipment. Cleaning, hygiene, odorless and comfortable environment; lightening and heating and calmness of the buildings; design, decoration, generally preferred soothing colors; surrounding posters, pictures, and writings; comfortable and novel patient rooms; privacy and ambiance of examination rooms; ultra-modern tools and equipment; comfortable waiting rooms are some considerable physical evidence for clients (Gümü¸s and Kaya 2018).
2.3.1.6
People in the Health Services
High interactions of service people and consumers make people a key component in the marketing mix of services, especially for the health sector. From the concierge to the head of the healthcare organization, all staff must be consumer oriented and act with this policy as an embedded culture of that organization. Many previous studies are underlining the importance of all workers’ attitude in a healthcare organization to make patients satisfied with the service received (Ataman and Aba 2016; Nitin et al. 2016; Karaçor and Arkan 2014; Torres et al. 2009; Choi et al. 2005). Customers of the health services are primarily patients therefore for the health sector, the customer-oriented approach is transformed to a patients-oriented approach while the customer satisfaction is called the “patients’ satisfaction” (Derin and Demirel 2013, p. 1113). Understanding and answering consumers’ needs and demands determine the performance of the service companies that have real difficulties in this dynamic environment due to dynamic changes in consumers’ needs and expectations. Tekin and Zerenler (2007) explain “customers’ satisfaction has become a difficult and dynamic objective that is hard to reach” (p. 168). It is tougher in the healthcare business that usually has consumers who have physical or psychological difficulties as patients. Reciprocal relationships between employees and consumers have already been scientifically approved (Chi and Gürsoy 2009, p. 246). Happy and satisfied workers
28
E. Demirba¸s
act polite and helpful even as problem solvers, but deep empathy through clients. Accordingly, the health sector that was concentrated on business and technical experiences to obtain a high-quality level in the past has also started to consider patients’ variable expectations, opinions, and feedback (Esato˘glu and Ersoy 1998; Ayaz and Soykan 2002). Patient satisfaction was defined as “how well the care service received meets a patient’s expectations” (Apay and Arslan 2009, p. 239). Wicks and Chin (2008) explained patients’ satisfaction process into three stages (p. 2438): (i) pre-experiences, perceptions, and word-of-mouth (WOM) inputs and feelings; (ii) actual experiences, perceptions, and word-of-mouth (WOM) inputs and feelings; (iii) Post-experiences, perceptions, and word-of-mouth (WOM) inputs and feelings. Thus, patients’ satisfaction is influenced by starting from the check-in process to checkout, including all healthcare and services delivered after checkout (Derin and Demirel 2013).
2.3.1.7
Managing Service Processes in the Health Services
“From the organization’s perspective, services are processes that have to be designed and managed to create the desired customer experience. Processes-which is the architecture of services- describe the method and sequence in which service operating system works and specify how they link together to create the value promised to customers”. According to Üner (1994), process management is to answer customers’ needs whatever and whenever they request. Moreover, process management brings the ability of continuous service performance (Tengilimo˘glu 2012). The business process of the health services starts with the appointment request system and terminates with the checkout of the health institute. The business process is more critical for the health services because most services requested are generally urgent, vital, and cannot be delayed and irreparable. Accordingly, this process should be carefully and successfully managed; otherwise, the service quality level will be unsatisfactory and annoying for customers due to poor, inefficient, frustrating, and slow performed process (Gümü¸s and Kaya 2018). Similarly, Karaçor and Arkan (2014) pointed out the high potency of processes of a healthcare organization, in the determination of patients’ satisfaction level. Meanwhile, Lovelock’s and Wirtz’s (2012) recommendation of “flowcharting which is a displaying technique the nature and sequence of the different steps in the service delivery, and blueprinting, which is a more detailed flow chart, with detailed design of customers services systems and also help to identify and to prevent and/or recover potential failures” (p. 245) is also stunning and highly useful for the health services management. Continuous process improvement that increases the efficiency of modules in a process and customers’ satisfaction being designed on their expected values is an integral part of the process management. Tengilimo˘glu (2012) explained the process management steps as “description of the process, determination of the interrelated activities, the appointment of the process owners, determination of the success criteria and the quality standards to evaluate the performance of the process” (p. 301).
2 Marketing in the Health Sector
29
Processes may be grouped (Rosingi et al. 2014) as follows: (i) primary types of business processes including production, marketing, sales, operation, customer services, finance, etc. These are the basic processes of a business being extremely important and fundamental. They deal with the basic values and work alongside the mission and vision of the business for the successful delivery of services or products to their clients. (ii). Support types of business processes including accounting, human resources, education, information technologies, building management, and maintenance. These processes are not involved in the delivery of the final product to the clients, but they create a suitable environment for the functioning of primary processes and they are focused on internal customers. (iii) Management processes are like the support processes which do not add value to the end consumer and are concerned with orientation and monitoring and analyzing the day-to-day business activities. As the concern of the process management primarily to create promised values to customers with the coherent performances of all stakeholders because of the holistic marketing approach, it may be meaningful to shortly mention the importance of the relationships marketing for the services, especially for the health services. Grönroos (1994) summarized the service management perspective as (p. 5): “a. from the product-based utility to total utility in the customer relationship, b. from short-term transaction to long-term relationships, c. from core product(goodservices) quality or the mere technical quality of the outcome to total customerperceived quality as the major driving to endure customer relationships”. Furthermore, Grönroos (1999) has redefined marketing based upon the relationship approach as (p. 328): “the process of identifying and establishing, maintaining, and enhancing and when necessary, also terminating relationships with customers and other stakeholders, at a profit so that the objectives of all parties involved are met; and this is done by mutual exchange and fulfillment of promises”. According to Grönroos, marketing approach is based upon relationships, interactions, and networks. He has recommended replacing marketing terms with customer relationships to be able to implement a culture of relationship marketing in an organization. This approach does include not only getting customers and creating transactions but also maintaining and enhancing ongoing relationships by making promises concerning all stakeholders within an organization.
2.3.1.8
Service Quality Perception as a Way of Consumers’ Evaluation of the Service Performance
The features of the services that are explained in Sect. 2.2 complicate the evaluation of the output of the service performance because there is no product in services; instead, there is a process (Grönroos 2001). Zeithaml (1981) indicated the difficulty of evaluating the outcome of services than goods due to the intangibility, heterogeneity, and inseparability features of services. Most services cannot be counted, tested, and verified before using them; hence, they do not have assured quality in advance. On the other hand, the labor-intensive services are heterogeneous and present variety
30
E. Demirba¸s
due to a provider, an employee, and a customer even could change day by day. It is difficult to settle uniformity due to the human factor. Similarly, the inseparability feature, in other words, the interaction between a consumer and a contact person, influences the performance of the service process. Parasuraman et al. (1985) defined service quality as “a measure of how much the delivered service level fits customers’ expectations” (p. 42). Parasuraman et al. (1985) also proposed the development of quality within a service company as an embedded culture to remove potential defects to reach sustainable superior service quality. Parasuraman et al. (1988) emphasized the prerequisite of delivering superior service quality for both success and sustainability in the market and pointed out consumers’ quality perception as the most efficient method to assess the quality of a service company performance due to the absence of objective measures to evaluate the quality level. According to Grönroos (1998), “the perception of the service process is important for the perception of the total quality of a service as an outcome” (p. 327). Furthermore, Grönroos (2001) split the perceived service quality into the dimensions of technical quality meaning “outcome quality of the process” in other words “what customers receive” (Van Riel et al. 2001, p. 361) and functional quality, referring “how the process itself functions” (p. 151). Parasuraman et al.’s (1988) service quality model that has been called SERVQUAL (p. 23) which has been the basic “skeleton” of the service quality perception includes five principal dimensions below (1991, p. 338): i. Tangibles: Appearance of physical facilities, equipment, personnel, and communication materials ii. Reliability: Ability to perform the promised service dependably and accurately. iii. Responsiveness: Willingness to help customers and provide prompt service. Assurance: iv. Assurance: Knowledge and courtesy of employees and their ability to inspire trust and confidence. v. Empathy: Caring, individualized attention the firm provides its customers. Perceived service quality presents a global judgment or attitude because of the superiority of a service, whereas satisfaction occurs related to “a specific transaction” (Parasuraman et al. 1988, p. 16). Moreover, perceived service quality means the level of discrepancy, in other words, GAP, between consumers’ perceptions and expectations including “consumers’ desires or wants as what a service provider should offer rather than would offer” (Parasuraman et al. 1988, p. 17). Baida et al. (2003) accept predicted service and a zone of tolerance that falls between the desired and adequate service levels as other elements of expectation. Moreover, they based expectations on word-of-mouth communications, personal needs, experience, and external communication realized by service providers (p. 115). Berry et al. (1985) concluded that comparison of service quality perception and expectations before receiving the service and actual experiences with the service result in consumers’ perception of service quality. Consequently (p. 46), if expectations are met, perceived service quality is satisfactory; if unmet, less than satisfactory; if exceeded, more than
2 Marketing in the Health Sector
31
satisfactory. Parasuraman, Zeithaml, and Berry-PBZ posited consumers’ difficulty to evaluate the service quality and they (1988) proposed to measure consumers’ perception of quality as overall evaluation (1985) to assess the quality of a service company due to unavailability of objective measures. They explained perceived service quality as “a form of attitude, related but not equivalent to satisfaction and the result of a comparison of expectations with the perception of actual performance” (p. 15). According to Parasuraman et al. (1985), the cognition level of the service quality is the difference between pre-sell service expectation and after-sell service perception. Furthermore, they pointed out the consideration of five gaps of services to be able to deliver consumers’ expected values. The un perception of customers’ expectations by the management, Gap1 occurs. Although management does not reflect customers’ expectations into the service quality specifications of the institution, Gap 2 arises. If employees do not understand well the service quality specifications and act divergently from those standards, this divergence results in Gap 3. Incorrect external communication of the service delivery to customers creates Gap 4. The overall differentiation of the perception of the service quality from expectations concludes in Gap 5 (Parasuraman et al. 1991, pp. 337–338): Gap 1: Difference between customer expectations and management perceptions. Gap 2: Difference between management perceptions of customer expectations. Gap 3: Difference between service quality specifications and the service delivered. Gap 4: Difference between service delivery and what is communicated about the service to customers. Gap 5: Perceived service quality, the customer-based performance measure, as defined in the model as the difference between customer expectations and perceptions, which in turn was hypothesized to be influenced by organizational Gaps 1–4. Previous studies on SERVQUAL and five GAPs were performed in different countries and the following summarized results were obtained (cited in Purc˘area et al. 2013, pp. 577–583): a. In the USA, the assurance had the lowest gap score, followed by reliability, responsiveness, empathy, and tangibles (Mangold and Babakus 1991, Babakus and Mangold 1992). b. In Hong Kong, the highest gap score was registered by the empathy dimension, followed by responsiveness, assurance, and reliability. c. In Singapore, responsiveness was the dimension that had the highest gap score, followed by assurance and reliability. d. In Oradea, Romania the highest gap score for empathy followed by reliability and assurance. e. In a patient forum of Romania, the tangible dimension turned out to have the highest gap score, followed by responsiveness and reliability. In tangible dimension, having a negative value means that marketing managers should invest as soon as possible consumers in service industries, lacking the technical knowledge, try to evaluate a service after tangible elements such as the environment
32
E. Demirba¸s
and the price. Managers should be careful in their healthcare environments maybe by applying strategies used in ergonomics, for example, music. To raise the scores of responsiveness and reliability dimensions, managers should pay great attention to the recruitment stage of their personnel based on backgrounds and communication with patients (Purc˘area et al. 2013).
2.4 Conclusion Specific characteristics of services which are intangibility, heterogeneity, inseparability, and perishability really differentiate operational and managerial activities of services, from the production of a good. The special specifications of services, accordingly the marketing mix of services, make the organization and the management of the health services much more sensitive and critical, even more vital that has been proven during the pandemic period. The human being is the center of the healthcare services which are generally visited by customers who feel uncomfortable due to any sickness they have, and this situation creates a hard time for the health sector to make customers satisfied and happy from services received. On the other side, internal customers’ satisfaction also highly affects the quality of services delivered. Accordingly, Grönroos (1999) redefined service marketing as relationship marketing to emphasize the importance of involving parties and their mutual promises, in the performance of services. Moreover, Parasuraman et al. (1985) described consumers’ satisfaction in services as related to superior service quality and pointed out that there is always a gap between the expected and perceived service qualities. The pandemic has been a period that has not been seen since the last century and it has broken almost all the rules. The health sector met with a demand that has not been seen for more than one hundred years. The yield management that is a system used in service management to balance the demand to successfully answer customers’ requests stood out like never in the health sector. In almost all hospitals, neither the physical evidence nor the people were adequate to handle positive patients. Not only intensive care units but also other departments without and in patients become insufficient to treat ever-increasing arrivals in the peak periods, even they could not welcome new arrivals. Some hospitals had to allocate or construct new departments to host and treat positive patients. Medical staff, unfortunately, were captured the virus from the patients, and sadly, some of them passed away. Besides this catastrophic end, the catch-up of the staff who tried to handle the excessive unexpected demand raised sometimes the trouble. It may be like a nightmare for the health staff and the management. They lived at war with the pandemic. On the other hand, the hospitals could not host their permanent patients. Sometimes, there was no place in the hospitals to take in them. Furthermore, some state
2 Marketing in the Health Sector
33
hospitals were suddenly appointed as the pandemic center, and they could not receive other arrivals even their follow-up patients who also lived hard times to continue their healthcare. All these realities revealed that all states must pay high attention to their health services and continuously ameliorate the healthcare conditions. Moreover, the composition of the marketing mix, especially the components of people, physical evidence, and process management, only belonging to services, is always critical and vital to be considered for unexpected worst cases.
References Al-Doghaither AH, Abdelrhman BM, Saeed AAW, Magzoub MEMA (2003) Factors influencing patient choice of hospitals in Riyadh, Saudi Arabia. J Roy Soc Public Health 123(2):105–109. https://doi.org/10.1177/146642400312300215 Apay S, Arslan S (2009) Hospitalized patient satisfaction level in a university hospital. TAF Prev Med Bull 8(3):239–244 Ataman H, Aba G (2016) Violence against health care workers: a retrospective study. Int J Health Serv Res Policy 1(1):20–27 Ayaz H, Soykan A (2002) Total quality management and the health sector. Clin Turkey J Psychiatry 3(1):19–26 Baida Z, Akkermans H, Gordijn J (2003) Serviguration: towards online configurability of real-world services. ICEC ‘03 Proceedings of the 5th International Conference on Electronic Commerce, 111–118 Babakus E, Mangold WG (1992) Adapting the SERVQUAL scale to hospital services: An empirical investigation. HSR: Health Servi Res 26(6):767–786. Bateson JEG (1979) Why we need service marketing. In: Ferrell OC, Brown SW, Lamb CW (eds) Conceptual and theoretical developments in marketing. American Marketing Association, Chicago, pp 131–146 Berry L (1980) Service marketing is different. Bus Week 30(3):24–29 Berry L (1986) Big ideas in services marketing. J Consum Mark 3(2):47–51. https://doi.org/10. 1108/eb008162 Berry L (1987) Big ideas in services marketing. J Serv Mark 1(1):5–9 Berry L, Zeithaml VA, Parasuraman A (1985) Quality counts in services too. Business Horizon, May–June, 44–52 Casati F, Shan M-C (2001) Dynamic and adaptive composition of e-services. Infor Sys 26:143–163 Chase RB (1978) Where does the customer fit in a service operation? Harv Bus Rev 56(November):137–142 Chi CG, Gürsoy D (2009) Employee satisfaction, customer satisfaction, and financial performance: an Empirical Examination. Int J Hosp Manag 28:245–253 Choi K, Lee H, Kim C, Lee S (2005) The service quality dimensions and patient satisfaction relationships in South Korea: comparison across gender, age, and types of services. J Serv Mark 19(3):140–149. https://doi.org/10.1108/08876040510596812 Demirba¸s E (2018) An overview of traditional and electronic word of mouth communication (WOM). Lectio Socialis 2(1):16–26 Derin N, Demirel ET (2013) Scale development study aimed at patient satisfaction which is the quality indicator in medical services. Inter J Soc Sci 6(2):1111–1130 Esato˘glu AE, Ersoy K (1998) Patients’ evaluations of hospital services (Continuous Quality Improvement in the Health Management, Editor: Çoruh M.). Haberal Education Foundation, Ankara
34
E. Demirba¸s
Grönroos C (1994) From marketing mix to relationship marketing: towards a paradigm shift in marketing. management decision. Sci Res 32:4–20 Grönroos C (1998) Marketing services: the case of the missing product. J Bus Ind Mark 13(4/ 5):322–338 Grönroos C (1999) Relationship marketing: challenges for the organization. J Bus Res 46:327–335 Grönroos C (2001) The perceived service quality concept-A mistake? Manag Serv Qual 11(3):150– 152 Grönroos C, Heinonen F, Isonlemi K, Lindholm M (2000) The net offer model: a case example from the virtual marketspace. Manag Decis 8(4):243–252 Gümü¸s R, Kaya A (2018) Marketing research in the health services. Cinius Publication, Istanbul. ISBN: 978-605-296-882-6 Karaçor S, Arkan A (2014) Marketing in health institutions: a research on the importance of the healthcare marketing mix factors for patients/consumers. Commun J Selçuk Univ 8(2):90–118 Karafakio˘glu M (1998) Health services marketing. ˙IU Business Administration Faculty Pub, ˙Istanbul Karahan K (2000) Services marketing. Beta, ˙Istanbul Keller KL (2001) Mastering the marketing communications mix: micro and macro perspectives on integrated marketing communication programs. J Mark Manag 17(September):819–847 Kitchen PJ, Brignell J, Li T, Jones GS (2004) The emergence of IMC: a theoretical perspective. J Advert Res 44(March):19–23 Kotler P (2000) Marketing management, The Millennium edn. Prentice-Hall, Upper Saddle River, NJ. ISBN:0-13-012217-3 Kotler P, Amstrong GM (2010) Principles of marketing. Prentice-Hall, Upper Saddle River, NJ. ISBN: 978-0-136-07941-5 Kotler P, Keller KL (2012) Marketing management, 14th edn. Pearson, Upper Saddle River, NJ. ISBN:978-0-273-75336-0 Laroche M, Bergeron J, Goutaland C (2001) A three-dimensional scale of intangibility. J Serv Res 4(1):26–38 Laroche M, Bergeron J, Goutaland C (2003) How intangibility affects perceived risk: the moderating role of knowledge and involvement. J Serv Mark 17(2):122–140 Levitt T (1972) Production-line approach to service. Harvard Business Review, September, 41–52. Lovelock C (1983) Classifying services to gain strategic marketing insights. J Mark 47(Summer):9– 20 Lovelock C, Gummesson E (2004) Whither services marketing? In search of a new paradigm and fresh perspectives. J Serv Res 7(1), 20–41. https://doi.org/10.1177/1094670504266131 Lovelock C, Wirtz J (2012) Services marketing, 7th edn. Pearson, Upper Saddle River, NJ. ISBN: 978-0-13-611874-9 Madhavaram S, Badrinarayanan V, McDonald RE (2005) Integrated marketing communication (IMC) and brand identity as critical components of brand equity strategy. J Advertising 31(4):69– 80. ISSN 0091-3367 Mangold WG, Babakus E (1991) Service quality: the front-stage vs. the back-stage perspective. J Serv Mark 5(4): 59–70 Mucuk ˙I (2014) Principles of marketing, 20th edn. Türkmen, Istanbul. ISBN: 978-605-4749-32-4 Nitin RV, Narendranath V, Devakumar G (2016) An empirical study on marketing mix strategies on healthcare services in a tertiary care hospital. Inter J Manage Appl Sci (IJMAS) 2(10):19–24 Odaba¸sı Y (1994) Health services marketing. Anadolu University Distance Education Faculty Publication, Eski¸sehir Odaba¸sı Y (1995) Marketing communication. Anadolu University Publication, Eski¸sehir Papatya G, Papatya N, Ham¸sıo˘glu AB (2012) Perceived service quality and patient satisfaction in healthcare institutions. Kırıkkale Univ J Soc Sci 2(1):87–108 Parasuraman A, Berry LL, Zeithaml VA (1985) A conceptual model of service quality and its implications for future research. J Mark (Fall):41–50
2 Marketing in the Health Sector
35
Parasuraman A, Zeithaml VA, Berry LL (1988) SERVQUAL: a multiple-item scale for measuring consumer perceptions of service quality. J Retail 64(1):12–40 Parasuraman A, Berry LL, Zeithaml VA (1991) Perceived service quality as a customer-based performance measure: an empirical examination of organizational barriers using an extended service quality model. Hum Resour Manag 30(3):335–364. https://doi.org/10.1002/hrm.393030 0304 Pilioura T, Tsalgatidou A (2001) E-services: current technology and open issues. Technologies for e-services. Lecture Notes Comp Sci 2193:1–15 Pride W, Ferrell OC (2003) Marketing: concepts and strategies, 12th edn. Houghton Mifflin, Boston Purc˘area VL, Gheorghe IR, Petrescu CM (2013) The assessment of perceived service quality of public health care services in Romania using the SERVQUA.L scale. Procedia Econ Finan:573– 585. https://doi.org/10.1016/S2212-567(13)00175-5 Rosingi von M, Scheel von H, Scheer AW (2014) The complete business process handbook. Science Direct, USA. ISBN: 978-0-12-799959-3 Tekin M, Zerenler M (2007) Flexible enterprise. Nobel, Ankara Tengilimo˘glu D (2012) Marketing of health services, 2nd edn. Siyasal, Ankara. ISBN:978-6055782–68-9 Tengilimo˘glu D, I¸sık O, Akbolat M (2015) Healthcare business management, 7th edn. Nobel, ˙Istanbul Torres E, Vasquez-Parraga AZ, Barra C (2009) The path of patient loyalty and the role of doctor reputation. Health Mark 26(3):183–197 Tüfekçi N˙IOG, Tüfekçi ÖK (2016) Research towards determining factor of private hospitals brand strategy in Isparta. Suleyman Demirel Univ J Fac Econ Adm Sci 21(1):321–338 Üner M (1994) Do the elements of the marketing mix vary in services marketing? Marketing World 8(43):2–11 Van Riel ACR, Liljander V, Jurriens P (2001) Exploring consumer evaluations of E-services: a portal site. Inter J Serv Manag 12(4):359–377 Vargo SL, Lusch RF (2004) Evolving to a new dominant logic for marketing. J Mark 68(January):1– 17 Waters H, Hussey P (2004) Pricing health services for purchasers: a review of methods and experiences. HNP World Bank Discussion Paper Wicks AM, Chin WW (2008) Measuring the three process segments of a customer’s service experience for an out-patient. Int J Health Care Qual Assur 21(1):24–38 Winer RS (2000) Marketing Management. Prentice-Hall, Upper Saddle River, NJ Wu CC (2011) The impact of hospital brand image on service quality, patient satisfaction, and loyalty. Afr J Bus Manage 5(12):4873–4882 Zeithaml VA (1981) How consumer evaluation processes differ between goods and services in the marketing of services. Am Mark Assoc:186–190
Esra Demirbas received a BS degree from ˙Istanbul Technical University (ITU), in the management engineering field, in 1988. She obtained an MBA degree from Bosphorus University in 1991. After two years as a marketing research assistant at ITU, she joined Koc Group as a management trainee in the headquarters, where she spent seven years. In 1996, she was appointed as a vice president of the collection department of Koçfinans, and in 2000, she was appointed as a deputy general manager of Koç Fiat Kredi. She terminated her professional life at the end of 2009 and returned to academics. While studying Ph.D., she was a part-time instructor at Bahcesehir University (BAU) between 2010 and 2014. She has been acting as an associate dean and a marketing instructor at the Faculty of Economics and Administrative Sciences in Istanbul Yeni Yuzyil University, Türkiye, since September 2014. She has several studies on marketing management, marketing research, strategic marketing, CSR marketing, and consumer behavior. She is fluent in English and French. She is married with two children.
Chapter 3
A Model Proposal for Solutions to the Problems Faced by Small and Mediums in the COVID-19 Process Ahmet Konak
and Agah Sinan Ünsar
Abstract In the study, the problems faced by Small and Medium Enterprises (SMEs), which have a crucial issue among businesses in Turkey, during the COVID19 pandemic and solutions for these problems are included. The research was conducted by adopting the maximum variation sampling method with 51 SME owners in Lüleburgaz operating during the pandemic. Study: It was conducted by adopting the principles of qualitative research and was designed in line with the phenomenology pattern. Qualitative research questions were prepared using the structured interview technique. The findings were analyzed using the thematic analysis method and the Analytics Pro version of the MAXQDA 2020 qualitative analysis program. The model proposal was created due to the analysis of the obtained data; it consists of four stages: Information Retrieval, Capital and Financial Management, Customer Relations Management, and Government Support. As a result of the research, it was revealed that the problems experienced by SMEs during the pandemic process should be evaluated in a situational framework. Keywords SMEs · Entrepreneurship · COVID-19 · Pandemic
3.1 Introduction SMEs have a critical place in the economy of many countries in the world; due to the emergence of the COVID-19 virus and its rapid spread globally, it has been affected in many ways. In the study, the problems faced by SMEs and solutions to overcome these problems are included. In the first part of the study, along with the concepts of entrepreneur and entrepreneurship, SMEs in Turkey and the world and This study was adapted from Ahmet Konak’s master’s thesis. A. Konak · A. S. Ünsar (B) Faculty of Economics and Administrative Sciences, Trakya University, Edirne, Turkey e-mail: [email protected] © The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd. 2023 K. T. Çalıyurt (ed.), Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II, Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application, https://doi.org/10.1007/978-981-99-5502-2_3
37
38
A. Konak and A. S. Ünsar
their definitions are included. The second part of the study covers the general COVID19 pandemic, the pandemic process, and the effects of the pandemic. In the third part of the study, the research’s method, findings, and model proposal are included. In this section, detailed information about the research method is given, and the analysis of the data obtained from the participants with the qualitative research program is presented as a result of the analysis of the findings; themes, categories, and codes were created and tabulated. As a result of general evaluations, a model proposal was created. Different studies were evaluated in terms of similar and different aspects; suggestions were made to the researchers of possible future studies; and the final results were included.
3.2 SME Definition In this chapter, SMEs, which is the abbreviation of the concept of “Small and Medium-Sized Enterprises”, are discussed. SME definition: The number of employees is made with certain numerical classifications, such as annual net sales revenue.
3.2.1 SMEs in the World and Turkey SME definitions may differ from country to country. SMEs can generally be determined by the number of employees, annual earnings, or the value of business assets. SME concept: It can be used for all kinds of businesses, such as family companies, sole proprietorships, or cooperatives (ILO 2015: 2). When evaluated within the scope of OECD countries, SMEs makeup 99% of all businesses. However, it is stated that the added value created by SMEs in OECD countries is between 50 and 60%. SME employees makeup about two-thirds of all employees. For this reason, SMEs are characterized as an essential part of employment in OECD countries (OECD 2019: 3). The role and importance of SMEs have existed for many years. SMEs, by academics, business owners, and managers, are seen as power and innovation elements of great importance for economies (Thrassou et al. 2020: 1–2). SMEs constitute 999 per thousand of the enterprises in Turkey (Mucuk 2018: 111). SMEs: According to the current definitions published in the Official Gazette, it is divided into sections as “micro”, “small” and “medium” sized enterprises (KOSGEB 2018: 12).
3 A Model Proposal for Solutions to the Problems Faced by Small …
39
3.2.2 COVID-19 Pandemic In this section, regarding the COVID-19 pandemic, which has had serious effects all over the world, the terminological evaluation of the pandemic, its historical processes, efforts to combat the pandemic, and the effects of the pandemic in different dimensions and areas are included.
3.2.3 Pandemic Concept The word “pandemic” has its origins in Greek. Word: It means “all” and describes people. On the other hand, the internationally accepted definition of the concept of pandemic is given in the Epidemiology Dictionary as follows: “An epidemic that affects the whole world or in very large geographies, reaches international dimensions and generally affects many people”. Definition of the concept of pandemic by WHO: It is expressed as an epidemic disease that no one or very few people are immune to, can easily be transmitted from person to person, and spread rapidly all over the world (Qiu et al. 2017: 3).
3.3 Announcement of COVID-19 Pandemic Process and WHO’s Targets On December 31, 2019, cases of pneumonia that could not be fully identified were announced by the World Health Organization’s China Representation. These cases were first detected in the province of Wuhan, located in the Hubei Province of the People’s Republic of China. On January 7, 2020, it was determined that there was a new type of coronavirus that has not been seen in humans until that day. The name of the disease caused by this virus has been determined as COVID-19. The name of this new type of virus is official; it has been identified as SARS-COV-2. The emerging new type of coronavirus has begun to spread rapidly in different countries. Except for China, this epidemic has been positioned as a pandemic by the World Health Organization as a result of the detection of new COVID-19 cases spreading rapidly and causing severe discomfort in 113 different countries (T.C. Sa˘glık Bakanlı˘gı 2020: 5). The strategic targets set by the World Health Organization for the COVID-19 pandemic are as follows (WHO 2020: 10): • Prevent human-to-human transmission, including reducing close contacts and secondary infections among healthcare workers, preventing increases in virus transmission rates, and preventing further international spread. • Infected patients as early as possible, to isolate and care for patients. • To determine the source of the animal infected with the virus and to reduce it.
40
A. Konak and A. S. Ünsar
• Related to the disease; to deal with the unknown about the extent of transmission and infection, treatment options, to act agile in diagnosis, treatment, and development of vaccines. • Communicating critical risk and incident information to the entire community and preventing the spread of misinformation. • Minimizing social and economic interaction through multi-sectoral collaborations.
3.4 Effects of the Pandemic on SMEs COVID-19 pandemic is unprecedented in both its complexity and severity (Gourinchas et al. 2020: 1). It is predicted that sectors such as wholesale and retail trade, accommodation, and food may be more affected by the COVID-19 outbreak than other sectors. It has been determined that the banking and e-commerce sectors have been less affected by the COVID-19 outbreak or increased in their activities. SMEs: It has been determined that the pandemic process is much more affected than large enterprises (ILO 2020: 24). COVID-19, with an impact far beyond the epidemiological field, has emerged as a crisis that has led to the reshaping of habits, relationships, working, and lifestyles. For this reason, the resulting pandemic conditions brought with it economic problems, especially the field of entrepreneurship (IDE 2020: 14). It is stated that SMEs, which face the danger of losing their important income sources, have limited raw materials, and have more limited financial resources, also experience significant problems. SMEs: It is argued that they are among the companies that have difficulties during the pandemic period, as they are in contact with a limited number of suppliers within the scope of the global supply chain and find less room for movement in price policies. As a result of the prolongation of the pandemic period, it is predicted that SMEs will have problems in managing their human resources. Many SMEs: It is stated that it is directly affected by its decreasing demands and problems related to the supply chain (ILO 2020: 4). SMEs: Due to their size and structure, they often struggle with profitability and cash flow (Juergensen et al. 2020: 500). Although it is difficult to predict the long-term effects of the COVID-19 pandemic, scientists state that companies that attach importance to digitalization during the epidemic will continue to capture important opportunities after the epidemic (Priyono et al. 2020: 4–5).
3 A Model Proposal for Solutions to the Problems Faced by Small …
41
3.5 Research Method, Findings, and Model Proposal In this chapter, the research method of the study titled “The Problems Encountered by SMEs in the COVID-19 Process and a Model Proposal for Their Solutions”, the findings obtained, and a model proposal for the problems faced by SMEs during the pandemic process are included.
3.5.1 Research Type Research: It was carried out by adopting the qualitative research method in order to identify the problems experienced by SMEs during the COVID-19 pandemic process in depth and to offer solutions to these problems by taking into account the opinions of SME owners. Research: It was created in line with the phenomenology pattern, which is one of the qualitative research designs. The phenomenology pattern is preferred in order to describe experienced events. In the phenomenology pattern, there are participants who have experience with the situation to be researched and these participants are determined by the researcher (Yurdakul 2013: 35–36).
3.5.2 Research Purpose Research: It was carried out to identify the problems faced by SMEs in Turkey during the pandemic process and to offer solutions to these problems in light of the information obtained from SME owners. The research, in addition to the COVID-19 pandemic, aims to help SMEs find solutions to similar problems that may occur in the future.
3.5.3 Research Importance Pandemic has caused many SMEs to suffer. In the research, the future of SMEs needs to aim to prevent uncertainty, one of the most important problems they face, with the solution proposals stated by SMEs. It is thought that the aim of the findings and solution proposals obtained in the research to guide SMEs and institutions that can help SMEs in case of a similar epidemic that may develop during the COVID-19 epidemic or afterward reveals the importance of the research in terms of the future of SMEs.
42
A. Konak and A. S. Ünsar
3.5.4 Research Population and Sample The universe of the research consists of entrepreneurs who have operated as SME owner during the COVID-19 pandemic, located in the Lüleburgaz District of Kırklareli Province. In the research, in order to identify the common problems experienced by SMEs, different types of SMEs were tried to be preferred for the sample as much as possible. This method, which is called “maximum variation sampling” and is one of the purposive sampling methods, examines the dimensions of the problems that arise as a result of searching for common points in different situations (Yıldırım and Sim¸ ¸ sek 2018: 119). The snowball sampling method was also used in order to increase the diffusion rate of the research and to facilitate the diversification of the participants. Snowball sampling method is defined as the participants helping the researcher to reach different participants by sticking to the sample characteristics (Yurdakul 2013: 84). It is aimed to reach at least 30 participants in order to better observe the problems experienced by SMEs related to the pandemic process. When the answers given by the participants to the research questions are started to be repeated and it is concluded that there is sufficient diversity on behalf of the participants, it was determined that the data collection process achieved its purpose, and the research was terminated when 51 participants were reached in total.
3.5.5 Research Questions Questions directed to the participants. In order to distinguish the participants demographically and to obtain the necessary data about the enterprises of the participants, the thesis was created by the responsible of the thesis in light of the relevant literature, business functions, and current developments. Research questions: It was prepared by adhering to the “structured interview” technique. The purpose of using the structured interview technique is stated as providing a comparison between the answers given by the participants to the questions (Yıldırım and Sim¸ ¸ sek 2018: 130). In order to understand the feelings and opinions of the participants better and in detail, 17 research questions were asked. Demographic questions and 17 research questions directed to the participants in order to create a model proposal for the problems faced by SMEs during the COVID-19 process and their solutions; “The Problems Encountered by SMEs in the COVID-19 Process and A Model Proposal for Their Solutions” is included in the ANNEX-1 of the ANNEX section of the master’s thesis.
3 A Model Proposal for Solutions to the Problems Faced by Small …
43
3.5.6 Aggregation of Research Data All processes of the study happened during the COVID-19 pandemic and some of the restrictions caused by it. In this direction, in terms of protecting the health of the researcher and participants, pandemic restrictions and facilitating the process, it was decided to collect the research data digitally. In order to ensure reliable collection of data, the “Google Forms” form creation and application tool was used. The data collected with this tool were exported with the “Google Sheets” and “Microsoft Excel” tools. The participants were natural persons and answered the research questions based on their own industry, observation, participant confirmation, and peer confirmation methods.
3.5.7 Analyzing Research Data In order to reveal the patterns and themes in the findings clearly and simply, the “thematic analysis” method was used. Thematic analysis takes place in the literature as a method of detecting, analyzing, and reporting the themes in the collected data. It ensures that the collected data are minimally organized and explained with rich details. Thematic analysis often overrides all of these and enables the interpretation of different items related to the research topic (Braun and Clarke 2006, pp. 79–80). MAXQDA 2020 Analytics Pro qualitative analysis program was used in the general analysis of the data, creating themes and codes, arranging the graphical and tabular displays of the data, comparative analysis of the data of the participants, and creating a code cloud.
3.5.8 Results In this chapter, the findings of the research and analysis are included. 1. Demographic Characteristics of Research Participants In the process of determining the participants, the individuals who were thought to have different variables and demographic characteristics were determined. In the sampling process, “Maximum variation sampling”, which is one of the purposive sampling methods, was preferred and it was aimed to reach demographically different and diverse participants. In this way, it is aimed to examine the dimensions of the problems that arise as a result of investigating the common points in different situations. In this context, the participants’ gender, age, education level, operating period of the enterprises, monthly family income, the longest residence in the growing period, and sector variables were selected to cover all possible variable diversity by adhering to the principle of maximum variation.
44 Table 3.1 Gender distribution of participants
A. Konak and A. S. Ünsar
Gender
Frequency
Man
42
Woman Total
9 51
The distribution of the participants according to the gender variable is shown in Table 3.1. Due to the use of natural methods in the determination of the participants, Table 12. Shows that there is a difference between the frequencies of male and female SME owners. It is known that the number of women entrepreneurs in Turkey is around 10% compared to the total number of entrepreneurs (T.C. Kalkınma Bakanlı˘gı 2018: 69). Therefore, it was concluded that the distribution of the participants according to the gender variable was at an acceptable level. Table 3.2. Shows the distribution of the participants by age, in order from smallest to largest. The age of the participants starts from 24 and reaches 66 years old. Based on this table, it can be seen that the maximum variation method is adhered to in terms of age in the sample. The educational status of the participants according to six different education levels is given in Table 3.3. The number of years the companies owned by the participants have been operating is shown in Table 3.4. The businesses owned by the participants start from the business that has been operating for 1 year and extend to a long-established family company of 72 years. Table 3.2 Distribution of participants by age
Table 3.3 Distribution of participants by educational status
Age
Frequency
24–34
6
35–45
22
46–56
16
57 +
7
Education status Primary school Middle school High school
Frequency 2 5 24
Associate degree
5
Bachelor’s degree
13
Graduate Total
2 51
3 A Model Proposal for Solutions to the Problems Faced by Small … Table 3.4 Operating period of the companies owned by the participants in years
45
Operating Period of the Company (Year)
Frequency
1–5
8
6–14
14
15–25
16
26–39
6
40 +
3
It is understood that the activity periods of the enterprises of the participants show maximum variation. The distribution of the monthly total family income of the participants is shown in Table 3.5. The monthly family income of the participants starts from the minimum wage levels of 2021 and reaches up to 50,000 TL. The distribution of the participants according to their settlements in their growing up age is given in Table 3.6. In Table 3.6, which shows the settlements of the participants who have SMEs, it is shown that nearly half of the participants grew up in the district. The fact that the research took place in a district can show that a large part of the participants owned a business in the region where they grew up. 2. Industry Variable The variables evaluated according to the answers given by the participants within the scope of the sectors and the work they do are included in this section. Table 3.5 Monthly total family income distribution of participants
Table 3.6 Distribution of settlement areas where participants stayed the most in the age of growth
Monthly Family Income (TL)
Frequency
Uncertain
1
2,850–5,000
17
5,001–10,000
21
10,001–20,000
8
20,001–30,000
3
30,000 +
2
Residential area
Frequency
Town/District
2
Big city
4
Bay
9
Province
11
District
25
Total
51
46
A. Konak and A. S. Ünsar
Justice and security, information technologies, glass, cement and soil, education, electrical electronics, food, construction, machinery, media, communications and publishing, metals, automotive, health, agriculture, hunting and fishing, textile, trade, transportation, logistics, and there is at least one participant from sectors such as communications. As can be understood from the sectors where the participants are, the business areas in which the participants operate vary. This provides an opportunity to examine the situation of many businesses operating during the COVID-19 pandemic and affected by the processes brought about by this period. 3. Code System MAXQDA 2020 Analytics Pro qualitative analysis program was used to create the themes, categories, and codes of the research. Because the relevant literature has just started to develop and there are not enough studies, the inductive method was adopted in light of the data obtained from the participants, and a code system consisting of themes, categories, and codes was created. In this way, the research and the code book are aimed to shed light on the work that can be done in the future. The codes created in line with the answers given by the participants to the research questions have different frequency values. It is observed that some codes are repeated more in the research data, and some are less repeated. The code frequencies of the negative feelings felt by the participants during the pandemic process are shown in Table 3.7. The code frequencies of the financial problems experienced by the participants are given in Table 3.8. Table 3.7 Negative feelings code frequencies
Negative Feelings
Frequency
Anxiety
14
Strain
11
Uncertainty
9
Hopelessness
4
Uneasiness
3
Feel bad
3
Trouble
2
Pessimism
2
Dissatisfaction
2
Sadness
2
Despair
1
Instability
1
Panic
1
Stress
1
Fear
1
3 A Model Proposal for Solutions to the Problems Faced by Small … Table 3.8 Financial problems code frequencies
Table 3.9 Technical issues code frequencies
47
Financial Problems
Frequency
Closing
16
Spending savings
13
Price instability
10
Reduction in transaction volume
5
Staying away from the customer
5
Employee payments
4
Negative profit
2
Inability to compete with large businesses
1
Technical Issues
Frequency
Supply issue
14
Shipping issues
3
Quarantine
1
The code frequencies of the technical problems experienced by the participants are given in Table 3.9. Many of the participants advocate that the financial difficulties brought by the pandemic should be solved together with the public. It is seen that it would be a good practice to fully fulfill the financial supports that can be provided by the public, such as the continuation of the short time working allowance throughout the pandemic, rent support, invoice and tax supports. By the participants, it was stated that the necessary support should be provided by the public in the process of compulsory closure of workplaces. One of the remarkable suggestions made by the participants is that the same support package applications may not be efficient due to the different characteristics of each business. It is argued that businesses with different number of employees, financial situations, and business lines should receive support in different sizes and types. These suggestions, which can be evaluated within the framework of the contingency approach, reveal a new dimension in the support that can be given during pandemic periods.
3.6 Model Proposal In line with the analysis of the answers given by the 51 participants to the 17 research questions and the codes and themes that emerged as a result of these analyzes, the problems faced by SMEs during the pandemic process and some solution suggestions for these problems were revealed. As a result of the findings obtained during
48
A. Konak and A. S. Ünsar
the research and the analysis of these findings, a model proposal has emerged for the problems faced by SMEs during the pandemic process. The model proposal created has been designed to be a roadmap for SMEs in future pandemics and similar situations. Model proposal, as a result of the analyses carried out, was determined that it should be applied in four stages. In this section, the titles of the model proposal are the stages of Information Retrieval, Capital and Finance Management, Customer Relations Management, and Government Support, which were examined. The model proposal of the research does not end with the State Support stage. Model proposal, as shown in Fig. 3.1, is situationally in a loop. Therefore, this model proposal may be as long as the duration of the pandemic and similar conditions. It is designed to be applied indefinitely for SMEs in pandemic and similar situations.
Fig. 3.1 Model proposal
3 A Model Proposal for Solutions to the Problems Faced by Small …
49
The first stage of the model proposal for the solution of the problems faced by SMEs during the pandemic process has been determined as Information Retrieval. The Information Retrieval section aims to reduce the impact of the negative feelings felt by SMEs at the beginning of the pandemic process and to inform SMEs about situations that may develop during the pandemic process. The related codes created in line with the answers given by the participants to the research questions and the code frequencies related to the current solution proposals of these codes are shown in Table 3.10. Information Retrieval, which is the first stage of model proposal, was designed by making use of the Current Solution Suggestions category and general evaluations that emerged as a result of the analysis of the research findings. The second stage of the model proposal for the solution of the problems faced by SMEs during the pandemic process has been determined as Capital and Finance Management. Capital and Financial Management phase, in general, is designed for the enterprise to manage and control its financial power in a balanced way during the pandemic process. It has been observed that businesses experience the most economic problems during the COVID-19 pandemic. For this reason, in the second stage of the model proposal, there are solutions based on capital and finance to provide direct control. Code frequencies of the Capital and Finance Solution Suggestions category, which emerged as a result of the analysis of the research findings, are shown in Table 3.11. Table 3.10 Current solution suggestions code frequencies
Table 3.11 Capital and finance solutions code frequencies
Current solution suggestions
Frequency
Implementing pandemic measures
21
Following the updates
18
Ensuring continuity
15
Benefiting from own experience
13
Learning from nearby businesses
5
Get educated
2
Capital and finance solutions
Frequency
Focusing on basic expenses
20
Receive bank loan
15
Controlled stock management
8
Not taking risks
7
Focusing on diversity and growth
3
Focusing on customer demands
3
Preferring cost-effective products
3
Not to borrow
2
Creating a campaign
2
50 Table 3.12 Solution suggestions for customers code frequencies
A. Konak and A. S. Ünsar
Solution suggestions for customers
Frequency
Customer satisfaction
19
Digitalization and e-commerce
17
Advertisement
6
Home delivery
4
The third stage of the model proposal for the solution of the problems faced by SMEs during the pandemic process has been determined as Customer Relations Management. During the pandemic period, the Customer Relations Management phase comes immediately after controlling the general financial power on behalf of businesses and taking the necessary financial measures. As a result of the analysis of the research findings, the importance of contacting customers effectively and some methods that can be applied during pandemic periods have been reached. The category of Solution Suggestions for Customers, which emerged as a result of the analysis of the research findings, contributed to the formation of the Customer Relations Management, the third stage of the model proposal. Code frequencies of the Solution Suggestions for Customers category are shown in Table 3.12. The fourth and final stage of the model proposal for the solution of the problems faced by SMEs during the pandemic process has been determined as State Support. The reason why State Support is the last stage of the model proposal, first of all, is to provide opportunities for businesses to find their own solutions during pandemic periods and to observe the performance of businesses during these periods and to produce support packages and solutions accordingly. As a result of the analysis of the research findings, the category of State-Based Solution Proposals and the codes within this category contributed to the formation of the State Support phase of the model proposal. The frequencies of the codes belonging to the category of Government-Based Solutions are shown in Table 3.13.
3.7 Conclusion and Recommendations In this chapter, there are final decisions about some of the elements we have determined as a result of the findings we have obtained as a result of the analyses made in the study and the general evaluations. An SME operating in a pandemic or similar process, first of all, should obtain information about his business through the relevant institutions and create a plan in this direction. Such plans to be made by SMEs should be different for every industry, even every business. It has been seen that every business is different in every aspect and a different roadmap should be determined for all businesses. It has been seen that the most critical issues that SMEs should pay attention to during the pandemic process are finance based. Therefore, the issues that SMEs have
3 A Model Proposal for Solutions to the Problems Faced by Small … Table 3.13 Code frequencies based on government solutions
51
State-based solution suggestions
Frequency
Financial support
15
Tax support
8
Determining a specific approach for each sector
7
Vaccination
5
Employee expenses support
5
Rental support
4
Normalization
2
Ensuring compliance with the rules
2
Avoid waste
2
Egalitarian approach
2
Having a strong economy
1
Credit support
1
and will experience the most are finance based. Financial problems that may arise will be managed successfully with the methods specified in the model proposal. During the pandemic period, some problems occur because many SMEs are closed for various reasons and that customers visit the enterprises much less proportionally. Digitalization and e-commerce are especially important elements for the solution of these problems. However, one of the issues that can be considered is to deliver products and services to customers. Delivering products and services to the customer without waiting for the customer to reach the enterprise reduces the problems of SMEs for customers that arise during the pandemic period. Therefore, it has been determined that keeping customer satisfaction at the highest level in pandemic and similar situations is of vital importance for SMEs. It has been revealed that the support to be provided by the public in the pandemic and similar situations that may occur should be planned at the best level. Determining public supports specifically for each enterprise will ensure that pandemics and similar situations are managed in the most efficient way for the state. Determining state supports specifically for each enterprise with high-level planning will bring about meeting the support needs of SMEs in the most efficient way. In the study, it was seen that the most important concept that emerged as a result of the analysis of the research data was the concept of “situational practices during the pandemic period”. Both the measures taken by SMEs and the supports provided by the public should be designed and implemented together with the principles of situational approach. Study: With the analysis of the data obtained, different suggestions and new concepts have emerged. In this direction, new studies on the subject and some suggestions for researchers interested in similar topics are given. Because the literature on the research topic is still developing, the research participants were determined by the maximum variation method and various SME owners were interviewed. It will be necessary to analyze these SMEs separately and to
52
A. Konak and A. S. Ünsar
create more specific models and solution proposals. Model proposals to be developed specifically for each sector and business line; it has been concluded that it will yield much more efficient results for the relevant sectors. It is thought that it would be appropriate to develop the ways businesses will follow in the process of pandemic and similar situations in a situational framework. Therefore, all of the methods to be determined for each business line or sector should be determined from a situational perspective. The research questions directed to the participants were meticulously formed in line with the management functions and the effects of the pandemic process. Therefore, the research questions are used to identify the problems of businesses and offer solutions to these problems in pandemic and similar situations. The form consisting of some demographic questions and 17 research questions can be used in similar situations and adapted to the type of research. This form is suitable for qualitative research. The model proposal, which was obtained with the findings obtained as a result of the analysis of the research data, can be evaluated as a roadmap for SMEs in pandemics and extraordinary situations such as pandemics. Researchers who plan to conduct various research on this subject can benefit from the designed model proposal and rearrange it in line with their own research. Researchers: In order to get permission and advice about the research form and model proposal, the thesis supervisors can contact the specified email addresses.
References Braun V, Clarke V (2006) Using thematic analysis in psychology. Qual Res Psychol 3:77–100 Gourinchas PO, Özcan S.K, Penciakova V, Sander N (2020) COVID-19 and SME Failures. Nber Working Paper Series, 1–54 IDE (2020) Beyond the pandemic: reimagining future entrepreneurship ecosystems. GEN Research ILO (2015) Small and medium-sized enterprises and decent and productive employment creation. International labour office, Geneva ILO (2020) The effects of COVID-19 on trade and global supply chains. Geneva, Switzerland: International labour organization research department. https://www.ilo.org/global/research/pub lications/WCMS_746917/lang--en/index.htm Juergensen J, Guimón J, Narula R (2020) European SMEs Amidst the COVID-19 Crisis: assessing impact and policy responses. J Ind Bus Econ 47:499–510 KOSGEB (2018) Stratejik Plan 2019–2023. Küçük ve Orta Ölçekli ˙I¸sletmeleri Geli¸stirme ve Destekleme ˙Idaresi Ba¸skanlı˘gı Mucuk ˙I (2018) Modern ˙I¸sletmecilik. ˙Istanbul: Türkmen Kitabevi OECD (2019) OECD SME and Entrepreneurship Outlook 2019. OECD Priyono, A., Moin, A, Putri VN (2020) Identifying digital transformation paths in the business model of SMEs during the COVID-19 Pandemic. J Open Innov: Technol, Mark, Complex 6(4):104, 1–22 Qiu W, Rutherford S, Mao A, Chu C (2017) The pandemic and its impacts. Health, Cult Soc 9–10:1–11 Kalkınma Bakanlı˘gı TC (2018) On Birinci Kalkınma Planı. Ankara: T.C. Kalkınma Bakanlı˘gı
3 A Model Proposal for Solutions to the Problems Faced by Small …
53
Sa˘glık Bakanlı˘gı TC (2020) Covid-19 (SARS-CoV-2 Enfeksiyonu) Genel Bilgiler, Epidemiyoloji ve Tanı. Ankara: T.C. Sa˘glık Bakanlı˘gı Halk Sa˘glı˘gı Genel Müdürlü˘gü Thrassou A., Vrontis D, Weber Y, Shams SR, Tsoukatos E (2020) The changing role of SMEs in global business. Cham, Switzerland: Springer Nature WHO (2020) Coronavirus disease 2019 (COVID-19) Situation Report—94. https://apps.who. int/iris/bitstream/handle/10665/331865/nCoVsitrep23Apr2020-eng.pdf?sequence=1&isAllo wed=y Yıldırım A, Sim¸ ¸ sek H (2018) Sosyal Bilimlerde Nitel Ara¸stırma Yöntemleri. Ankara: Seçkin Yayıncılık Yurdakul IK (2013) Kartopu Örneklemesi. In A. A. Kurt, Bilimsel Ara¸stırma Yöntemleri (p. 190). Eski¸sehir: Anadolu Üniversitesi
Ahmet Konak graduated from Beykent University with a Bachelor’s in International Logistics and Transportation Department. He then pursued a Master’s Degree in Entrepreneurship from Trakya University, followed by a doctoral program in Management and Organization, which he is pursuing at the same institution. Konak’s academic interests include Entrepreneurship, Management and Organization, and Strategic Management. He has also contributed to several academic book chapters. In addition, he is the founder of Konak Akademi, which provides high-level consulting services in Entrepreneurship and E-commerce. Agah Sinan Ünsar graduated from Anadolu University Open Education Faculty Business Administration Department in 1990. He worked as a civil servant at Trakya University between 1992– 1998. In 1998, Trakya University. Between 1998-2004, he gave lectures at the faculty as an Instructor. After completing his Ph.D. education, which he started in 1998 at Istanbul University Social Sciences Institute, in 2003, he was appointed to the staff of Assistant Professor at Trakya University ˙I.˙I.B.F. He got the title of Associate Professor in the “Management and Organization” field by successfully passing the Associate Professor exam in 2010. He was appointed as a professor in 2015. He continues working as a lecturer in the business administration department and has taught various undergraduate, graduate, and doctoral courses for 21 years. His areas of expertise are human resource management and organizational behavior. He undertook and completed nearly 25 thesis advisories in his master’s and doctorate education. He also has articles and papers published at the national and international level. He is still the Head of the Department of Management and Organization, Health Management and Entrepreneurship. Ünsar is married and has two children.
Chapter 4
Taxation of Healthcare Sector in India Jagbir Singh Kadyan
Abstract Healthcare has become one of India’s largest sectors, in terms of both revenue and employment. Healthcare comprises hospitals, medical devices, clinical trials, outsourcing, telemedicine, medical tourism, healthcare insurance, and medical equipment. According to Govt. of India’s budget 2021, India’s public expenditure on healthcare stood at 1.2% of the GDP. Most of the healthcare expenses in India are borne by the patients and their families. Healthcare insurance is also gaining momentum in India. By the year 2022, Indian healthcare market is expected to grow threefold, amounting to | 8.6 trillion (US$ 133.44 billion). Taxes in India are levied by the central government and the state government. Some minor taxes are also levied by the local authorities such as the municipalities and local governments. The Government of India has been encouraging the development of healthcare sector by providing various tax incentives, rebates, and deductions from the gross total income to individuals as well as to the public and private organizations. This chapter discusses about the healthcare sector of India, the budgetary allocation and spending towards healthcare sector, taxation of healthcare sector, and the different tax sops and incentives that are provided to the healthcare sector in India. Keywords Healthcare · Taxation · Scientific Research & Development · Corporate Tax · Tax Incentives & Exemptions
Abbreviations AB BE FY FWS GDP
Autonomous Bodies. Budget Estimate. Financial Year Family Welfare Schemes. Gross Domestic Product.
J. S. Kadyan (B) Swami Shraddhanand College, University of Delhi, New Delhi, India e-mail: [email protected] © The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd. 2023 K. T. Çalıyurt (ed.), Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II, Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application, https://doi.org/10.1007/978-981-99-5502-2_4
55
56
J. S. Kadyan
INR MoHFW NASCP NHM PMJAY RE RSBY USD WHO
Indian Rupee Government of India, Ministry of Healthcare and Family Welfare National AIDS & STD Control Program. National Health Mission. Pradhan Mantri Jan Arogya Yojana. Revised Estimates. Rashtriya Swastha Bima Yojna. United States Dollar. World Health Organization
4.1 Introduction to the Healthcare Sector in India It is healthcare that is real wealth and not pieces of gold and silver. Mohandas K. Gandhi.
India is home to several alternative medicine practices such as Yoga, Ayurveda, Unani, Sidha, Homeopathy, and Acupuncture which are popular not only among Indian but also among the foreigners. India’s competitive advantage lies in its large pool of well-trained medical professionals. According to the report of National Investment Promotion & Facilitation Agency’s strategic investment research units report, India: Pharmacy to the World, July 31, 2020, India is one of the largest producers of generic medicines and the pharmaceutical industry is currently the 3rd largest in the world in terms of volume and ranks 14th in terms of value. The Indian pharmaceutical industry is expected to grow to US$ 100 billion by the end of 2025. Pharmaceutical exports from India stood at USD 16.3 billion in FY 2019–20. The Indian health sector is projected to increase threefold to INR | 8.6 trillion (US$ 133.44 billion) by 2022. Also, India has emerged as a popular destination for medical travel. The industry now has some of the best world-class medical equipment, infrastructure, and doctor. India presently has around 18% of the global medical tourism market. The government is attempting to expand the industry by making it easier for tourists to travel to the country for medical treatment. After all, India has cutting-edge medical facilities, respected healthcare professionals, top-notch nursing care, and traditional medicinal treatments. The Indian biotechnology industry was valued at US$ 64 billion in 2019 and is expected to reach US$ 150 billion by 2025. During the year 2020, the gross direct premium income underwritten by healthcare insurance grew 17.16% on the year-toyear basis amounting to INR | 51,637.84 crore (US$ 7.39 billion). India also has the largest number of manufacturing sites approved by the United States Food and Drug Administration outside of the USA. According to the economic survey report 2019–20 and a report published in Deccan Herald (Deccan Herald, Jan 31, 2020), the (allopathic doctor) doctorpopulation ratio in India is 1:1456 against the WHO recommendation of 1:1000.
4 Taxation of Healthcare Sector in India
57
Healthcare sector in India mainly comprises of the following segments which are publicly as well as privately owned. • Hospital Segment: While the government healthcare includes government healthcare centers, district hospitals, and general hospitals, the private healthcare includes nursing homes, mid-tier and top hospitals. • Pharmaceutical Segment includes a manufacturing, extraction, processing purification, and packaging of chemical materials for use of medication. • Diagnosis Segment includes businesses and laboratories that offer analytical or diagnostic services including body fluid analysis. • Medical Equipment & Supplies Segment includes establishments primarily manufacturing medical equipment and supplies like surgical, dental, orthopedic, ophthalmologic, laboratory instruments, etc. • Medical Insurance Segment includes healthcare insurance and medical reimbursement facilities covering an individual’s hospitalization expenses incurred due to sickness. • Tele Medicine Segment has enormous potential in meeting the challenges of healthcare delivery to rural and remote areas besides several other applications in education training and management in healthcare sector services. Among the prominent ministries and departments of the Government of India, Ministry of Healthcare and Family Welfare (MoHFW) caters to the needs of healthcare sector as well as family welfare in India through its two departments, viz. Department of Healthcare and Family Welfare and Department of Healthcare Research. While the Department of Healthcare and Family Welfare is responsible towards implementing healthcare schemes, and regulating medical education and training, the Department of Healthcare Research is broadly responsible for conducting medical research. The revised estimate in 2020–21 (| 82,928 crore) includes | 14,217 crore for COVID-19 emergency response and healthcare system preparedness package, and COVID-19 vaccination for healthcare and frontline worker. According to above Chart 4.1, Budgetary allocation of Ministry of Health and Family Welfare, during the year 2019–20, the Ministry of Healthcare and Family Welfare had received a budgetary allocation of | 64,258 crore (| 642,580 million), out of which | 62,397 crore (| 623,970 million) were for Health and Family Welfare Department and | 1,861 crore (| 18,610 million) were for Health Research Department. During the year 2020–21, the Ministry of Healthcare and Family Welfare had received a budgetary allocation of | 82,928 crore (| 829,280 million), out of which, | 78,866 crore (| 788,660 million) were for Health and Family Welfare Department and | 4,062 crore (| 40,620 million) were for Health Research Department. It is worth noting that the revised estimate during the year 2020–21 (| 82,928 crore) (| 829,280 million) includes | 14,217 crore (| 142,170 million) for COVID-19 emergency response and healthcare system preparedness package, and COVID-19 vaccination for healthcare and frontline worker.
58
J. S. Kadyan
Chart 4.1 Budgetary allocation of Ministry of Health and Family Welfare (in | crore) (Note BE—Budget Estimate; RE—Revised Estimates. Sources Expenditure Budget 2021–22; PRS)
During the year 2021–22, the Ministry of Healthcare and Family Welfare had received a budgetary allocation of | 73,932 crore (| 739,320 million), out of which, | 71,269 crore (| 712,690 million) were for Health and Family Welfare Department and | 2,663 crore (| 26,630 million) were for Health Research Department (Chart 4.2). During the year 2019–20, the budgetary allocation of funds allocation for the Ministry of Health & Family Welfare (MoHFW) was | 64,258 crore (| 642,580 million). MoHFW allocated | 62,397 crore (| 623,970 million) to the Department of Health & Family Welfare and | 1,861 crore (| 18,610 million) to the Department of Health Research. Both the departments of MoHFW, viz. Department of Health & Family Welfare and Department of Health Research, have allocated their funds as under. While the highest allocation of 54% amounting to | 34,660 crore (| 346,600 million) was done towards National Health Mission (NHM), which was allocated to National Rural Health Mission; National Urban Health Mission; Tertiary Care programs; Strengthening of State Drugs Regulatory System; and Human Resources for Health & Medical Education. The lowest allocation of 0.09% amounting to |57 crore (| 570 million) was found to be done towards Rashtriya Swasthya Bima Yojna. During the year 2020–21 BE, the budgetary allocation of funds allocation for the Ministry of Health & Family Welfare (MoHFW) was | 82,928 crore (| 829,280 million). MoHFW allocated | 78,866 crore (| 788,660 million) to the Department of Health & Family Welfare and | 4,062 crore (| 40,620 million) to the Department of Health Research. Both the departments of MoHFW, viz. Department of Health &
4 Taxation of Healthcare Sector in India
59
Chart 4.2 Allocation of funds towards healthcare by MoHFW (Note During the year 2021 RE, |23,860 under the head “Others” includes | 14,217 crore towards COVID-19 emergency response and vaccination of healthcare and frontline worker. Source Ministry of Health and Family welfare, Govt. of India. https://www.mohfw.gov.in/)
Family Welfare and Department of Health Research, have allocated their funds as under. While the highest allocation of 42% amounting to | 35,144 crore (| 351,440 million) was done towards National Health Mission (NHM), which was allocated to National Rural Health Mission; National Urban Health Mission; Tertiary Care programs; Strengthening of State Drugs Regulatory System; and Human Resources for Health & Medical Education. The lowest allocation of 0.03% amounting to |29 crore (| 290 million) was found to be done towards Rashtriya Swasthya Bima Yojna. During the year 2021–22 BE, the budgetary allocation of funds allocation for the Ministry of Health & Family Welfare (MoHFW) was | 73,932 crore (| 739,320 million). MoHFW allocated | 71,269 crore (| 712,690 million) to the Department of Health & Family Welfare and | 2,663 crore (| 26,630 million) to the Department of Health Research. Both the departments of MoHFW, viz. Department of Health & Family Welfare and Department of Health Research, have allocated their funds as under. While the highest allocation of 49% amounting to | 36,576 crore (| 365,760 million) was done towards National Health Mission (NHM), which was allocated to National Rural Health Mission; National Urban Health Mission; Tertiary Care programs; Strengthening of State Drugs Regulatory System; and Human Resources for Health & Medical Education. The lowest allocation of 0.001% amounting to |01 crore (| 10 million) was found to be done towards Rashtriya Swasthya Bima
60
J. S. Kadyan
Chart 4.3 Actual utilization of Budget by Department of Healthcare and Family Welfare (2010–11 to 2020–21) (Source https://prsindia.org/budgets/parliament/demand-for-grants-2020-21-analysishealth-and-family-welfare)
Yojna. During this year, additional funds were allocated two heads, viz., COVID19 emergency response and health system preparedness package, amounting of | 13,857 crore (| 138,570 million) (18.74%), and COVID-19 vaccination for healthcare worker and frontline worker, amounting | 360 crore (| 3 600 million) (0.48%). According to above Chart 4.3: actual utilization of budget by Department of Healthcare and Family Welfare (2010–11 to 2020–21), It is observed that, from the period from 2010–11 to 2014–15, the Department of Healthcare and Family Welfare had not utilized their budgets fully, but from the year 2016–17 onward the department has utilized their budget fully and overshot the budget by 12% in 2015–16, 2% in 2016–17, 9% in 2017–18, and 21% in 2020–21. Healthcare sector in India is growing at a tremendous pace owing to its strengthening coverage, services, and increasing expenditure in the healthcare sector by the public as well as private organizations. There has been a rising demand for affordable healthcare delivery systems due to the increasing healthcare costs, technological advancements, the emergence of new diseases, and pandemics. According to the above Chart 4.4, Growing Trends of India’s Healthcare Sector (US$), healthcare sector in India has been witnessing a growing trend and it is expected to record a CAGR of 17.69%. Healthcare sector has become one of the largest contributing sectors in terms of revenue and employment generation in India. This sector is growing at a rapid pace owing to its strengthening coverage, service, and increasing expenditure by public as well private player by the year 2022. It is estimated that, by the year 2020, it shall reach to US$ 193.83 billion, and by the year 2000, it is estimated to reach US$ 372 billion (Chart 4.5). According to Table 4.5., Government Healthcare Expenditure as a Percentage of GDP, above, Government Healthcare Expenditure has been witnessing a steady growing trend. It has witnessed a rise from 1.2% of the GDP in the year 2014 to
4 Taxation of Healthcare Sector in India
61
Chart 4.4 Growing Trends of India’s Healthcare Sector (US$) (Note F-Forecast. Source Frost and Sullivan, LSI Financial Services, Deloitte)
Chart 4.5 Government Healthcare Expenditure as a Percentage of GDP (Note BE-Budgeted Estimate, RE-Revised Estimate. Source World Bank, Economic Survey 2020)
1.8% in the year 2020. It is expected to rise at a level of 19.7% of the GDP by the year 2027. In the budget for the year 2021, India’s public expenditure on healthcare was 1.2% of the GDP and the government is planning to increase the public healthcare spending to 2.5% of the GDP by 2025. This ambitious goal/target of the government seems possible because, over a period of time, greater penetration of affordable healthcare insurance services augmented to the rise in healthcare spending, a trend which is likely to be intensified further in the coming year. Due to the growth of Indian economy, the incomes in the hands of its citizens are raising and the quality of life has been improving. It has become easier to have access to high-quality healthcare services and facilities and there is greater awareness among people with regard to personal healthcare and hygiene. Besides, the economic prosperity is also leading to the improvement in affordability for generic medicines in the market. According to Chart 4.6 above, direct jobs in Indian healthcare sector, direct job for Allopathic doctors are estimated to rise to 621 million by the year 2022 as compared to 494 million in the year 2017. The healthcare specialists’ direct jobs are estimated to rise to 311 million by the year 2022 as compared to 248 million in the year 2017.
62
J. S. Kadyan
Chart 4.6 Direct Jobs in India’s Healthcare Sector. 2017–2022 (Note The 2022 estimates for nurses and midwives may be high given the limited capacity to train and deploy an additional 1.9 million nurses and midwives in a 5-year period. Source Ministry of Skill Development & Entrepreneurship)
Dentists’ direct jobs are estimated to rise to 88 million by the year 2022 as compared to 111 million in the year 2017. Nurses and midwives’ direct jobs are estimated to rise to 3645 million by the year 2022 as compared to 1753 million in the year 2017. Pharmacists’ direct jobs are estimated to rise to 377 million by the year 2022 as compared to 300 million in the year 2017 and similarly, the other healthcare professionals’ direct jobs are estimated to rise to 2332 million by the year 2022 as compared to 1855 million in the year 2017. NSDC - National Skill Development Council has estimated that the healthcare sector will directly employ around 7.5 million people by 2022, adding approximately 2.7 million new jobs between the yea| 2017 and 2022—over 500,000 new jobs per year (Chart 4.7). Out-of-pocket expenditures are the payments that are done directly by an individual at any point of service where the entire cost of the healthcare service is not covered under any financial protection schemes.
Chart 4.7 Major out-of-pocket healthcare expenditures (Source Economic Survey Report 2020– 21)
4 Taxation of Healthcare Sector in India
63
According to the Economic Survey Report 2020–21, the overall out-of-pocket expenses in India on healthcare is around 60% of the total expense done towards the public healthcare expenditures (which is one of the highest in the world). The highest portion of the out-of-pocket expenditures in India is found to be done towards pharmacies attributing 47% followed by 31% towards private medical facilities and 8% towards government general hospital. The lowest portion of 7% each has been found to be done towards medical and diagnosis. The survey also highlights that increasing the spending on public healthcare from 1% of the GDP to 2.5–3% of GDP will help in reducing the out-of-pocket expenses from 60 to 30%.
4.2 Taxation of Healthcare Sector in India Overview of Taxation in India The central government and the state government both levy taxes in India. Local authorities, such as municipalities and local governments, levy a variety of minor taxes. Taxes in India can be broadly classified into the following two categories. • Direct Taxes: These taxes are levied on incomes of individuals, corporate, and all other entities as defined under Section 4.2(31) of the Income Tax Act 1961. Direct taxes are imposed by the central government, state government, and municipalities and local authorities. • Indirect Tax: These taxes are levied on transactions related to goods and services and are paid by the transacting entities to the central government, state government, and municipalities and local authorities, depending on the locations, uses as well as the nature of the goods and services. Government of India constantly attempts to reduce the burden of taxes on the healthcare care and medical expenditure by way of giving tax exemptions and soaps under direct taxes as well as indirect taxes, viz. Income Tax as well as GST—Goods & Service Tax. Even though healthcare care services are exempted from taxes, following healthcare care services are taxable under GST: sale of medicines, tests done from outside accredited laboratory and giving consultancy, food supply to attendants or visitors or outpatients on chargeable basis, consultancy fees paid to senior doctors, and rental income of the hospital from giving premises on rent (Table 4.1). Direct Tax Income earning entities in India are subject to payment of income tax as per Income Tax Act 1961. The applicability and the quantum of the tax largely depend upon the nature, type, location, time, and the sources of the income earned. According to Section 4.2(31), the direct taxpayer entity could be anyone of the following. • Individual • Hindu Undivided Family (HUF)
64
J. S. Kadyan
Table 4.1 Taxation in India Type of Tax
Taxes by Central Government
Taxes by State Government
Direct Tax: Levied on Incomes of Individuals, Corporate and all other entities
1. Income Tax: Tax on income of a person Tax on Salaries Tax on income from House Property Tax on Capital Gains Tax on Profits and Gains from Business and Profession Tax on Other Income
1. Stamp Duty and Registration: Levied for the transaction performed by way of sale /purchase/ lease/ conveyance deed, etc 2. Property Tax: Levied generally by the of municipalities or local authorities
Indirect Tax: Levied on transactions related to goods and services. It is collected and paid by transacting entities selling goods or services
1. Customs Duties: Duties on Import and Export of goods 2. Central Good & Service tax: Taxes on provision of Services and Supply of Goods 3. Integrated Good & Service tax: Tax on Interstate Supply of Goods and Services 4. Central Excise: Taxes on Alcohol for human consumption and Petroleum Products
1. State Good & Service tax: Taxes on provision of services and supply of goods 2. Value Added Tax (VAT): Taxes on Alcohol for human consumption and Petroleum Products
*
• • • • • •
Alcohol for human consumption and Petroleum products
Body of Individuals (BOI) Association of Persons (AOP) Local Authorities Corporate Firms Companies Any Artificial Juridical Persons
There are different income tax rates applicable to different entities as mentioned above. Few of these entities have been discussed below. Individuals and HUF earning up to INR 2.5 Lakhs in the previous year are exempted from the liability of paying income tax. However, if the income exceeds INR 2.5 lakhs during the previous year, following income tax rates shall be applicable (Table 4.2).
4 Taxation of Healthcare Sector in India
65
Table 4.2 Income tax slab rate applicable for New Tax regime – FY 2020–21 Income Tax Slab
New Regime Income Tax Slab Rates for FY 2020–21 (Applicable for All Individuals & HUF)
| 0.0 – | 2.5 Lakhs
NIL
| 3.00 lakhs – | 5.00 Lakhs
5% (tax rebate u/s 87a is available)
| 5.00 lakhs- | 7.5 Lakhs
10%
| 7.5 lakhs – | 10.00 Lakhs
15%
| 10.00 lakhs – | 12.50 Lakhs
20%
| 12.5 lakhs- | 15.00 Lakhs
25%
> | 15 Lakhs
30%
| 5.00 lakhs- | 7.5 Lakhs
10%
Source https://www.canarahsbclife.com/tax-university/articles/what-is-the-income-tax-slab-for2020-21.html
4.2.1 Individuals Income Tax Rates: Individuals & HUF In addition to above income tax, • Additional healthcare and education cess at the rate of 4% will be added to the income tax liability in all cases (increased from 3% since FY 18–19). • Surcharge applicable as per tax rates below in all categories mentioned above: 10% of Income tax if total income > |50 lakh 15% of Income tax if total income > |1 crore 25% of Income tax if total income > |2 crore 37% of Income tax if total income > |5 crore
4.2.2 Corporate Income Tax Rates Corporate entities for the purpose of taxation have been broadly classified into two categories, viz. domestic company as well as foreign company. The taxes applicable on these different types of companies are explained as follows (Table 4.3).
4.2.2.1
Domestic Company
In addition to above income tax, Surcharge and Cess shall be applicable as mentioned below: (a) Surcharge: The amount of income tax shall be increased by a surcharge at the rate of 7% of such tax, where total income exceeds one crore rupees but not exceeding ten crore rupees and at the rate of 12% of such tax, where total income exceeds ten crore rupees.
66
J. S. Kadyan
Table 4.3 Income tax rates applicable in case of domestic companies for assessment year 2021–22 and 2022–23 are as follows: Domestic Company
Assessment Year 2021–22
Assessment Year 2022–23
♦ Where its total turnover or gross receipt during the previous year 2018–19 does not exceed | 400 crore
25%
NA
♦ Where its total turnover or gross receipt during the previous year 2019–20 does not exceed | 400 crore
NA
25%
♦ Any other domestic company
30%
30%
Source:https://incometaxindia.gov.in/pages/domestic-company-specific-content.aspx
The surcharge shall be subject to marginal relief, which shall be as under: Where income exceeds | 1 crore but not exceeding | 10 crore, the total amount payable as income tax and surcharge shall not exceed total amount payable as income tax on total income of | 1 crore by more than the amount of income that exceeds | 1 crore. Where income exceeds | 10 crore, the total amount payable as income tax and surcharge shall not exceed total amount payable as income tax on total income of | 10 crore by more than the amount of income that exceeds | 10 crore. (b) Healthcare and Education Cess: The amount of income tax and the applicable surcharge shall be further increased by healthcare and education cess calculated at the rate of four percent of such income tax and surcharge. Note: The Government of India has introduced the Taxation (Amendment) Ordinance Act, 2019, on September 20, 2019. Section 115BAA and Section 115BAB were inserted in the Income Tax Act, 1961, by the Finance Minister, Ms. Nirmala Sitharaman, in the Union Budget 2020, in order to give benefit of the reduced tax rate of the domestic companies. While existing domestic companies have been provided an option to pay tax at a concessional rate of 22%, new domestic companies set up on or after October 1, 2019, and commencing manufacturing before March 31, 2023, would have the option to pay tax at 15% (Table 4.4) Special Tax Rates Applicable to a Domestic Company In addition to above income tax, Surcharge and Cess shall be applicable as mentioned below: a) Surcharge: The rate of surcharge in case of a company opting for taxability under Section 115BAA or Section 115BAB shall be flat 10% irrespective of amount of total income. b) Healthcare and Education Cess: The amount of income tax and the applicable surcharge shall be further increased by healthcare and education cess calculated at the rate of four percent of such income tax and surcharge.
4 Taxation of Healthcare Sector in India
67
Table 4.4 Special income tax rates applicable in case of domestic companies for assessment year 2021–22 and 2022–23 are as follows: Domestic Company
Assessment Year 2021–22 Assessment Year 2022–23
♦ Where it opted for Section 115BA
25%
25%
♦ Where it opted for Section 115BAA 22%
22%
♦ Where it opted for Section 115BAB
15%
15%
Source https://incometaxindia.gov.in/pages/domestic-company-specific-content.aspx
c) MAT—Minimum Alternate Tax: The domestic company who has opted for special taxation regime under Section 115BAA & 115BAB is exempted from provision of MAT. However, no exemption is available in case where Section 115BA has been opted. Note: In that case, the provisions of Minimum Alternate Tax (MAT) applies, tax payable cannot be less than 15% (+HEC) of “Book profit” computed as per Section 115JB. However, MAT is levied at the rate of 9% (plus surcharge and cess as applicable) in case of a company, being a unit of an International Financial Services Centre and deriving its income solely in convertible foreign exchange.
4.2.2.2
Foreign Company
In the case of a foreign company, the applicable income tax rates shall be as under. Assessment Year 2021–22 and Assessment Year 2022–23 (Table 4.5). In addition to above income tax, Surcharge and Cess shall be applicable as mentioned below. a) Surcharge: The amount of income tax shall be increased by a surcharge at the rate of 2% of such tax, where total income exceeds one crore rupees but not exceeding ten crore rupees and at the rate of 5% of such tax, where total income exceeds ten crore rupees. However, the surcharge shall be subject to marginal relief, which shall be as under: Table 4.5 Income tax rates applicable to foreign companies for assessment years 2021–22 & 2022–23 Nature of Income
Tax Rate
Royalty received from government or an Indian concern in pursuance of an agreement 50% made with the Indian concern after March 31, 1961, but before April 1, 1976, or fees for rendering technical services in pursuance of an agreement made after February 29, 1964, but before April 1, 1976, and where such agreement has, in either case, been approved by the Central Government Any other income Source https://incometaxindia.gov.in/pages/foreing-company-specific-content.aspx
40%
68
J. S. Kadyan
• Where income exceeds one crore rupees but not exceeding ten crore rupees, the total amount payable as income tax and surcharge shall not exceed total amount payable as income tax on total income of one crore rupees by more than the amount of income that exceeds one crore rupees. • Where income exceeds ten crore rupees, the total amount payable as income tax and surcharge shall not exceed total amount payable as income tax on total income of ten crore rupees by more than the amount of income that exceeds ten crore rupees. b) Healthcare and Education Cess: The amount of income tax and the applicable surcharge shall be further increased by healthcare and education cess calculated at the rate of four percent of such income tax and surcharge.
4.3 Income Tax Deduction Available Towards Healthcare The various income tax deductions available to an individual assessee towards medical and healthcare expenses are provided under Section 80D, 80DD, and 80DDB of Income Tax Act 1961.
4.3.1 Section 80D: Deduction for Premium Payment Towards Healthcare Insurance Policy When Parents Are Senior Citizen Section 80D of the Income Act provides an increased deduction of |50,000 in case any parent of the assessee is senior citizen. An individual resident in India of the age of 60 year or more at any time during the relevant previous year is treated as a senior citizen.
4.3.2 Deduction in Respect of Payment Towards Preventive Healthcare Check-Up Section 80D of the IT Act allows a deduction of up to |5,000 in respect of payment made towards preventive healthcare check-up of self, spouse, dependent children, or parents made during the previous year. Cash may be used to pay for the preventive healthcare check-up. The deduction of |5,000 is counted within the overall limit of |25,000 or |50,000 as the case may be.
4 Taxation of Healthcare Sector in India
69
4.3.3 Deduction in Respect of Expenses Towards Medical Treatment Section 80DDB allows tax deduction on expenses incurred by an individual on himself or a dependent towards the treatment of specific diseases as stated in the act. The deduction amount can be availed for the sum actually paid or |40,000, whichever is lower. The maximum deduction amount in case of a senior citizen is |1 lakh. The amount of deduction shall be reduced by the amount paid by an insurance company or reimbursed by the employer.
4.3.4 Deduction for Medical Treatment of a Dependent Person with Disability Sections 80DD of the Income Tax Act cove| deduction for the medical expenditure incurred for self or for a dependent person. A dependent person can be spouse, children, parents, brothers, and the sisters of the assessee. A deduction up to maximum of |75,000 will be allowed under the section. The maximum deduction limit increases to |1.25 lakh in case of cases of severe disability. Severe disability means where the disability percentage is 80% or more.
4.3.5 Section 80G: Deduction for Donation and Contribution Made Contributions made to certain relief funds and charitable institutions can be claimed as a deduction under Section 80G of the Income Tax Act.1 All donations, however, are not eligible for deductions under Section 80G. Only donations made to prescribed funds qualify as a deduction. This deduction can be claimed by any taxpayer— individuals, company, firm, or any other person.
1
Income Tax India, Deduction in respect of donations to certain funds, charitable institutions, etc. https://incometaxindia.gov.in/_layouts/15/dit/pages/viewer.aspx?grp=act&cname=cmsid&cval= 102120000000075772&searchfilter=%5B%7B%22crawledpropertykey%22:1,%22value%22:% 22act%22,%22searchoperand%22:2%7D,%7B%22crawledpropertykey%22:0,%22value%22:% 22income-tax+act,+1961%22,%22searchoperand%22:2%7D,%7B%22crawledpropertykey%22: 29,%22value%22:%222020%22,%22searchoperand%22:2%7D%5D&k=&isdlg=0.
70
J. S. Kadyan
4.3.6 Section 80GGA: Donations Towards Scientific Research or Rural Development Donations made towards scientific research or rural development to approved institutions and funds are eligible for deductions u/s 80GGA of the Income Tax Act. This deduction is allowed to all assessees except those who have an income (or loss) from a business and/or a profession. 100% of the amount that is donated or contributed is considered eligible for deductions. The donations eligible for deductions under Section 80GGA are as mentioned below. • Any sum paid to a research association which undertakes scientific research, or a sum paid to a college, university, or any other institution to be used for scientific research that is all approved by the prescribed authority under Section 35(1) (ii). • Sum paid to a research association which undertakes research in social science or statistical research, or sum paid to a college, university, or any other institution to be used for the same purpose, and these must all be approved by the prescribed authority under Section 35(1) (iii). • Sum paid to an approved association or institution which undertakes any program of rural development and is approved under Section 35CCA. • Sum paid to an approved association or institution which undertakes training of person(s) for implementing programs of rural development. • Sum paid to a public sector company, local authority, or an approved association or institution which carries out projects or schemes approved under Section 35AC. • Sum paid to notified Rural Development Fund. • Sum paid to notified Fund for Afforestation. • Sum paid to notified National Poverty Eradication Fund. • If a deduction has been allowed under Section 80GGA, such expenses shall not be deductible under any other provision of the Income Tax Act. The other income tax deductions available to the assessees in the form of deductions and incentives have been discussed separately under the heading, “Income tax incentives to the Healthcare Sector”, in the following part of this chapter. These include relevant contents of Sections 10, 11, 12, 35 and Section 80 of the Income Tax Act 1961 pertaining to healthcare.
4.4 Indirect Tax—GST—Goods & Services Tax Act 2017 GST is known as the Goods and Services Tax. It is an indirect tax which has replaced many indirect taxes in India such as the excise duty, VAT, purchase tax, and sales tax. The GST journey began in the year 2000 when a committee was set up to draft law. It took 17 years from then for the law to evolve. The Goods and Service Tax Act was passed in the parliament on March 29, 2017, and came into effect on July 1, 2017.
4 Taxation of Healthcare Sector in India
71
Goods and Service Tax (GST) is levied on the supply of goods and services. Goods and Services Tax Law in India is a comprehensive, multi-stage, destination-based tax that is levied on every value addition. GST is a single domestic indirect tax law for the entire country. Goods and Service Tax (GST) comprises of three components, namely CGST— Central Goods and Service Tax; SGST—State Goods and Service Tax; and IGST— Interstate Goods and Service Tax. i. CGST: It is the tax collected by the central government on an intra-state sale. It is a tax on the transactions happening within a state of India. ii. SGST: It is the tax collected by the state government on an intra-state sale. It is a tax on the transactions happening within a state of India. iii. IGST: It is a tax collected by the central government for an inter-state sale. It is a tax on the transactions happening in-between any of the two states of India.
4.4.1 Chargeability of GST on Healthcare Sector Following are the Healthcare services which are chargeable to tax under the GST. i. Sale of Medicines is Taxable under GST. Although most of the medicines are taxed at 5% under GST laws, few are also taxed at 12% and some at 18%. We need to identify the HSN of the medicines/consumables / injectables and implants to ascertain the rate of tax applicable to them. If medicines are purchased for resale, then ITC is available, and sale would attract tax. ii. In an establishment, tests done from outside accredited laboratory and giving consultancy are not clinical establishment, and hence, tax exemption is not available. iii. Food supply to attendants or visitors or outpatients on chargeable basis is not exempted. Further, tax is payable by supplier of foods if supply of food is outsourced. iv. Tax payable if hospital gives part of premises on rent—GST is applicable on any rent paid/payable for the premises given on rent/lease by a hospital. v. GST is applicable on any amounts paid to doctors, who are not on the payroll, but are paid on consultation basis by the hospitals.
72
J. S. Kadyan
4.5 GST Exemption Available Towards Healthcare Services. Following healthcare services are exempted from Goods and Services Tax i) Healthcare Services by a Clinical Establishment or Authorized Medical Practitioner or Paramedics. The above-mentioned terms have been defined / clarified by GST Notification No. 9/2017- Integrated Tax (Rate) dated 28.06.2017; vide entry no 77. There are four terms used as per the said notification: healthcare services; clinical establishment; authorized medical practitioner; and paramedics. We need to understand these terms appropriately in order to claim tax exemptions under the GST. ii) Healthcare Care Services: The said notification defines healthcare care services as any service by way of diagnosis or treatment or care for illness, injury, deformity, abnormality, or pregnancy in any recognized system of medicines in India and includes services by way of transportation of the patient to and from a clinical establishment, but does not include hair transplant or cosmetic or plastic surgery, except when undertaken to restore or to reconstruct anatomy or functions of body affected due to congenital defects, developmental abnormalities, injury. Thus, all treatments excluding cosmetic treatments have been covered by this definition. iii) Clinical Establishment: As per the said notification, meaning of clinical establishment is: – Clinical establishment means a hospital, nursing home, clinic, sanatorium, or any other institution by whatever name called that offers services or facilities requiring diagnosis or treatment or care for illness, injury, deformity, abnormality, or pregnancy in any recognized system of medicines in India, or a place established as an independent entity or a part of an establishment to carry out diagnostic or investigative services of diseases. iv) Authorized Medical Professional: As per the said notification, authorized medical professional means: – A Medical practitioner registered with any of the councils of the recognized system of medicines established or recognized by law in India and includes a medical professional having the requisite qualification to practice in any recognized system of medicines in India as per any law for the time being in force. The definition of authorized medical professional brings out the following prerequisites: • Practitioner should be registered with any medical council. • Practitioner should have requisite qualification to practice. • Such qualification should be of any system of medicine recognized in India.
4 Taxation of Healthcare Sector in India
73
The recognized medical systems in India are - Allopathic, Ayurveda, Siddha, Unani, Homeopathy, Yoga, and Naturopathy. Accordingly, qualified doctors hold recognized degrees in any of the above systems and are registered with their respective medical councils. v) Paramedics: These are trained healthcare professionals such as nursing staff, physiotherapists, technicians, and lab assistants. They are accountable for their services when provided independently and therefore exempt. Services by them in a clinical establishment would be in the capacity of employee and not provided in independent capacity and will thus be considered as services by such clinical establishment. Similarly, services of assisting an authorized medical professional would be considered as services by such authorized medical professional only. vi) Services Provided by Veterinary Doctors: (Entry no 48): This entry exempts services in relation to healthcare of animals and birds from GST. This entry does not have any prerequisite with regard to qualification, recognition, or affiliation of veterinary doctors. vii) Blood Banks: (Entry no 76): Cord Blood Banks include other Blood Banks and thus the services provided by Cord/Other Blood Bank for preservation of stem cells or any other services for such preservation are covered in Entry No: 76 and are thus exempted from the payment of GST. viii) Ambulance Services: (Entry no 77): Providing of ambulance services is also exempt from the ambit of GST. GST is not applicable on ambulance services provided to government under National Healthcare Mission. ix) Medical Tests: (Entry no 77): Medical tests (either done in own clinical establishment or done in the separate clinical establishment setup especially for such test) are covered in entry no. 77 and are thus exempted from payment of GST. x) Bio Medical Waste: (Entry no 78): This entry excludes unconditionally services provided by operators of the common biomedical waste treatment facility to a clinical establishment by way of treatment or disposal of biomedical waste or the processes incidental thereto. Thus, services provided to hospitals by way of treatment and disposal of bio medical waste are exempted from the payment of GST. xi) Room Rent for Patient (Entry no 77): Room rent charged from the patients is exempted from the payment of GST.
74
J. S. Kadyan
xii) Bundled Healthcare Care Services Provided by the Hospitals: Combinations of multiple interlinked healthcare services which cannot be segregated and are provided by a hospital to its patients are exempted from GST. xiii) Retention Money Kept by Hospital from Payments to Consultants/ technicians. In some cases, hospital allows private doctors to use consulting rooms in hospitals. The patient pays fees to hospital out of which hospital pays certain amount to the private doctor/technician. The amount retained by the hospital is towards providing ancillary services like infrastructure, nursing, paramedic care, emergency services, etc. Such retention money is exempted from payments of GST. xiv) Services Provided by Rehabilitation Professionals. Rehabilitation professionals recognized under the Rehabilitation Council of India Act, 1992, by way of rehabilitation, therapy, or counseling and such other activity as covered by the said Act at medical establishments, educational institutions, rehabilitation centers established by central government, state government, or union territory or an entity registered under Section 4.12AA of the Income Tax Act, 1961 (43 of 1961) are exempt w.e.f. 1–1-2019.
4.6 Tax Incentives and Deductions Available Towards Healthcare Under Income Tax Act 1961 Income Tax Act 1961 provides various incentives, rebates, deduction, and concessions for the healthcare sector in India. We shall be discussing the prominent sections of Income Tax Act which incentivizes the healthcare sector in India. The prominent sections related to healthcare sector discussed are Sections 4.10(23C), 11, 12, 35, and 80(IB) of the Income Tax Act 1961. i) Section 10(23C) of the Income Tax Act is a specific exemption available to certain government and non-government universities and educational institutions. Income received by any university or educational institution existing solely for educational purposes and not for purposes of profit, and which is wholly or substantially financed by the government is fully exempt from tax vide Section 4.10(23C)(iiiab). Hence, a government educational institution is fully exempt from income tax without any separate approvals as long as it is not for profit purpose. The exemption for non-government (private) educational institutions depends upon the aggregate annual receipts of the university / educational institution.
4 Taxation of Healthcare Sector in India
75
ii) Educational Institutions/medical Institution with Annual Receipts up to | 5 Crore: Section 4.10(23C) (iiiad) provides that the income earned by any university or educational institution existing solely for educational purposes and not for the purposes of profit shall be exempt from tax if the aggregate annual receipts of such university or educational institution do not exceed | 5 crore. Thus, an educational institution having receipts up to | 5 crore can claim full exemption under the above clause without requiring a separate approval or registration. Here, it is important to note that the term “annual receipts” has not been defined under the law. Keeping in mind the intention of the provisions, annual receipts should mean receipts from the various fees and charges collected by the institution. It can also include the receipts from donations. iii) Educational Institutions/medical Institution with Annual Receipts Exceeding | 5 Crore: Exemption in the case of an educational institution having receipts exceeding | 5 crore is governed by Section 4.10(23C)(vi) which states that income earned by any university or other educational institution existing solely for educational purposes and not for purposes of profit, other than those mentioned in sub-clause (iiiab), shall be exempt if they are approved by the prescribed authority. Thus, where the aggregate receipt of the institution exceeds | 1 crore, the institution needs a separate approval for claiming the exemption u/s 10(23C). iv) Section 11 of the Income Tax Act—Exemption for Trusts Income received from a charitable/religious trust will be tax exempt under Section 4.11, provided that the activity being performed is incidental to the trust/ institution’s objectives and a separate set of books of accounts is kept by the trust/ institution. Conditions for Availing Exemption under Section 11 In order to avail exemption under Section 4.11 of the Income Tax Act,2 the following conditions must be satisfied: • The creation of the trust must be done for the fulfillment of a lawful purpose. The establishment of the trust must be for charitable purposes, precisely what Section 4.11 deals with. According to Section 4.2(15), charitable purpose includes relief of the poor; education; yoga; medical relief; preservation of the environment; and preservation of monuments or places or objects of artistic or historic interest; and the advancement of any other object of general public utility (Charitable Purpose, 2021). 2
Income Tax India, Section 4.11, https://incometaxindia.gov.in/Pages/i-am/trust.aspx?k=Exempt ions.
76
J. S. Kadyan
• Exemptions to Hospitals If an assessee is running a hospital for a humanitarian cause, income tax shall be exempted. The same exemption is applicable to a foundation running a hospital for a similar cause. • Providing Financial Assistance Any establishment of the assessee providing financial assistance to schools, colleges, or any educational institutions is exempt under Section 4.11 of the Income Tax Act, 1961. • Running a School/College A society which is running a school/college is granted an exemption under Section 4.11 of the Income Tax Act, 1961. v) Section 12 of the Income Tax Act: Income of Religious Trusts or Institutions from Voluntary Contributions. Any voluntary contribution received by a trust or institution formed wholly for charitable or religious purposes (not being contributions made with a specific direction that they shall form part of the corpus of the trust or institution) shall be deemed to be the income received for charitable or religious purposes from property held under trust wholly and will qualify for exemption to the extent such income is utilized for the purposes of the trust or set apart for future application as referred to in Section 4.11 and also subject to the fulfillment of conditions laid down in Section 12A. The value of any medical or educational services provided by a charitable or religious trust operating a hospital, medical facility, or educational facility as referred to in Section 13(3) shall be deemed to be income chargeable to income tax if such services are rendered to the following persons: • • • • •
The author of the trust or the founder of the institution. Any person who has made a total contribution exceeding | 50,000. Where such author, founder, or person is a HUE, a member of the HUF. Any trustee of the trust or manager of the institution. Any relative of such author, founder, person, member, trustee, or manager as aforesaid. • Any concerned in which any of the person in clauses (i) to (vi) has a substantial interest. Where the aggregate of funds of the trust invested in a concern in which any person has a substantial interest does not exceed 5% of the capital of that concern. Note: The term “value” refers to the cost or benefit of any benefit or facility offered to any of the people listed above for free or at a reduced charge.
vi) Section 35 of the Income Tax Act 1961: Expenditure on Scientific Research. The government has urged our industrial and business sector to take Make in India concept in all facets of life. They have urged to use Indian local products and Indian manufactured parts to boot Indian economy.
4 Taxation of Healthcare Sector in India
77
Scientific research plays important role in development of any country. The industrial houses are encouraged to establish their own research house or to donate in various universities, IITs, and other education institutions. Section 35 of the Income Tax Act, 1961, deals with expenditure of scientific research and allows such expenditure as revenue expenditure to the business houses. vii) Section 35 (1): Revenue Expenditure Incurred on In-House Scientific Research. If an assessee incurs any expenditure on scientific research inside its premises or for development of scientific facility for development of its own business, then deduction of expenditure is allowed as revenue expenditure. The most important condition is that the expenditure should be for development of his business, or it relates to his business. Note: where salary has been paid to an employee engaged in scientific research or any expenditure has been incurred on purchase of materials used in scientific research, such salary or expenditure paid or incurred after March 31, 1973, but within a period of three year immediately preceding the commencement of business shall be considered to have been paid or incurred in the previous year in which the business commenced to the extent certified by the authority prescribed for the purpose under Rule 6 of the Income Tax Rules, 1962, i.e., Director-General (Income Tax Exemptions) in concurrence with the Secretary. Department of Scientific Research and Industrial Research, GOI. Amount Allowed as deduction: whole amount (100%) expended on scientific research during previous financial year shall be allowed as revenue expenditure. viii) Section 35(2): Capital Expenditure Incurred for Own Scientific Research. Where an assessee has incurred any capital expenditure on its own scientific research, then such whole expenditure is allowed as deduction during previous year in which it has incurred. Following conditions are required to be complied with. • The assessee should incur expenditure of Capital Nature on Scientific Research and there are no requirements that such expenditure should be capitalized in Books of Accounts. • Where capital expenditure incurred before commencement of business of assessee, the aggregate of such expenditure, incurred within three years immediately preceding commencement of business, is deemed to have been incurred in the previous year in which business is commenced. • Capital expenditure after February 29, 1984, is not allowed if held on purchase of land. • If the assets acquired are sold without having been used for any other purposes, the surplus or the deduction allowed, whichever is less, shall be chargeable to tax as income from business and profession of the previous year in which such sale
78
J. S. Kadyan
has taken place. Any excess of surplus over deduction allowed shall be chargeable to tax under income from Capital Gain. • The depreciation on the assets used in scientific research shall not be allowed in any year. ix) Section 35(2AA) D: Contribution to National Laboratory. If payments made to. University, IITs, National Laboratory, or any other Specified Person as approved by Specified Authority then the amount of deduction: • For AY 2018–19 to 2020–21 – shall be 150% of the actual payment & • For AY 2021–22 onwards – 100% of the actual payment. Note 1: above expenditure which is deductible under above previsions of the Income Tax Act, 1961, shall not be allowed to be deducted in any other sections of the Act, 1961. Note 2: The aforesaid deduction will not be denied merely on the ground that after assessee has paid the amount to the aforesaid institutions; the authority has withdrawn the approval granted to those institutions to carry on scientific research. x) Section 35 (2AB): Expenses on In-House Research and Development. A provision of Section 35(2AB) has been inserted in the Income Tax Act, 1961, from the Assessment Year, AY 1998–99. It provides for a deduction in respect of expenditure on in-house research and development expenses subject to the following. • Taxpayer is a company. • The company should engage in the business of biotechnology or any business of manufacture or production of any article or thing except those specified in the XI Schedule. • The company has incurred expenditure on scientific research (whether it to revenue or capital) during previous year. The expenditure on scientific research in relation to drugs and pharmaceutical shall be including the expenditure incurred on clinical trial, regulatory approvals, and filing of an application for patent. • The expenditure should not be held on purchase of land. • The company has entered into an agreement with the prescribed authority for cooperation in such research and development facility for audit of accounts maintained for that facility or fulfills such conditions related to the way of maintenance of accounts and records, audit and submission of report to the authority. • The company should apply in Form 3CK, with Research and Development Authority approved the same in Form 3CM. The Prescribed Authority should approve the facility within a period of 120 days from the date of application, and
4 Taxation of Healthcare Sector in India
79
if approval not received within prescribed time, then deduction to the company shall not be disallowed. • The company shall maintain a separate book of account for each Approved Research Facility and same shall be audited every year as may be prescribed by authority. • An Audited Report in Form 3CL A shall be filed electronically by the Company with authority within due date of filing Income Tax Returns as may be prescribed. Amount of Deduction shall be as under. • For the AY 2018–19 to 2020–21 – 150% of the actual payments • For the AY 2021–22 onwards – 100% of the actual payments. Note1: A project approved under provisions of Section 35(1) (iia): shall be prohibited to claim weighted deduction under Section 35(2AB). However, deduction under Section 35(1(i)/(ii) can be claimed up to 100% of amount spent as the revenue or capital expenditure on the scientific research during previous year. Note 2: Other Points to remember, in respect of above expenditure no deduction is allowed in any other provisions of Income Tax Act, 1961. xi) Section 8oIB: Deduction in Respect of Profits and Gains from Certain Industrial Undertakings Other Than Infrastructure Development Undertakings. In case of an assessee, who’s the gross total income includes income from profits or gains from any business as specified, then, deduction is allowed from such profits and gains of an amount equal to such percentage and for such number of assessment years as specified in this section. The amount of deduction in the case of an undertaking deriving profits from the business of operating and maintaining a hospital in a rural area/other than excluded area shall be hundred percent of the profits and gains of such business for a period of five consecutive assessment years, beginning with the initial assessment year, if. • Such hospital is constructed at any time during the period beginning on October 1, 2004, and ending on March 31, 2008: (for hospitals in rural area) and April 1, 2008, and ending on March 31, 2013 (for hospitals in other than the excluded area). • The hospital has at least one hundred beds for patients. • The construction of the hospital is in accordance with the regulations, for the time being enforce, of the local authority; and • The assessee furnishes along with the return of income and the report of audit.
80
J. S. Kadyan
4.7 Conclusions In this chapter, the author has attempted to discuss the healthcare sector of India from the taxation point of view. The budgetary allocation and spending by the Government of India towards the healthcare sector has been highlighted. The taxation system of India, which is quite complex in nature, has been explained in a very simple manner and to the point. The most relevant sections of the Income Tax Act as well as Goods and Service Tax Act have been discussed in this chapter. The mechanism of direct tax as well as indirect tax, comprising of Income Tax Act 1961 and GST, Goods and Service Tax Act, 2017, as applicable to the health sector only in India has been explained. Few recommendations are also suggested towards better management of healthcare services and the taxation. The government needs to take timely and appropriate steps to make healthcare services well within the reach of its citizens by increasing the GDP allocation towards healthcare, improving the healthcare infrastructure, raising awareness, and enacting relevant regulations. Increased spending would result in a higher doctor-to-patient ratio and improved facilities. According to the economic survey report 2019–20 and a report published in Deccan Herald (Deccan Herald 2020), the (allopathic doctor) doctor-population ratio in India is 1:1456 against the WHO recommendation of 1:1000. The report further states that, India spends a meager 3.6 percent of its GDP on healthcare which is way below the average of 7.6 percent among OECD and various BRICS countries. In order to further improve the healthcare system in India, the government needs to lower the tax rates on those very essential products and services which are necessarily required to be consumed to save one’s life during the infection period. The revenue deficit caused may be recovered by marginally increasing the tax rates for HNI—High Networth Individual—assessees, as well as super rich citizens and large business houses and Multinational Corporation. Corporates social responsibility programs of the corporates may be directed towards catering to the healthcare needs of the society. Various tax sops and deduction may also be announced as a special measure towards prevention of further spread of the epidemics and providing the healthcare services to the people within the companies’ areas or they may also be encouraged to adopt a particular area of the city, any town, or villages where there is a severe need of healthcare.
References Advance ruling no KAR ADRG 4/2018. Tathagat Healthcare Care Centre LLP, Karnataka. https://tax guru.in/wp-content/uploads/2018/05/Tathagat-Health-Care-Centre-LLP-AAR-Karnataka.pdf Charitable Purpose u/s 2(15). What is charitable purpose for an NGO? Retrieved on June 07, 2021. https://www.incometaxforngos.org/charitable-purpose-u-s-2-15
4 Taxation of Healthcare Sector in India
81
Deccan Herald, (January 31, 2020) The doctor-population ratio in India is 1:1456 against WHO recommendation. Retrieved on October 6, 2021. https://www.deccanherald.com/business/ budget-2020/the-doctor-population-ratio-in-india-is-11456-against-who-recommendation-800 034.html Deepak J, Ani CA (November 11, 2020) Taxability of Health Care services under GST. Retrieved on December 22, 2020. https://taxguru.in/goods-and-service-tax/taxability-health-care-servicesgst.html Doctors Day: violence against medical professionals our healthcare system and possible solution. Retrieved on September 25, 2021. https://www.indiatvnews.com/health/world-doctors-day-vio lence-against-medical-professionals-our-healthcare-system-and-possible-solution-716137. Employment in healthcare sector (2021) Retrieved on September 26, 2021. https://www.niti.gov. in/sites/default/files/2021-03/InvestmentOpportunities_HealthcareSector_0.pdf Impact of GST on Healthcare and Pharma Sector (June 29, 2021) Retrieved on February 17, 2021. https://cleartax.in/s/gst-impact-on-healthcare-pharma-sector Income tax rates for Companies, Co-operative society and Local authority for assessment year 2021–22 and 2022–23. Retrieved on December 18, 2021. https://incometaxindia.gov.in/boo klets%20%20pamphlets/e-pdf-income-tax-rates-english-2022.pdf Income tax rates for financial year 2020–21 / assessment year 2021–22. Retrieved on October 20, 2020. https://taxguru.in/income-tax/income-tax-rates-financial-year-2020-21-assessment-year2021-22.html Income tax rates for financial year 2020–21 and 2021–22. Retrieved on February 15, 2021. https:// taxguru.in/income-tax/income-tax-rates-fy-2020-21-fy-2021-22.html India: Pharmacy to the World, Invest India, Strategic Investment Research Unit, July 31, 2020. Retrieved on November 18, 2020. https://www.investindia.gov.in/siru/india-pharmacy-world Investment opportunities in healthcare sector (2021) Retrieved on August 18, 2021. https://www. niti.gov.in/sites/default/files/2021-03/InvestmentOpportunities_HealthcareSector_0.pdf Ministry of Chemical & Fertilizers, Government of India, 05 March 2020. Retrieved on November 20, 2020. www.pib.gov.in/PressReleaseDetail.aspx?PRID=1605361 Ministry of Finance, Government of India. Economic Survey, 2020–21, Retrieved on June 10, 2021. https://www.indiabudget.gov.in/economicsurvey/. Ministry of Finance, Govt. of India (2017) Notification no. 9/2017-Integrated Tax (Rate). https:// gstcouncil.gov.in/sites/default/files/All-rate-notification/Notification9-IGST.pdf Ministry of Finance, Govt. of India (2018) Clarifications regarding GST in respect of certain services. https://cbic-gst.gov.in/pdf/circularno-32-cgst.pdf Ministry of Finance, Govt. of India (2020) Clarifications regarding GST in respect of certain services. https://cbic-gst.gov.in/pdf/circularno-32-cgst.pdf Ministry of Finance, Govt. of India (2020) Donations eligible under section 80GGA of Income Tax Act 1961. Retrieved on November 16, 2021. www.incometaxindia.gov.in No GST exemption to non-clinical body on healthcare services. Retrieved on January 18, 2020. https://taxguru.in/goods-and-service-tax/no-gst-exemption-non-clinical-body-health care-services.html Outlook of India’s healthcare sector, Retrieved on September 25, 2020. https://store.frost.com/out look-of-india-s-healthcare-industry-2020.html Pharmaceutical industry report (November 2022) Retrieved on January 15, 2022. https://www.ibef. org/industry/pharmaceutical-india.aspx Pharmaceutical Industry Report (November 2022) Retrieved on January 15, 2022. https://www. ibef.org/industry/pharmaceutical-india.aspx Report by United States Food and Drug Administration on the State of Pharmaceutical Quality (2021). Retrieved on April 01, 2021. www.fda.gov/media/125001/download. Report on Healthcare Industry in India, 2021. Retrieved on May 29, 2021. https://www.ibef.org/ industry/healthcare-presentation What is the income tax slab for FY 2020–21? (2020) Retrieved on December 27, 2020. https://www. canarahsbclife.com/tax-university/articles/what-is-the-income-tax-slab-for-2020-21.html
82
J. S. Kadyan
World Bank Economic Survey (January 2020) Retrieved on September 18, 2021. https://thedocs. worldbank.org/en/doc/4aa0b654ecdbaf8302d5901aaada3fbf-0350012021/related/Global-Eco nomic-Prospects-January-2020.pdf Surcharge on income tax as applicable for financial year 2020–21 and 2021–22. Retrieved on February 15, 2021. https://taxguru.in/income-tax/income-tax-rates-fy-2020-21-fy-2021-22. html
Jagbir Singh Kadyan is a Commerce, Management, Economics, and Social Work postgraduate. Master of Commerce from Savitribai Phule Pune University & Tilak Maharashtra University, Pune, India; Master of Management Science from Bharati Vidyapeeth Deemed University, Pune, India; Master of Economics from Savitribai Phule Pune University, Pune, India and Master of Social Work from IGNOU–Indira Gandhi National Open University, New Delhi, India. He holds a Ph.D. in CSR-Corporate Social Responsibility from Maharishi Dayanand University, Rohtak, Haryana, India. He is an Accredited Management Teacher by AIMA—All India Management Association, New Delhi, India; Certified CSR Professional by ICSI- Institute of Company Secretary of India, New Delhi, India. Editorial Board Member; Reviewer for various national, international, and Scopus-indexed journals. Research guide for Ph.D. scholars and evaluated over 17 Ph.D. theses on Commerce & Business Management subjects for different Indian universities. He has been a Principal Investigator for 02 Innovation Research Projects awarded by the Cluster Innovation Centre, University of Delhi, New Delhi, India. He has also been a Principal Co-ordinator for 03 projects funded by AICTE—All India Council of Technical Education, Govt. of India. He worked in the industry for over 15 Years before venturing into academics and research, wherein he has completed over 14 years. Published over 40 articles & research papers in UGC Care; Scopus Indexed Journals. Co-authored 06 books and contributed 08 chapters with national and international publications like IGI-Global, Springer & Palgrave publications. Delivered keynote addresses and invited lectures at national and international symposiums, seminars, and conferences. Also received several best research papers and best presentation awards. He has been a visiting faculty of Marketing and Consumer Behaviour for MBA & BBA programs of Pokhara University affiliated Uni-Globe College, Kathmandu, Nepal, and with DSEU– Delhi Skills; Entrepreneurship University, New Delhi, India for their BBA Banking & Insurance program. He works as Assistant Professor with the Dept. of Commerce, Swami Shraddhanand College, University of Delhi, New Delhi, India, and Honorary Associate Director with the Centre for Socio-economic; Sustainability Research, New Delhi, India.
Chapter 5
Sustainability Based Medical Waste Logistics in Healthcare Enterprises: A University Hospital Application Kadir Kaan Göncü
Abstract Reverse logistics can be defined as the processes of correct collection, sorting, classification, and processing of products that are at the end of their useful life for re-evaluation, inclusion in production, or disposal from the consumer to the manufacturer, the retailer, or their legal counterparts. Reverse logistics has an important place in the concept of sustainability. Reverse logistics is an indispensable partner for sustainability, which expresses the efforts to leave a more livable environment for future generations. The primary purpose of medical waste logistics, which has a special place among reverse logistics activities, is to collect, transport, and dispose of waste safely and economically without harming the environment and public health. Medical wastes pose a severe risk to the hospital and hospital environment and threaten public health and the entire environment. All medical wastes that are not properly collected and subjected to process control affect the rate of spread of diseases. Reverse logistics has an important place in the concept of sustainability. Reverse logistics is an indispensable partner for sustainability, which expresses the efforts to leave a more livable environment for future generations. The primary purpose of medical waste logistics, which has a special place among reverse logistics activities, is to collect, transport, and dispose of waste safely and economically without harming the environment and public health. Medical wastes pose a severe risk to the hospital and hospital environment and threaten public health and the entire environment. Keywords Health systems · Healthcare industry · Hospital · Medical waste · Waste management · Hospital waste
K. K. Göncü (B) Social Vocational College, Trakya Üniversitesi, Edirne Merkez, Turkey e-mail: [email protected] © The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd. 2023 K. T. Çalıyurt (ed.), Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II, Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application, https://doi.org/10.1007/978-981-99-5502-2_5
83
84
K. K. Göncü
5.1 Introduction Reverse logistics can be defined as the processes of correct collection, sorting, classification, and processing of products that are at the end of their useful life for the purpose of re-evaluation, inclusion in production or disposal, from the consumer to the manufacturer, the retailer, or their legal counterparts. Reverse logistics has an important place under the concept of sustainability. Reverse logistics is an indispensable partner for sustainability, which expresses the efforts to leave a more livable environment for future generations. The main purpose of medical waste logistics, which has a special place among reverse logistics activities, is to collect, transport, and dispose of wastes in a safe and economical way without harming the environment and public health. Medical wastes not only pose a serious risk for the hospital and hospital environment, but also threaten public health and the entire environment. All medical wastes that are not properly collected and subjected to process control affect the rate of spread of diseases. Reverse logistics has an important place under the concept of sustainability. Reverse logistics is an indispensable partner for sustainability, which expresses the efforts to leave a more livable environment for future generations. The main purpose of medical waste logistics, which has a special place among reverse logistics activities, is to collect, transport, and dispose of wastes in a safe and economical way without harming the environment and public health. Medical wastes not only pose a serious risk for the hospital and hospital environment, but also threaten public health and the entire environment. All medical wastes that are not collected properly and not subject to process control affect the rate of spread of diseases.
5.2 Logistics Logistics: It includes the effective realization and monitoring of materials, service processes, and information flow in the processes from production to consumption in order to meet the needs of customers. The most important concept in logistics is to respond to customer needs in the most effective way. This process requires the supply of the goods at the desired place and time from the seller, who is the production point, to the buyer, who is the consumption point (Kaymak 2010). The American Manufacturing and Inventory Control Association (APICS) defines logistics as the science of sourcing, shipping, and distributing products and materials in the appropriate time and quantity in an industry context. Logistics can be defined as a means of providing resources such as products, services, and people where and when needed. Logistics management consists of the activities of planning, implementing, and controlling all logistics-related processes (Tekin 2014). Logistics is one of the most important functions in a workflow. Logistics activities carried out in order to meet the needs of customers in terms of businesses show us the most basic purpose of logistics. The aim of logistics management is to manage the
5 Sustainability Based Medical Waste Logistics in Healthcare Enterprises …
85
forward and reverse flow in the process from the starting point to the consumption place in the most effective and efficient way to meet the demands of the customers (Erdal 2014). Logistics is also one of the focus sectors of the European economy, as it contributes to economic growth and plays a key role in international competitiveness (Soysal et al. 2018). When evaluating logistics processes in terms of businesses, we can basically examine them under four headings. Those titles are: supply, production, distribution, and reverse logistics (Yalçı et al. 2017).
5.3 Reverse Logistics The logistics and supply chain literature mostly consists of studies that examine the forward flow of products, that is, the processes from raw material to delivery of products to the customer. In fact, when the definition of “logistics management” of the Logistics Board of Directors is examined, the expression “effective and efficient management of product, service and information backflows” is also included. As can be understood from this expression, reverse logistics constitutes an important subbranch of supply chain and logistics disciplines. In addition, reverse logistics emerges as a multidisciplinary field as it is an area of interest for environmental, economic, and marketing disciplines (Sorkun and Onay 2016). Unlike forward logistics, reverse logistics covers the reverse flow of factors that are subject to logistics (from consumer to production point) (Çakır 2016). Reverse logistics is the process of planning, controlling, and executing the efficient and cost-effective flow of raw materials, currently in-process stocks, products, and related information from the point of consumption to the point of manufacture, in order to recover or properly dispose of them. The concept of reverse logistics is generally defined as the processes of effective planning, implementation and control of secondary material warehouses, material flow and related information in order to recover or destroy material in the opposite direction of the traditional supply chain (Kaymak 2010). Businesses that want to gain competitiveness focus on areas such as supply chain and logistics management. Businesses attach special importance to reverse logistics strategies as a result of consumers’ increasing environmental awareness (Kaymak 2010). Reverse logistics is defined as “going the wrong way on a one-way street” because of the importance of shipping products one way. In the late 1990s, reverse logistics began to be defined as “the role of logistics in product returns, resource reduction, recovery, material substitution, material reuse, waste disposal and incineration, repair and remanufacturing” (Karaçay 2005). It is possible to express reverse logistics as activities required to reuse, repair, reproduce, recycle, or dispose of products (Alkan et al. 2020). Reverse logistics is the reverse flow of raw materials, work-in-process or finished goods, and associated information from the point of final consumption to the point
86
K. K. Göncü
of origin. Since reverse logistics is a relatively new field, in the literature, reverse logistics is expressed as return logistics and different concepts with the same meaning (Fettahlıo˘glu and Birin 2016). Unlike elements in the forward logistics network, there are more units in the reverse logistics network. A reverse flow supply chain consists of all elements of the forward logistics network as well as third-party logistics firms acting as demand points, secondary markets, disposal centers, collection points, and more (Ayvaz et al. 2013). The development of reverse logistics products includes programs for the recycling of hazardous materials, disposal of old equipment and recovery of resources, as well as inventories, restocking, withdrawals, and the formation of excess inventory (Coelho et al. 2011). Reverse logistics is the process of collecting and redistributing products from the customer to the manufacturer and retailer with the aim of reusing, reproducing, or destroying products that are at the end of their useful life (Zarbakhshnia et al. 2018). Recycling and related issues have received increased attention in recent years, so some countries have established legislation focusing on waste management. This phenomenon is mainly observed in developing countries where practices related to waste management and reverse logistics are in their infancy (Guarnieri et al. 2020). Today, due to the rapid consumption of natural resources, the recovery of products that have completed their useful life is becoming increasingly important. Logistics activities are important for businesses due to the recovery of recyclable products, the improvement of reusable products and their reuse in production activities, the reduction of land use for waste, savings in energy consumption and labour costs. For these reasons, it becomes necessary for businesses to plan and implement reverse logistics activities. On the other hand, as a result of the increase in environmental awareness in the society, the enactment of legal regulations made by the states forces businesses to implement reverse logistics activities (Öçal 2021). Reverse logistics has an important place under the concept of sustainability. While sustainability refers to the efforts to leave us a more livable environment for future generations, reverse logistics does just that (Çetin and Sain 2018). The gradual deterioration of the ecological balance and the individual’s requests for measures depending on this situation raised the awareness of government and non-governmental organizations. The desire to preserve the ecological balance has led to measures to be taken, and the businesses, which see that these measures have become profitable, have led them to comply with these measures and follow new production strategies (Nakıbo˘glu 2007). Reverse logistics includes specific processes for reverse logistics, along with various processes that also apply to supply and distribution logistics. These can be listed as follows: Collection, Separation, Transport and Transfer, Storage, Processing (Dyckhoff et al. 2013). When the activities put forward during the reverse logistics processes are examined, the consequences of direct reuse, repair, product refurbishment, remanufacturing, partial use of products, recycling, incineration, and burial are encountered (Öçal 2021).
5 Sustainability Based Medical Waste Logistics in Healthcare Enterprises …
87
5.4 Concept of Waste and Management The concept of waste is an economics origin term that has been found in the literature as a result of the change in consumption habits in parallel with the progress of industry and technology. At the same time, waste can be defined as the by-products that are the source of environmental problems, emerge in all processes related to both production and consumption, remain as a result of obtaining the benefit, and need to be removed (Aykut 2014). The main purpose of waste management is to collect, recycle, reuse wastes in the most economical way in a way that does not harm human health and the environment, and finally, to dispose of them safely by reducing the amount and volume (Özerol 2005).
5.4.1 Medical Waste Concept and Its Qualities In the literature, different definitions are used to express wastes originating from health institutions. Although the term “medical waste” is used very often, the terms “medical hazardous waste” and “health waste” are also frequently preferred. Although definitions are generally made with reference to the European Waste Catalogue list, there are different approaches about which type of waste should be in which class (Kurt Azap 2015). Healthcare waste is a general term used to describe wastes containing blood and infectious agents originating from healthcare facilities. In some references, these wastes are defined as clinical wastes, medical wastes, biomedical wastes, hospital wastes, healthcare wastes, infectious wastes, hazards, and biohazards (Noman et al. 2018). There are growing concerns around the world about the adverse effects of healthcare waste generated in hospitals, particularly in low- and middle-income countries. Hazardous wastes can cause adverse effects on both human populations and the environment due to their physical, chemical, and biological properties (Marcos ve di˘gerleri 2022). Wastes from health institutions are classified as hazardous and harmful wastes as they are permanent wastes in the air, water, and soil and disrupt the ecological balance, apart from domestic solid wastes, and special precautions should be taken for the production, transportation, storage, and disposal of these wastes. As in all other institutions, the amount of waste in health institutions is increasing day by day in proportion to the services they provide. In order to eliminate the danger risks that this increase may cause, it is necessary to determine the management stages from collection to disposal by taking the necessary precautions (˙Ilgün 2010). According to the World Health Organization, biomedical wastes constitute one of the most important waste categories that pose significant potential risks to humans and the environment. Biomedical waste is defined as the production of waste material in health institutions, medical research facilities, laboratories, and private clinics.
88
K. K. Göncü
This category of waste materials includes chemicals, drugs, medical instruments, needles, syringes, diagnostic samples, blood and radioactive materials (Antoniadou et al. 2021). According to the regulation, wastes originating from health facilities are collected in four main groups as domestic, medical, hazardous, and radioactive wastes in accordance with the classification system of the World Health Organization (Küçük 2013). In order to increase recycling, especially in recent years, WHO calls for medical equipment to be made from easily recyclable and standard materials for all member states (Soysal 2015). Medical waste management constitutes a very important process in terms of ensuring hygiene in the hospital environment and protecting personnel and public health (Ba¸sarı Kurucu 2011). Concepts expressing hospital wastes and medical wastes are often confused. Medical waste is only a part of hospital waste (Table 5.1). Table 5.1 Classification of wastes from health institutions (T.C. Resmi Gazete, 25 Ocak 2017) Domestic Waste
Medical Waste
Hazardous Waste
A: General Waste
Sections with healthy people, the section where the non-patients are examined, first aid areas, administrative units, cleaning services, waste from kitchens, warehouses, and workshops: Wastes from medical centers, except those mentioned in groups B, C, D, E, F, and G
B: Packaging Waste
Reusable, recoverable wastes originating from all administrative units, kitchens, warehouses, workshops: Paper, cardboard, plastic, glass, metal, etc.
C: Infectious Wastes
Wastes that require special handling and disposal to prevent the spread of infectious agents
D: Pathological Wastes
Anatomical waste tissues, organs, and body parts and wastes generated during medical interventions such as surgery, autopsy, etc.
E: Sharps Medical Waste
Waste that can cause stings, punctures, abrasions, and injuries
F: Hazardous waste
Wastes that will be subject to special treatment due to their physical and chemical properties or due to legal reasons – Hazardous Chemicals – Cytotoxic and cytostatic drugs – Amalgam Wastes – Genotoxic and cytotoxic wastes – Pharmaceutical Waste – Wastes containing heavy metals – Pressure Containers
Radioactive Waste G: Radioactive Waste
It is collected and removed in accordance with the provisions of the Turkish Atomic Energy Authority Legislation
5 Sustainability Based Medical Waste Logistics in Healthcare Enterprises …
89
5.5 Reverse Logistics Process Related to Medical Wastes The main purpose of medical waste logistics is to collect, transport, and dispose of wastes in a safe and economical way without harming the environment and public health. Medical wastes not only pose a serious risk for the hospital and hospital environment, but also threaten public health and the entire environment (Özerol 2005). The medical waste management process is an important part of being able to control infectious diseases. All medical wastes that are not properly collected and subject to process control affect the rate of spread of diseases (Aydın 2013). New diagnosis and treatment methods developed in parallel with the development of technology rapidly increase the amount of medical waste generated in health institutions. Considering the dangers in the content of medical wastes, medical wastes should be collected, transported, temporarily stored, and disposed of by reducing their volume and amount without mixing with other wastes (Eren 2019). In order to protect the health of healthcare workers, patients, and the public, it is necessary to manage medical wastes with a systematic approach from the moment they are produced in the waste cycle to the final disposal stage. In the last 20– 30 years, significant developments in the field of health have led to an increase in the population and the number and size of health facilities, an increase in the qualityof-care services, the proliferation of disposable medical products, and an increase in the production of medical waste (Küçük 2013).
5.6 Medical Waste Collection and Disposal Process Responsibility for the disposal of medical wastes in Turkey is given to municipalities in metropolitan cities and to local administrations in other places or to persons or organizations whose authority has been delegated by the Regulation on Control of Medical Wastes. The maintenance of inspections and sanctions is under the responsibility of the Ministry of Environment and Urbanization (Aydemir 2017).
5.7 Cost of Medical Waste Waste fees/costs produced in accordance with the Regulation on Control of Medical Wastes belong to the waste generating institutions. Necessary expenses for the collection, transportation, and disposal of the produced wastes are paid by the waste producers to the disposal institutions and organizations. Disposal fee of medical wastes is determined and announced every year by the Provincial Local Environment Board, which is structured under the Ministry of Environment and Urbanization and is reported to the ministry. Medical waste disposal fees vary according to
90
K. K. Göncü
Table 5.2 Medical waste producers (T.C. Resmi Gazete, 25 Ocak 2017) Health institutions producing Health institutions producing large amounts of waste medium amount of waste (a) University Hospitals and Clinics (b) General Purpose Hospitals and Clinics (c) Maternity Hospitals and Clinics (d) Military Hospitals and Clinics
(a) Health centers, medical centers, and dispensaries (b) Outpatient centers (c) Morgues and Autopsy Centers (d) Organizations that conduct research and experiments on animals (e) Old age asylum and nursing homes (f) Medical and biomedical laboratories (g) Animal hospitals (h) Blood banks and transfusion centers (i) Emergency and first aid centers (j) Dialysis centers (k) Rehabilitation Centers (l) Biotechnology laboratories and institutes (m) Medical research centers
Health institutions producing small amount of waste (a) Other units where Health Services are provided (doctor’s offices, dental and oral health clinics, etc.) (b) Veterinary clinics (c) Acupuncture centers (d) Physical therapy centers (e) Home treatment and nursing services (f) Beauty, ear piercing, and tattoo centers (g) Pharmacies (h) Ambulance Services (i) Zoos
provinces and health institutions (Aydemir 2017). According to the regulation, the list of medical waste producers is as follows (Table 5.2). Issues such as separation, collection, transportation, and temporary storage of medical wastes are regulated as detailed below according to the Medical Waste Control Regulation (T.C. Resmi Gazete, 25 Ocak 2017). Medical wastes are collected separately from other wastes at the source by health personnel. While collecting medical waste, “ATTENTION! MEDICAL WASTE” bags with the inscription in red are used. Wastes with sharp and penetrating properties are collected with boxes or containers bearing the phrase “CAUTION! CUTTING AND DRILLING MEDICAL WASTE” (Fig. 5.1).
5.7.1 Transportation of Medical Wastes in the Health Institution Medical waste bags are collected and transported in a covered container/container/ bucket by personnel trained for this job within the health institution. Pathological waste collection containers are transported by wheeled medical waste transport vehicles. It cannot be transported in the exact vehicle with medical and other wastes.
5 Sustainability Based Medical Waste Logistics in Healthcare Enterprises …
91
Fig. 5.1 Medical waste emblem (D˙IKKAT! TIBBI ATIK [ATTENTION! MEDICAL WASTE]. Resource: Official Gazette, Republic of Turkey, January 25, 2017)
Medical waste containers/containers/buckets are cleaned and disinfected regularly every day. The personnel must wear unique orange clothes and use protective equipment during transportation. The route of the waste transport vehicles is determined as far as possible from the areas with heavy human and patient traffic.
5.7.2 Temporary Storage of Medical Waste in a Healthcare Organization Medical wastes can be kept in the medical waste temporary storage or container before being transported. The waiting period can be extended up to one week if appropriate. In health institutions that produce up to 1 kg of medical waste per day, medical wastes can be kept in containers with lids for a maximum of 48 h. Health institutions that produce less than 50 kg of medical waste per day can establish a temporary medical waste warehouse.
5.7.3 Transport of Medical Waste to Processing Facilities Medical wastes must be transported safely to the medical waste processing facility without spreading around and without leaking water. Transfer stations are not used to transport medical waste. Transport vehicles are cleaned and disinfected after
92
K. K. Göncü
unloading medical waste. The vehicles used for the collection and transportation of medical waste are not used for other works or other wastes. The outer surfaces of the medical waste transport vehicles are orange and must have the expression “ATTENTION! MEDICAL WASTE”.
5.8 Medical Wastes Disposal Methods Due to their physical, chemical, and biological properties, the need to dispose of waste from health facilities separately from other wastes has emerged. Many disposal methods can be applied to safely dispose of medical wastes with appropriate disposal methods without harming the environment and human health. Based on the medical waste production data, it is seen that the classification, risks, advantages, and disadvantages of various disposal methods differ according to the medical waste technologies. It is seen that the disposal methods of medical waste have different advantages and disadvantages in terms of environmental health and sustainability. What is important here is the application of different disposal methods for different types of wastes. In other words, it is the use of whatever method the harmful effect of waste will be minimized. Only in this way can the environment and human health be protected. For example, while infected body fluids, sharp and piercing tools, and reusable materials can be disinfected, human and body parts and chemical wastes are unsuitable for disinfection (Küçük 2013). The main medical waste disposal methods are Combustion Technologies, Vapor Disposal Technologies, and Chemical Disposal Technologies.
5.9 Regulations on Management of Medical Wastes While implementations regarding the management of medical wastes are carried out in Turkey, the Medical Waste Control Regulation and the Hazardous Waste Control Regulation, which are based on the General Sanitary Law and the Environmental Law, and which are regulated by considering the European Union Legislation, are used. The purpose of the Medical Waste Control Regulation is as follows (T.C. Resmi Gazete, 25 Ocak 2017): ARTICLE 1 – (1) The purpose of this Regulation, from the formation of medical wastes to their disposal. a) To prevent the direct or indirect delivery of medical wastes to the receiving environment in a way that harms the environment and human health, b) To determine and implement the principles, policies and programs, and legal, administrative and technical principles for the collection of medical waste separately at the source without harming the environment and human health, transportation within the health institution, temporary storage, transportation to the medical waste processing facility and disposal.
5 Sustainability Based Medical Waste Logistics in Healthcare Enterprises …
93
5.10 Duties and Responsibilities All stakeholders in the medical waste collection, transportation, temporary storage, and disposal processes are jointly responsible for the damage caused by environmental pollution and deterioration caused by medical waste. According to the Medical Waste Control Regulation, the obligations of the institutions and organizations responsible for the management of medical waste and the basic principles regarding the subject (T.C. Resmi Gazete, 25 Ocak 2017).
5.10.1 Authority and Duties of the Ministry To determine policies so that medical wastes can adapt to nature and the environment, to cooperate and coordinate the implementation of the regulation, and to take measures, when necessary, to carry out control and customary inspections of all activities in the process from the formation of waste to its disposal, and to license medical waste processing facilities.
5.10.2 Duties and Authorities of Provincial Directorates To control all activities covering medical waste management, to impose sanctions in case of violation of the legislation, to issue transportation licenses to institutions or organizations that will transport waste, to inspect and revoke licenses when necessary, to examine and implement the waste management plans offered by local governments, to monitor activities and to impose sanctions in cases of violation of the legislation, to organize or have training programs organized.
5.10.3 Obligations of Municipalities To prepare, present, and implement management plans for medical wastes and to inform the public; to collect waste from temporary storage and to transport it to waste processing facilities; to dispose or provide pathological wastes treated with chemicals; to sterilize or dispose of wastes; to establish or have a medical waste processing facility established for these purposes, and to obtain an environmental license for these facilities, to ensure regular training of the personnel in charge, to ensure that they use unique clothing and protective equipment, to record the amounts of wastes collected, transported, sterilized, or disposed of.
94
K. K. Göncü
5.10.4 Obligations of Health Institutions To establish systems that will minimize waste at the source, to make protocols with local governments for collecting, transporting, and disposal of waste, to collect waste separately, to transport it within the organization, and to prepare management plans covering the measures to be taken in case of an accident by providing temporary storage, to use the bags and containers determined by the regulation when collecting wastes, to provide regular training of its staff, to immunize them, and to undergo health checks at maximum every six months, to meet the expenditures required for waste management, to keep records of information on the rate of medical waste.
5.11 Case Study In this part of the study, a calculation has been made to draw attention to the cost that a university hospital operating in Edirne must bear to dispose of medical waste. Trakya University Hospital gave information on the amount of medical waste used in the study. The rates and prices related to the cost used in the calculation were determined by the Edirne Province 2021 Local Environment Committee Decision (Table 5.3). Medical waste unit prices, which are applied in accordance with the 2021 Local Environment Board Decisions of the province of Edirne, are as given in the list below. Medical waste unit prices applied in accordance with the Decisions of the Local Environmental Board in 2021 (Edirne) Hospitals, Family Health Centers, Private Polyclinics, Dialysis Centers and Beauty Centers and other medical waste producers. (Collection, Transport, Sterilization, and Disposal Fees VAT excluded) (TRY/ KG) + VAT.1 Center of Edirne 3,50 TRY/KG (VAT Excluded) Lalapa¸sa 3,50 TRY /KG (VAT Excluded) Sülo˘glu 3,50 TRY /KG (VAT Excluded) Havsa 3,50 TRY /KG (VAT Excluded) Uzunköprü 3,50 TRY /KG (VAT Excluded) Meriç 3,50 TRY /KG (VAT Excluded) Kırklareli 5,85 TRY /KG (VAT Excluded) Doctor’s Offices. Oral and dental health clinics. Veterinary offices. Medical analysis laboratories (Collection, Transport, Sterilization, and Disposal Fees VAT included) (TRY/MONTHLY) Center of Edirne 55 TRY /KG (VAT Excluded) Lalapa¸sa 55 TRY /KG (VAT Excluded) 1
Value Added Tax.
070704
080317
080317
150106
160215
7133359
7132752
7132763
7133373
7132792
60380
450
400
7200
Kilogram
Kilogram
Kilogram
Kilogram
Kilogram
Off-Site
Off-Site
Off-Site
Off-Site
Off-Site
R13
R12
R13
R12
R13
(continued)
200556 - 4R ÇEVRE VE ENERJI SANAYI VE TICARET ANONIM SIRKETI
1028005 - FILIZ GERI DÖNÜSÜM SISTEMLERI ELEKTRIK TAAHHÜT SANAYI VE TICARET LIMITED SIRKETI
200556 - 4R ÇEVRE VE ENERJI SANAYI VE TICARET ANONIM SIRKETI
111838 - EKOLOJIK ENERJI A.S. ÇORLU SUBESI
111838 - EKOLOJIK ENERJI A.S. ÇORLU SUBESI
Quantity Unit of Where the Waste Waste processing facility / municipality that accepts measurement procedure is processing medical waste /exporter done method
Hazardous parts 150 removed from wastrel equipments
Mixed packing
Waste print toners containing hazardous materials
Waste print toners containing hazardous materials
Other organic solvents, washing liquids and main solutions
Declaration Waste code Waste name control no.
Table 5.3 Trakya University 2021 Waste Declaration Form
5 Sustainability Based Medical Waste Logistics in Healthcare Enterprises … 95
160506
180103
180106
180109
7132795
7133378
7133370
7133350
850
Medicines other than 18 01 08
Chemicals containing or consisting of dangerous substances 2420
1506
Kilogram
Kilogram
Kilogram
Kilogram
Off-Site
Off-Site
Off-Site
Off-Site
R13
D9
D9
R13
(continued)
200556 - 4R ÇEVRE VE ENERJI SANAYI VE TICARET ANONIM SIRKETI
1031582 - ATLAS KATI ATIK YÖNETIM SANAYI VE TICARET LIMITED SIRKETI EDIRNE SUBESI
1031582 - ATLAS KATI ATIK YÖNETIM SANAYI VE TICARET LIMITED SIRKETI EDIRNE SUBESI
200556 - 4R ÇEVRE VE ENERJI SANAYI VE TICARET ANONIM SIRKETI
Quantity Unit of Where the Waste Waste processing facility / municipality that accepts measurement procedure is processing medical waste /exporter done method
Waste whose 484640 collection and disposal is subject to special treatment in order to prevent infection
Laboratory chemicals consisting of or containing hazardous substances, including mixtures of laboratory chemicals
Declaration Waste code Waste name control no.
Table 5.3 (continued)
96 K. K. Göncü
R9
478,730
pcs/year
Capacity Unit
10742 - DEHA BITKISEL ATIK YAG TOPLAMA GERI KAZANIM BIODIZEL ÜRETIMI SANAYI VE TICARET A.S. DILOVASI SUBESI
Inpatient hospital services for human health provided by public institutions (including state university hospitals, excluding private specialized hospitals and dentistry, transportation by ambulance, medical laboratory testing activities)
Off-Site
86.10.05
Kilogram
200556 - 4R ÇEVRE VE ENERJI SANAYI VE TICARET ANONIM SIRKETI
NACE name
730
R13
NACE code
Oils and fats other than 20 01 25
Off-Site
200126
Kilogram
7133361
Fluorescent lamps 150 and other mercury-containing waste
200121
Quantity Unit of Where the Waste Waste processing facility / municipality that accepts measurement procedure is processing medical waste /exporter done method
7133345
Declaration Waste code Waste name control no.
Table 5.3 (continued)
5 Sustainability Based Medical Waste Logistics in Healthcare Enterprises … 97
98
K. K. Göncü
Sülo˘glu 55 TRY /KG (VAT Excluded) Havsa 55 TRY /KG (VAT Excluded) Uzunköprü 55 TRY /KG (VAT Excluded) Meriç 55 TRY /KG (VAT Excluded) Kırklareli 5,85 TL/KG (VAT Excluded) To determine the fee for the collection, transportation, and disposal of pathological wastes that have undergone chemical treatment as 5 TRY/KG (VAT Included), Hospitals, Family Health Centers, Private Polyclinics, Dialysis Centers and Beauty Centers and other medical waste producers (Collection, Transport, Sterilization, and Disposal Fees VAT Excluded) (TRY/ KG) + VAT Ke¸san 3,5 TRY /KG (VAT Excluded) ˙Ipsala 3,50 TRY /KG (VAT Excluded) Enez 3,50 TRY /KG (VAT Excluded) Gelibolu 5,85 TRY /KG (VAT Excluded) Kırklareli 5,85 TRY /KG (VAT Excluded) Tekirda˘g 5,85 TRY /KG (VAT Excluded) Doctor’s offices. Oral and dental health clinics. Veterinary practices. Medical analysis laboratories (Collection, Transportation, Sterilization, and Disposal Fees) (including VAT) (TRY/MONTHLY) Ke¸san 55 TRY /KG (VAT Excluded) ˙Ipsala 55 TRY /KG (VAT Excluded) Enez 55 TRY /KG (VAT Excluded) Gelibolu 5,85 TRY /KG (VAT Excluded) Kırklareli 5,85 TRY /KG (VAT Excluded) Tekirda˘g 5,85 TRY /KG (VAT Excluded) To determine the fee for the collection, transportation, and disposal of pathological wastes that have undergone chemical treatment as 5 TRY/KG (VAT included), Considering that the amount of waste that requires special treatment to be disposed of in Trakya University Medical Faculty Hospital, which we examined as a case study, is 484640 kg by 2021, it can be determined that the cost to be incurred is 484640 X 3.50 = 1.696.240 TL + VAT.
References Alkan G, Yılmaz B, Suzan O (2020) Tersine lojistik alanındaki yayınların bibliyometrik analiz yöntemiyle de˘gerlendirilmesi. Atatürk Üniversitesi ˙Iktisadi ve ˙Idari Bilimler Dergisi 34(3):711– 729 Antoniadou M, Varzakas T, Tzoutzas I (2021) Circular economy in conjunction with treatment methodologies in the biomedical and dental waste sectors. Circular Eco Sustain 1(2):563–592
5 Sustainability Based Medical Waste Logistics in Healthcare Enterprises …
99
Aydemir ˙I (2017) Türkiye’de Çevre Bilinci Kapsamında Tıbbi Atık Üretim Süreçleri ve Yönetimi. Bingöl Üniversitesi Sosyal Bilimler Enstitüsü Dergisi (BUSBED) 7(13):295–311 Aydın N (2013) Sa˘glık Sektöründe Ters Lojistik. Balkan ve Yakın Do˘gu Sosyal Bilimler Dergisi:142–148 Aykut Ü (2014) Çevresel açıdan tıbbi atık yönetimi: Antalya örne˘gi. T.C. Beykent Üniversitesi Sosyal Bilimler Enstitüsü Yüksek Lisans Tezi Ayvaz B, Kaçtıo˘glu S, Varol K (2013) Belirsizlikler altında tersine lojistik a˘g tasarımı literatür taraması. ˙Istanbul Ticaret Üniversitesi Fen Bilimleri Dergisi 12(24):1–15 Ba¸sarı Kurucu ZN (2011) Tıbbi atık lojisti˘gi ve ˙Istanbul ilinde incelenmesi. Bahçe¸sehir Üniversitesi Fen Bilimleri Enstitüsü Yüksek Lisans Tezi Çakır TE (2016) Bir tersine lojistik faaliyeti olarak tıbbi atıkların toplanmasında araç rotalama uygulaması. Sakarya Üniversitesi Sosyal Bilimler Enstitüsü Yüksek Lisans Tezi, ˙I¸sletme Ana Bilim Dalı / Üretim Yönetimi ve Pazarlama Bilim Dalı Çetin O, Sain AD (2018) Lojistik Sektöründe Sürdürülebilirlik Uygulamaları. IV. ˙International Caucasus-Central Asia Foreign Trade and Logistics Congress:910–921 Coelho TM, Castro R, Gobbo JA Jr (2011) PET containers in Brazil: opportunities and challenges of a logistics model for post-consumer waste recycling. Resour Conserv Recycl 55(3):291–299 Dyckhoff H, Lackes R, Reese J (2013) Supply chain management and reverse logistics. Springer Science & Business Media, Berlin Heidelberg Erdal M (2014) Satınalma ve Tedarik Zinciri Yönetimi, 3. Baskı. Beta, ˙Istanbul Eren E (2019) Tıbbi atık lojisti˘ginde i¸s sa˘glı˘gı ve güvenli˘gi süreçlerinin iyile¸stirilmesi. T.C. Yıldız Teknik Üniversitesi Fen Bilimleri Enstitüsü Doktora Tezi Fettahlıo˘glu HS, Birin C (2016) Sürdürülebilirlik Açısından Tersine Lojistik Faaliyetlerini ve Sürdürülebilir Pazarlamayı Etkileyen Faktörlerin Analitik Hiyerar¸si Yöntemi ile Belirlenmesi. Kahramanmara¸s Sütçü ˙Imam Üniversitesi ˙Iktisadi ve ˙Idari Bilimler Fakültesi Dergisi 6(2):89–114 Guarnieri P, Cerqueira-Streit JA, Batista LC (2020) Reverse logistics and the sectoral agreement of packaging industry in Brazil towards a transition to circular economy. Resour Conserv Recycl 153:1–12 ˙Ilgün A (2010) Katı atık yönetimi ve ters lojistik. T.C. Namık Kemal Üniversitesi Fen Bilimleri Enstitüsü Yüksek Lisans Tezi Karaçay G (2005) Tersine lojistik: Kavram ve i¸sleyi¸s. Çukurova Üniversitesi Sosyal Bilimler Enstitüsü Dergisi 14(1):317–332 Kaymak G (2010) Tıbbi Atık sterilizasyon Sisteminde Tersine Lojistik Uygulaması. Marmara Üniversitesi Sosyal Bilimler Enstitüsü Yüksek Lisans Tezi, ˙I¸sletme Bölümü ˙I¸sletme Ana Bilim Dalı, Uluslararası ˙I¸sletmecilik Bilim Dalı Küçük A (2013) Tıbbi atık yönetiminin ekonomisi. Sayı¸stay Dergisi 90:73–95 Kurt Azap Ö (2015) Hastanelerde Tıbbi Atık Yönetimi. Toplum ve Hekim 30(6):403–408 Marcos PM, Tara RZ, Arthur CN, Giulia RD, Julia LL, Raphael TD, Leo H (2022) Healthcare waste generation in hospitals per continent: a systematic review. Environ Sci Pollut Res 29(28):42466– 42475 Nakıbo˘glu G (2007) Tersine Lojistik: Önemi ve Dünyadaki Uygulamaları. Gazi Üniversitesi ˙Iktisadi ve ˙Idari Bilimler Fakültesi Dergisi 9(2):181–196 Noman E, Nik Norulaini N, Al-Gheethi A, Nagao H, Talip BA (2018) Selection of inactivation medium for fungal spores in clinical wastes by supercritical carbon dioxide. Environ Sci Pollut Res 25(22):21682–21692 Öçal B (2021) Tersine Lojistik Uygulamalarının Çevresel ve Sosyal Sürdürülebilirli˘ge Etkisi. Süleyman Demirel Üniversitesi ˙Iktisadi ve ˙Idari Bilimler Fakültesi Dergisi 26(4):521–532 Özerol ˙IH (2005) Tıbbi Atık Stratejileri Nelerdir? EN/ISO Normları Nelerdir? Avrupa’da Birlik? ABD’nin Yakla¸sımı? Ülkemizde Durum? 4. Ulusal Sterilizasyon Dezenfeksiyon Kongresi:434– 472 Sorkun MF, Onay M (2016) Ürün modülerli˘ginin ters lojistik süreçleri üzerinden tedarik zinciri stratejilerine etkisi. Sosyal ve Be¸serî Bilimler Dergisi 8(2):41–57
100
K. K. Göncü
Soysal A (2015) Dünyada Tıbbi Atık Sorunu. Toplum ve Hekim Cilt: 30 Sayı: 5 Soysal M, Çimen M, Demir E (2018) On the mathematical modeling of green one-to-one pickup and delivery problem with road segmentation. J Clean Prod 174:1664–1678 T.C. Resmi Gazete (25 Ocak 2017) (Sayı: 29959) - Tıbbi Atıkların Kontrolü Yönetmeli˘gi. https:// www.resmigazete.gov.tr/eskiler/2017/01/20170125.pdf Tekin E (2014) E-Lojistik ve ˙Ilaç Da˘gıtımında E-Lojistik Uygulamaları. Selçuk Üniversitesi Sosyal Bilimler Enstitüsü, Doktora Tezi, Selçuk Üniversitesi / Sosyal Bilimler Enstitüsü / ˙I¸sletme Ana Bilim Dalı / Üretim Yönetimi ve Pazarlama Bilim Dalı Turkish Republic Official Gazette, January 25, 2017, Number 29959. Regulation on Control of Medical Waste Yalçı EB, Altu˘g N, Koldere Akın Y (2017) Tüketicilerin Sosyal Sorumluluk Bilinci Do˘grultusunda Tersine Lojisti˘ge Bakı¸s Açıları. Akademik Bakı¸s Dergisi Sayı 60:383–395 Zarbakhshnia N, Soleimani H, Ghaderi H (2018) Sustainable third-party reverse logistics provider evaluation and selection using Fuzzy SWARA and developed Fuzzy COPRAS in the presence of risk criteria. Appl Soft Comput 65:307–319
Kadir Kaan Göncü was born in Adıyaman in 1977. He completed his high school education at Birecik High School. In 1994, he started his undergraduate education at Trakya University, Faculty of Arts and Sciences, Department of Physics. After completing his undergraduate education at Anadolu University Department of Business Administration, which he started in 2002, he got his Master’s in Business Administration at Trakya University Social Sciences Institute in 2008. He established Göncü Computer Industry and Trade Limited in 2001 and maintained his partnership until 2012. He started to work as a Lecturer at Trakya University Edirne Vocational School of Social Sciences in 2013 and continues to work. He has an associate degree from the Department of Justice and has a Class A Occupational Safety specialization certificate. He completed his Ph.D. education, which he started in 2017 at Trakya University, Department of Business Administration, in 2022. His particular areas of interest include multi-criteria decision-making methods, production systems, efficiency, supply chain management, and logistics.
Chapter 6
Evaluating Working Conditions in Healthcare During COVID-19 Crisis Jamil Kobrossi
and Walid Dagher
Abstract The coronavirus disease (COVID-19) pandemic, the Beirut blast and the destruction of two nearby hospitals, and the country’s financial meltdown crippled the Lebanese healthcare sector. This work aimed to analyze the working conditions and associated dysfunctions in a medium size hospital during COVID-19. The objective is to identify the root causes of the dysfunctions linked to working conditions. A faceto-face survey targeted the leadership at a hospital in north Lebanon. The survey was conducted to assess the effectiveness of the model. The study period began in August and ended in September 2020. Overall, the learners observed the chaos and identified the root causes of the dysfunctions during COVID-19. Keywords COVID-19 pandemic · Root causes · Working conditions · Healthcare · Leadership
6.1 Introduction On November 5, 2019, Moody’s Investors Service downgrades Lebanon’s rating to Caa2 (Reuters 2019). The national debt crisis, the financial meltdown, and the capital control in the banking sector crippled the country and in particular, the healthcare sector. In addition to the World Health Organization (WHO), regarding the outbreak of the coronavirus disease (COVID-19) in the People’s Republic of China and with transportations confirmed in the Republic of Korea, Japan was issued on January 23, 2020 (Liguori and Winkler 2020), that was later exported worldwide. At the time, the WHO committee did not declare COVID-19 as a public health emergency of international concern (PHEIC) (WHO 2020a). Followed by the Beirut massive J. Kobrossi Faculty of Business Management, University of Balamand-Kelhat, El Koura, Lebanon e-mail: [email protected] W. Dagher (B) Issam Fares Faculty of Technology, University of Balamand-Kelhat, El Koura, Lebanon e-mail: [email protected] © The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd. 2023 K. T. Çalıyurt (ed.), Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II, Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application, https://doi.org/10.1007/978-981-99-5502-2_6
101
102
J. Kobrossi and W. Dagher
port explosion on August 4, 2020 that shook Lebanon, destroyed the port, and two major hospitals, with at least 70 reported dead, and thousands injured (Betz Wallace 2020). On August 21, 2020, the World Health Organization reported more than 22 million cases of and 780,000 deaths (WHO 2020b). The first infection of the coronavirus in Lebanon was on February 21, 2020, and on June 13, 2020, 1422 cases were reported with a rate of 208/million person (Bizri et al. 2020). Leaders in the healthcare industry have attempted to develop a comprehensive list of organizational objectives with some success. They have also excelled in creating policies and guidelines for enhancing profitability through managing healthcare information technologies efficiently. However, they failed to consider the equipment and number of hospitals bed needed to support the population in a case of national disaster Meares, H. D., and Jones, M. P. (2020). They fail to see the impact of technology on innovation and business. For example, the use of electronic health records (EHRs) enhances the quality of care, facilitates the flow of information, improves quality of life, increases efficiency, saves life, and reduces waste. The digitalization of health records eliminated the problems involved with maintaining the paper trail and improved communications among hospital team members (Seth and LeeThomas 2020). For example, the advanced technology of robot-assisted surgeries allows miniaturized instruments to make tiny incisions, which result in shorter hospital stays, faster recovery, reduced pain and blood loss, and minimized risk of infection. Offering modern quality care services attracts public awareness and gives forward-looking hospitals an edge over competitors. Improving quality of care while keeping costs down has always been the two most frequently researched topics in the field of healthcare (Zemmar et al. 2020). Can efficient application and management of innovative technology reduce data entry errors? The fast-changing pace of technology creates multidimensional changes and transforms the business practices in most departments, which in turn forces the decision-makers to integrate the new technology in their strategic plans (Mollart et al. 2020). How can today’s leaders’ use to traditional modes of communication and interaction, manage the new technological complexity in their organizations when their skills have lagged the growth of electronic methods? They are now depending on physicians’ recommendations to make strategic decisions on what technology to adopt and how to implement it. Shifting the decision-making process to physicians who are not experts in new technology is not the best way for hospital managers to deal with technological innovation and is likely to leave the organization in constant turmoil. The traditional approach has failed to efficiently manage the new technologies, and this failure may lead to higher healthcare costs because of the high cost of new (Savage 2020). To be able to choose the best of the new technologies for adoption and to utilize them in a twenty-first-century business model effectively, healthcare leaders need to embrace a new management model and new objectives to face the challenges. In addition, the hospital teams must be strategically trained to align their tasks with the organization’s new objectives. Many questions face hospital managers that must be dealt with to maintain growth and best health practices Catalyst, N. (2020). What are the new processes, procedures, methods, and tools required to train new healthcare
6 Evaluating Working Conditions in Healthcare During COVID-19 Crisis
103
employees? Given the high initial cost of deploying new technology. How can the hospital provide sustainable, quality care that is affordable for most people? The aim of the study is to identify the root causes of the dysfunctions during the COVID-19 pandemic and what working conditions should be taken into consideration to minimize the effect of future pandemic. More specifically is to identify the root causes of the dysfunctions linked to working conditions.
6.2 Methodology The data collection method and sampling solicit information from upper management using a semi-structured face-to-face interview in a medium size hospital. The survey consisted of 36 questionnaires to convert the collected data into information. The sampling taken from a population size of nine managers managing different departments in the hospital. Sampling upper management from different departments is a key to measure the true value and to increase the confidence level in our assessment. The precision measurements focused on grouping key ideas and dissecting the collected data by breaking them into themes and sub-themes. The majority of the managers are men and represents 69% of the sampling population. It was decided to include additional participants to increase the female participants count to generate new information. Two male technicians in the information technology, two females in the quality assurance, and a male medical administrator contributed to the survey. The first sample consisted of the general manager and an external consultant. The second sample collected data from seven managers from different departments. The third sample focused on participants in three different departments. Each group was visited at different date and time intervals that was suitable to the participants. The answers to the questionnaire were documented and kept confidential. The data collection resulted in a 100% response rate in upper management, nursing, quality assurance, human resources, finance, purchasing, information technology, and maintenance. The female participation was increased because of the uneven distribution of males and females. The management average age of the participants was in the same range while the third sampling in the quality assurance and the information technology technicians were younger. In order to measure the leadership process and the dysfunctions in the organization, six sections were selected that could have affected an organization. Each of the variables were equally weighted 20% during the analysis. Working conditions affected the employees’ behavior due to physical workload, atmosphere at work, work hours, equipment and supplies, layout and arrangement of the premises. The coronavirus disease (COVID-19) affected the mental health of healthcare staff at the frontline due to the overwhelming workload and lack of proper personal protective equipment (PPE). The fear factor, the long hours, the lack of respiratory machine, and lack of beds in the hospital caused depression and anxiety (Zhou et al. 2020).
104
J. Kobrossi and W. Dagher
6.3 Control Variables The study attempted to have a variety of samples but the management in the organization was a male dominant and in the same age range. The female participants were increased and focused on the level of education of each manager that could influence the leadership skills (Ugurluoglu et al. 2015). The survey sampled upper management and three actors from two different departments.
6.4 Evaluation of Working Conditions During COVID-19 In order to evaluate the working conditions at the hospital during COVID-19, fifteen face-to-face actors were surveyed. The questions of the survey focused on capturing the dysfunctions during COVID-19 from various actors and from different disciplines. The rules and regulations were first assessed. As a result, 85% of the participants agreed that the doctors did not follow the rules at the hospitals and did not fill out the patients’ records. In turn, the hospital hired a resident doctor to complete the patients’ records. This means when doctors fail to follow the rules they are bound to make mistakes. However, 92% of the participants stated that patients have to wait more than an hour to see a doctor. Then 64% of the 200 part-time doctors moderately contribute to economic growth, and 57% have little advantage on administrative paperwork. Doctors do not fill out the paper works when sending the patients to the hospital and 4% of the managers find the Dictaphone little efficient (Fig. 6.1). The result of the assessed survey points out a lack of communication-coordination-cooperation among the staff and the doctors. The patient’s waits indicate lack of proper procedure, lack of synchronization, and poor time management. Half of the managers are dissatisfied with the hospitals procedures; 57% describes the culture differences between the patients and the staff as very bad. Then 71% are very dissatisfied with the communication among team members; 78% are also very dissatisfied with the lack of respect to hierarchy reporting (Fig. 6.2). The assessed survey questions point again to a lack of communication-coordination-cooperation, lack of synchronization. Lack of meetings, improper reporting, and poor patients– staff relationship. The latter indicates the mode of management practices at the hospital. Almost all the managers or at most 92% are very dissatisfied with the patients’ records keeping and archiving. While 35% of the managers’ claim that the lab work and medical files are always lost and another 35% claim that, sometimes the lab work and the medical files are lost. Then 92% of the managers are very dissatisfied with the audit conducted with the doctors (Fig. 6.3). The assessment indicates improper record keeping, inadequate information system, lack of space, lack of communication-coordination-cooperation, and poor-quality control. The above
6 Evaluating Working Conditions in Healthcare During COVID-19 Crisis
105
Fig. 6.1 Dysfunctions caused by the physicians
dysfunctions cripple the organization performance and create silo groups within and across different departments. Three different departments are very dissatisfied with the data entry. The nursing staff, the infirmary, and the administration were 83% very dissatisfied with the data entered into the system due to an inadequate information system. While the information technology department shows 83% efficiency in transferring the ERM and ECHOS scans to the Radio Information System (RIS) (Fig. 6.4). Four different departments responded 83% as very dissatisfied with the delivery time of the lab work, medicine, pharmacy, and intensive care unit. The lab work is late because of power outage and lack of maintenance support on the interrupted power supply, the delivery time of the medicine and the pharmacy are late because they are out of stock due to cash flow problem. The intensive care unit is affected by other departments. The delivery time of the radiology department is 57% dissatisfied and the information technology team responded more than one day to answer a call due to employee shortages (Fig. 6.5). The managers were 64% very dissatisfied with the clinical waste disposal, while 85% were very dissatisfied about the maintenance and repair at the hospital, also
106
J. Kobrossi and W. Dagher
Fig. 6.2 Ill processes
Fig. 6.3 Poor records keeping
85% responded with lack of training and 92% were very dissatisfied with the low operating budget (Fig. 6.6). As far as the vendors’ time delivery, managers responded with 92% very dissatisfied and 85% claimed the inventory control to be inefficient (Fig. 6.7).
6 Evaluating Working Conditions in Healthcare During COVID-19 Crisis
Fig. 6.4 Inaccurate data entry
Fig. 6.5 Delays in deliveries
107
108
J. Kobrossi and W. Dagher
Fig. 6.6 Lack of training
Fig. 6.7 Lack of operations control
The quality assurance is 64% inefficient and 57% answered very dissatisfied with the hospital food (Fig. 6.8). Eighty-five percent of workspace is inefficient, and 71% of hospital circulation is inefficient (Fig. 6.9). The result analysis pointed out to the root causes of the dysfunctions at the hospital. The working conditions were broken down into six primary sub-themes: Layout and agreement and of the premises represented 1%, equipment and supplies 7%, nuisance tasks 3%, physical conditions of work 9%, physical workload 2%, and 3% atmosphere at work. While the communication-coordination-cooperation were divided into three main sub-themes: communication-coordination-cooperation, 6%
6 Evaluating Working Conditions in Healthcare During COVID-19 Crisis
109
Fig. 6.8 Poor processes
Fig. 6.9 Lack of workspace and poor circulation
related to the internal services, 18% relationship to teamwork, and 1% related to communication-coordination-cooperation between the network and home office. The work organization was divided into four primary sub-themes: Distribution of tasks which represented 2%, interest of the work 2%, workload 2%, and rules and regulations 19%. Time management was broken into five main sub-themes: respecting deadlines and represented 16%, planning and scheduling of activities 4%, adequacy of job training 2%, training needs 2%, and available competency 1% (Savall et al. 2008) (Fig. 6.10). Strategic implementation was broken down into 4 sub-themes: breaking down and organizing strategic implementation represented 1%, 18% tools for strategic implementation, 6% for information systems, and 0% for mode of management (Fig. 6.11).
110
J. Kobrossi and W. Dagher
Fig. 6.10 Lack of leadership
Fig. 6.11 Lack of strategic planning
6.5 Conclusion In this study, the data generated 10 root causes of dysfunctions that affected the operations during COVID-19 (Fig. 6.11). 1. The layout and arrangement of the premises changed the circulation workflow to accommodate the COVID-19 patients. 2. The financial crisis forced the leaders to shut down two floors at the hospitals.
6 Evaluating Working Conditions in Healthcare During COVID-19 Crisis
111
3. The failed uninterrupted power supplies (UPS) and the constant power failure in the hospital interrupted the laboratory tests. 4. The pharmacy was out of supplies and product deliveries were late. 5. The physical conditions and fear of COVID-19 cases put the medical team and staff under a lot of pressure. 6. The atmosphere at work was unhealthy and could not keep the employee engaged and efficient. 7. The communication-coordination-cooperation breakdown among team members and across all departments prevented planning and killed performance. 8. The distribution of tasks, lack of interest at work, and workload created many dysfunctions in the departments. 9. Rules and regulations were not followed. 10. Respecting deadlines, planning, training, and competency were not applied. The observer learned that leaders could not effectively lead the crisis at the hospital because they lacked the tools for strategic decision-making, lacked training, lacked a disaster recovery plan, lacked procedures across departments, lacked synchronization, and lacked communication. The observers identified the root causes of the dysfunctions during COVID-19 that may be considered to develop a disaster recovery plan. The study did not address the hospital financial crisis but succeeded in pointing out the root causes of the dysfunctions encountered during the COVID-19 crisis. The results obtained point out to the areas where working conditions could be improved to encourage employee engagement, efficiency, communicating, coordinating, cooperating, planning, training, and performance. A futuristic study will focus on building a conceptual model for a post-pandemic focusing on enhancing the working conditions in the healthcare place. The COVID19 pandemic proved how weak is our healthcare systems worldwide and in particular in Lebanon.
References Betz B, Wallace D (2020) Beirut blast: Massive explosion shakes Lebanon’s capital; at least 70 dead, thousands injured, August 4. Retrieved from https://www.foxnews.com/world/explosionlebanon-capital-beirut on 1 July 2022 Bizri AR, Khachfe HH, Fares MY, Musharrafieh U (2020) COVID-19 pandemic: An insult over injury for Lebanon. J Commun Health 46:1–7. Catalyst N (2020) Lessons from CEOs: Health care leaders nationwide respond to the covid-19 crisis. NEJM Catalyst Innovations in Care Delivery 1(4) Liguori E, Winkler C (2020) From offline to online: Challenges and opportunities for entrepreneurship education following the COVID-19 pandemic. Entrepreneurship Education and Pedagogy, 3(4), 346–351. https://doi.org/10.1177/2515127420916738 Meares HD, Jones MP (2020) When a system breaks: A queuing theory model for the number of intensive care beds needed during the COVID-19 pandemic. Med J Aust 212(10):1
112
J. Kobrossi and W. Dagher
Mollart L, Newell R, Geale SK, Noble D, Norton C, O’brien AP (2020) Introduction of patient electronic medical records (EMR) into undergraduate nursing education: An integrated literature review. Nurse Educ Today 94:104517 Reuters (2019) Moody’s downgrades Lebanon cites default rick, November 5. Retrieved from https://www.dailymaverick.co.za/article/2019-11-05-moodys-downgrades-lebanon-citesdefault-risk/ Savage M (2020) Transforming medical competency into medical management capability: Developing physician leaders by finding management in medicine, Karolinska Institutet Savall H, Zardet V, Bonnet M (2008) Releasing the untapped potential of enterprises through socioeconomic management. Retrieved from http://ns3040652.ip-164-132-163.eu/siteiseor/ISEOR_ ANGLAIS/pdf/publications-anglaises/Book_Eng_chap5-web.pdf on 15 July 2022 Seth M, LeeThomas H (2020) Fostering change and innovation in health care delivery. Retrieved from https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0587 on 15 July 2022 Ugurluoglu O, Saygılı M, Ozer O, Santas F (2015) Exploring the impacts of personal factors on self-leadership in a hospital setting. Int J Health Plann Manage 30(1):3–13 Zemmar A, Lozano AM, Nelson BJ (2020) The rise of robots in surgical environments during COVID-19. Nat Mach Intell 2(10):566–572 Zhou Y, Zhou Y, Song Y, Ren L, Ng CH, Xiang Y, Tang Y (2020) Tackling the mental health burden of frontline healthcare staff in the COVID-19 pandemic. China’s experiences. Psychol Med 51:1–2.
Jamil Kobrossi is Senior Lecturer in the Faculty of Business Administration and a Professional IT Director with twelve years of experience in managing the IT infrastructure of five university campuses with thirty years of management experience in the Americas, Europe, Middle East, and Africa backed by a Doctorate in Business Administration, a Master of Science in Computer Information Systems, and a Bachelor of Science in Electrical Engineering; sixteen years of IGT experience in managing and implementing projects in Data Centers Operations. He is expert in International Consultancy with extensive experience implementing projects from concept to completion, and trained and skilled professional in leading large groups of people, managing conflicts, empowering teams, building positive environments, and maintaining good communication. He has practical experience in Socio-Economic Approach to Management in Healthcare, Organizational Development, Management Control, Lean and Agile Management, Total Quality Management, and Six Sigma. Expert in identifying Operations’ Hidden Costs in healthcare and converting them to added values. Walid Dagher is an Assistant Professor and Chairman of Business Management and Administration at the University of Balamand, Lebanon. He is a member of the Academy of Marketing Science (AMS). He is a crucial member and coordinator with European NGOs & specialists for CLERH (Lebanese Council for Experts for Human Resources). He is a dedicated instructor and life coach: “Girls leading the next century”. His research interests are in management, marketing, managerial economics, employees performance, CSR, organizational innovativeness, leadership, social media, and business administration. He is a team player with strong team leadership capabilities, excellent communication skills, and good project management skills.
Part III
Economic Issues in Health Sector
Chapter 7
Fighting Against COVID-19: The Role of Consolidated Fiscal Policies and Transparency in Data Sharing Görkem Sariyer
and Ece Acar
Abstract With COVID-19, the importance of integrity and transparency in health systems was once again highlighted all over the world. All countries took many fiscal and non-fiscal precautions to fight against this pandemic, trying to protect the functionality of health systems and to minimize the damage to the public by keeping the spread of the pandemic under control. In addition to non-fiscal responses like curfews, travel bans, social distance, closure of public areas, isolation, etc., countries also made fiscal responses by allocating budgets only to combat the pandemic. Fiscal responses were also split into two categories: the entire budget allocated for the fight against the pandemic and the budget allocated only to health issues. The budgets under both categories were announced by many counties at the beginning of each quarter, starting from October 2020, January 2021, and April 2021. However, from the global context, it was observed that there were very serious differences between the fiscal responses namely financial support provided by the countries. Also, while some countries did not share any data in this area, it was also observed that some of the other countries did not take any fiscal responses. In this study, which will be developed by examining the data of many countries in depth and comparatively, we aim to analyze the success of countries that share their data in a transparent, regular way in managing the COVID-19 pandemic. This study highlights not only the consolidated fiscal policies but also the integrity and transparency in data sharing policies of health systems to fight with this pandemic and to decrease the possible risk in economies arising from this pandemic in the long run. Keywords COVID-19 · Fiscal budgets · Budget transparency
G. Sariyer (B) · E. Acar Department of Business Administration, Faculty of Business, Yasar University, Izmir, Turkey e-mail: [email protected] E. Acar e-mail: [email protected] © The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd. 2023 K. T. Çalıyurt (ed.), Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II, Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application, https://doi.org/10.1007/978-981-99-5502-2_7
115
116
G. Sariyer and E. Acar
7.1 Introduction The whole world has been fighting the COVID-19 epidemic since 2019. Since the epidemic turned into a pandemic, the economies of many countries around the world have come under a great burden that they cannot handle. Therefore, it is very clear that this struggle is not only taking place on the health front, but there is also a great war that goes beyond the struggle on the economic front. In the process of managing this war, the economic systems of the countries have actually proven how healthy they are. The concepts of health and economy have actually appeared together and intertwined for years, but this process has officially proven to us that these two concepts are actually inseparable and important. To cope with this struggle, governments used budgets, which are important support tools of public finance. Therefore, in such a crisis period, budgeting has become a significant policy instrument in order to give a comprehensive respond to the crisis. Usually in all countries the respond on the revenue side of the budget is much stronger compared to the expenditure side (Schick 2009). However, this is not a typical economic crisis; this is a health crisis seriously affecting and waiting support from economy. Therefore, the budgets created for the aim of managing pandemic can be considered as budgets with only expenditure side and not revenue side. The revenue here may be thought as to survive this crisis without any damage. Another important aspect to cope with such a crisis is to ensure transparency both for fiscal and non-fiscal measures. Because where governments are open and transparent to the public, citizens’ awareness increase, thereby they would feel to be more involved in actions (Moon 2020). However, in times of crisis, governments may overlook controls to provide immediate action. Even if they provide transparency, the cognitive load required to understand and address complex issues can hinder constructive discussion (Moll and Quayle 2021). Therefore, governments need to be very careful, especially regarding financial measures at such circumstances. Considering COVID-19 as a multifaceted worldwide crisis, this chapter provides broad perspective on countries’ budgetary response to COVID-19 pandemic. In fact, the purpose of this chapter is to analyze the success of countries in terms of budget transparency regarding countries’ level of development. The data of this study was received from the International Monetary Fund’s (IMF) database of fiscal response monitor to COVID-19 which summarizes key fiscal measures governments have announced against COVID-19, and 190 countries’ fiscal responses in respective three announcement (October 2020, January 2021, and April 2021) periods were analyzed. The results mainly show that while G20: advanced economies and G20: emerging markets countries were transparent, countries listed in other selected emerging markets and selected low-income developing countries had problems in terms of fiscal response transparency. The results also show that while some of the countries were transparent in sharing sub-total fiscal responses against COVID19, they did not keep their success for being transparent in sharing their budgets specifically for health.
7 Fighting Against COVID-19: The Role of Consolidated Fiscal Policies …
117
The remainder of the chapter is structured as follows: Section 7.2 briefly outlines theoretical background of budget transparency and budgetary response to crisis. Section 7.3 demonstrates empirical analysis. Section 7.4 discusses the results and Sect. 7.5 presents conclusion.
7.2 Theoretical Background The main component of public finance management system is primarily the development of the financial dimension of the system in line with the government’s strategy, that is, the creation of the budget. Then, the execution of appropriations, in-year monitoring and reporting, year-end reporting and auditing are involved in the implementation of the system (Ball 2020). Therefore, it is very clear that budgets are the main drivers of public financial management system. However, in times of crisis, things can work differently, and governments may have to make contingency plans accordingly. Likewise, economic dimension of COVID-19 pandemic has caused unexpected variations from normal budgeting system. The difficult and uncertain environment released by COVID-19 pandemic has revealed exactly this situation. In order for governments to respond quickly to the needs of the moment, budgets have been created that prioritize public spending to protect health and livelihoods that are fit for purpose, leaving income out of the question. At the same time, budget flexibility was given to ministries so that they could deal effectively with the crisis. As the COVID-19 pandemic is also a very difficult process to manage from an economic point of view, it has become crucial for the government to provide clear and concise policy guidelines by providing information with budget responses (Narayan and Kommunuri 2021). When all these are taken into account, the following sub-sections highlight the budget transparency and budgets during crisis in line with the research question of this chapter.
7.2.1 Budget Transparency The demand for transparency has increased in many areas in recent years. In general terms, transparency means institutions and organizations’ releasing information they are accustomed to withholding. Hence, without pressure voluntary transparency will rarely come into scene (Florini 2000). From public point of view, fiscal transparency “entails being open to the public about the government’s past, present, and future fiscal activities, and about the structure and functions of government that determine fiscal policies and outcomes” (IMF 2008). Again, from public point of view but more specifically, this time budget transparency and it is defined as “the full disclosure of all relevant fiscal information in a timely and systematic manner” (OECD 2020). Budget transparency is a tool that influences the quality of governance and thus encourages governments to be more accountable. Considering agency theory and
118
G. Sariyer and E. Acar
public choice theory, a high level of transparency reduces the information asymmetry between government and citizens. Thus, citizens can better follow the actions of the government (Bisogno and Cuadrado-Ballesteros 2021). In order to increase accountability and decrease information asymmetries, governments should allow citizens to follow different steps of the budgeting process, that is, they should be transparent. However, just to fulfill some legal obligations in terms of transparency, governments may publish some information even if it is not useful to citizens. It is also a fact that too much information presented in the name of transparency can create information pollution, that is, uncertainty and confusion (Grimmelikhuijsen 2012). Therefore, while during disclosure process to citizens for transparency, governments should consider the quantity of information as well as the quality and present adequate and explanatory information (Cook et al. 2010). Transparency is essential at all levels to build public trust and support. In particular, when we have adequate and accessible information about the financial performance and position of the government, the better we can ensure that its financial position is sound (Ball 2020). When concepts such as COVID-19, transparency, budget, success, and trust are brought together, we come across the example of New Zealand. The transparent structure of the New Zealand government is also being used to show the nature and scope of this transparency during the pandemic process. With the “go early, go hard” strategy, the government showed the possible effects of the pandemic in its financial statements at the very early stage. The government also reflected the estimated financial effects of the pandemic to its strategy reports (Narayan and Kommunuri 2021). The release of the New Zealand government’s full set of accrualbased financial statements during the pandemic with a detailed four-year outlook and ten-year long-term forecasts is indicative of its stance towards transparency (Moll and Quayle 2021). Therefore, it seems that in such crisis processes, transparency is very important in terms of managing the situation.
7.2.2 Budgets During Crisis We all agree that COVID-19 started as a health issue however turned into an economic crisis worldwide. One of the government’s duties is to prepare the financial budget and share it with its citizens and not to compromise on accountability and transparency in this process. In fact, governments accustomed to economic crises were caught off guard when faced with a multifaceted crisis like COVID-19. Because the pandemic has affected governments in terms of health, social, and economic aspects. Governments struggling to overcome the health crisis have started to take action economically and to work on how to overcome the effects of the economic crisis created by the pandemic. In this situation, some governments acted proactively while others lagged behind. While some ignored the concepts of transparency, accountability, and therefore trust, others strictly adhered to these concepts and implemented their fiscal policies.
7 Fighting Against COVID-19: The Role of Consolidated Fiscal Policies …
119
Given the unprecedented uncertainties in the context of the COVID-19 crisis, it will be difficult for all countries to prepare budgets for many years in the unpredictable future. It is a fact that in the coming years, budgeting and its approval will gain even more importance with the pandemic. Authorities need to put more emphasis on clarity, credibility, and public focus. First of all, it is necessary to increase the confidence in the government’s financial, economic, and social strategy. In this context, to assure the citizens governments should focus on following points during budget documentation: explanation of assumptions and uncertainty in the fiscal and economic outlook; production of forward-looking guidance on financing; and presentation of the benefits and impacts for different groups in the economy (Curristine et al. 2020). Furthermore, from academic point of view there are plenty of research about budgeting process during COVID-19 crisis. For instance, Moll and Quayle (2021) studies transparency process of three Australian state governments in the context of providing accountability for economic response to pandemic. They found that information provided by the governments is questionable. Also, Ahrens and Ferry (2021) focuses on the accounting and accountability practices of the UK government’s response pandemic. Their findings suggest that with the crisis extending over longer budget and financial reporting periods, a spending review is necessary for better planning. Moreover, Argento et al. (2020) compared budgetary implications of three Nordic countries: Norway, Finland, and Sweden. They found that their attitudes towards fighting against health crisis affected their attitudes towards fighting against budgetary crisis. In light of this theoretical background, by analyzing the panel data of 190 countries’ fiscal responses summarized in IMF database of fiscal response monitor to COVID-19, we aim to comparatively analyze the success of these countries in terms of their budget transparency.
7.3 Data and Methodology Data for this study was received from IMF database of fiscal response monitor to COVID-19. Key fiscal measures governments have announced or taken in selected economies in response to the COVID-19 pandemic were summarized in this database. Additional spending or foregone revenues of each country in response to COVID19 was reported in terms of USD billion dollars and percentage (%) of GDP in this data source. Moreover, in addition to sub-total values of these fiscal measures, the measures taken just for health were also documented. While the first report has been published in October 2020, the updated cumulative reports were published in a quarterly basis. Based on their development levels, these selected economies were grouped in five categories as follows: • G20: advanced economies • G20: emerging markets • Other selected advanced economies
120
G. Sariyer and E. Acar
• Other selected emerging markets • Selected low-income developing countries. In this study, fiscal measures taken by governments in terms of % of GDP for each country listed in these five development level categories were used. First three reports respectively documented in October, January, and April were investigated. Key fiscal measures governments have announced in response to COVID-19 as of September 11, 2020, were summarized in the report published in October. While the second report published in January summarized the cumulative measures as of December 31, 2020, the third report summarized the cumulative measures as of March 17, 2021. For each of these periods, sub-total measures and also the measures just in the health sector were comparatively analyzed for each country in this study. Thus, using panel data of 190 countries listed in the IMF fiscal response monitor database for three reported periods, it was mainly aimed to analyze total, and health system related fiscal measures taken by governments in response to COVID-19. Since transparency is a key driver in managing pandemic situations, it was also aimed to identify the governments, which were more transparent in sharing fiscal measure responses. Governments taken almost no sub-total and/or health system related fiscal measures were presented in this study. For each of the five development level categories, the main statistics (minimum, maximum, and average) of the sub-total and health-related fiscal measures were also described. Thus, it was finally aimed to quantitatively compare the fiscal responses of countries based on their development levels.
7.4 Results The study data set included 190 countries’ panel data where the number of countries for each development level category (G20: advanced economies, G20: emerging markets, other selected advanced economies, other selected emerging markets, selected low-income developing countries) were respectively as 10, 10, 27, 84, and 59. The countries having no announcements on sub-total and/or health sector-related fiscal measures for each of the analyzed three periods were summarized in Table 7.1. In Table 7.1, it was observed that all of the 20 countries listed in G20: advanced economies and G20: emerging markets announced both of their sub-total and health sector related fiscal measures in response to COVID-19 for all of the report periods. This showed that the governments of G20: advanced economies and G20: emerging markets followed a transparent policy in fiscal responses announcements. It was also observed that, almost all of the 27 countries listed in other selected advanced economies, except San Marino and Norway, were also transparent in sharing their fiscal responses. While Norway had no announcement only in health sector measures of the first report period, fiscal measures of this country started to be announced in January 2021. Although San Marino had no announcement in the first two report dates on both the sub-total and health sector measures, at least the sub-total measures of this country started to be announced in the third report date. On the other hand, it
7 Fighting Against COVID-19: The Role of Consolidated Fiscal Policies …
121
Table 7.1 List of countries with no-announcements Category
Fiscal measures
Sep 11, 2020
Dec 31, 2020
Mar 17, 2021
G20: advanced economies (N = 10)
Sub-total
NA
NA
NA
Health
NA
NA
NA
G20: emerging markets (N = 10)
Sub-total
NA
NA
NA
NA
NA
NA
Other selected advanced Sub-total economies (N = 27) Health
Health
San Marino
San Marino
NA
San Marino, Norway
San Marino
San Marino
Other selected emerging Sub-total markets (N = 84)
Anguilla, Belarus, Ecuador, Guyana, Lebanon, Montserrat, Oman (n = 7)
Anguilla, Belarus, Ecuador, Guyana, Lebanon, Montserrat, Oman (n = 7)
Angola, Anguilla, Guyana, Lebanon, Montserrat, Oman (n = 6)
Angola, Anguilla, Belarus, Belize, Bosnia and Herzegovina, Bostwana, Brunei Darussalam, Ecuador, Guyana, Kazakhstan, Kuwait, Lebanon, Libya, Montserrat, Oman, Paraguay, Qatar, Thailand, the United Arab Emirates, Uruguay (n = 20)
Angola, Anguilla, Belarus, Belize, Bosnia and Herzegovina, Brunei Darussalam, Ecuador, Guyana, Kazakhstan, Kuwait, Lebanon, Libya, Montserrat, Oman, Paraguay, Thailand, the United Arab Emirates, Uruguay (n = 18)
Anguilla, Belize, Brunei Darussalam, Guyana, Kazakhstan, Kuwait, Lebanon, Libya, Montserrat, Oman, Paraguay, Qatar, Thailand, the United Arab Emirates, Uruguay (n = 15)
Bhutan, Eritrea, Yemen (n = 3)
Bhutan, Eritrea (n = 2)
Bhutan, Eritrea, Nepal, Tanzania (n = 4)
Health
Selected low-income Sub-total developing countries (N = 59)
was mainly observed that countries grouped in other selected emerging markets and selected low-income developing countries were not transparent as the countries of higher development levels. It was presented that 8.33, 8.33, and 7.14% of the other selected emerging market countries did not announce their sub-total fiscal measures, respectively, in the first, second, and third report dates. Non-transparency percentages of these other selected emerging market economies in health sector measures were calculated as 23.81, 21.43and 17.86% in the three respective periods. For the countries listed in selected income developing countries while non-transparency percentages in sub-total fiscal measures were calculated 5.08, 3.39, and 6.78% respectively,
122
G. Sariyer and E. Acar
the respective percentages in health sector fiscal measures were 10.17, 6.78, and 10.17%. Thus, it was concluded that for the last two development level categories while the countries were relatively more transparent in announcing their sub-total measures, they were more nontransparent in sharing their health sector measures. In this study, the main descriptive statistics were also calculated in order to present the difference in the taken fiscal measures of the five development level categories. The results were summarized below in Table 7.2. In Table 7.2, it was mainly observed that highest minimum and average statistics on the sub-total fiscal measures were obtained in G20: advanced economies for all the three report periods. However, the maximum values of sub-total fiscal measures were obtained for other selected advanced economies. This un-expected result was obtained for the country Macao SAR listed in other selected advanced economies. When the fiscal measures of this category countries analyzed, it was also observed that besides Macao SAR, New Zealand and Singapore had also higher sub-total fiscal measures for all three report dates compared to almost all G20: advanced economies and G20: emerging market economies countries. While the New Zealand spent 19.5, 19.1, and 19.3% of the country GDP in the respective three announcement periods, Singapore announced that 16.1, 16.3, and 16.0% of its GDP was spent in response to COVID-19 in these periods. Another interesting finding was obtained for other selected emerging markets and selected low-income developing countries. It was observed that countries categorized in these development levels obtained close and even more statistics compared to the countries listed in the first three development levels. This result was related to the financial support granted by the IMF to support Table 7.2 Minimum, maximum, and average statistics of fiscal measures (% of GDP) of the countries in each category Sep 11, 2020
Dec 31, 2020
Mar 17, 2021
Category
Fiscal measures Min Max Avg Min Max Avg Min Max Avg
G20: advanced economies (N = 10)
Sub-total
3.5
12.5 8.2
3.4
Health
0.3
1.5 0.8
0.3
5.3
1.6 0.5
7.5
2.0
Sub-total
0.6
8.3 3.3
0.7
8.3
3.5 0.7
8.8
4.0
G20: emerging markets (N = 10) Other selected advanced economies (N = 27) Other selected emerging markets (N = 84)
16.7 11.3 4.5
25.5 12.8
Health
0.1
1.8 0.5
0.1
1.8
0.6 0.1
1.8
0.8
Sub-total
2.5
25.0 7.1
1.8
25.3
7.4 0.8
27.4
8.5
Health
0.0
1.0 0.5
0.0
1.8
0.8 0.0
2.0
0.8
Sub-total
0.0
17.7 3.6
0.0
17.6
3.7 0.0
17.2
3.8
Health
0.0
5.1 0.7
0.0
5.0
0.7 0.0
8.0
0.9
0.0
10.6 2.4
0.0
13.0
2.8 0.0
15.8
3.1
Selected Sub-total low-income developing countries (N = 59)
7 Fighting Against COVID-19: The Role of Consolidated Fiscal Policies …
123
the fight against COVID-19 by this group of countries. On the other hand, when the sub-total and health sector measures were compared, it was also observed that fiscal measures allocated to health were not much in the total for all of the development levels. Finally, when these cumulative measures in the respective three announcement periods were compared, it was mainly observed that the highest measures were taken in the first period (until September 11, 2020). In Table 7.3, the countries that have taken (almost) no sub-total and/or health sector fiscal measures in fighting against this pandemic were also presented. The 0.0 values in fiscal measures were represented the practically no taken measures, since the values were converted and shown in one decimal. Once again in Table 7.3, it was observed that all of the countries listed in G20: advanced economies and G20: emerging markets had taken at least some level of their % of GDP in the fight against COVID-19. Thus, it was concluded that G20: advanced economies and G20: emerging markets were both transparent and taking fiscal measures in response to COVID-19. Similarly, the countries listed in other selected advanced economies were taken fiscal measures. Only Denmark in this category had almost no spending of its GDP for health sector. This can be related with the almost perfection of the health system in Denmark (Olagnier and Mogensen 2020). However, at least some of the countries listed in other selected emerging markets and selected low-income developing countries had taken almost no fiscal measures in response to COVID-19. Table 7.3 List of countries with (almost) no additional spending or foregone revenues Category
Fiscal measures
Sep 11, 2020
Dec 31, 2020
Mar 17, 2021
G20: advanced economies (N = 10)
Sub-total
NA
NA
NA
Health
NA
NA
NA
G20: emerging Sub-total markets (N = 10) Health
NA
NA
NA
NA
NA
NA
Sub-total
NA
NA
NA
Health
Denmark (n = 1) Denmark (n = 1) Denmark (n = 1)
Other selected advanced economies (N = 27)
Other elected Sub-total emerging markets Health (N = 84)
Selected low-income developing countries (N = 59)
Sub-total
Turkmenistan
Turkmenistan
Turkmenistan
Iraq, Nauru, Palau, Turkmenistan, Vanuatu (n = 5)
Iraq, Nauru, Palau, Turkmenistan, Tuvalu, Vanuatu (n = 6)
Iraq, Palau, Turkmenistan, Vanuatu (n = 4)
Lao P.D.R., Tanzania (n = 2)
Lao P.D.R., Tanzania (n = 2)
Lao P.D.R., Tanzania (n = 2)
124
G. Sariyer and E. Acar
As a final analysis, the sub-total and health sector fiscal measures of G20: advanced economies and G20: emerging markets countries were represented in a clustered bar chart form for the three announcement periods. While sub-total measures were shown in the primary vertical axis of these charts, health sector measures were shown in the secondary vertical axis. In Fig. 7.1, it was mainly observed that while Australia, Japan, the United Kingdom, and the USA had relatively close sub-total measures in terms of % of their GDP in the first two periods, the USA significantly increased its spending or foregone revenue during the third period. Another important finding of Fig. 7.1 relates to health sector measures of the United Kingdom. It was seen that the United Kingdom increased its health sector related measure to 5.3 and 7.5% of its GDP in second and third quarters, while this measure was only around 1.5% of its GDP in the first announcement period. This finding can be linked to the problems of health system in the United Kingdom. During COVID-19 pandemic, mainly for inadequate healthcare workers and physical capacities, the health system of this country was highly criticized (Hunter 2020) and thus this government adopted relatively higher measures and actions compared to many other countries (Zala et al. 2020). In Fig. 7.2, it was observed that for all of the three periods, Brazil took the highest sub-total measures between the G20: emerging market countries. However, when the health sector measures were analyzed, it was observed that Saudi Arabia had the highest values. Indeed, it was observed that Saudi Arabia’s fiscal measures in the health sector accounted for the majority of the sub-total. On the other hand, Turkey and Mexico were observed as the countries taking lowest sub-total fiscal measures within the G20: emerging markets countries. On the other hand, while China was observed to take higher sub-total measures compared to many of the other G20: emerging market countries, it had the lowest health sector related fiscal measures.
Fig. 7.1 Sub-total and health sector measures (as % of GDP) for G20: advanced economies for the three announcement periods
7 Fighting Against COVID-19: The Role of Consolidated Fiscal Policies …
125
Fig. 7.2 Sub-total and health sector measures (as % of GDP) for G20: emerging markets for the three announcement periods
7.5 Conclusion This chapter primarily takes a broad view of countries’ budgetary response to the COVID-19 pandemic. More specifically, the chapter analyzes the success of countries in terms of budget transparency regarding their level of development. It is a phenomenon that is already known how important transparency is in terms of managing the pandemic. In this context, initially it was analyzed whether the countries made an announcement about their budgetary response in the face of pandemic. As a result of the analysis, it was concluded that the G20 countries (both advanced economies and emerging markets) have announced to the public the financial measures they have taken for all periods of the pandemic so far. Moreover, it has been revealed that advanced economies other than G20 countries have also presented the necessary information about fiscal measures to the public. In this respect, we can say that the governments of advanced economies (but also emerging markets in G20 countries) are following a transparent policy by announcing information about the financial measures taken during the pandemic to their citizens. On the contrary, the governments of developing and low-income economies remain rather weak in transparency. It was concluded that while these countries were relatively straightforward in announcing their sub-total measures, they were not as transparent in their health sector measures. In addition, considering the level of development of the economies, it has been concluded that the financial measures to manage the pandemic taken by the G20 countries and other selected advanced economies are higher. When we examine the budgets allocated by the countries for the pandemic in proportion to their GDP, the highest result is in these economies. These are expected results. However, another
126
G. Sariyer and E. Acar
remarkable result was found in emerging markets and low-income developing countries. It is observed that these economies allocate close or even higher budgets when compared to other developed and developing economies. The reason for this is not something that those governments do themselves but related to the financial support provided by the IMF in the fight against the pandemic. It has been concluded that countries with G20 countries both advanced and emerging economies and other advanced economies other than G20 have used some of their GDP in the fight against the pandemic. Therefore, it can be concluded that these countries took the necessary financial measures managing the pandemic and disclosed these measures in a transparent manner. On the contrary, it was concluded that emerging economies and low-income countries did not take or could not take the necessary financial measures and did not share information about them. As a theoretical contribution, this chapter puts forward the budget responses of countries in the fight against the pandemic, taking into account their level of development. This is important because the crisis is not only about health but also about economy and in this process, while some economies are successful, some are having difficulties. The results show that developed economies stand out with the budgets they allocate and the transparent policy they display on this issue. Of course, another issue is whether these developed economies are transparent because they are developed or are they developed because they are transparent. This is another topic of discussion. In terms of practical implications, we argue that governments can willingly focus on transparency by following a firm and clear strategy in dealing with unexpected crises. Governments can be more successful in handling with this and similar crises if they transparently involve the citizens affected by this uncertainty in the process to a certain extent.
References Ahrens T, Ferry L (2021) Accounting and accountability practices in times of crisis: a Foucauldian perspective on the UK government’s response to COVID-19 for England. Acc Audit Account J 34(6):1332–1344 Argento D, Kaarbøe K, Vakkuri J (2020) Constructing certainty through public budgeting: budgetary responses to the COVID-19 pandemic in Finland, Norway and Sweden. J Public Budg Account Financ Manag 32(5):875–887 Ball I (2020) Reflections on public financial management in the Covid-19 pandemic. J Account Organ Chang 16(4):655–662 Bisogno M, Cuadrado-Ballesteros B (2021) Budget transparency and governance quality: a crosscountry analysis. Publ Manage Rev 24:1–22. Cook FL, Jacobs LR, Kim D (2010) Trusting what you know: information, knowledge, and confidence in social security. J Polit 72(2):397–412 Curristine T, Doherty L, Imbert B, Rahim FS, Tang V, Wendling C (2020) Budgeting in a crisis: guidance for preparing the 2021 budget. IMF Special Series on COVID-19 1:1–10. Florini A (2000) The politics of transparency. Paper presented at the Annual Meeting of the International Studies Association, Los Angeles.
7 Fighting Against COVID-19: The Role of Consolidated Fiscal Policies …
127
Grimmelikhuijsen S (2012) A good man but a bad wizard. About the limits and future of transparency of democratic governments. Inf Polit 17(3–4):293–302. Hunter DJ (2020) Covid-19 and the Stiff upper lip-the pandemic response in the United Kingdom. N Engl J Med 382(16):e31 IMF (2008) Fiscal transparency. Available at http://www.imf.org/external/np/fad/trans/index.htm Moll J, Quayle A (2021) Transparency of emergency state government spending: the case of COVID19 in Australia. In 13th Interdisciplinary Perspectives on Accounting Conference (IPA). Moon MJ (2020) Fighting COVID-19 with agility, transparency, and participation: wicked policy problems and new governance challenges. Public Adm Rev 80(4):651–656 Narayan AK, Kommunuri J (2021) New Zealand Government’s budgetary response to the COVID19 pandemic. Pac Acc Rev 33:596–602 OECD (2020) OECD best practices for budget transparency. Available at https://www.oecd.org/ governance/budgeting Olagnier D, Mogensen TH (2020) The Covid-19 pandemic in Denmark: big lessons from a small country. Cytokine Growth Factor Rev 53:10–12 Schick A (2009) Crisis budgeting. OECD J Budg 9(3):119 Zala D, Mosweu I, Critchlow S, Romeo R, McCrone P (2020) Costing the COVID-19 pandemic: an exploratory economic evaluation of hypothetical suppression policy in the United Kingdom. Value Health 23(11):1432–1437
Görkem Sariyer, Ph.D., works as an Associated Professor in the Department of Business Administration at Ya¸sar University, Turkey. She received her BSc degree from Software Engineering Department; her MSc degree from the Applied Statistics Department, at Izmir University of Economics, Izmir, Turkey; and her Ph.D. from Department of Industrial Engineering and Operations Management, at Koç University, Istanbul, Turkey, on modeling strategic customers’ decision and behavior on queuing type service systems. Her research interest includes operations planning and decision-making in service/manufacturing systems. She focuses primarily on emergency health services. She joined the Yasar University Department of Business Administration in September 2013. She is also vice dean since 2016. Ece Acar, Ph.D., is working as an Assistant Professor in the Department of Business Administration at Yasar University, Turkey. After completing her undergraduate studies at the Faculty of Economics and Administrative Sciences at Dokuz Eylül University, she completed Master’s from the European Studies Department and Ph.D. from the Business Administration Department at ˙Izmir University of Economics. She started her academic career as a Research Assistant in 2004 at ˙Izmir University of Economics and continued her academic career as Lecturer in 2010 at the same University. In 2014, she was appointed to the assistant professorship at Ya¸sar University. She works as a full-time academician at the Faculty of Business at Ya¸sar University. Her research interests are corporate governance, financial reporting, disclosure, and corporate social reporting. She has several published research on Accounting, Corporate Governance, and Financial Reporting.
Chapter 8
Investigation of Dyspnea and Quality of Life in Patients with Heart Failure Eda Ertu˘grul and Serap Ünsar
Abstract This descriptive and cross-sectional study was planned to investigate dyspnea and quality of life in patients with heart failure and affecting factors. The study was carried out with 143 patients who applied to a City Hospital in Istanbul with the diagnosis of heart failure between November 01, 2019 and April 30, 2020. The data of the study were collected using a “Patient Information Form”, the “Left Ventricular Dysfunction Scale”, and the “Basal Dyspnea Index Scale”. Shapiro–Wilk test, independent groups t test, Mann–Whitney U test, Kruskal–Wallis, Pearson correlation as well as descriptive methods (mean, Standard deviation, frequency) were used in the NCSS (Number Cruncher Statistical System) 2007 (Kaysville, Utah, USA) program for the analysis of data. Analysis, KR-20 and Cronbach’s alpha were used. Statistical significance was accepted as p c
C
B
A
Measurements
1.97
2.03
1.91
2.45
1.64
1.87
2.57
1.55
Rank Mean
(continued)
p = ,948
X2 = ,329 Sd = 2
P < 0.05
p = ,000
X2 = 31.01 Sd = 2
P < 0.05
p = ,000
X2 = 52.51 Sd = 2
Statistical Analysis
Table 12.5 According to some physiological variables of intubated and sedated intensive care unit patients’ comparison of aspiration and position measurements (n = 91)
208 F. Güçlü and S. Ünsar
2.14
97.3 ± 2
C
Aspiration Sequence
After Aspiration
B
C
Aspiration Sequence
After Aspiration
B
C
2,91 1.75
20.6 ± 4.88
16.8 ± 4.45
2.04
36.5 ± 0.136
1,34
2.08
36.5 ± 0.147
15.6 ± 3.55
1.88
36.5 ± 0.179
Friedman Test
Difference Results: a < b - a < c - b > c
Before Aspiration
A
Respiration Count
Difference Results: –-
Before Aspiration
A
Fire
Difference Results: a < b - a < c
After Aspiration
Rank Mean
Mean ± SD
Measurements
Table 12.5 (continued)
P < 0.05
p = ,000
After Position
Position Sequence
Before Position
After Position
Position sequence
16.4 ± 40.5
17.7 ± 4.31
15.9 ± 3.95
36.5 ± 0.168
36.5 ± 0.1
36.5 ± 0.121
97.2 ± 1.72
Mean ± SD
Difference Results: a < b - a < c - b > c
C
B
Before Position
Difference Results: –-
C
B
X2 = 132.27 Sd A =2
P > 0.05
p = ,186
After Position
Difference Results: –-
C
Measurements
X2 = 3.36 Sd = A 2
P < 0.05
Statistical Analysis
1.9
2.66
1.45
2.01
2.12
1,87
2
Rank Mean
P < 0.05
p = ,000
X2 = 84.33 Sd = 2
P > 0.05
p = ,074
X2 = 5.21 Sd = 2
P > 0.05
Statistical Analysis
12 Evaluation of Pain in the Critical Care Unit Patients Who Had Intubated … 209
210
F. Güçlü and S. Ünsar
Table 12.6 Correlation results of the measurement scores of the CPOT and RSS (n = 91) Variables
CPOT Measurements
RSS Measurements
Aspiration
Position
Aspiration Sequence
Position Sequence
Aspiration
Aspiration Sequence
rrho : -0,562 p < 0,001
rrho :-0,279 p: 0,007
Position
Position Sequence
rrho :-0,577 p < 0,001
rrho : -0,650 p < 0,001
rrho : Spearman’s rho correlation coefficient p < 0.01: Spearman’s rho correlation coefficient p value
The correlation results of the scores of the CPOT and RSS are presented in Table 12.6. A statistically significant negative linear (p < 0.000) and moderate correlation was found between the RSS aspiration order measurement scores and the CPOT aspiration order measurements. As the RSS aspiration order measurement scores increased, the CPOT aspiration order measurement scores decreased. A statistically significant negative linear (p < 0.000) and moderate correlation was found between the RSS position order measurement scores and the CPOT aspiration order measurements. As the RSS measurement scores during positioning increased, the scores of CPOT during suctioning decreased. During aspiration and positioning, the patient’s level of alertness increased, and pain intensified.
12.7 Discussion Intubated and sedated patients in intensive care units experience pain due to endotracheal tube. The use of sedative, neuromuscular blocking agents makes the assessment of pain difficult. In this case, it is recommended to use behavioral and physiological indicators for pain assessment (Akyol 2017; Arbour and Gélinas 2014; Korhan 2012; Tülin and Çelik 2019). The duration of intensive care hospitalization was 4.62 ± 11.11 days, intubation period was 3.23 ± 6.18 days, and sedation period was 2.76 ± 2.70 days. In the (Menekli et al. 2021) study of Menekli et al., the duration of intensive care hospitalization was 10.23 ± 8.78, the duration of intubation was 6.37 ± 7.81.; Puntillo et al. (2016) reported the duration of hospitalization as 7 days; Korhan et al. (2013) reported the duration of intubation as 20.45 ± 3.58 days. In our study, when we examined the pain scores and behaviors of endotracheal aspiration and positioning procedures, 95.6% of intubated and sedated patients felt pain during endotracheal aspiration and 67% felt pain during positioning. Many nursing interventions performed in intensive care units cause pain in patients. Ayasrah (2016) reported that 89.9% of patients experienced pain and endotracheal aspiration and positioning were the most painful procedures in his study In the study of Robleda
12 Evaluation of Pain in the Critical Care Unit Patients Who Had Intubated …
211
et al. (2016), 86% felt pain during endotracheal suctioning and changing position. In a study by Esen et al. on pain behaviors during aspiration and (Esen et al. 2010a, 2010b) change of position, it was reported that one-third of the patients felt pain. As seen in our study, the proportion of patients who felt pain in aspiration and position change procedures, which are among the painful procedures performed in intensive care units, is quite high. It is thought that the inability of the intubated and sedated patient who cannot communicate to express the need for analgesia and the anxiety caused by the inadequacy of sedation in invasive and noninvasive procedures may increase the feeling of pain. In this study, pain scores associated with aspiration and positioning procedures were evaluated. The ICPS score during aspiration and positioning was 5.13 ± 1.70 and 3.42 ± 1.57, respectively. Aspiration and positioning showed an increase compared to before. In the study of Al Sutari et al. (2014), it was determined that the first three interventions with the highest behavioral pain score were aspiration, positioning, and invasive intervention, respectively. Ribeiro et al. (2017) reported that the pain score during aspiration was significantly higher in their study. The study by Olsen et al. (2021) and the study by Ito et al. (2022) found that patients experienced pain during positioning. In our study, pain intensity during aspiration was higher than pain intensity during positioning. Similar to this, when we look at the studies conducted in our country, Esen et al.’s (2010a, 2010b) and Akta¸s’s (2016) studies also reported that pain scores increased during aspiration and positioning, and the pain score during aspiration was higher than the pain score during positioning. Aspiration is an invasive procedure compared to positioning. In this process, we think that weaning the patient from the ventilator and draining the secretions with the help of an aspiration catheter are traumatic and the severity of pain associated with the aspiration procedure is higher. In our study, grimacing, which was absent before aspiration, increased to 45.1% during aspiration, protective body movements increased from 11 to 58.2%, fighting with the ventilator increased from 1.1 to 68.1%, and muscle tension increased from 9.9 to 52.7%. Mechanically ventilator-dependent patients in intensive care units are unable to communicate verbally due to sedation and altered state of consciousness, and therefore cannot give physical and psychological responses to the pain they experience. They can express their pain experience behaviorally. Therefore, it is accepted that observation of pain behaviors is a valid approach in pain assessment (Alakan et al. 2018). When assessing pain experiences, the most frequently observed pain behavior was reported to be grimacing (Aslan et al. 2007). In studies conducted with patients on mechanical ventilation, pain behaviors observed included grimacing face and forehead, facial redness, trying to make sounds, sighing, biting the intubation tube, moving the treated area away from the painful stimulus, clenching the fist, bending the knees towards the abdomen, and pushing the person performing the treatment (Gündo˘gan, Bor et al. 2016; Sarıcao˘glu et al. 2005). Robleda et al. (2016) reported significant increases in facial expression and limb movements during aspiration. Efe et al. (2020) reported tense facial expression and/or grimacing, ventilator non-compliance, and increased muscle tension behaviors. Esen et al. (2010a, 2010b) observed that 46.6% of the patients pulled their legs towards their abdomen, 26.7%
212
F. Güçlü and S. Ünsar
supported the incision site, 6.7% chewed the intubation tube, and 20% both supported the incision site and pulled their legs towards their abdomen during aspiration. In a study of painful procedures including tracheal aspiration and position change, it was reported that observed pain behaviors included “grimacing” (42.8%), “closing eyes” (33.7%), “restlessness” (26.8%), “startling” (23.7%), and verbal “mumbling” (23.7%) (Puntillo et al. 2014). In our study, grimacing, which was absent before aspiration, increased to 45.1% during aspiration, protective body movements increased from 11 to 58.2%, fighting with the ventilator increased from 1.1 to 68.1%, and muscle tension increased from 9.9 to 52.7%. Tense facial expression increased from 12.1% before the position to 65.9% during the position, protective body movements increased from 5.5 to 58.2%, ventilator compliance coughing but tolerating ventilator response increased from 17.6 to 60.4%, muscle tension increased from 12.1 to 50.5%. In Vázquez et al.’s (2011) study, facial tension increased by 52%, restlessness agitation by 42%, fighting the ventilator by 31%, and muscle tension by 24%. Esen et al. (2010a, 2010b) reported that 50% of the patients pulled their legs towards the abdomen, 25% supported the incision site, and 25% chewed the intubation tube during positioning. Patients describe their pain during aspiration by fighting with the ventilator, causing alarms to be activated. Since there is an intervention in the respiratory tract in the aspiration process, it is thought that when it is disconnected from the mechanical ventilator, aspirated and reconnected, it spends power to ensure the same harmony, so it is thought to react mostly with the ventilator. In the position, the tension of the tube, the folding of the respiratory circuits in the head and neck, creates a feeling of discomfort in the mouth and face, and it is thought that the patient may express his pain with his face if his head is not placed appropriately in the position. It has been reported in the literature that pain stimulates the sympathetic nervous system and increases heart rate, respiratory rate, and blood pressure, causing psychological and physiological changes (Nesek Adam et al. 2015). In the study by Menekli et al., there was a significant difference in mean systolic and diastolic blood pressure, heart rate, respiratory rate, and saturation scores before, during, and after endotracheal aspiration (Menekli et al. 2021). Arroya-Novoa et al. reported that tracheal aspiration in the intensive care unit increased systolic and diastolic blood pressure and pulse rate (Arroyo-Novoa et al. 2008). In our study, while heart rate, mean arterial pressure, and respiratory rate increased during aspiration and positioning and a significant difference was found, there was no change in body temperature. Saturation decreased during aspiration and increased after aspiration, while there was no change in saturation during positioning. The literature reported changes in hemodynamic parameters, while some studies reported no change (Ayasrah 2019; Damico et al. 2020; Erden Demir et al. 2018; Ribeiro et al. 2017; Robleda et al. 2016). It is thought that the increase in sympathetic activity with pain, separation of the patient from the mechanical ventilator, moving the patient in bed, and stress affect the vital signs of the patients. In our study, as the level of sedation during aspiration-positioning increased, the pain level of the patients decreased, and as the pain level increased, the level of sedation decreased. Payen et al. (2001) reported a negative correlation between the
12 Evaluation of Pain in the Critical Care Unit Patients Who Had Intubated …
213
Behavioral Pain Scale score and the RSS score in a study conducted in intensive care patients under sedation. According to this information, the response to pain decreases as the level of sedation increases. It is similar to the results in our study. If the level of sedation to be applied and monitored during the procedure is not kept at appropriate levels, it is thought that the patient wakes up with the painful stimulus and the level of sedation decreases.
12.8 Conclusion In this study, it was determined that the pain level during aspiration was higher than the pain level during positioning in intubated and sedated patients in intensive care unit. In line with these results, it is recommended that pain behaviors of intubated and sedated patients treated in intensive care should be monitored with valid and reliable scales, treatment and care protocols should be established to reduce pain intensity during aspiration, in-service training should be planned for intensive care nurses to manage pain behaviors of intubated and sedated intensive care patients, and future studies should be conducted with larger case numbers.
References Akta¸s S (2016) Entübe ve sedatize yo˘gun bakım hastalarının a˘grı davranı¸slarının belirlenmesi (Yüksek Lisans Tezi). Cumhuriyet Üniversitesi Sivas Akta¸s YY, Karabulut N (2014) Mekanik ventilasyonlu hastada a˘grı de˘gerlendirmesi. Gümü¸shane Üniversitesi Sa˘glık Bilimleri Dergisi 3(4):1132–1146 Akyol AD (2017) Yo˘gun Bakım Hem¸sireli˘gi, 1st edn. ˙Istanbul Tıp Kitabevleri, ˙Istanbul Al Sutari MM, Abdalrahim MS, Hamdan-Mansour AM, Ayasrah SM (2014) Pain among mechanically ventilated patients in critical care units. J Res Med Sci 19(8):726 Alakan YS, ¸ Edibe Ü, Fizyoterapi HÜSBF (2017) Yo˘gun Bakım Hem¸sireli˘ginde A˘grı De˘gerlendirmesi ve A˘grı Yönetimi. Hacettepe Üniversitesi Sa˘glık Bilimleri Fakültesi Dergisi, 4(2), 12–29, 2017. https://dergipark.org.tr/tr/download/article-file/377042 Arbour C, Gélinas C (2014) Behavioral and physiologic indicators of pain in nonverbal patients with a traumatic brain injury: an integrative review. Pain Manag Nurs 15(2):506–518 Arroyo-Novoa CM, Figueroa-Ramos MI, Puntillo KA, Stanik-Hutt J, Thompson CL, White C, Wild LR (2008) Pain related to tracheal suctioning in awake acutely and critically ill adults: a descriptive study. Intensive Crit Care Nurs 24(1):20–27 Aslan E, Arlı K, Yavuz M, Aytaço˘glu ˙I, Temiz K, Çınar E (2010) Yo˘gun Bakımdaki Sedatize Hastaların A˘grılı Uygulamalara Tepkileri. Anestezi Dergisi, 18(3), 163–167. https://search.trd izin.gov.tr/tr/yayin/detay/110783 Aslan FE, Karada˘g S¸ (2007) A˘gri: Yo˘gun bakım ünitesinde hem¸sireye hastanın yerine dü¸sünme ve hissetme zorunluluk ve sorumlulu˘gu yükleyen bir sorun. Yo˘gun Bakım Hem¸sireli˘gi Dergisi 11(2):89–95 Ayasrah S (2016) Care-related pain in critically ill mechanically ventilated patients. Anaesth Intensiv Care 44(4):458–465 Ayasrah SM (2019) Pain among non-verbal critically Ill mechanically ventilated patients: Prevalence, correlates and predictors. J Crit Care 49:14–20
214
F. Güçlü and S. Ünsar
Çelik S (2016) Yo˘gun bakım hastalarında a˘grı yönetimi. Yo˘gun Bakım Hem¸sireli˘gi Dergisi 20(1):1– 8 Damico V, Macchi G, Murano L, Forastieri Molinari A (2020) Incidence of pain at rest and during nursing procedures in ICU patients: a longitudinal observational study. Ann Ig 32(4):407–418 Damico V, Murano L, Cazzaniga F, Dal Molin A (2018) Pain prevalence, severity, assessment and management in hospitalized adult patients: a result of a multicenter cross-sectional study. Ann Ist Super Sanita 54(3):194–200 Efe AK, Çaydam ÖD (2020) Yo˘gun bakımda mekanik ventilasyon tedavisi alan hastaların invaziv giri¸simlere ba˘glı a˘grı davranı¸slarının de˘gerlendirilmesi. Avrasya Sa˘glık Bilimleri Dergisi 3(1):23–34 Erden S, Demir N, Ugras GA, Arslan U, Arslan S (2018) Vital signs: Valid indicators to assess pain in intensive care unit patients? An observational, descriptive study. Nurs Health Sci 20(4):502–508 Esen H, Onturk K, Badir A, Aslan F (2010a) Entube ve sedatize yogun bakim hastalarinin pozisyon verme ve aspirasyon sirasindaki agri davranislari. Acibadem Universitesi Saglik Bilimleri Dergisi 1(2):89–93 Esen H, Öntürk ZK, Badır A, Aslan Eti F (2010b) Entübe ve sedatize yo˘gun bakım hastalarının pozisyon verme ve aspirasyon sırasındaki a˘grı davranı¸sları. Acıbadem Üniversitesi Sa˘glık Bilimleri Dergisi 1(2):89–93 Gündo˘gan O, Bor, C, Korhan E. A, Demira˘g K, Uyar M (2016) Eri¸skin Yo˘gun Bakım Hastasında A˘grı De˘gerlendirmesi: Critical-Care Pain Observation Tool Ölçe˘gi’nin Türkçe Versiyonunun Geçerlik Güvenirlik Ara¸stırması. Journal of the Turkish Society of Intensive Care/Türk Yogun Bakim Dernegi Dergisi, 14(3), https://cms.galenos.com.tr/Uploads/Article_13594/93-99.pdf Hamilton, D. K (2020) Design for Critical Care: Des. Heal Ito Y, Teruya K, Nakajima E (2022) Evaluation of pain severity in critically ill patients on mechanical ventilation. Intensive Crit Care Nurs 68:103118 Konateke S, Güngörmü¸s Z (2018) Yo˘gun bakımda a˘grı, sedasyon ve konfor yönetiminde hem¸sirenin rolü. Social Sciences Studies Journal 4(20):3041–3045 Korhan EA (2012) Yeti¸skin yo˘gun bakım hastasında a˘grının de˘gerlendirilmesi. Yo˘gun Bakım Hem¸sireli˘gi Dergisi 16(2):57–65 Menekli T, Dogan R, Yaprak B (2021) Pain behaviors and hemodynamic parameters of intubated and sedatized intensive care patients during aspiration. Medicine 10(3):798–803 ´ M., Grizelj-Stojˇci´c, E., Smiljani´c, A., & Skok, I. Nesek Adam V, Matoli´c M, KARAMAN ILIC, (2015) Pain management in critically ill patients. Period Biol 117(2):225–230 Olsen BF, Valeberg BT, Jacobsen M, Småstuen MC, Puntillo K, Rustøen T (2021) Pain in intensive care unit patients—A longitudinal study. Nurs Open 8(1):224–231 Payen J.-F, Bru O, Bosson J.-L, Lagrasta A, Novel, E, Deschaux I, Pierre L, Jacquot C (2001) Assessing pain in critically ill sedated patients by using a behavioral pain scale. Critical care medicine, 29(12), 2258–2263 Puntillo KA, Max A, Chaize M, Chanques G, Azoulay E (2016) Patient Recollection of ICU Procedural Pain and Post ICU Burden: The Memory Study. Crit Care Med 44(11):1988–1995. https://doi.org/10.1097/CCM.0000000000001875 Puntillo K. A, Max A, Timsit J.-F, Vignoud L, Chanques G, Robleda G, Roche-Campo F, Mancebo J, Divatia JV, Soares M (2014) Determinants of procedural pain intensity in the intensive care unit. The Europain® study. Am J Respir CritAl Care Med, 189(1), 39–47 Ribeiro CJN, Bezerra DS, Lima AGCF, Fernandes CCF, Menezes MG, d. V., & Ribeiro, M. d. C. d. O. (2017) Pain during tracheal aspiration in patients with traumatic brain injury undergoing mechanical ventilation. Revista Dor 18:332–337 Rijkenberg S, Stilma W, Bosman RJ, van der Meer NJ, van der Voort PH (2017) Pain measurement in mechanically ventilated patients after cardiac surgery: comparison of the Behavioral Pain Scale (BPS) and the Critical-Care Pain Observation Tool (CPOT). J Cardiothorac Vasc Anesth 31(4):1227–1234
12 Evaluation of Pain in the Critical Care Unit Patients Who Had Intubated …
215
Robleda G, Roche-Campo F, Membrilla-Martínez L, Fernández-Lucio A, Villamor-Vázquez M, Merten A, Baños J (2016) Evaluation of pain during mobilization and endotracheal aspiration in critical patients. Medicina Intensiva (english Edition) 40(2):96–104 Sarıcao˘glu F, Akıncı SB, Dal D, A. Ü. (2005) Yo˘gun bakım hastalarında analjezi ve sedasyon. Hacettepe Tıp Dergisi 36(2):86–90 Selva A, Sanabria A. J, Pequeno S, Zhang Y, Sola I, Pardo-Hernandez H, Selva C, Schünemann H, Alonso-Coello P (2017) Incorporating patients’ views in guideline development: a systematic review of guidance documents. J Clin Epidemiol, 88, 102–112 Terzi B, Kaya N (2017) A planned admission protocol application in intensive care units. Nurs Crit Care 22(6):362–371 Tsuruta R, Fujita M (2018) Comparison of clinical practice guidelines for the management of pain, agitation, and delirium in critically ill adult patients. Acute Medicine & Surgery 5(3):207–212 Tülin K, Çelik S (2019) Yo˘gun bakım hastalarını mekanik ventilasyondan ayırma sürecinde do˘ga temelli ses terapisinin etkisi. Cukurova Medical Journal 44:119–132 Uyar M, Çankaya G, Korhan EA, Khorshıd L (2013) Amerikan yo˘gun bakım hem¸sireler birli˘ginin sedasyon de˘gerlendirme ölçe˘ginin Türkçe çevirisinin güvenirlik çalı¸sması. Florence Nightingale Journal of Nursing 21(1):40–48 Vázquez M, Pardavila MI, Lucia M, Aguado Y, Margall M, Asiain MC (2011) Pain assessment in turning procedures for patients with invasive mechanical ventilation. Nurs Crit Care 16(4):178– 185
Fatma Güçlü was born in Tekirda˘g in 1993. She completed his primary, secondary, and high school education in Tekirda˘g. She graduated from Trakya University (TU), Faculty of Health Sciences, Department of Nursing in 2015. She worked as a nurse at the Private American Hospital between September 2015 and November 2015. She was appointed to Edirne Sultan 1. Murat State Hospital in November 2015. She started her Master’s degree in Internal Medicine Nursing at Trakya University Institute of Health Sciences, Department of Internal Medicine Nursing in September 2016. Currently, in Edirne Sultan 1.Murat State Hospital, she works as a nurse in the Step General Intensive Care Unit. Serap Unsar was born in Edirne in 1973. He completed his primary, secondary, and high school education in Edirne. She graduated from Istanbul University Florence Nightingale School of Nursing in 1993. In 1993, he started to work as a research assistant at Trakya University (TU) Vocational School of Health Services. In the same year, she started her Master’s degree in Internal Medicine Nursing at Istanbul University (IU) Institute of Health Sciences. After completing his Master’s degree in 1996, he started his doctoral studies in the same year and graduated in 2001. He was a Lecturer at the School of Health at T.U. between 1999 and 2002, an Assistant Professor between 2002 and 2010, an Associate Professor in 2010, and a Professor in 2015. He has 11 articles published within the scope of SCI-Expanded, 21 Master’s and 3 doctoral thesis management, 24 national and international article authorship, 43 international/national congress papers, 1 international book chapter authorship, 8 national book chapter authorship, 8 publication incentive and scientific performance awards, 8 professional organization membership, Nursing Department Chair, board member, etc. She is married with two children and is currently working in the Department of Internal Medicine Nursing, Faculty of Health Sciences.
Chapter 13
Corruption in the Health Sector: Case Study of Kosovo Luan Vardari, Berk Arapi, and Qëndresa Kukaj
Abstract Comprehensive development, growth, and prosperity of all social ranks are among the fundamental problems of many countries. The health sector is of great importance for people or societies to lead a healthier, higher quality, and happier life. The health sector is a vital sector for the society, and the resources allocated to this sector and the revenues obtained have a significant share in the national economies. One of the most important problems or uncertainties in the health sector is that this sector is a multi-actor or multi-managed structure. Healthcare sectors of countries are run by both local and central governments. This multi-factor structure also creates a suitable environment for corruption and this sector is more vulnerable to corruption. The study aimed to analyze the general healthcare system of Kosovo. The research has been conducted with the aid of questionnaire consisted of 23 questions that was applied to 160 participants. The participants were generally asked about their personal opinions on the health system, their trust, and their thoughts on corruption in the health system. The results revealed that the majority of the participants did not trust in the health system in Kosovo, and they generally are in opinion that opposition and corruption are happening at a large extent. Keywords Health Sector · Corruption · Bribery · Kosovo
L. Vardari (B) Faculty of Economic, University “UKSHIN HOTI” Prizren, Prizren, Kosovo e-mail: [email protected] B. Arapi Faculty of Medicine, Istanbul University Cerrahpa¸sa, Istanbul, Turkey e-mail: [email protected] Q. Kukaj Faculty of Business and Management, “Universum” College, Lipjan, Kosovo e-mail: [email protected] © The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd. 2023 K. T. Çalıyurt (ed.), Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II, Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application, https://doi.org/10.1007/978-981-99-5502-2_13
217
218
L. Vardari et al.
13.1 Introduction Corruption is one of the most common problems of the past and present, negatively affecting the health sector. This negative impact affects individuals and households, and there is evidence of adverse effects on subsistence levels as health and wellbeing of citizens (Vian 2008). Compared to past, currently national governments, international organizations, and non-governmental organizations are more dedicated to combat corruption (Transparency International 2019). While there is a need for comprehensive reforms to address corruption, there are steps that should be considered, first of all that of political will for sectoral and local reforms (Spector 2005). Therefore, corruption inhibits sectorial competition, reduces investment, and negatively affects economic growth. By reducing tax revenues, it bases the distribution of income, which causes an unequal distribution of income distribution, a decrease in public investment and in health sector (Collier 2002). The structure of the health sector, which is the main subject of the study, and the opinions of the citizens on this subject will be determinant in this study. Corruption is not an unknown issue for Kosovo. Monitoring the corrupted environment and developing anti-corruption policies remain an ongoing battle for the rule of law in the new country. The distant prospect of membership in the European Union gives Kosovo a framework to follow; however, local actors are responsible for combating this phenomenon and creating an optimistic state for development. The health system in Kosovo is regulated by the Law on Health 2004/4 and 04 / L-125 (Law on Health (2012/04-L-125)). The basic principles of healthcare defined by these laws are: equality; all inclusion and not discrimination; quality; honesty and accountability; prioritizing cost-effective healthcare interventions; sustainability and continuity; prevention and early detection of diseases; co-responsibility and solidarity. According to Law 04 / L-125, the financing of healthcare in the Republic of Kosovo in both public and private system is conducted based on the combined financing model, through the budget and the health insurance system, public and private. However, a health insurance fund as part of the public health insurance system has not yet been established as a result of the still not approved specific law for mandatory implementation. Therefore, currently, public healthcare in Kosovo is financed mainly from Kosovo budget, that of municipalities and co-payments from health service users who are not exempt. However, a large percentage of health expenses are covered by the patients themselves in the form of out-of-pocket expenses (Miller et al. 2000). Moreover, widespread corruption in the health system significantly increases the costs of prevention and the remedy of the different diseases by the citizens. This study focuses on corruption in Kosovo’s public institutions. Through the survey, research, analysis, and reliable data, it aims to raise awareness of citizens on corruption and to promote the fight against corruption in public institutions as well as in decision-making processes. The specific objectives of this study are: defining the perceptions and experiences of citizens regarding corruption in public healthcare system in Kosovo, encouraging activism among citizens in promoting the fight
13 Corruption in the Health Sector: Case Study of Kosovo
219
against corruption in the health system, raising the voice of the citizens of Kosovo for a healthier and corruption-free health system, and furthermore, in promoting transparency and accountability of public investments in the public healthcare system of Kosovo.
13.2 Corruption in Kosovo The causes of corruption are transnational and like corruption itself, are universal. Nevertheless, there are some underlying causes that are specific to a particular state or society. Some political scientists attribute high levels of corruption to certain historical and cultural traditions. According to Treisman (1998), a culture of mistrust and private spirit promotes higher rates of corruption than occurring in communities where general trust and civic engagement are strong. Distrust and suspicion increase the demand for corrupt services by private agents. Although Kosovo has a consistent legislative framework that supports public consultation and citizen participation in decision-making processes, its implementation remains weak. This is evident in cases of public hearings organized by municipalities, where the number of participants is very low, and sometimes no one participates (Participatory Budget Planning 2012). The reasons for this are multiple but can be summarized in one main argument: the lack of trust of citizens in the consultation process and in the governance system in general. In Kosovo, about 72% of citizens of all ethnicities are dissatisfied with the economic direction towards which the country is heading, and over 60% of them show political pessimism, which means that they are dissatisfied with the direction of political developments in the country. In addition, “Kosovo’s Public Participation Index this year is 0.16 (compared to 0.13 in June 2011), which shows that public participation in political and civic life in Kosovo has increased slightly, but still remains very low” (UNDP 2012). Another reason behind the high levels of corruption in Kosovo is considered to be the culture of impunity. This is strongly supported by a large imbalance between corruption reporting by citizens and the media, and the level of public institutions’ response to these reports contributes greatly to increased apathy and disregard: an impression that everyone is doing that, which is the “lubricant” that makes the government work and make things happen. In this situation, people are reluctant to report corruption, not only for security reasons but also because it is not beneficial (Heidenheimer and Johnston 2009). The fight against corruption is widely seen by the general public as a result of external pressures, rather than as a process driven by internal demands. Kosovo institutions have embraced the “over-institutionalization” approach, creating structure upon structure in the fight against corruption, which only serves to strengthen the bureaucracy. Such an approach has led to a disorientation of institutional energies and to a game of constant transfer of responsibility established among public institutions. This jeopardizes the undermining of the functional independence of the entire institutional framework, particularly the separation of institutional responsibilities
220
L. Vardari et al.
throughout the policy development cycle, implementation and enforcement, and the assessment of their impact. Law amendments are made hastily, failing to respond to the reality of the situation on the ground (Spector et al., 2003). On the ground, the high level of informal economy and economic parallels results in a low rate of fulfillment of tax obligations, which is a key indicator of how connected citizens feel to government structures. This means that the less citizens feel in their pocket the decisions of the government, the less they are willing to demand accountability from the government. In this context, the fight against the informal economy and the increase in the level of employee registration and taxation directly contribute to the fight against corruption. The dominant role of the executive branch is seen as another important cause of corruption. Parliamentary oversight is weak and the independence of the judiciary is still to be achieved (Spector et al., 2003). Other causes of corruption can be found in the lack of human capacity in the judiciary to investigate and prosecute corruption, the lack of prosecutors and judges specializing in corruption, but also the perceived lack of courage to prosecute senior officials, public for corruption crimes, instantaneous corruption, and lack of witness protection in corruption cases. Moreover, the lack of transparency and accountability in the finances of political parties is also perceived as the main producers of corruption in Kosovo, the whole lack of transparency in their financing only repeats and perpetuates this perception (Distler 2014).
13.3 Corruption in Health Sector Bribery in healthcare enables a partial privatization of the public sector, where patients finance healthcare through informal payments, thus reducing the burden of public finances to finance healthcare. This may be a reason for the tolerance that has been done to this type of corruption these 2 decades. Corruption in healthcare provision is more common, and is considered systemic, in the transition economies of Central and Eastern Europe (European Commission 2013). In Western European countries, bribery in healthcare provision is rarer and limited to specific areas, as well as in isolated cases in pre- and post-operative treatment. According to the WHO, Building Blocks are Health Systems Framework. The most distinct corruption risks are further elaborated in the continuation of this study. These include (UNDP 2014): • • • • •
Informal payments made outside of formal payments for services or supplies. Staff issues, including private practice by public employees. Exceeding the payment limits. Medical products, including procurement corruption and theft. Drugs.
In addition to informal payments, four other important human resource management issues have been raised: the politicization of appointments and the lack of management capacity; inappropriate patient movements in the private sector due to
13 Corruption in the Health Sector: Case Study of Kosovo
221
double practice by physicians; financial conflicts of interest which may affect the prescription; and absences from the workplace (Table 13.1). The politicization in the framework of qualified managers is not very deep in the health sector in Kosovo. Managers point out that reforming institutions is not the same as changing the mentality, and the challenge in the health sector is a lack of personal responsibility: “People need to watch and monitor a lot … they do not feel responsible for reporting on time”, said an interviewee. Managers point out poor communication skills and failure to delegate responsibilities as elements of demotivating new staff. These issues contribute to the poor functioning of control management systems, which minimizes the likelihood of detecting and sanctioning abuses (Gaumer 2007). According to the UNDP report (2014), it reveals that health systems in Kosovo are changing rapidly due to current health reform efforts. This entails both risks and opportunities. Corruption thrives if procedures and expectations are unclear, and there must be a strong communication strategy that promotes reforms to the public. Also, new reforms such as the health insurance fund would create opportunities for new types of corruption, such as fraud with the reimbursement system. However, the new reforms also rely on a commitment to increased funding, access to care and greater accountability for performance by healthcare providers contracted by the Health Insurance Fund. The installation of an internal audit system at the municipal and central level will be of great importance for the success of the reforms.
13.4 Methodology and Findings This study was conducted in seven municipalities of Kosovo. The quantitative research method was applied. The “ordinary stratified sampling” technique was used to determine the sample, where the general population was divided into smaller groups known as strata, based on the common characteristics of the members of these strata: • The first stratification was done based on ethnicity, where three different subgroups were created. • The second strata were done based on settlements. For each municipality, the sample was extended to urban and rural areas according to official KAS statistics. • The third strata were done based on the number of surveys conducted in each settlement (starting point). The starting points in the current research were determined according to the random method. The survey was conducted online from May 2 to July 15, 2020. This survey has a 95% confidence level. 160 Kosovo citizens over the age of 18 participated in the study were: Albanians (138), Turks (12), and Bosnians (2). The sample was afterward weighed to reflect the ethnic structure in Kosovo. The questionnaire was initially tested to identify logical and substantive problems while the interviewers were trained.
222
L. Vardari et al.
Table 13.1 Areas that are vulnerable to corruption in the health sector of Kosovo Health system building block
Activities
Risks of corruption
Kosovo assessment data
Leadership and governance
Policymaking; legislation; regulatory functions
Regulatory coverage; conflict of interest at the highest levels; broad corruption; bribes or influence exercised on drug registration and licensing/ quality control of drugs; Lack of standards or regulatory control of public and private institutions
World Governance Indicators suggest that governance is generally weak in Kosovo. In 2012, Kosovo scored − 0.39 in government effectiveness and −0.62 in controlling corruption from a possible rate of +2.5 to −2.5. The current Minister of Health has been adept at passing most appropriate Health Legislation with the support of national and international stakeholders. Most of the respondents thought that the policies were right, but that the implementation was lame. Politicization in general, including the health and justice system, affects staff selection and good governance. Previously, senior officials (including the former director of the Kosovo Medical Agency, a Secretary General)
Provision of services
Provision of services by frontline health workers; coordination by managers
Informal payments; referring patients to private practices; deficiencies; theft of supplies or equipment
Problem with informal payments, but recent data seem to show lower rates (e.g., 4- 16% depending on source). We did not speak to patients directly about this study. There is great concern with physicians referring patients to their private practices, and who are absent from work during working hours in private clinics. Respondents mentioned the risk of using financial incentives for doctors to refer patients to specific pharmacies or other ancillary services
Human resource
Selection, positioning, training, promotion, and staff discipline
Promotion and grading in employment inappropriate positions in organizations and inconsistent transfer practices (i.e., contrary to professional ethics)
Staff’s decisions are considered to be policy-influenced. No concerns have been raised regarding the corruption, bribery, and misallocation in hiring impunity is a problematic issue; people are not accountable for their performance
(continued)
13 Corruption in the Health Sector: Case Study of Kosovo
223
Table 13.1 (continued) Health system building block
Activities
Risks of corruption
Kosovo assessment data
Medical products and technologies
Selection, procurement, distribution, and use of medical products
Bribes are added to the selection list; financial relations between doctors and private pharmacies; treatment of surplus for financial gain; procurement corruption (secret agreements between bidders, tribute payments, sharing of confidential information in favor of certain bidders)
The supply of medicines is limited. < 50% of their requests can be received. It is not clear whether the drugs were ever purchased (due to budget shortfalls) or directed for sale in the private sector, or both. Former MoH staff has been accused of drug corruption (director of the hospital pharmaceutical service). MoH has recently started with reforms in pharmaceutical procurement (January 2014). Economic operators now distribute secondary and tertiary level drugs directly to their facilities based on hospital requirements and with the approval of the Health Financing Agency. Lack of supplies of medicines may be due to small quantities required by health institutions and insufficient penalties/safeguards in supplying delay contracts. In procurement, there is high staff turnover, insufficient number of staff, and possible lack of capacity for technical supervision (i.e., addressing the needs, specification setting). Irrational exploitation is a problem in itself and there are concerns about financial motivation for prescribing and referrals
Financing
Resource allocation, collection of user fees, insurance, contracting
Derivation of official revenues from tariffs; appropriation of budgeted funds; insurance fraud
Newly enacted laws, such as those related to the health insurance fund and the HUCSK, mean that systems will change. Insurance regulations should take into account fraud control measures. Contracts with providers should require accountability from institutions for control over individual providers requesting informal payments. It is necessary to improve the capacity for cost-effective planning, procurement and monitoring and evaluation in the MoH and the Health Financing Agency
Source UNDP (2014)
224
L. Vardari et al.
13.4.1 Demographic Profile of Respondents The study comprises 160 respondents. 68, or 42.5% were men and 84, or 52.5% were women. Most of the respondents were of 25–34 age, or 42.5%, followed by those 35–44 age who make up 32.5 of the total respondents, while the least represented age groups in the survey are probably those ranging from 18 to 24 years old as well as those over 45 years old. This distribution can be justified by the fact that the questionnaire was distributed electronically and the groups that probably tend to use the most electronic means of communication are of 28–45 age range (Tables 13.2 and 13.3). In terms of ethnicity, the largest number of respondents, more precisely 138, were of Albanian ethnicity, followed by 12 citizens of Turkish ethnicity, and those of Bosnian ethnicity, which in total were 2 in number (Table 13.4). From the total percentage of the respondents, 86.8% were from urban areas, while only 13.2% were in rural areas. More specifically, 38.2% from Prishtina, 39.5% from Prizren, 7.9% from Gjakova, and the rest of the respondents were from Mitrovica, Peja, Gjilan, and Ferizaj (Tables 13.5 and 13.6). Table 13.2 Gender percent Frequency Valid
Missing
Percent
Valid percent
Cumulative percent
Female
84
52.5
55.3
Male
68
42.5
44.7
Total
152
95.0
100.0
100.0
8
5.0
160
100.0
Frequency
Percent
Valid percent
Cumulative percent
System
Total
55.3
Table 13.3 Age percent Valid
18–24
28
17.5
18.4
18.4
25–34
68
42.5
44.7
63.2
35–44
52
32.5
34.2
97.4
45–54
4
2.5
2.6
152
95.0
100.0
Total Missing Total
System
8
5.0
160
100.0
100.0
13 Corruption in the Health Sector: Case Study of Kosovo
225
Table 13.4 Ethnicity Frequency Valid
Albanian Bosnian
Missing
138
Percent 86.3
Valid percent
Cumulative percent
90.8
90.8 92.1
2
1.3
1.3
Turks
12
7.5
7.9
Total
152
95.0
100.0
100.0
Valid percent
Cumulative percent
System
Total
8
5.0
160
100.0
Table 13.5 Residence Frequency Valid
Missing
Urban
132
Percent 82.5
86.8
Rural
20
12.5
13.2
Total
152
95.0
100.0
8
5.0
160
100.0
System
Total
86.8 100.0
Table 13.6 Region Frequency Valid
36.3
38.2
Prizren
Cumulative percent 38.2
60
37.5
39.5
77.6
Mitrovica
2
1.3
1.3
78.9
Gilan
6
3.8
3.9
82.9
8
5.0
5.3
88.2
Gjakova
12
7.5
7.9
96.1
Ferizaj
6
3.8
3.9
152
95.0
100.0
8
5.0
160
100.0
Total Total
Valid percent
58
Peja
Missing
Percent
Pristina
System
100.0
13.4.2 Health Services Questions The most visited institutions by the citizens during the period of 2000–2020 year resulted to be the Family Medicine Centers, visited by 61.8% of citizens, followed by hospitals with 19.7%, University Clinical Center of Kosovo with 14.5%, and other institutions with 3.9%. This can be explained by the fact that MFMCs are the first address for patients, and then with the instructions of MFMCs visit other institutions (Table 13.7).
226
L. Vardari et al.
Table 13.7 Which of the healthcare institutions have you most frequently visited during the years 2000–2020? Frequency Valid
Valid percent
Cumulative percent
Family Medicine Center
94
58.8
61.8
61.8
Hospital
30
18.8
19.7
81.6
University Clinical Center of Kosovo
22
13.8
14.5
96.1
Others Total Missing
Percent
System
Total
6
3.8
3.9
152
95.0
100.0
8
5.0
160
100.0
100.0
Table 13.8 What is the level of satisfaction of the health services for the following institutions? (University Clinical Center of Kosovo (UCCK)) Frequency Valid
Cumulative percent
Strongly disagree
12
7.5
7.9
7.9
42
26.3
27.6
35.5
Neutral
50
31.3
32.9
68.4
Agree
44
27.5
28.9
97.4
4
2.5
2.6
152
95.0
100.0
Total Missing
Valid percent
Disagree
Strongly agree
Total
Percent
System
8
5.0
160
100.0
100.0
Regarding the respondents’ answers on the level of satisfaction with the services provided by various health institutions, the highest percentage of dissatisfaction was given to University Clinical Center of Kosovo. Thus, for UCCK, 35.5% of respondents said they are dissatisfied or not at all satisfied. Similarly, 35.5% of the citizens were dissatisfied with the work of the regional hospitals. While citizens seem to be mostly satisfied with the services of Family Medicine Centers in their communities, since only 26.3% of them have expressed a measure of dissatisfaction (Tables 13.8, 13.9, and 13.10).
13.4.3 Perceived Level of Corruption in Health Sector This level of dissatisfaction is in direct proportion to the citizens’ perception of the level of corruption in the above-mentioned institutions. 65.8% of surveyed citizens think that corruption in UCCK is high or very high. As for the regional hospitals,
13 Corruption in the Health Sector: Case Study of Kosovo
227
Table 13.9 What is the level of satisfaction of the health services for the following institutions? (Regional hospitals) Frequency Valid
Missing
Percent
Valid percent
Cumulative percent
Strongly disagree
16
10.0
10.5
10.5
Disagree
36
22.5
23.7
34.2
Neutral
64
40.0
42.1
76.3
Agree
36
22.5
23.7
Total
152
95.0
100.0
8
5.0
160
100.0
System
Total
100.0
Table 13.10 What is the level of satisfaction of the health services for the following institutions? (Family Medicine Center) Frequency Valid
Strongly disagree
Valid percent
Cumulative percent
6
3.8
3.9
3.9
Disagree
34
21.3
22.4
26.3
Neutral
34
21.3
22.4
48.7
Agree
70
43.8
46.1
94.7
8
5.0
5.3
152
95.0
100.0
Strongly agree Total Missing
Percent
System
Total
8
5.0
160
100.0
100.0
this is the opinion of 53.9% of the citizens. Despite these, for MFMCs, only a small part of the citizens, or 19.7%, think that the level of corruption is high or very high (Tables 13.11, 13.12, and 13.13). Table 13.11 What is the perception on the level of corruption in public healthcare institutions? (University Clinical Center of Kosovo) Frequency Valid
Cumulative percent
Very high
30
18.8
19.7
19.7
70
43.8
46.1
65.8
Average
36
22.5
23.7
89.5
Low
14
8.8
9.2
98.7
2
1.3
1.3
152
95.0
100.0
8
5.0
160
100.0
Total Total
Valid percent
High
Very Low Missing
Percent
System
100.0
228
L. Vardari et al.
Table 13.12 What is the perception on the level of corruption in public healthcare institutions? (Regional hospitals) Frequency Valid
Valid percent
Cumulative percent
Very high
26
16.3
17.1
17.1
High
56
35.0
36.8
53.9
Average
48
30.0
31.6
85.5
Low
20
12.5
13.2
98.7
2
1.3
1.3
152
95.0
100.0
Very Low Total Missing
Percent
System
Total
8
5.0
160
100.0
100.0
Table 13.13 What is the perception on the level of corruption in public healthcare institutions? (Family Medicine Centers) Frequency Valid
Very high High
Total
Valid percent
Cumulative percent
6
3.8
3.9
3.9
24
15.0
15.8
19.7
Average
54
33.8
35.5
55.3
Low
46
28.8
30.3
85.5
Very Low
22
13.8
14.5
152
95.0
100.0
8
5.0
160
100.0
Total Missing
Percent
System
100.0
When asked about the differences in the level of corruption in health institutions in the last two years, 21.1% of citizens stated that they think that the level of corruption has increased, 44.7% claim that it has remained same, only 11.8% think that the level of corruption has decreased, and 22.4% stated that they do not know or do not have an opinion (Table 13.14). As per to the reduction of the level of corruption in the health system, one-third of respondents have not had information on the issue or have refused to answer. Meanwhile, 42% think that some measures have been implemented, but the results were low, 15.8% think that some measures have been implemented and some results have been achieved and 7.9% think that no measures have been implemented so there have not been any results (Table 13.15).
13 Corruption in the Health Sector: Case Study of Kosovo
229
Table 13.14 What are the perceptions on the change in the level of corruption in the public health system in last two years? Frequency Percent Valid percent Cumulative percent Valid
It has grown
32
20.0
21.1
21.1
It has remained the same
68
42.5
44.7
65.8
It has decreased
18
11.3
11.8
77.6
I do not know Total Missing System Total
34
21.3
22.4
152
95.0
100.0
8
5.0
160
100.0
100.0
Table 13.15 What are your perceptions on the implementation of effective anti-corruption policies or measures in health system by local public authorities? Frequency Valid
Cumulative percent
64
40.0
42.1
42.1
Yes, some measures have been implemented and some results have been achieved
24
15.0
15.8
57.9
No measures have been implemented so there have been no results
12
7.5
7.9
65.8
Total Total
Valid percent
Yes, some measures have been implemented but the results have been small
I do not know/I refuse Missing
Percent
System
52
32.5
34.2
152
95.0
100.0
8
5.0
160
100.0
100.0
13.4.4 Reported Level of Corruption The study highlights a disturbing fact regarding the provision of health services in public institutions, which shows that 6.6% of citizens have always been unable to receive health services from public institutions and are forced to seek these services in private institutions. 56.6% of citizens stated that the same thing happened to them often, whereas only 11.8% stated that they never faced this kind of situation before (Table 13.16). To further explore the issue of providing healthcare services in public institutions, citizens were asked about the behavior of doctors, nurses, and technical staff of public health institutions while providing services. The responses revealed that 80.5% of citizens agreed that doctors refer patients to the private clinics and hospitals where
230
L. Vardari et al.
Table 13.16 How often did you encounter the situation when you were supposed to go to private health institution due to the lack of services in public institutions? Frequency Valid
Missing
Percent
Valid percent
Cumulative percent
Always
10
6.3
6.6
6.6
Often
86
53.8
56.6
63.2
Rarely
38
23.8
25.0
88.2
Never
18
11.3
11.8
Total
152
95.0
100.0
8
5.0
160
100.0
System
Total
100.0
they also work. As working hours regard, 60.5% of respondents think that doctors do not respect their schedule, while 26.3% of them are neutral on this issue. A similar percentage, 58.8% are in the opinion that doctors in public health institutions refer patients to certain pharmacies for drug purchase (Tables 13.17, 13.18, and 13.19). When the issue of misuse of funds of public institutions by doctors and staff of these institutions was raised, it was noticed that citizens were reluctant in their answers. Thus, when asked if they agree with the statement that doctors misuse the medical equipment of public health institutions for personal purposes, 44.7% stated that they are neutral, and only 36.8% stated that they agree or fully agree. The answer was similar when the respondents were asked if they think that doctors misuse essential list drugs from public institutions for personal benefits (Tables 13.20 and 13.21). The results of the survey reveal that the citizens of Kosovo think that doctors in the public health system are offered informal payments in order to receive better health services. Thus, 61.9% of citizens express a level of compliance with the statement that doctors are offered informal payments in order to receive better services. 30.35 Table 13.17 Do you agree or disagree with the following statement about the public health system in Kosovo (1–5)? (Doctors refer patients to their private surgeries or the private hospitals/clinics where they are employed) Frequency Valid
Total
Valid percent
Cumulative percent
Strongly disagree
2
1.3
1.3
1.3
Disagree
8
5.0
5.3
6.6
Neutral
18
11.3
11.8
18.4
Agree
80
50.0
52.6
71.1
Strongly agree
44
27.5
28.9
152
95.0
100.0
8
5.0
160
100.0
Total Missing
Percent
System
100.0
13 Corruption in the Health Sector: Case Study of Kosovo
231
Table 13.18 Do you agree or disagree with the following statement about the public health system in Kosovo (1–5)? (Doctors in public healthcare institutions do not respect working hours) Frequency Valid
Strongly disagree
Valid percent
Cumulative percent
2
1.3
1.3
1.3
Disagree
16
10.0
10.5
11.8
Neutral
42
26.3
27.6
39.5 64.5
Agree
38
23.8
25.0
Strongly agree
54
33.8
35.5
152
95.0
100.0
Total Missing
Percent
System
Total
8
5.0
160
100.0
100.0
Table 13.19 Do you agree or disagree with the following statement about the public health system in Kosovo (1–5)? (Doctors refer patients to certain pharmacies for drugs purchase) Frequency Valid
Valid percent
Cumulative percent
Strongly disagree
6
3.8
3.9
3.9
Disagree
8
5.0
5.3
9.2
Neutral
44
27.5
28.9
38.2
Agree
50
31.3
32.9
71.1
Strongly agree
44
27.5
28.9
152
95.0
100.0
8
5.0
160
100.0
Total Missing
Percent
System
Total
100.0
Table 13.20 Do you agree or disagree with the following statement about the public health system in Kosovo (1–5)? (Doctors misuse the medical equipment of public health institutions for personal benefits) Frequency Valid
Strongly disagree Disagree
Total
Valid percent
Cumulative percent
4
2.5
2.6
2.6
24
15.0
15.8
18.4
Neutral
68
42.5
44.7
63.2
Agree
40
25.0
26.3
89.5
Strongly agree
16
10.0
10.5
152
95.0
100.0
8
5.0
160
100.0
Total Missing
Percent
System
100.0
232
L. Vardari et al.
Table 13.21 Do you agree or disagree with the following statement about the public health system in Kosovo (1–5)? (Doctors misuse drugs found in the essential drug list (free drugs) for personal benefits) Frequency Valid
Strongly disagree Disagree
Valid percent
Cumulative percent
3.8
3.9
3.9
22
13.8
14.5
18.4
Neutral
62
38.8
40.8
59.2
Agree
36
22.5
23.7
82.9
Strongly agree Total Missing
Percent
6
System
Total
26
16.3
17.1
152
95.0
100.0
8
5.0
160
100.0
100.0
stated that they are neutral and only 9.2% stated that they do not agree with this statement (Table 13.22). A larger percentage of respondents, respectively 65.8% (40.8% agree and 25.0% strongly agree), agree with the statement that doctors are offered informal material goods and non-monetary gifts in order to receive better services from them (Table 13.23). Citizens are in the opinion that nurses are less corrupted than doctors. 59.2% (32.9% agree and 23.3% strongly agree) of respondents agreed with the statement that nurses are offered informal payments in order to benefit from better health services in public health institutions. While the perceived level of corruption is even lower for technical staff, where 44.7% of citizens think that they are offered informal payments (Tables 13.24, 13.25, 13.26, and 13.27). As the Table 13.28 shows, the majority of citizens, or 51.3% (26.3% agree and 26.0% strongly agree), are against nepotism in public health institutions, stating that personal or family ties should not be used in order to receive better health Table 13.22 Do you agree or disagree with the following statement about the public health system in Kosovo? (Doctors are offered informal payments in order to (in exchange to) receive better health services) Frequency Valid
Strongly disagree Disagree
Total
Valid percent
Cumulative percent
2
1.3
1.3
1.3
10
6.3
6.6
7.9
Neutral
46
28.8
30.3
38.2
Agree
48
30.0
31.6
69.7
Strongly Agree
46
28.8
30.3
152
95.0
100.0
8
5.0
160
100.0
Total Missing
Percent
System
100.0
13 Corruption in the Health Sector: Case Study of Kosovo
233
Table 13.23 Do you agree or disagree with the following statement about the public health system in Kosovo? (Doctors are offered material goods (non-monetary/gifts) in order to receive better health services) Frequency Valid
Strongly disagree Disagree
Valid percent
Cumulative percent
1.3
1.3
1.3
14
8.8
9.2
10.5
Neutral
36
22.5
23.7
34.2
Agree
62
38.8
40.8
75.0 100.0
Strongly agree Total Missing
Percent
2
System
Total
38
23.8
25.0
152
95.0
100.0
8
5.0
160
100.0
Table 13.24 Do you agree or disagree with the following statement about the public health system in Kosovo? (Nurses are offered informal payments in order to receive better health services) Frequency Valid
Strongly disagree
Valid percent
Cumulative percent
2
1.3
1.3
1.3
Disagree
24
15.0
15.8
17.1
Neutral
36
22.5
23.7
40.8
Agree
50
31.3
32.9
73.7
Strongly agree
40
25.0
26.3
100.0
152
95.0
100.0
Total Missing
Percent
System
Total
8
5.0
160
100.0
Table 13.25 Do you agree or disagree with the following statement about the public health system in Kosovo? (Technical staff (laboratory technicians, radiologists, etc.) are offered informal payments in order to receive better health services) Frequency Valid
Strongly disagree
1.3
Valid percent 1.3
Cumulative Percent 1.3
Disagree
26
16.3
17.1
18.4
56
35.0
36.8
55.3
Agree
44
27.5
28.9
84.2 100.0
Strongly Agree
Total
Percent
Neutral
Total Missing
2
System
24
15.0
15.8
152
95.0
100.0
8
5.0
160
100.0
234
L. Vardari et al.
Table 13.26 Do you agree or disagree with the following statement about the public health system in Kosovo? (Technical staff (laboratory technicians, radiologists, etc.) are offered material (nonmonetary) goods in order to receive better health services) Frequency Valid
Strongly disagree Disagree
Valid percent
Cumulative percent
1.3
1.3
1.3
22
13.8
14.5
15.8
Neutral
60
37.5
39.5
55.3
Agree
46
28.8
30.3
85.5
Strongly agree Total Missing
Percent
2
System
Total
22
13.8
14.5
152
95.0
100.0
8
5.0
160
100.0
100.0
Table 13.27 Do you agree or disagree with the following statement about the public health system in Kosovo? (Nurses are offered material (non-monetary) goods in order to receive better health services) Frequency Valid
Strongly disagree Disagree
Valid percent
Cumulative percent
4
2.5
2.6
2.6
20
12.5
13.2
15.8
Neutral
46
28.8
30.3
46.1
Agree
42
26.3
27.6
73.7
Strongly agree
40
25.0
26.3
152
95.0
100.0
8
5.0
160
100.0
Total Missing
Percent
System
Total
100.0
services. Notwithstanding, it is worrying that a large percentage of citizens or 43.4% of respondents have stated that they think it is okay to use these informal connections. Table 13.28 Do you think personally, or family connections should be used to receive better health services? Frequency Valid
Cumulative percent
41.3
43.4
43.4
No
78
48.8
51.3
94.7
8
5.0
5.3
152
95.0
100.0
Total Missing
Valid percent
66
I refuse to answer
Total
Percent
Yes
System
8
5.0
160
100.0
100.0
13 Corruption in the Health Sector: Case Study of Kosovo
235
Another worrying fact is that when asked whether they themselves have provided monetary or non-monetary goods in order to receive better health services in the last 12 months, 60.8% of respondents answered with yes, which means that 32.9% of citizens have given money and 28.9% have given non-monetary material goods. This represents a high level of self-reported corruption among the citizens of Kosovo (Table 13.29). Moreover, 14.5% of citizens stated that they gave money or material goods because they were enforced and 15.8% said that they gave them voluntarily (Table 13.30). Considering the type of health services for which more monetary and material goods were provided, the survey results showed a relatively equal distribution. Respondents claim that physical therapy medical services, pharmaceutical services, and medical care services for chronic diseases have stated that they have provided monetary and material goods by 7.2%. While the highest level of bribery turns out to be given for emergency medical care services, 21% of surveyed citizens stated that they gave a bribe (Table 13.31). Despite the high reported level of corruption in this survey, only 3.9% of respondents stated that they reported corruption in health institutions before official authorities. This implies that the citizens themselves may be maintaining such a high level of corruption in health institutions (Table 13.32). Table 13.29 Have you donated money or other non-monetary goods to receive better health services in the last 12 months? Frequency Percent Valid percent Cumulative percent Valid
Yes, I gave money
50
31.3
32.9
32.9
Yes, I have given material (non-monetary) goods
44
27.5
28.9
61.8
No, he did not give any money or material goods
58
36.3
38.2
152
95.0
100.0
8
5.0
160
100.0
Total Missing System Total
100.0
Table 13.30 What were the reasons for giving money or material goods? Frequency Valid
Missing Total
Percent
Valid percent
Cumulative percent
I was enforced
22
13.8
14.5
14.5
I gave voluntarily
24
15.0
15.8
30.3
I did not give
106
66.3
69.7
Total
152
95.0
100.0
System
8
5.0
160
100.0
100.0
236
L. Vardari et al.
Table 13.31 Which of the medical services did you most often give money or material goods in public healthcare institutions? Frequency Valid
Valid percent
Cumulative percent
Medical services of physical therapies
11
6.9
7.2
7.2
Pharmaceutical services
11
6.9
7.2
14.5
Emergency medical care services
32
20.0
21.1
35.5
Medical care services for chronic diseases
11
6.9
7.2
42.8
I have not given money or material goods
87
54.4
57.2
152
95.0
100.0
Total Missing
Percent
System
Total
8
5.0
160
100.0
100.0
Table 13.32 Have you filed (experienced) cases of corruption before official authorities/ institutions? Frequency Valid
Missing Total
Percent
Valid percent
Yes
6
3.8
3.9
No
146
91.3
96.1
Total
152
95.0
100.0
8
5.0
160
100.0
System
Cumulative percent 3.9 100.0
13.5 Results and Recommendations Through this study, we aimed to analyze public opinion about perceptions and experiences in relation to corruption in the public healthcare system in Kosovo. The survey was conducted during the period May–July, which was attended by 160 citizens of Kosovo over 18 years who have visited at least once one of the public health institutions in Kosovo. Through the data from this study, we aim to reveal the experiences of citizens in this very important sector of welfare and at the same time increase the level of awareness of corruption. In line with the results of past research, this research has found that citizens perceive the level of corruption in health institutions in Kosovo as very high. The research draws five important conclusions:
13 Corruption in the Health Sector: Case Study of Kosovo
237
• Citizens are largely dissatisfied with the health services provided in all public health institutions, including the University Clinical Center of Kosovo, Regional Hospitals, and Family Medicine Centers. • Citizens perceive the level of corruption in all public health institutions as very high. According to them, the most corrupt institution is the University Clinical Center of Kosovo, followed by the Regional Hospitals and lastly the Family Medicine Centers. • A large percentage of citizens, or 44.7%, think that the level of corruption in the last two years has remained the same, while another 21.1% think that it has only increased. • There is a belief among citizens that in public institutions they are often denied health services in order to seek private providers of these services. In this regard, they also think that doctors and other support staff in public health institutions tend to abuse their authority and the resources of these institutions for personal benefit. • In support of their perceptions about the high level of corruption in public health institutions, 61.8% of surveyed citizens indicate that they themselves have given money or material goods in order to receive better health services in public institutions, either voluntarily or because they have been conditioned to do so. Meanwhile, only a small percentage of them, 3.9%, indicate that they have reported cases of corruption to the relevant authorities. This is a disturbing fact and raises doubts that the citizens themselves are the ones who maintain such a high level of corruption in public health institutions.
References Collier MW (2002) Explaining corruption: An institutional choice approach. Crime Law Soc Chang 38(1):1–32 Democratic Effective Municipality Initiative Report (2012) Participatory budget planning. https:// www.yumpu.com/en/document/view/53066143/participatory-budget-planning Distler W (2014) Kosovo: Konflikt und Intervention. In: Intervention als soziale Praxis. Springer VS, Wiesbaden. https://doi.org/10.1007/978-3-658-06846-2_5 European Commission (2013) Study on corruption in the healthcare sector. Publications Office of the European Union, Luxembourg. https://doi.org/10.2837/58154 Gaumer G (2007) Kosovo report on management accountability in the health sector. World Bank, Washington, DC Heidenheimer AJ, Johnston M (2009) Corruption: Concepts and contexts. Transaction publishers. New Jersey, pp 6–14 Law on Health (2012/04-L-125) Constitution of Kosovo. http://www.kuvendikosoves.org/common/ docs/ligjet/Ligji%20per%20shendetesi.pdf Miller W, Grødeland A, Koshechkina T (2000) If you pay, we’ll operate immediately. J Med Ethics 26:301–311 Spector BI (2005) Fighting corruption in developing countries: strategies and analysis. Kumarian Press, Bloomfield. CT, pp 1–9
238
L. Vardari et al.
Spector IB, Winbourne S, Beck LD (2003) Corruption in Kosovo: observations and implications for USAID. United States Agency for International Development. Available at: https://www. hsdl.org/?view&did=446299 Transparency International (2019) Global corruption perception index: Special focus on corruption and health. Pluto Press, London. https://images.transparencycdn.org/images/2019_CPI_ Report_EN_200331_141425.pdf Treisman D (1998) The causes of corruption: a cross-national study. University of California, p 4 UNDP (2012) Public pulse report III. Public Opinion Polling. Prishtina. UNDP and USAID, p 9. https://www.undp.org/content/dam/kosovo/docs/PublicPulse/PP3/Public_Pulse_3_eng_web. pdf UNDP (2014) Corruption risk assessment in the Kosovo health sector. United Nations Development Program. Pristina. https://www.undp.org/content/dam/kosovo/docs/SAEK/UNDP%20S AEK%20Corruption%20Risk%20Assessment%20in%20Health%20December%202014% 20-%20Alb.pdf Vian T (2008) Review of corruption in the health sector: theory, methods and interventions. Health Policy Plan 23:83–94. https://doi.org/10.1093/heapol/czm048
Luan Vardari is Assistant Professor of Finance in the Faculty of Economics at University “UKSHIN HOTI” Prizren. He received his Master’s degree (MA) in Finance (Balkan Countries Stock Markets) in 2012 from Trakya University and finished his Ph.D. in Business Administration at Trakya University in 2019. He teaches finance courses at graduate and undergraduate levels. His research interests include financial markets and institutions, portfolio optimizations, and international finance. He is the founder and editor-in-chief of PRIZREN SOCIAL SCIENCE JOURNAL. He is editor in book chapters and articles in national and international journals. Berk Arapi is a highly accomplished cardiovascular surgeon and researcher based in Istanbul, Turkey. With a specialization in Cardiovascular Surgery from Istanbul University Cerrahpa¸sa Faculty of Medicine, he has made significant contributions to the field. His expertise is backed by his extensive academic background, including a medical degree from Selçuk University Meram Faculty of Medicine. His passion for advancing medical knowledge is evident through his research and numerous publications. With a commitment to excellence in patient care, he continues to make a significant impact as an Assistant Professor at Istanbul University Cerrahpa¸sa Faculty of Medicine. Qëndresa Kukaj is a Lecturer in the Economics Faculty at AAB College in Kosovo. She received a Master of Arts in Economics degree from Vanderbilt University, TN, USA (2017), and a Master of Arts Degree in Business Administration from University “Haxhi Zeka” in Peja (2016). She is currently continuing her Ph.D. studies in Economics at Hungarian University of Agriculture and Life Sciences (MATE) as a Stipendium Hungaricum Scholarship holder. She is experienced in project development and management in the field of higher education. Her research focuses on higher education and labor markets.
Index
A Advanced economies, 116, 119–126
B Biohazardous waste, 87 Biomedical waste, 73, 87 Budgetary response, 116, 117, 125 Budget transparency, 116, 117, 119, 125
C Characteristics of services, 18, 19, 21, 32 Chemical waste, 92 Community mechanism, 199 Coronavirus pandemic, 145 Corruption, 4, 9, 10, 180–182, 218–222, 226–229, 232, 235–237 COVID-19, 8–10, 22, 23, 26, 37–43, 46, 49, 59, 60, 101, 103, 104, 110, 111, 116–120, 122–125, 144, 145, 147, 152–154, 156–158, 160–162, 164, 165, 170, 171, 174, 195 COVID-19 mobile apps, 145, 146, 150, 163, 168, 174–176 COVID-19 tracing apps, 144–146 Cytotoxic waste, 88
D Data sharing, 116 Digital health, 144 Disinfection, 92 Disposal, 73, 84–89, 92–94, 96, 105 Distribution channels, 9, 25
E Economic globalization, 193 eHealth, 147 Emerging markets, 116, 119–126 Epidemiological studies, 192
F Financial measures, 50, 116, 125, 126 Fiscal budgets, 116 Fiscal policy, 118 Fiscal response, 116, 119, 120
G Generational curse breaker, 192 Genotoxic waste, 88 Global health policy, 192 Great Escape, 192 Greece, 180, 182–185 Grey relational analysis, 145, 147, 150, 163, 174, 176 Grey systems theory, 146, 147, 150, 174, 176
H Hazardous waste, 87, 88 Health and well-being, 195, 197, 218 Healthcare system, 9, 57, 80, 111, 180, 182, 183, 192, 194, 198, 218, 236 Health infrastructure, 192 Health services, 8, 11, 19–29, 32, 33, 90, 181, 183, 184, 197, 225–227, 229, 230, 232–235, 237
© The Editor(s) (if applicable) and The Author(s), under exclusive license to Springer Nature Singapore Pte Ltd. 2023 K. T. Çalıyurt (ed.), Integrity, Transparency and Corruption in Healthcare & Research on Health, Volume II, Accounting, Finance, Sustainability, Governance & Fraud: Theory and Application, https://doi.org/10.1007/978-981-99-5502-2
239
240 Health services marketing, 21–31 Health staff, 18, 20, 32, 182, 183 Health system, 10, 60, 120, 123, 124, 180, 182, 183, 185, 218, 219, 221–223, 228–234 Hierarchy in health services, 22 Human Development Index (HDI), 194 Human tissues, 130 I Incineration, 85, 86 Infectious disease, 18, 89 Infectious waste, 87, 88 Informal health payments, 180 Integrity, 11, 184, 192–194 Internal audit, 10, 221 L Laboratory waste, 87 Life-Evaluation Index (LEI), 198 Low income countries, 120–123, 126 M Marketing, 20, 21, 24, 29, 32, 85 Marketing mix of services, 18, 21, 23, 27, 32 Medical operations research, 184 Medical sharps, 88, 90, 92, 144 Medical waste, 73, 84, 87–97 Mobile apps, 144–147, 150, 169, 174–176 Multi-criteria decision-making, 149 Multiple service users, 194 N National COVID-19 apps, 144, 146, 150, 152, 175 P Pandemic, 9–11, 18, 20–22, 25, 26, 32, 33, 38–43, 46–52, 60, 103, 111, 116–120, 123–126, 144, 145, 180, 185, 195
Index Pareto Improvement, 196, 197 Pathological waste, 88, 90, 93, 98 People, 6, 8, 20, 21, 23, 24, 27, 32, 33, 39, 61, 62, 76, 80, 84, 88, 103, 130, 144–146, 151, 174, 176, 180, 184, 185, 191–198, 219, 222 Personal protective equipment (PPE), 103 Person-centered care/system, 194 Pharmaceutical waste, 88 Physical evidence, 19, 26, 27, 32, 33 Pricing, 23 Promotion, 24, 199, 222
R Recycling, 86, 88 Regional health service, 197 Reverse logistics, 84–86, 89
S Sanctions, 89, 93, 221 SARS-COV-2, 39, 180, 185 Segregation, 74, 195 Service process, 28, 30, 84 Service quality perception, 18, 29, 30 Services, 6–8, 10, 17–21, 25–30, 32, 33, 51, 57, 60, 63, 71–74, 76, 84, 87, 89, 180–183, 194, 197, 198, 219, 220, 226, 229, 230, 232, 237 Shadow economy, 181 Skill upgradation, 198 Sterilization, 94, 98 Storage, 86, 87, 90, 91, 93, 94 Sustainability, 23, 30, 84, 86, 92, 182, 185, 191, 218
T Tele medicine, 10, 57 Transport, 11, 46, 72, 84, 86, 89–91, 93, 94, 97, 98, 101
W Waste reduction, 86