Ultrasound Teaching Manual: The Basics of Performing and Interpreting Ultrasound Scans [4 ed.] 3132437603, 9783132437609
Step by Step to Proficiency in Diagnostic Ultrasound This workbook is divided into lessons that guide you—like an instr
145 51 16MB
English Pages 176 [173] Year 2021
Ultrasound Teaching Manual: The Basics of Performing and Interpreting Ultrasound Scans
The Most Important Planes in Abdominal Ultrasound
Standard Planes with Appropriate Transducer Position and Drawing Templates
Title Page
Copyright
MedOne Access Information
Contents
Introduction
Physical Principles and Technical Fundamentals
New Techniques
Artifacts
Artifacts / Quiz
Practical Tips and Tricks for the Beginner
Lesson 1 Retroperitoneum, Sagittal Plane
Retroperitoneum, Sagittal Plane
Upper Retroperitoneum
Lower Retroperitoneum
Retroperitoneum
Quiz
Lesson 2 Retroperitoneum, Transverse Plane
Retroperitoneum, Transverse Plane
Quiz
Lesson 3 Porta Hepatis, Gallbladder, Biliary Tract
Porta Hepatis and Gallbladder
Porta Hepatis
Gallbladder
Biliary Tract
Lesson 4 Liver
Liver
Quiz
Lesson 5 Kidneys, Adrenal Glands, Renal Transplants, Spleen
Kidney
Renal and Adrenal Tumors
Renal Transplants
Spleen
Quiz
Lesson 6 Thyroid Gland, Lymph Nodes, Gastrointestinal Tract
Thyroid Gland
Thyroid Gland: Pathologic Examples
Lymph Nodes
Gastrointestinal Tract
Gastrointestinal Tract: Colon
Gastrointestinal Tract
Quiz
Lesson 7 Bladder and Reproductive Organs
Bladder:
Bladder and Reproductive Organs
Bladder: Normal Findings
Bladder
Male Reproductive Organs
Female Reproductive Organs
Quiz
Lesson 8 FAST, eFAST, Lung
FAST
eFAST
Lung
Pleura
Ribs and Lung
Lung
Quiz
Lesson 9 Pediatrics
Skull and Central Nervous System
Central Nervous System: Normal Variants
Pediatrics: Skull and Central Nervous System
Pediatrics: Hip
Pediatrics: Kidneys
Pediatrics
Pediatrics: Gastrointestinal Tract
Appendices
Primer of Ultrasound Findings
Index
Template for Report of Normal Findings
Diagram Templates for Standard Planes
Answers to Quizzes
Thanks to Contributors / Hands-on Ultrasound Courses
List of Abbreviations
Examination Algorithms
OBB-QuEexrasmchinnaitttieo:n P Aalngkorreitahtimtis
References
Legend of Numbered Structures
Table of Normal Values for Adults
Recommend Papers
![BASICS OF MUSCULOSKELETAL ULTRASOUND. [2 ed.]
9783030739058, 3030739058](https://ebin.pub/img/200x200/basics-of-musculoskeletal-ultrasound-2nbsped-9783030739058-3030739058.jpg)




![Vascular Ultrasound: B-Mode, Color Doppler and Duplex Ultrasound, Contrast-Enhanced Ultrasound [Team-IRA] (True PDF) [1 ed.]
3132405434, 9783132405431](https://ebin.pub/img/200x200/vascular-ultrasound-b-mode-color-doppler-and-duplex-ultrasound-contrast-enhanced-ultrasound-team-ira-true-pdf-1nbsped-3132405434-9783132405431.jpg)



![Ultrasound Teaching Manual: The Basics of Performing and Interpreting Ultrasound Scans [4 ed.]
3132437603, 9783132437609](https://ebin.pub/img/200x200/ultrasound-teaching-manual-the-basics-of-performing-and-interpreting-ultrasound-scans-4nbsped-3132437603-9783132437609.jpg)
- Author / Uploaded
- Matthias Hofer
File loading please wait...
Citation preview
Sono Grundkurs Ultrasound Teaching Manual Ein Arbeitsbuch für den Einstieg
The Basics of Performing and Interpreting Ultrasound Scans
Matthias Hofer Matthias Hofer
Online-Version in via medici
Fourth Edition
Mit GIT-Bildmaterial von Alexiscontributions Müller-Marbach With by Alexis Müller-Marbach and Jasmin D. Busch 4 in 1: SK-Haltung, Sonobild + Anatomieskizze
10. Auflage
4 in 1: • Transducer position • Ultrasound image • Anatomic diagram • Illustrative online videos
+ anschauliche Videofilme online!
The Most Important Planes in Abdominal Ultrasound (UA = upper abdomen; LA = lower abdomen)
s
Sagittal upper abdomen left paramedian plane
Sagittal upper abdomen right paramedian plane
Oblique lower abdomen para-iliac plane
Transverse epigastric plane
Transverse upper abdomen
Oblique right upper abdomen
Right oblique subcostal plane (hepatic veins)
Longitudinal transhepatic plane
Transverse right midabdomen
High plane of the left flank
Median sagittal suprapubic plane
Transverse suprapubic plane
In this book, the point at the end of the position mark on the transducer corresponds to the right edge of the respective image. Think about which organs will be visualized in which respective imaging plane. To find the solutions, fold this page out and look on the back.
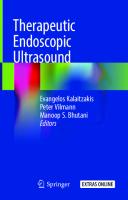
Standard Planes with Appropriate Transducer Position and Drawing Templates 1. Sagittal upper abdomen,
1 2
left paramedian plane (aorta)
3
9
13
32 a
34 47
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), rectus abdominis muscle (3), lung (47), left lobe of the liver (9), stomach (26) pancreas (33) aorta (1 ) celiac trunk (32) le t gastric artery (32a), superior mesenteric artery (17), superior mesenteric vein (23), diaphragm (13), five hypoechoic „eggs“: esophagus (34), crus of diaphragm (13), vertebral body (35) le t renal vein (2 ) hori ontal part o the duodenum (46) confluence of the portal vein (12)
26 32
13
23
33 12
17 46
25 b
15
35 35
3 13
2
1
9
47
2. Sagittal upper abdomen,
< 45° 11 18 66
right paramedian plane (IVC)
26
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), rectus abdominis muscle (3), lung (47), diaphragm (13), right atrium (114), stomach (26) pancreas (33) caudate lo e o the liver ( a) in erior vena cava (16) verte ral ody (3 ) right renal artery (24a), branch of the portal vein (11) with accompanying ile duct ranch (66) and ranch o the hepatic artery (18), main vein (10) of the left lobe of the liver (9), acoustic shadow (45) behind the vertebral bodies (35)
33
10 24 a
9a
35
16
114
45
47
1
2
3. Oblique lower abdomen, para-iliac plane
3/4 21
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), common iliac vein (22), external iliac vein (22a) and internal iliac vein (22b), common iliac artery (21), external iliac artery (21a) and internal iliac artery (21b), vertebral body (35), rectus abdominis muscle (3) or oblique muscles (4)
21 a 22 a
22
22 b 21 b
35
1
2
4. Transverse epigastric region (celiac trunk)
3 7
26
18 32
46
9
8
11
33
19
16
20
15
13
13
35
5. Transverse upper abdomen
1
2
(renal vein crossing)
3 8
26 33 b
33 a 12 17
46
16 35
24 a
33 c 20
15 13
25 b 24 b
6. Oblique right upper abdomen
1
2
3
(porta hepatis)
7
10 11 11
66
18 46
26 33 20
17 25 b
11
9
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), rectus abdominis (3), ligamentum teres (7) and falciform ligament (8), liver ( ) stomach (26) gastric all (74) pancreas (33) duodenum (46) con luence o the portal vein (12) superior mesenteric artery (17), splenic vein (20), aorta (15), inferior vena cava (16) right renal artery (24a) and le t renal artery (24b), diaphragm (13),vertebral body (35)
74
7
9
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), rectus abdominis (3), ligamentum teres (7) and falciform ligament (8), liver ( ) stomach (26) pancreas (33) duodenum (46) portal vein (11), hepatic artery (18), splenic artery (19) from the celiac trunk (32), splenic vein (20), aorta (15), inferior vena cava (16) diaphragm (13) verte ral ody (3 )
15 16 35
13
24 b
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), rectus abdominis (3) ligamentum teres (7) liver ( ) stomach (26) pancreas (33) duodenum (46) con luence o the portal vein (11) hepatic artery (1 ) common ile duct (66) splenic vein (20), aorta (15), right renal artery (24a) and left renal artery (24 ) in erior vena cava (16) le t renal vein (2 )
Standard Planes with Appropriate Transducer Position and Drawing Templates 7. Right oblique subcostal plane
1
2 3
(hepatic veins)
9
10
13 45
16
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), rectus abdominis muscle (3), liver (9), hepatic veins (10), diaphragm (13), in erior vena cava (16) acoustic shado (4 ) ehind lung (47), measurement of width of hepatic veins ( ) in the periphery o the liver < 6 mm
47
2
8. Longitudinal transhepatic plane
1
4
showing right kidney
9
45
29 13
30 31
9
44 5
47
35
13
9. Transverse plane showing right
1
2
kidney and IVC
3 9
10
80
26
17
14
46
33
33
12 16
29 30
15
25 b 24 b
35
13
24 a
116
44
1
2
left flank (spleen)
13 37 45 33
74
20
1
(bladder and uterus)
77
39
41 46
46
43 d
40 122
1
2
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), rectus abdominis muscle (3), acoustic shadow (45) behind the small bowel (46) and pu ic one (4 ) ladder (3 ) ladder all (77) reverberation artifacts (51a), uterus (39), endometrium (78), vaginal portion (os) of cervix (40), vagina (41), rectum (43d), rectouterine pouch of Douglas (122)
38
78 45
11. Median sagittal suprapubic plane
48
3 46 51 a
6
12. Transverse suprapubic plane
(bladder and prostate gland)
3
46
51 a
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), intercostal muscles (116) lung (47) diaphragm (13) spleen (37) stomach (26) stomach all (74) small o el (46) colon (43) tail of the pancreas (33), splenic vein (20) Caution: Top edge of image = lateral Bottom edge of image = medial
26
2
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), rectus abdominis muscle (3), liver (9), hepatic veins (10), gallbladder (14), gall ladder all ( 0) stomach (26) duodenum (46) renal parenchyma (29), medullary pyramids (30), renal caliceal system with renal pelvis (31), psoas major muscle (44), vertebra (35), right renal artery (24 a), right rena lvein (2 a) in erior vena cava (16) aorta (1 ) confluence of the portal vein (12), pancreas (33), superior mesenteric artery (17)
10. High plane of the
43 46
47
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), oblique muscles (4), liver (9), hepatic veins (10), diaphragm (13), lung (47), renal parenchyma (29), medullary pyramids (30), renal caliceal system with renal pelvis (31), acoustic shadow (45) behind colon (43), connective tissue (5), psoas major muscle (44), vertebra (35), diaphragm (13)
43
38
45
77 70
42 43 d
45
Visualized organs and vessels: Skin (1), subcutaneous fatty tissue (2), rectus abdominis muscle (3) linea al a (6) acoustic shado (4 ) ehind the small o el (46) acoustic enhancement (70) ehind the urinary bladder (38) with jets of urine from the ureteric orifices, bladder wall (77), reverberation artifacts (51a), prostate (42) or ovaries (91), rectum (43d)
Ultrasound Teaching Manual The Basics of Performing and Interpreting Ultrasound Scans Fourth expanded and revised edition Matthias Hofer, MD, Associate Professor, MPH, MME (Univ. Bern) Director of Education at the University Institute of Diagnostic, Interventional and Pediatric Radiology (DIPR) Dept. Head: Univ.-Prof. Johannes Heverhagen, MD, Inselspital Bern, Bern University, Switzerland
With Ultrasound Images from: Alexis Müller-Marbach, MD Head of Dept. of Gastroenterology, Hepatology and Palliative Care Helios Hospital Niederberg, Germany Jasmin D. Busch, MD, Associate Professor Section Head of Pediatric Radiology, Inselspital Bern, Bern University, Switzerland
930 Images
Stuttgart · New York · Delhi · Rio de Janeiro
Library of Congress Cataloging-in-Publication Data is available from the publisher. This book is an authorized translation of the 10th German edition published and copyrighted 2020 by Georg Thieme Verlag, Stuttgart. Title of the German edition: Sono-Grundkurs Translator: John Grossman Illustrators: Dr. Willi Kuhn, Ramona Sprenger
© 2021 Georg Thieme Verlag KG Georg Thieme Verlag KG Rüdigerstrasse 14, 70469 Stuttgart, Germany +49 [0]711 8931 421, [email protected] Thieme Publishers New York 333 Seventh Avenue, New York, NY 10001, USA +1-800-782-3488, [email protected] Thieme Publishers Delhi A-12, Second Floor, Sector-2, Noida-201301 Uttar Pradesh, India +91 120 45 566 00, [email protected] Thieme Publishers Rio, Thieme Publicações Ltda. Edifício Rodolpho de Paoli, 25º andar Av. Nilo Peçanha, 50 – Sala 2508 Rio de Janeiro 20020-906 Brasil +55 21 3172 2297 / +55 21 3172 1896
Important note: Medicine is an ever-changing science undergoing continual development. Research and clinical experience are continually expanding our knowledge, in particular our knowledge of proper treatment and drug therapy. Insofar as this book mentions any dosage or application, readers may rest assured that the authors, editors, and publishers have made every effort to ensure that such references are in accordance with the state of knowledge at the time of production of the book. Nevertheless, this does not involve, imply, or express any guarantee or responsibility on the part of the publishers in respect to any dosage instructions and forms of applications stated in the book. Every user is requested to examine carefully the manufacturers’ leaflets accompanying each drug and to check, if necessary in consultation with a physician or specialist, whether the dosage schedules mentioned therein or the contraindications stated by the manufacturers differ from the statements made in the present book. Such examination is particularly important with drugs that are either rarely used or have been newly released on the market. Every dosage schedule or every form of application used is entirely at the user’s own risk and responsibility. The authors and publishers request every user to report to the publishers any discrepancies or inaccuracies noticed. If errors in this work are found after publication, errata will be posted at www.thieme.com on the product description page. Some of the product names, patents, and registered designs referred to in this book are in fact registered trademarks or proprietary names even though specific reference to this fact is not always made in the text. Therefore, the appearance of a name without designation as proprietary is not to be construed as a representation by the publisher that it is in the public domain.
Cover design: Thieme Publishing Group Typesetting by Ramona Sprenger, Cologne www.einraumapartment.de Printed in Germany by Druckerei Steinmeier, Deiningen
DOI 10.1055/b000000431 ISBN 978-3-13-243760-9 Also available as an ebook: eISBN (PDF): 978-3-13-243761-6 eISBN (ePub): 978-3-13-243762-3
5 4 3 2 1
This book, including all parts thereof, is legally protected by copyright. Any use, exploitation, or commercialization outside the narrow limits set by copyright legislation, without the publisher’s consent, is illegal and liable to prosecution. This applies in particular to photostat reproduction, copying, mimeographing, preparation of microfilms, and electronic data processing and storage.
To access the additional media content available with this e-book via Thieme MedOne, please use the code and follow the instructions provided at the back of the e-book.
4
Contents Standard planes (front cover flap) Physical principles Image generation, sound transmission, reflection Echogenicity, frequency ranges Operation and features of ultrasound units Selection of ultrasound units, types of transducers
8 9 10 11
New techniques Panoramic imaging, 3D, Clarify Vascular Enhancement Harmonic imaging, phase inversion, Contrast agents Ultrasound CT Pulse compression, precision upsampling Diagnostic ultrasound catheter
12 13 14 15 16 17
Artifacts Reverberation, section thickness, acoustic enhancement Acoustic shadowing, mirror-image artifacts Side-lobe artifact, quiz for assessing progress Practical tips and tricks for the beginner
18 19 20 21
Lesson 1
Retroperitoneum, Sagittal plane Anatomy Upper retroperitoneum, normal findings Lower retroperitoneum, normal findings Aortic aneurysm Right heart failure Quiz
24 25 26 27 29 30
Lesson 2
Retroperitoneum, Transverse Plane Anatomy Normal findings Age-related echogenicity Acute pancreatitis, chronic pancreatitis Pancreatic tumors Retroperitoneal lymph nodes Quiz
32 33 34 35 36 37 38
Lesson 3
Porta Hepatis, Gallbladder, Biliary Tract Anatomy Porta hepatis Normal findings Portal hypertension Portal vein thrombosis, lymph nodes Gallbladder Cholecystitis Differential diagnosis of cholecystitis Gallstones Gallbladder polyps, cholestasis Biliary tract
40 41 42 43 44 45 46 47 48
Lesson 4
Liver Anatomy of the segments of the liver Sagittal plane, organ size, lateral angle
50 51
Transverse plane, hepatic veins Right heart failure Normal variants, fatty liver Focal fatty infiltration, focal sparing in fatty infiltration Cysts, echinococcosis (CE) Echinococcosis (CE), hepatic hemangiomas Focal nodular hyperplasia (FNH) Cirrhosis of the liver Hepatocellular carcinomas, liver abscesses Liver metastases, hypervascular metastases Hypovascularized liver metastases Quiz
52 53 54 55 56 57 58 59 60 61 62
Lesson 5
Kidneys, Adrenal Glands, Renal Transplants, Spleen Anatomy of the kidneys and adrenal glands Normal findings Normal variants, renal cysts Kidney degeneration, nephritis Urinary obstruction Differential Diagnosis of Urinary Obstruction Renal calculi, renal infarction Benign renal tumors, malignant renal tumors, adrenal tumors Normal findings Determining the size of a renal transplant, lymphoceles Spleen Anatomy, examination technique Spleen size, splenomegaly Splenomegaly, splenic infarcts, practical suggestion Lymphomatous infiltration, splenic hematomas, hyperechoic lesions, splenic cysts Quiz
64 65 66 67 68 69 70 71 72 73 74 75 76 77 78
Lesson 6
Thyroid Gland, Lymph Nodes, Gastrointestinal Tract Anatomy, volumetric measurements, normal values Normal findings Goiter Focal solid nodules, thyroiditis Lymph nodes Neck: lymph nodes Differential diagnostic criteria, perfusion parameters Differential diagnostic criteria, reactive inflammatory Retroperitoneal lymph nodes Gastrointestinal tract Anatomy, wall layers Gastric tumors Crohn's disease Intestinal intussusception, hernias, contrast enema Wall thickening, diarrhea, appendicitis Fecal impaction, colitis, colon carcinoma Diverticulitis Quiz
80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95
Physikalische Grundlagen Contents / Technik
Where Do I Find Which Chapter?
Lesson 7
Bladder and Reproductive Organs Anatomy Bladder Examination technique, determining postvoiding residual bladder volume Indwelling catheter and differential diagnosis of cystitis, wall thickening, internal echoes and sedimentation, ureteral peristalsis Reproductive organs Prostate and testis Undescended testis, orchitis, hydrocele Endovaginal ultrasound, image orientation Uterus: normal findings Uterine tumors Ovaries: volume, menstrual cycle phases Ovarian cysts and tumors Pregnancy testing Placenta position and gender determination Quiz
98 99
Pneumonia, pulmonary infarct, bronchial carcinoma
Quiz
Lesson 1
101 102 103 104 105 106 107 108 109 110
112 114 115 116 117 118 119 120 121 122
Retroperitoneum, Sagittal Plane
124 125 126 127 129 130 131 132 133 134 135 136 137 138 139 140 141 142
23
Lesson 2
Retroperitoneum, Transverse Plane
31
Lesson 3
Porta hepatis, Gallbladder, Biliary Tract
39
Lesson 4
Liver
49
Lesson 5
Kidneys, Adrenal Glands, Renal Transplants, Spleen
63
Lesson 6
Thyroid Gland, Lymph Nodes, Gastrointestinal Tract
Lesson 9
Pediatrics Skull and central nervous system Anatomy of the CSF spaces Normal findings in the sagittal plane Normal variants Normal findings in the coronal plane Cerebral hemorrhage Hydrocephalus Spinal canal Hip Preparation and positioning Normal findings Setup and measurement errors Graf`s classification of Infant Hips Kidneys, Bladder, Spleen Kidneys in newborns Diffusely increased echogenicity, nephrocalcinosis Urinary obstruction and reflux Urinary obstruction, voiding cystourethrogram Renal and adrenal tumors Urachus, ureterocele, spleen size Gastrointestinal tract Pyloric hypertrophy, reflux, Hirschsprung's disease
7
100
Lesson 8
FAST, eFAST, Lung, FAST algorithm eFAST algorithm Seashore sign, barcode sign Lung mobility, pulmonary pulse Lung point in pneumothorax Pleura Quantifying pleural effusions Pleuritis, empyema, mesothelioma Ribs Costal fractures, costal metastases Lung
Physical Principles
79
Lesson 7
Bladder and Reproductive Organs
97
Lesson 8
FAST, eFAST, Lung
111
Lesson 9
Pediatrics
123
Appendices
143
11 5
6
Tips for the Reader Appendices Primer of Ultrasound Findings Index Template for Report of Normal Findings Template for Report of Normal Findings Answers to Quizzes Thanks to Contributors, Hands-on Ultrasound Courses List of Abbreviations Examination Algorithms References Space for Your Notes and Drawing Exercises
144 148 149 150 155 159 160 161 166 167
How can you best profit from this book? How can you use this manual optimally? As you work through the individual chapters, you can benefit from several methodical and didactic features. Find it quickly ... Find a chapter: You will find the respective tab for each chapter on page 5. Find tough quiz questions for in-depth study. Find cross-referenced figures: The figures are numbered according to the page on which they appear. For example, Fig. 115.2 is on page 115. Find an explanatory figure or diagram supplementing the text. They are highlighted in the accompanying text in color and are almost always on the same page, eliminating the need to page through the book looking for them. Find numbered structures. Their reference numbers appear in bold in the accompanying text or on the back cover flap (the same number for each structure is used throughout the entire book).
Find keywords on page 148 (or on pages 4-6). Find for each structure normal values and checklists. These are also provided on laminated, water-resistant, pocket-sized cards. Why we call this book a "workbook"? A unique feature of this book is that you can use each page as a quiz to test your knowledge. The diagrams contain reference numbers instead of labels. This means you can go through the material a second time and use any figure to test which structures you know and which you still have to learn. The quiz questions and drawing exercises have a similar purpose. In this way, you can become familiar with several efficient study methods that allow you to integrate new material into your long-term memory faster – even though this requires you to take a more active approach to learning. Not only do I wish you good luck with this course, I also hope you have fun doing it! Matthias Hofer, MD, Associate Professor, MPH, MME, Summer 2020 Director of Education at the University Institute of Diagnostic, Interventional and Pediatric Radiology (DIPR) Inselspital Bern, Bern University, Switzerland
What does the respective color coding mean in the diagrams? Tumors
Connective tissue, fat
Arteries
Liver, thyroid gland
Veins
Muscles
Gallbladder wall
Gastric lumen
Pancreas
Air, bone
Bile
Acoustic shadow
Kidney
Spleen, lymph nodes
Urine
Prostate, uterus, ovary
Introduction
Physical Principles and Technical Fundamentals
8
New Techniques
12
Artifacts
18
Quiz
20
Practical Tips and Tricks for the Beginner
21
8
Physical Principles and Technical Fundamentals Image Generation
Sound Transmission in Human Tissue Ultrasound images are generated not by X-rays but by Air 331 m/s sound waves that are sent by a transducer into the huLiver 1549 m/s man body and reflected there. In abdominal ultrasound, Spleen 1566 m/s m = 1540 m/s the frequencies used generally are between 2.5 and 5.0 Muscle 1568 m/s megahertz (MHz; see p. 11). The primary condition Bone 3360 m/s required for sound wave reflections is the presence of so-called "impedance mismatches." These occur at Table 8.1 the interface between two tissue layers with different sound transmission properties (interfaces in Fig. 8.1). It is interesting to note that different soft tissues show TransTransonly minor differences in the transmission speed of ducer ducer sound (Table 8.1). Gel Skin Only air and bone are marked by massively different sound transmission in comparison with other human 2 tissue. For this reason ultrasound units can be operated at Interface A a preselected medium frequency of approximately 1540 m/s without producing any major inaccuracies in the 2 Interface B calculated origin ("depth") of the echo. 45 The processor computes the depth of origin of the echo 2 Interface C from the time difference detected between emission of the sound impulse and return of the echo. b Fig. 8.1 a Echoes from tissue close to the transducer (A) arrive earlier (tA) than echoes from deeper tissues (tB, tC in Fig. 8.1a). The mean frequency is strictly theoretical since the processor cannot know which type of tissue the sound waves traversed.
Which Component of the Sound Wave is Reflected? Fig. 8.1a shows on the left three tissue blocks traversed by sound waves that differ only minimally in their transmission velocity (indicated by similar gray values). Each interface only reflects a small portion of the original sound waves ( ) as echo ( ). The right–hand diagram shows a larger impedance mismatch at the interface A between the different tissues (Fig. 8.1b). This increases the proportion of reflected sound waves ( ) in comparison to the tissues shown on the left. However, what happens if the sound waves hit air in the stomach or a rib? This causes a so-called “total reflection,” as illustrated at interface B in Fig. 8.2b: The transducer does not
detect any residual sound waves deep to this structure from which it can generate an image. Instead, the total reflection creates an acoustic shadow (45). Conclusion: Intestinal or pulmonary air and bone are impenetrable by sound waves, precluding any imaging deep to these structures. The goal will later be to work around intestinal air or ribs by maneuvering the transducer. The pressure applied to the transducer against the abdominal wall (see p. 21) and the acoustic gel that displaces air between the surface of the transducer and the patient’s skin (see p. 22) play a significant role.
From a “Snowstorm” to an Image … Do not get discouraged if at first you can only make out a blinding "snowstorm" on ultrasound images. You will be surprised how soon you will learn to recognize the ultrasound morphology of individual organs and vessels. Fig. 8.2 visualizes the gallbladder (14) as a 1 black structure and shows two round 2 polyps (65) within it. The surround4 ing gray "snowstorm" corresponds to 5 74 the hepatic parenchyma (9) which 46 80 14 is traversed by hepatic vessels (10, 9 65 11). How can you quickly work out 45 10 which structures in the image appear bright and which are dark? The key 11 lies in the concept of echogenicity 9 11 45 (see p. 9). 9 Fig. 8.2
a
Gallbladder with polyps
b
Physical Principles and Technical Fundamentals What Does the Term "Echogenicity" Mean?
Please use the following terms:
These fluids are anechoic (= black):
Tissues or organs with many intrinsic impedance mismatches produce many echoes and appear "hyperpericardial or Hyperechoic (= bright) echoic" = bright. In contrast, tissue and organs with few pleural effusion, impedance mismatches appear “hypoechoic” = dark. ascites, cysts, Hypoechoic (= dark) Consequently, homogeneous fluids without impedance blood, urine, bile, mismatches (blood, urine, bile, cerebrospinal fluid, cerebrospinal fluid Anechoic (= black) pericardial or pleural effusion, ascites, cyst secretion) appear “anechoic” = black. The number of impedance mismatches does not depend on the physical density (= mass per unit of volume). This is best illustrated with a fatty liver (9). On this noncontrasted CT scan (Fig. 9.1a), the parenchyma of a fatty liver appears darker (i.e., less dense) than hepatic vessels or normal liver (Fig. 9.1b). This is due to the lesser density of fat in comparison with normal liver tissue. On ultrasound the fatty deposits produce more impedance mismatches (Fig. 9.1c) than in normal liver tissue (Fig. 9.1d). Consequently, a fatty liver appears more echogenic (brighter) on ultrasound despite its significantly lower physical density. A common misunderstanding: What do ultrasound examiners mean when they refer to a "dense liver"? Either they are not expressing themselves clearly or they have failed to grasp the fundamental principle of ultrasound imaging and how it differs from radiography. Ultrasound does not visualize physical tissue densities but differences in sound transmission (impedance mismatches) which are unrelated to density.
Fig. 9.1
a
CT: Fatty liver
b
CT: Normal liver
Fig. 9.1
c
Ultrasound: Fatty liver
d
Ultrasound: Normal liver
Generation and Frequency Ranges of Sound Waves Sound waves are generated by the reverse “piezoelectric effect.” The pressure waves of an echo distort crystals, causing them to emit an electrical impulse. The reverse takes place during transmission. A transducer includes many such crystals. Depending on the impulse applied, they can produce sound waves of various frequencies specified in megahertz (MHz). A “3.75–MHz” transducer does not exclusively emit pressure waves (sound waves) at a frequency of 3.75 MHz. That is merely the specified median frequency (= “center frequency”). In fact, such a transducer may emit sound wave frequencies between, for example, 2 and 6 MHz. So-called "multi frequency transducers" have the additional capability to increase or decrease this center frequency
and the surrounding bandwidth of transmitted sound frequencies. In thin patients or children, for instance, the bandwidth can be shifted (say 4–8 MHz with a center frequency of 6 MHz) to achieve better spatial resolution. However, this decreases the depth penetration of the sound waves. In very obese patients, the use of lower frequencies (1–5 MHz with a center frequency of 2.5 MHz) can be appropriate to achieve the necessary penetration, but at the cost of lower resolution (see p. 11). Newer methods base their image generation on frequency shifts or harmonic frequencies of the echo in relation to the original ultrasound impulse (see p. 13).
9
10
Physical Principles and Technical Fundamentals Operating an Ultrasound Unit Many controls on different ultrasound units are quite similar in function and arrangement regardless of the manufacturer. Therefore this section will look at the console of one unit supplied by Samsung (Fig. 10.1), which will then be used to introduce common technical terms. Selection of Transducer and Preset After you have switched on the unit (A) and it has booted, select the appropriate preset (PS) and the appropriate transducer for the respective examination and enter the current patient data (PD). You will usually select a linear array transducer (L) for evaluating the thyroid gland and the extremities but a convex array transducer (C) for abdominal examinations. The sector transducer (E) is used primarily in echocardiography, and the endovaginal transducer (G) is used for gynecologic examinations. Selecting the Image Mode, Gain, and Focus Usually you will begin with "normal" black and white or B-mode ultrasound (B), before later possibly switching to color-coded imaging (C). If you also wanted to obtain a flow profile from a blood vessel, you would then activate the Doppler mode (D) as well. This unit is equipped with control knobs that increase the respective signal (gain) of the active imaging mode when turned clockwise and reduce it when turned counterclockwise. The amplification (gain) can also be adjusted using the depth gain compensation feature (G). The transducer angle (A) must also be entered to determine flow velocities in Doppler mode. If you wish to display the change in a line of the image over time, switch to M-mode (MM). You can also set the specific depth range that is to have the best spatial resolution; here you use a toggle switch to set one or more focal zones (FZ) in your penetration depth. A few units also have a CW Doppler (CW) that measures frequency shifts (= flow speeds) not by means of depth gain compensation but as the summation of all speeds over an entire line of the image. Magnification and Zoom Function Especially with smaller target structures, you can significantly increase your detection of pathologic changes by magnifying the target organ (Mag) organ or zooming (Z) certain parts of the image. One common feature on almost all units is the position of the freeze or stop button (St) in the lower right corner of the console. This freezes the moving image. It is recommended to rest one finger of your left hand lightly on this button during the examination to minimize delay in capturing a desired image.
Size and Distance Measurements After freezing (St) you can retrieve individual images from digital storage with the cine loop function: To do so, turn the trackball (T) to the left to 9:00 o'clock and go back image by image until you reach the desired one. Depending on the manufacturer and preset, up to eight simple measurements (M) can be performed one after the other on the frozen image. Use the trackball (T) and the set button (S) to define the beginning and end positions of your measured distances. It may be helpful to switch to double image mode (2x) for comparative measurements in different planes. Right next to this on most units is another button for switching back to single image mode (1x). More complex measurements such as volume measurements or flow indexes can be accessed with the measurement program (MP). Helpful Extras When you want to explain the imaging findings to the patient or a colleague, it is helpful to activate a pointer (P) which you can move across the frozen image with the trackball (T) to point out the findings you are explaining. If you really want to score points with your patients, install an additional monitor below the ceiling in their field of view. Well equipped units also offer automatic image optimization (QS), several hot keys for frequently used settings (P1-P3), and also several transducer sockets (SP) spare you the time and hassle of plugging and unplugging probes.
PS PD G D MM A CW L W P MP M T S
TS F EB BB C Z E FK V B P1-P2 QS ST SP
Fig. 10.1 Console and keypad
Physical Principles Physikalische and Technical Grundlagen Fundamentals / Technik Selection of Ultrasound Units In addition to large color Doppler units, ultrasound units with connections for several multi frequency transducers have proven especially useful in a hospital setting. Such mobile units are easily moved from the ultrasound suite to the ward or intensive care unit (Fig. 11.1). The most important precaution when transporting the unit is to make sure that transducers are safely stowed so that dangling cables cannot become caught on doorknobs, gurneys, etc. A transducer that falls on the floor can easily represent a loss of €3000–7000 ($3300–7700) depending on the model. For the same reason, the transducer should never be left unattended on the patient’s abdomen when the examination is interrupted, for instance by a telephone call. Stowing the transducer in the frame with the cable hanging avoids unnecessary kinking that can lead to broken conductors in the cable. Types of Transducers Of the many types of transducers, only the three most important ones will be discussed here (endovaginal transducers, see p. 103). A linear array transducer or "parallel scanner" emits parallel sound waves into the tissue and produces a rectangular image (Fig. 11.2a). The width of the image and the number of scan lines remain constant at all tissue levels. Linear array transducers have the advantage of good near-field resolution and are primarily used with high frequencies (5.0–10.0 MHz or higher) for evaluating soft tissue and the thyroid gland. Their disadvantage is the large contact surface. This can lead to air gaps between skin and transducer when it is applied to a curved body contour (loss of acoustic coupling). Furthermore, acoustic shadowing (45) caused by ribs, lungs, or intestinal gas can greatly degrade image quality. Consequently, linear array transducers are rarely used for visualizing abdominal organs.
A sector transducer produces a fanlike image that is narrow near the transducer and increases in width with deeper penetration (Fig. 11.2b). This type of transducer has become established primarily in cardiology with lower frequencies (2.0–3.0 MHz) allowing deeper penetration. Due to the fanlike propagation of the sound waves, the heart can be well visualized through a small intercostal window without acoustic shadows from the ribs. The disadvantages of this type of transducer are their poor near-field resolution and decreasing line density in the far field with correspondingly decreasing resolution. Moreover, finding the desired imaging plane is difficult and takes some practice. A curved or convex array transducer is a combination of the two types described above (Fig. 11.2c). The shape of the monitor image resembles a coffee filter and combines good near-field resolution with relatively good far-field resolution. The major advantage of the slightly curved contact surface is its ability to displace interfering intestinal air outside the imaging plane by applying increasing pressure (see p. 21). With this type of transducer, however, one has to accept decreasing resolution with increasing depth and, in certain locations, acoustic shadowing behind the ribs. This type is usually used in abdominal ultrasound with center frequencies from 2.5 MHz (in very obese patients) to 5.0 MHz (in slender patients). The average frequency (center frequency) is usually 3.5–3.75 MHz. Memory aid: The higher the frequency, the better the resolution and the worse the penetration. The best way to remember this is to compare it to that loud music from your neighbor’s apartment. Which tones best penetrate even thick walls? The basses. These lower frequencies travel farther (i.e., penetrate deeper), see page 9.
Linear
Sector
Convex (curved array)
Ribs
45
45
45
60°
45
90°
Fig. 11.1
Fig. 11.2
a
b
c
11
12
New Techniques Panoramic Imaging (SieScape®) New high-performance image processors generate extensive ultrasound images from data acquired as the examiner moves the transducer slowly and continuously over the region of interest. With some practice, the examiner can produce impressive and undistorted images that allow distance measurements accurate to within 1–3% even on a curved body surface. Fig. 12.1 shows a sagittal scan with massive pleural effusion (69),
68 69
47
compressive atelectasis of the lung (47), and, inferior to the liver (9), anechoic ascites (68) that appears to inundate the small bowel (46). Fig. 12.2 impressively illustrates the position of the placenta (94) relative to the fetus. The high contrast resolution even allows evaluation of the interface between the fetal liver (9) and heart (114).
94
46
9
9
114
16 15
Fig. 12.1
Fig. 12.2
(With kind permission of Drs. C.F. Dietrich and D. Becker, from Farbduplexsonographie des Abdomens, Schnetztor-Verlag, Konstanz, Germany)
3-D Visualization Especially in obstetrics, the three-dimensional visualization of fetal facial features improves the diagnosis of malformations such as cleft lip and palate. This technique can now visualize the physiognomy of the fetal skull with amazing accuracy (Fig. 12.3). Of course, conventional cross-sectional imaging techniques can also detect skeletal and other malformations, albeit less impressively and clearly than three-dimensional ultrasound.
Fig. 12.3
Clarify Vascular Enhancement Technology This technique is based on an algorithm that is able to significantly reduce the blurring on B-mode scans resulting from partial volume or section thickness artifacts. Flow information from the power Doppler mode is used, which helps to improve the spatial resolution of vascular contours on the B-mode image.
Fig. 12.4
a
"Normal" image of the carotid artery ...
b
… with Clarify
The result is significantly improved visualization of findings such as the contours of hard and soft plaque in the carotid arteries (Fig. 12.4b) compared with the visualization achieved by the conventional technique shown in Fig. 12.4a. It also facilitates evaluation of peripheral vascular rarefaction in the liver as the lumens of the hepatic veins and portal venous branches are more clearly visualized in the hepatic parenchyma (Fig. 12.5).
Fig. 12.5 Hepatic vessels
New Techniques The material on the following five pages is not an absolute prerequisite for the first practice sessions and can be skipped. Beginners may prefer to move from here directly to the preparations for Lesson 1 (see p. 21). After some initial practice they should return to these pages to reinforce their fundamental understanding of ultrasound imaging. Tissue Harmonic Imaging (THI): This technique does not use the fundamental frequency of the original ultrasound impulse but their harmonics, integer multiples of the fundamental frequency (for example 7.0 MHz for a fundamental frequency of 3.5 MHz). These harmonics increase with increasing penetration, but their amplitude (intensity) remains far less than that of the base signal. The advantage of these harmonics is that they hardly arise at all near the transducer, but only
develop with increasing penetration depth (Fig. 13.1). Consequently, they are less affected by the major sources of scattered image noise, which occurs especially in the anterior abdominal wall. Why do harmonics develop only with increasing penetration depth? Ultrasound waves are distorted as they traverse tissues with varying acoustic properties. Their pressure waves compress and relax the tissue as they penetrate it. Compressed tissue increases the speed of sound. However, as the tissue relaxes, the speed decreases, causing the trough of the pressure wave to propagate more slowly. The resulting distortion of the wave form (Fig. 13.2) induces harmonics. This is a cumulative effect that increases with the depth of penetration. Consequently, the amplitudes of the harmonic frequencies initially increase with penetration depth until this increase is offset by general absorption (Fig. 13.1). Sound pressure
Intensity
Fundamental frequency
+
Harmonic frequencies
Depth
Skin level
Depth
ear eld
Increasing depth
ar eld
Fig. 13.2
Second Harmonic Imaging: This technique uses only the doubled frequency of the base signal for imaging. To avoid any overlapping of the range of the fundamental frequency (Fig. 13.3a) a narrowband signal must be used to distinguish the stronger components of the fundamental frequency from the weaker components of the harmonic (Fig. 13.3b). However, the narrower
bandwidth of the signal leads to a slight reduction in contrast and spatial resolution. In spite of these shortcomings, this technique has markedly improved the detection of details (Fig. 13.4b) compared with conventional ultrasound imaging (Fig. 13.4a), especially in obese patients (whose abdominal wall produces excessive scattering).
Intensity
Fig. 13.1
a
Intensity
Fundamental frequency b
Frequency
Harmonic frequency range Frequency
Fig. 13.3 Phase Inversion Technique: A broadband technique has since become established that allows the use of dynamically optimized harmonic multiples of the transmitted frequency with a broader bandwidth (Fig. 14.1c, Ensemble® THI). With this technique, image optimization no longer depends on the narrow bandwidth of the fundamental frequency (Fig. 14.1a) to cleanly separate it from its harmonics (Fig. 14.1b). Two successive pulses are transmitted in such a way that the phase (upward excursion of the pressure = positive, downward excursion = negative) of the second pulse is inverted to the phase of the first pulse (Fig. 13.5).
Fig. 13.4
a
b
Pulse 1
Pulse 2 (inverted) Sum of Pulse 1 +2
Fig. 13.5
a
Linear
b
Nonlinear
13
14
New Techniques If the echoes of both signals are added, the sum equals zero as long as the signal has not undergone any changes in the body. As a result, both fundamental frequency echoes Fundamental frequency are suppressed (Fig. 13.5a) whereas the second harmonic signal compoFig. 14.1 a nents are enhanced (Fig. 13.5b). Fig. 14.2 depicts a case showing acoustic shadowing ( ) deep to intrarenal calcifications (b) that are undetectable by conventional imaging (a). In addition, the renal cyst ( ) appears better demarcated and can be classified as benign with greater confidence.
2nd harmonic imaging
broadband harmonic imaging [MHz] c
b
Contrast Enhancement The echogenicity of blood and tissue can be enhanced with microbubbles with a diameter of 3–5 µm that pass through the capillaries and create more impedance b Fig. 14.2 a mismatches within the blood stream (Fig. 14.3). So far, several contrast enhancement agents have been introduced and about 50 additional agents are under development. The contrast agent Levovist® consists of tiny air bubbles ( ) about 3 µm in diameter (95% < 10 µm), which are stabilized with a thin envelope of palmitic acid (Fig. 14.4). They are initially bound to galactose microparticles that dissolve in the blood and release the microbubbles. The dry powder can be mixed by the examiner in different concentrations. The suspension passes through the pulmonary circulation, but is only injectable for about 8 minutes after preparation. Hypergalactosemia is a contraindication. Measuring just a few millimeters, the microbubbles are comparable in size to erythrocytes (Fig. 14.5), which explains how they are able to pass through the capillaries. Ultrasound impulses with low sound pressure make these microbubbles vibrate at what is known as a low "mechanical index" of 0.05–0.2. Contrast images are created using the nonlinear resonance frequency exclusively. Alternatively, one can use a higher mechanical index around 1.0–1.5 to cause the microbubbles to burst and emit a significantly stronger signal (although Fig. 14.3 only during a single passage).This is known as the burst method. The contrast agent Sonovue® consists of an aqueous solution of sulfur hexafluoride (SF6) stabilized by a phospholipid layer (Fig. 14.6). The median size of the bubbles is about 2.5 µm (90% < 8 µm) with an osmolality of 290 mOsmol/kg. One possible advantage of this contrast agent is that the Galactose suspension remains stable for over 6 hours, allowing it to be used for several applications. The best results are achieved in conjunction with the tissue harmonic imaging (THI) technique, referred to as "contrast harmonic imaFig. 14.4 ging (CHI)." Frequently, the term contrast-enhanced ultrasound (CEUS) is also used. A specific sound pressure causes the bubbles to vibrate and emit harmonic echoes. As a result, contrast harmonic imaging (Fig. 14.7b) can detect multiple liver metastases significantly better than noncontrasted imaging (Fig. 14.7a).
SF6
SF6 Phospholipid layer
SF6
SF6
Fig. 14.5 Microbubbles
Fig. 14.6 Sonovue®
Fig. 14.7
a
Noncontrasted
b
CEUS
New Techniques Spatial Compounding (SonoCT®T) There is another technique for suppressing artifacts. "Real-time compound imaging" does not scan an image line by line (Fig. 15.1a), instead it scans from different angles and merges this data into an image in real time (Fig. 15.1b). Up to nine different slices can be scanned,
allowing more precise visualization of tissue information. This is illustrated here by the morphology of arteriosclerotic plaque in the carotid artery ( in Fig. 15.2a) compared with conventional imaging (Fig. 15.2b).
a
(Conventional)
Fig. 15.1
(SonoCT)
a
b
This technique has exhibited obvious advantages in ultrasound imaging of the breast and musculoskeletal system. Fig. 15.3b shows improved visualization of an entire biopsy needle ( ) in the breast parenchyma in comparison with conventional imaging (Fig. 15.3a), making it possible to advance the needle to the suspicious lesion with greater precision.
Fig. 15.3
a
b
Fig. 15.4
b
The combination of SonoCT® scanning with tissue harmonic imaging (see p. 13) has shown promising results. It allows detailed visualization of hepatic lesions (Fig. 15.5) or fetal morphology in prenatal ultrasound screening (Fig. 15.6). The high performance computer
Fig. 15.5
Fig. 15.2
Fig. 15.6
systems now available can easily combine SieClear® or SonoCT® with three-dimensional (Fig. 15.7) and panoramic imaging techniques (Fig. 15.4). Here, almost the entire liver at the level of the hepatic venous system is visualized (see p. 52).
Fig. 15.7
15
New Techniques Pulse Compression This technique is derived from one originally developed for radar. Its main advantage is improved visualization of deep structures. It is not possible to increase penetration depth simply by increasing transmission power as this would produce undesirable thermal and mechanical effects. However, it is possible to increase the duration of the transmitted pulses and to modulate their frequency in a specific pattern ("chirp coding"). In this manner, the individual transmitted impulse has greater energy although its amplitude remains unchanged (Fig. 16.1a). The reflected echoes are then decoded by a chirp receiver filter and transformed back into shorter echoes of correspondingly higher amplitude (Fig. 16.1b).
Transmitted chirp pulse
Received chirp pulse
Decoded received signal Variation of frequency and amplitude
Fig. 16.1 Principle of pulse compression
The result is greater penetration depth with the degree of anatomic detail normally achieved only with lower frequencies and lower (and correspondingly worse) resolution. Fig, 16.2c shows a hypoechoic mass (54) deep to the thyroid gland (81) which would not have been visualized without pulse compression (Fig. 16.2a).
85 / 90
81
45
54
45
Fig. 16.2
a
c
b
Precision Upsampling In conventional image processing techniques with high-frequency transducers, ultrasound echoes are scanned at a rate of only about 2–5 times the speed of the maximum frequency components of the echo (wide grid in Fig. 16.3a). Consequently, these echoes are only detected at a few points along their curve, and the monitor image really represents only an approximation of the actual echo signal (Fig. 16.4a). More complex reconstruction algorithms can record the duration and amplitude of the actual echo signal far more accurately (narrower grid in Fig. 16.3b). The result is that the structures of the radial tendon ( ) shown here are visualized with significantly higher definition (Fig. 16.4b).
Amplitude
16
With precision upsampling
Conventional sampling Time
Fig. 16.3
a
b
Fig. 16.4
a
b
New Techniques Diagnostic Ultrasound Catheter Miniaturized transducers are another new development. These transducers are available in fine catheters only 3 mm in diameter that can be rotated 160° in any direction (Fig. 17.1). Fig. 17.2 shows the size of an AcuNav probe (= Accurate Navigation by Siemens)
in comparison with a TEE transducer of the type used within the esophageal lumen. The small size of the disposable catheter allows it to be advanced into the heart via the venous system.
Fig. 17.1
Fig. 17.2
This technique can visualize a previously poorly accessible atrial septal defect ( ) in a B-mode scan (Fig. 17.3a) at higher frequencies around 7.5 MHz. It can also visualize the flow through the shunt on a color-coded Doppler image (Fig. 17.3b) significantly more precisely than was previously possible. This also makes it easier to monitor instrumental closure of the atrial septal defect ( in Fig.
17.3c) and verify the success of the procedure. The advantages of this technique in comparison with TEE are its superior image quality and the elimination of the need for sedation or general anesthesia. This in turn makes it possible for the patient to cooperate during the examination (holding breath, Valsalva maneuver, etc.) and makes the examination less stressful for the patient.
Fig. 17.3
a
The catheter system can also be advanced through the right heart into the inferior vena cava and there be used to guide insertion of a direct intrahepatic portosystemic shunt (DIPS). From the inferior vena cava, it is possible to visualize adjacent esophageal varices ( in Fig. 17.4) or retroperitoneal lymph nodes (55) with very high spatial resolution (Fig. 17.5). Some the nodes shown here are necrotic (57). Note that the layers of the wall ( ) of the adjacent duodenum (46) are also shown in high definition.
b
c
46
57 55 Fig. 17.4
Fig. 17.5
17
18
Artifacts Reverberation: The monitor image does not always reflect the true echogenicity. There are visual phenomena that do not correspond to the actual anatomy that are generally referred to as "artifacts." The image generation illustrated on p. 8 assumes that the echoes always return directly from the point of reflection to the transducer. The processor makes the same assumption when computing the depth of the site of reflection. In reality, this is not always the case: On their way back to the transducer, the reflected sound waves can encounter impedance mismatches that reflect some of them back into deeper tissue. There
they are again reflected off an interface and reach the transducer eventually but with some delay (Fig. 18.1). The processor evaluates the delayed arrival of the returning echoes as increased penetration depth, and these echoes are visualized too far down on the image. Usually this phenomenon is lost in the background noise of the image. However, against an anechoic background such as the lumen of the urinary bladder (38) or gallbladder, these reverberations appear as lines parallel to the anterior abdominal wall (51a in Fig. 18.2). These sound waves can "bounce back and forth" repeatedly, producing a series of parallel lines (51a).
5 Transducer
Skin
2
3
46
Gel
46
l
51a 51a
77
38
Interface A
45
Interface B
77
45 51b
70
Fig. 18.1
Fig. 18.2
a
Section thickness artifact: The far wall of the urinary bladder can appear similarly indistinct. If the bladder wall (77) or the wall of a cyst or the gallbladder is not perpendicular to the sound lobe but tangential to it, this wall, too, will be indistinctly visualized (51b in Fig. 18.2). Such section thickness artifacts must be distinguished from sedimented material (small concrements, sludge, blood
b
clots, 52 in Fig. 18.3). However, these are usually more sharply demarcated from the remaining lumen and can be disturbed with the transducer. Transducer
Scatter
2
70
Refraction
6
5
64
38 38
45 70 46/45
Fig. 18.3
a
b
Distal acoustic enhancement: Relative enhancement of the echoes (70) occurs behind large vessels or cavities (64) filled with homogeneous (anechoic) (Fig. 18.4). In Figures 18.2 and 18.3 the tissue posterior to the bladder (38) appears almost white and cannot be evaluated. How does this happen? Wherever sound waves travel for some distance through homogeneous fluid, they are not reflected and do not attenuate. Thus, behind the gallbladder, bladder, cysts, or major vessels, there is more “unspent” acoustic
52
70 70
45
Fig. 18.4 energy than in surrounding areas of the image. This results in a more hyperechoic (brighter) appearance (70) of the underlying tissue that does not correspond to its "true" characteristics. In theses cases, it is advisable to use time gain compensation (TGC) to reduce the echogenicity of deeper image levels. This acoustic enhancement can also be a useful criterion for differentiating anechoic cysts (which show distal acoustic enhancement above a certain size) from hypoechoic hepatic lesions (which do not usually exhibit this phenomenon).
Artifacts Acoustic Shadowing Bands of markedly reduced echogenicity (hypoechoic or anechoic = black) occur deep to strong reflectors such as ribs, concrements, some ligaments, and gastrointestinal air. As a result, the inferior ribs or the pubic bone can obscure deeper structures in the same manner as air in the stomach or bowel. The examiner can also exploit this effect to a a detect calcified gallstones (49) in the 2 1 gallbladder (14) as in Fig. 19.1, renal 2 4 4 calculi (49 in Fig. 70.2), or arterios5 5 3 74 2 clerotic plaques (49 in Fig. 29.1). In46 26 testinal air can either cast hypoechoic 9 9 9 80 10 (dark) shadows or cause hyperechoic 80 62 (= bright), "comet tail" artifacts due 14 49 14 5 to vibration of small gas bubbles or 49 49 45 46 multiple reflection. 9 45 Deep to round cavities whose walls 9 45 70 45 70 lie tangential to the sound beam, 70 13 edge shadows (45) can occur (Fig. 19.2). These shadows are caused by Fig. 19.1 b Fig. 19.2 b scatter and refraction (Fig. 18.4). In the case of the gallbladder (14) in Fig. 19.2, one must examine the image carefully to correctly identify the acoustic shadow (45) as a gallbladder edge shadow and avoid mistakenly interpreting it as part of the hypoechoic less fatty portion (62) of the liver (9). Acoustic shadowing due to duodenal air (46) is commonly misinterpreted as acoustic shadows from stones in the adjacent gallbladder. Do you remember the phenomenon responsible for the false hyperechoic appearance (70) of the liver parenchyma deep to the gallbladder (14) in Fig. 19.2?
Mirror-Image Artifact Strongly reflecting interfaces such as the diaphragm (13) can deflect sound waves in such a manner that they mimic a lesion on the other side of the diaphragm (Fig. 19.3). The sound waves are deflected laterally by the diaphragm, encounter a reflector (R), and are reflected back to the diaphragm, which in turn reflects them back to the transducer. The processor can only base its calculation of the distance of the object on the time of flight
of the sound pulse. Therefore, the object (R’) incorrectly appears too deep on the image. Fig. 19.4 shows the inferior vena cava (16) as a mirror image projected above the diaphragm (16’). Additionally, the mirror image of the hepatic parenchyma (9) appears on the pulmonary aspect of the diaphragm (9’). Fig. 53.2 shows another example of a mirror-image artifact.
1/2
3 9
11
45
10 R
13
16
9
R’
16' 13
Fig. 19.3 Path of sound in a mirrorimage artifact
Fig. 19.4
a
b
9'
45
19
20
Artifacts / Quiz Side-Lobe Artifact So far, we have assumed that the sound waves propagate in a straight line from top to bottom in the image (dark blue lobe in Fig. 20.1). In fact, the sound waves also propagate in several secondary "side-lobes" that can cause undesirable scatter and blurring. When such a side lobe strikes a strong reflector, the processor can incorrectly assign the obliquely reflected sound waves
to adjacent lines of the image (Fig. 20.2). The farther laterally the waves are reflected, the longer their path and time of flight and the deeper the processor will project the echoes on the image. This often results in an arclike extension of a strongly reflecting interface ( in Fig. 20.3). This characteristic arc is typical of the side-lobe artifact.
Transducer Skin
Gel
51c
Fig. 20.1 Side lobes
Fig. 20.2 Path of sound in a side-lobe artifact
Fig. 20.3 Example of a side-lobe artifact
Quiz on Technical Fundamentals and Technique Before beginning practical exercises or Lesson 1, you are invited to test which information you have really understood and are able to recall and where you still have
gaps. You can check your answers by going back to the previous pages. The answer to image question 4 is on page 154.
1.
3.
How does the processor compute the depth of the reflected echo? Can you deduce at least three artifacts from this principle and explain them in detail to a colleague or fellow student?
4.
Look at Fig. 20.4 and explain the names and origin of all artifacts you can recognize.
Which structures are almost always anechoic (= black) on ultrasound images? Name four physiologic and four pathologic ones.
Physiologic:
Pathologic:
·
·
·
·
·
·
·
·
2.
Which frequencies do you use for which examination and why? Specify the respective bandwidth in MHz and sketch the monitor display of the corresponding type of transducer. When do you use which transducer? Why?
Fig. 20.4
Practical Tips and Tricks for the Beginner I Spatial Orientation Before beginning practical exercises in a practice setting or an ultrasound workshop, you should first become familiar with spatial orientation in the three-dimensional space of the abdomen. To make the first step easy, we will initially consider only two perpendicular planes, the vertical (sagittal) imaging plane and the horizontal (transverse) plane. Your active participation is now required to ingrain these two planes in your memory.
Step 2: Before you look up the answer, repeat the exercise for the short-axis (transverse) plane. Here, the convention is that the image is displayed on the monitor as viewed from the caudal perspective (from the patient’s feet) (Fig. 21.1b). Again write down four of the six possible directions on the back of the filter. Again two will be wrong, but different ones this time. Once you have thought about your results, check the answer on page 155.
Step 1: Take a (European) coffee filter (there is no hospital where you will not find one) or draw the outline of a coffee filter on a piece of paper. Most filters have the same general shape as an ultrasound image generated by a convex transducer (see p. 11). Now imagine along which margin of the image (= edge of the coffee filter) the patient’s respective anterior, posterior, left, right, cranial, and caudal structures must lie when you view the imaging plane from the patient’s right side according to international convention (Fig. 21.1a). Hold the coffee filter against your abdomen and imagine that the sound waves propagate from the linea alba toward the spine. Write down four of the six possible directions on the edges of the coffee filter or your drawing. Two will be wrong, but why? (It is worth your while. You will always remember this if you figure it out for yourself.)
The next problem will be the acoustic shadow created by superimposed intestinal air. The solution is usually not to use more gel (as many beginners think) but to vary the pressure applied to the transducer.
Fig. 21.1
a
Sagittal plane
b
Transverse plane
How Much Pressure Should I Apply to the Transducer? too suddenly so as not to startle the patient or cause unnecessary pain (Fig. 21.3). The trick is to maintain this pressure. That will increasingly and gently displace intestinal air from the imaging plane. The acoustic shadow (45) will disappear and the pancreas (33) and other vessels will be clearly visualized (Fig. 21.2 b). This principle is especially helpful for visualizing retroperitoneal lymph nodes and vessels in the mid and lower abdomen as well. In infants, this maneuver is usually superfluous and counterproductive because of their lower pain threshold and defensive reaction.
The beginner is usually concerned about causing discomfort to the patient and does not press the transducer firmly against the abdominal wall. As a result of this hesitation ( ), the air normally present in the lumen of the stomach or bowel (26) remains in place and its acoustic shadow (45) obscures the view of the pancreas (33) and adjacent vessels posterior to it (Fig. 21.2a). The extrahepatic common bile duct (66) and the portal vein (11) are also often obscured by gastric or duodenal air. The solution in adults is to apply measured, slowly increasing pressure ( ). Do not apply pressure
1
1 74 9 11
2
2
9
74
26
66
45 16
66
16 35
Fig. 21.2
36
a
35
36
Slight pressure
33
26
11
33
16 35
35
b
36
35
Greater pressure
36
35
Fig. 21.3 Applying pressure
21
22
Practical Tips and Tricks for the Beginner II Relevance of adequate breathing instructions: Beginners are naturally reluctant to give the patient very direct instructions. Nonetheless, almost all patients are very cooperative when you explain the following situation to them: Image quality (and therefore the validity of your findings) in the upper abdomen is often markedly improved when the patient inhales very deeply to displace the liver caudally. Why? In a neutral breathing position (Fig. 22.1a), portions of the liver (9) and spleen are not the only structures obscured by acoustic shadows of the caudal lung segments. Often the pancreas (33) and its surroundings cannot be visualized because of the air content
of the stomach (26). However, when the liver (9) in maximum inspiration (Fig. 22.1b) is displaced caudally ( ), the air-filled bowel and stomach (26) are also displaced caudally, allowing a good view of the pancreas and important lymph nodes. The same principle greatly improves visualization of the kidneys and hilum of the liver (see below). Please use clear breathing instructions such as: "Take a deep breath with your mouth open [pause] and now please hold your breath." Remember to instruct the patient immediately to exhale after an adequate pause (on average 10 to 12 seconds, but maximum of 20 seconds) or as soon as you have frozen the image. This instruction is not nearly as trivial as you may think.
1
1
2
2
9
9
74 74
74
26
26 9
45
9
33
a
Neutral respiratory position
Visualizing the hilum of the liver: Should you be unable to visualize the hilum of the liver despite the tricks discussed above, try to visualize the porta hepatis through an intercostal window in expiration (Fig. 22.2). If this is also unsuccessful, place the patient in the left lateral decubitus position (Fig. 22.3). The liver’s own weight will shift it closer to the anterior abdominal wall, displacing bowel loops and exposing the porta hepatis with its important vascular structures (see p. 41).
33
45
15
15
Fig. 22.1
45
26
Good breathing instructions are not only well received by the patient, they also avoid undue strain on the patient’s respiratory system and expedite the examination of the upper abdomen significantly. These maneuvers are superfluous when examining the lower abdomen.
b
After deep inspiration
Fig. 22.2 Visualization through an intercostal window
Fig. 22.3 Left lateral decubitus position
Test your skills: Please look at Figures 22.4 and 22.5. Both show poor-quality images. Determine which was obtained with too little gel and which with too little pressure. Fig. 22.6 shows an optimal image obtained with proper pressure and an adequate amount of gel. All three images were obtained in the same patient in rapid succession. The answer can be found on page 155.
Fig. 22.4
Fig. 22.5
Fig. 22.6
Lesson 1 Retroperitoneum, Sagittal Plane
With images from Matthias Hofer and Alexis Müller-Marbach rights
Anatomy
24
Normal Findings
25
Aortic Aneurysm
27
Right Heart Failure
29
Quiz
30
24
Lesson 1
Retroperitoneum, Sagittal Plane Anatomy In the posterior section of the cranial retroperitoneum, the pulsing aorta (AO, 15) and the inferior vena cava (IVC, 16) with its typical "double-beat" sign are the primary vascular structures (Fig. 24.1) that facilitate orientation. At the aortic origin of the celiac trunk (32), where it branches into the splenic artery (19), hepatic artery (18), and left astric artery (32a) as well as in the vicinity of the superior mesenteric artery (17), there are regional lymph nodes that represent common sites for lymph node metastases of the stomach, liver (9), gall bladder (14), and pancreas (33) as well as both adrenal glands (155) and both kidneys (29).
However, in contrast to the drawing shown here, there is a relevant lateral distance between the aorta and the inferior vena cava known as the aortocaval space in which abnormally enlarged lymph nodes can also occur. Fig. 24.2 shows the immediate topographic relationship to the porta hepatis (slightly further posterior), where the hepatic artery (18) and the common bile duct (66) obscure the portal vein (11) which courses posterior to them. You will find these and all other numbers on the legend on the back cover flap, and the numbers shown there match every page in the book.
34 155
155
16
13
18 27
13
13
10 17
24a 25a 150 28
29
19 25b
15
47 9
21
11
66a
22 21
14
66
b a
18
33c
46
43b
46
22b
43c 23
38
Fig. 24.1 Posterior retroperitoneum
20
33a 75
43
37
32a 32 19 33b
43
22a
16
66b
150 44
34
10
17
Fig. 24.2 Anterior retroperitoneum
(Schuenke M, et al: THIEME Atlas of Anatomy–Internal Organs, 3rd ed. Stuttgart: Thieme, 2020. Illustrations by M. Voll, K. Wesker.)
Video Clips and Clinical Examinations The accompanying video clips for Lesson 1 contain in-depth information on ultrasound anatomy (Video clip 1.1a) as well as practical tips for performing a meticulous, uniform scan of the upper retroperitoneum in sagittal planes. Clinical considerations are not limited to the detection and diagnostic classification of enlarged lymph nodes. The examination is also intended to exclude disorders such as aortic aneurysm (see p. 27–28) or pelvic venous thrombosis ascending into the inferior vena cava as well as to assess whether in the setting of acute right heart failure the inferior vena cava (16) and hepatic veins (10) are dilated (see p. 29). The examination involves the practical challenge of having to displace gastrointestinal air in the duodenum (46), transverse colon (43b), and in the anteriorly located stomach (not shown here) out of the respective imaging plane by applying adequately dosed pressure, strong enough in order to visualize the posterior retroperitoneal vascular structures and lymph nodes. Video clip 1.1b shows you some helpful hints that are focused on transducer position and application of pressure, whereas Video clip 1.1c explains the resulting ultrasound images in greater detail.
Lesson 1
Upper Retroperitoneum
Normal Findings Before you work through this page, please complete the exercise on page 21 to familiarize yourself with spatial orientation in sagittal planes. You should only proceed here when you are completely familiar with this orientation and the physical principles discussed on pp. 8–11. From here on, you will be assumed to have this basic knowledge.
vertebra. At the left margin of the image you will see the thin hyperechoic line of the diaphragm (bare area, 13) that exhibits a hypoechoic muscular extension (13 a) at the anterior margin of the aorta, which can easily be mistaken for a retroperitoneal lymph node, just like the esophagus (34).
The goal of examining the retroperitoneum goes beyond evaluation of the retroperitoneal vessels. It is also intended to exclude disorders such as aortic aneurysm or thrombosis of the vena cava. An additional goal is to become familiar with the vascular anatomy of this region because obliquely imaged vessels can easily be mistaken for oval lymph nodes, which are also hypoechoic. Correct identification of the individual vessels also greatly facilitates spatial orientation and provides landmarks to aid in identifying other structures later. The transducer is placed along the linea alba perpendicular to the abdominal wall, and the Fig. 25.1 beam is swept through the upper abdomen in a fanlike motion (Fig. 25.1). For now, commit only the normal anatomy in sagittal planes to memory: When you tilt the transducer to the patient’s right side (Fig. 25.2a), you will find the liver (9) the aorta (15), the celiac trunk (32), and the superior mesenteric artery (SMA, 17) on the left anterior to the
Farther inferiorly, crossing between the superior mesenteric artery (17) and the aorta (15) is the obliquely visualized left renal vein (25b). Beginners often misinterpret the hypoechoic oval shape of this vein as a pathologic lymph node. Compare this to the cross section at the same level (Fig. 33.3) and the anatomic sketch in Fig. 32.1. Farther anteriorly (closer to the transducer) at the posterior margin of the pancreas (33), you will find the confluence of the portal vein (12). Air in the stomach (26) can produce acoustic shadows at the inferior margin of the liver. Now tilt the transducer to the patient’s left side (Fig. 25.3a) to visualize the inferior vena cava (IVC, 16) in a right paravertebral location and its junction with the right atrium (114). The diameter of the aorta and inferior vena cava are measured perpendicular to their longitudinal axes (see pp. 27–29). Within the liver (9) hepatic veins (10), branches of the left portal vein (11), and (anterior to it) the hepatic artery (18) may be distinguished. In this plane the caudate lobe (9a) is separated from the rest of the hepatic parenchyma (9) by a thin hyperechoic septum. The maximum craniocaudal diameter of the caudate lobe should measure less than 5.0 cm and its anteroposterior diameter less than 2.5 cm. 1
2
6
5 3
26
23
13 115
9
11
74 46
33 17
10 11
12
32
25b
13
35
34 15
114
36 36
Fig. 25.2
a
b
Longitudinal section of the aorta
45
c
5
1
3
13
11 10
66
9
a
b
Longitudinal section of the inferior vena cava
c
33 11
16
Fig. 25.3
26
18
9a
114
47
2
35
24a 45
13 45
25
26
Lesson 1
Lower Retroperitoneum Normal Findings After you have examined the upper retroperitoneum, move the transducer along the aorta and inferior vena cava (Fig. 26.1a) inferiorly ( ). In addition to visualizing the lumens of these major vessels, the examiner must also tilt the transducer (Fig. 25.1) to search for enlarged perivascular lymph nodes on either side of the vessels. Enlarged lymph nodes will invariably appear as hypoechoic oval structures (see pp. 87 and 37). Abnormally enlarged lymph nodes can also occur anterior and posterior to the major vessels as well as in the aortocaval
Fig. 26.1
a
space. In the absence of a retroaortic mass, the distance between the posterior wall of the aorta and the anterior margins of the vertebrae should not exceed 5 mm, if there is no aortic kinking in patients with chronic arterial hypertension. It is always best to perform this examination in two planes (see pp. 32 and 33). The iliac vessels arising caudal to the aortic bifurcation are identified in the same manner and examined in two planes (see Video clip 1.2c):, parallel to the axis of the vessel (Fig. 26.2) and perpendicular to it (Fig. 26.3).
c
b
The confluence of the external iliac vein (22a) and internal iliac vein (22b) is a common site for enlarged regional lymph nodes (Fig. 26.2). The iliac artery (21) is anterior to the vein (above it on the image). When in doubt, a simple compression test can help you distinguish the two vessels. Because of its lower intraluminal pressure, the vein is more easily compressed with the transducer
than the artery. On the transverse image (Fig. 26.3), one can often distinguish iliac vessels from hypoechoic bowel contents in loops of the small bowel (46) by intestinal peristalsis alone. If necessary, one can try to induce peristalsis by rapidly varying the pressure applied to the transducer. 4 2 46
46
5
74
74
46
46
46
21a
46
21
22a
22 21b 35
Fig. 26.2
a
b
22b
35
c
1 4
46
46
74
46 74
46
46
a
b
c
46
46
46
Fig. 26.3
4
2
*
74
22 35
21
45
Lesson 1
Retroperitoneum
Aortic Aneurysm Circumscribed dilations of the vascular lumen usually occur as a result of arteriosclerotic lesions and localized weakening of the arterial wall, and, less often, secondary to trauma. Ectasia is defined as a dilation of the aortic lumen greater than 25 mm and less than 30 mm. It can also occur in combination with an aneurysm (Fig. 27.1), which is defined as a diameter greater than 30 mm in the suprarenal abdominal aorta or 40 mm in the aortic arch. The dilation can be fusiform or saccular. Complications can include dissection of the layers of the aortic wall (dissecting aneurysm) or mural thrombosis (52), which can lead to peripheral or abdominal emboli. Risk factors for rupture include increasing aneurysm size, diameter exceeding 50 or 60 mm, respectively, and outpouching of the wall resembling a diverticulum. A concentric lumen in a thrombosed aneurysm can have a protective effect, whereas
an eccentric lumen is deemed to be at increased risk of rupture. As a rule, the risk of rupture increases with aneurysm size. However, the indication for surgical intervention depends on many individual factors so that it is not possible to define an absolute threshold. Any ultrasound evaluation of an aneurysm must determine the following crucial facts: The maximum craniocaudal length of the dilation (Fig. 27.2), its maximum transverse diameter (Fig. 27.3), and any dissections, thrombosis, and involvement of visceral branch arteries (celiac trunk, superior mesenteric artery, renal arteries, and iliac arteries). The primary artery supplying the spinal cord (great radicular artery of Adamkiewicz) is variable in its segmental level, and because of its narrow caliber it is not usually detected on ultrasound images. Supplementary spiral CT or angiography (DSA) are usually required to visualize the arterial supply to the spinal cord.
Suprarenal aorta Infrarenal aorta
1
2
Checklist Aortic diameter
5
< 25 mm < 20 mm
3
46
46
Distance to spine Posterior wall Memory aid:
Vertebra < 5 mm 2.5–2.0 = 0.5
Aortic ectasia Aneurysm
25–30 mm > 30 mm
Table 27.1 Normal values for abdominal aorta
15
45
45
70 45
Fig. 27.1
a
Aortic aneurysm
b
1
2 3
74 46
6
3
74 46
5 45
52
45
15 53
45
45
Fig. 27.2
a
Sagittal plane
b
Partial thrombosis
c
3
1
2
74
74 52
45
15 35 a
Transverse plane
b
Crescentic thrombus
c
46
5
46
Fig. 27.3
3
6
45
27
28
Lesson 1
Retroperitoneum Aortic Aneurysm Aside from the quantitative estimation of whether the finding still represents aortic ectasia (luminal diameter less than 2.5 cm in the abdomen, Fig. 28.2) or must be classified as an aortic aneurysma (Fig. 28.3) with a
luminal diameter exceeding 3 cm, partially thrombosed or dissected aortic aneurysms require the evaluation of additional interpretation criteria:
Questions about aortic aneurysms: • Craniocaudal length? • Aortic origins of other arteries involved? • Dissection: Which origins of true false lumens? • Partial thrombosis: Concentric eccentric? • Signs of contained rupture? Table 28.1 Interpretation criteria
Fib. 28.2 Aortic ectasia
Fib. 28.3 Aortic aneurysm
Where the patent, perfused arterial lumen is encased within circular mural thrombosis, the generally hard thrombus provides a certain degree of protection against rupture of the concentric lumen. However, in the case of eccentric or peripheral thrombus (52) as in Fig. 28.4, there is an increased risk of rup1/2 5 3 ture. With very hypoechoic thrombi, 9 the extent of the thrombosis is often 32 17 underestimated or the lesion is even 15 missed entirely on B-mode scans 13 45 (Fig. 28.5a) and supplementary 15 52 35 color-coded studies (Fig. 28.5c) are required to define the demarcation 35 45 between the perfused aortic lumen 45 (15) and a crescentic thrombus (52) 45 such as that shown here. b Fib. 28.4 a Sagittal plane 1/2 9 11 9
155 29
Fib. 28.5
a
Transverse plane
46 33a 24a
26
17 12
16 13 35
3/5
15 52
33c
45
49
c
b
Color-coded study
Indication for Contrast-Enhanced Ultrasound When in doubt, contrast-enhanced ultrasound (CEUS, see p. 14) can help to determine which arteries arise from the true lumen and which from the false one in a dissection. It can also demonstrate a contained rupture ( ) in the periaortic retroperitoneum (Fig. 28.7a) which a noncontrasted or color-coded duplex scan would have failed to detect ( in Fig. 28.7b). Fib. 28.7
a
CEUS with aneurysm
b
Lesson 1
Retroperitoneum
Systematic examination of the retroperitoneum must include evaluation of the venous system in addition to any changes in the aorta and lymph nodes. The inferior vena cava (IVC) can be distinguished from the aorta by its anatomic location (right prevertebral location, not left). A further distinguishing characteristic is its typical precordial double pulse (as opposed to the single pulse of the aorta). Along the wall of the aorta (15) in older patients you will often find echogenic arteriosclerotic plaques (49). When calcified, these lesions can create acoustic shadows (45) (Fig. 29.1).
Right Heart Failure When evaluating the inferior vena cava (16), be alert to any dilation exceeding 20 mm (25 mm in young athletes) as this suggests venous congestion proximal to the right atrium consistent with right heart failure (Fig. 29.2). It is important to obtain the measurements perpendicular to the longitudinal axis of the vein. Be careful to avoid exaggerating the size of the lumen of the vena cava by mistakenly including hepatic veins (10) that enter the vena cava inferior to the diaphragm (Fig. 29.2). When in doubt, perform the vena cava collapse test during forced inspiration. Instruct the patient to inhale as deeply as possible through the nose with the mouth closed. The sudden drop in intrapleural pressure collapses the subdiaphragmatic vena cava or at least briefly reduces its diameter to one-third or less of its initial value (see Video clip 1.1c). The challenge for the examiner is to maintain the imaging plane in the center of the inferior vena cava during the sudden expansion of the chest on inspiration. Alternatively, this test can be performed when imaging the upper abdomen in
a
74
• Dilated hepatic veins
> 6 mm in the periphery of the liver
• IVC does not collapse on forced inspiration • Possible pleural effusion, often initially unilateral on the right Table 29.1 Interpretation criteria for right heart failure
3
2
15
49
22 a 49
44
22 b
10 70
45
Arteriosclerotic plaques
45
16
16
47
21 a
21 22
10
49
49
1
2
26
9
13
b
> 20 mm or > 25 mm in young athletes
a
46
Fig. 29.1
• IVC dilated
1/2
5
45
Checklist for right heart failure
a
1 3
the transverse plane, or the diameter of the peripheral hepatic veins may be evaluated (see p. 52). Do you remember the reason why the liver tissue in Fig. 29.2 posterior to the distended inferior vena cava appears to be more hyperechoic than anterior to it? If not, please review the artifacts on page 18 and name this phenomenon. Secondary to an inguinal puncture, images of the distal iliac vessels (Fig. 29.3) can occasionally show a hematoma (50) in the vicinity of the iliac artery (21) or vein (22). Persistent blood flow into the hematoma through a patent communication with the arterial lumen is referred to as a “false aneurysm.” This is distinguished from a true aneurysm by the fact that there is no outpouching of all layers of the vascular wall but a perivascular hematoma secondary to a full thickness tear in the wall (Fig. 29.3). A differential diagnosis must distinguish subacute or chronic inguinal hernias from psoas major abscesses within the true pelvis, lymphoceles, synovial cysts in the hip and larger ovarian cysts, and from metastases with central liquefactive necrosis (57).
70 13
Fig. 29.2
b
9
Engorged inferior vena cava
44 57
50 45
35
45
45
Fig. 29.3
b
Para-iliac lymph nodes
29
30
Lesson 1
Quiz Before proceeding to the material in Lesson 2, you can test whether you have really mastered the learning points and contents of Lesson 1 by answering the questions below. Pursued with a little determination, this self-evaluation can effectively prevent you from simply
1.
Which anatomic direction corresponds to the left edge of the image on sagittal scans? For practice, label the coffee filter shown here. Remember which of the following six anatomic directions cannot appear on the edges of the filter: anterior, posterior, left, right, cranial, caudal.
2.
What is the maximum normal luminal diameter of the inferior vena cava and abdominal aorta? What is the definition of aortic ectasia and aortic aneurysm? What questions would you as an examiner seek to answer using ultrasound images? What are the limits of ultrasound imaging (when would supplementary CT or DSA be better)?
skimming through this workbook superficially without any long-term benefit from your reading. Enjoy the test. You will find the answers to questions 1 through 6 on the preceding pages. You may look up the answers to the image in question 6 on page 156 later.
Suprarenal aorta
45° Abrupt caliber changes of the portal vein Possible enhanced "embankment" of the portal vein Regenerating nodules with displaced vessels
Additional Findings in the Late Stage • Rounded organ shape (obtuse marginal angles) • Shrinkage of the liver • Signs of portal hypertension Fig. 58.4 Widened angle Fig. 58.5 ... with variable of the hepatic veins ... caliber
Table 58.6
As the disorder progresses, the presence of regenerating nodules causes widening ( ) of the normally acute angle (compare to Fig. 50.6) of the confluences of the hepatic veins (10); one observes wider confluence angles (Fig. 58.4) in these veins, which under magnification often exhibit irregular vascular contours ( ) as well (Fig. 58.5).
The late stage characterized by shrinkage of the liver often includes portal hypertension (see p. 42) with ascites (68). The altered surface of the organ is thus obvious at first glance (Fig. 58.7a) or at the latest with appropriate magnification (Fig. 58.7c), which inexperienced examiners should always use if they do not want to overlook cirrhosis of the liver. Compensatory hypertrophy of the caudate lobe can also be a sign of liver damage.
2 4 68 9
13 11 47
Fig. 58.7
a
Liver shrinkage with ascites
b
80 68
14 5 45
11 5
74
46 c
Magnified surface
Lesson 4
Liver
Hepatocellular Carcinomas Aside from complications such as portal hypertension and portal vein thrombosis (see pp. 42–43), malignant liver tumors often occur as late sequelae of cirrhosis of the liver. Therefore it is important to inspect every cirrhotic liver carefully and thoroughly for focal masses (see Video clip 4.1c) to detect a hepatocellular carcinoma (54) as early as possible (Fig. 59.1). When in doubt, perfusion of the focal lesion is evaluated using contrast-enhanced ultrasound (CEUS) with a contrast agent (see p. 14). Typical findings in the early arterial phase include peripheral enhancement with individual
4
2
radial vessels extending into the center of the tumor (Fig. 59.2a). Any central necrosis (57) in the tumor will not enhance during the arterial phase (Fig. 59.2b) and portal venous phase (Fig. 59.2c). A typical feature of hepatic malignancies is that arteriovenous shunts within the tumor tissue lead to an early washout phenomenon in the late venous phase in comparison with the normal hepatic parenchyma (Fig. 59.2d), making the tumor area appear more hypoechoic, although not as early and as markedly as with liver metastases (see pp. 60–61).
5
1
4
54
68
68
2
9 57
54
18
9
9
Fig. 59.1
a
Hepatocellular carcinoma
Fig. 59.2
b
Arterial phase
Fig. 59.2
b
c
Portal venous phase
a
Early arterial perfusion phase
d
Late venous phase
Liver Abscesses As abscesses can also develop a central necrosis, they represent an important differential diagnosis to hepatic malignancies. An acute liver abscess (58) can exhibit a pronounced reaction in adjacent tissue or none at all (Fig. 59.3). Chronic abscesses frequently
develop a double wall and show internal echoes within the lesion (Fig. 59.4). In the presence of clinical signs of infection, one must be careful to actually scan the entire liver so as not to miss any subphrenic abscesses (Fig. 59.5).
2 3
45
9 18
58
9 14
Fig. 59.3 Acute liver abscess
43/46
Fig. 59.4 Chronic abscess
Fig. 59.5 Subphrenic location
59
60
Lesson 4
Liver Liver Metastases The liver is the site of metastases not only of gastric and colorectal carcinomas but often also metastases from hematogenous seeding in patients with bronchial and breast carcinomas. Metastases (56) in the hepatic parenchyma (9) are highly variable in their ultrasound morphology. Typically, but by no means invariably, they exhibit a hypoechoic perifocal halo in the tissue adjacent to the metastasis as in Figs. 60.1 and 60.2. The echo-
4
1
2
4 46
genicity of metastases varies from more hypoechoic lesions to ones with hyperechoic centers (Fig. 60.1) to more hyperechoic lesions (Figs. 60.2 and 60.3). Depending on the type of tumor, the speed of its growth, and/or the immune response or chemotherapy, regressive changes such as scarring, hyperechoic fibrosis or calcification (Fig. 60.2), or central necrosis (57) can also occur (Fig. 60.3).
2
4
74
5
47
47
74 46
2 4
14 9
80
45
47
45
70
45
9
11
b
Signs of regression
The decisive finding for excluding the differential diagnoses of parasites (see p. 55), focal nodular hyperplasia (see p. 57), or cirrhotic changes (see p. 58) when evaluating
Fig. 60.3
b
16 9
13 47
13
Fig. 60.2
11
56
45
13
Typical halo
b
9
56 57
10
10
57
56 45
56
56
13
Fig. 60.1
9
5
Central necrosis
focal lesions of the liver is not so much their echogenicity as their pattern of enhancement with a contrast agent on contrast-enhanced ultrasound (CEUS).
Hypervascularized Metastases The primary tumors are often neuroendocrine tumors such as thyroid carcinomas or carcinoids. In the arterial perfusion phase of the contrast agent (about 15–45 seconds after injection, see p. 14), these show increased perfusion proceeding from the periphery of the metastasis (56) in comparison with the adjacent normal hepatic parenchyma (Fig. 60.4a). In the portal venous phase (approximately 45–120 seconds after contrast injection),
Fig. 60.4
a
Arterial phase
b
the hyperperfused zone expands into the center of the lesion, sparing only central areas of necrosis (Fig. 60.4b), and often shows early washout. The distinguishing feature of malignant metastases occurs particularly in the late venous phase (approximately 2–5 minutes after injection) in the form of an early washout phenomenon which makes the lesion appear more hypoechoic than the normal hepatic parenchyma in the vicinity (Fig. 60.4c).
Portal venous phase
c
Late venous phase
Lesson 4
Liver
Hypovascularized Liver Metastases Primary tumors that produce hypovascularized liver metastases primarily include colorectal carcinomas. The early washout phenomenon in the late venous phase of contrast perfusion is due to the tendency of malignant tissue to develop increased quantities of pathologic arteriovenous shunts. These shunts circumvent the time-consuming passage through the capillary system that occurs in normal liver tissue (9) with the result that the contrast agent leaves the metastatic tissue (56) early and appears in the hepatic veins (10) after only 20–30 seconds.
9
56
56
Fig. 61.1 Plain scan The noncontrasted images of the case shown here demonstrated several hyperechoic lesions (56) with ill defined hypoechoic halos (Fig. 61.1). In the end of the arterial phase (about 15–45 seconds after contrast injection, but also later in heart failure), the obviously hypovascularized metastases here were already more hypoechoic than the adjacent hepatic tissue (Fig. 61.2).
Fig. 61.2 End of the arterial phase In the further course of the study in the portal venous phase (about 45–120 seconds), the echogenicity can partially equalize or remain hypoechoic (Fig. 61.3). Focal and multifocal areas of increased or reduced fatty infiltration (see p. 54), which a differential diagnosis must consider, do not exhibit any differences in perfusion to normal hepatic tissue.
Fig. 61.3 Portal venous phase The difference in echogenicity between benign and malignant lesions becomes particularly noticeable in the late venous drainage phase, in which the metastases enhance particularly markedly ( ), setting them apart from the adjacent hepatic parenchyma (Fig. 61.4). Here, too, the difference in echogenicity results from the increased number of arteriovenous shunts in the malignant tissue, leading to an early washout phenomenon.
Fig. 61.4 Late venous phase
14
61
62
Lesson 4
Quiz Please take this quiz to test your command of the material presented in Lessons 3 and 4. You will find the answers to the questions on the preceding pages. You will find the answers to the image quiz on page 156. It is best to
check the answers only after you have worked through all questions. Getting the answers too early ruins the suspense and defeats the purpose of the quiz.
1.
Repeat the drawing exercise for the standard imaging plane of the porta hepatis. Where are hepatic artery and bile duct in relation to the portal vein and inferior vena cava? Please compare your drawing with Fig. 41.2c.
2.
What is the name of the imaging plane that visualizes the hepatic venous star? How do you hold the transducer to obtain this plane? Draw the corresponding body markers and sketch the appearance of the hepatic venous star. What measurements can you make at which locations? For what purpose?
3.
Write down six characteristics of portal hypertension and eight criteria of cirrhosis of the liver. Compare your answers with the checklists on pages 42 and 85, and repeat this exercise over the next few days until you remember every finding (leave time to rest in between!).
4.
Do you remember the sites of predilection for focal fatty infiltration and focal areas of reduced fatty infiltration of the liver? How can you distinguish these processes from hepatic malignancies?
5.
What is the maximum diameter of the common bile duct? Above what diameter in mm would you suspect obstructive cholestasis?
6.
Write down several differential diagnoses for Fig. 62.4. The solution is on page 156.
7.
Review the following three ultrasound images. Write down the imaging planes, the organs and vessels visualized, and your differential diagnosis. Include all changes and your interpretation as some images include several pathologic processes.
Fig. 62.4
Fig. 62.1 Imaging plane: Organs: Vessels: Differential diagnosis:
Fig. 62.2
Fig. 62.3
Lesson 5 Kidneys, Adrenal Glands, Renal Transplants, Spleen
Kidneys and Adrenal Glands: Anatomy
64
Normal Findings
65
Normal Variants, Renal Cysts
66
Kidney Degeneration, Nephritis
67
Urinary Obstruction
68
Differential Diagnosis of Urinary Obstruction
69
Kidney Stones, Renal Infarcts
70
Tumors
71
Renal Transplants
72
Spleen: Anatomy, Examination Technique
74
Spleen Size, Curtain Trick, Splenomegaly
75
Splenomegaly, Splenic Infarcts
76
Focal Splenic Lesions
77
Quiz
78
64
Lesson 5
Kidney Anatomy of the Kidneys and Adrenal Glands The right kidney (29) lies in the retroperitoneal space posterior to the hepatorenal recess (pouch of Morison) and the right hepatic lobe. It lies immediately lateral to the spinal column so that the right renal vein (25a) only needs to cover a short distance to reach the inferior vena cava (16) (Fig. 64.1). The right renal artery (24a) typically but not invariably courses posterior to the vena cava. Its anatomy is highly variable; it can branch early or there can be accessory renal arteries which arise either from the aorta or even from the common iliac artery in the form of an inferior polar artery. Lying like a cap on the upper pole of the kidney (27), the right adrenal gland (155) is very well supplied by several arteries and is often the site of metastases of bronchial and other carcinomas. Normally both kidneys are highly mobile with respiration and displace along the bed of the psoas major muscle (44), which courses posteriorly. The examiner can exploit this mobility to avoid acoustic shadows of the ribs or intestinal air. Within the kidney, the renal pelvis (31) located in the center is differentiated from the outer parenchyma (29) and the medullary pyramids (30) located outside the parenchyma/pelvis (PP) border, ( – – – in Fig. 64.2). These medullary pyramids contain tubules that drain into the calices (149) at the tip of the respective papilla. In adults the length of the kidney from the upper pole (27) to the lower pole (28) measures between 10 and 12 cm depending on the person's height.
16 13 155
27
32 18 24a
29
17
25a
15 28
16
44
Fig. 64.1 Right kidney in the retroperitoneum
27 30
30
30
30 29
149
149
31
24b
150 29 28
The left kidney lies posterior to the tail of the pancreas (33c) and has a shorter left renal artery (24b) and a longer left renal vein (25b) compared with the right kidney (Fig. 64.3). Lying on the upper pole of the left kidney (27) in an anterocranial position is the left adrenal gland (155). The first regional nodal groups of the kidney lie at the renal hilum in the vicinity of the aorta (15) and celiac trunk (32). The key to the other numbers may be found in the legend on the back cover flap.
83
Fig. 64.2 Structure of the kidney
34
16
19
13 15 11
155
27
109 20
32
18 19 23 20 24 b 25b 17 33b 15 33a
33c 29
23 46
(Schuenke M, et al: THIEME Atlas of Anatomy–Internal Organs, 3rd ed. Stuttgart: Thieme, 2020. Illustrations by M. Voll, K. Wesker.)
13
28 150
44
Fig. 64.3 Topography of the left kidney
47
2
Lesson 5
Kidney
Normal Findings The right kidney can be well visualized in a longitudinal section through the liver from the anterior axillary line with the patient positioned supine after deep inspiration (Fig. 65.2a). Alternatively, the transducer can be placed parallel to the intercostal spaces with the patient in the left lateral decubitus position (Fig. 65.1a). Scan each kidney thoroughly in two planes. The left kidney can be visualized in the transverse and longitudinal planes with the patient supine or in the right lateral decubitus position (see Video clips 5.1a–c). Deep inspiration should displace the kidney to the level of the psoas major muscle (44), that is caudally 3–7 cm. This displacement can be exploited to place the kidneys in a better acoustic window between the ribs and intestinal air. Normally, the parenchyma of the right kidney is isoechoic to hepatic parenchyma (Fig. 65.3). It should be at least 1.3 cm thick in adults. A "string of pearls" visualized along the border between the outer paren-
chyma (29) and the hyperechoic central renal caliceal system (31) in the typical longitudinal plane (Fig. 65.2) represents the hypoechoic medullary pyramids (30). They should not be mistaken for anechoic cysts or renal calices. The central region of the kidney appears hyperechoic because of the many impedance mismatches between the walls of vascular structures, connective tissue, and fat. The right renal hilum is well visualized in the transverse plane (Fig. 65.3) as is the course of the renal vein (25) extending to the inferior vena cava (16) (see Video clips 5.2a, b). Be alert to hypoechoic masses within the hyperechoic suprarenal fat capsule at the upper pole of the kidney (27) as these suggest adrenal tumors. An important measure of chronic kidney damage is the ratio of the thickness of the hypoechoic peripheral parenchyma to the hyperechoic renal pelvis in the center. This parenchyma to pelvis (PP) index decreases with age (see Table 65.4): Checklist of Normal Renal Values Kidney length: 10–12 cm Kidney width: 4–6 cm Respiratory mobility: 3–7 cm Width of parenchyma: 1.3–2.5 cm PP index: Age < 30 years Age 30–60 years Age > 60 years
Fig. 65.1
a
> 1.6 : 1 1.2–1.6 : 1 1.1 : 1
Table 65.4
b
5
4 9
43
30 31 13
29
45
44
27
47
Fig. 65.2
a
b
Longitudinal section of the kidney
c 1
2 5
4
10
10 9 14
30 29 31
Fig. 65.3
a
b
Transverse section of the kidney
c
25
16
65
66
Lesson 5
Kidney Normal Variants
Renal Cysts
The normal shape of the kidney (Fig. 65.2) can exhibit several developmental variants. Hyperplastic columns of Bertin can protrude from the parenchyma (29) into the central renal pelvis (31). However, these columns are isoechoic to the rest of the renal parenchyma. An isoechoic parenchymal bridge can completely divide the renal pelvis, or partial or complete duplex kidneys (Fig. 66.1) may be present with separate ureters and blood supply for each moiety.
Dysontogenetic cysts (64) are usually anechoic as in the liver (see p. 55). Above a certain size as in Fig. 66.2 they show distal acoustic enhancement (70). Do you remember the other criteria for differentiating cysts from hypoechoic renal tumors in obese patients? If not, see the checklist on p. 55. Peripheral cysts lying on the renal capsule and projecting outward are distinguished from parenchymal cysts (Fig. 66.2), and parapelvic and pelvic cysts. These latter cysts can be mistaken for a urinary obstruction in the renal pelvis (31) because of their location (see pp. 68 and 73). The examiner should note the diameter of the cyst and its location (upper or lower pole; or upper, middle, or lower third of the kidney) and carefully examine its immediate vicinity for any signs of a tumorous mass. Some malignant renal tumors contain cystic components that may be significantly more conspicuous than the actual solid component of the tumor. Isolated renal cysts are of no clinical significance and require only long-term follow-up. In contrast, the adult form of familial polycystic kidneys (Fig. 66.3) can produce multiple cysts (64) with progressive growth in middle age. These cysts can reach a considerable size. Polycystic degeneration leads to kidney failure in early adulthood as a result of displacement and thinning of the renal parenchyma. These patients eventually require dialysis.
A horseshoe kidney with prevertebral bridges can at first glance be misinterpreted as a preaortic lymphoma or thrombosed aortic aneurysm. An undulating kidney surface due to persisting fetal lobulation is occasionally observed in children and young adults. Although slightly domed, the surface of the kidney itself is smooth. There may be fine indentations between the medullary pyramids. These indentations must be differentiated from the more triangular scars occurring secondary to renal infarcts (see Fig. 70.3), which are most often found in older patients with renal artery stenosis or suprarenal aortic aneurysm. About 10% of all patients show localized parenchymal thickening along the lateral border of the left kidney, usually caudal to the adjacent lower pole of the spleen. This "dromedary hump" is a normal bulge that can be difficult to differentiate from an actual renal tumor.
4
1
2
1
4
1
4
5
29 29 31
11
29
9
31
64
Partial duplex kidney
5 64
30
Fig. 66.2
29 64
31 70
Fig. 66.1
9
13
64
27 b
2 3/5
74 46
9
2
64 47
70
70
43 64
45
31 44
2 5
b
Renal cyst
Fig. 66.3
b
Polycystic kidneys
Lesson 5
Kidney
Kidney Degeneration renchyma (29). This increases its contrast against the hypoechoic medullary pyramids (30 in Fig. 67.3). This results in what are known as "punched out" medullary pyramids. Compared with the adjacent spleen or liver tissue (9), the parenchyma of the inflamed, infiltrated kidney appears significantly more hyperechoic (Fig. 67.3) than it normally does (see Fig. 66.2).
Slowly progressive narrowing of the outer parenchyma with increasing age is physiologic (see p. 65). Increased parenchymal atrophy (Fig. 67.1) also occurs secondary to repeated inflammation or in the setting of high-grade renal artery stenosis. Reduced perfusion can involve the entire kidney or circumscribed infarcts can occur, as is often the case in embolic disorders (see Fig. 70.3). In end-stage disease, narrowing of the parenchyma (29) can be so pronounced that it is barely visualized on ultrasound (Fig. 67.2). This imaging example of a shrunken kidney shows the most common associated findings of degenerative calcifications (53) or calculi (49) that are visualized indirectly because of their acoustic shadows (45). Shrunken kidneys can be so small that ultrasound scans fail to detect them. Loss of function in a kidney can be fully compensated by the contralateral kidney, which shows compensatory hypertrophy. When a shrunken kidney is detected on one side, one should first determine the parenchyma to pelvis (PP) index (see p. 65). A normal index suggests congenital renal hypoplasia. Usually the combination of examination of the contralateral kidney and color duplex ultrasound evaluation of renal perfusion can establish a diagnosis.
Unfortunately, the increased echogenicity of the renal parenchyma does not allow any conclusions as to the cause of the inflammation. The same phenomenon occurs with interstitial nephritis, chronic glomerulonephritis, diabetic nephropathy, renal amyloidosis (autoimmune infiltration), and urate nephropathy. This latter form results from an elevated serum uric acid concentration in gout or increased tissue destruction. Ultrasound does not make any significant contribution to a differential diagnosis among the various causes of inflammation. However, it is useful for following up nephritis during therapy and for excluding additional complications. Using Doppler ultrasound to determine the resistance index (a measure of renal perfusion) can provide valuable information about the course of infiltration or the onset of acute rejection in transplanted kidneys. When in doubt, ultrasound-guided needle biopsy can obtain renal tissue for histologic evaluation. In acute nephritis, the parenchyma can be diffusely hypoechoic and widened, and the border between the parenchyma and renal pelvis can appear indistinct or blurred. In normal kidneys this border is invariably sharply demarcated.
Nephritis The kidney reacts to various causes of inflammation with a relatively uniform morphologic picture on ultrasound. The kidney can appear normal in acute pyelonephritis or where inflammation is limited to the glomeruli. However, it later increases in size due to edema. Interstitial infiltration also increases the echogenicity of the pa-
2
4 9
31 29
46 74
45
45
10
b
Kidney stones
29
45
49/53
45
45
Fig. 67.2
b
46
11
29
13
Fig. 67.1
9
31
31
27 47
74
46
30 29
1
4
4 9
49
2
1
2
74 46
25 a
45
13
Shrunken kidney
Fig. 67.3
29
27 b
Nephritis
30
74 45
35
67
68
Lesson 5
Kidney Urinary Obstruction The many impedance mismatches exhibited by the renal caliceal system and the walls of the numerous vascular structures make the normal central pelvic complex appear very hyperechoic (see Figs. 65.2 and 67.1). In the absence of urinary obstruction, the pelvic complex is traversed only by narrow hypoechoic lines corresponding to small blood vessels or parts of the collecting system. As diuresis increases after intake of a large amount of fluid or under diuretics, the secretion effect can cause the collecting system (87) within the pelvic complex (31) to appear more pronounced than usual (Fig. 68.1).
1
Checklist of Urinary Obstruction
5
43
First degree:
only renal pelvis is dilated
29
Second degree:
calices are also dilated
Third degree:
additional parenchymal narrowing
Fourth degree:
hydronephrosis (residual parenchyma barely visible)
45
Four degrees of urinary obstruction are distinguished in adults, up to and including hydronephrosis. In first-degree obstruction, the renal sinus (87) is dilated but the dilation does not involve the caliceal necks (Fig. 68.2). The thickness of the parenchyma is normal. In
1
9
30
29
46
24 31
29 30
30
45
b
First-degree urinary obstruction
74
43
Normal diuresis effect
2
4
45
29
9
45
Second-degree urinary obstruction
5
5 5
45
31
45 70
b
4
2 29
30
5
5 44
Fig. 68.3
44
70
5
Fig. 68.2
28
29
second-degree urinary obstruction, the caliceal necks and calices are dilated as well (Fig. 68.3). Third-degree urinary obstruction is characterized by pressure atrophy and narrowing of the outer renal parenchyma (29) as well (Fig. 68.4):
31
44
31
Fig. 68.1
149
149
45 30
1
30
2
46
30
31
45
9
4
2
87
Table 68.1 Checklist for degrees of urinary obstruction in adults
2
4
Fig. 68.4
b
29
45
Third-degree urinary obstruction
Lesson 5
Kidney
Urinary Obstruction prostatic hypertrophy in men (see p. 101) include gynecologic tumors (see p. 105) and calculi (49) lodged in the ureter (150) causing retrograde urinary stasis (Fig. 69.2). Common sites for lodged ureter calculi are circled in Fig. 69.3: At the origin of the ureter, at the crossing of testicular vessels in the male and ovarian vessels in the female and/or the iliac vessels, and at the distal insertion of the ureter into the bladder wall.
Chronic urinary obstruction finally leads to destruction of the parenchyma of the affected kidney so that fourthdegree urinary obstruction in adults corresponds to the full picture of hydronephrosis (Fig. 69.1). Where both kidneys are affected, the result is near total loss of function so that dialysis is indicated. You will find the classification of urinary obstruction in children on pages 138 and 139. The most common causes aside from
13 16 27 155 24a 18 29
25a 28
17
21
2 4
1
9
5
5
149
43/46 149
31
22
150 22b 21b
21a
46
74
49
150
5
44
4
149
149
22a
46
43 45
44
83
38
31 13
44
155 / 5
35
Fig. 69.1
15
16
150
32a 19 25b
b
35
45
45
45
Fourth-degree urinary obstruction
Fig. 69.2
b
Ureter calculus
Fig. 69.3 Narrow points in the ureter (Schuenke M, et al: THIEME Atlas of Anatomy– Internal Organs, 3rd ed. Stuttgart: Thieme, 2020. Illustrations by M. Voll, K. Wesker.)
Differential Diagnosis of Urinary Obstruction Patients with an ampullary type of renal pelvis or slightly more prominent hilum vessels (25) can also show a sparse hypoechoic renal pelvis (Fig. 69.4) that is of no clinical significance. However, here the renal vessels usually appear finer than the typical thickening seen in first-degree urinary obstruction (see Fig. 68.2). When in doubt, the differential diagnosis may be resolved by color duplex sonography. There, the more rapidly flowing blood is color-coded whereas the static or slowly flowing urine remains anechoic (= black). It is more difficult to distinguish urinary obstruction from multiple pelvic cysts (64) because these cysts lack any flow and thus are not colorcoded by color duplex sonography (Fig. 69.5). In order to make this distinction, you can look for direct, black (filled with fluid) connections to the renal pelvis and ureter.
1
1 4
2
2
43/46
4
43/46
5
30
29 25
5
37
45
25
29 30
31
35 35
74
87
27
87
45 64
31
35
35 35
Fig. 69.4
b
Ampullary renal pelvis or Fig. 69.5 prominent hilum vessels
b
Distinguishing pelvic cysts from urinary obstruction
69
70
Lesson 5
Kidney Kidney Stones Detecting stones in the kidney (nephrolithiasis) is more difficult than detecting stones in the gallbladder (see p. 46) because the hyperechoic stones (49) often lie within the equally hyperechoic renal pelvis (31 in Fig. 70.1) and therefore are not contrasted against the relatively hypoechoic fluid in the vicinity of the stone. Stones in an obstructed renal sinus are a notable exception as the contrast is greater here. The examiner must be particularly alert to acoustic shadows (45) caused by kidney stones or calcifications. Fig. 70.2 shows an example of extensive renal calcifications (49) in a patient with hyperparathyroidism and a markedly elevated serum calcium level. Depending on its composition, a kidney stone (49) can be completely transparent to sound waves (Fig. 70.1) or be so reflective that only its proximal surface is visualized as a hyperechoic dome (Fig. 70.2). The differential diagnosis includes the arcuate arteries between the renal cortex and the medullary pyramids (bright echoes without acoustic shadows), vascular calcifications in diabetic patients, and calcified scarring secondary to renal tuberculosis. Papillary calcifications secondary to phenacetin abuse are a less common cause. Large staghorn calculi are difficult to diagnose if there is only weak distal acoustic shadowing because the large calculus can easily be mistaken for the hyperechoic renal pelvis. Renal concrements can dislodge and migrate into the ureter (Fig. 68.4). Depending on their size, they can pass into the bladder unnoticed or produce colicky pain
a
a
1 43/46
37
27
In addition to digital subtraction angiography (DSA), noninvasive color duplex sonography is useful for detecting renal artery stenosis. Visualizing and evaluating small accessory renal arteries is especially difficult. They can arise from the aorta in the immediate vicinity of the main renal artery, or they can arise from the aorta farther from it as upper or lower "polar arteries." In rare cases, they can also arise from the common iliac artery.
a
9
49 49
30
44
44
Fig. 70.1
35
b
5
29 31
29
35 13
45
Fig. 70.2
b
45
45
Nephrocalcinosis
9 71
45 31
45
45
Kidney stone
2
4
29
35 45
71
45
31
29
74
46
29
29
2
46
9
31 31
Circumscribed renal infarcts (71) have been observed as a result of a renal embolus from an aortic aneurysm (see p. 27) or renal artery stenosis. These infarcts conform to renal arterial territories and are broadbased at the renal surface and tapered toward the renal hilum. The result is a triangular defect (Fig. 70.3) in the renal parenchyma (29), which in the late stage progresses to a hyperechoic scar. The location and typical shape of these hyperechoic scars should prevent them from being confused with kidney stones or renal tumors.
4
45
49
Renal Infarcts
2
4
2
4
during their passage. They can also become lodged in the ureter and cause acute urinary obstruction. In addition to detecting urinary obstruction, the value of ultrasound lies in excluding other causes of pain such as pancreatitis or colitis as well as excluding free fluid in the pouch of Douglas (see p. 100).
47
Fig. 70.3
13 35
b
47
Renal infarct
25
Lesson 5
Renal and Adrenal Tumors
Benign Renal Tumors
Adrenal Tumors
Solid benign renal tumors (fibromas, adenomas, and hemangiomas) are altogether rare and show an inhomogeneous morphology on ultrasound images. Their internal echoes and lack of distal acoustic enhancement distinguish them from fluid-filled cysts. Only the angiomyolipoma – a benign mixed tumor comprising vessels, muscular tissue, and fat – has a characteristic appearance in its early stage that clearly distinguishes it from a malignant process. A small angiomyolipoma (72) is similarly hyperechoic and sharply demarcated as the renal pelvis (31) (Fig. 71.1). Its ultrasound morphology resembles that of a hepatic hemangioma (see p. 56). Angiomyolipomas only become inhomogeneous as their size increases; they then become difficult to differentiate from other types of tumors.
The left adrenal gland lies anteromedial (not cranial) to the upper pole of the left kidney. The right adrenal gland usually lies slightly cranial to the upper pole of the right kidney and posterior to the inferior vena cava. In adults, both adrenal glands are largely obscured by the hyperechoic perirenal and suprarenal fat capsule. This is not the case with the adrenal glands in newborns (see p. 140). Hormone-producing adrenal tumors such as adenomas in aldosteronism (Conn syndrome) or hyperplasia in the setting of Cushing's syndrome are generally too small to be detectable on ultrasound. Clinically apparent pheochromocytomas are the only such lesions that can usually be detected on ultrasound. By the time symptoms appear, these lesions will often have attained a size of several centimeters so that 90% of them are detectable on ultrasound. When in doubt, order a supplementary CT scan.
Malignant Renal Tumors Small renal cell carcinomas (54) are often isoechoic to the rest of the renal parenchyma (29). Only as their growth progresses do they become more inhomogeneous and can create a bulge in the contour of the kidney depending on their location (Fig. 71.2). If a carcinoma has been detected, both renal veins and the inferior vena cava must be carefully examined for tumor tissue to exclude vascular invasion. Renal carcinomas occasionally develop tumorous extensions into these vessels and occur bilaterally in up to 5% of all cases. If the tumor penetrates the renal capsule and infiltrates the surrounding tissue, the kidney can lose its physiologic mobility with respiration (see p. 65). Some malignant renal tumors can also contain cystic components. Therefore it is important to look for solid masses in the vicinity of what appear to be benign renal cysts.
a
a
1 2 47
46 30
74
74 43
Fig. 71.1
45 b
47
4
Angiomyolipoma
5 54
45
b
29
45 44
44
Renal cell carcinoma
54
47
Fig. 71.3
5
31
45
49
29
45
74 46
29
5
31
Fig. 71.2
13 37
30
31
2 4
4
72
29 45
a
1
2
4
Ultrasound is more helpful in detecting adrenal metastases (54), which usually appear as hypoechoic masses (Fig. 71.3) between the upper pole of the kidney and the spleen (37) or caudal margin of the liver, respectively. These lesions must be differentiated from superficial renal cysts. Because the adrenal glands are richly vascularized, hematogenous spread of metastases from carcinomas of the bronchus, breast, or kidney is common. The echogenicity of a suprarenal mass neither allows a conclusion as to whether it is benign or malignant, nor does it differentiate the mass from a neurinoma arising from a sympathetic ganglion.
13
b
45 44
35
Adrenal metastasis
71
72
Lesson 5
Renal Transplants Normal Findings Renal transplants are placed in the right or left renal fossa and connected to the iliac vessels. Like normal kidneys, they are systematically examined in two planes ( and in Fig. 72.1), the difference being that the transducer must be positioned over the lateral lower abdomen with patient supine. Because of the superficial position of the renal transplant not far beneath the skin, there is typically no interposed intestinal gas. This position greatly facilitates the ultrasound follow-up examination.
Fig. 72.1
a
Scanning procedure ...
b
... of renal transplants
A normal transplanted kidney can show a usually permanent volume increase of up to 20% postoperatively. The parenchyma (29) appears wider (Fig. 72.2) than in native kidneys. It is normal for the echogenicity of the parenchyma to be slightly greater than in native kidneys, increasing the contrast to the medullary pyramids (30). Ultrasound follow-up studies at close intervals are initially indicated to exclude progressive inflammatory infiltration. A prominent fluidfilled renal pelvis or slight first-degree urinary obstruction (see Figs. 68.1 and 68.2) is often observed, but without a functional impairment of the transplant that would justify intervention. The obstruction is best documented on the transverse image (Fig. 72.3) and carefully measured to avoid missing progressive obstruction that may require therapeutic intervention.
Early Detection of Rejection The renal transplant should be further evaluated for sharp demarcation against surrounding tissues and for a sharply demarcated border between the parenchyma (29) and renal pelvis (31). Blurring of the border between parenchyma and renal pelvis or an increase in volume since the previous examination can be warning signs of beginning rejection. Therefore, the longitudinal and transverse diameters are measured and documented to allow a valid comparison with subsequent studies (see p. 73). Doppler sonography is then used to determine the resistance index (RI) of the vessels in the transplant. This is an important indicator of the onset of rejection. In the ongoing absence of rejection, both the dosage of immunosuppressives and the frequency of ultrasound follow-up examinations can usually be reduced over time. 2
4
45
29 31 30
Fig. 72.2
a
b
Renal transplant in sagittal plane
28 29
c
1
2
4
46
29
25 31
45
Fig. 72.3
a
b
Renal transplant in transverse plane
c
30
74 46
29
Lesson 5
Renal Transplants
Determining the Size of a Renal Transplant
Lymphoceles
To obtain an accurate size measurement, first scan the transplant longitudinally ( Fig. 73.1b) until you have visualized its maximum length. The diagram in Fig. 73.1a illustrates how choosing an imaging plane too far lateral (black dotted line) would falsify the length measurement by making the kidney appear too short. The transducer must be tilted as indicated by the straight arrows ( ) to obtain the actual maximum length (dL). Then the transducer is rotated slightly (Fig. 73.1c) to make sure that the kidney has not been mistakenly visualized obliquely as indicated by the red dashed line ( in Fig. 73.1a). If necessary, the angle should be corrected as indicated by the curved arrow ( ) by rotating the transducer ( ). The purpose of this two-step manipulation of the transducer is to avoid errors that might cause you to document a foreshortened length. Such a measurement error could lead to subsequent misdiagnosis because the seemingly increased volume on follow-up images could suggest a rejection reaction.
A postoperative lymphocele (73) can develop as a complication of renal transplantation (Fig. 73.2). Lymphoceles usually occur between the lower pole of the renal transplant (29) and the bladder (38), although they are also observed elsewhere in the vicinity of the transplant. Not every lymphocele is an indication for intervention; small lymphoceles often resolve spontaneously. Large lymphoceles can occasionally be initially mistaken for the bladder at first glance.
29
Urinary Obstruction Urinary obstruction (87) is an equally common postoperative complication that can result from reimplantation of the ureter. Depending on its severity, it can require temporary placement of a catheter (59) to ensure drainage (Figs. 73.3 and 73.4) so as to prevent damage to the parenchyma (29) of the transplant.
31 29 30
Fig. 73.1
dL
a
c
b
a
a
a
2
4
2 4
46
31
70 29
Fig. 73.2
Lymphocele
59
44
45
b
29
31 59
73 87
Fig. 73.3
b
5
74
29
38
29
5
4
46
77 45
1 2
74 46
Urinary obstruction with ...
45 59
45
30 45
Fig. 73.4
74 46
87
29
b
... Drainage catheter
73
74
Lesson 5
Spleen Anatomy The spleen is loosely attached to the diaphragm (13) by the splenorenal ligament and lies in its bed relatively far posterior and lateral within the peritoneum; depending on its size, it may be in contact with the left lobe of the liver (9). It is supplied by the splenic artery (19), which arises from the celiac trunk (32) and follows a retroperitoneal course along the cranioposterior margin of the pancreas (33) to the hilum of the spleen (Fig. 74.1). The splenic vein (20) also follows a medial retroperitoneal course posterior to the pancreas and (here obscured by the head of the pancreas) joins the superior mesenteric vein (23) to form the portal vein (11). The stomach, air-filled small bowel loops (removed in this view), and the left colic flexure (43) all lie anterior
and caudal to the spleen. The acoustic shadow of this gastrointestinal air effectively prevents anterior or anterolateral visualization of the spleen on ultrasound. The only option is to visualize the organ from a posterolateral position or between two ribs (109) through an intercostal window as shown below. The spleen (37) also acts as an acoustic window to the tail of the pancreas (33c), which is often difficult to visualize in its entire extention from an anterior position because of overlying gastric air. The distal splenic artery (19) often branches into several individual arteries before entering the spleen. The same applies to the main branches of the splenic vein, which only merge into the main trunk of the splenic vein (20) at the hilum.
13 13 10
47
16 27
11 155
66 29
46
9
109
47
34 32a 19
32 18 33b
19
34 19
33c
20
33c 33a
2
37
37
43 46
43b 23
17
Fig. 74.1 View of the retroperitoneum
43c
Fig. 74.2 Intraperitoneal bed of the spleen
(Schuenke M, et al: THIEME Atlas of Anatomy–Internal Organs, 3 ed. Stuttgart: Thieme, 2020. Illustrations by M. Voll, K. Wesker.) rd
The key to the other numbers may be found in the legend on the back cover flap.
Examination Technique The spleen is primarily visualized with the patient supine. It is best to have the responsive patient lie close to the left edge of the examining table and place the left arm behind the head (Fig. 74.3). This widens the intercostal spaces and facilitates applying the transducer parallel to one of them from a posterolateral position (see Video clip 5.3b). The examiner should stand up or sit on the right edge of the examining table to be able to reach the patient's posterior axillary line. The examination is performed in expiration (see Video clip 5.3c) to prevent the lung (47) from expanding caudally and obscuring the spleen (37) with an acoustic shadow (45) (see Figs. 75.1b and c). Alternatively, one can perform the examination with the patient in the right lateral decubitus position (see Fig. 75.1a). However, especially in older patients this is more time consuming, and gravity causes the spleen to lie at an unfavorable distance from the posterolateral chest wall.
Fig. 74.3 Posterolaterally from the posterior axillary line
Lesson 5
Spleen
Spleen Size The normal adult spleen measures about 4 cm x 7 cm x 11 cm (the "4711 rule"), whereby the longitudinal dimension (L) can be as much as 13 cm (instead of 11 cm) without any clinical significance, for instance in patients who have had infectious mononucleosis. The thickness or
diameter (D, measured from the hilum to the diaphragmatic capsule of the spleen) provides more information: If it exceeds 6 cm (instead of 4 or 5 cm), additional tests are indicated to exclude a lymphatic disorder, unless venous congestion is present due to portal hypertension. 4 47 x
x
L
D 37
45
x
43 45
20
74
19
33
13 47
Fig. 75.1
a
Lateral visualization of the spleen
a
1/2
b
Normal findings
a 2
43 37
47
43
5
20 37
20 45
5
74 26
47
Fig. 75.2
13
b
Measuring spleen size
Curtain Trick
4
47
c
26
x
45
45
20
45
26
45
Without curtain trick
13
Fig. 75.3
b
74
With curtain trick
Splenomegaly Acute viral infections are the most common cause of diffuse, homogeneous enlargement of the spleen. In the case of infection with Epstein-Barr virus (infectious mononucleosis), the disease can resolve and leave behind slight to moderate splenomegaly with rounded poles. This often persists for life but has no clinical significance. An important differential diagnosis to consider is portal hypertension in which the branches of the splenic vein (20) are dilated (Fig. 75.4).
In some patients, the cranial spleen (37) is obscured by acoustic shadows (45), either spontaneously or after deep inspiration where the lung (47) extends too far into the costodiaphragmatic recess (Fig. 75.2). In such cases, one can take advantage of the fact that the spleen will often return to its cranial position more slowly than the lung during slow expiration following maximum inspiration. This relative motion makes the acoustic shadow recede like a "curtain" (see Video clip 5.3c). The examiner must wait for the right moment and then tell the patient to immediately hold his or her breath. This maneuver often succeeds in visualizing the regions of the spleen immediately beneath the diaphragm (along the left edge of the image in Fig. 75.3). The lower pole of the spleen is occasionally obscured by acoustic shadows behind bowel loops (43). 2
5 47
4 46
37 20
45 20
20
26
46
33 45
74
13
Fig. 75.4
a
Splenomegaly ...
b
... in portal hypertension
45
75
76
Lesson 5
Spleen Splenomegaly in Leukemia
Splenic Infarcts
Splenomegaly typically accompanies systemic hematologic diseases, such as acute or chronic lymphatic leukemia (CLL). Fig. 76.1 shows a spleen in a leukemia patient with an adjacent accessory spleen (86) and the tail of the pancreas (33c) close to the splenic hilum. In principle, any disorder involving increased turnover of erythrocytes, such as a hemolytic anemia or polycythemia vera, can cause splenomegaly. In such cases the spleen may be grossly enlarged, even extending into the pelvis (Fig. 76.2), and may exhibit focal infarcts (Fig. 76.3). The "kissing phenomenon" may also be observed, in which the massively enlarged spleen displaces the stomach and extends as far as the left lobe of the liver. When evaluating the spleen, it is important to be alert to any signs of thickening. The original crescentic or half moon shape with tapered poles is lost, and the poles appear rounded or thickened (Fig. 76.1). Ectopic splenic tissue in the vicinity of the bed of the spleen, which is occasionally present as a remnant of embryonic development, can also become hypertrophic when stimulated. Consequently, "accessory spleens" (86) at the hilum (Fig. 76.1) or lower splenic pole are not uncommon in diffuse splenomegaly. They have the same echogenicity as the rest of the splenic parenchyma (37) and are sharply demarcated. However, they can be difficult to differentiate from enlarged lymph nodes (55) as illustrated in Fig. 76.2.
Focal infarcts (71) are especially likely to occur in the setting of rapidly progressive splenomegaly. Early-stage infarcts appear as hypoechoic areas within perfused hyperechoic areas (Fig. 76.3). Supplemental color duplex sonography can establish the status of splenic perfusion quickly and noninvasively.
2
47
Neither size nor echogenicity of the enlarged spleen reveals the nature of the underlying disease. If you unexpectedly detect splenomegaly, you should examine all accessible nodal groups (para-aortic, portal, parailiac, and cervical nodes) for enlargement suggestive of a systemic hematologic disorder. You should also exclude portal hypertension by measuring the diameter of the splenic vein (normal value < 12 mm), portal vein (< 15 mm), and superior mesenteric vein, and by searching for portocaval anastomoses at the porta hepatis. Spleen size should be documented as accurately as possible to allow follow-up examinations to determine whether size has increased or decreased, such as can occur after resolution of a viral infection or secondary to chemotherapy in the interim, depending on the underlying disease. Keep this in mind when you perform the initial examination.
1
2
4
Practical Suggestion
1/5
4
2
43 5
37
37 86
47
55 / 86
45
47
13
Fig. 76.1
20
33 c
37
13
45
b
4
Accessory spleen
Fig. 76.2
b
71
71
55 / 86
37 37
45
20
45
Splenomegaly
Fig. 76.3
b
Splenic Infarcts
Lesson 5
Spleen
Lymphomatous Infiltration
Hyperechoic Lesions
Non-Hodgkin lymphoma can present with an isolated hypoechoic splenic lesion or there may be inhomogeneous involvement of the entire spleen. An enlarged spleen that appears homogeneous on conventional ultrasound scans can nevertheless contain lymphomatous focal lesions that escape detection. The detection rate has increased markedly with the introduction of contrast agents used in combination with harmonic imaging (see p. 14).
Spherical and homogeneous hyperechoic lesions that are sharply demarcated from the splenic parenchyma generally represent benign splenic hemangiomas, with features identical to those of hepatic hemangiomas (see p. 56). Such findings may also represent hyperechoic calcifications secondary to tuberculosis infection or cirrhosis of the liver. Multiple hyperechoic focal lesions (53) give the spleen the appearance of a "starry sky" (Fig. 77.3). Such lesions also occur as postinfectious scarring. Splenic abscesses and the less common splenic metastases can exhibit a rather varied ultrasound morphology, depending on age and immune status. Unfortunately there are no simple, reliable ultrasound criteria for differential diagnosis.
Splenic Hematomas Definitive exclusion of splenic hematomas is of utmost importance in trauma patients as an acute hemorrhage may initially be contained within the splenic capsule (intracapsular or subcapsular injury). The splenic capsule may rupture only after some delay (in about 50% of all cases within the first week), precipitating a lifethreatening hemorrhage into the abdominal cavity (delayed splenic rupture). Therefore, one must carefully exclude a hypoechoic lesion or delicate hypoechoic double contour of the splenic capsule. Some splenic hematomas (50) are also inhomogeneous (Fig. 77.1) or isoechoic to the surrounding splenic parenchyma (37). The two ( ) in Fig. 77.1 indicate the sites where you should search for anechoic intraabdominal fluid (indicative of hemorrhage). These sites are along the abdominal aspect of the diaphragm (13) posterior to the upper pole of the spleen and in the vicinity of the lower pole of the spleen (Fig. 77.2).
Splenic Cysts Congenital splenic cysts are anechoic and less common than hepatic cysts. Their ultrasound morphology does not differ from hepatic cysts (see p. 55). Acquired Fig. 77.4 Echinococcus splenic cysts develop secondary to trauma or infarction, or in the setting of parasitic infestation. Fig.77.4 shows a CT scan with cysts containing obvious radial septa ( ) in the setting of echinococcosis of the liver and spleen.
68 37
29
1
2
47
47
5
13
68
37
50 20
45
Fig. 77.1
b
45
13
Contained splenic hematoma
45
47
Fig. 77.2
b
Bleeding into abdominal cavity
43
45
37 20
29 13
2 37
46
37
45
5
47
43
37
50
1
116
20
37
Fig. 77.3
b
"Starry sky" spleen
45
77
78
Lesson 5
Quiz These study questions are intended to help you to test your knowledge so you can clear up any comprehension problems or close any gaps before you move on to the next organ system.
Pursued with a little determination, you will find the quiz rather enjoyable. You will find the answers on the preceding pages (questions 1-4 and 7-8) or on page 157 (images 5, 6, and 10).
1.
From memory, draw a typical longitudinal section of the right kidney, paying attention to the position of the medullary pyramids relative to the border between the parenchyma and renal pelvis (maximum 2 minutes). Repeat this task for a transverse section of the right kidney at the level of its hilum, and consider its position relative to the liver and the inferior vena cava. Repeat both tasks (important: at intervals of more than 2 hours) until you are able to complete them without any errors.
7.
Write down the normal size measurements of the spleen in adults, and put the significance of splenomegaly in perspective.
8.
What trick do you know to visualize the subdiaphragmatic portions of the spleen when you encounter superimposed pulmonary air? How does it work?
9.
You unexpectedly discover splenomegaly. How do you proceed?
2.
Make a rough sketch showing the different forms of the normal kidney compared with the respective findings in first through third-degree urinary obstruction. Discuss the differentiating criteria with a fellow student. Validate your sketches by comparing them with the images on pages 68-69.
10. Systematically
3.
How do you recognize nephrolithiasis? List a few possible underlying disorders that can cause kidney stones. With the help of other sources from the literature, provide a differential diagnosis of hematuria (evidence of blood in the urine).
4.
Do you remember the normal values for kidney size, the parenchyma to pelvis (PP) index, and the degrees of urinary obstruction in adults? Write down your values and compare them with those listed on pages 65 and 68.
5.
evaluate the image in Fig. 78.4. Proceed in the order recommended in the primer on ultrasound on page 144 to give your thoughts proper direction.
Carefully examine the two ultrasound images in 78.1 and 78.2 and write down the imaging planes; all visualized organs, vessels, and muscles; and of course your working diagnosis and your reasoning behind it. Fig. 78.1
6.
Fig. 78.4
Fig. 78.2
This image (Fig. 78.3) shows a transverse section of the upper abdomen at the level of the renal vessels. Describe the organs and vessels you can recognize. Which vessel is atypical in its course and what conclusion do you draw from that?
Fig. 78.3
Lesson 6 Thyroid Gland, Lymph Nodes, Gastrointestinal Tract
Thyroid Gland: Anatomy
80
Normal Findings
81
Goiter
82
Focal Solid Nodules, Thyroiditis
83
Lymph Nodes: Cervical Lymph Nodes
84
Differential Diagnosis riteria, Perfusion Parameters
85
Enlargement, Metastases
86
Retroperitoneal Lymph Nodes
87
Gastrointestinal Tract:
With gastrointestinal images from Matthias Hofer and Alexis Müller-Marbach
Anatomy
88
Gastric Tumors
89
Crohn's disease
90
Intestinal Intussusception, Hernias
91
Differential Diagnosis of Diarrhea, Appendicitis
92
ural
ic ening,
Fecal Impaction, Colitis, Colon Carcinoma
93
Diverticulitis
94
Quiz
95
80
Lesson 6
Thyroid Gland Anatomy of the Thyroid Gland The isthmus of the thyroid (81a) lies directly posterior to the sternohyoid muscle (89) and sternothyroid muscle (90), anterior and lateral to the trachea (84). The common carotid artery (83) courses posterolateral to the lateral lobes of the thyroid (81) and the internal jugular vein (83) is further lateral. The vagus nerve (169) courses between these two vessels (Figs. 80.1 and 80.2).
169
83
The esophagus (34) lies posterior to the trachea, often slightly offset in a left paramedian location, anterior to the anterior and middle scalene muscles (88) and the cervical vertebrae (35). The sternocleidomastoid muscle (85) forms an anterolateral shield overlying the cervical neurovascular bundle. The key to the other numbers may be found in the legend on the back cover flap.
82b
1
2 81a
85
88
83
81a 82
123 84
90
84
81
82
88
83
Platysma
89
81
83
34 88
35
85
88 169
16a 83 Fig. 80.1 Anterior view of the neck
Fig. 80.2 Transverse section at the level of the thyroid
(Schuenke M, et al: THIEME Atlas of Anatomy–Head, Neck, and Neuroanatomy, 3rd ed. Stuttgart: Thieme, 2020. Illustrations by M. Voll, K. Wesker.)
Volumetric Measurements To determine the volume of the thyroid gland, the maximum transverse and sagittal (anteroposterior) diameters of each lobe are measured on transverse sections. The respective values are multiplied by the craniocaudal length as measured on the sagittal section and the product is multiplied by 0.5. The result corresponds to the volume of each lateral lobe (in mL), with a margin of error of approximately 10%. The volume of both lobes should be < 25 mL in men and < 18 mL in women.
When evaluating the volume of the thyroid, one should take into account that Germany, in contrast to most of its European neighbors, does not iodize drinking water and is thus among the few remaining iodine-deficient regions. Whereas the statistical average values of the German population are "normal" values in the statistical sense, they do not reflect the normal physiologic case.
Normal Thyroid Volume Values The volume of the thyroid gland in girls younger than 15 years old is slightly higher than the volume in boys. To properly answer the question of whether iodine prophylaxis is indicated, the upper threshold values in milliliters are specified here for both iodine deficiency (black numbers) and for iodine sufficiency (white numbers in Table 80.3). Age Female Male The white numbers in parentheses specify the normal Newborns < 2.3 (1.5) < 3.5 (2.0) values for children in Europe who do not live under conditions of iodine deficiency. The respective highest < 4.7 (3.0) < 3.8 (2.9) 1– 4 years volume of both thyroid lobes together that is still 5–10 years < 6.5 (5.0) < 6.0 (5.4) regarded as normal is specified here as determined by 11–12 years < 1.6 (14.1) < 13.9 (13.2) the volume formula 0.5 x A x B x C. The average volumes are often considerably lower. Adults < 18.0 < 25.0 Table 80.3
Lesson 6
Thyroid Gland
Normal Findings The patient's head is placed in slight hyperextension and thyroid gland is examined using a linear transducer with 7.5 or more MHz (Fig. 81.1a). The organ is scanned in successive transverse planes beginning cranially and moving caudally (see Video clips 6.1a–c). Next, sagittal images are obtained through each thyroid lobe (Fig. 81.1b). The midline acoustic shadow of the trachea (84) and, farther laterally, the anechoic cross sections of the carotid artery (82) and jugular vein (83) provide anatomic landmarks. The thyroid parenchyma (81) lies between these vessels and the trachea (Fig. 81.1c). A thin parenchymal band (isthmus) anterior to the trachea connects the two lobes of the thyroid (Fig. 81.2). The carotid
artery (82) usually lies in a posteromedial location, and is round and incompressible in the transverse plane. The jugular vein (83) is farther anterolateral. It exhibits a typical biphasic venous pulse and is compressible when gentle pressure is applied to the transducer. When in doubt about the identity of any of the vascular structures, the examiner can ask the patient to briefly press with the mouth closed. The resulting venous congestion distends the jugular vein, which usually provides a clear anatomic landmark. The normal thyroid parenchyma is slightly more hyperechoic (brighter) than the sternohyoid (89) and sternothyroid (90) muscles anterior to it and the sternocleidomastoid (85) muscle farther lateral (Fig. 81.2).
81
Fig. 81.1
a
b
c
5
2
81 83
89/90
90 /89
85
81
51 84
82
82 34
88
Fig. 81.2
a
b
Small cysts (64) in the thyroid gland (81) may not cause any distal acoustic enhancement (Fig. 81.3b) and must
be differentiated from hypoechoic nodules and obliquely visualized vessels.
1/2 85
81
a
b
35
c
5
Fig. 81.3
88
45
35
64
35
35
35
35
45
45
45
45
c
81
82
Lesson 6
Thyroid Gland: Pathologic Examples Goiter
(64 in Fig. 82.3). With progressive degeneration, these anechoic cysts can reach a considerable size (Fig. 82.5) and can also show central hyperechoic hemorrhages ( ) (Fig. 82.6).
In regions with insufficient dietary intake of iodine, the most common diffuse thyroid disorder is iodine deficiency goiter, i.e., diffuse enlargement of the thyroid gland. Compared with their normal appearance (Fig. 82.1), both lobes of the thyroid are enlarged and thickened (Fig. 82.2), often with a thickened isthmus as well. The iodine deficiency frequently leads to isoechoic nodules ( ) within the goiter. Where they occur peripherally, they can cause protrusion of the organ surface (Fig. 82.4). In chronic iodine deficiency, these nodules (54) will often develop regressive calcifications or cysts
1/5
5
2
81
81
51 84
82 88
45
35
Fig. 82.1
b
Normal findings
Fig. 82.4 Thyroid nodules
64 81
54
82
82
88
84
81
82 34
51
81
84
81
34
88 35
35
Fig. 82.2
b
Goiter
Fig. 82.5 Cyst ...
88
82 88
88
45
85
90
90
90
90
85
83
Malignant degeneration of hyperechoic or isoechoic nodules is so rare (less than 1%) that it lies below the normal malignancy rate of the German population. Hypoechoic thyroid nodules behave differently (see next page).
35
45 45
Fig. 82.3
b
35 45
Thyroid nodules
Fig. 82.6 ... with hemorrhage
83
Lesson 6
Thyroid Gland: Pathologic Examples
Focal Solid Nodules The differential diagnosis of hypoechoic focal thyroid lesions includes degenerative nodules with small cysts and benign adenoma, but also thyroid carcinoma. Hypoechoic nodules therefore require supplementary scintigraphy. "Hot" nodules on a scintigram are hormone-producing adenomas (72) and frequently appear on ultrasound scans with a hypoechoic rim within normal thyroid parenchyma (81 in Fig. 83.1). In contrast to the typical ultrasound morphology of hepatic metastases (see p. 60), a hypoechoic rim (halo) in the thyroid gland does not suggest malignancy. "Cold" nodules on a scintigram that are hypoechoic (54) require further evaluation (needle aspiration for cytology or biopsy) to exclude malignancy (Fig. 83.2).
a
a
5 72
72 81
54
84
45
Fig. 83.2
b
90
81
82
45
Fig. 83.1
5
85
b
Thyroiditis In florid Graves' disease diffuse hypervascularization is nearly pathognomonic (Fig. 83.3). The systolic peak speeds exceed 100 cm/sec on average with flow volumes per minute over 150 mL/min. The hyperperfusion will initially persist for some time even after medical therapy with normal thyroid metabolism; it only decreases later in the course of the disorder. Although hyperperfusion in Hashimoto thyroiditis (Fig. 83.4) shows a
85
85
82
a
Fig. 83.3
Graves' disease
81
81
a
b
85
89 / 90
83 81
similar picture, it is less pronounced than in florid Graves' disease. Chronic lymphocytic infiltration typically produces a permanent diffuse hypoechoic appearance in the otherwise hyperechoic thyroid parenchyma. In de Quervain's thyroiditis the inflammation does not usually involve the entire thyroid gland diffusely but infiltrates the organ unevenly, creating inhomogeneous hypoechoic areas of edema (Fig. 83.5).
Fig. 83.4
82 a
b
Hashimoto thyroiditis
Fig. 83.5
b
de quervain's thyroiditis
83
84
Lesson 6
Lymph Nodes Cervical Lymph Nodes Enlarged lymph nodes (55) appear as oval hypoechoic masses and are often located in vicinity of the cervical neurovascular bundle (Fig. 84.1) along the internal jugular vein (83) and carotid artery (82), but also in the submental region. Physiologic lymph nodes that show reactive enlargement in the setting of viral or bacterial infection are usually elongated, with a ratio of maxi-
mum longitudinal diameter to maximum transverse diameter (L/T ratio) of over 2.0. They can also appear in groups (Fig. 84.2). A lymph node exhibiting an L/T ratio over 2 with a central hyperechoic hilum ( in Fig. 84.3) and a prominent hilar vascular pattern (see pp. 85-86) can be evaluated as benign [6.1].
5
85 89
83
82
85
85
81
55
84
55
55 55
55
55
55
55
45
Fig. 84.1
45
45
Fig. 84.2
b
35
83
35
Fig. 84.3
b
In contrast, thickened, spherical lymph nodes with an L/T ratio around 1.0 without a hilum sign are suspicious for pathologic enlargement due to a process such as lymphoma or metastasis, which can occasionally show central necrosis ( in Fig. 84.4). Infants tend to develop more severe nodal swelling than adults even in the setting of secondary inflammatory reactions. Occasionally they even develop abscesses with liquefaction in the affected lymph nodes, which can also appear as anechoic areas. Infraclavicular lymph nodes can also be readily demonstrated on ultrasound, for example in sarcoidosis as shown in Fig. 84.5. When in doubt, additional criteria for differential diagnosis can be applied. These include visualizing the branching pattern of the intranodal blood vessels on color duplex sonography, determining the pulsatility index (PI) or resistance index (RI) at that site, and quantifying tissue elasticity, "elastography." You will find examples of each on the next few pages. Criteria
Benign
Malignant
Ratio length / width Hilum sign Vascularization
> 2.0 Positive Centered in the hilum
~ 1.0 Negative Diffuse or branch
Table 84.1 Benign vs. malignant lymph nodes
55
Fig. 84.4
Fig. 84.5
b
Lesson 6
Lymph Nodes
Differential Diagnostic Criteria The L/T ratio described on the previous page can only be correctly calculated when you rotate the transducer 180° around the axis of its cord over the center of the lymph node. A lymph node that appears to have a low L/T ratio (Fig. 85.1) may then show an oval L/T ratio of 3.0 as the visualization more closely approaches as its "true" diameter (Fig. 85.2). Although its hilar architecture is preserved ( ) there may indeed be metastatic infiltration ( ) in such an elongated lymph node (Fig. 85.2). Especially when higher center frequencies over 10 MHz are used,
it is occasionally possible to demonstrate multiple metastases in a single lymph node ( in Fig. 85.3). As the metastasis grows, the L/T ratio approaches the value for a sphere (1.0) (Fig. 85.4). However, lymphomas in particular usually respect the capsule and tend to grow and displace tissue only within the affected lymph node (Fig. 85.5). In contrast, advanced metastases later infiltrate the capsule ( ) and can then spread to surrounding tissue (Fig. 85.6).
Fig. 85.1 Cross section of lymph node
Fig. 85.2 Lymph node with a small metastasis
Fig. 85.3 Two metastases in one node
Fig. 85.4 Spherical shape of lymph node metastasis
Fig. 85.5 Lymphomas with intact capsule
Fig. 85.6 Metastasis infiltrating capsule
Fig. 85.7 Reactive inflammatory lymph node with PI = 1.37, RI = 0.73
Fig. 85.8 Malignant lymph node with PI = 2.27, RI = 0.92
Perfusion Parameters Where perfusing vessels can be measured within the lymph node, PI values < 1.6–1.8 and RI values < 0.8–0.9 suggest a benign process (Fig. 85.7), whereas PI and RI values above this gray area are more typical of malignancy (Fig. 85.8). However, these are not absolute threshold values but approximate values.
85
86
Lesson 6
Lymph Nodes Differential Diagnostic Criteria The fact that a lymph node is primarily sharply demarcated is no guarantee that it is benign. Nor does the echogenicity of a lymph node reliably identify it as malignant or benign, even though lymphomas often appear homogeneously hypoechoic (relative to adjacent muscle) and exhibit an L/T ratio of about 1 (spherical) (Fig. 86.1). In contrast, the metastases of a
Abb. 86.1 Homogeneously hypoechoic lymphoma
malignant melanoma are almost invariably highly hypoechoic (Fig. 86.2). The intranodal perfusion pattern on color duplex sonography [6.1] is another differentiating criterion. An node infiltrated by lymphoma typically exhibits a tree-like perfusion pattern (Fig. 86.3) that can often be traced into the periphery.
Abb. 86.2 Hypoechoic metastasis of a melanoma
Abb. 86.3 Tree-like perfusion in lymphomas
Fig. 86.4 Positive hilum sign
Fig. 86.5 Central perfusion in a lymph node
Reactive Inflammatory Lymph Node Enlargement In contrast, benign lymph nodes usually exhibit intact hilar architecture ( in Fig. 86.4) and a central pattern of perfusion that cannot be traced into the periphery (Fig. 86.5).
Lymph Node Metastases Lymph node metastases on the other hand typically exhibit an irregular perfusion pattern that can be traced into the periphery of the node (Fig. 86.6). Findings may also include central liquefaction as in Fig. 86.7. On elastography the malignant lymph nodes usually show stiffer (higher) values (here encoded in red) > 2 (Fig. 86.8) compared with the reactive inflammatory lymph nodes, although the accuracy of this method is still limited (depending on the examiner's experience, sensitivity is only about 62% and specificity is about 84% [6.1]).
Abb. 86.6 Malignant nodal metastasis
Abb. 86.7 Nodal metastasis with central necrosis
Abb. 86.8 Elastography with nodal metastasis
Lesson 6
Lymph Nodes
Retroperitoneal Lymph Nodes On the last few pages, the shape of the lymph node (ratio of maximum longitudinal diameter to maximum transverse diameter or L/T ratio) and the hilum sign (see p. 84) have been described as evaluation criteria as have a few supplementary criteria on color duplex sonography (pulsatility index or PI, perfusion pattern, and elastography) (see pp. 85–86). Retroperitoneal lymph nodes (55) often lie at a greater depth and adjacent to numerous other neurovascular structures. The decreased spatial resolution at center frequencies around 3.5 MHz makes it easier to miss them or mistake them for obliquely visualized blood vessels. At the hilum of the liver, for example, overlying intestinal gas or obesity can create local conditions not conducive to ultrasound. In such cases there is a risk of confusing sections of the hepatic artery (18) with preportal lymph nodes (55) anterior to the portal vein (11) as in Fig. 87.1. A proven technique in such cases is to carefully and systematically scan the porta hepatis, continuously sweeping in only one direction. With this manual technique, local blood vessels will either continuously decrease in caliber or increase as they merge with other vessels, whereas lymph nodes will suddenly appear and equally suddenly disappear. This helpful diagnostic distinction will be lost if the examiner simply sweeps the transducer back and forth more or less randomly. When examining lymph nodes at the root of the mesentery, distinguishing isolated enlarged lymph nodes (55) from obliquely visualized small bowel loops (46) can require the examiner's full concentration as the bowel loops can also be hypoechoic and exhibit a similar oval shape (Fig. 87.2). Where numerous lymph nodes (55) form a conglomerate as in Fig. 87.3, it helps to be a little patient so that peristalsis in the bowel loops can be used as an additional differentiating criterion. The same applies to differentiating bowel loops from lymph nodes in the vicinity of the iliac vessels (21) in the lower abdomen (Fig. 87.4).
1 3 55 55 74
55 46
55
2
55 55 74 46 55
55
55 55 55 55 46 55
35 45
Fig. 87.2
b
35
11
11
18
5
45
9
Fig. 87.1
b
Periportal lymph nodes
45
4
55
46
45
55
45
16
Lymph node conglomerate
21
46 45
45
b
4
5
55
46
55 74
55
Fig. 87.3
2
46
55 55
53
55
8
11
33
55
46
45
Mesenteric lymph nodes
9
74
46
74
45
5
5
1
2
16
15 45
74
3
1
3
3
1 2
45
Fig. 87.4
b
Para-iliac lymph nodes
87
88
Lesson 6
Gastrointestinal Tract Anatomy of the Gastrointestinal Tract The anterior wall of the stomach (26) lies against the posterior wall of the left lobe of the liver (9), and its posterior wall is in contact with the body (33b) and tail of the pancreas. The spleen (37) lies to the left of and lateral to the stomach, and the transverse colon (43b) with the greater omentum lies caudal to it. Along its lesser curvature courses the left gastric artery (32a) arising from the celiac trunk (32), and the splenic artery (19) courses posterior to the stomach along the cranial margin of the pancreas. Just caudal to the lesser omentum with the hepatic artery (18), portal vein (11), and common bile duct (66), the antrum of the stomach joins the duodenum (46), which surrounds the head of the pancreas (33a) in the shape of a C. The other numbers may be found on the back cover flap of this book.
9
9 14
37
26
18
11
15
16 66
32a 32
19
33b 43
43
46
33a
43b
Fig. 88.1 (Schuenke M, et al: THIEME Atlas of Anatomy–Internal Organs, 3rd ed. Stuttgart: Thieme, 2020. Illustrations by M. Voll, K. Wesker.)
Layers of the Stomach Wall The normal wall structure of the gastrointestinal (GI) tract consists of five layers, which appear alternatively hyperechoic and hypoechoic (Fig. 88.3). From the inside out, these are the hyperechoic margin of the mucosa (74a), the very thin hypoechoic muscularis mucosae (74b), the hyperechoic submucosa (74c), the thicker hypoechoic tunica muscularis (74d), and the hyperechoic serosa (74e). However, this outermost layer appears to merge with the hyperechoic capsule of the liver (Fig. 88.2) on ultrasound. The posterior serosa
cannot always be clearly distinguished from the adjacent pancreas (33) in the presence of lipomatosis (see p. 34). Depending on its degree of contraction, the entire thickness of the stomach wall varies between 5 and 7 mm. The hypoechoic tunica muscularis (74d) alone should be under 5 mm unless it is visualized in the middle of a peristaltic wave (Fig. 88.4). Occasionally gastric air (47) creates acoustic shadows (45) that obscure the view of the posterior wall of the stomach. 2
3
3
5 9
74d
8
74b
74e
9
47
74c
26
46
33c
33a
20
74
45
16
17
15 35
Fig. 88.2
a
Transducer position for the stomach
b
Layers of the stomach wall
c
26
74 a b c d
1
2
3
3 7 46
9
5
74d
e
74 16
9
Fig. 88.3
a
Alternating echogenicity
Fig. 88.4
a
Cross section of the pylorus ...
b
... in a peristaltic wave
45
45
Lesson 6
Gastrointestinal Tract
Gastric Tumors gastric emptying (Fig. 89.2). In the example shown here, the delayed gastric emptying was caused by a large mural tumor (54) that had obliterated the normal layers of the stomach wall ( ) over a distance of several centimeters ( ) and expanded from the wall into the lumen like a polyp.
A gastric carcinoma (54) initially develops as a focal lesion at one location on the stomach wall (74), where it can cause circumscribed thickening of the wall (Fig. 89.1) and obliterate the normal layering of the stomach wall (see previous page). A dilated lumen (26) can be an indirect sign of a tumor-induced delay in
74
Fig. 89.3 CT in lymphoma 3
3 9
13
2 3 54/ 74 74a
2
5 26
74
46/5
26
9
54
45
31
45
47
Fig. 89.1
29
45
b
70
Fig. 89.2
Antral carcinoma
Since gastric air often prevents complete visualization of the posterior wall of the stomach on ultrasound images, modalities such as endoscopic ultrasound or diagnostic CT are frequently applied. Here, the transmural thickening of the wall involving the entire circumference of the stomach that typically occurs in lymphomatous infiltration is more clearly visualized (Fig. 89.3). CT also allows precise evaluation of whether the tumor has infiltrated adjacent organs and regional lymph nodes regardless of the gas content of the gastrointestinal tract. However, histologic determination of the type of tumor requires gastroscopy. Finally, a radiologic double contrast transit study is indicated. This study allows the examiner
to search the mucosal folds for atypical lesions, rigid segments, and ulcer craters (Fig. 89.4). Quiz: Can you tell how this patient with normal findings was positioned? Supine, left or right lateral decubitus, or head-down position? (Answer: see p. 158). As in lymphoma, portal hypertension (see p.42) can be accompanied by circumferential thickening of the entire wall of the stomach (74). Color duplex sonography often shows a radial pattern of increased vascularity (Fig. 89.5) and the other signs of cirrhosis of the liver (see p. 58).
2
1 3
5
74
Wall thickening ...
b
74
26
45
a
3
43 b
9
Fig 89.5
Fig. 89.4 Normal transit study
Delayed gastric emptying
b
... in portal hypertension
45
c
Radial vessels on color duplex sonography
89
90
Lesson 6
Gastrointestinal Tract Crohn's disease Normally the bowel walls are so thin that they are barely visualized. However, in inflammatory bowel disorders, the layers of the bowel wall (74) are markedly thickened and the lumen is constricted as can occur in patients with Crohn's disease (Fig. 90.1). A vanced cases can show such massive mural thickening (Fig. 90.2) that the process can be misinterpreted as a tumor (see p. 93) or
2
1
3 74
5
74
intussusception of the bowel (see p. 91) . Where the mural thickening is due to inflammation (Fig. 90.3a), using color coding in the affected segments can demonstrate significant hyperperfusion of the wall (Fig. 90.3b) as in this patient with sigmoiditis in the setting of Crohn's disease.
Fig. 90.3
1
3
74 46
46
4
4 5
2
46
74 46
45
74
45 45
70
35
45
Fig. 90.1
Plain scan
b
Mural thickening in crohn's disease
Fig. 90.2
45
b
Bull's-eye sign in crohn's disease
One of the most common complications in this clinical picture is the development of fistulas, abnormal passages through which the inflammatory bowel segment communicates either with other adjacent organs (such as the bladder or adjacent bowel loops) or with the skin as in Fig. 90.4. Here, in the left lower
Fig. 90.3
b
Hyperperfusion in sigmoiditis
abdomen a bowel segment (43) in the vicinity has become inflamed, leading to development of a colocutaneous fistula and thickening of the bowel wall (74). The lumen of the fistula ( ) was precisely visualized on contrast-enhanced ultrasound (Fig. 90.4b).
1/2 46
3
3
43
74 43
Fig. 90.4
a
Noncontrasted image of colocutaneous fistula
b
Lumen of the fistula on contrast-enhanced ultrasound
c
d
74 43
74
43 45
Lesson 6
Gastrointestinal Tract
Intestinal Intussusception Intussusception most commonly occurs in infants between the ages of 6 and 9 months. Boys are affected more often than girls. The rule of thumb is that intussusception very rarely occurs before the age of 3 months and after the age of 3 years and thus is rather unlikely. Typical symptoms include episodic pain of sudden onset interspersed with asymptomatic or minimally symptomatic intervals. Usually the terminal ileum at the cecal pole displaces into the colon through the ileocecal valve, creating a ring-like intestinal wall within the lumen of
a
74
a
4 74
74d 46
74
a
1/2
46 9
the colon (Figs. 91.1 and 91.2). Less often, intussusception occurs in the jejunum as well. The result is an outer hypoechoic muscular layer (74d) separated from the inner invaginated muscularis by the hyperechoic mucosa (74b). Visualized end on, this produces what is known as a "target sign" or "bull's-eye sign". Occasionally two hyperechoic mucosa layers (74b) of both bowel segments are detectable (Fig. 91.2). Fig. 91.3 shows the appearance of intussusception (74) on CT, seen here next to fluid-filled colonic segments (43).
74
74 74
74b
16 15 43
43
46
74
74
9
35 29
43 45
Fig. 91.1
45 b
"Target sign" in ...
45
46
Fig. 91.2
b
45
74
43 43 29
46
... intestinal intussusception
Fig. 91.3
b
Intussusception on CT
Hernias Protrusion of a bowel loop (46) through the anterior abdominal fascia (6) is observed particularly around the umbilicus (Fig. 91.4) and along the linea alba. The width of the hernia ( ) is of particular importance to the risk of incarceration; where the hernia is wider, there is less of a risk of impingement of the blood vessels supplying the herniated bowel 46 / 120 74 segment (120). One should be alert to any ischemic thickening of the herniated bowel 6 74 45 6 wall (74) as it is an indirect sign of hypoperfusion (not present in the example shown). Fig. 91.4
a
Umbilical hernia
b
Contrast Enema Where intussusception has been confirmed by one of the two methods mentioned, an immediate attempt should be made to reduce the intussuscepted bowel segment ( ) by means of a retrograde contrast enema (Fig. 91.5). This is necessary in order to promptly prevent or resolve compression of the vessels of the involved mesenteric root. In this example, the small bowel was intussuscepted as far as the mid and transverse colon. Ideally, the hydrostatic pressure of the retrograde injection of contrast medium completely pushes back the intussuscepted intestinal segment, so the child is spared a surgical intervention. The ultrasound follow-up examination after reduction is important. There should be no evidence of a target sign.
Fig. 91.5 Contrast enema
91
92
Lesson 6
Gastrointestinal Tract Differential Diagnosis of Mural Thickening The differential diagnosis of Crohn's disease must also consider ischemic wall thickening such as can occur secondary to mesenteric ebolism, high-dose catecholamine therapy (Fig. 92.1), and gluten enteropathy (sprue). Patients generally exhibit increased fluid
in the bowel and, in the late stage, loss of the folds of Kerckring. In the acute stage they also exhibit thickening of the mucosa and submucosa (Fig. 92.2), but this does not affect the entire bowel wall as in Crohn's disease(see p. 90). 2 3
74 a
46
68
Fig. 92.1 Ischemia of the bowel wall
Fig. 92.2
Mucosal thickening in sprue
b
Diarrhea In watery diarrhea, the bowel loops contain a large amount of anechoic fluid (46 in Fig. 92.3). These intraluminal fluid accumulations should not be mistaken for extraluminal ascites. In fecal impaction (see Fig. 93.1) or Hirschsprung's disease (see p. 142), the bowel contents are more echogenic.
Appendicitis
74
3 46
46
74
46 46
46 46 45
Fig. 92.3
b
46
46 46 45
74
Fluid-filled bowel loops in diarrhea
Appendix, Normal Values
Normal
Inflammatory
Wall thickness a imum e ternal diameter
≤ 2 mm ≤ 6 mm
≥ 3 mm ≥ 7 mm
Table 92.4
A normal vermiform appendix has an inner hyperechoic layer surrounded by an outer hypoechoic layer (Fig. 92.5). The maximum diameter of a normal appendix should not measure more than 6 mm and the wall should be no more than 2 mm thick. External diameters of 7 mm or more and/or wall thickness of 3 mm or more are pathologic. Additionally, acute appendicitis typically causes edematous wall thickening, which appears as a thick hypoechoic ring with a hyperechoic center (mucosa and narrowed lumen) in the transverse plane (Fig. 92.6a).
Fig. 92.5 Normal findings (without peristalsis)
74 a
c 74 d74 /e
Fig. 92.6
In the longitudinal plane (Fig. 92.6b), the thickened appendix can be distinguished from other bowel segments by its lack of peristalsis and its dead end. One can also test for local tenderness by gently applying pressure with the transducer. The perifocal bowel loops can show a reactive reduction in peristalsis. Presence of abscess presents as an increasingly inhomogeneous and hyperechoic conglomerate with an ill-defined border which in its late stage makes the appendix difficult to identify.
Acute appendicitis
b
Lesson 6
Gastrointestinal Tract: Colon
Fecal Impaction Normally, only the wall of the colon near the transducer can be evaluated because the colon contains so much gas that the lumen or opposite wall cannot be evaluated. However, fecal material is occasionally retained, especially in older patients (fecal impaction, Fig. 93.1). Here it is seen in the transverse colon (43) without gas, allowing good evaluation of both walls of the colon.
5
In inflammatory thickening of the colonic wall (74) in the setting of colitis, the edematous semilunar folds can become much more prominent than usual, as seen here in the sigmoid colon (Fig. 93.2). Alternatively, thickening of the colonic wall can be ischemic, as is seen in mesenteric infarction or mesenteric venous thrombosis. The differential diagnosis is made by measuring perfusion on color duplex sonography.
3 74
5 43 43
15 16 35
Fecal impaction
Fig. 93.1
Colitis
1 2 6
3
b
1
4
4
2
5
46
74 43 43
Wall thickening in colitis
Fig. 93.2
43
74
45
74
b
Colon Carcinoma Depending on the stage there can be higher-grade constriction of the lumen (Fig. 93.5) by the tumor (54), which in combination with melena can lead to impaired passage of feces.
In normal colonic segments the wall is so thin that it is barely visible at the margin of the haustra (43 in Fig. 93.3). In carcinoma of the colon (Fig. 93.4) there is circumscribed solid tumorous mural thickening (54).
2
3 43
43
43
74
5
4
1
4
1
5
43
54
43
5
1
74
5
43
54
45
45
77 74
45 45
2 48
5
45
38
46
45
43
70
70 45
Fig. 93.3
b
Normal findings
Fig. 93.4
b
Longitudinal section of colon carcinomat
Fig. 93.5
b
Transverse section of colon carcinoma
93
94
Lesson 6
Gastrointestinal Tract Diverticulitis
pericolic fat ( ), the pericolic tissue in the vicinity of the diverticulum ( ) is ill-defined and shows edematous thickening ( ) consistent with inflammation. Fig. 94.3 shows a hyperechoic air bubble (47) in a small diverticulum with beginning thickening of the bowel wall (74) in the immediate vicinity of the diverticulum in an early stage diverticulitis.
Colonic diverticula are not rare but often occur in older patients in the absence of inflammation. Fig. 94.1 shows a diverticulum (54) that communicates via its narrow neck ( ) with the lumen of the adjacent colon (43). However, here the colonic wall (74) appears suspiciously thickened, a finding also seen on a CT scan of the same patient (Fig. 94.2). Whereas the central rectosigmoid junction is still sharply demarcated from its
4 5 46
2
4
45
43
74
3
4
46
74
2
2
74
46 22
45
21
3
54
3
6
43 64
54
1
4
46
22
74 2
47
70
Fig. 94.1
b
45
2
Fig. 94.2
Neck of diverticulum
b
Fig. 94.3
Diverticulitis on CT ...
When in doubt, the examiner enlists the help of the patient, who can often identify the point of maximum pain with great precision, and then visualizes the respective colonic segment in the transverse (Fig. 94.4a) and longitudinal planes (Fig. 94.4b) to evaluate
b
… in the early stage
whether localized wall thickening ( ) is present in the vicinity of the diverticulum ( ). Advanced stages will also show significant thickening of the pericolic connective tissue (5) as an accompanying hyperechoic reaction as in Fig. 94.5.
1 2
4
5 74
74f
5
43 47
a Fig. 94.4 Colonic diverticulum
b
45
43
47 45
Fig. 94.5
Advanced diverticulitis
b
47 45
74
Lesson 6
Quiz
Here again are a few quiz tasks from the chapter you have just finished. You will find the answers on the preceding pages. The solution to the image is on page 157.
1.
What distinguishing features do you know for evaluating the malignancy status of lymph nodes? List at least three criteria for physiologic and malignant nodal enlargement, respectively.
2.
What do benign adenomas of the thyroid typically (but not invariably) look like? Which criteria taken together suggest a thyroid malignancy?
3.
Please write down the normal values for the maximum diameter of the vermiform appendix and its wall thickness.
4.
Can you draw the layers of the stomach wall here and label their respective echogenicity?
5.
Do you remember how a diverticulum of the bowel differs from diverticulitis? Please write your differential diagnostic criteria here.
6.
Please specify five conceivable causes for the phenomenon shown in Fig. 95.1.
Criteria for a benign process
Fig. 95.1
Criteria for malignancy
95
Lesson 7 Bladder and Reproductive Organs
Bladder: Anatomy
98
Examination Technique, Bladder Volume
99 100
Indwelling Catheter, Differential Diagnosis of ystitis
Reproductive Organs: ale Reproducti e Organs
101
rostate land, estes Undescended estis, Orc itis, pididymitis, ydrocele, Inguinal ernia
102
emale Reproducti e Organs ndo aginal Ultrasound
103
Uterus ormal indings, Intrauterine Device (IUD)
104
Uterine umors
105
O aries
olume,
enstrual ycle
ases
O aries ysts and umors, Infertility erapy
106 107
regnancy esting, ctopic regnancy
108
lacenta osition, ender Determination
109
Quiz
110
98
Lesson 7
Bladder and Reproductive Organs Anatomy Urinary Tract: The two ureters (150) course from the kidneys (29) through the retroperitoneum anterior to the psoas major muscle (44) after crossing the iliac vessels (21 and 22) to the posterior margin of the bladder (38), which lies in a subperitoneal location (Fig. 98.1). Immediately posterior to the bladder is the rectum (43d) and between the two lies the pouch of Douglas (122), a common site of free abdominal fluid (blood, ascites, peritoneal dialysis fluid) at the far caudal end of the peritoneal cavity (Fig. 98.2).
34
155
16
13
24a
27
25a
155
17
150
29
25b 150
22 21
21
44
b a
43 d
Fig. 98.1
22a
38
83
The cervical region (40) of the uterus (39) lies posterior to the bladder at the cranial end of the vagina (41). Depending on how full the bladder (38) is, the uterus usually lies anteflexed on the roof of the bladder as shown in Fig. 98.2 or assumes a more vertical position as the bladder fills. Only rarely is the uterus retroflexed, and in these cases it is significantly more difficult to visualize in a transabdominal view due to interposed intestinal gas. In the center of the uterus one will find an endometrium (78) of varying height and echogenicity depending on the phase of the cycle (see p. 104).
6 2 77 48 152 38 39
41
78 122
40
43d
43d
Male Reproductive Organs: In men the prostate (42) is located on the floor of the bladder (38). The urethra (152) passes through it. The normally air-filled rectum (43d) lies directly posterior to the prostate. The seminal vesicles (42a) lie immediately cranial to it in the median plane. They typically appear hypoechoic on ultrasound images. In men the retrovesical pouch (122) is located cranial to these structures. It is the lowest point in the peritoneal cavity. Except in the case of an undescended testis (see p. 102), the testis (98) lies within the scrotum (100).
Fig. 98.2
2 6
152 42a
122
The key to the numbers not mentioned here may be found on the back cover flap.
© 2021 Thieme. All rights reserved.
98 / 100 38
The pubic symphysis (48) presents a barrier to direct transabdominal visualization of the bladder and reproductive organs that must be circumvented by appropriate transducer positioning (see p. 99 and Video clip 7.1).
(Schuenke M, et al: THIEME Atlas of Anatomy–Internal Organs, 3rd ed. Stuttgart: Thieme, 2020. Illustrations by M. Voll, K. Wesker.)
48
77
Fig. 98.3
19
15
28
22b
Female Reproductive Organs:
13
18
42 43d
Lesson 7
Bladder: Normal Findings
Examination Technique The bladder is systematically scanned in a suprapubic transverse plane (Fig. 99.1a) and in the sagittal plane (Fig. 99.1b). The examiner must perform the scan slowly enough to detect any suspicious wall thickening or intraluminal masses (see Video clip 7.1c). Including the adjacent lateral perivesical tissue in the scan has proven effective. Wherever possible, the examination should be performed a b with the patient’s bladder maximally filled Fig. 99.1 after drinking a large amount of clear liquid and before voiding or, in catheterized patients, after clamping the indwelling catheter. This will better visualize the bladder wall. Examining the empty bladder after the patient has voided has no diagnostic value. The normal bladder (38) on a typical transverse image (Fig. 99.2) lies posterior to the two rectus muscles (3) and cranial and anterior to the rectum (43). When full it exhibits the shape of a rectangle with rounded corners. In the sagittal plane (Fig. 99.3) the bladder appears more triangular. The prostate in males (42) or the vagina in females (see Figs. 101.2 and 103.1) can be visualized caudal to the bladder.
Determining Postvoiding Residual Bladder Volume Where neurogenic dysfunction or obstruction due to hypertrophy of the prostate gland (see p. 101) is suspected, the bladder volume should be calculated to determine the postvoiding residual bladder volume. The maximum transverse diameter (Fig. 99.2b) is determined on the transverse image and the maximum craniocaudal diameter on the sagittal image (the horizontal dotted line in Fig. 99.3b). To obtain a suitable sagittal scan, it will often be necessary to tilt the transducer caudally as indicated by the arrow (Fig. 99.3a) to prevent the acoustic shadow (45) of the pubic bone (48) from obscuring your view. The maximum anteroposterior diameter (vertically dotted line on both images) must then be determined in one of the two planes. The postvoiding residual bladder volume is then calculated in milliliters according to the simplified volume formula as the product of the three diameters multiplied by 0.5. Even though a postvoiding residual bladder volume up to 100 mL has been described as physiologic in the literature, one should consider an outlet obstruction wherever the postvoiding residual bladder volume exceeds 50 mL. Determining Bladder Volume:
Bladder volume= A x B x C x 0.5 1
2
5 3
3 46
38
45 77
Fig. 99.2
b
Bladder in the transverse plane
45 70
70 42 a
a
46
6
43
70
42 a
c
2
1 74
3
5
46
3
48
77
45
38 45
46
46
Fig. 99.3
a
b
Bladder in the sagittal plane
c
74
42 a 43 d
42
45
99
Lesson 7
100 Bladder Indwelling Catheter and Differential Diagnosis of Cystitis
to the sound beam and can mimic intraluminal matter (see p. 18). These artifacts must be differentiated from actual sediments of crystals, small blood clots (52), or calculi (49) along the bladder floor (Fig. 100.3). Sediment can be mobilized by rapidly varying the pressure applied to the transducer (be careful with a full bladder). This maneuver will naturally fail to separate an actual mural tumor from the bladder wall.
In patients with an indwelling catheter (76) the bladder (38) is usually collapsed, effectively preventing reliable evaluation (Fig. 100.1). Therefore the catheter should be clamped some time prior to the examination (remember to do this!) to allow the bladder to fill. Only in the presence of an advanced edema of the bladder wall (77) is it possible to diagnose cystitis (Fig. 100.2) without first allowing the bladder to fill. Wall thickness in a distended (filled) bladder should not exceed 4 mm. After voiding, even the normal bladder wall is irregular and up to 8 mm thick, potentially masking mural polyps or circumscribed tumors.
Ureteral Peristalsis Incidental findings occasionally include signs of inflow into the bladder from the ureteral ostia due to propulsive ureteral peristalsis. In infants one must also exclude urete roceles (see p. 141). Free fluid: In any abdominal trauma, it is essential to confirm or exclude free fluid (68) in the abdomen. Fig. 100.4 shows free fluid in its typical location in the pouch of Douglas posterior to the uterus (39), such as can occur in acute intraabdominal bleeding or ascites.
Wall Thickening Diffuse wall thickening involving the entire circumference is usually due to edema in the setting of cystitis. A circumscribed area of wall thickening is more suggestive of a mural tumor. The differential diagnosis in males must consider a trabeculated bladder, which can occur in response to a bladder outlet obstruction in prostatic hypertrophy. When in doubt, transrectal or (in females) vaginal endoscopic ultrasound at higher frequencies or CT studies can provide more information.
1
2
5
3
Internal Echoes and Sedimentation
a
1
5 74
3
3 77
46
38
43/47
74
74
46
74
Fig. 100.4
a
Ascites ...
45
5
74 b
43
46
Blocked balloon ...
Fig. 100.2
2
3
5 5
38
45
70
b
1
38
77 45
... in the pouch of Douglas
76
45
45
74
3
74
45
51a 38
45
b
a
77
45
43 d
68 46
2 46
74
39 40
43 76
Fig. 100.1
45
1
2
41
38
Even the healthy bladder is never entirely anechoic (= black). Reverberation artifacts (51a) induced by the anterior abdominal wall (Fig. 100.3) are usually projected into the lumen of the bladder (38) near the transducer. Section thickness artifacts (51b) are often observed in the posterior bladder distal to the transducer. These are caused by the oblique course of the bladder wall relative
a
51a
77
... of an indwelling catheter
70 70
77 / 51b 39
Fig. 100.3
b
49 / 52
Sediment on the floor of the bladder
Lesson 7
Male Reproductive Organs 101
Prostate Gland percentage of older men have prostatic hypertrophy (Fig. 101.2), which can cause voiding difficulties and trabeculation of the bladder (see Fig. 100.2). An enlarged prostate gland (42) elevates and indents the floor of the bladder (38). The bladder wall (77) is usually well demarcated and appears as a smooth, hyperechoic line (Fig. 101.2). Prostate cancer (54) frequently arises in the periphery of the gland. It can invade the bladder wall and eventually protrude into the bladder lumen (Fig. 101.3). Increasing urethral compression can lead to diffuse hypertrophy of the bladder wall (77), which then appears thickened (Fig. 101.3).
Transabdominal ultrasound examination of the reproductive organs requires a full bladder (38) to displace gas-filled bowel loops (46) cranially and laterally and prevent their acoustic shadows (45) from interfering with visualization. The prostate gland (42) is at the bladder floor anterior to the rectum (43) and is visualized and measured in the suprapubic transverse and sagittal planes (Fig. 101.1).
Prostatic Hypertrophy The normal prostate gland should not measure more than 5 cm x 3 cm x 3 cm and its calculated volume should not exceed about 25 mL (A x B x C x 0.5). However, a high
5
2
2 3
48
6
45
38
42
54
70
Fig. 101.1
b
77
Prostate size
45
38 45
42 / 54
77 70
70 74
Fig. 101.2
b
Prostatic hypertrophy
Fig. 101.3
b
Prostate carcinoma
Testes and Scrotum The adult testis (98) is normally homogeneously hypoechoic and clearly demarcated from the layers of the scrotum (100). It measures about 3 cm x 4 cm in the longitudinal plane (Fig. 101.4). The upper pole of the testis is covered by the epididymis (99), which extends along the margin of the testis. In children, an undescended testis should be excluded on the transverse image (see p. 102), which must show both testes next to each other in the scrotum.
48
51
45 42
43
43
46
3
77
42
70
77
38
51
45 70
77
46
3
46 38
38
5
2
5
70
1
100 99
98
47 45
Fig. 101.4
a
Testis: normal findings
b
45
Lesson 7
102 Male Reproductive Organs Undescended Testis
If both testes are not found in the scrotum at 3 months, the undescended or ectopic testis must be located. The testis (98) is frequently found in the inguinal canal near the abdominal wall (2/5) as shown in Fig. 102.1. If the testis cannot be located on ultrasound, a supplementary MRI scan is indicated as malignant degeneration can occur in an undescended or ectopic testis.
5
2 99
98
47
47 47
46
Fig. 102.1
a
Testis in the inguinal canal
Fig. 102.2 Perfusion of the testis
b
Orchitis and Epididymitis The differential diagnosis of sudden severe scrotal pain radiating into the inguinal region must consider an incarcerated inguinal hernia, testicular or epididymal inflammation, and testicular torsion. Testicular tissue can tolerate ischemia for only about 6 hours before irreversible necrosis sets in. Where "only" inflammation is present, Doppler ultrasound will demonstrate perfusion with arterial pulses in the flow profile ( in Fig. 102.2). The affected side may even show hyperperfusion. Torsion leads to considerably reduced or absent testicular perfusion in comparison with the contralateral testis. Orchitis or epididymitis typically shows edematous enlargement of the testis (98) or epididymis (99) as well as thickening of multiple layers of the scrotal wall
a
74
(100), as shown in Fig. 102.3. Equivocal findings can be resolved by comparison of contralateral size.
Hydrocele and Inguinal Hernia A homogeneous anechoic fluid accumulation (Fig. 102.4) is either a hydrocele (64) or a varicocele. A varicocele enlarges with the Valsalva maneuver and shows detectable perfusion on color duplex sonography. Occasionally, a herniated bowel loop (46) is seen in the inguinal canal or scrotum together with a hydrocele (64) next to the normal testis (98, Fig. 102.5). A malignant testicular tumor usually produces inhomogeneous changes in the testicular parenchyma. Malignant but still well-differentiated seminomas can be homogeneous with mostly unremarkable ultrasound morphology.
a
a
47
99 64
99
47
98
99
98
64 46
45
100
Fig. 102.3
b
Epididymitis
98
100
Fig. 102.4
b
Hydrocele
Fig. 102.5
b
Differential diagnosis of varicocele
Lesson 7
Female Reproductive Organs 103
The transabdominal visualization (Fig. 103.1) of the uterus (39) including the ovaries (91), vagina (41), and rectum (43) requires a full bladder (38) as an acoustic window. Because of the depth of penetration required,
lower frequencies around 3.5 MHz are used with correspondingly limited resolution. Gynecologists often prefer endoscopic ultrasound as an alternative because of its higher spatial resolution (see below). 2
38
51a 39
41
51c
43 d 51b
40
45 45
Fig. 103.1
a
45
122
c
b
Endovaginal Ultrasound Because of the proximity to the target organs, transvaginal transducers (Fig. 103.2) can be operated at higher frequencies (8–12 MHz or more) with correspondingly higher spatial resolution (see p. 11). Another advantage of endovaginal ultrasound is that the bladder need not be full. An assortment of electronic and mechanical transducers with variable imaging sectors (70–180°) is available. Transducers that emit an eccentric sound beam must be rotated 180° to visualize the contralateral ovary. In contrast to transabdominal imaging, the caudocranial endovaginal scan visualizes findings "upside down." The sound waves propagate from the bottom to the top of the image (Fig. 103.3). This orientation visualizes intestinal loops (43) with acoustic shadows (45) in the upper half of the image, whereas the uterus (39) and cervical region (40) are visualized in the lower half near the transducer.
cranial
anterior
posterior caudal
sagittal
Fig. 103.2
a
view
b
Image Orientation Many gynecologists prefer sagittal planes viewed from the patient’s left side, the opposite of the convention used by internists. The bladder (38) and other anterior anatomic structures are on the left side of the image (Fig. 103.3) whereas the cervix (40) and other posterior structures are on the right side.
35 39
45
45
78
45
2
39
43
48
77
38
78
38
Fig. 103.3
a
Normal anteflexed uterus on an endovaginal image
b
c
40
Lesson 7
104 Female Reproductive Organs Uterus: Normal Findings
the myometrium (39) (Fig. 104.2). After ovulation, the secretory endometrium increasingly loses its central echo ( in Fig. 104.3) until the endometrium becomes entirely hyperechoic.
The thickness of the endometrium (78) varies with the menstrual cycle. Immediately after menstruation, only a thin hyperechoic central line is observed (Fig. 104.1). Later, around the time of ovulation, the endometrium (78) is demarcated by a thin hyperechoic rim ( ) from
a
a
a
45
45
45
43 / 46
43 / 46 47 39
78
46
H 39
39 40
Fig. 104.1
47
78 78
38
Fig. 104.2
b
Fig. 104.3
b
b
The normally homogeneous hyperechoic myometrium can be traversed by vessels appearing as anechoic areas. The body (39) and cervix (40) of the uterus do not differ in echogenicity. In premenopausal women, 2 times the height (H) of the endometrium (78) should be less than 15 mm ( in Fig. 104.3). In postmenopausal women, that measurement should be less than 6 mm, unless the patient is undergoing hormone replacement therapy. To avoid exaggerating size due to oblique sectioning, the measurements should be obtained exclusively on longitudinal sections of the uterus.
a
Intrauterine Device (IUD)
a
45
d
46/45
39
45
47
D 78
92
78
40 41
Fig. 104.4
b
Correctly seated IUD
39
Fig. 104.5
b
92 40
Displaced IUD
An IUD (92) is easily recognized by its high echogenicity with acoustic shadowing (45) and should be located at the fundus in the uterine cavity. The distance between the IUD (d) and the fundal extension of the endometrium should be less than 5 mm, and the distance to the end of the fundus (D) less than 20 mm (Fig. 104.4). Longer distances (Fig. 104.5) suggest the IUD is displaced toward the cervix (40) and is no longer providing sufficient contraceptive protection.
Lesson 7
Female Reproductive Organs 105
Uterine Tumors The normal uterus is demarcated by hyperechoic serosa and shows a homogeneous hypoechoic myometrium (39). Myomas (54) are the most common benign uterine tumors. They arise from the smooth musculature and usually occur in the uterine body. For preoperative planning of a myomectomy, myomas are categorized as intramural or transmural (Fig. 105.1), submucosal (Fig. 105.2), or subserosal projecting from the outer uterine surface (Fig. 105.3). A submucosal myoma can easily be mistaken for endometrial polyps (65 in Fig. 105.2).
1
a
a
2
Fig. 105.1
40 46
b
122
45
Uterine myoma
45
46
54
46
39
78
46
45
65 / 54
41 43
47
74
47
78
45
a
45
39
54
Myomas exhibit a homogeneous or concentric crescentic echo pattern and are sharply demarcated with a smooth surface. However, they can also contain calcifications with acoustic shadowing or central necroses. The size of myomas should be accurately measured and documented on follow-up to exclude rapid progression indicative of rare sarcomatous degeneration. Note that sudden enlargement of a myoma in early pregnancy can be benign in nature.
39
40
Fig. 105.2
b
Submucosal myoma
Fig. 105.3
b
Subserosal myoma
Postmenopausal endometrial hyperplasia (Fig. 105.4) can be induced by administration of estrogens, by estrogen-secreting ovarian tumors, or persistent follicles. Persistently high estrogen levels increase the risk of the endometrial hyperplasia degenerating into an adenocarcinoma (54 in Fig. 105.6). Malignancy criteria include an endometrium that measures more than 6 mm after or 15 mm before menopause, exhibits an inhomogeneous echo pattern, and is irregularly demarcated as in Fig. 105.6. A hypoechoic accumulation of blood ( ) in the uterine cavity (hematometra) can be caused by postinflammatory adhesions in the cervical canal following conization or by a cervical tumor (Fig. 105.5). a
23 21
39 54 40
Fig. 105.4 Endometrial hyperplasia
Fig. 105.5 Hematometra
Fig. 105.6
b
Uterine carcinoma
Lesson 7
106 Female Reproductive Organs Volumetric Measurements of the Ovaries The ovaries (91) are visualized in a craniolateral sagittal plane (Fig. 106.1) and are usually located in the immediate vicinity of the iliac vessels (21 and 22). To measure their volume, the ovaries are also visualized in a transverse plane. The product of the three diameters multiplied by 0.5 provides an adequate estimate of ovarian volume. In
a
adults, the values range from 5.5 to 10 cm3, with a mean of 8 cm3. Ovarian volume is not affected by pregnancies, but continuously decreases in postmenopausal women from about 3.5 to 2.5 cm3, depending on the length of time since menopause.
a
a
21
21 b
43
45
91
22
45
93
74
21
43
93 38
Fig. 106.1
b
Normal Findings
Fig. 106.2
b
91
74
22
91
43
Graafian follicle
22
68 64
46
39
Fig. 106.3
b
Corpus luteum cyst
Menstrual Cycle Phases In the first days of a new mestrual cycle, several follicles (93) are normally visible as small 4–6 mm anechoic cysts within the ovary. Beginning with the 10th day of the cycle (Fig. 106.2), a dominant follicle (Graafian follicle) measuring about 10 mm in diameter begins to mature. It shows linear growth of about 2 mm per day, reaching a preovulatory diameter of 1.8 cm to 2.5 cm. This process is accompanied by regression of the remaining follicles. For infertility treatment and in vitro fertilization (IVF), ultrasound follow-up examinations performed at close intervals are important in that they can trace follicular maturation and occasionally even demonstrate the time of ovulation. Follicle size exceeding 2 cm, demonstration of a small mural ovarian cumulus, and digitations within the follicular wall are regarded as signs of imminent ovulation. Following the ovulation, the Graafian follicle disappears or at least markedly decreases in size. At the same time, free fluid may be detectable in the pouch of Douglas. Vascular proliferation into the ruptured follicle transforms it into the progesterone-producing yellow body (corpus luteum), which remains visible for only a few days as a hyperechoic area at the site of the former follicle. If nidation occurs, the corpus luteum persists and can remain visible as a corpus 45 luteum cyst (64) up to the 14th week of pregnancy (Fig. 106.3). Abnormalities of follicular development include 45 premature follicular luteinization 45 47 leading to missed ovulation and formation of a follicular cyst (64 in Fig. 64 106.4). A follicular cyst that remains 46 larger than 3 mm for more than one 91 menstrual cycle may represent a persistent follicle (see next page). b Fig. 106.4 a Follicular cyst
Lesson 7
Female Reproductive Organs 107
Ovaries: Cysts and Tumors An ovarian cyst exceeding 5 cm in diameter (see p. 106) is suspicious for tumor. Malignancy must be suspected especially where a cyst exhibits septa and/ or solid internal echoes ( ) or increased wall thickness (Fig. 107.1). Similar features are found in dermoid cysts (Fig. 107.2), which account for 15% of unilateral ovarian tumors. Their internal echoes ( ) correspond to sebum, hair, and other tissue components. They
Fig. 107.1 Ovarian carcinoma
should initially be regarded as benign and only rarely degenerate into malignancies. These findings must be distinguished from hemorrhagic or endometriotic cysts, which either contain fluid levels ( ) within their lumens (Fig. 107.3) or can be completely filled with homogeneous blood products (50 in Fig. 107.4). Do you know why the fluid level in Fig. 107.3 is almost vertical on the image? The answer is on page 158.
Fig. 107.3 Hemorrhagic cyst
Fig. 107.2 Dermoid cyste
Infertility Therapy Simply measuring the hormone levels of an externally stimulated cycle neither allows one to definitively exclude hyperstimulated ovaries (Fig. 107.5) nor does it provide reliable information about the number of stimulated follicles (93). Ultrasound monitoring of the number of growing Graafian follicles is indicated so that discontinuation of the hormone therapy can be considered where there are more than two stimulated follicles and the patient can take contraceptive measures if necessary.
46 68
45
45
45 47
About 5% of women have polycystic ovaries syndrome (PCO), characterized by lack of typical follicular maturation. This is usually attributable to adrenal hyperandrogenism. The typical features of PCO are multiple small cysts (64) arranged like a string of pearls primarily along the periphery of the ovary around a hyperechoic stroma (91 in Fig. 107.6). Homone therapy can help resolve undesired infertility in such cases.
45
45
45 93
50
21 22
93
43 / 46
45 74
22 b
47
93
21 b
64 64 91
64 74 46
91
Fig. 107.4
b
Endometriotic cysts
Fig. 107.5
b
Hyperstimulated ovaries
Fig. 107.6
b
Polycystic ovaries
Lesson 7
108 Female Reproductive Organs Pregnancy Testing
Threshold Discussion
regnancy testing is not limited to measuring h in the maternal blood or urine. The ultrasound examination should not only confirm the pregnancy, it can also exclude an ectopic pregnancy and detect a multiple pregnancy that hormone testing is unable to confirm (Figs. 109.3, 109.4). Intravaginal ultrasound can detect an early intrauterine pregnancy, here our first daughter Lea Céline, once the chorionic cavity has reached a diameter of about 2–3 mm. If you look very closely, you will discover a tiny hyperechoic point (Fig. 108.1). This size is generally reached 14 days after conception, or 4 weeks and 3 days after the last menstruation. The original vesicle in the body of the uterus (39), which is surrounded by hyperechoic endometrium (78), grows at a rate of about 1.1 mm per day and develops into the gestational sac (170), within which the embryo (95) can later be detected (Fig. 108.2). Embryonic cardiac activities begin at a gestational age of 6 weeks with a heart rate of 80–90 beats per minute. In later stages, ultrasound can also verify the proper number of fingers and toes or exclude pathology such as fetal diaphragmatic defects or heart defects. Our second daughter Joana was very cooperative in this regard (Fig. 108.3).
Ultrasound waves have been known to awaken fetuses in the third trimester, which then show spontaneously the movements of a child. Contrary to the opinion of many midwives, this phenomenon is absolutely harmless. According to the guidelines of the American Institute of Ultrasound in Medicine (AIUM), sound energies below 100 mW/cm2 or 50 J/cm are safe. Because the energies delivered with B-scan ultrasound (black and white) are far lower than the threshold values, current knowledge indicates that neither relevant thermal injury to tissue nor mutagenic effects are to be expected. It is only in color Doppler ultrasound and pulsed wave Doppler studies that the threshold values mentioned can be reached and exceeded during longer examinations. Therefore, any unnecessary color Doppler studies should be avoided during the sensitive phase of organogenesis in the first trimester despite the fact that there has been no evidence to date of any damaging effect of ultrasound waves [7.1].
Ectopic Pregnancy
51a
In an ectopic pregnancy (Fig. 108.4), the embryo (95) is outside the uterus (39). Because of the consequences it entails (including risk of hemorrhage), it is important not to overlook this pathologic condition.
38 51c
170 39
45
41
78 40 122
Fig. 108.1
a
Early pregnancy
43 / 45
b
2 170
23 43 / 45
21
95
78
170
Fig. 108.2
b
Embryo
39
45
39
38
96
47
78
170
39
97
95
95
35
Fig. 108.3
91
b
Fetal development
45
39
Fig. 108.4
b
Ectopic pregnancy
Lesson 7
Female Reproductive Organs 109
Placenta Position The normal location of the placenta is near the fundus along the anterior or posterior uterine wall. In about 20% of cases, the placenta (94) will show one or more unilocular or multilocular cysts or lacunae (64), which usually have no functional significance Fig. 109.1). However, an association with maternal diabetes or rhesus incompatibility has been suggested. However, the location of the placenta 2 should only be definitively deter3 mined at about the end of the second 95 39 trimester. This is because the increas39 ing expansion of the lower uterus can change what began as a placenta 94 39 109 previa in early pregnancy to a normal 64 96 or low-lying placenta (distance to 94 40 internal os of the cervix < 5 cm). 95 97 Three types of placenta previa are 97 distinguished: total placenta previa, 45 38 45 which totally covers the internal os of the cervix (40); partial placenta Fig. 109.1 b Placental cyst Fig. 109.2 b Placenta previa previa, which partially covers the internal os (Fig. 109.2); and marginal placenta previa, which encroaches on the internal os. The evaluation of placental structure has become less important as placental and fetal perfusion can be evaluated with Doppler ultrasound.
Multiple Pregnancies In multiple pregnancy, it must be determined whether the embryos (95) share a common placenta ( in Fig. 109.4) or each embryo is supplied separately. For parents-to-be (and their obstetrician) it is not only important to know whether to expect twins (Fig. 109.3) or even triplets (Fig. 109.4). Some also want to know whether they are expecting a daughter (Fig. 109.5) or son (Fig. 109.6).
Gender Determination Remember to reveal the gender of the fetus to the parents only when asked or if it has been previously requested. Above all, you should be certain of this determination. Early in pregnancy, it is possible to mistake (?) the umbilical cord ( ) for a clitoris or penis ( ), and the female labia for the scrotum ( ) (Figs. 109.5, 109.6).
Fig. 109.3 Twins
95
Fig. 109.4 Triplets
Fig. 109.5 Umbilical cord ...
Fig. 109.6 ... a boy!
Lesson 7
110 Quiz To complete this chapter, we again offer you the opportunity to test which details you have remembered and where your knowledge is still patchy. The answers to quiz
1.
On page 107, you were asked why a fluid level in a hemorrhagic endometrial cyst was vertical on the ultrasound image. Do you know the answer? If not, please review the description of the sagittal imaging planes on endovaginal ultrasound on p. 103.
2.
An 18-year-old male patient presents with severe pain in the left scrotum, which began about three hours earlier and radiates into the left groin. What are the main causes you must consider in a differential diagnosis? How much time do you have to establish the diagnosis? Which ultrasound methods do you plan to use?
3.
How do you recognize imminent ovulation on an ultrasound scan? What should change after the ovulation? How many days after the last menstruation or conception it is possible to document nidation on endovaginal ultrasound?
4.
A 58-year-old female patient is referred to you for a routine gynecologic examination. The patient had undergun menopause at age 52 years and has not taken any hormone medications within the last 5 years. You perform an endovaginal ultrasound examination and detect the findings shown in Fig. 110.1. The transverse thickness of the endometrium is 18 mm. What is your tentative diagnosis and what further steps would you take?
questions 1 through 6 can be found on the preceding pages, while the answer to the image question (no. 4) is on page 157 at the end of the book.
Fig. 110.1
Lesson 8 FAST, eFAST, Lung
FAST
112
eFAST, M-mode
114
Seashore Sign, Barcode Sign
115
Pleural Mobility, Pulmonary Pulse
116
Lung Point in Pneumothorax
117
Pleura: uantifying Pleural Effusions Pleuritis, Empyema, Mesothelioma
118 119
Ribs: Costal Fractures and Metastases
120
Lungs:
With images from Matthias Hofer and Georg Groß
Pneumonia
120
Bronchial Carcinoma, Pulmonary Infarct, Pulmonary Metastases, Pulmonary Edema
121
Quiz
122
Lesson 8
112 FAST FAST The FAST method (Focused Assessment with Sonography for Trauma) represents a technique for quickly and reliably excluding or confirming life-threatening bleeding into the serous cavities of the chest and abdomen in trauma patients. This standardized method [8.1–8.3] is also suitable for diagnosing parenchymal tears in the spleen or liver. Trauma patients are usually supine in the ambulance, emergency room, or shock room. Therefore, the examiner must consider where gravity will cause relevant hemorrhages to collect. From a lateral view of the torso
of a supine patient (Fig. 112.1) it quickly becomes apparent that free fluid will primarily collect in the pouch of Douglas in the lesser pelvis ( ) and in the cranial portion of the peritoneal cavity ( ). This pattern of distribution (anatomic predilection) is essentially attributable to the lumbar lordosis ( ). Free fluid in the pleural cavities (in this case hemothorax) also drains posteriorly into the costodiaphragmatic recess ( ) unless prevented from doing so by the presence of extensive pleural adhesions from previous pleuritis (see Fig. 117.3).
3
46
1
33 16
17
2
15
29
Fig. 112.1
4
29
Fig. 112.2
Fig. 112.3
The hematoma is also lateralized on both sides within the abdominal cavity. This is because the spine causes anterior protrusion of the overlying median peritoneum relative to its lateral periphery (Fig. 112.2). As a result, one rarely finds larger accumulations of blood close to the midline because the intraperitoneal hematoma follows gravity and drains laterally and posteriorly ( ). Accordingly, the transducer positions shown in Fig. 112.3 are now internationally accepted for rapid evaluation. First transducer position: The transducer is initially placed on the epigastrium in the transverse plane and tilted caudally (Fig. 112.4a) to evaluate the heart and pericardium for possible hemopericardium. Such a hemorrhage will be detectable as an anechoic rim of fluid (79) in the circular marginal spaces around the cardiac cavities (114 in Fig. 112.4b). Be sure to adjust the unit for sufficient penetration depth and a small zoom factor to visualize the posterior borderline of the pericardial sac ( ). 83 3
1
2
79
79
13 115
a
Transducer position for ...
b
... visualizing the pericardium ...
c
115
114
114
47
Fig. 112.4
114 114
79
47
... from beneath the xiphoid
9
69
68 29
Fig. 112.5
a
Transducer position for ...
b
... right hemothorax and ...
c
47
... pouch of Morison
Lesson 8
FAST 113
The second transducer position on the right anterior axillary line (Fig. 112.5a) also detects a right anechoic hemothorax (69 in Fig. 112.5b) and possible bleeding (68) into the hepatorenal recess (pouch of Morison) between the liver (9) and the right kidney (29) (Fig. 112.5c). The third transducer position on the left posterior axillary line (Fig. 113.2a) is used to exclude left hemothorax, which can lie cranial to the diaphragm (13) either laterally ( ) close to the transducer or medially at the lower edge of the image ( ). This transducer position can also detect splenic hematomas (50) in rupture of the spleen (Fig. 113.2b) as well as hemorrhage (68) into the abdominal cavity, here into the pouch of Koller, the recess between the spleen (37) and left kidney (29) (Fig. 113.3). The transducer must be angled anteriorly so that the sweep also includes the posterior costodiaphragmatic recess and perisplenic space (Fig. 113.1).
Fig. 113.1 The transducer is angled anteriorly to visualize the posterior pouch of Koller.
2 47
5 37 50
50
45
68 37
20
29
37
45
Fig. 113.2
a
Third transducer position
b
13
Fig. 113.3 perisplenic hemorrhage
Splenic hematoma
Fourth transducer position: Finally, the transducer is placed on the median suprapubic region in the sagittal plane and angled caudally (Fig. 113.4a) to evaluate the pouch of Douglas (122) between bowel loops (46), bladder (38), and rectum (43) to detect any blood (68) that might be present there (Fig. 113.4b). In larger hematomas, hemorrhage may also be detectable on the roof of the bladder and anterior to the bladder (if full). An experienced examiner can perform the entire FAST examination without photo documentation in as little as 20–30 seconds (hence the acronym). This dynamic procedure is convincingly illustrated in Video clip 8.1a–c. 1 46
3
5 74 77
51a 38
45
39
40 68
43 d
122
46
Fig. 113.4
a
Transducer position for the ...
b
... sagittal suprapubic plane
c
... and the pouch of Douglas
45
Lesson 8
114 eFAST eFAST The so-called "extended FAST algorithm" is intended to quickly exclude pneumothorax in trauma patients or, if present, to estimate its size in order to identify tension pneumothorax requiring aspiration and drainage. Each hemithorax is divided into four quadrants and systematically examined for a pneumothorax space. The transducer is positioned sequentially in a sagittal plane at each of the four positions marked in Fig. 114.1.
Close to the transducer, the resulting ultrasound image shows the anterior or lateral chest wall with the skin (1), subcutaneous tissue (2), pectoralis muscles (117), intercostal muscles (116) between the hypoechoic ribs (109), and, on the posterior aspect of the ribs, the pleural border (101) before the lung (47), which is visualized at a greater depth (Fig. 114.2).
1 2 109
117
116
109 101 45
45 47
PSL
AAL PAL
Fig. 114.1 Transducer position for eFAST
Fig. 114.2
a
Sagittal thoracic plane
b
M-mode
109
positioned in one of the intercostal spaces (ICS) to preclude any acoustic shadowing from the ribs (109). The change in echo behavior from this single line of the image is then plotted against time (= X axis). Chest wall
To evaluate the respiratory mobility and size of the lung, one line of the image in a M-mode is defined as the Y axis (vertical yellow line in Fig. 114.3) and
109
Lung
101
47 sec 1
Fig. 114.3
a
Line of the image in an ICS
b
2
3
4
5
6
In the superficial layers of the chest wall, nearly horizontal lines will form over the time axis because the skin, subcutaneous tissue, and musculature remain in a nearly constant position: No change in the location of the echo => horizontal lines.
7
M-mode image
However, this changes beginning at the depth of the pleural border (101). Within the lung tissue (47) the motion of physiologic or artificial respiration and arterial pulsation over time will create small regular changes
in the location of the origin of the echoes. As a result, instead of horizontal lines indicative of constant position, there is a finely granulated snowstorm here that resembles a random pattern of grains of sand.
Lesson 8
eFAST 115
Seashore Sign name "seashore sign," which suggests physiologic expansion of the lung without pneumothorax at this location (Fig. 115.2). A small pneumothorax with formation of a circumscribed space may nonetheless be present at another location, For this reason, all four quadrants of both halves of the lung are examined.
Where the lung is fully expanded and extends in the imaged area as far as the parietal pleural border (101), the upper (proximal) portion of the resulting M-mode image resembles a row of waves parallel to the seacoast, while the lower (distal) portion of the image resembles a sandy beach (Fig. 115.1). This has given rise to the
Chest wall
101
101
Lung Fig. 115.1
a
Seashore sign
b
In M-mode in ...
c
Fig. 115.2 ... a fully expanded lung
Barcode Sign layers of the chest wall remain in a constant position, the reverberation echoes do not change their depth or position over time. Therefore the resulting M-mode image shows only horizontal lines in a constant position which because of their varying thickness resemble a barcode on a product label (Fig. 115.3). Such a "barcode sign" is found at those locations on the chest wall where there is air in the interpleural space and thus pneumothorax ( ) is present at this location (Fig. 115.4).
However, if the lung is not fully expanded and does not extend as far as the chest wall in the imaged area, the air in the interpleural space will cause total reflection of the sound waves directly at the pleural border (101). You will then see echoes against the hypoechoic background that have been reflected back and forth several times between the layers of the chest wall. Because they arrive back at the transducer late, the image processor incorrectly projects them deep within the lung (see reverberation artifacts, p. 18). However, as the
101
Fig. 115.3
a
Barcode sign
b
In M-mode in ...
c
Fig. 115.4 ... pneumothorax
Lesson 8
116 eFAST Pleural Mobility Where the lung is fully expanded and extends in the imaged area as far as the parietal pleural border (101), the respiratory excursion of the lung will produce observable left-right displacement ( ) of pulmonary
tissue on the normal B-mode image (Fig. 116.1). This respiratory mobility is more readily discernible in the dynamic image sequence in Video clip 8.2.
101
101
47
Fig. 116.1 Lung mobility
Fig. 116.2
a
Pulmonary pulse ...
b
... in M-mode
c
... during respiratory standstill
Pulmonary Pulse During Respiratory Standstill When another intercostal image line is recorded over time and patients are asked to hold their breath or artificial respiration of unconscious patients is briefly interrupted, the pleural border (101) will show vertical lines ( ) or blurred stripes in the otherwise homogeneously granular pattern of the lung (47) as in Fig. 116.2. These vertical lines correspond to shifts in the proximal portions of the lung occurring as a result of perfusion with the arrival of the arterial pulse wave. They are synchronous with the pulse, vary with the heart rate, and are evidence of a fully expanded lung at the site being examined (Video clip 8.3). In pneumothorax neither pleural mobility nor a pulmonary pulse can be demonstrated during respiratory standstill.
A small pneumothorax with only a small amount of air in the interpleural space will not cause the affected lobe of the lung with its elastic fibers to completely contract toward the hilum of the lung. In such cases ultrasound can detect the border up to which the lung is still expanded and lies against the chest wall (Fig. 116.3) or, respectively, the area beyond which a pneumothorax (102) is present during physiologic or artificial respiration (Fig. 116.4). Determining this so-called "lung point" makes it possible to estimate the size of a pneumothorax (see next page).
102 16
114
109
16 15
109
15
35 34
Fig. 116.3 Pneumothorax on inspiration: lung extends up to the chest wall
114
35 34
Fig. 116.4 Pneumothorax on expiration between chest wall and lung
Lesson 8
eFAST 117
Lung Point While systematically evaluating all four quadrants of the chest (see p. 114) the examiner may conceivably place the transducer directly on the border between the expanded lung and the pneumothorax (Fig. 116.4). If this is the case, the M-mode image at that location will show a picture alternating between the seashore
sign and the barcode sign, depending on how the lung expands and contracts during respiration (Fig. 117.1). This limit to pulmonary expansion is known as the "lung point." Detection of this phenomenon ( ) is regarded as sufficient evidence of partial or complete pneumothorax.
Inspiration Fig. 117.1
a
Lung point ...
b
Expiration
... on the M-mode image demonstrating the limit to pulmonary expansion
c
Diagnostic Accuracy in Excluding Pneumothorax The particular advantage of the eFAST algorithm is that it can be applied in the prehospital phase of emergency treatment, for example in the ambulance, and that it can be performed quickly in the event a chest radiograph cannot be quickly obtained. Add to this the fact that not every pneumothorax ( ) is as easy to diagnose as the one shown in Fig. 117.2, in which both the lung and the pneumothorax (102) are readily identifiable. Many patients exhibit postpleuritic adhesions ( ) between the two pleural membranes. These adhesions tether parts of the lung to the chest wall and can lead to incomplete collapse of the lung with residual expansion, findings that can be difficult for the inexperienced diagnostician to recognize (Fig. 117.3).
102
Fig. 117.2 "Classic" mantle pneumothorax
The strength of the radiograph is that it can demonstrate an acute threat to the patient's life from tension pneumothorax (Fig. 117.4), which because of the severely reduced venous return flow to the heart can lead to acute heart failure before the reduced area of gas exchange reaches a critical level. In Fig. 117.4 the right lung has completely collapsed toward the hilum. The high pressure in the right pleural cavity has caused it to herniate into the contralateral left side ( ), displacing the heart and mediastinum laterally to the left. This has created a kink at the junction of the inferior vena cava with the right atrium, severely reducing the venous return flow to the heart. Such cases require prompt aspiration of the overpressurized pleural cavity and placement of a pleural suction drain to reexpand the lung.
102
Fig. 117.3 Partial pneumothorax Fig. 117.4 Tension pneumothorax with postpleuritic adhesions with midline shift
Lesson 8
118 Lung Quantifying Pleural Effusions on Chest Radiographs On conventional PA radiographs of the lung, pleural effusions are usually only detectable as lateral basal shortening of the costophrenic angle ( ) once the volume of the effusion has exceeded about 200–500 mL. On AP radiographs of a supine patient, the detection limit is even higher, at 500–1000 mL. Smaller volumes are only detectable on lateral films or radiographs obtained with the patient in the right lateral decubitus position (Fig. 118.1). The crescentic opacity ( ) suggests that the RLD
effusion at the lateral chest wall extends farther cranially (Fig. 118.2). In fact, the fluid is nearly horizontal in the chest cavity ( ) of a sitting or standing patient and in the lateral area only leads to greater cumulative absorption of X-rays (Fig. 118.3). The opacity on the radiograph obscures compressive atelectasis of the lateral basal segments of the lung, which is detectable on the ultrasound image.
Lateral
Posterior
Effusion surrounds lung in a horseshoe pattern
Lateral
PA
47
AP 69
Summation of absorption of effusions Anterior
Fig 118.1 Detection limits on radiographs
Fig. 118.2 Effusion in the costophrenic angle on a PA radiograph
Fig. 118.3 Summation effect
Quantifying Pleural Effusions on Ultrasound On ultrasound images pleural effusions are detectable without comparable artifacts. Images are best obtained with the patient sitting (or standing if possible). Even significantly smaller effusion volumes (69) are clearly detectable as anechoic (black) areas between the dome of the diaphragm (13) and the lung (47), which depending on the size of the effusion can exhibit compressive atelectasis (118 in Fig. 118.5). The semiquantitative estimation of the effusion volume is performed on ultrasound with the patient sitting and the transducer in a posterior or lateral position. The
2
maximum craniocaudal extent ( H ) of the anechoic fluid is measured and then the shortest distance (D ) between the caudal margin of the lung and the dome of the diaphragm (13 in Fig. 118.6). The sum of these two values (in cm) is multiplied by a factor of 70 to estimate the effusion volume in milliliters (Table 118.4).
Volml = (H + D [cm]) x 70 Table 118.4 Calculation of pleural eddusions
1 117 109 116 118
Lateral chest wall H
74 45
a
Basal pleural effusion ...
b
118 47 69
47
Fig. 118.5
D
116 69 13
… in a sitting patient
29 13
26
Fig. 118.6 Calculating the effusion volume
Lesson 8
Pleura 119
Other Pleural Changes either sedimented corpuscular blood components in hemothorax or an accumulation of pus in the pleural cavity (pleural empyema, 58 in Fig. 119.2). After chronic recurrent pleuritis, adhesions develop between the visceral and parietal pleura with decreased respiratory mobility and diffuse widening of the pleural border (101) with fibrous and partially calcified components consistent with pleural fibrosis (Fig. 119.3).
Larger pleural effusions (69) usually lead to accompanying compressive atelectasis (118) in the adjacent basal segments of the lung. Fig. 119.1 also shows signs of pneumonia (119) in the form of hyperechoic air inclusions resembling rice kernels and exhibiting a branching pattern in the consolidated and otherwise barely ventilated lung tissue. If internal echoes from sedimentation ( ) in the pleural fluid are detected, they may represent
1
1 2
117
2
2 5
116
69
117
13
118
118
26
119
13
51a
9
58
58
47
47
Fig. 119.1
b
101
69
69
Large pleural effusion
Fig. 119.2
b
Pleural empyema
This must be distinguished from malignant changes in the setting of bronchial or mammary tumors such as pleural carcinosis which can cause nodular irregular pleural thickening ( ) (Fig. 119.4) but which shows increased perfusion ( ) on power Doppler (Fig. 119.4b).
Fig. 119.3
b
Dry pleuritis
Mesotheliomas show a similar picture with extensive irregular pleural thickening ( ) as in Fig. 119.5. The lesions cover the chest cavity like a carpet and invade the diaphragm (13) with footlike tumor extensions.
13
69
9 9 69
Fig. 119.4
a
Pleural carcinosis on a noncontrastet scan
b
Perfusion image
Fig. 119.5 Mesothelioma
Lesson 8
120 Ribs and Lung Ribs
produces a convex but smoothly demarcated protrusion ( ) of the contour of the rib that lacks a visible fracture line (Fig. 120.2). However, where ultrasound findings include an irregular bulbous and inhomogeneous hypoechoic distension of the rib, then one must consider the differential diagnosis of a costal metastasis (56) of a malignant process ( in Fig. 120.3).
One may suspect a rib fracture in a patient with a history of trauma or even after a spontaneous event such as a severe coughing attack. In the presence of an acute fracture, a step-off ( ) will be detectable in the cortex of the rib (109) with a fracture line (168) at the clinically suspicious site (Fig. 120.1). Chronic rib fractures are characterized by formation of a callus which typically 1
1
1
2
2
117
5
117
109
Fig. 120.1 Acute fracture
109
56
168 109
2 117 117
45
45 / 47
Fig. 120.2 Chronic fracture
Fig. 120.3 Costal metastasis
Pneumonia effusions which partially expands in deep inspiration (see Video clip 8.4) and postobstructive atelectasis (which develops distal to a plug of mucus or a centrally stenosing bronchial carcinoma) which shows fluid-filled bronchi referred to as a "fluid bronchogram" ( in Fig. 120.6). Especially in immunocompromised patients, complications of pneumonia can include a pulmonary abscess (58) with central liquefaction (57 in Fig. 120.7a). Doppler ultrasound will often show marginally pronounced hyperperfusion (Fig. 120.7c).
In lobar pneumonia the inflammatory edema and retention of secretions and mucus leads to consolidation of the inflammatory lung tissue (119) with only greatly reduced residual ventilation of the alveoli (Fig. 120.4). Typical findings include a positive air bronchogram ( in Fig. 120.5) of the branching pattern of air-filled and therefore hyperechoic bronchi against the fluid-filled adjacent lung tissue, often with parapneumonic effusion. This must be distinguished from two forms of hypoechoic pulmonary atelectasis: compressive atelectasis in large pleural
2
2
1
2
69
116 69
119
119 118
47
47 45
45
Fig. 120.4 Lobar pneumonia
47
Fig. 120.5 Air bronchogram 1
13
Fig. 120.6 Fluid bronchogram 116
2 58 57 47 58
47 45
45
Fig. 120.7
a
Pulmonary abscess ...
b
... with signs of marginal ...
c
... hyperperfusion on power Doppler
Lesson 8
Lung 121
Bronchial Carcinoma a peripheral pulmonary infarct (Fig. 121.2), a power Doppler or color duplex scan is performed to determine whether perfusion ( ) is detectable in the changed area (Fig. 121.1c).
A pulmonary tumor (54) that lies in the periphery of the lung and not in a central location or near the hilum will be detectable on an ultrasound scan (Fig. 121.1a). In order to distinguish such a hypoechoic focal lesion from
1 2 117
116 54 47 45
47 45
Fig. 121.1
a
Bronchial carcinoma
c
b
... Perfusion image
Pulmonary Infarct Like renal infarcts (see p. 70) pulmonary infarcts (71) also exhibit a conical shape in the periphery and appear as hypoechoic biconvex zones or triangles on the pleural border (101) like shown in Fig. 121.2.
1
2 116
117 71
2
118 116
71
101
Possible complications include infarct pneumonia (Fig. 121.3) and, in the presence of fulminant pulmonary embolisms, dilation ( ) of the retrosternal right ventricle (114) consistent with the acute right heart strain in cor pulmonale (Fig. 121.4). 2
1
117
115 114
119 47 45
47 45
Fig. 121.2 Peripheral infarct
47 45
45
Fig. 121.3 Infarct pneumonia
Fig. 121.4 Acute dilation of the right ventricle
Pulmonary Metastases When a bronchial carcinoma creates a bronchial obstruction, the lung segments ventilated by this bronchus develop atelectasis (118). Ipsilateral or contralateral pulmonary metastases (56) that may be present within this area can then be identified as spherical or oval zones or triangles with a hyperechoic halo (Fig. 121.5), some of which may exhibit central necrosis and liquefaction.
Pulmonary Edema In pulmonary congestion or edema due to left heart failure, the ultrasound image will show an increased number of what are known as B lines particularly in the peripheral lower lung fields. These lead to long "comet tail" artifacts ( ) that move back and forth with respiration (flashlight phenomenon, Fig. 121.6, Video clip 8.5).
2
1
56
9
13 10
118
47 45
56
Fig. 121.5 Pulmonary metastases
Fig. 121.6 B lines in pulmonary edema
Lesson 8
122 Quiz To complete this lesson, the study questions below give you the opportunity to test your knowledge and close
any remaining gaps. The answers can be found on the preceding pages or in the appendix on page 158.
1.
FAST position 2
Which three hemorrhages can you simultaneously confirm or exclude in FAST positions 2 and 3?
• • • FAST position 3 • • •
2.
Please briefly repeat in keywords what causes the seashore sign and the barcode sign. What do each of them suggest?
3.
What three conditions must be met so that the pulmonary pulse phenomenon can be observed on M-mode images?
1. 2. 3.
4.
Look at Fig. 122.1 on this page. It shows the lung visualized through an intercostal window. Identify the image details shown and formulate your differential diagnosis and tentative diagnosis.
Fig. 122.1
5.
This image was obtained from an anterolateral position above the right pectoralis muscles. Please formulate your tentative diagnosis and differential diagnoses.
Fig. 122.2
Lesson 9 Pediatrics
Skull and Central Nervous System (CNS): Anatomy of the CSF Spaces Normal Findings in the Sagittal Plane Normal Variants Normal Findings in the Coronal Plane Cerebral Hemorrhage Hydrocephalus, Cerebral Atrophy Shunt in Hydrocephalus, Spinal Canal
124 125 126 127 129 130 131
Hip: Preparation and Positioning Normal Findings Setup and Measurement Errors Graf`s Classification of Infant Hips
132 133 134 135
Kidneys, Bladder, Spleen: Kidneys and Typical Variants in Newborns Diffusely Increased Echogenicity, Nephrocalcinosis Urinary Obstruction and Reflux
138
Renal and Adrenal Tumors
140 141
Patent Urachus, Hematoma and Cystitis, Ureterocele, Spleen Size in Pediatrics
With images from Matthias Hofer and Jasmin D. Busch
136 137
Gastrointestinal Tract: Pyloric Hypertrophy, Reflux, Hirschsprung's disease
142
Lesson 9
124 Skull and Central Nervous System Anatomy of the CSF Spaces
The external CSF spaces and other superficial structures CSF spaces in newborns [9.3] are visualized with a linear transducer at 5.0–7.5 MHz in order to achieve sufficient resolution (Fig. 124.1). SCW (sinocortical width) < 3 mm The normal width of the anterior horns (103) measured CCW (craniocortical width) < 4 mm from the midline falx cerebri (106) is no more than 13 IHW (interhemispheric width) < 6 mm mm ( ) in newborns. The measurement is made at SVW (lateral ventricle width, the junction with the foramina of Monro (144) or with anterior horn) < 13 mm the third ventricle (124), which itself should be no wider than 10 mm. (width of third ventricle) < 10 mm 3rd VW The interhemispheric fissure (146), which is defined as the shortest distance between the superior frontal gyri ( ), has a maximum width of 6 mm in the neonate (Fig. 124.1c). Sinocortical width (147, < 3 mm) and craniocortical width (148, < 4 mm) are determined to exclude cerebral atrophy (with expansion of the subarachnoid space) or obstructive hydrocephalus (with narrowing of the subarachnoid space).
140
148 147
136 146
126
103
131 128
Fig. 124.1
a
b
Coronal section
c
103c
144
124 124
103a 103b
144
103c
103a 125
110
103b
125
Fig. 124.2 Lateral view of ventricle
Fig. 124.3 Top view of ventricle
(Schuenke M, et al: THIEME Atlas of Anatomy–Head, Neck, and Neuroanatomy, 3 ed. Stuttgart: Thieme, 2020. Illustrations by M. Voll, K. Wesker.) rd
Optimal conditions for examining newborns and infants include not only a quiet environment free of any hectic activity, a prewarmed gel, and a heat lamp over the examination table, but also the presence of a person emotionally close to the child. The examination is performed through the anterior fontanel (Fig. 124.1)
until it closes at the age of about 9 to 18 months. The size of the acoustic window steadily decreases with age, making it increasingly difficult to visualize lateral and peripheral cerebral structures, even with maximal tilting of the transducer.
Lesson 9
Skull and Central Nervous System 125
Normal Findings in the Sagittal Plane The transducer is placed on the fontanel and the skull is systematically scanned in the sagittal plane with a slow and continuous sweep from right to left (Fig. 125.1a). The individual examiner should best stick to a unchanging examination sequence. This reduces the chances of confusing the two sides. For example, one can begin in the median plane (Fig. 125.2), adjusting the zoom factor so that the hyperechoic margin of the occipital bone ( ) is barely
126
132
128
visible. Then one scans first the left and then the right hemisphere systematically for pathologic changes (Fig. 125.3). It is important to verify normal morphology of the corpus callosum (126) and the overlying cingulate gyrus (130). The cerebellum (110) is visualized as a hyperechoic structure posterior to the pons (145) in the posterior cranial fossa (see Fig. 125.2).
130 132
124 144
a
129
145 141
Fig. 125.1
134
125
Fig. 125.3
Fig. 126.1 Fig. 125.2 c
b
The thalamus (129) lies at the center of the laterally oblique imaging planes (Figs. 125.2 and 125.3). The anechoic CSF in the lateral ventricle (103) is above the thalamus and contains the hyperechoic choroid plexus (104), whose contour should appear smooth without local bulging. This must be distinguished from a choroid plexus hemorrhage (see p. 129). Where the corpus callo-
103
124
110
sum (126) is normally developed, the cerebral sulci (133) of the parietal and occipital lobes do not extend to the lateral ventricles, but are interrupted by the cingulate gyrus (130). A midline section including the pons (145), hyperechoic cerebellum (110), and fourth ventricle (125) is shown in Fig. 125.2, whereas Fig. 125.3 shows an oblique sagittal section through the left lateral ventricle.
130 126
133
128
145
124
105
127 110 125
45
45 Fig. 125.2
a
b
c
133
103 105
138
45 105 Fig. 125.3
a
b
5
10
c
129
130
104 105
Lesson 9
126 Central Nervous System: Normal Variants Choroid plexus cysts: Occasionally small unilateral choroid plexus cysts (64) can occur (Fig. 126.1). Small perinatal hemorrhages or viral infections have been discussed as possible causes. If the cyst is small and does
not impair the CSF circulation, it generally has no clinical consequence. Only larger parenchymal defects that are isoechoic to CSF (porencephaly) suggest areas of hemorrhage resorption or cerebral malformations. 140 103
133
121
126
129 64 104 105
45
Fig. 126.1
a
c
b
Preterm newborns: The normal cerebral sulci can be totally absent in preterm newborns delivered around the 28th week of gestation or, depending on gestational age, they can be less well developed than in term newborns. However, this is not necessarily indicative of a genuine maturation disturbance. Accordingly, the CSF spaces in a preterm newborns are more capacious and occasionally asymmetric (Fig. 126.3). The corpus callosum is often incompletely developed in preterm newborns as well. It then appears as a thin hypoechoic line in the coronal plane, usually just above the cavum of the septum pellucidum. These physiologic signs of immaturity will have to be monitored on follow-up studies to distinguish them from impaired CSF flow or genuine hypoplasia or agenesis of the corpus callosum (Fig. 126.4).
normal variant that is not necessarily indicative of impaired CSF flow. Fig. 126.3 shows a wide anechoic CSF space lateral to the choroid plexus (104) on the left, but not on the right. Agenesis of the corpus callosum: Many developmental disorders, syndromes, and metabolic disorders involve the corpus callosum, and involvement may also be secondary to hypoxia or infection. The spectrum of callosal abnormalities ranges from partial to complete absence (agenesis) of the corpus callosum. In the coronal plane (Fig. 126.4a), agenesis of the corpus callosum leads to a "steer horn" appearance of both anterior horns ( ), which are farther apart and farther lateral than normal. In the sagittal plane (Fig. 126.4b), the cingulate gyrus is also absent in the area of agenesis (see Fig. 125.2) so that the gyri of the cerebral hemispheres extend to the lateral ventricles ( ). This makes it easy to detect even partial agenesis of the corpus callosum. This example (Fig. 126.4) shows not only prominent lateral ventricles but also a prominent subarachnoid space ( ) consistent with diffuse cerebral atrophy (compared to Fig. 124.1).
Cavum of the septum pellucidum: Incomplete fusion of the septum pellucidum between the anterior horns leads to a CSF-filled cavum of the septum pellucidum (128). This is usually obliterated within the first few months of life but in rare cases persists into adulthood (Fig. 126.2). Slight asymmetry of the lateral ventricles (103) is another
a
a
105
140 164
a
140
136
132
105 103
138 131 103 128 129 104
Fig. 126.2
b
Fig. 126.3
b
Fig. 126.4
b
Lesson 9
Pediatrics: Skull and Central Nervous System 127
Normal Findings in the Coronal Plane After scanning in the sagittal plane, the transducer is rotated 90 degrees to scan in the coronal planes. The transducers that have proven most useful are multifrequency sector transducers (Fig. 127.1c) with a small contact coupling area and a center frequency of about 3.0 MHz for infants, 5.0 MHz for ages 6–8 months, or 7.5 MHz for preterm and term newborns. Mixed type transducers are now available that combine the good near-field resolution of linear transducers with a beam that diverges in the deeper layers. This
makes it possible to visualize a wider segment of the brain (Fig. 127.1c). The skull is scanned in the coronal and sagittal planes with a slow and continuous sweep of the transducer (Figs. 127.1a, b). The examination passes through and documents five standard coronal planes. The examiner begins anteriorly (Fig. 127.2) and inspects the periventricular white matter (131), which is physiologically more hyperechoic than the adjacent cortex (132). The transducer rests on the superior sagittal sinus (136).
135 132 103
132
131 124 Fig. 126.2
104
Fig. 126.3 Fig. 128.1
Fig. 127.1
a
110 Fig. 128.3 Fig. 128.2
Linear
Sector
Mixed type
c
b
136 140
132
105
Fig. 127.2
a
b
The plane immediately posterior to the first one (Fig. 127.3) intersects the anterior horns of both lateral ventricles (103), which in this plane should not contain any hyperechoic choroid plexus. Slight ventricular asymmetry
131
131
45
c
can still be physiologic or can be due to oblique sectioning. The shape of the hyperechoic Sylvian fissure (134) resembles a Y rotated 90° (see Fig. 128.1).
140 103 133 129 105
Fig. 127.3
a
b
c
132
Lesson 9
128 Pediatrics: Skull and Central Nervous System Normal Findings in the Coronal Plane The transducer is now moved posteriorly to the next imaging plane to document the communication between the lateral ventricles (103) and the third ventricle (124) through the interventricular foramen of Monro (144 in Fig. 128.1). In addition to anechoic
cerebrospinal fluid, the hyperechoic choroid plexus (104) is visualized in the lumen of this ventricular communication. This hyperechoic choroid plexus must not be mistaken for an intraventricular hemorrhage, which would be equally hyperechoic. 140 103
134
104
144
124
105
Fig. 128.1
a
b
Tilting the transducer further anteriorly (Fig. 128.2a) causes the sound waves to propagate further occipitally. This visualizes the curved bodies of both lateral ventricles, which merge with the temporal horns (Fig. 128.2b). Here it is also easy to determine the width of
132
c
the lateral ventricles (103) and thickness of the choroid plexus (104), which is normally smoothly demarcated. The thalamus, internal capsule, and putamen are located medially.
135
140 132
131 103 133
104
105
Fig. 128.2
a
b
Placing the transducer at an extreme angle (Fig. 128.3a) visualizes the somewhat ill-defined and hyperechoic occipital white matter (131 in Fig. 128.3b), which surrounds the ventricle in a pattern resembling a butter-
110
c
fly. Note the many sulci (133) that traverse the cortex as hyperechoic lines because of their rich vascularity and connective tissue. The normal widths of the CSF spaces are shown on page 124.
133
132 131
45
Fig. 128.3
a
b
45
c
131
105
Lesson 9
Pediatrics: Skull and Central Nervous System 129
Cerebral Hemorrhage Cerebral hemorrhages occur according to the following pathophysiologic mechanism:
Cerebral hemorrhage: Grading
The ventricles are lined by an epithelium known as the ependyma. The subependymal tissue layer lies beneath it. This tissue layer proliferates between the 24th and 32nd weeks of gestation and becomes richly vascularized. During this time, this germinal matrix is very sensitive to fluctuations in blood pressure as the mechanism for regulating intracerebral blood flow is not yet fully developed.
Grade 2 With additional ventricular extension without ventricular dilation (involving more than 50% of the lumen
As a result, fetal cerebral hemorrhages (50) very often occur in the subependymal region or in the region of the choroid plexus. In newborns, bleeding commonly occurs in the caudothalamic groove (121) between the head of the caudate nucleus (138) and the thalamus (129 in Fig. 129.2). Three grades of cerebral hemorrhage are distinguished according to severity (Table 129.1); all can occur with or without parenchymal hemorrhage.
Grade 1 Isolated subependymal hemorrhage
Grade 3 With additional ventricular dilation (involving more than 50% of the lumen) +
Additional extension into the cerebral parenchyma
Table 129.1 140
133
126 121 138
129 50 104
Fig. 129.2
140
140 133
105
133
132
105 129
50
129
105 104
Fig. 129.3
126 50/ 104
133 131
105 132
129 104 45
45
Fig. 129.4
b
71
105
103
b
103
130
Fig. 129.5
105
b
Ultrasound Morphology Acute hemorrhage (50) is hyperechoic compared with the adjacent cerebral parenchyma (132) and for the reasons outlined above is usually located in the vicinity of the ventricular system (Fig. 129.3). An irregularly shaped or bulging choroid plexus (104) suggests a hemorrhage (50) into the plexus (Fig. 129.4). An earlier intrauterine
hemorrhage that has been resorbed leaves behind CSF-filled parenchymal defects (71) that can be mistaken for dilation of a lateral ventricle (103 in Fig. 129.5). The differential diagnosis between a periventricular parenchymal defect and genuine hydrocephalus is discussed on the next page.
Lesson 9
130 Pediatrics: Skull and Central Nervous System Hydrocephalus Obstructive (noncommunicating) hydrocephalus (Fig. 130.1) is usually caused by posthemorrhagic adhesions that obstruct the free flow of cerebrospinal fluid out of the ventricular system. Less frequent causes include compression of CSF channels by an aneurysm of the vein of Galen, a biconvex (!) cyst of the septum pellucidum (see cavum of the septum pellucidum, Fig. 126.2) obstructing the foramen of Monro, or aqueduct stenosis. Isolated dilation of the fourth ventricle occurs where aqueduct stenosis is accompanied by obstruction of the foramina of Luschka and Magendie. The resulting increase in pressure in the lateral ventricles initially produces rounded and distended
temporal horns because here the pressure of the surrounding cerebral parenchyma is lowest. Thickening and dilation of the entire lateral ventricles only occurs later (Fig. 130.1) and is accompanied by distension and dilation of the entire lateral ventricle and simultaneous narrowing of the subarachnoid space. The resulting increase in pressure must be slowly relieved by a diversionary CSF shunt ( in Fig. 130.2). In chronic hydrocephalus, excessively rapid decompression could place excessive strain on the external cerebral vessels (with risk of hemorrhage). After a CSF shunt has been placed, follow-up examinations are indicated to monitor the position of the shunt and exclude malfunction.
136
Fig. 130.1
148
147
140
148 136 132
147
132
146
146
71
138
103 Fig. 130.2
Fig. 130.3
b
Fig. 130.4
71 103 b
Cerebral Atrophy The width of the subarachnoid space can differentiate obstructive hydrocephalus from an enlarged ventricular system due to cerebral atrophy. Here, a linear transducer is used because of its better near-field resolution. Fig. 130.3 shows significant widening of all CSF spaces ( ) in diffuse cerebral atrophy involving both hemispheres (see Fig. 124.1). Note the unusually good visualization of the superior sagittal sinus (136). Unilateral parenchymal
defects (71) result in widening of the ipsilateral subarachnoid space (148) in comparison with the contralateral side (Fig. 130.4). Additionally, the superficial cerebral sulci are more prominent in cerebral atrophy, whereas they tend to be effaced in obstructive hydrocephalus.
Lesson 9
Pediatrics: Skull and Central Nervous System 131
Monitoring the Shunt in Hydrocephalus Where ultrasound findings such as progressive ventricular enlargement suggest malfunction of the CSF shunt, the examiner should evaluate not only the intraventricular position of the shunt tip (Fig. 130.2) but also the entire length of the shunt catheter. The adjacent radiographs show a disconnected ( ) shunt (Fig. 131.1a) and a follow-up image after shunt revision (Fig. 131.1b) in a child with a ventriculoperitoneal shunt. On the second radiograph, the catheter has been reconnected to the coupling. Shunts occasionally need to be replaced or revised after several years as the child grows taller.
Fig. 131.1
a
Valve dislocation
b
after correction
Spinal Canal In infants, the conus medullaris (142) of the spinal cord (141) is visualized on a posteroanterior scan of the prone patient preferably using a high-frequency (10-18 MHz) linear transducer (Fig. 131.2). The spinal cord is demarcated from the anechoic spinal CSF space (140) by the delicate hyperechoic line of the pia mater. The hyperechoic double line in the center of the cord is not the central canal but the interface between the white commissure and the anterior median fissure. The fibers of the cauda equina (143) extend caudally and are visualized as a hyperechoic structure around the conus medullaris ( ), which should not extend below the L2-L3 disk space in the newborn. Anatomic landmarks: The beginning of the sacrum can be identified by its fused S1 vertebra, which is the first structure to protrude posteriorly (toward the transducer ) from the straight line of the vertebrae. Occasionally, a cyst ( ) can be found in the filum terminale, which usually does not have any clinical significance.
140 141 142 36
L1 Fig. 131.2
a
Prone position
b
Conus medullaris
35 36
35
143 36 35
36 35
36
S1
c
The progressive ossification of the vertebral arches makes visualization of the spinal cord increasingly difficult on ultrasound images, and gradually requires the use of magnetic resonance imaging (MRI). It is important to verify unrestricted mobility of the spinal cord with respiration and pulse. This can be documented on M-mode studies. Absent pulsation, distortion, or a low conus medullaris and fixation of the cord to the posterior wall of the spinal canal suggest a tethered cord syndrome, which is often caused by an intraspinal lipoma or epidermoid cyst. A tethered cord can also occur from fixation of neural structures as a result of postsurgical scarring.
Lesson 9
132 Pediatrics: Hip Preparation for Hip Examination Early exclusion of hip dysplasia in a newborn requires precision. It is also crucial to perform the various steps of the examination quickly before the newborn becomes restless. A changing table with tray is placed in the examining room or adjoining room to allow the mother or the person accompanying the child to remove the diaper without stress and clean the newborn if necessary. A heat lamp over the examination table will prevent the newborn from becoming cold (Fig. 132.1).
Positioning the Newborn The examiner places the newborn in a special cradle in a precise 90° lateral position. Then the mother can place her
Changing table
left hand beneath the newborn's head and her right hand on the upper shoulder. Most term infants exhibit strong flexion and react to unexpected extension of their legs with resistance and restlessness. Experienced examiners take care not to extend the upper leg more than necessary. The edge of the examiner's left hand gently presses the infant's thigh to prevent anteversion of the femoral neck. The goal is to obtain moderate extension in slight internal rotation (Fig. 132.2), without allowing the knee to move forward ( ) past the edge of the positioning cushion into external rotation as shown in Fig. 132.3. A foot switch is used to freeze the image so that the examiner has both hands free for positioning the newborn if necessary and guiding the transducer.
Mother
Free floor space
Foot switch
Examiner Ultrasound unit
Fig.132.1 Setting in the ultrasound suite
Fig. 132.2 Positioning the newborn
Fig. 132.3 Positioning errors
Ultrasound Documentation The German Quality Assurance Agreement on the Infant Hip requires that each hip be photographed twice and measured once at a minimum of 1.7 power magnification in the standard plane defined by Graf without any tilt. The following structures must be clearly identifiable: the osteochondral junction (line of the growth plate between the ossified femoral shaft and the cartilaginous femoral head and greater trochanter), the femoral head (153), the fold of the transition from the joint capsule to the perichondrium of the femoral neck, the joint capsule itself,
the acetabular labrum (158), the cartilaginous acetabular roof, the ilium (112) including its inferior margin, and the bony promontory of the acetabular rim (159), right next to the transition point ( , see p. 133). Once the inferior margin of the ilium has been clearly visualized, the usability test is performed: The imaging plane is centered on the inferior margin of the ilium by rotating the transducer around the axis of the cord (Fig. 133.6) and corrected to obtain the median imaging plane. The acetabular labrum can then be visualized without having to search for it.
157 156 112 45 Fig. 132.4 Transducer position
Fig. 132.5
a
Standard plane
b
162 158
160
153 159 165 161
Anatomic diagram
45
Lesson 9
Pediatrics: Hip 133
Graf favors an image in which the ilium is visualized perpendicular to the upper margin of the image. Yet many radiologists, internists, and pediatricians prefer the orientation they are more familiar with: Here, cranial structures are visualized along the left margin of the image and the lateral structures close to the transducer appear along the upper margin of the image. However, Graf maintains that there is evidence that this manner of visualization may be associated with a higher error rate [9.3]. First the baseline is drawn: This line originates at the
Fig. 133.1 Baseline at the ilium
Fig. 133.2 Inferior margin of the ilium
To construct the line for the cartilage roof angle beta ( ) one irst determines the transition point according to the concave-convex rule by moving laterally along the concavity of the acetabulum from the inferior margin of the ilium. After an acoustic interruption, the convex curve extends cranially along the ilium. The transition point lies at that point where the acetabular concavity joins the convexity. It can be readily identified by the acoustic interruption ( in Fig. 133.4). The correct imaging plane is found by having the examiner rotate the transducer around the axis of its cord or, respectively, counterclockwise ( in Fig. 133.6): If he or she rotates the cranial part of the transducer too far
Fig. 133.4 Bony convexity
"Z point" (the insertion of the rectus femoris tendon on the ilium) and extends distally, tangential and parallel to the sharply demarcated ilium with the hip extended (Fig. 133.1). Then the inferior margin of the ilium ( in Fig. 133.2) and the center of the lateral acetabular labrum ( in Fig. 133.3) are identified. To determine the angle alpha of the bony roof, this inferior margin of the ilium ( in Fig. 133.2) is identified and using that as a center of rotation, a tangential line is drawn along the bony acetabulum (Fig. 133.5).
Fig. 133.3 Acetabular labrum
anteriorly, the line of the ilium will also course obliquely to the transducer as in Fig. 134.2. The farther the acoustic shadow extends medial to the bony promontory, the more the hip is ossified. In a type I hip with an angular promontory, the transition point lies directly in the bony acetabular promontory. A line is now drawn laterally from this transition point through the center of the acetabular labrum (Fig. 133.5). The rule for identifying a type IIc unstable but still centered hip and differentiating it from a type D decentering hip (critical range hip) is as ollo s: The value determines the hip type where it is more than 77° [9.2].
Fig. 133.5 Alpha and beta lines
Fig. 133.6 Rotating the transducer
Lesson 9
134 Pediatrics: Hip Measurement Errors Especially in a restless newborn, it is easy for the examiner to lose the correct imaging plane. Where the transducer tilts posteriorly ( in Fig. 134.1a) this usually produces a medially convex, curved course ( ) of the ilium (Fig. 134.1b) away from the transducer. However, where the transducer is tilted anteriorly
Posterior tilt
Fig. 134.1
b
Posterior error plane
If the examiner angles the transducer too far caudally (Fig. 134.4a), the line of the ilium also courses obliquely and the osteochondral junction is often more blurred ( ) or no longer identifiable ( in Fig. 134.4b). Because of the many sources of error and the great clinical significance of this screening examination, it is best performed by experienced examiners.
(Fig. 134.2a) or rotated, the echo of the ilium approaches the transducer obliquely ( in Fig. 134.2b). Angling the transducer too far cranially (Fig. 134.3a) also visualizes the course of the ilium obliquely (Fig. 134.3b) and often makes it impossible to clearly visualize its inferior margin.
Cranial angulation
Anterior tilt
Fig. 134.2
b
Anterior error plane
Fig. 134.4
a
Caudal angulation
Fig. 134.3
b
b
Cranial error plane
Caudal error plane
Lesson 9
Pediatrics: Hip 135
Classification of infant hips according to Graf In hip dysplasia, the femoral head ( ) increasingly migrates craniolaterally. On the radiograph (Fig. 135.2), the bony acetabular roof is no longer close to the horizontal line ( ) but courses laterally at a steeper cranial angle ( ). The MR image (Fig. 135.3) shows the extreme case of a dislocated femoral head ( ) and an empty acetabulum ( ) that is obvious in comparison with the contralateral side. The alpha angle measured on ultrasound decreases with increasing severity of the dysplasia. s a rule o thum rapid gro th should cause the angle to expand from a minimum postpartum value of 50° to an angle of at least 60° by the beginning of the fourth month of life. Statistically, the optimum angle is 64°. The maturation curve shows a very strong, exponential increase only in the first few weeks of life, after which it continues at a plateau. Therefore, it is important to make the diagnosis as early as possible so that adequate therapy appropriate to the stage of the disorder can be promptly initiated to stabilize the femoral head and
Fig. 135.1
Fig. 135.2
Transient synovitis of the hip: Thickened synovia and joint effusion are typical findings of acquired hip disorders. The child is positioned supine and examined with a highfrequency linear transducer placed on the anterior hip (Fig. 135.4a). The normal joint space (168) appears as a thin anechoic space between the hyperechoic joint capsule (163) and the anterior contour of the femoral epiphysis (166) and metaphysis (167 in Fig. 135.4b). The indentation of the femoral growth plate (107) between them is easily identified. Measurements of the height of the epiphysis ( ) obtained on follow-up examinations can easily establish a loss of height such as can occur in necrosis of the femoral head. A transient joint effusion frequently
Classification of Infant Hips According to Graf [9.2] Alpha I (normal) II a+ II a– II c II d III (eccentric) IV (dislocated)
> 60° 56–59° 50–55° 44–49° 44–49° < 44° < 44°
Beta
Femoral head centered centered centered centered centered eccentric
< 55° 55–70° 55–70° 55–77° > 77° > 77° undetermined dislocated
securely center it within the acetabulum. For example, a type IIa-hip (Fig. 135.1) persisting after the age of 6 weeks represents defective maturation. For further detailed information, consult the extensive monograph by Reinhard Graf ([9.3] see p. 133 below).
Fig. 135.3 develops in the setting of viral infection and appears as anechoic widening ( ) of the joint space (Fig. 135.5). Where an anechoic joint effusion persists longer than two weeks or internal echoes are detected within the effusion, clinical and laboratory tests or supplementary MRI studies are indicated to rule out Legg– Calvé–Perthes disease or septic arthritis. Fig. 135.5 2 5 163
168
107 166
Fig. 135.4
a
b
c
167
Lesson 9
136 Pediatrics: Kidneys The next two pages present the crucial morphologic characteristics in newborns and children that play an important role and differ from findings in adults.
Kidneys in Newborns Before examining the kidneys in the prone newborn (Fig. 136.1a), one should first examine the bladder with the patient supine as it can only be evaluated when full and newborns often void during the examination. After this, the newborn is positioned prone and posteroanterior scans of both kidneys are performed with a highfrequency 10–18 MHz linear transducer in the longitudinal plane (Fig. 136.1) and transverse plane (Fig. 136.2). Anteroposterior transhepatic scanning (see p. 65) or lateroposterior examination with the patient in the lateral decubitus position is more suitable only in older infants. Lower center frequencies of 3.5–5 MHz are preferred in older children. Reference values of childrens’ kidneys are defined in percentiles depending on childrens’ body height. A summary can be found on the following page.
Typical Variants in Newborns Compared with adults, the kidney in newborns shows a more diffusely hyperechoic outer parenchyma (29)
with sharper contrast to the hypoechoic medullary pyramids (30). The triangular shape of the medullary pyramids is therefore more sharply defined in newborns than in adults, whose pyramids appear more rounded. Many neonatal kidneys also show residual fetal lobulation and gradually assume an increasingly smooth oval contour only later in infancy. The hyperechoic central renal caliceal system (31) initially appears as a thin line in newborns and only increases gradually in width during infancy. This is due to the increasing deposition of fat between blood vessels and calices. As a result the anechoic renal pelvis is more conspicuous in a newborn. It can measure up to 5 mm in width in the absence of any urinary obstruction (see p. 138). The "dromedary hump," a bulge in the left lateral renal cortex opposite the lower pole of the spleen, is also typical of the shape of the kidney in younger children and usually disappears as the organ grows. Hyperplastic columns of Bertin can traverse the hyperechoic pelvic region as hypoechoic parenchymal bridges, mimicking renal duplication (see Fig. 66.1). Neither finding has a mass effect, and neither should be confused with a renal tumor.
109
29
30 45
31 30
74 46
Fig. 136.1
a
b
Lumbar longitudinal section of the kidney
46
46
74
c
154
31
150 25
29 35
Fig. 136.2
a
b
Lumbar transverse section of the kidney
c
46
Lesson 9
Pediatrics: Kidneys 137
Diffusely Increased Echogenicity Diffusely increased echogenicity in the renal parenchyma in newborns is regarded as normal (see previous page). Yet even in later infancy it is a sign of parenchymal damage (Fig. 137.1). Findings then include renal parenchyma (29) that appears isoechoic or hyperechoic to the liver (9) and particularly to the medullary pyramids (30). Aside from glomerulonephritis, possible causes include diffuse leukemic infiltration and medication-induced damage such as can occur secondary to multiple chemotherapy (Fig. 137.2), shown here with nascent obstruction in the renal pelvis (31). Diffusely increased echogenicity in the kidney should invariably prompt the examiner to search for pleural effusion (see Fig. 55.3) and ascites in the true pelvis (Fig. 137.3). In the presence of proteinuria and hypoproteinemia, such findings suggest nephrotic syndrome. The example in Fig. 137.3 was intentionally selected to emphasize the risk of misinterpretation when the examination is performed after voiding. The bladder (38) is nearly empty after voiding, so that the ascites (68) adjacent to the small uterus (39) could easily be mistaken for the bladder.
Nephrocalcinosis The deposition of crystals that occurs in nephrocalcinosis initially creates a hyperechoic rim around the medullary pyramids, later extending to the caliceal
Height (cm)
m – 2 SD
Newborns < 55 55–70 71–85 86–100 101–110 111–120 121–130 131–140 141–150 >150
3.40 3.00 3.60 4.50 5.30 5.85 6.35 6.90 7.40 7.90 8.60
30
9 29
30
Fig. 137.1
b
29 30 30 31
4.16 4.35 5.00 5.90 6.60 7.10 7.65 8.20 8.70 9.25 9.95
30
30
30
31
150
Fig. 137.2
39
30
68 47
47 47 b
3
30
30 29
4.92 5.70 6.40 7.30 7.90 8.35 8.95 9.50 10.00 10.60 11.30
apices or diffusely throughout the pyramids. This inverts the contrast between these structures, with hyperechoic medullary pyramids and a relatively hypoechoic parenchymal rim. The calcifications initially show no acoustic shadowing. Possible causes include tubular acidosis, urate nephropathy with massive cell destruction in the setting of chemotherapy, vitamin D overdose, and therapy with ACTH or furosemide. The picture of diffusely hyperechoic medullary pyramids resembles that in a dehydrated newborn with protein precipitation. These deposits of Tamm–Horsfall protein are reversible within a few days when the newborn is rehydrated.
4 30
m + 2 SD
Table 137.1 Table of normal kidney sizes in children [9.3]
4 9
m
68
41
40
43 d
45
45
Fig. 137.3
38
77
b
47 45
74
Lesson 9
138 Pediatrics Urinary Obstruction and Reflux When the initial ultrasound screening examination of a newborn is performed, it is crucial to detect any stenosis of the ureteropelvic or ureterovesical junction or any vesicoureteral reflux with secondary obstruction so as to avoid any subsequent damage to the kidneys. Remember that the delicate anechoic renal pelvis (31) in newborns may be up to 5 mm wide (Fig. 138.1) in the absence of any urinary obstruction. Where the renal pelvis measures between 5 and 10 mm in width (Fig. 138.2), follow-up examinations at short intervals are indicated to clarify whether findings represent a congenital ampullary pelvis or a pathologic progressive dilation of the collecting system.
Only a renal pelvis exceeding 10 mm in width with clubbed calices (149) or a dilated ureter (150) are indications for an immediate diagnostic workup (Fig. 138.3). A voiding cystourethrogram is generally obtained (see next page). Width of the renal pelvis in newborns [9.3] Normal
< 5 mm
Follow-up indicated
5–10 mm
Suspected pathologic dilation
> 10 mm
Table 138.4
4
154
30
30
30
29 31 30
29 74
Fig. 138.1
30
b
29
Fig. 138.2
30
b
Where there is continuous dilation of the ureter (150) as in Fig. 138.3 and the renal pelvis (31), a ureteropelvic stenosis can be reliably excluded as the cause of the urinary obstruction. However, isolated dilation of the renal pelvis with or without caliceal clubbing should be further evaluated with a voiding cystourethrogram or
149
31
31
30 46
29
30
30
150
Fig. 138.3
b
intravenous urogram to exclude vesicoureteral reflux or stenosis of the ureteropelvic junction. The example in Fig. 138.3 shows a thinned parenchyma 29) due to urinary obstruction. Here, immediate diagnostic workup is indicated and possibly decompression as well.
Lesson 9
Pediatrics 139
Possible Sequelae of Urinary Obstruction When urinary obstruction is not detected early, it can lead to thinning of the parenchyma (29 in Fig. 139.2) and gradually progress to a shrunken kidney (see Fig. 67.3) with corresponding loss of renal function. Chronic urinary tract infections or metabolic disorders can also induce crystalline deposits ( ) in the dilated calices of the caliceal system (Fig. 139.3).
Grades of reflux in children Grade I Grade II Grade III Grade IV Grade V
Reflux into ureter only Reflux into pelvicaliceal system Additional beginning ureteral dilation and caliceal clubbing Increasing ureteral dilation and caliceal clubbing Pronounced ureteral dilation and beginning parenchymal thinning
Table 139.1
29 31 150 47 45
Fig. 139.2
a
45
Fig. 139.3
b
Voiding Cystourethrogram A voiding cystourethrogram excludes or confirms vesicoureteral reflux and should be performed in patients with recurrent urinary tract infections or urinary obstruction in the infection-free interval after antibiotic therapy. Normally (Fig. 139.4), even during voiding through the urethra ( ), the full bladder shows no retrograde reflux into the ureters ( ). The images are obtained in a slightly oblique projection to avoid misinterpreting the adjacent cortex of the ilium (imaged end on) as grade I reflux (into distal ureter only). Reflux into the caliceal system ( ) is referred to as grade II reflux (Fig. 139.5). Grade III is reached where there is extensive dilation of the ureter and beginning clubbing of the calices.
Fig. 139.4
Fig. 139.5
Grade IV reflux in children is characterized by increasing caliceal clubbing and ureteral dilation; grade V refers to cases where parenchymal thinning is also present (Table 139.1). The chronic end stage is characterized by tortuosity of the entire dilated ureter as seen in Fig. 139.6.
Benign Renal Tumors Aside from fibromas in neurofibromatosis (Recklinghausen's disease), benign masses in the pediatric kidney include angiomyolipomas, which occur in combination with Bourneville–Pringle disease (tuberous sclerosis) and resemble adult angiomyolipomas (see Fig. 71.1).
Fig. 139.6
Lesson 9
140 Pediatrics Nephroblastoma
Nephroblastoma (54) is the second most common malignant mass encountered in children (Figs. 140.1 and 140.2). Also known as Wilms' tumor, it leads to complete destruction of the normal renal anatomy and frequently exhibits an inhomogeneous hyperechoic internal structure and impairs urinary drainage from the remaining parenchyma (29) as in Fig. 140.3. It is important to examine the contralateral kidney to exclude bilateral involvement, which is observed in up to 10% of all cases.
a
29
13 44
29
54
29
54
13
45 45 b
45
45
45
Fig. 140.2
29
57
57
Fig. 140.1
4
47
30
54
29
5
a
a
b
Fig. 140.3
149 44
35 b
Lymphomatous Infiltration and Metastases appears as a Y shape craniomedial to the upper pole of the kidney. However, this difference in echogenicity disappears during infancy and adult adrenal glands are barely distinguishable from perirenal fat (see Fig. 67.1). In newborns, bleeding in the adrenal glands is usually visualized as a hypoechoic area ( ) at the upper pole of the kidney (Fig. 140.5). If this finding is indeed a hematoma, it should measurably decrease in size within a month. If its size is unchanged, laboratory tests or MRI must be performed to exclude a cystic neuroblastoma. Adenomas of the adrenal gland are less common. Because of their small size they are often detectable only on noncontrasted high-resolution CT densitometry studies.
Malignant infiltration of the kidneys from lymphomas or metastatic disease is less common. The difference in echogenicity between involved areas and normal renal parenchyma (29) may not be very conspicuous (Fig. 140.3), and some such lesions are identifiable only by central necrosis (57) or associated urinary obstruction in adjacent caliceal groups (149).
Adrenal Gland In newborns and preterm neonates, the hypoechoic adrenal cortex can invariably be distinguished from the hyperechoic medulla (155 in Fig. 140.4). On a posteroanterior scan, the adrenal gland typically
109 47
30 29
30
31
29 30
155 13
Fig. 140.4
a
b
Fig. 140.5
Lesson 9
Pediatrics 141
Patent Urachus In the newborn, the bladder is best examined in longitudinal and transverse suprapubic planes (Fig. 141.1a) as long as it is still filled (this means at the beginning of the examination!). Particular attention should be paid to the roof of the bladder (Fig. 141.1b) to avoid missing a patent urachus. This will appear as a hypoechoic channel ( ) along the anterior abdominal wall between the umbilicus ( ) and the roof of the bladder (Fig. 141.2).
Fig. 141.1
a
b
Hematoma and Cystitis
Ureterocele
In children, the most common masses in the bladder (38) are blood clots (52), which usually occur in the setting of hemorrhagic cystitis (Fig. 141.3). This child received chemotherapy in preparation for a bone marrow transplant. As in adults (Fig. 100.2), cystitis manifests itself as circular wall thickening (77).
In infants presenting with urinary obstruction, one must exclude a uterocele (151) in addition to stenosis at the ureteropelvic or ureterovesical junction. An ureterocele can project into the bladder lumen as a thin membranous structure (Fig. 141.4) that can change size and shape depending on the level of filling. This image also shows a dilated distal ureter (150).
a
a
1
2
a
1
2
3
3
47 74
46
51 38
38
77 74
45
52
45
Fig. 141.2
Fig. 141.3
b
Height [cm] Newborns < 55 55–70 71– 85 86–100 101–110 111–120 121–130 131–140 141–150 > 150
m – 2 SD 2.90 2.13 2.44 2.23 2.61 3.02 3.38 3.37 4.10 4.61 4.36
Fig. 141.4
b
Length of spleen [cm] m m + 2 SD 4.07 2.91 3.46 3.71 4.69 4.88 5.26 5.31 5.96 5.81 6.18
5.24 3.69 4.48 5.19 6.77 6.74 7.14 7.25 7.82 7.01 8.00
Table 141.1 Normal values for spleen size according to height [9.4]
74
151
77
150 43
47
43
b
Spleen Size in Pediatrics While the "4711 rule" applies to adults with the caveats discussed above, the size of the spleen in children is measured craniocaudally along the midaxillary line (not parallel to the intercostal space), and is specified relative to height (according to Weitzel, D.: Sonographic Organometrics in Childhood, Mainz).
Lesson 9
142 Pediatrics: Gastrointestinal Tract Pyloric Hypertrophy In pediatrics, the hypoechoic muscular layer of a term newborn up to 2 months old should not exceed 4 mm. The entire diameter of the pylorus should measure less than 15 mm. Pyloric hypertrophy is present whenever the transverse diameter (Fig. 142.1) exceeds these
values or the pylorus measures more than 16 mm in length in the longitudinal plane (Fig. 142.2). Failure to detect gastroduodenal passage of gastric contents substantiates the diagnosis.
Gastroesophageal Reflux To confirm an insufficient lower esophageal sphincter with esophageal reflux in children, the child should be examined after drinking a small amount of fluid or, if it is a newborn, with the stomach filled after nursing. In either case, the swallowed fluid invariably contains air bubbles (47) and will be visualized as hyperechoic motion within the stomach (26), often with comet tail artifacts or acoustic shadows (45 in Fig. 142.3). After the esophageal
hiatus of the diaphragm is identified in the proper sagittal plane (see Fig. 25.2), one observes the esophagus for some time with head-dependent table positioning to watch for retrograde passage of gastric contents through the cardia and into the esophagus. In adults, it is preferable to perform pulsed fluoroscopy after ingestion of an oral contrast medium.
1
3
74
2/5
3
m 22 m
5
9
7
5 mm
9
47
26 33
10
26
9
Fig. 142.1
74 b
9
5
Pyloric hypertrophy on a transverse section ...
26
74
12
Fig. 142.2
b
3
33 b
11
... and on a longitudinal section
45
74 5
Fig. 142.3
b
Hirschsprung`s Disease The distinguishing feature of Hirschsprung's disease is the aganglionic and therefore narrowed colonic segment with massive dilation of the colonic segment proximal to it (43), whose luminal width differs significantly from adjacent bowel loops (46 in Fig. 142.4). 74 74 Familial clustering involves boys in 46 46 about 80% of all cases. A typical funnel 74 -shaped junction is observed between the narrowed segment and the 45 megacolon. Often the dilated lumen 43 contains only a little intestinal gas (47) with distal acoustic shadowing (45), 47 46 allowing good sound transmission 45 through the retained fecal matter. b Fig. 142.4 a
Appendices
Primer of Ultrasound Findings
144
Index
148
Template for Report of Normal Findings
149
Diagram Templates for Standard Planes
150
Answers to Quizzes
155
Thanks to Contributors Hands-on Ultrasound Courses
159
List of Abbreviations
160
Examination Algorithms
161
References
166
Space for Your Notes and Drawing Exercises
167
144 Primer of Ultrasound Findings When communicating with experienced colleagues, novices are occasionally confused about which terms to use to describe findings clearly and concisely. This
A
B
brief review is intended as a guide to use until you have become more familiar with the common terms.
General Description of the Ultrasound Morphology of a Finding: Imaging plane?
Name the imaging plane (see front cover flap). Is the lesion visualized in the longitudinal or transverse plane?
Where?
Location, side, position within an organ or relative to other organs and vessels, i.e., central, hilar peripheral, subcapsular, adherent to the wall.
Number?
Lesions may be focal or unifocal, multiple, or diffusely distributed.
How large?
Specify in mm or cm. Important for follow-up examinations: Estimate progression or regression, such as can occur under therapy.
Shape?
Round, oval, spherical thickened.
Demarcation?
Sharp (likely benign) ill-defined (= sign of infiltration, as in inflammation or malignancy).
Echogenicity?
Anechoic (= homogeneous fluid), hypoechoic, or hyperechoic (possibly relative to surroundings).
Echo texture?
Homogeneous inhomogeneous, finely granular coarse, septated. Recently introduced categories also include elastic deformation (using special scanning technique).
Acoustic phenomena?
Acoustic shadow, edge shadow, total reflection, acoustic enhancement, section thickness, mirror image, side lobe, reverberation artifacts.
Expansion?
Displacement or infiltration of adjacent structures or vessels? Caution: Mass effects can also occur with benign cysts and are therefore not necessarily a sign of malignancy.
stellate, wedge-shaped, geographic, irregular,
Useful Terms (in alphabetical order)
(
application, possible meaning)
Ampullary
Developmental variant of the renal pelvis ( can mimic obstruction)
Delayed
Late splenic hemorrhage can occur after trauma
Anechoic
Black ( homogeneous fluids: blood, urine, bile, cyst contents, pericardial or pleural effusion)
Density
Term is occasionally used incorrectly. The echogenicity of a tissue on an ultrasound image has little to do with its physical density.
Artifacts
Visual findings lacking physical correlates
Depth Adjustment of gain) to sound compensation penetration depth
Biliary air
Air inclusions in bile ducts ( to papillotomy or abscess)
Diffuse
Distribution pattern, as in increased echogenicity
Bull's-eye sign
Concentric circles of alternating echogenicity ( intussusception; differential diagnosis: bowel wall inflammation)
Dissection
Complication (
Caliber change
Abrupt changes in caliber (diameter) of the branches of the portal vein ( cirrhosis of the liver)
Double-barrel Immediate adjacency of two anechoic shotgun sign ductal structures in the hepatic parenchyma ( dilation of intrahepatic ducts parallel to portal venous branches)
Capsule line
Thin hyperechoic border of an organ ( absent in cirrhosis of the liver)
Eccentric
Adherent to the wall ( location of thrombus in blood vessels)
Comet tail
Resonance artifact deep to pulmonary air or bowel gas
Echogenicity
"Brightness" of the pixels (increases with the number of impedance mismatches)
Concentric
At a pericentral location in a vessel ( thrombus or calcification)
Ectasia
Curtain trick
Respiratory maneuver ( improves visualization of the spleen)
Edge shadows Acoustic phenomenon occurring deep to the edge of the gallbladder and cysts
secondary
aortic aneurysm)
Dilation of the lumen of the abdominal
aorta > 2.5–3.0 cm
Primer of Ultrasound Findings 145 Fluke of a whale
Typical appearance of the celiac trunk in the transverse plane
Perifocal Plaque
FNH
Focal nodular hyperplasia of the liver
Polycyclic
Focal
Circumscribed lesion (focus)
Focal zone
Part of the image with the highest vertical resolution Respiratory maneuver ( vena cava collapse test) Overall amplification of ultrasound signal Hypoechoic rim of a lesion ( typical of hepatic metastases) Convex pouching ( typical of colon) Benignity criterion for lymph nodes Bright ( as in fatty degeneration of parenchymal organs) Dark, few echoes ( muscle, subcutaneous fat, parenchyma)
Forced inspiration Gain Halo Haustration Hilum fat sign Hyperechoic Hypoechoic Ill-defined
Demarcation ( criterion of infiltration in malignancy and inflammation) Impedance Interface between tissue layers with mismatch differing velocity of sound propagation that produces echoes Indentation Blunt, convex protrusion with displacement of adjacent structures ( tumors) Infiltration Spread into adjacent structures ( malignancy criterion) Inhomogeneous Irregular pattern of distribution or echogenicity Iris sign Jet sign Kinking L/T ratio Liquefaction LN Lobe of sound beam
Typical progression of enhancement in a liver hemangioma on spiral CT and contrast-enhanced ultrasound Inflow from the ureter into the bladder on color duplex sonography (intrastenotic and poststenotic acceleration of flow) Tortuous, angular course ( aortic aneurysm) Longitudinal diameter divided by transverse diameter ( malignancy status of lymph node) Usually anechoic ( as in the center of abscesses, metastases) Lymph node The acoustic wave front has a finite thickness section thickness artifact
Mass
Mass
Metastasis
Spread of a malignancy from one part of the body to another Having several foci in a single organ ( Typical finding in renal degeneration)
Multifocal Narrowing of renal parenchyma Necrosis
Hypoechoic, usually central area of liquefaction ( abscess or central metastasis)
Nodular
Multifocal distribution pattern of lesions
Nutcracker
Compression of the left renal vein by the aorta and superior mesenteric artery
Oscillating peristalsis Pennate
Back and forth motion of bowel contents Exhibiting parallel stripes ( pattern typical of muscles such as the psoas major)
PP index Predilection Pseudocysts Pulsation Rarefaction Respecting Reverberation
Marginal zone around a lesion Hyperechoic calcified zone in blood vessels Tuberous or resembling cauliflower ( structure of tumor in the stomach or bladder) Parenchyma to pelvis index ( kidney findings) Typical location of a lesion or abnormality ( Complication of pancreatitis) Simple ( arteries such as aorta), double ( veins such as inferior vena cava) Decreased vascularity ( cirrhosis of the liver) Failure to invade vascular structures is inconsistent with infiltrative growth ( benignity criterion) Repetitive echoes (artifact)
Section thickness Apparently ill-defined border of an artifact obliquely sectioned wall of a hollow organ ( important to consider in differential diagnosis of gallbladder sludge or bladder sediment) Septate, Anechoic hollow spaces are divided by septated hyperechoic lines ( cysts, cystic ovarian tumors, aortic dissection) Sharp Demarcation ( benignity criterion) Side-Lobe occurs in anechoic structures Artifact next to strong reflectors Sludge Hyperechoic sediment in the gallbladder Spoke-wheel Pattern of echogenicity ( focal nodular pattern shyperplasia of the liver, septation in echinococcal cysts) Starry sky Multiple hyperechoic focal lesions ( in tuberculosis of the spleen) Stenosis Narrowing of a vessel or hollow organ Stent Tube implanted to maintain patency of vascular stenosis String of Configuration of the medullary pyrpearls amids along the border between the parenchyma and renal pelvis, pattern of dilation of the pancreatic duct in pancreatitis Target sign Concentric circles of alternating echogenicity ( bowel intussusception) Thickening Variation in shape ( margins of the the liver in hepatic disorders) Total reflection A black shadow occurs deep to bone and air Trackball Triangular Vena cava collapse test Wall thickness Wedge-shaped
Important control device on the ultrasound unit Typical three-sided configuration ( organ infarcts) Examination maneuver in forced inspiration ( in suspected right heart failure) Diagnostic criterion ( in hollow organs, vascular structures) Pattern of increased parenchymal echogenicity ( typical pattern in infarct)
146 Primer of Ultrasound Findings The following list contains terms that are applicable to certain organ systems. For each organ, terms for spatial orientation are listed, followed by typical ultrasound changes that may provide information about the underlying disorder. Then any features and considerations specific to the organ are listed. This section is intended as a concise, time-saving review. Liver
Spatial terms • Subdiaphragmatic, subcapsular perihilar, central; specify segment (not only lobe), periportal, parahepatic, focal, diffuse Typical morphology Possible diagnosis • Diffuse increase in echogenicity Fatty liver • Diffuse loss of sound penetration with depth Fatty liver • Geographic, sharply demarcated differences in echogenicity around the gallbladder bed or near the portal bifurcation Focal fatty infiltration or focal sparing in fatty infiltration • Spherical anechoic and sharply demarcated lesions with edge shadows and distal acoustic enhancement Benign cysts • Septated cysts Echinococcosis (spleen involved?) • Singular or multiple lesions with hypoechoic rim (= halo) Metastases • Spherical hyperechoic and sharply demarcated lesion without halo Hemangioma • Double-barrel shotgun sign along portal vein branches Dilated intrahepatic bile ducts • Intraductal hyperechoic, oval lesions with acoustic shadowing Gallstones or air in the bile ducts • Absent capsule line, peripherally rarefied vessels, thickened organ edges and "pruned portal tree" Cirrhosis (shrunken liver only in late-stage disease)
Specific considerations • Differential diagnosis may require contrast harmonic imaging and elastographic techniques • Spiral CT or contrast-enhanced ultrasound: multiphase study with typical contrast enhancement pattern diagnostic of hemangioma: "iris sign" Gallbladder Spatial terms • Endoluminal, adherent to the wall, infundibular, fundal Typical morphology Possible diagnosis • Hypoechoic, multilayered, edematous wall thickening, possibly with perifocal ascites Acute cholecystitis • Hyperechoic intraluminal sedimentation Sludge (differential diagnosis: section thickness, reverberation, and side-lobe artifacts) • Hyperechoic, spherical to oval intraluminal lesion with distal acoustic shadowing Cholecystolithiasis • Focal wall thickening or hyperechoic lesion adherent to the wall without acoustic shadow Polyp Spleen Spatial terms • Subdiaphragmatic, subcapsular, central, perihilar, perisplenic, parasplenic Typical morphology Possible diagnosis • Thickened organ shape Splenomegaly in viral infection, lymphoma, or portal hypertension • Triangular or wedge-shaped area of decreased echogenicity Suggests infarct => color duplex sonography • Inhomogeneous patchy parenchyma Suggests lymphomatous infiltration • Parasplenic round mass isoechoic to spleen Accessory spleen, lymph node • Hypoechoic, bandlike discontinuity in the parenchyma, possibly with subcapsular hypoechoic fluid Suggests splenic rupture (free abdominal fluid?)
Pancreas Spatial terms • Head, uncinate process, body, tail, disseminated, peripancreatic, omental bursa (lesser sac) Typical morphology Possible diagnosis • Diffuse increase in echogenicity Lipomatosis • Hypoechoic edematous enlargement, applying pressure to transducer is painful, anechoic peripancreatic fluid may be present Acute pancreatitis • Organ atrophy with focal hyperechoic calcifications with acoustic shadowing, possibly with irregular dilation of the pancreatic duct Chronic pancreatitis • Anechoic, cystic cavity in the pancreatic region Pseudocyst (differential diagnosis: bowel loop) Specific considerations • Endoscopic ultrasound allows intraluminal visualization through the stomach Adrenal Glands Typical morphology Possible diagnosis • Unilateral or bilateral hypoechoic thickening Adenoma (differential diagnosis: metastasis) Specific considerations • Differential diagnostic modalities include dynamic densitometry using spiral CT (contrast washout curve) Kidneys Spatial terms • Parapelvic, pelvic, perihilar, subcapsular, parenchymal, cortical, pericapsular, polar, perirenal, at the pelvic–parenchymal border, unilateral, bilateral; do not forget to specify the side (body markers) Typical morphology Possible diagnosis • Homogeneous, anechoic, round to oval, sharply demarcated lesion with distal acoustic enhancement Cyst • Homogenous, hyperechoic, sharply demarcated, spherical lesion Angiolipoma • Row of round hypoechoic lesions without distal acoustic enhancement along the border between the parenchyma and renal pelvis resembling a string of pearls
Primer of Ultrasound Findings 147 Physiologic medullary pyramids • Hypoechoic pelvic thickening or prominent pelvis Urinary obstruction (differential diagnosis: pelvic cyst, ampullary renal pelvis) • Parenchymal thinning with PP index < normal and kidney size < 10 cm Renal atrophy • Inhomogeneous mass with expansion Suggests malignancy • Inhomogeneous patchy parenchyma Suggests infarct Specific considerations • Differential diagnostic modalities include densitometry on spiral CT and perfusion pattern on color duplex sonography • Ectopic kidney, horseshoe kidney • Accessory renal arteries Gastrointestinal Tract Spatial terms • Intraluminal, adherent to the wall; also specify abdominal quadrant for bowel Typical morphology Possible diagnosis • Bull's-eye or target sign (concentric structure of alternating echogenicity) Intussusception • Focal hypoechoic wall thickening with discontinuity of the layers of the wall Suggests malignancy (differential diagnosis: lymphoma, more likely disseminated than focal) Specific considerations • Hypotonic visualization of the gastric wall is possible using water as an anechoic intraluminal medium • Endoscopic ultrasound (of gastric and rectal wall) is an option • Peristalsis can be provoked by rapidly alternating pressure on the transducer Bladder Spatial terms • Intraluminal, adherent to the wall, intravesical, extravesical, perivesical, bladder floor, bladder roof Typical morphology Possible diagnosis • Hyperechoic material with gravitational sedimentation pattern Sludge, hematoma • Diffuse, hypoechoic wall thickening Cystitis
• Focal wall thickening, possibly extending into lumen as polypoid projection Suggests malignancy • Spherical, anechoic, sharply demarcated perivesical structure Bladder diverticulum • Hyperechoic intraluminal circle Balloon of indwelling catheter (rare differential diagnosis: ureterocele in children) • Suddenly appearing linear intraluminal inhomogeneity Jet sign from ureteral peristalsis and differing concentration of urine Specific considerations • Remember to clamp an indwelling catheter prior to examination so the bladder will be full and allow adequate evaluation of the bladder wall Vessels and Retroperitoneum Spatial terms • Paraaortic, retro-aortic, preaortic, paracaval, retrocaval, precaval, aortocaval, prevertebral, retrocrural, mesenteric, para-iliac, inguinal, cervical Typical morphology Possible diagnosis • Endoluminal material of varying echogenicity Thrombus • Diameter of thrombosed vein more than twice that of the accompanying artery Sign of acute thrombosis (< 10 days) • Dilated aortic lumen containing a hyperechoic membrane Dissected aortic aneurysm • Hypoechoic oval structure adjacent to a vessel Typical lymph node • Oval lymph node (L/T ratio > 2) with hilum fat sign Benignity criterion for lymph nodes • Homogeneously hypoechoic spherical lymph node (L/T ratio ~ 1) without hilum fat sign Typical of lymphoma (determine perfusion pattern on color duplex sonography) Specific considerations • Color duplex sonography often provides additional information Thyroid Gland Spatial terms
• Isthmus, lobes (specify side), subcapsular, at upper or lower pole Typical morphology Possible diagnosis • Isoechoic nodular lesions with hypoechoic rim Typical of adenoma • Cystic anechoic lesions, often multifocal Nodular transformation induced by iodine deficiency • Hypoechoic nodular lesions Suggest malignancy if scintigram shows cold (inactive) lesions • Normally hyperechoic parenchyma appears diffusely hypoechoic Hashimoto's thyroiditis • Thyroid enlargement with illdefined hypoechoic areas within otherwise normal echogenicity Subacute de Quervain's thyroiditis Specific considerations • Findings are often best interpreted together with scintigraphy and color duplex sonography
c
Checklists The third part of this review comprises the checklists and tables of standard values which are not repeated here to save space. They are listed on the pocket-sized cards and/or on the following pages: Subject
Page
Aortic aneurysm
27
Right heart failure
29
Acute and chronic pancreatitis
35
Normal values for the porta hepatis 41 Portal hypertension
42
Acute cholecystitis
45
Cyst criteria
55
Liver cirrhosis criteria
58
Normal renal values, PP index
65
Benign vs. malignant lymph nodes 84 Appendix, normal values
92
CSF spaces in newborns
124
Cerebral hemorrhage
129
Classification of infant hips according to Graf
135
Width of the renal pelvis in newborns
138
Grades of reflux in children
139
148 Index A Abscess 59, 120 Accessory spleen 76 Acoustic enhancement 18 Acoustic shadow 19 AcuNav 17 Acute transient synovitis of the hip 135 Adamkiewicz 27 Agenesis of the corpus callosum 126 Air bronchogram 120 Anatomy 24, 32, 40, 50, 64, 74, 80, 88, 98, 124 Aneurysm 27–28 Angiomyolipoma 71 Aorta 24–28 Appendicitis 92 Applying pressure 21 Artifacts 18–20 Ascites 12, 95 Atelectasis 118, 119, 121 B B lines in pulmonary edema 121 Bandwidth 9, 13 Barcode sign 115 Bile ducts 40, 41, 48 Blood clots 100, 141 Breathing instructions 20 Bronchial carcinoma 121 C Carotid plaque 17 Catheter 73, 100 Cavum of the septum pellucidum 126 Center frequency 9 Cerebral atrophy 124–126 Cerebral hemorrhage 129 Cervix 103 Cholecystitis 44–45 Cholestasis 47 Chorionic cavity 108 Choroid plexus 124 Cine loop 10 Cirrhosis of the liver 58 Clarity of detail 12 Colitis 93–94 Collapse test (inferior vena cava) 29, 52 Columns of Bertin 66 Common bile duct 40, 48 Compound imaging 15 Concretion 46, 70 Congested liver 51 Conn syndrome 71 Contrast agent 14, 58, 61 Contrast enema 91 Contrast harmonic 14 Costophrenic angle 51 Cruveilhier-Barmgarten disease 42, 43 CSF shunt 130 CSF spaces 124 Curtain trick (spleen) 75 Cystitis 100 Cysts 55, 66, 81–82 D De Quervain's thyroiditis 83
Delayed splenic rupture 77 Density 9 Dermoid cyst 107 Diagram templates for standard planes 150–154 Diarrhea 92 Dilation 27, 139 Dissection 27, 28 Diverticulitis 94 Doppler ultrasound 10, 13, 19 Double-barrel shotgun sign 47 Drainage catheter 48 Dromedary hump 66 Duodenum 33, 88 E Echinococcus 55, 77 Echo 8 Echogenicity 9 Ectasia 27 Ectopic pregnancy 108 Edge shadows 19, 46 eFAST 114–117 Elastography 86 Embankment 51, 54 Endometriosis 107 Endometrium 104 Endoscopic ultrasound 35, 103 Epididymitis 102 ERCP 48 F FAST 112–113 Fatty infiltration (liver) 54 Fatty liver 9, 53–54 Fecal impaction 93 Focal nodular hyperplasia (FNH) 57 Follicle 106 Foramen of Monro 124, 127 Freeze 10 Frequencies 8, 11 G Gain 10 Gallbladder 40, 44–47 Gallstones 47 Gel quantity 22 Gender determination 109 Goiter 82 Graafian follicle 106 Graves' disease 83 H Halo sign 60, 83 Harmonic imaging 13 Hashimoto's 83 Hemangioma 56, 77 Hematometra 105 Hepatic steatosis 54 Hepatic veins 52 Hepatitis 58 Hepatocellular carcinoma 59 Hernia 91 Hilum sign, hilum fat sign 84
Hip dysplasia 132–135 Hirschsprung's 142 Hodgkin 87 Hydrocele 102 Hydrocephalus 130 I Iliac vessels 26 Image generation 8 Impedance 8 Indwelling catheter 100 Inferior vena cava 24–26, 29 Infertility 106 Intercostal spaces 114–115 Intestinal intussusception 91 Intrauterine device (IUD) 104 Intussusception 91 Iodine deficiency 82 Iris sign 56 IUD 104 K Kidney failure 66 Kidney stones 70 Koller pouch 113 L L/T ratio 84 Legg–Calvé–Perthes disease 132 Lesser sac 33 Leukemia 37, 84–87 Light adaptation 12 Liver 49–62 Liver abscess 59 Liver cirrhosis criteria 58 Liver hemangioma 56 Liver metastases 60, 61 Lung mobility 116 Lung point 117 Lymph nodes 37, 84–87 Lymphocele 73 Lymphoma 87 M Medullary pyramids 65, 136–137 Megahertz 9, 11 Mesothelioma 119 Metastases 60–61, 121 Midline shift 117 Mirro-image artifact 19 Morison Pouch 112 Myoma 105 N Near-field resolution 11 Nephritis 67 Nephroblastoma 140 Nephrocalcinosis 70 Nephrolithiasis 70 Neurinoma 71 Newborns 136–141
Non-Hodgkin lymphoma 77, 87 O Operation 10 Orchitis 102 Orientation 21, 32 Ormond 68 Ovulation 106 P Pancreas 32-36 Pancreatic carcinoma 36 Pancreatitis 35 Panorama image 12, 15 Parasites 55 Partial loss of volume 118 Penetration depth 10–11 Pericardial effusion 112 Peristalsis 87, 92 Peritoneal carcinosis 35 Phase inversion 13 Piezoelectric effect 9 Placenta position 109 Plaque 15 Pleural effusion 12, 118–119 Pleural empyema 119 Pleuritis 119 Plexus cysts 126 Pneumonia 120 Pneumothorax 114–117 Polyps 46 Porta hepatis 40–41 Portal hypertension 42–43 Portal vein 40–43 Portal vein thrombosis 43 Position of lumen 27–28 Postvoid residual bladder volume 99 Pouch of Douglas 100, 106, 112 Pouch of Morison 112 Precision up-sampling 16 Pregnancy testing 108 Primer of ultrasound findings 144–147 Prostate carcinoma 101 Pulmonary abscess 120 Pulmonary edema 121 Pulmonary metastases 121 Pulmonary pulse 116 Pulsatility index (PI) 85 Pulse compression 16 Pyloric hypertrophy 142 Q Quantifying pleural effusions 118 Quizzes for assessing progress 30, 62, 78, 95, 110, 122 R Rarefaction 58 Reflux 138–139, 142 Rejection reaction 73 Renal atrophy 67 Renal carcinoma 71 Renal cyst 66 Renal duplication 66, 136 Renal infarct 67, 70 Renal transplant 72–73
Template for Report of Normal Findings 149 Retroperitoneum 23–38 Reverberation 18 Reverberation artifact 18, 115 RI (resistance index) 85 Rib fracture 120 Ribs 114, 120 Right heart failure 29, 52 Risk of rupture 27 S Seashore sign 115 Section thickness artifact 18 Segments of the liver 50 Shrunken liver 58 Side lobe 20 Side-lobe artifact 20 SieScape 12 Sludge 46 SonoCT 15 Sonovue 14 Sound waves 8 Spatial orientation 21, 98 Spinal canal 131 Spleen size 142 Splenic infarct 76–77 Splenic rupture 77, 113 Splenic vein thrombosis 35 Splenomegaly 76 Starry sky spleen 77 T Tables of normal values: aorta 27, inferior vena cava 28, portal vein 41, kidney 65, spleen 141, appendix 92, CSF spaces 124, thyroid gland 80, Hip 135 Target sign 90–91 Target sign 91 Tension pneumothorax 117 Testis 101–102 Tethered cord syndrome 131 Thyroid carcinoma 83 Thyroiditis 83 Total gain 10 Total reflection 8 Trabeculated bladder 100 Trackball 10 Transducer pressure 21 Transit study 89 Types of transducers 11 U Ultrasound of the skull 124–130 Umbilical hernia 91 Undescended testis 102 Upper GI study 89 Urachus 141 Ureter dilation 139 Ureterocele 141 Urinary obstruction 68, 138–139 Uterine carcinoma 105 V Varicocele 102 Vascular rarefaction 58 Venous star (liver) 52 Volume formula 99
The Ultrasound Agreements valid since 1 April 2017 pursuant to § 135, paragraph 2, of the German Social Code, Vol. V, stipulate that at minimum the medical documentation must mention the patient's identity (name and age), the examiner's identification, the date of the examination, the line of inquiry, in applicable cases limited visualization, and a description of findings specific to the organ (except in the case of normal findings). Additionally, the diagnosis or tentative diagnosis and the diagnostic and/or therapeutic consequences deduced from that diagnosis must be stated. Below you will find a template for report of normal findings which should be adapted and/or supplemented as the individual case requires. Template for report of normal findings for patient ______________________________ Date of birth _________________ The examination was performed with/without contrast agents with a _______ MHz transducer/with the following additional technology: THI / CHI / SonoCT/ CEUS ___________ Retroperitoneum: The retroperitoneum is well visualized without evidence of lymph node enlargement or other pathologic masses. Aorta and inferior vena cava are unremarkable. Pancreas: The parenchyma is homogeneous without evidence of focal lesions or inflammation. The size of the pancreas is within the normal range/ ______, with the head measuring _______ cm, the body ____________ cm, and the tail _______ cm. The pancreatic duct is normal/cannot be visualized / ____________ and measures ______ (Delete inapplicable text.) Liver: The liver is of normal size and shape and exhibits a smooth border. The parenchyma is homogeneous without evidence of focal masses. Echogenicity is normal. Intrahepatic biliary ducts and vessels appear normal. Gallbladder and bile ducts: The gallbladder is of normal size and ductal diameter without evidence of inflammatory wall thickening, stones, or sludge. The common bile duct is completely visualized / visualized as far as _____________. The beds of both adrenal glands are unremarkable without evidence of a mass. Kidneys: Both kidneys are well visualized, show normal respiratory mobility, and are of normal longitudinal size, with the right kidney measuring _____ cm and the left kidney _____ cm in length. The parenchyma is homogeneous and of normal width in both kidneys. The PP index of the right kidney is 1:_____ and of the left kidney 1:_____. No evidence of calculi, congestion, or pathologic masses. Spleen: The spleen is normal in size for the patient’s age, measuring _____ cm in length and _____ cm in width, and exhibits a homogeneous parenchyma. No evidence of focal lesions on the plain ultrasound scan / application of __________reveals_______________. Abdominal Cavity: No evidence of free fluid. Gastrointestinal Tract: The thickness of the gastric wall is within the normal range, measuring _____ mm. No evidence of focal thickening of the wall of the stomach, small bowel, or colon. Normal peristalsis was observed. Bladder: The wall has a smooth contour and normal thickness, measuring _____ mm. Normal postvoid residual bladder volume of _____ mL. No evidence of calculi, diverticula, or ureterocele. Reproductive Organs: The uterus is of normal size for the patient’s age, measuring _____ x _____ cm. The thickness of the endometrium multiplied by 2 is _____ mm. No evidence of retained secretion or focal masses. No evidence of free fluid in the pouch of Douglas. The ovaries are well visualized / not visualized on the (right / left) and are of normal size; the right ovary measures _____ x _____ cm and the left ovary _____ x _____ cm. The prostate gland is homogeneous and of normal size, measuring _____ x _____ x _____ cm. No evidence of focal masses or calcifications. The seminal vesicles are unremarkable. Conclusion: Unremarkable normal findings in the abdomen and retroperitoneum. (Don’t forget to address the clinical line of inquiry. Delete inapplicable text.) Remarks: _______________________________________________________________
150 Diagram Templates for Standard Planes On the pages with the quiz questions, I suggested the approach of using drawing exercises to help you memorize tomographic anatomy. How is this supposed to work? It works with surprisingly little effort: The idea is to draw and label specific standard planes from memory (in the cafeteria on a napkin during a coffee break, or at night on any piece of paper) with long intervals in between. Do not spend more than two minutes on this exercise!
1.
Sagittal upper abdomen, left paramedian plane (AO)
3.
Oblique lower abdomen, para-iliac plane
5.
Transverse upper abdomen (renal vein crossing)
Then fill in your gaps using the diagram templates copied from this page. You just have to keep these copies with you (in your lab coat pocket). Only begin a new attempt after this exercise has left your short-term memory (> 2–4 hours). You will be surprised how few attempts it takes to master the tomographic anatomy if you pursue these tasks with a little determination. Have fun with it . . .
2.
,45°
Sagittal upper abdomen, right paramedian plane (IVC)
4.
Transverse upper abdomen (celiac trunk)
6.
Oblique right upper abdomen (porta hepatis)
Please label the vessels and organs yourself when doing these exercises so that you can better memorize them. The solutions, which structure corresponds to which organ or vessel, can be found on page 151.
Diagram Templates for Standard Planes 151 To help you memorize topographic anatomy as effectively as possible, you can compare the figures shown here to the diagram templates on page 150. If in doubt, you can use the legend on the back cover flap to quickly check the numbers and see which structure corres-
1.
2.
1 2
34 47
13
25 b
15
11 18 66
46
24 a
35
16
114
35
45
47
2
Sagittal upper abdomen, right paramedian plane (IVC)
4.
1
1
2 3
3
7
21
8
21 a 22 a
22
46
9
16 13 35
Oblique lower abdomen, para-iliac plane
6.
46
24 a
13
3 74 26
33 b 33 a 12 17 16
11 11
33 c
13
66
18 46
26 33 20 15
9
16
25 b 24 b
Transverse upper abdomen (renal vein crossing)
17 25 b
11 20
15 35
7
10
8
9
20
15
1
2
3 7
33
19
Transverse upper abdomen (celiac trunk)
1
2
32
11
21 b
35
26
18
22 b
5.
33
9a
17
Sagittal upper abdomen, left paramedian plane (AO)
26
10
35
3.
< 45° 9
23
33 12
32
2
47
26
32 a
3 13
3
9
13
ponds to which respective organ, muscle, or vessel. Your retention of this material depends heavily on the number of times you do these active drawing exercises and the time intervals between repetitions. Good luck!
24 a
35
13
Oblique right upper abdomen (porta hepatis)
152 Diagram Templates for Standard Planes These diagrams naturally represent idealized situations, and the structures they show are not always visualized in the same plane in every patient. Yet this is not important. What matters is that you know where to look for, say, the pancreas or the origins of the renal arteries in obese patients with limited sonographic visibility. Most physicians are visual learners, and you are most likely one
as well. With time, you will develop a "visual template" of the normal findings in every standard plane, and you will immediately notice any deviation ("something doesn’t look right here"). That is the goal. You can even go one step further and write in the normal values where you find double-headed arrows ( ). This will help you to memorize these values as well.
We have included a minor mistake for the advanced reader on this page. Can you find it?
7.
Right oblique subcostal plane (hepatic veins)
9.
Transverse plane (right kidney and IVC)
11.
Median sagittal suprapubic plane (bladder and uterus)
8.
Longitudinal transhepatic plane (right kidney)
10.
High plane of the left flank (spleen)
12.
Transverse suprapubic plane (bladder and prostate gland)
The solutions, where to find which organ or vessel, can be found on the next page.
Diagram Templates for Standard Planes 153 Here you will find the solution to which structure on page 152 corresponds to which respective muscle, organ, or
7.
8.
1
2 3
vessel. If anything is unclear, you can check the numbers in the legend on the back cover flap.
2
1
4 9
10
13
13
Right oblique subcostal plane (hepatic veins)
10.
3
10
46
33
13
24 a
15
74
26
20
48
3 46
12.
1 6
2 3
51 a
38 41
46
High plane of the left flank (spleen)
46
77
78 46
47
44
51 a
45
45 33
35
1
39
37
25 b 24 b
Transverse plane (right kidney and IVC) 2
13
26
17
14
12 16
30
116
1
2
43/46
80
33
29
35
13
Longitudinal transhepatic plane (right kidney)
1
9
44 5
47
47
2
30 31
9
45
16
11.
45
29
9
9.
43
40 122
Median sagittal suprapubic plane (bladder and uterus)
38
43 d
45
77 70
42 43 d
Transverse suprapubic plane (bladder and prostate gland)
45
154 Diagram Templates for Standard Planes Here you find three additional standard planes for your drawing exercises from the transverse plane of the thyroid, the subxiphoid plane of the four chambers of the heart, and sagittal parasternal sections of the lung. The
13a.
solutions, which area corresponds to which vessel or muscle, etc., are shown directly opposite in four-color figures. The key to the respective numbers can be found in the legend on the back cover flap.
13b. 1 2 a 85
84
81
83
169 82
2 90
169 82
35
85
5
81
34 88
88
89
88
83 88
Transverse section at the level of the thyroid
14a.
14b.
1 2
3 79 13
79 114 115
114
115
114
114
47
79
47
Transverse subxiphoid section of the heart
15a.
15b.
1 2 109
117
116
109 101 45
45 47
Sagittal thoracic plane
47
Answers to Quizzes 155 Answer to Fig. 20.4
1
2
The image shows a longitudinal section of the aorta (15). Its wall contains hyperechoic calcifications (arteriosclerotic plaques, 49), with posterior acoustic shadows (45). The larger plaque could have been easily overlooked without the acoustic shadow because it is located immediately adjacent to hyperechoic (= bright) bowel gas (46), which also creates an acoustic shadow. Below (= posterior to) the aorta (15) we also see the phenomenon of distal acoustic enhancement (70).
9
64 49
46
70
15
70
45 45
Answer to Fig. 21.1
5/6
9
45
Fig. 155.1
Prior to beginning the practical sessions, you should become familiar with spatial orientation in a three-dimensional space. To make the first step easy, we will initially consider only two planes perpendicular to each other: the vertical (sagittal) plane (Fig. 155.2) and the horizontal (transverse) plane (Fig. 155.3). Sagittal planes On page 21 you were asked to use a Anterior coffee filter to help picture how the sound waves propagate through the body when the transducer is placed on the anterior abdominal wall. Both Cranial Caudal planes display the anterior abdominal wall at the upper edge of the image (up = anterior). As the conPosterior vention is to view all sagittal images from the patient’s right side (Fig. b 155.2a), the patient’s cranial struc- Fig. 155.2 a tures are displayed at the left edge of the image (left = cranial) and the Transverse planes caudal structures at the right edge. Anterior Rotate the transducer 90° counterclockwise to place it in the transverse plane. As this plane is viewed from below (caudal) all the structuRight Left res are reversed (left = right, Fig. 155.3b). The same imaging convention is used for transverse planes in Posterior CT and MRI. It all makes good sense: If you stand at the foot of the bed b before a supine patient, the patient’s Fig. 155.3 a liver (on the patient’s right side) will be on the left in your field of view. Only neurosurgeons prefer to view CT images of the cranium from above as this corresponds to their intraoperative perspective.
Answers to Figs. 22.4–22.6 When viewing these three images, it is apparent on the left image that the structures on the whole are more poorly visualized than usual. The image in Fig. 22.4 seems blurred and is diffusely obscured by scatter. This is due to the typical beginner’s error of applying insufficient pressure to the transducer, not too little gel. If the amount of gel is indeed inadequate or the examiner breaks the skin coupling by tilting the transducer, an image like that shown in Fig. 22.5 will result: A black
band appears along the margin of the lost coupling (here on the right side of the image) beginning immediately at the skin-transducer interface and not only in a deeper plane. This finding distinguishes lost skin coupling from acoustic shadows behind ribs, bowel gas, gallstones, or renal calculi. In Fig. 22.6 the same plane in the same patient was imaged a few seconds later with better coupling and sufficient pressure on the transducer. All structures are visualized far more clearly.
156 Answers to Quizzes Answer to Fig. 30.2 (Question 6) Answer to Fig. 38.1 (Question 4) Answer to Fig. 62.4 (Question 6) 3
1
2 2
3 9 13 11
10
5
79
45
8
33
6 9
9
11 45
7 33 a 12
16
13
80 25
80
9
33 c
45
29
24 b 35
13
46
11
20
15
24 a
Imaging plane: Sagittal upper abdomen, paramedian plane over the inferior vena cava (16) Organs: Liver (9), heart, and pancreas (33) Structures: Diaphragm (13), hepatic vein (10), portal branch (11), caudate lobe (9a) Significant finding: Anechoic space (79) between myocardium/epicardium and diaphragm Diagnosis: Pericardial effusion (79) Differential diagnosis: Epicardial fat
26 33 b
16
2 9
3
17
1
3
13
31
13
Imaging plane: Transverse section at the level of the renal vein crossing Organs: Liver (9), stomach (26), and pancreas (33) Vessels: Aorta (15), inferior vena cava (16), renal artery (24), renal vein (25), superior mesenteric artery (17), confluence of the portal vein (12) Structures: Ligament (7, 8), rectus abdominis muscle (3), lumbar vertebra (35) Significant finding: Prominent lumen of the renal vein (25) Diagnosis: Still physiologic, no pathologic dilation of the left renal vein (due to nutcracker syndrome between 15 and 17)
Imaging plane: Right oblique subcostal plane Organs: Liver (9), gallbladder (80), kidney (29) Significant finding: Inhomogeneous, poorly demarcated area along the caudal margin of the liver Diagnosis: Cholecystitis with marked wall thickening (80) Differential diagnosis: Parasitic involvement of liver or gallbladder, sludge, bowel content
Answer to Fig. 62.1 (Question 7) Answer to Fig. 62.2 (Question 7) Answer to Fig. 62.3 (Question 7) 1
2
2
3/4
5
26
11
3
47
9
5
9
10
63
56
56
45 46
27 13
45
5 11
56
47 47
56 9
29
13
35
Imaging plane: Right oblique subcostal plane Organs: Liver (9), stomach (26), small bowel (46) Significant finding: Homogeneous, hyperechoic, sharply demarcated area (63), multiple round to oval intrahepatic lesions with hypoechoic rim Diagnoses: Focal fatty infiltration (63) and multiple hepatic metastases (56) with at least two episodes of metastatic spreading as new and older metastases are visible next to each other
45
69
Imaging plane: Sagittal plane along the right midclavicular line Organs: Liver (9), kidney (29), lung (47) Diagnosis: Subdiaphragmatic hepatic metastasis (56) with hypoechoic rim and pleural effusion (69) Differential diagnosis: Hyperechoic appearance suggests hemangioma, but the halo is inconsistent with this
61 45 13
9
13
Imaging plane: Sagittal upper abdomen, right paramedian plane Organs: Liver (9), lung (47), diaphragm (13) Significant finding: Hyperechoic, partially inhomogeneous intrahepatic mass Diagnosis: Hemangioma (61) with draining vein (10) Differential diagnosis: Hyperechoic metastasis, hepatic tumors of other origin
Answers to Quizzes 157 Answer to Fig. 78.1 (Question 5) Answer to Fig. 78.2 (Question 5) Answer to Fig. 78.3 (Question 6) 1
46
9
29
28
45
26
54
33
24
31
17
31 29
64
5
9
9
29
3
46
4
13
2
4
2 2
45
45
15
16
54
45 55
27
47
45
70
Imaging plane: Intercostal plane of the right flank Organs: Liver (9), kidney (29), lung (47), bowel (46) Structures: Diaphragm (13), renal pelvis (31) Significant finding: Anechoic, spherical, sharply demarcated lesion (64) at the upper pole of the right kidney, with distal acoustic enhancement (70) Diagnosis: Renal cyst (64) Differential diagnosis: Adrenal tumor with cystic components
35
Imaging plane: Intercostal plane of the right flank in left lateral decubitus position Organs: Liver (9), bowel (46) with acoustic shadow (45), kidney (29) Structures: External and internal oblique muscles (4), upper and lower poles of the kidney (27 and 28) Significant finding: Ill-defined hypoechoic lesion (54) in the renal parenchyma (29) with mass effect Diagnosis: Renal cell carcinoma Differential diagnosis: Renal lymphoma, metastasis, hypertrophied column of Bertin, hemorrhagic renal cyst
Imaging plane: Transverse upper abdomen in an infant Organs: Liver (9), pancreas (33) Significant finding: Poorly demarcated organs and large, inhomogeneous tumor (54) in the right paravertebral region. The tumor displaces the right renal artery (24) anteriorly over a long segment. Suspected lymph node metastasis (55) between the aorta (15) and lumbar vertebra (35) Diagnosis: Metastatic nephroblastoma Differential diagnosis: Neuroblastoma of the right sympathetic chain
Answer to Fig. 78.4 (Question 10) Answer to Fig. 95.1 (Question 6) Answer to Fig. 110.1 (Question 4) 4 47
2 43
5
4
2
1
45
54 54
45
74
74
37 45
45
45 46
45
78
45 46
18 mm
43c 74
13
37
47
Imaging plane: High plane of the left flank in the right lateral decubitus position Organs: Spleen (37), lung (47), colon (43), diaphragm (13) Significant finding: Several sharply demarcated homogeneously hyperechoic lesions (54) in the splenic parenchyma without a hypoechoic rim Diagnosis (rare finding): Multiple splenic hemangiomas Differential diagnosis: Hyperechoic metastases, vasculitis in systemic lupus erythematosus, histiocytosis X
5 46
5
39
46 74
Imaging plane: Sagittal plane of the left flank Organs: Colon (43), small bowel (46) oblique muscles (4) Significant finding: Thickening of the colonic wall (74) Diagnosis: Ischemia of the bowel wall Differential diagnosis: Colitis, colon carcinoma
9 43d
Imaging plane: Endovaginal view of the uterus Organ: Uterus (39) Significant finding: Inhomogeneously hyperechoic endometrium (78), widened to about 18 mm in a menopausal woman without hormonal therapy (see question). Diagnosis: Suspected endometrial carcinoma Work-up: Fractionated dilation and curettage for histologic evaluation
158 Answers to Quizzes Answer to question on page 56:
2
4
5
68
Fig. 56.3a shows two pathologic fluids: 68 = Ascites caudal to the diaphragm 69 = Pleural effusion cranial to the diaphragm has led to compressive atelectasis of the basal segments of the lung (47) 61 = Hemangioma with draining veins (10)
9
47
61
13 45
68
9
47
Fig. 158.1
a
10
69
13
b
Answer to Question on the Upper GI Series on Page 89 Gravity causes the contrast medium (white) to collect in the more posterior fundus and in the pylorus and duodenum. The more anterior body of the stomach is easily evaluated on a double-contrast study. The patient is therefore supine. If the examiner wants to evaluate the gastric fundus, the table must be adjusted to bring the patient into a more upright position or the patient must be placed in the right lateral decubitus position to cause the contrast medium to flow out of the fundus.
To visualize the duodenal bulb on the right side, the patient must be placed in a left lateral position. Please remember to register your patients only for an early morning upper GI series (in a fasting patient) and note that gastric peristalsis may need to be suppressed by medication (beware of the side effects of intravenous scopolamine methylbromide!) to achieve a reliable result. It is advisable to tell patients beforehand to try not to belch and release the air produced by the effervescent powder. How else will they know?
Answer to Question on Page 107
Answer to Question 1 on Page 122
Fig. 103.2b illustrates the anatomic orientation on endovaginal images. The right edge of the image is posterior. The blood clot in the supine patient therefore appears on the right edge of the image in Fig. 107.3 as gravity brings it to rest in a posterior location.
FAST position 2 allows one to exclude liver lacerations, hemorrhage into the pouch of Morison, and right hemothorax. FAST position 3 covers ruptures of the spleen, hemorrhage into the pouch of Koller, and left hemothorax.
Answer to Question 3 on Page 122 The three conditions for demonstrating the pulmonary pulse are a fully expanded lung (on the side being scanned), the presence of an arterial pulse (cardiac output), and respiratory standstill or briefly interrupted artificial respiration, for example with the "inspiration hold" key pressed.
Answer to Fig. 122.1 (Question 4)
Answer to Fig. 122.2 (Question 5) 1
1
2
2
116
117
118 56
116 69
71
47
47 45
Imaging plane: Thoracic intercostal plane Organ: Lung (47) Structures: Chest wall (1, 2, 116, 117) Significant finding: Hypoechoic region (71) near the pleura Diagnosis: Peripheral pulmonary infarct Differential diagnosis: Peripheral bronchial carcinoma; therefore perfusion imaging with color duplex sonography is indicated
45
Imaging plane: Thoracic intercostal plane Organ: Lung (47) Structures: Chest wall (1, 2, 116) Significant finding: Hypoechoic, solid visualization of large areas of the lung (118) with even less hypoechoic focal lesions (56) Diagnosis (rare finding): Postobstructive atelectasis with liquefied metastases
Thanks to Contributors / Hands-on Ultrasound Courses 159 This revised and expanded edition could not have been realized without the support of numerous helpers. Since 1991, more than 15,000 course participants and 300 ultrasound instructors have contributed to the continuing optimization of this book in systematic evaluations with their feedback and constructive criticism. I wish to thank them all. I would specifically like to mention the following persons and institutions: I am indebted to Ramona Sprenger for the excellent graphic production including the integration of colored diagrams by Willi Kuhn and for the entire layout of the book, based on the previous drafts by Inger Wollziefer. Jochen Neuberger and Michael Zepf of Georg Thieme Verlag have contributed decisively to ensuring that the production and combination with the new media server have gone smoothly and efficiently. We cordially thank Samsung and Marburger Bund Foundation for their continuous support of our ultrasound courses for our physician colleagues (see below). Alexis Müller-Marbach, MD has contributed many new exemplary images from gastroenterology, Georg Groß, MD several pulmonary ultrasound images, Prof. C.F. Dietrich Fig. 57.2, Christoph Sproll, MD several images on the differential diagnosis of lymph nodes. I thank my colleagues Jörg Schaper, MD, H.D. Matthiessen, MD and
Jasmin D. Busch, MD for valuable information regarding ultrasound examination of the infant hip. I cordially thank my wife Stefanie Ole Martin, MD and Christian Weigel, MD for their critical review and additional creative suggestions. Finally, I would like to thank the 38 current ultrasound trainers of our Working Group Medical Didactics and honor their willingness to provide ongoing, intensive, video-supported continuing education: Bastian Benner, Franca Bergfelder, Jonathan Brück, Klemens Freitag, Ira Gabor, Arnd Giese, Fabian Girke, Stephanie Göller, Lisa Haddad, Elisabetha Hahn, Tessa Hattenhauer, Annika Hogrebe, Anna-Lena Hotze, Maike Hüssmann, Kai Jannusch, Anne Jäckel, Marie Klar, Kathrin Klein, Shining Liu, Nicole Majewski, Jean-Luc Niederst, Alice Martin, Ole Martin, Felix Mohr, Sara Naisar, Johanna Noelle, Ralf Rulands, Nora Schlecht, Stefan Schmidt, Thomas Schmidt, Rene Stegemann, Isabell Stetter, Richard Truse, Rebecca Voigt, Elena van Loon, Christian Weigel, Daniel Weiss, Björn Wieland. Bern, Summer 2020 Matthias Hofer, MD, Associate Professor, MPH, MME (Director of Education at DIPR, University of Bern)
Information on hands-on ultrasound courses Even comprehensive textbooks will never be able to provide the necessary opportunity to practice how to handle the transducer or to convey how best to deal with patients in an ultrasound examination. We therefore recommend combining this book with the included video clips and with ultrasound courses in which one can acquire sound and systematic knowledge of this elegant diagnostic method under qualified supervision. In cooperation with Marburger Bund Foundation, the editor offers ultrasound courses for physicians. This manual is also intended as introductory reading for these ultrasound courses; it has gradually developed from approximately 30 years of classroom experience with students and physicians. These courses are also offered in English and are characterized by a high proportion of hands-on exercises and a favorable student to teacher ratio: A maximum of five participants share an ultrasound workplace under the supervision of a specially trained instructor. These small groups are one of the key factors contributing to a successful learning experience. Information about dates, course content, registration formalities, and course fees are available from this web site:
www.medidak.de Additional courses are available for those who would later like to go one step further and enter the world of color duplex sonography. Interdisciplinary elementary courses providing an introduction to color duplex sonography are designed according to the same quality criteria with respect to teaching and method. They are held in Düsseldorf (in German) and on request also at other locations in English. A manual entitled "Teaching Manual
of Color Duplex Sonography, Stuttgart: Thieme; 2010" is also available to accompany this course. Both courses share a common structure. Brief theory modules are integrated intermittently into longer practice modules, and drawing exercises consolidate the student's understanding of tomographic anatomy and typical vascular flow patterns. More specific literature on the subject may be found here: Hofer M, Kamper L, Heussen N, Martin O, Heverhagen J. Relevance of clinical expertise between clinician versus student instructors on ultrasound course efficiency. Ultraschall Med 2020 in press. N. Nourkami-Tutdibi N, Tutdibi E, Schmidt S, Zemlin M, Abdul-Khaliq H, Hofer M. Long-term knowledge retention after peer-assisted abdominal ultrasound teaching: Is PAL a successful model in obtaining knowledge retention? Ultraschall Med 2020; 41(1): 36-43 Hofer M, Kamper L, Miese F et al. Quality indicators for the development and didactics of ultrasound courses in continuing medical education. Ultraschall Med 2012; 33(1): 68–75 Hofer M, Kamper L, Sadlo M, Sievers K, Heussen N. Evaluation of an OSCE-assessment tool for abdominal ultrasound courses. Ultraschall Med 2010; 32: 1–8 Hofer M, Jansen M, Soboll S. Potential improvements in medical education as retrospectively evaluated by candidates for specialist examinations. Dtsch. Med. Wschr. 2006; 131: 373–378 Hofer M, Schiebel B, Hartwig H-G et al. Didactic training of ultrasound instructors. Ultraschall Med 2002; 23: 267–273
160 List of Abbreviations
AAL
Anterior axillary line
EFW
AC
Abdominal circumference
ACTH Adrenocorticotropic hormone
ERCP Endoscopic retrograde cholangiopancreatography
AIUM American Institute of Ultrasound in Medicine AO
Aorta
ASD
Atrial septal defect
AP
Anteroposterior
Estimated fetal weight
MRI
Magnetic resonance imaging
mW
Milliwatt
ESWL Extracorporeal shock wave lithotripsy
NHL
Non-Hodgkin lymphoma
NT
Nuchal translucency (fetal)
FAST
Focused assessment with sonography for trauma
PA
Posteroanterior
FCC
Fetal cranium circumference
PAL
Posterior axillary line
FL
Femur length (fetus)
PCO
Polycystic ovaries (syndrome) Pulsatility index
AVHR Ratio of anterior horn with to width of ipsilateral hemisphere
FNH
Focal nodular hyperplasia
PI
FOD
BBrightness mode (black mode and white) ultrasound
Fronto-occipital diameter (fetus)
PP Parenchyma to index pelvis index
FW
Fetal weight
PSL
GI tract
Gastrointestinal tract
GW
Gestational week
PVHR Ratio of posterior horn width to width of ipsilateral hemisphere
HCG
Human chorionic gonadotrophin
PW
Pulsed wave (Doppler)
RI
Resistance index
Cholecystectomy
ICS
Intercostal space
RLD
CCL
Chronic lymphatic leukemia
IHW
Interhemispheric width
Right lateral decubitus (position)
CCW
Craniocerebral width of the subarachnoid space
IUD
Intrauterine device
SAS
Subarachnoid space
IVC
Inferior vena cava
SCW
Color duplex sonography
IVF
In vitro fertilization
Sinocortical width of the subarachnoid space
CEUS Contrast-enhanced ultrasound
IVU
Intravenous urogram
SD
Standard deviation
LA
Lower abdomen
SLE
Systemic lupus
CHI
Contrast harmonic imaging
LN
Lymph node
CNS
Central nervous system
SMA
Superior mesenteric artery
CRL
Crown–rump length (fetus)
THI
Tissue harmonic imaging
CSF
Cerebrospinal fluid
L/Tratio Longitudinal diameter divided by transverse diameter
UA
Upper abdomen
Computed tomography
LVW
Lateral ventricle width
VE
Vascular enhancement
Continuous wave (Doppler)
m
Mean
VHR
Ventriculohemispheric ratio
Diameter or thickness
MA
Midabdomen
dAO
Aortic diameter
Midclavicular line
VolB
Volume of the bladder
MCL
VSD
Ventricular septal defect
DSA
Digital subtraction angiography
MHz
Megahertz
VW
Ventricle width
(unit of frequency)
YS
Yolk sac
BC
Bronchial carcinoma
BPD
Biparietal diameter of the head
CBD
Common bile duct
CCD
Chorionic cavity diameter
CCE
CDS
CT CW D
dVC
Diameter of the vena cava
Parasternal line
erythematosus
Examination Algorithms 161 How Do I Scan Which Organ Step by Step? The following examination sequences do not represent a dogmatic "only possible correct" approach. Instead they provide a useful aid to inexperienced ultrasound examiners for how they can scan certain vascular regions or
organs carefully and completely. These tabular sequences of steps are most easily learned when viewing the digital video clips which you can access online on MedOne (see information and access code on page 3).
The following terms are used to describe these specific transducer motions: Transducer tilt: Sweep left or right
Transducer rotation: Clockwise or counterclockwise
Transducer angulation: For example, cranial or caudal
Shift transducer to a parallel position: Along the longitudinal axis of the transducer
Fig. 161.1
Fig. 161.1
Fig. 161.1
Fig. 161.1
a
b
c
d
Lesson 1: Sagittal scan of the retroperitoneum (aorta, inferior vena cava, lymph nodes) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Place the transducer on the median epigastrium and break the skin coupling cranially. The lost coupling creates a shadow along the left side of the image (left = cranial). Couple the transducer (= press it posteriorly). Instruct the patient to take a deep breath (pause briefly) and hold their breath. Tilt the transducer to the right to send the sound waves into the left paraaortic region. Adjust the magnification and then slowly and continuously tilt the transducer back to the median plane. As you do this, exclude paraaortic lymph node- and verify the correct shape and diameter of the aorta. Sweep through the aortocaval space. Are there enlarged lymph nodes? (= lymph node- ?). Sweep through the inferior vena cava (IVC diameter? IVC thrombosis?) Sweep to the right paracaval region (lymph node- ?) and increase pressure on the transducer EXACTLY when the patient takes a breath. As you pause to let the patient breathe, shift the transducer to a parallel position one transducer width caudally while maintaining pressure on it. Instruct the patient to again take a deep breath (and again maintain pressure on the transducer). Make the same slow sweeping motion backwards from the right paracaval region to the left paraaortic region. Let the patient take a few breaths. If you have not yet reached the aortic bifurcation: Again shift the transducer one transducer width caudally and repeat steps 3–9. Visualize the aorta and a long segment of its intimal/medial border in a central longitudial plane. Freeze the image, let the patient breathe, measure the suprarenal and infrarenal aortic diameters. Visualize the inferior vena cava in a central longitudial plane and verify sharp vascular contours. Freeze the image, let the patient breathe, measure the diameter of the inferior vena cava and caudate lobe.
Lesson 1: Performing the vena cava collapse test 1 2 3 4 5 6 7 8 9 10
Place the transducer on the right paramedian epigastrium and break the skin coupling cranially. The lost coupling creates a shadow along the left side of the image (left = cranial). Couple the transducer (= press it posteriorly). Demonstrate to the patient "live" forced inspiration through the nose with the mouth closed. Optimize the zoom to visualize the inferior vena cava in the sagittal plane just below the diaphragm in a neutral respiratory position. Freeze the image and then switch to double image mode (second window is active). Place your left hand on the freeze button, then instruct the patient to take a sudden deep breath as previously demonstrated. Once the minimal vena caval diameter has been reached, freeze the image and let the patient breathe again. If necessary, go back through the digital memory (using the trackball) and select the appropriate image. Measure the original diameter (first window) and the minimal diameter of the inferior vena cava in the second window. When in doubt, determine the diameters of the peripheral hepatic veins (see p. 52).
Lesson 1: Scanning both iliac neurovascular bundles 1 2 3 4 5
Place the transducer obliquely on the left lower abdomen between the umbilicus and the anterior superior iliac spine and press it posteriorly. Break the skin coupling cranially; the lost coupling creates a shadow along the left side of the image (left = cranial). As breathing commands are neither necessary nor effective in the lower abdomen, let the patient breathe normally. Tilt the transducer medially to send the sound waves laterally toward the iliopsoas muscle. Increase pressure on the transducer to displace intestinal gas from the imaging plane and allow visualization of the retroperitoneum.
162 Examination Algorithms 6 7 8 9 10
Slowly shift the transducer medially to a parallel position or tilt it until the iliac bifurcation comes into the image. Optimize the magnification and zoom factor so you can readily detect any venous thrombosis or arterial plaque. Continuously sweep medially past the iliac vessels to the bladder (perivascular lymph node- ?). Rotate the transducer 90° counterclockwise and perform the compression test on the cross-section of the vessel to exclude thrombosis. Repeat steps 1–10 on the contralateral side.
Lesson 2: Systematic scanning of the pancreas in the transverse upper abdominal plane 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Place the transducer in the transverse plane in the epigastric angle and break the skin coupling on the patient's right side. The lost coupling creates a shadow along the left side of the image (everything is reversed). Tilt the transducer caudally to send the sound waves cranially toward the heart. Place the transducer at an acute angle and press it posteriorly below the level of the ribs. Instruct the patient to take a deep breath (pause briefly) and hold their breath. Then slowly and continuously bring the transducer into an upright position, change your grip, and shift it caudally to a parallel position. Continuously scan first the tail of the pancreas and then its body and head. Continue caudally past the caudal margin of the head of the pancreas and the uncinate process. Let the patient take a few breaths and EXACTLY at that moment slightly increase posterior pressure on the transducer. Instruct the patient to take a deep breath (pause briefly) and hold their breath. On the way back, scan the head of the pancreas cranially until the body appears (stop!). At this point, rotate the transducer 5–15° counterclockwise until the tail of the pancreas appears as well. Freeze the image and immediately let the patient breathe normally. Measure the three diameters of the organ (head, body, tail) perpendicular to the longitudinal axis of the organ (width of the duct?).
Lesson 3: Systematic scanning of the porta hepatis in the oblique right upper abdominal plane 1 2 3 4 5 6 7 8 9 10 11 12
Place the transducer on the right epigastrium (parallel to the left costal arch) in the oblique right upper abdominal plane. Break the skin coupling on the patient's right side; the lost coupling creates a shadow along the left side of the image (everything is reversed). Instruct the patient to take a deep breath (pause briefly) and hold their breath. Press the transducer posteriorly. Tilt the transducer slightly laterally, caudally, and to the right to initially send the sound waves across the porta hepatis. Optimize the magnification and zoom factor if applicable so as not to miss even small periportal lymph nodes. Then slowly sweep caudally across the porta hepatis (periportal lymph node ? collaterals?) ... ... past the portal vein. Then let the patient take a few breaths. As you pause to let the patient breathe, increase the pressure slightly during the first expiration. Have the patient inhale again and sweep back cranially until the portal vein appears. Then rotate the transducer around the axis of its cord until a long segment of the course of the portal vein is visualized. Freeze the image and immediately let the patient breathe normally. Measure the diameter of the portal vein at the hilum (without the thickness of the wall) at a right angle to its longitudinal axis.
Lesson 3: Systematic scanning of the gallbladder in two planes 1 2 3 4 5 6 7 8 9 10 11 12
Place the transducer in the sagittal plane in the right midclavicular line just below the right costal arch, then angle it cranially. Break the skin coupling cranially; the lost coupling creates a shadow along the left side of the image (left = cranial). Instruct the patient to take a deep breath (pause briefly) and hold their breath. Press the transducer posteriorly. Tilt the transducer to the right (laterally) to send the sound waves into the perivesical region (medially). Optimize the magnification and zoom factor if applicable so as not to miss even small lesions of the gallbladder wall. Then slowly and continuously tilt the transducer back to the sagittal midclavicular line and scan the gallbladder ... ... until you have passed the lateral margin of the gallbladder. Sweep the transducer back to the center of the gallbladder and freeze the image. Immediately let the patient breathe normally, and measure the thickness of the wall. As you pause to let the patient breathe, rotate the transducer 90° counterclockwise. Instruct the patient to again take a deep breath, place the transducer at an acute angle, and scan toward the liver cranial to the gallbladder. Slowly scan the gallbladder caudally (focal or diffuse wall thickening, gallstones?) ... ... past its caudal margin (fluid around the gallbladder?). Then let the patient exhale.
Lesson 4: Scanning the left lobe of the liver in two planes 1 2 3 4 5 6
Place the transducer on the right paramedian epigastrium parallel to the inferior vena cava. Break the skin coupling cranially; the lost coupling creates a shadow along the left side of the image (left = cranial). Instruct the patient to take a deep breath (pause briefly) and hold their breath. Angle the transducer slightly cranially so that the border of the diaphragm is just visible along the left side of the image. Shift the transducer to the left to a parallel position, then tilt it and press it posteriorly, and ... ... scan the subdiaphragmatic segments (at sufficient magnification) past the left lateral margin (typical boomerang shape). Then let the patient take a few breaths.
RS85
Made for Professionals
New technologies support your in-depth diagnosis nnovative Samsung technologies offer superb image uality and A supported diagnostic tools. he rystal Architecture of the RS85 and the S ue transducers allow clear and highly detailed ultrasound images. pert tools for e.g. liver idney and thyroid such as S real time image fusion shearwave imaging and other uantitative tools offer new perspectives and additional information to support your daily diagnostics.
Ultrasound system RS85
Approval and registration process for RS85 may differ by country.
Scan code or visit www.samsunghealthcare.com
164 Examination Algorithms 7 8 9 10 11
As you pause to let the patient breathe, angle the transducer caudally and then again have the patient inhale. On the way back, scan the caudal portions of the left hepatic lobe medially as far as the inferior vena cava. As you pause to let the patient breathe, rotate the transducer 90° counterclockwise into the transverse plane. Place the transducer at an acute angle, press it posteriorly, couple it cranially, and scan toward the heart. After deep inspiration, slowly and continuously scan the left hepatic lobe craniocaudally, change your grip, and scan past the caudal border of the liver (focal hepatic lesions?). Let the patient breathe normally.
Lesson 4: Scanning the right lobe of the liver in two planes 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Coming from 4.1., reduce the magnification 2–3 steps (adjust for greater penetration depth). Apply a thin oblique line of gel along the right costal arch. Position the transducer in a right sagittal paramedian plane over the inferior vena cava and directly beneath the right costal arch. Shift the transducer to a parallel position 2–3 cm caudally, press it posteriorly, and angle it sharply cranially. Have the patient breathe in deeply (a knee cushion will relax the anterior abdominal wall). With the diaphragm visualized at the left edge of the image, slowly slide the transducer obliquely and laterally along the right costal arch, ensuring good acoustic coupling at the cranial edge of the transducer (focal hepatic lesions?). Adjust the zoom factor so that the hyperechoic border of the diaphragm is barely visible. Shift the transducer to a parallel position as far as the right anterior axillary line. From here sweep laterally past the border of the organ. Let the patient take a few breaths. As you pause to let the patient breathe, take the transducer out of its cranial angulation. After instructing the patient to breathe in, scan the caudal portions of the right hepatic lobe as far as the inferior vena cava on the way back. Finally, with the transducer now in the sagittal plane over the inferior vena cava, instruct the patient to continue breathing. As you pause to let the patient breathe, place the transducer in an oblique subcostal plane parallel to the right costal arch. Break the right (lateral) skin coupling; the lost coupling creates a shadow along the left side of the image (everything is reversed). Place the transducer at a very acute angle (shift your grip to withdraw the back of your hand), press it, and direct the sound waves cranially. After deep inspiration, slowly and continuously scan the right hepatic lobe craniocaudally, ... ... scanning past the caudal border of the liver and back to the hepatic venous star. There freeze the image, let the patient breathe, and measure the diameter of the peripheral hepatic veins distal to the second venous confluence. Then shift the transducer one transducer width laterally and caudally to a position parallel to the right costal arch. Again press the transducer posteriorly, hold it at an acute angle, and, after the patient has inhaled deeply, systematically scan the lateral portion of the right hepatic lobe for focal hepatic lesions. Finally, let the patient breathe normally.
Lesson 5: Scanning of both kidneys in two planes 1 2 3 4 5 6 7 8 9 10 11 12
Place the transducer in the sagittal plane in the right midaxillary or anterior axillary line (or left posterior axillary line) just below the right costal arch. Break the skin coupling cranially; the lost coupling creates a shadow along the left side of the image (left = cranial). Angle the transducer cranially so that the patient does not have to displace the kidney too far caudally by inhaling. Instruct the patient to take a deep breath (pause briefly) and hold their breath. Optimize the magnification and zoom factor to better detect focal kidney lesions. Sweep the transducer lateromedially, possibly rotating it 5–15°clockwise until ... ... the imaging plane is parallel to the longitudinal axis. Sweep past the borders of the organ. As you pause to let the patient breathe, rotate the transducer 90° counterclockwise into the transverse plane. After another deep breath, slowly and systematically scan the kidney craniocaudally past the lower pole (note that medullary pyramids can be difficult to distinguish from focal kidney lesions). As you pause to let the patient breathe, rotate the transducer 90° clockwise back into the longitudinal plane of the kidney. After deep inspiration, sweep or rotate the transducer to visualize the true maximum longitudinal section of the kidney. Freeze the image, let the patient breathe, and measure the kidney size and parenchyma to pelvis (PP) index.
Lesson 5: Complete scanning of the spleen 1 2 3 4 5 6 7 8 9
Place the transducer in the high plane of the left flank parallel to an intercostal space in the posterior axillary line. Break the skin coupling cranially; the lost coupling creates a shadow along the left side of the image (left = cranial). Use different intercostal windows and shift the transducer to different parallel positions until the spleen is optimally visualized. Optimize the zoom factor so that the immediate perisplenic region is barely visible. To avoid interference from pulmonary air, have the patient inhale only slightly or perform the scan in expiration. If necessary use the curtain trick with rapid expiration after inspiration. It is possible to scan the entire spleen merely by sweeping through different intercostal windows. As you do this, pay attention to the tail of the pancreas and possible accessory spleens. Visualize the greatest diameter of the spleen with visible hilar vessels and freeze the image. Let the patient breathe normally. Measure the craniocaudal size of the organ then measure the thickness at the splenic hilum in a perpendicular plane.
OBB-Querschnitte: ExaminationPankreatitis Algorithms 165 23 Lesson 6: Scanning of the entire thyroid gland using the thyroid preset with the patient's neck slightly hyperextended 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Instruct the patient to place the right hand on the left shoulder (to support the examiner's arm). Place a linear transducer in the transverse left paramedian cervical plane, resting your forearm on the patient's forearm. Break the medial skin coupling; the lost coupling creates a shadow along the left side of the image (everything is reversed). Set the magnification so that the thyroid gland appears as large as possible on the image without being truncated. Use the Valsava maneuver to distend the internal jugular vein in order to clearly identify the vessels on the image. Then slowly tilt the transducer cranial and, beginning to the thyroid gland, continuously scan it craniocaudally. Visualize the greatest diameter of the left thyroid lobe by tilting or rotating the transducer and freeze the image. Rotate the transducer 90° clockwise into the sagittal plane and break the skin coupling cranially (left = cranial?). Slowly and continuously scan the thyroid lateromedially (focal thyroid lesions?). Measure the longitudinal diameter and anteroposterior thickness of the left thyroid lobe and save the measurement image. After saving the second image apply some acoustic gel to the transducer and spread it over the right cervical region. In the right paramedian transverse plane now continuously scan the right thyroid lobe craniocaudally (focal lesions?). Visualize the largest transverse diameter, freeze the image, and measure the diameter. Repeat steps 8–11 for the right thyroid lobe and document all measured values. In the median transverse plane slowly scan the thyroid isthmus craniocaudally (focal lesions?).
Lesson 7: Scanning of the urinary bladder in two planes 1 2 3 4 5 6 7 8 9 10 11 12
Place the transducer in the median sagittal suprapubic plane (breathing commands are not necessary when scanning the lower abdomen). Break the skin coupling cranially; the lost coupling creates a shadow along the left side of the image (left = cranial). Angle the transducer caudally and ensure caudal acoustic coupling with the anterior abdominal skin. Shift the transducer to a left lateral position and slowly scan the bladder, moving from a left perivesical location through the median plane to a right perivesical location (focal or diffuse wall thickening? concretion?). If only the cranial portions of the wall have been visualized in a full bladder, then scan the caudal portions on the way back from right to left (Caution: pay attention to the zoom factor!). In the median sagittal plane, visualize the maximum size of the bladder and then measure the craniocaudal and anteroposterior diameter (not including the wall thickness). Document the measured image. In female patients repeat the sagittal scan to visualize the uterus and cervix. Rotate the transducer 90° counterclockwise into the suprapublic transverse plane. Shift the transducer to a parallel position 3–5 cm cranially and scan the roof of the bladder craniocaudally, ... ... scanning past the caudal border of the floor of the bladder (prostate, seminal vesicles, uterus?). Sweep the transducer back to the largest diameter of the bladder and measure and document it. In male patients scan and measure the prostate and seminal vesicles in two planes.
Lesson 8: FAST algorithm in emergency medicine 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Position the transducer in the transverse plane in the epigastrium, place it at an acute cranial angle, and couple it. On the respirator, press the "inspiration hold" key or ask the respirator operator to do so. Reduce the magnification until the posterior wall of the pericardium is visualized at the lower edge of the image. Scan the heart with a generous tilting motion and be alert to any epicardial rim of fluid. Apply some acoustic gel to the transducer and spread it along the right anterior axillary line or midaxillary line just beneath the ribs. Place the transducer on the right anterior axillary line or midaxillary line and briefly break the skin coupling cranially (for orientation). Angle the transducer far cranially to visualize the pouch of Morison and costodiaphragmatic recess. After adjusting the zoom, sweep lateromedially (free fluid or liver lacerations?). Continue respiration, apply some acoustic gel, place the transducer on the left posterior axillary line parallel to a caudal intercostal space, and couple it. Break the skin coupling cranially; the lost coupling creates a shadow along the left side of the image (left = cranial). Use different intercostal windows and shift the transducer to different parallel positions until the spleen is optimally visualized. Optimize the zoom factor so that the spleen, right kidney, and both pulmonary recesses are well visualized. In expiration, scan the entire bed of the spleen (pouch of Koller, splenic rupture, hemothorax?). Continue respirating the patient, apply acoustic gel, and place the transducer in the suprapubic median sagittal plane. Briefly break the skin coupling cranially (orientation okay? left edge of image = cranial). Angle the transducer caudally and then perform short bilateral paramedian sweeps (pouch of Douglas, rectovesical pouch?).
Important note: These scanning algorithms merely represent an aid for systematic yet time-saving scanning of the regions of interest mentioned. However, if you find any pathologic or focal lesions, they must be measured and documented in two planes. Where indicated, additional examination steps must then be undertaken; for example, determination of the perfusion pattern of a contrast agent over time (contrast-enhanced ultrasound) or similar methods.
166 References [6.1]
Bhatia CSS, Cho CCM, Yuen CYH et al. Realtime qualitative ultrasound elastography of cervical lymph nodes in routine clinical practice: Interobserver agreement and correlation with malignancy. Ultrasound in Med & Biol 2010 (36): 1990–1997
[7.1]
Nyborg WL. Biological effects of ultrasound: Development of safety guidelines. Part II: General review. Ultrasound in Med & Biol 2001 (27): 301–333
[8.1]
Ligawi SS, Buckley AR. Focused abdominal US in patients with trauma. Radiology. 2000 (217): 426–429
[8.2]
Rose JS. Ultrasound in abdominal trauma. Emerg Med Clin North AM. 2004 (22): 518–599
[8.3]
Brooks A, Davies B, Smethhurst M, Connolly J. Prospective evaluation of non-radiologist emergency abdominal ultrasound for haemoperitoneum. Emerg Med J. 2004 (21): e5
[9.1]
Libicher M, Tröger J: US measurement of the subarachnoid space in infants: normal values. Radiology 1992 (184): 749–751
[9.2]
Graf R. Sonografie der Säuglingshüfte und therapeutische Konsequenzen. 6th ed. Stuttgart: Thieme, 2010
[9.3]
Dinkel E et al: Kidney size in childhood. Sonographical growth charts for kidney length and volume. Pediatr Radiol 1985 (15): 38–43
[9.4]
Weitzel D: Untersuchungen zur sonografischen Organometrie im Kindesalter, Mainz)
[9.5]
Chudleigh P, Pearce JM: Obstetric ultrasound: how, why, and when. Churchill Livingstone, Edinburgh 1992
[9.6]
Hadlock FB et al: Sonographic estimation of fetal weight. The value of femur length in addition to head and abdomen measurements. Radiology 1984 (150): 535–540
Legend of Numbered Structures 1 Skin 2 Fatty tissue (subcutaneous and peritoneal) 3 Rectus abdominis muscle 4 Oblique muscles 5 Connective tissue, fascia, septa 6 Linea alba 7 Ligamentum teres 8 Falciform ligament 9 Liver; 9a caudate lobe 10 Hepatic vein 11 Portal vein and its branches 11a Umbilical vein 12 Confluence of the portal vein (from 20 and 23) 13 Diaphragm 14 Gallbladder 15 Abdominal aorta 16 Inferior vena cava 16a Superior vena cava 17 Superior mesenteric artery 18 Hepatic artery 19 Splenic artery 20 Splenic vein 21 Common iliac artery 21a external iliac artery, 21b internal iliac artery. 22 Common iliac vein 22a external iliac vein, 22b internal iliac vein 23 Superior mesenteric vein 24 a right, b left renal artery 25 a right, b left renal vein 26 Stomach (often contains air) 27 Upper pole of kidney 28 Lower pole of kidney 29 Renal parenchyma 30 Medullary pyramids 31 Renal caliceal system with pelvis 32 Celiac trunk 32a Left gastric artery 33 Pancreas 33a Head, 33b body, 33c tail 34 Esophagus 35 Vertebral body 36 Intervertebral disk 37 Spleen 38 Bladder 39 Uterus 40 Os of the cervix 41 Vagina 42 Prostate gland 42a Seminal vesicles 43 Colon (often contains air) ascending a, transverse b, descending c, rectum d 44 Psoas major muscle 45 Acoustic shadow behind air (GI system, lung) 46 Small bowel (duodenum, jejunum, ileum) 47 Lung, air-filled or, see 45, intestinal gas 48 Pubic bone 49 Stone, concretion, calcific plaque 50 Hematoma (solid and liquid components) 51 Artifacts: reverberation a section thickness b, side-lobe c
52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74
75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105 106 107
Blood clots, thrombus Fibrosis, partially calcified Mass (tumor or diverticulum) Lymph nodes or lymphoma Metastasis Liquefaction (necrosis) Abscess, partially liquefied Catheter, stent Air inclusions in bile ducts (biliary air) Hemangioma Focal sparing in fatty infiltration (liver) Focal fatty infiltration (liver) Cyst (fluid-filled) Epithelial outgrowth (polyp) Common bile duct; Hepatic duct a, cystic duct b Sludge (thickened bile) Free fluid in the abdomen (ascites) Pleural effusion Distal acoustic enhancement Infarct Adenoma or angiomyolipoma (benign thyroid and renal tumors) Lymphocele Gastric and bowel wall: mucosa a muscularis mucosae b, submucosa c tunica muscularis d, serosa e, diverticulum f Pancreatic duct Balloon of a urinary catheter Bladder wall Endometrium Pericardial effusion Gallbladder wall Thyroid gland 81a Isthmus Carotid artery; internal 82a, external 82b Internal jugular vein Trachea Sternocleidomastoid muscle Accessory spleen Urinary obstruction (in renal pelvis and calices) Anterior scalene and longus colli muscles Sternohyoid muscle Sternothyroid muscle Ovary Intrauterine device (IUD) Follicle (in ovary) Placenta Embryo or fetus Umbilical cord with umbilical vessels Amniotic fluid Testis Epididymis Scrotum – layers of the wall Pleural border Pneumothorax Lateral ventricle (CNS); temporal horn a, occipital b, central c Choroid plexus Skull Central echo of the falx cerebri Femur
108 109 110 111 112 113 114 115 116 117 118 119 120 121 122 123 124 125 126 127 128 129 130 131 132 133 134 135 136 137 138 139 140 141 142 143 144 145 146 147 148 149 150 151 152 153 154 155 156 157 158 159 160 161 162 163 164 165 166 167 168 169 170
Thigh Rib Cerebellum Arm and hand Pelvis Spinal canal Chambers of the heart Myocardium Intercostal muscles Pectoralis and latissimus dorsi muscles Pulmonary atelectasis Pneumonia Hernia Caudothalamic groove Pouch of Douglas Subclavian artery Third ventricle (CNS) Fourth ventricle (CNS) Corpus callosum Fornix Cavum of the septum pellucidum Thalamus Cingulate gyrus White matter Gray matter (cortex) Cerebral sulci Sylvian fissure Anterior fontanel Superior sagittal sinus Internal capsule Caudate nucleus Putamen and pallidum Cerebrospinal fluid (CSF) Spinal cord Conus medullaris Cauda equina Foramen of Monro Pons (CNS) Longitudinal fissure Sinocortical width of the subarachnoid space Craniocortical width of the subarachnoid space Calices of the renal caliceal system Ureter Ureterocele Urethra Femoral head Autochtonous musculature of the back Adrenal gland Gluteus minimus muscle Gluteus medius muscle Acetabular labrum Cartilaginous convexity (hip) Bony acetabular roof Ischium Ossification center of the femoral neck Joint capsule Triradiate cartilage of the acetabulum Capitis femoris ligament Capital femoral epiphysis Femoral metaphysis Joint cavity or fracture line Vagus nerve Gestational sac (amnion)
Table of Normal Values for Adults The normal values specified on this page are subject to variation within and among individuals and therefore represent only approximate values for adult patients from a Caucasian population. These guideline values represent mean values from the literature and refer to measurements in the standard planes discussed previously. The values for the vascular structures are specified as the Diameter of superior mesenteric artery Abdominal aorta
< 0.5 cm
Diameter: < 2.5 cm (suprarenal) < 2.0 cm (infrarenal) 2.5–3.0 cm = ectasia > 3.0 cm = aneurysm
Angle between aorta and SMA Transverse diameter: Wall thickness:
You will find the normal values for pediatrics on pages 124, 135, 137, 138, and 141 as well as on the pocketsize cards. Lymph node
≤ 6 mm ≤ 2 mm
(Benignity criterion)
Spleen
Organ size: < 11.0 cm (from upper to lower pole) < 4.0 cm (thickness > 6 cm suggests lymphoma)
Adrenal gland
Maximum thickness: < 1.0 cm
Gallbladder
Kidney Wall thickness: < 0.3 cm preprandial < 0.5 cm postprandial Maximum size of gallbladder: < 11.0 x 4.0 cm (longitudinal x transverse)
Biliary tract
Common bile duct: > 0.6 cm or < 0.9 cm postcholecystectomy Intrahepatic bile ducts: < 0.4 cm
Gynecology
Ovary
Bladder
Liver
Uterus (nulliparous): 5.0–8.0 cm length 1.5–3.0 cm thickness Endometrium (double thickness): < 1.5 cm (premenopausal) < 0.6 cm (postmenopausal) IUD-fundus distance: < 2.0 cm (greater = dislodged) IUD-endometrium distance: < 0.5 cm Volume: 5.5–10.0 cm3/ovary premenopausal 2.5–3.5 cm3/ovary postmenopausal Yolk sac: 0.3–0.5 cm Fetal cervical subcutis thickness (between 10th and 14th weeks of pregnancy): < 0.3 cm (greater: neck edema)
Longitudinal diameter divided by transverse diameter: > 2.0 (1.0 = round, suspicious)
Hilum fat sign
< 30 °
Distance between aorta and lumbar vertebra < 0.5 cm Appendix
respective inner diameters of the vascular lumens without regard to the wall, whose thickness can vary between individuals.
Maximum size, respiratory mobility: 10.0–12.0 cm longitudinal diameter 4.0–6.0 cm transverse diameter 3.0–7.0 cm respiratory mobility 1.3–2.5 cm width of parenchyma Parenchyma to pelvis (PP) index: > 1.6 : 1 (under 30 years) 1.2–1.6 : 1 (31–60 years) 1.1 : 1 (over 60 years)
Pancreas
Maximum diameter: < 3.0 cm (head) < 2.0 cm (body) < 2.5 cm (tail) < 0.2 cm (pancreatic duct)
Prostate gland
Maximum size: < 5.0 cm (transverse) < 3.0 cm (sagittal and craniocaudal)
Thyroid gland
Maximum size: 4.0–7.0 cm (craniocaudal) 1.0–3.0 cm (transverse) 1.0–2.5 cm (sagittal) Volume (both lobes together): < 18 mL (women) < 25 mL (men)
Inferior vena cava Diameter: < 2.0 (< 2.5 cm in young athletes) < 1/3 of original lumen on forced inspiration
Wall thickness: < 0.4 cm (filled bladder) < 0.8 cm (postvoiding) Residual bladder volume: < 50 ml Volume: < 550 ml (women) < 750 ml (men)
Splenic vein
Diameter: < 1.0 cm (> 1.2 cm c suggests portal hypertension)
Portal vein
Diameter: < 1.3 cm normal 1.3–1.5 cm gray area > 1.5 cm c suggests portal hypertension
Sagittal size in right midclavicular line: < 13.0–15.0 cm Lateral angle: < 30° (left lateral margin) < 45° (right caudal lobe)
Hepatic veins
Diameter: ≤ 0.6 cm (distal peripheral portions) ≥ 0.7 cm c suggests right heart failure
Volume formula
0.5 x A x B x C (simplified)