Immune Reactions and Experimental Models in Rheumatic Diseases: Proceedings of the Fourth Canadian Conference on Research in the Rheumatic Diseases Toronto, October 15-17, 1970 9781487595968
The proceedings of the fourth Canadian conference on research in the rheumatic diseases, these papers centre on two main
216 54 19MB
English Pages 356 Year 1972
Preface
Contents
IMMUNE REACTIONS
Immune Reactions: Introduction and Summary Comments
The Release of Acid Hydrolases and Cationic Protein from Polymorphonuclear Leucocytes Exposed to Immune Complexes
Lysozyme (Muramidase) in Rheumatoid Arthritis
Proteolytic Mechanism of Allergic Inflammation with Reference to the Arthus Reaction
Immunoglobulin Complexes in Serum and Synovial Fluid of Persons with Rheumatoid Arthritis
The Complement System in Rheumatoid Synovitis: The Relationship of Synovial Fluid Complement Levels to the Clinical, Radiological, and Pathological Changes in Rheumatoid Arthritis
Complement Metabolism in Rheumatoid Arthritis
Serum and Synovial Fluid Proteins in Rheumatoid Arthritis
Serum and Synovial IgG, IgM, C3, and SMA-12 in Arthropathies
The Nature and Properties of Kinin-Forming Substances in Synovial Fluid in Rheumatoid Arthritis
Studies of the Induction of Lymphocyte Transformation by Synovial Fluid from Patients with Rheumatoid Arthritis
Clinical and Haematologic Criteria for the Diagnosis of Systemic Lupus Erythematosus
Immunoglobulins in the Normal Skin in Systemic Lupus Erythematosus
In Vitro Testing for Cellular Immunity to Denatured DNA in Systemic Lupus Erythematosus
Human Anti-endothelial Antibodies
Possible Immunological Mechanisms of Tissue Injury in Joint Diseases
A New Rheumatoid Factor Detectable with Sheep Erythrocytes Sensitized with Bovine Serum
Microbiological Antibody Studies in Séropositive and Séronégative Rheumatoid Arthritis
A Continuing Study of the Effect of Synovectomy on Living Articular Cartilage
The Effect of Synovectomy on Synovium and Cartilage in Rheumatoid Arthritis
EXPERIMENTAL MODELS
Experimental Models: Introduction and Summary Comments
Immune Complex Disease: Effect of Introduction of Immune Complexes into the Tracheobronchial Tree
The Effect of Iron-Dextran on Experimental Synovitis in Guinea-Pigs
Studies on the Pathogenesis of Experimental Arthritis in the Guinea-Pig
An Experimental Investigation of the Local Effects of Phenylbutazone, Gold Thiomalate, and Radioactive Colloidal Gold Administered Intra-articularly to Rabbits
Transplantation of Articular Cartilage in Domestic Fowls: A Model for the Study of the Immune Response to Allogeneic Cartilage
Fine-Structural Correlates of Endothelial Permeability in Vascular Fibrinoid Injury
A Murine Complement Defect as a Tool in the Analysis of Immunosuppression by Antilymphocyte Serum
The Possible Role of a Micro-organism in the Pathogenesis of Adjuvant-Induced Disease in Rats: The Effect of Total Body Radiation and Splenectomy
The Process of Ossification of Vertebral Ligaments in Experimental Adjuvant-Induced Arthritis
Aleutian Disease of Mink: A Virus-Induced Disease with Pathological Features Resembling Systemic Lupus Erythematosus
Experimental Models of Rubella Virus Infection
A Method of Organ Culture: Its Use as an Experimental Model
Tissue Culture Studies of Rheumatoid Synovial Cells
Microbiology of Synovial Membranes and Synovial Fluid in the Arthritides
Blocks in the Assembly of Immunoglobulin Polypeptide Chains in the Mouse Plasma Cell Tumours MOPC-173 and MPC-11
MISCELLANEOUS PAPER
The Role of Elastin in Health and Disease
The Role of Elastase in the Pathogenesis of the Connective Tissue Diseases
A Metabolic Site of Action of Cortisone of Hexosamine and Connective Tissue Metabolism
Collagen Synthesis in Normal and Injured Mature Rabbit Articular Cartilage
In Vivo Studies of Surfaces of Cartilage
Arthroscopy of the Knee
Tryptophan Metabolism in Rheumatoid Arthritis and Scleroderma
Gold 'Nephrosis'
Return to Work in Rheumatoid Arthritis
Total Hip Replacement
Ankylosing Spondylitis: A 20-Year Follow-up Review
Effects of Long-Term Treatment with Allopurinol on Iron Metabolism in Man
An Analysis of the Renal Response to Varying Plasma Urate Concentrations
The Influx of Uric Acid and Other Purines into Everted Jejunal Sacs of the Rat
Index of Authors
Recommend Papers


![Comorbidity in Rheumatic Diseases [1st ed. 2017]
9783319599632, 9783319599625, 3319599631](https://ebin.pub/img/200x200/comorbidity-in-rheumatic-diseases-1st-ed-2017-9783319599632-9783319599625-3319599631.jpg)
![A Short History of the Gout and the Rheumatic Diseases [Reprint 2019 ed.]
9780520339484](https://ebin.pub/img/200x200/a-short-history-of-the-gout-and-the-rheumatic-diseases-reprint-2019nbsped-9780520339484.jpg)


![Rheumatic Diseases and Syndromes Induced by Cancer Immunotherapy: A Handbook for Diagnosis and Management [1 ed.]
9783030568238, 9783030568245](https://ebin.pub/img/200x200/rheumatic-diseases-and-syndromes-induced-by-cancer-immunotherapy-a-handbook-for-diagnosis-and-management-1nbsped-9783030568238-9783030568245.jpg)


- Author / Uploaded
- Duncan A. Gordon (editor)
File loading please wait...
Citation preview
Immune Reactions and Experimental Models in Rheumatic Diseases
THE C O N F E R E N C E WAS HELD UNDER THE AUSPICES OF THE CANADIAN RHEUMATISM ASSOCIATION AND THE CANADIAN ARTHRITIS AND RHEUMATISM SOCIETY
Immune Reactions and Experimental Models in Rheumatic Diseases P R O C E E D I N G S OF THE FOURTH CANADIAN CONFERENCE ON RESEARCH IN THE RHEUMATIC DISEASES T O R O N T O , O C T O B E R 15-17, 1970 E D I T E D BY D U N C A N A. G O R D O N
PUBLISHED FOR THE CANADIAN ARTHRITIS AND RHEUMATISM SOCIETY BY U N I V E R S I T Y OF T O R O N T O PRESS
©University of Toronto Press 1972 Toronto and Buffalo Printed in Canada ISBN 0-8020-3282-6 Microfiche ISBN 0-8020-0121-1 LC 74-163 806
Preface
The Fourth Canadian Conference on Research in the Rheumatic Diseases, sponsored by the Canadian Rheumatism Association and the Canadian Arthritis and Rheumatism Society, was held at the Royal York Hotel in Toronto on October 15-17, 1970. The first such conference took place in Toronto in 1955, and the second and third followed at five-year intervals. A comparison of the proceedings of the conferences over the years reflects the considerable growth of interest in the rheumatic diseases since the founding of the Canadian Arthritis and Rheumatism Society in 1949. Without question we are indebted to the Society for the successful development of research into the rheumatic diseases in Canada during these years. Significantly, the Proceedings of the 1970 meeting represent in the main an account of current work being done by Fellows, former Fellows, and Grantees of the Society. The themes of the Conference - Immune Reactions and Experimental Models reflect the principal areas of current concern to researchers who now are in receipt of Society support. The first part of the Proceedings consists of reports on immunological aspects of the rheumatic diseases. Following the discovery some twenty years ago that the rheumatoid factor was an antibody came an appreciation that rheumatoid arthritis was a disease characterized by increased immunological activity. Since then investigators have been intrigued as to whether or not the rheumatoid factor and other immune factors are involved in the pathogenesis of the disease. Although the characterization of the rheumatoid factor contributed significantly to our understanding of the immunoglobulin system in man, the relationship of these immunoglobulins to the production of arthritis was not clear. Subsequently the discovery that synovial fluid leucocytes contain intracytoplasmic
vi
Preface
inclusions consisting of immune complexes led to an awareness of the role of chemotaxis and phagocytosis, as well as of lysosomes and their enzymes, in the production of rheumatoid inflammation of the joints. The observation of a decrease in haemolytic complement in rheumatoid synovial fluid drew further attention to this system. The recognition that complement could be one of the prime mediators responsible for rheumatoid synovitis is particularly significant since the complement system can be activated by immune complexes, including those containing the rheumatoid factor. Thus, a relationship between increased immunological activity and the production of synovitis can now be postulated in rheumatoid arthritis. The second part of the Proceedings contains papers on animal or experimental model diseases which have certain features in common with human rheumatic disorders. Some of the model diseases, such as adjuvant disease of rats, occur as a result of immunological manipulation by the investigator, whereas others, such as Aleutian disease of mink, are spontaneous naturally occurring diseases, apparently induced by a slow virus infection. In either case, a study of the interplay of genetic, microbiological, and immunological factors is extremely valuable, the implications for understanding the nature of human rheumatic disease being of special interest. The contributions of Dr K. Frank Austen of the Robert Breck Brigham Hospital and Harvard Medical School in Boston and Dr Carl M. Pearson of the Division of Rheumatology of the University of California Medical School in Los Angeles enhanced the Conference tremendously. Dr Austen gave the introduction and summary to the first part on Immune Reactions, and Dr Pearson acted in the same capacity for the second part on Experimental Models. It was a privilege to have the participation of these teacher-scientists in the Conference, and we are grateful to both of them. Although the Proceedings include a good deal of information which increases our understanding of the pathogenesis of rheumatic diseases, more questions have been raised than answered. One interesting problem concerns the possible existence of an antigen which provokes and perpetuates rheumatoid joint inflammation and another the relevance to studies in man of the information obtained from studying experimental models. Questions such as these will determine the directions to be taken by research into the rheumatic diseases in the next ten years. We are indebted to the Canadian Rheumatism Association and the Canadian Arthritis and Rheumatism Association for having made the Conference and the publication of these Proceedings possible. D.A.G.
Contents
PREFACE
V
I M M U N E REACTIONS
Immune Reactions: Introduction and Summary Comments / K. FRANK AUSTEN
The Release of Acid Hydrolases and Cationic Protein from Polymorphonuclear Leucocytes Exposed to Immune Complexes / NORTON s. TAICHMAN, NARENDRANATH S. RANADIVE, and WALDEMAR PRUZANSKI
Lysozyme (Muramidase) in Rheumatoid Arthritis / WALDEMAR PRUZANSKI, M. LYNN RUSSELL, and METRO A. OGRYZLO
Proteolytic Mechanism of Allergic Inflammation with Reference to the Arthus Reaction / KEIJI UDAKA Immunoglobulin Complexes in Serum and Synovial Fluid of Persons with Rheumatoid Arthritis / IRVIN BRODER, REUBEN BAUMAL,
3
10 16 20
DUNCAN A. GORDON, MURRAY B. UROWITZ, and EILLEEN SHINDER
32
SHAUN RUDDY, JOSEPH M. CORSON, J. LELAND SOSMAN, PETER H. SCHUR, and K. FRANK AUSTEN
40
The Complement System in Rheumatoid Synovitis: in. The Relationship of Synovial Fluid Complement Levels to the Clinical, Radiological, and Pathological Changes in Rheumatoid Arthritis / MELVIN c. BRITTON, Complement Metabolism in Rheumatoid Arthritis / ARTHUR WEINSTEIN, D. K. PETERS, DAVID L. BROWN, and RODNEY BLUESTONE
51
M. LYNN RUSSELL, WALDEMAR PRUZANSKI, DUNCAN A. GORDON, and METRO A. OGRYZLO
57
ANDRÉ LUSSIER
63
Serum and Synovial Fluid Proteins in Rheumatoid Arthritis / Serum and Synovial IgG, IgM, C3, and SMA-12 in Arthropathies /
viii
Contents
The Nature and Properties of Kinin-Forming Substances in Synovial Fluid in Rheumatoid Arthritis / HENRY z. MOVAT, M. LYNN RUSSELL, and DUNCAN A. GORDON
Studies of the Induction of Lymphocyte Transformation by Synovial Fluid from Patients with Rheumatoid Arthritis / T. DOUGLAS KINSELLA Clinical and Haematologic Criteria for the Diagnosis of Systemic Lupus Erythematosus / THOMAS BITTER Immunoglobulins in the Normal Skin in Systemic Lupus Erythematosus /
68 71 77
JOHN S. PERCY, BRUCE A. BARTHOLOMEW, and CHARLEY J. SMYTH
84
WALTRAUD RIEDEL
90
In Vitro Testing for Cellular Immunity to Denatured DNA in Systemic Lupus Erythematosus / JOANNE MARSH, B. MOOKERJEE, JOHN s. PERCY, and Human Anti-endothelial Antibodies / c. KIRK OSTERLAND, ROBERT G. BRICKER, and K. J. LINDQVIST
Possible Immunological Mechanisms of Tissue Injury in Joint Diseases / TARUNENDU CHOSE and JOHN F. WOODBURY
A New Rheumatoid Factor Detectable with Sheep Erythrocytes Sensitized with Bovine Serum / MARGUERITE EPP and DONALD M. MITCHELL Microbiological Antibody Studies in Seropositive and Seronegative Rheumatoid Arthritis / DUNCAN A. GORDON, GLADYS PAWLIN, and ARTHUR E. FRANKLIN
A Continuing Study of the Effect of Synovectomy on Living Articular Cartilage / ROBERT D. GALWAY and RICHARD L. CRUESS The Effect of Synovectomy on Synovium and Cartilage in Rheumatoid Arthritis / NELSON s. MITCHELL and NORA SHEPARD
97
102 106 112 120 125
EXPERIMENTAL MODELS
Experimental Models: Introduction and Summary Comments / CARL M. PEARSON
Immune Complex Disease: Effect of Introduction of Immune Complexes into the Tracheobronchial Tree / JOHN BIENENSTOCK and NEIL JOHNSTON The Effect of Iron-Dextran on Experimental Synovitis in Guinea-Pigs /
144 145
ALASTAIR G. MOW AT, THOMAS F. DISNEY, and JOHN H. VAUGHAN
154
BRANISLAV BELOVIC and T. DOUGLAS KINSELLA
160
Studies on the Pathogenesis of Experimental Arthritis in the Guinea-Pig / An Experimental Investigation of the Local Effects of Phenylbutazone, Gold Thiomalate, and Radioactive Colloidal Gold Administered Intra-articularly to Rabbits / ROBERT B. SALTER and DONALD F. PRIOR Transplantation of Articular Cartilage in Domestic Fowls: A Model for the Study of the Immune Response to Allogeneic Cartilage / WILLIAM A. SILVER
Fine-Structural Correlates of Endothelial Permeability in Vascular Fibrinoid Injury / ISTVAN HÜTTNER, GEORGE ROÑA, and ROBERT H. MORE A Murine Complement Defect as a Tool in the Analysis of Immunosuppression by Antilymphocyte Serum / BERNHARD CINADER, HOMI F. JEEJEEBHOY, SHU-YI w. KOH, and ANTONINE G. RABBAT The Possible Role of a Micro-organism in the Pathogenesis of AdjuvantInduced Disease in Rats: The Effect of Total Body Radiation and Splenectomy / MORTON A. KAPUSTA, LYGERI HADJIPETROUKOUROUNAKIS, and A. DANIEL ROTENBERG
165 174 179 189
203
Contents The Process of Ossification of Vertebral Ligaments in Experimental AdjuvantInduced Arthritis / HANS K. UHTHOFF Aleutian Disease of Mink: A Virus-Induced Disease with Pathological Features Resembling Systemic Lupus Erythematosus / HINRICH TABEL, DONALD G. INGRAM, and LARS KARST AD
Experimental Models of Rubella Virus Infection / PETER B. DENT and L. AVILA A Method of Organ Culture : Its Use as an Experimental Model / JOHN F. CROCKER and ROBERT L. VERNIER Tissue Culture Studies of Rheumatoid Synovial Cells / DENYS K. FORD Microbiology of Synovial Membranes and Synovial Fluid in the Arthritides / J. A. EMBIL, J. F. L. WOODBURY, K. R. ROZEE, and SHIRLEY MACDONALD
Blocks in the Assembly of Immunoglobulin Polypeptide Chains in the Mouse Plasma Cell Tumours MOPC-173 and MPC-11 / REUBEN BAUMAL, R. LASKOV, and MATTHEW D. SCHARFF
ix 208
218 230 238 244 247 251
MISCELLANEOUS PAPERS
The Role of Elastin in Health and Disease / WILLIAM H. KIRKALDY-WILLIS and WILLIAM A. SILVER
259
DAVID P. VARADI
265
The Role of Elastase in the Pathogenesis of the Connective Tissue Diseases / A Metabolic Site of Action of Cortisone of Hexosamine and Connective Tissue Metabolism / TASSOS ANASTASSIADES Collagen Synthesis in Normal and Injured Mature Rabbit Articular Cartilage / RAIMO u. REPO and NELSON s. MITCHELL In Vivo Studies of Surfaces of Cartilage / DONALD c. MCGILLIVRAY and
280 287
DUGALD L. GARDNER
290 293
HOUPT, METRO A. OGRYZLO, and MARNIE M. HUNT
298
ABDELNOUR
304
WALTERS
314 320
DONALD C. GRAHAM, and PHILLIP S. ROSEN
325
JOHN F. FILBEE, EMMANUEL G. FLORENTIS, and JOHN F. L. WOODBURY
331
HUGH A. SMYTHE
336
ABUL H. KHAN, S. WILSON, and JOHN C. CRAWHALL
342
Arthroscopy of the Knee / ROBERT w. JACKSON and DALE D. MCCARTHY Tryptophan Metabolism in Rheumatoid Arthritis and Scleroderma / JOSEPH B. Gold 'Nephrosis' / MANFRED HARTH, A. CAMERON WALLACE, and GEORGE M. Return to Work in Rheumatoid Arthritis / HAROLD s. ROBINSON and KAY Total Hip Replacement / LESLIE H. TRUELOVE, A. G. JORGENSEN, and G. LAW Ankylosing Spondylitis: A 20-Year Follow-up Review / HUGH A. LITTLE, Effects of Long-Term Treatment with Allopurinol on Iron Metabolism in Man / An Analysis of the Renal Response to Varying Plasma Urate Concentrations / The Influx of Uric Acid and Other Purines into Everted Jejunal Sacs of the Rat / INDEX OF AUTHORS
345
This page intentionally left blank
Immune Reactions and Experimental Models in Rheumatic Diseases
This page intentionally left blank
Immune Reactions: Introduction and Summary Comments K. FRANK AUSTEN
In attempting to summarize the portion of this symposium on immune reactions in rheumatoid arthritis (and related connective tissue diseases), it may be helpful for me to present my own view of the derangement of the immunologie effector mechanisms in rheumatoid arthritis and indicate how today's presentations relate to such a scheme (Figure 1 ). Two lines of evidence indicate that the synovial fluid of patients with rheumatoid arthritis contains altered human immunoglobulins of a class capable of activating the complement sequence: Hannestad (1) directed attention to the presence of aggregates of IgG in some rheumatoid synovial fluids on the basis of a precipitating reaction with IgM rheumatoid factor; while Winchester, Kunkel, and Agnello (2) identified immune complexes by precipitation with IgM rheumatoid factor or the binding subunit, Clq, of Cl, followed by acid dissociation and identification of the predominant ingredients as IgG and IgG rheumatoid factor. The synovial fluid complexes appeared in higher concentration and contained a portion which sedimented more rapidly in density gradient ultracentrifugation than the complexes in the respective serum; further, the smaller serum complexes failed to precipitate with Clq and yielded less precipitate with IgM rheumatoid factor than the synovial fluid complexes (2). As noted in this symposium by Russell and associates (see pp. 57-62), rheumatoid synovial fluid, especially from séropositive individuals, exhibits a higher concentration of immunoglobulins - IgG, IgA, and IgM - than sometimes observed in the corresponding serum or in synovial fluids of individuals with gouty or degenerative arthritis. Of particular note are the studies of Broder, Gordon, and Urowitz (see pp. 32—9) From the Harvard Medical School Department of Medicine, Robert B. Brigham Hospital, Boston, Massachusetts.
Figure 1
Immune Reactions: Introduction and Summary Comments
5
which recognize soluble immune complexes, termed rheumatoid biologically active factor (RBAF), in serum and synovial fluid of rheumatoid patients by using a bioassay system wherein such complexes release histamine from isolated, perfused guinea-pig lung. This factor contains IgG but not IgA, IgM, or the third component of complement (C3); it does not cryoprecipitate, is not anticomplementary, and does not correlate in titre with the estimated content of IgM rheumatoid factor or complexes of intermediate size in the same biologic fluid; nonetheless, it is most reminiscent of the complexes described by Winchester, Kunkel, and Agnello (2) which fail to precipitate Clq. Intra-articular depletion of whole-complement activity in the presence of normal or elevated serum levels in patients with rheumatoid arthritis was first noted in 1964 by Pékin and Zvaifler (3) and Hedberg (4). Quantitative studies in our own laboratory of individual complement components by the methods available at that time (5) revealed relative reductions in intra-articular fourth (C4) and second (C2) complement components in rheumatoid effusions as compared to the levels of these components in synovial fluids of individuals with degenerative arthritis; these reductions are consistent with the intra-articular activation of first component (CÏ) and inactivation of its natural substrates, C4 and C2. Hedberg (6) noted that the intra-articular depletion of whole-complement activity was proportional to the titre of rheumatoid factor in the serum or synovial fluid; and Winchester, Kunkel, and Agnello observed that in fluids with approximately equal concentrations of complexes of IgG-IgG rheumatoid factor, the anticomplementary activity increased with the quantity of detectable IgM rheumatoid factor in the same fluid (2). In initial in vitro studies, the effect of IgM rheumatoid factor on complement fixation by aggregated IgG was recorded as inhibitory (7), but more recent investigations in which the anticomplementary activity of the altered immunoglobulin was controlled by reduction and alkylation have revealed the augmentative effect of rheumatoid factor on complement activation ( 8 ). Further, although in vitro model systems employing rabbit antibody to the sheep red cells (9) or to bovine serum albumin (10) demonstrate the capacity of IgM rheumatoid factor to block the binding site of the rabbit immunoglobulin for Clq, the substitution of its own binding site, under appropriate conditions, enhanced complement fixation. The available findings in model systems are thus now in accord with the clinical observations that the most profound reductions in intra-articular complement occur in patients with IgM rheumatoid factor and suggest that this factor contributes to tissue injury through its reaction with altered IgG to activate further the complement sequence (11). The recognition of IgM rheumatoid factors of varying specificity, as noted by Epp and Mitchell (see pp. 106-11), raises the question of their relative capacity to augment or even diminish complement fixation by altered human IgG. In order to understand better the extent and possible mechanisms of the intraarticular activation of the complement sequence in rheumatoid arthritis, in our
6
K. F. Austen
laboratory we have recently examined the functional titre of five complement components by effective molecule titrations of paired serum and synovial fluid specimens (12, 13, 14). Certain synovial fluids from patients with séropositive rheumatoid arthritis exhibited marked reductions in Cl measured either in terms of haemolytic function or by the protein concentration of the Clq subunit using radial immunodiffusion. The failure of most joint fluids of séropositive patients to show a reduction in Cl may reflect the dissociation of activated Cl (Cl ) from the altered immunoglobulins at physiologic ionic strength (15). Activation can, however, be inferred in all fluids of séropositive individuals from the parallel reductions in the intra-articular levels of C4 and C2. In synovial fluids of séronégative patients, only C4 was depleted to a statistically significant extent as compared to the findings in the fluids of patients with degenerative joint disease. That the action of Cl on C4 and C2 resulted in the intra-articular assembly of C3 convertase is suggested by the depletion of C3 haemolytic titre in joint fluids of séropositive patients (13) with the appearance in the fluid of breakdown products of the C3 protein (16). The cleavage of C3 by convertase is known to release a small fragment, C3a, with anaphylatoxic activities (17), capable of producing a local increase in vascular permeability when injected intracutaneously into man (18). The major fragment, C3b, remains bound to the cellular intermediate or presents in the fluid phase as the inactive protein C3i; the presence of C3b on a cell surface or immune complex confers the ability to participate in immune adherence (19), an event thought to enhance phagocytosis of the complex by polymorphonuclear leucocytes (20) or macrophages (21). The localization by immunofluorescence of immunoglobulins and the complement proteins, C3 (22), Clq, and C4 (23) in the synovial fluid polymorphonuclear leucocytes of patients with séropositive rheumatoid arthritis is consistent with the view that intra-articular immune complexes have undergone phagocytosis, possibly in an enhanced fashion, through the presence of the 3b fragment on the altered immunoglobulins and with the attendant release of lysosomal and other intracellular (24) enzymes. In this regard, it is noteworthy that the ingestion of immune complexes by rabbit neutrophils was found by Taichman, Ranadive, and Pruzanski (see pp. 10-15) to be associated with the release of cathepsins, lysozyme, and lysosomal cationic protein, while the deposition of such complexes in rabbit skin, the Arthus reaction, was demonstrated by Udaka (see pp. 20-31) to release SH-dependent proteases from the macrophage population. Of direct relevance to the role of enhanced phagocytosis with release of intracellular constituents into the synovial fluid in rheumatoid arthritis is the report of Pruzanski, Russell, and Ogryzlo (see pp. 16-19) of increased levels of lysozyme in the synovial fluid with a lesser elevation in the paired serum sample, and the report by Lussier (see pp. 63-7) of the extraction of material with antigenic characteristics of C3 from the synovial fluid leucocytes. Activation of the complement sequence beyond C3 step to involve C5, C6, and C7 is indicated by the finding of chemotactic activity characteristic of both the
Immune Reactions: Introduction and Summary Comments
1
macromolecular 567 complex and the C5a fragment (25). The C5a fragment is not only chemotactic for polymorphonuclear leucocytes but possesses anaphylatoxic activity as well (26). Finally, recent studies of the terminal or ninth component of complement reveal a joint fluid level in séropositive patients that is only one-half that observed in the séronégative group (14). Thus, activation of Cl in the synovial fluid of séropositive patients appears to be associated to some extent with completion of the entire cytotoxic sequence within the joint space. It is important to note, however, that evaluation of the complement system on the basis of a component utilization profile within the joint space does not take into account differences in rates of component influx or efflux as modified by the articular inflammatory process. Studies of the metabolism of purified radiolabelled C3, such as those conducted by Weinstein, Brown, and Bluestone (see pp. 51—6), are essential to the recognition of increased total catabolism and did reveal a fractional catabolic rate of 8 per cent of the plasma pool per hour in a patient with rheumatoid vasculitis, while the rate in the remaining series was 2.5 to 3 per cent, similar to that of other studies in normal individuals (27). The finding that rheumatoid arthritis is characterized by the intra-articular fluid phase activation of an effector system of immunologie tissue injury does not reveal the nature of the aetiologic event and does not account for the characteristic destructive proliferative synovitis. It could be argued that the latter is an expression of cellular immunity to the same event responsible for the humoral findings in the surrounding fluid, but it is equally appealing to suggest that the tissue changes are a consequence of the fluid phase abnormality itself. The finding of Kinsella (see pp. 71-6) that synovial fluids of patients with rheumatoid arthritis stimulate mitogenesis of buffy coat lymphocytes of autologous or homologous, rheumatoid or non-rheumatoid origin could be attributed to either cellular immunity or to an effect of immune complexes (28). The latter possibility is supported by the correlation of the mitogenicity of a synovial fluid with its content of IgG and C3 containing polymorphonuclear leucocytes, and would relate the lymphoid hyperplasia of the rheumatoid synovium to the fluid phase abnormalities. Immunofluorescent studies (29, 30) have demonstrated C4, C3, and immunoglobulins in rheumatoid synovial tissue, and such deposits could represent ingestion of immune complexes by phagocytic synovial cells with attendant release of lysosomal enzymes. Indeed, synovial lining cells from patients with rheumatoid arthritis are filled with secondary lysosomes presumably reflecting increased lysosomal activity (31). The lysosomes are striking in the electron micrographs of early rheumatoid synovitis shown by Mitchell and Shepard (see pp. 125-43). In considering mechanisms of enhanced lysosomal activity other than phagocytosis, the studies on the effect of exposing organ cultures of chick limb-bone rudiments to rabbit antiserum against fowl erythrocytes in the presence of complement (32) merit examination. The cartilaginous rudiments so treated become soft and fragile while exhibiting much increased lysosomal activity; restoration of the rudiment to control medium
8
K. F. Austen
again permits growth of bone and cartilage but often in a distorted fashion. The activation of tissue lysosomal enzyme activity with enzyme release and concomitant tissue injury observed in the explant experiments in response to an immunologie insult are noteworthy but limited in implication by the requirement for antibody directed against membrane antigen. Duplication of the experimental effects was not achieved by antibody to non-tissue antigen but remains a possibility with evolving knowledge of how to demonstrate bystander effects of complement upon cells not specifically sensitized. Thompson and Lachmann (33) and Gotze and Miiller-Eberhard (34) have shown that a trimolecular complex of activated C5, C6, and C7 can interact with an unsensitized bystander cell to yield an intermediate susceptible lysis upon interaction with C8 and C9. Further, Ghose and Woodbury (see pp. 102-5) report antibodies directed against synovial cells in the serum of rheumatoid patients. The capacity of the synovial tissue to aggravate the fluid phase abnormality in rheumatoid arthritis by contributing both IgG and IgM antiglobulins (35) would serve to perpetuate the events leading to intra-articular injury in this disease. It is thus possible to consider that both the activation of synovial tissue lysosomal activity with secondary tissue destruction and fibrotic repair and the lymphocytic infiltration with appearance of plasma cells and elaboration of rheumatoid factors which contribute to and perpetuate the intraarticular disease process are secondary to the humoral immunochemical abnormalities. The other presentations do not bear directly on the above reaction scheme but introduce critical points in regard to other aspects of the connective tissue diseases. The recognition by Movat, Russell, and Gordon (see pp. 68—70) that synovial fluid contains the prekallikrein activator (36) as well as kallikrein (37) implies a potential role for the kinin-forming system in some forms or phases of intraarticular inflammation. It should be noted, however, that the earlier report of a kinin-like peptide in rheumatoid effusions (38) has not been confirmed as being bradykinin in studies employing a radioimmunoassay for this nonapeptide (39). The experimental studies on the effects of synovectomy in the rabbit knee joint by Galway and Cruess (see pp. 120—4) again lead to a consideration of the role of lysosomal enzymes in articular cartilage injury. The report of Marsh, Mookerjee, and Percy (see pp. 90-6) showing that DNA suppressed migration of peripheral blood leucocytes from some patients with systemic lupus erythematosus could be used to invoke cellular immunity, but the role of immune complexes in this particular assay system requires further exclusion. Of particular clinical interest is the finding of Percy, Bartholomew, and Smyth (see pp. 84-9) that the clinically normal skin from patients with systemic lupus erythematosus reveals deposition of immunoglobulins in high incidence. Finally, the fascinating demonstration by Osterland (see pp. 97-101) of antibody to vascular endothelium in polymyositis more than in other connective tissue diseases and of even greater incidence in renal allograft recipients awaits further study in terms of its biologic consequences.
Immune Reactions: Introduction and Summary Comments
9
REFERENCES 1 HANNESTAD, K. Clin. Exp. Immunol. 2: 511, 1967 2 WINCHESTER, R. j., AGNELLO, v., and KUNKEL, H. G. Clin. Exp. Immunol. 6: 689, 1970 3 PEKIN, T. J., JR.. and ZVAIFLER, N. j. J. Clin. Invest. 43: 1372, 1964 4 HEDBERG, H. Acta Rheum. Scand. 10: 109, 1964 5 FOSTIROPOULOS, o., AUSTEN, K. F., and BLOCH, K. j. Arthritis Rheum. 8: 219, 1965 6 HEDBERG, H. ActaMed. Scand. (Suppl.) 479,1967 7 ZVAIFLER, N. j., and BLOCK, K. J. Arthritis Rheum. 5: 127, 1962 8 ZVAIFLER, N. j., and SCHUR, P. H. Arthritis Rheum. 11: 523, 1968 9 SCHMID, F. R., ROITT, i. M., and ROCHA, M. j. J. Exp. Med. 132: 673, 1970 10 TESAR, j. T., and SCHMID, F. R. J. Immunol. 105: 1206, 1970 1 1 BRITTON, M. C., RUDDY, S., CORSON, J. M., SOSMAN, J. L., SCHUR, P. H., and AUSTEN, K. F.
This volume, pp. 40-50 12 RUDDY, s., BRITTON, M. c., SCHUR, p. H., and AUSTEN, K. F. Ann. New York Acad. Sci. 168: 161,1969 13 RUDDY, s., and AUSTEN, K. F. Arthritis Rheum. 13: 713, 1970 14 RUDDY, s., EVERSON, L. K., SCHUR, p. H., and AUSTEN, K. F. J. Exp. Med. 134: 259s, 1971 15 RAPP, H. J., and BORSOS, T. J. Immunol. 91: 826, 1963 16 ZVAIFLER, N. j. J. Clin. Invest. 48: 1532, 1969 17 COCHRANE, c. o., and MÜLLER-EBERHARD, H. J. J. Exp. Med. 122: 99, 1968 18 LEPOW, I. H., WILMS-KRETSCHMER, K., PATRICK, R. A., and ROSEN, F. s. Amer. J. Path. 61: 13, 1970 19 NELSON, R. A. In The Inflammatory Process, edited by B. W. Zweifach, L. H. Grant, and R. T. McCluskey (Academic Press, New York, 1965), p. 819 20 GIGLI, i., and NELSON, R. A. Exp. Cell Res. 51: 45, 1968 21 PERLMANN, P., PERLMANN, H., MÜLLER-EBERHARD, H. J., and MANNI, J. A. Science 163: 937,
1969 22 VAUGHAN, j. H., BARNETT, E. v., SOBEL, M. v., and JACOX, R. F. Arthritis Rheum. 11: 125, 1968 23 BRITTON, M. c., and SCHUR, P. H. Arthritis Rheum. 14: 87, 1971 24 AXLINE, s. G., and COHN, z. A. I. Exp. Med. 131: 1239, 1970 25 WARD, p. A., and ZVAIFLER, N. J. J. Clin. Invest. 50: 606, 1971
26 SHIN, H. S., SNYDERMAN, R., FRIEDMAN, E., MELLORS, A., and MAYER, M. M. Science 162: 361,
1968
27 CARPENTER, C. B., RUDDY, S., SHEHADEH, I. H., MÜLLER-EBERHARD, H. J., MERRILL, J. P., and
AUSTEN, K. F. J. Clin. Invest. 48: 1495, 1969 28 BLOCH-SHTACHER, N., HiRSCHHORN, K., and UHR, J. w. Clin. Exp. Immunol. 3: 889, 1968
29 RODMAN, W. W., WILLIAMS, R. C., BILKA, P. J., and MÜLLER-EBERHARD, H. J. Lab. Clin. Med.
69: 141, 1967 30 FISH, A. j., MICHAEL, A. F., GEWURZ, H., and GOOD, R. A. Arthritis Rheum. 9: 267, 1966 31 BARLAND, R., NoviKOFF, A. B., and HAMERMAN, D. Trans. Ass. Amer. Phys. 77: 239, 1964 32 LACHMANN, p. j., COOMBS, R. R. A., FELL, B., and DINGLE, j. T. Int. Arch. Allerg. 36: 469, 1969 33 THOMPSON, R. D., and LACHMANN, p. j. J. Exp. Med. 131: 629, 1970 34 GOTZE, o., and MÜLLER-EBERHARD, H. j. J. Exp. Med. 132: 898, 1970 35 SMILEY, j. D., SACKS, c., and ZIFF, M. J. Clin. Invest. 47: 624, 1968 36 KAPLAN, A. p., and AUSTEN, K. F. I. Immunol. 105: 802, 1970 37 WUPPER, K. D., TUCKER, E. s., and COCHRANE, c. G. J. Immunol. 105: 1307, 1970 38 KELLERMEYER, R. w., and GRAHAM, R. c. New Eng. J. Med. 279: 754, 1968 39 TÁLAMO, R. c., HABER, E., and AUSTEN, K. F. J. Lab. Clin. Med. 74: 816, 1969
The Release of Acid Hydrolases and Cationic Protein from Polymorphonuclear Leucocytes Exposed to Immune Complexes N O R T O N S. TAICHMAN, NARENDRANATH S. R A N A D I V E , AND WALDEMAR PRUZANSKI
Polymorphonuclear leucocytes (PMNL) appear to play an important role in the pathogenesis of numerous forms of experimental hypersensitivity (Table i). Several investigators have proposed that the release of PMNL lysosomes may be triggered by immune reactions occurring in the synovial fluids of rheumatoid arthritics (1, 2). Since PMNL lysosomes contain a battery of biologically active constituents (Table n), it is thought that these agents may mediate tissue damage in rheumatoid arthritis. One mechanism which stimulates the liberation of PMNL lysosomes occurs as a consequence of the uptake of immune precipitates ( 3 ). This appears to be relevant in the development of the local Arthus reaction (4) and in immune aggregate shock (5). Significant numbers of PMNL isolated from rheumatoid arthritis exúdales contain various inclusions, such as rheumatoid factor complex (6). Since phagocytosis of this aggregate leads to lysosomal discharge in vitro (7), it seems reasonable to contemplate that a similar event may take place in synovial fluids. Recently, a factor or factors which display many characteristics of soluble immune complexes have been isolated from sera and synovial exudates of rheumatoid arthritis patients (8). These findings have generated interest into the possible role of soluble complexes in the initiation and progression of the disease. It is known that such complexes can produce experimental dermal inflammatory lesions (9, 10) and are implicated in the development of serum sickness in rabbits (4). In the latter syndrome, soluble complexes in antigen excess appear to become From the University of Toronto Division of Experimental Pathology and the Rheumatic Disease Unit, the Wellesley Hospital, Toronto, Ontario. Supported by a research grant from the Canadian Arthritis and Rheumatism Society.
Acid Hydrolases from Polymorphonuclear Leucocytes
11
TABLE I P A R T I C I P A T I O N OF PMNL LYSOSOMES IN E X P E R I M E N T A L H YPERS ENS I TI V ITY
Local Arthus reaction Generalized Arthus reaction (immune aggregate shock) Passive cutaneous anaphylaxis (heterocytotropic antibody) Glomerulonephritis of acute nephrotoxic nephritis Arteritis of serum sickness Local Shwartzman reaction Generalized Shwartzman reaction TABLE II REPRESENTATIVE CONSTITUENTS OF PMNL LYSOSOMES
Enzymes
Miscellaneous
Acid RNAase Cationic proteins and polypeptides Acid DNAase Mucopolysaccharides Acid phosphatase Glycoproteins Alkaline phosphatase Endogenous pyrogen (5-glucuronidase Phagocytin (3-galactosidase Cathepsins Neutral proteases Lysozyme Hyaluronidase Elastase Collagenase Peroxidase Kinin-forming hydrolases Kinin-inactivating hydrolases Phospholipase Aryl sulphatase Plasminogen activating enzyme Lipases
segregated in the walls of blood vessels. PMNL infiltrate into these areas and appear to be responsible for the disruption of the elastic lamina, fibrinoid necrosis, etc. (11). Circumstantial data suggest that PMNL lysosomes mediate these changes (12). It should be pointed out that the mechanisms of the synovitis which often accompanies serum sickness are unknown. It is conceivable that soluble complexes leaking into joint cavities could lead to the attraction of PMNL and the subsequent liberation of lysosomes in the involved joints. These considerations prompted our undertaking a series of experiments to ascertain if soluble immune complexes could effect the release of PMNL lysosomes. We reasoned that such an event might be important in the over-all story of the pathology of rheumatoid arthritis. Rabbits were immunized with 50 mg of bovine serum albumin (BSA) emulsified in complete Freund's adjuvant. Six weeks later, antisera were collected, pooled
12
N. S. Taichman, N. S. Ranadive, W. Pruzanski
(440 jUg AbN), and heated to 56°c for 30 minutes to destroy the components of complement. Two major types of immune complexes were incubated with PMNL : preformed and in situ complexes. Preformed complexes (PFC) were prepared by adding appropriate amounts of BSA to washed BSA/anti-BSA equivalence precipitates; 0.5 ml (220 /¿g AbN) was then incubated with the cells. In situ complexes (isc) were formed in the presence of the cells by a 10-minute preincubation with 0.5 ml of antiserum (220 /u.g AbN). BSA was then added to the cultures. Both PFC and isc contained identical amounts of antigen and antibody in the form of equivalence precipitates or complexes in varying zones (5 to 30 times) of antigen excess. Equivalence precipitates were employed as a positive control since they had already been shown to stimulate lysosome discharge (3). PMNL-rich (80-90 per cent) peritoneal exúdales were produced by glycogen injection in rabbits. Harvested cells were washed and suspended in a modified Hanks buffer containing 50 units penicillin per ml, 10 mg streptomycin per ml, and 0.1 per cent gelatin. One millilitre amounts of the suspension (100 X 10fi PMNL) together with the immune reagents in a total volume of 3.0 ml were placed in polypropylene tubes and incubated with constant agitation for periods up to 2 hours in a water bath at 37°c. Triplicate or quadruplicate tubes were set up for each experiment. At the conclusion of the incubations, cells were sedimented by centrifugation and supernatants were employed for the estimation of various acid hydrolases and cationic protein. The latter material can be extracted from PMNL lysosomes (13) and is capable of causing the release of histamine from intact mast cells (14). The results of these experiments are recorded in Table in. It is evident that PFC and isc equivalence precipitates are active in triggering the extracellular liberation of acid protease (2 per cent haemoglobin at pH 2.5 was the substrate), lysozyme, and cationic protein. Isc formed in varying zones of antigen excess also possessed this property but the potency diminished as the proportion of antigen in them increased. On the other hand, PFC were, in general, not as active as similar concentrations of isc. Release phenomena did not occur when incubations were carried out at 4°c or in the absence of glucose. Neither PFC nor isc formed in antigen excess stimulated the release of acid phosphatase, /3-glucuronidase, or ribonuclease from PMNL. All the enzymes monitored in these studies are, to varying degrees, localized within PMNL lysosomes. Since it appeared as if acid protease and lysozyme were labilized, we had anticipated that a similar pattern would have been apparent with additional marker enzymes. This has not proved to be the case. It may be speculated that acid protease and lysozyme were derived from soluble cytoplasmic compartments rather than from lysosomes. However, this explanation does not take into account the release of cationic protein, which is localized in lysosomes (13, 14). We feel that the answer to this enigma may involve one of the following considerations: (a) there may be a selective as opposed to a wholesale pouring out of lysosomal constituents from the cell; (b) assuming that several lysosomal
Acid Hydrolases from Polymorphonuclear Leucocytes
13
TABLE III ACID HYDROLASE AND CATIONIC PROTEIN RELEASE FROM PMNL EXPOSED TO IMMUNE COMPLEXES FOR 30 M I N U T E S
Per cent releasef Acid protease
Lysozyme
Cationic protein
PPTS
10.5 4.0 3.3 3.2
26.4 13.7 6.1 6.6
31.8 26.4 14.0 3.9
PPTS
15.1 10.7 9.3 5.9 2.4
28.8 30.5 17.9 12.1 -
36.4 32.2 31.0 16.3 -
Preformed complexes* x 5 Ag xlOAg x20Ag In-situ complexes x 5 Ag
x 10 Ag
x20Ag x30Ag
* PPTS = equivalence precipitates, x 5 Ag = complexes formed at 5 times antigen excess, etc. t Extracellular concentration is expressed as a percentage of the total activity in cell suspensions and represents net activity following subtraction of background values (i.e., spontaneous liberation of these agents from cells in buffer alone and inherent activity in the reagents).
enzymes were liberated, they might have missed detection by being inactivated or by complexing to other substances; (c) two major release systems may have been set in motion, one involving lysosomes (cationic protein release) and one soluble cell fractions (acid protease and lysozyme secretion). In an attempt to resolve this dilemma we intend to fractionate PMNL incubated with immune stimuli into three fractions: nuclear, cytoplasmic, and lysosomal. Each fraction will be tested for lysosomal enzyme activity to determine if there has been an internal redistribution of hydrolases. In addition, lactic dehydrogenase will be assayed in the ambient fluids of the cultures as a marker for non-lysosomal enzyme. Data collected from such experiments should enable us to pin-point the source of acid protease and lysozyme and to determine if other enzymes participate in the response to PFC or isc stimulation. It is difficult to rationalize the finding that isc in antigen excess are more active than identical amounts of PFC. Since PFC were produced from immune precipitates washed free of extraneous serum components, we felt that serum or plasma constituents may be necessary to support release. This turned out not to be the case because the inclusion of fresh homologous heparinized plasma or either fresh or heated serum failed to enhance the potentials of PFC and actually inhibited the response to isc. Further, isc produced with partially purified antibody were just as potent as such complexes formed in whole antiserum.
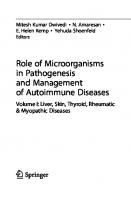
Figure 1 An electron micrograph of a group of PMNL exposed to isc formed at 10 times antigen excess for a 30-minute period. Note the formation of numerous phagocytic vacuoles (VAC) within all the cells. These lacunae also contain remnants of lysosomes (L) and ingested particulates, presumably antigen-antibody precipitates (PPT). Mitochondria (MIT); nucleus (NUC). X 1,360
Acid Hydrolases from Polymorphonuclear Leucocytes
15
When the isc response was monitored by phase contrast microscopy, we noted that the cells were surrounded by a granular material. This was not a feature in cultures exposed to PFC. We suspected that this material might be the remnants of disintegrating cells. This interpretation did not, however, concur with our finding that the majority of PMNL in isc systems remained vital, as evaluated by dye exclusion tests. Electron microscopic studies revealed that the debris was not of cellular origin but strongly suggested that it was immune precipitates which were being phagocytosed by PMNL (Figure 1). This was verified by allowing isc to form in test tubes but in the absence of PMNL. Within 10 minutes a definite precipitate was observed, even in tubes at 30 times antigen excess. Such findings were not anticipated. As already outlined, immune precipitates can cause lysosome release from PMNL; thus, the activity of isc may be due to such particulates rather than to soluble immune complexes per se. In order to settle this issue we are currently employing a modified type of isc preparation, which is formed by the addition of the total amount of antigen to antiserum. After antigen and antibody interact for 10 to 30 minutes, the complexes are added to PMNL. We have found that the modified preparations are as potent in triggering the release reactions as conventional isc. Our next step is to centrifuge these complexes and find out whether it is the precipitate or the supernatant (soluble complexes) portion of the preparation which accounts for release. These experiments are in progress. In summary, we are still not in a position to state whether soluble immune complexes can stimulate the release of intracellular constituents from PMNL. We are hopeful that future studies will provide more insight into this question, thereby adding to our knowledge of the pathogenetic potentials of such complexes. REFERENCES 1 ZVAIFLER, N. j. Arthritis Rheum. 8: 289, 1965. 2 WEISSMANN, G. Rheumatology 1:1, 1967 3 MOV AT, H. z., URIUHARA, T., MACMORINE, D. R. L., and BURKE, J. s. Life Sci. 3: 1025, 1964 4 COCHRANE, c. G. Advances Immunol. 9: 97, 1968 5 MOVAT, H. Z., URIUHARA, T., TAICHMAN, N. S., ROWSELL, H. C., and MUSTARD, J. F.
Immunology 14: 637, 1968 6 VAUGHN, J. H., BARNETT, E. v., soBEL, M. v., and JACOX, R. F. Arthritis Rheum. 11: 125, 1968 7 ASTORGA, G., and BOLLET, A. J. Arthritis Rheum. 8: 511, 1965 8 BAUMAL, R., and BRODER, i. Clin. Exp. Immunol. 3: 555, 1968 9 ISHIZAKA, K., and CAMPBELL, D. H. Proc. Soc. Exp. Biol. Med. 97: 639, 1958 10 COCHRANE, c. G., and WEIGLE, w. o. J. Exp. Med. 108: 591, 1958 11 KNIKER, w. T., and COCHRANE, c. G. J. Exp. Med. 122: 83, 1965 12 COCHRANE, c. G., and AIKEN, B. s. J. Exp. Med. 124: 733, 1966 13 RANADIVE, N. s. Fed. Proc. 28: 363,1969 14 RANADIVE, N. s., and COCHRANE, c. G. J. Exp. Med. 128: 605, 1968
Lysozyme (Muramidase) in Rheumatoid Arthritis WALDEMAR PRUZANSKI, M. LYNN RUSSELL, AND METRO A. OGRYZLO
In an earlier report describing the measurement of lysozyme (muramidase) in various forms of arthritis, it was shown that in patients with rheumatoid arthritis the activity of this enzyme was frequently higher in the synovial fluid than in the serum. With few exceptions, the levels in both the serum and synovial fluid exceeded those found in other forms of articular disease or in healthy controls ( 1 ). Lysozyme circulating in the blood is presumed to be produced by polymorphonuclear leucocytes and monocytes (2). However, the source of lysozyme in the synovial fluid remains speculative. Synovial lining cells have been found to produce various enzymes (3, 4, 5) and may therefore also contribute to the production of lysozyme. On the other hand, it may be assumed that the large number of white cells in the synovial fluid frequently found in inflammatory arthritis may also play a role. In the present report, lysozyme activity was estimated in the synovial fluids (219), sera (147), and urines (91) of patients with various articular diseases. All the patients were admitted to the University of Toronto Rheumatic Disease Unit. The patients with rheumatoid arthritis conformed to the classical or definite type in accordance with American Rheumatism Association classification criteria (6). Lysozyme activity was estimated by the lysoplate method of Osserman and Lawlor as previously described ( 1 ). Purified human lysozyme from the urine of a patient with monocytic leukaemia served as a standard. The concentration of lysozyme was expressed in micrograms of purified human lysozyme per millilitre of buffer. From the University of Toronto Rheumatic Disease Unit, Immunoproteins Research Laboratory, the Wellesley Hospital, Toronto, Ontario. Supported by a research grant from the Canadian Arthritis and Rheumatism Society.
Lysozyme in Rheumatoid A rthritis
17
Quantitation of IgG, IgA, and IgM was performed on immunoplates obtained from Hyland Laboratories, Los Angeles, California. The latex fixation test was performed according to the method of Singer and Plotz (7). Statistical evaluation of results was done with the aid of the University of Toronto Central Computer, applying the CURVEFIT program. Lysozyme activity was high in 32 per cent of sera from rheumatoid arthritics and in some patients with séronégative polyarthritis and gout. In general, serum lysozyme activity was normal in patients with osteoarthritis and ankylosing spondylitis. Increased lysozyme activity was demonstrated in 72 per cent of synovial fluids from rheumatoid joints. In more than half of the estimations, the level exceeded 20 /tAg/ml (Table i). Some increase in lysozyme activity was also found in several patients with séronégative polyarthritis, ankylosing spondylitis, acute synovitis, and gout. None of the patients with osteoarthritis, tear of the semilunar cartilage, or non-bloody traumatic effusion had a high lysozyme activity in the synovial fluid. TABLE I ACTIVITY OF SERUM AND SYNOVIAL FLUID LYSOZYME IN RHEUMATOID
Diagnosis
ARTHRITIS
No. of estimations
Range and mean ± 1 s.d. (ug/ml) 6.6-13.8 9.69±1.80
No. of estimations between 15 and 20 ug/ml 0
No. of estimations higher than 20 ug/ml
Normal individuals' serum
20
Rheumatoid arthritis serum
97
5.7-48.2 12.6±5.4
26 (27%)
5(5%)
Rheumatoid arthritis synovial fluid
137
5.9-100.0 23.4±13.4
29 (21%)
70 (51%)
0
Synovial fluid lysozyme activity was higher than that in the serum in 86 per cent of simultaneous estimations in rheumatoid arthritics. Conversely, in osteoarthritics, the serum level of lysozyme exceeded that found in synovial fluid in 72 per cent of estimations. In other forms of arthritis, the results were not as clear. Urinary lysozyme activity was always normal provided that renal function was normal. As in healthy individuals, no correlation was observed between the activity of lysozyme and the number of polymorphonuclear leucocytes and monocytes in the venous blood of patients with various forms of arthritis (Table n). In synovial fluids, the results were much more variable and were scattered over a very wide range. This may imply that there is an additional source of lysozyme or that a rapid turnover and destruction of white cells, with release of the lysosomal constituents into the liquid milieux, contribute to the high lysozyme activity. No significant correlation was found between serum lysozyme and synovial fluid lysozyme
18
W. Pruzanski, M. L. Russell, M. A. Ogryzlo
TABLE II RELATIONSHIP BETWEEN LYSOZYME ACTIVITY AND THE N U M B E R OF P O L Y M O R P H O N U C L E A R L E U C O C Y T E S A N D MONOCYTES IN THE SERUM AND SYNOVIAL FLUID
{(serum lysozyme ug/ml)/(polymorphonuclears + monocytes/ml)} x 100 Diagnosis
No. of estimations
Range and mean ± s.d.
Healthy individuals' serum
20
0.067-0.600 0.280± 0.120
Rheumatoid arthritis serum
43
0.066-1.057 0.278 ±0.200
Rheumatoid arthritis synovial fluid
52
0.046-14.800 1.012 + 2.556
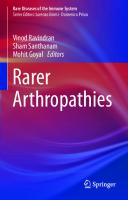
Figure \ Synovial fluid lysozyme in various functional classes of rheumatoid arthritis.
Lysozyme in Rheumatoid Arthritis
19
Figure 2 Lysozyme in two simultaneously aspirated joints.
activity, or between either of these and the number of polymorphonuclear leucocytes and monocytes in the corresponding fluids. No correlation was detected between the activity of lysozyme and the level of immunoglobulins or the titre of the latex fixation test. Serum activity of lysozyme was not related to the functional class of rheumatoid arthritis, although synovial fluid lysozyme activity was higher in patients who were more disabled (Figure 1 ). In simultaneously aspirated samples of synovial fluid, the level of lysozyme was higher in the more severely involved joint (Figure 2), indicating that it may be a good index of the activity of the disease. REFERENCES 1 PRUZANSKI, w., SAITO, s., and OGRYZLO, M. A. Arthritis Rheum. 13: 389, 1970 2 BRIGGS, R. s., PERILLIE, p. E., and FINCH, s. c. J. Histochem. Cytochem. 14: 167, 1966 3 LUSCOMBE, M. Nature (London) 197: 1010, 1963 4 HARRIS, E. D. JR., COHEN, G. L., and KRANE, s. M. Arthritis Rheum. 12: 92, 1969 5 WEGELIUS, o., KLOCKARS, M., and VAiNio, K. Acta Med. Scand. 183: 549, 1968 6 ROPES, M. W., BENNETT, G. A., COBB, S., JACOX, R. F., and JESSAR, R. A. Bull. Rheum. DÍS.
9: 175, 1958 7 SINGER, j. M., and PLOTZ, c. M. Amer. J. Med. 21: 888, 1956
Proteolytic Mechanism of Allergic Inflammation with Reference to the Arthus Reaction KEIJI UDAKA
As is well known, the cutaneous Arthus reaction is a typical example of allergic inflammation. It is characterized by morphological features, such as oedema, erythema, and haemorrhage, and the chronological sequence in which these features develop after injection of antigen into an immunized animal ( 1 ). The process can be considered as consisting of three sequential events: (i) immunization; (ii) the antigen-antibody interaction which initiates the chain of events leading to tissue injury; and (iii) tissue injury and inflammation. Immunization, the antigenantibody interaction, and some of the sequelae are well understood, but the mechanism which leads to tissue injury, particularly the chemical substances which mediate the injury, has not been fully elucidated. Recently, in our laboratory, evidence has accumulated which indicates that two distinct protease systems (one SH-dependent and the other SH-independent) are activated during the Arthus reaction (1, 2). These enzymes may conceivably be the trigger which initiates the chain of events leading to immunologie tissue injury following antigen-antibody interactions. Two SH-dependent (SH-Px, SH-P2) and two SH-independent (NSH-P1; NSH-P2) enzymes have been isolated from the Arthus lesions ( 3 ). One of these, SH-Pj, is probably specific to the Arthus reaction, because it is not found in the inflammation caused by thermal or chemical injury (4). It increases in parallel with the development of the Arthus lesion and decreases as the inflammation subsides (5-7). It has also been shown that the inactivation of this protease is due to local increase of specific inhibitor (8). Both the From the University of Toronto Department of Pathology, Division of Experimental Pathology, Toronto, Ontario. Supported by a research grant from the Canadian Arthritis and Rheumatism Society.
Proteolytic Mechanism of A llergic Inflammation
21
protease and its inhibitor are released in vitro from mononuclear cells during antigen-antibody interactions (9, 10). The other enzymes (SH-P2, NSH-Pj, NSHP2) probably occur in many inflammatory lesions, for example, in thermal and chemical injury (4). It has also been found that several types of vasoactive peptide, able to cause enhanced vascular permeability and haemorrhage, are released in the Arthus reaction (11, 12) and that the formation of these peptides requires the sequential activation of two distinct proteases ( 3 ). By analogy with the formation of plasma kinins, it was postulated that the tissue proteases present in inflamed lesions act by producing 'tissue kinins.' The present paper describes the isolation of tissue proteases and a haemorrhagic factor (HRL.) from cutaneous Arthus lesions and discusses the possible role of these factors in the mechanism of induction and progression of the inflammatory reaction. MATERIALS AND METHODS
Adult male albino rabbits (1.8-2.0 kg) were used. Sensitization of the Rabbits Ten milligrams of bovine serum albumin (BSA) in complete Freund's adjuvant was injected into 10 sites in both legs or, in a few experiments, three subcutaneous infections of 5 ml of 3 per cent BSA were given on three consecutive days. The BSA (five times crystallized; Nutritional Biochemical Corporation) had been further purified to a high degree by preparative polyacrylamide gel electrophoresis (13). Antibody titre was determined by a quantitative precipitation method. The animals were used when their antibody protein reached 0.8 to 1.2 mg per ml of serum. Induction of the Arthus Reaction The Arthus reaction was elicited in the abdominal skin. Unless otherwise stated, 0.1 ml of 2.5 per cent BSA was injected into each of 20 sites. The subsequent inflammatory responses were estimated by gross inspection. The reaction became apparent in 2 hours, reached its peak in 20 to 24 hours, and then decreased in intensity. Skin lesions of 6 hours, 12 hours, and 24 hours duration were used in this experiment. Untreated abdominal skin from BSA immunized rabbits was used as a control. Preparation of Skin Acetone Powder As has been described in detail previously (5), normal and inflamed skin was excised immediately after the animals were killed. The skin was finely cut and frozen at —80°c. The pieces of frozen skin were cut into slices about 50 /¿ thick with a freezing microtome and were dehydrated with cold acetone.
22
K. Udaka
Chromatography Gel filtration was carried out using Sephadex G-50 and G-25 (Pharmacia Fine Chemicals, Inc.) following the method of Porath (14). Ion-exchange chromatography was performed using DEAE-Sephadex A-50 (Pharmacia Fine Chemicals, Inc.), Bio-Gel DM-100, Dowex 50W-X2 (Bio-Rad Laboratory), DE-32, and CM-32 (Microgranular form, Whatman Co., Ltd.). The DEAE-Sephadex, DE32, CM-32, and Bio-Gel DM-100 were prepared according to the method of Sober et al. (15). Dowex 50W-X2 was prepared by the method of Moore and Stein (16). Details of the experimental procedure will be given in a separate paper (17). Both stepwise and gradient elutions were carried out as shown in Figure 1. Fractions were collected at room temperature in an automatic fraction collector set to deliver 112 drops (3 ± 0.02 ml) per tube. The flow rate was maintained between 35 and 40 ml per hour, using an Isco's Precision Metering Pump (Model 300). Protein Determination Concentration of the eluted protein was determined by ultraviolet absorption at 280 m/u,, using a standard cell of 1 cm light path. Protease Assays Protease activity was estimated by the casein digestion method of Kunitz (18) slightly modified (4). Enzyme solutions were mixed with 1 per cent casein ( 1 ml) and incubated at 37°c at pH 7.1 (0.2 M phosphate, 1 per cent NaCl) for 30 minutes. Protease activity was expressed in terms of optical density of the trichloracetic acid filtrate at 276 m^u,. Esterase activity was measured by hydroxamate formation or with the pH-stat. In the hydroxamate method, 1 ml of 10 mM ester and 0.1 ml of enzyme were incubated in 0.05 M tris or phosphate buffer at pH 6.0-8.6 at 37°c for 10 minutes. The reaction was stopped by addition of 2 ml of alkaline hydroxylamine solution (a mixture of equal volumes of 2 M hydroxylamine hydrochloride and 3.5 M sodium hydroxide). After one minute, 1 ml of 4 N hydrochloric acid was added. The decrease of absorbance at 500 m/¿ was read after the addition of 1 ml of 10 per cent ferric chloride in 0.1 N hydrochloric acid. In the pH-stat method, 1 ml of 10 mM ester was incubated with 0.025 ml of enzyme solution in 0.15 M potassium chloride at pH 6.0-8.0 at 37°c. The released carboxyl group was titrated by a standard solution of 0.1 M or 0.05 M sodium hydroxide using a Metrohm's pH-stat. Haemorrhagic Test 0.1 ml of the sample was injected intradermally at various concentrations into the abdominal skin of rabbits at 1 hour, 45, 30, 15, and 5 minutes before killing of the animal. The 'cleared' specimens were prepared according to the method of Hurley
(19).
Proteolytic Mechanism of Allergic Inflammation
23
Reagent Papain (crystalline, Nutritional Biochemical Corp.), trypsin (crystalline, Mann Research Laboratories), and a-chymotrypsin (Mann Research Laboratories) were prepared by the procedure previously described (20). Benzoyl-L-arginine ethylester HC1 (BAEE, Mann Research Laboratory), acetylL-tyrosine ethylester (ATEE, Mann Research Laboratories), p-tosyl-L-arginine methylester (TAME, Mann Research Laboratories), benzyloxycarbonyl-L-lysine benzyl ester tosylate (Z. Lys. OB2, Cycle Chemical Corp.), and benzyloxycarbonyl-L-lysine methylester-HCl (Z. Lys. OMe, Cyclo Chemical Corp.) were used as synthetic enzyme substrates. Cysteine hydrochloride and glutathione (Cys-SH; GSH, Nutritional Biochemical Corp.) were dissolved in 1 per cent sodium chloride at a concentration of 0.1 M, and diluted as needed. Before use, the SH content was measured by the amperometric method previously described (21). p-Chrolomercuribenzoic acid (Nutritional Biochemical Corp.) was recrystallized three times by the method of Hellerman and Chinard (22). Its mercury content was 56.54 per cent by iodometric titration (theoretical value, 56.17 per cent Hg). A weighed amount of the acid was dissolved in a slight excess of 0.5 N sodium hydroxide and then diluted to the appropriate volume. Usually a 0.02 M solution was used as a stock solution. Soybean trypsin inhibitor (SBTI, five times recrystallized, Nutritional Biochemical Corp. ) was suspended in buffered saline at a concentration of 5 ml/ml and suitably diluted. e-Aminocaproic acid (EACA, Mann Research Labs., Inc.) was dissolved in water at a concentration of 1.0 M. The purified inhibitor of the SH-dependent protease was prepared from rabbit skin with healing Arthus lesions according to the procedure previously described (20). It was dissolved at a concentration of 500/ig/ml in 0.16 M saline, and diluted as needed. This inhibitor inactivated papain (100 /u, g inhibited 14/u.g of papain) as well as the SH-dependent protease present in Arthus lesions, but had no effect on trypsin or a-chymotrypsin (20). The inhibitor has a molecular weight of 12,500(23). RESULTS
Isolation and Preliminary Characterization of Tissue Proteases Released from Cutaneous Arthus Reactions Skin extracts were prepared from normal and inflamed lesions at various stages of the Arthus reaction and were fractionated with ammonium sulphate into three fractions: euglobulin, pseudoglobulin, and albumin. The SH-dependent protease activity was concentrated predominantly in the euglobulin fraction; it increased in parallel with the inflammation and decreased when the inflammation subsided (4-6). Ten millilitres of the euglobulin fraction containing protease was applied to a
24
K. Udaka
column of DEAE-Sephadex A-50 (2.0 X 20 cm) which had previously been equilibrated with 0.02 M phosphate buffer of pH 7.4. As shown in Figure la, the protease was separated into two active components, one eluted in the second peak, the other in the fourth. The mean specific activity was about 0.31 and 0.22, respectively. The yields of each fraction were about 28 per cent and 30 per cent of the starting preparation. The fraction from the second peak was then chromatographed on a Bio-Gel DM-100 column (1.5 X 15 cm), which had been equilibrated with 0.01 M phosphate buffer of pH 8.2. As shown in Figure Ib, six fractions were identified. Active components were
Figure 1 Chromatography of euglobulin fraction containing protease prepared from 12-hourold Arthus lesions. The upper figure (a) shows the results with DEAE-Sephadex A-50 (solid line, £2»; triangle spot, protease activity). The lower figure (b) shows the results with Bio-Gel DM-100. The values shown here represent further chromatography of the second peak obtained with DEAE-Sephadex A-50 (upper). (Dotted line shows KC1 gradient.)
Proteolytic Mechanism, of Allergic Inflammation
25
TABLE I E F F E C T OF P - C H L O R O M E R C U R I B E N Z O A T E , C Y S T E I N E , S O Y B E A N T R Y P S I N I N H I B I T O R , B - A MI N O C A P R O I C A C I D ,
AND
A R T H U S S H - PI N H I B I T O R O N T I S S U E P R O T E A S E S
Protease activity (E27f>) Saline PCMB(10- 4 A/) 3
Cys-SH (10- M) SBTI (250 mg/ml) EACA (0.2 M)
Arthus SH-P inhibitor*
SH-P!
SH-P2
NSH-P!
NSH-P2
0.198 0.026 0.380 0.194 0.196 0.044
0.220 0.042 0.315 0.216 0.220 0.052
0.088 0.090 0.090 0.084 0.082 0.086
0.102 0.098 0.052 0.096 0.100 0.108
*Used at concentration of 0.5 mg/ml. For enzyme assay see text.
eluted in the second, third, and fifth peaks. The mean specific activity of the fractions was 1.1, 0.27, and 1.88. The proteases eluting in the second and fifth peaks were SH-dependent, since they were inhibited by /7-chloromercuribenzoate, but easily reactivated by the addition of reduced glutathione or cysteine (Table i). They were arbitrarily named SH-?! and SH-P2. The other two proteases were SH-independent. They eluted in the third peak of Bio-Gel DM-100 (Figure Ib) and the fourth peak of DEAE-Sephadex A-50 (Figure la). These enzymes were named NSH-Pi and NSH-P2. By caseinolysis, the pH optima of SH-Pj, SH-P2, and NSH-Pi were 7.1, 7.0-7.4, and 6.8-7.6, respectively, while that of NSH-P2 was 7.6-8.2. The two NSH-Ps had esterolytic activity on tyrosin ethylester and benzoyl-L-arginine ethylester, but neither of the SH-Ps had such activity. Only NSH-P2 was inactivated by 10~3 M cysteine. Both SH-Ps were inactivated by the natural Arthus SH-P inhibitor (24, 25), but the NSH-Ps were not. Neither the SH-Ps nor the NSH-Ps were inactivated by EACA or SBTI (Table i). SH-P! is probably a specific enzyme activated during the development of the Arthus reaction, but SH-P2, a common enzyme, occurred in many inflammatory lesions, for example, in thermal and chemical injury (4). SH-P, was isolated mainly from the 6-12-hour-old Arthus lesions, and SH-P2 from 12-24-hour-old lesions. In Vivo Effect of Tissue Proteases When the partially purified SH-P1 or SH-P2 was injected intradermally into the abdominal skin of rabbits, a dose of 5 /¿g induced a significant inflammatory response characterized by haemorrhage (Figure 2). The reaction was more marked with SH-Pi, which sometimes caused necrosis in 12-24 hours. There was a parallel between the proteolytic activity and the intensity of the inflammatory response. A similar response was observed when papain was injected in a dose of over 20 fig. No such responses were observed when NSH-Pi or NSH-P2 was injected in a dose of over 100 ¿¿g. Little response was induced by 30 /¿g of trypsin and 50 fig of chymotrypsin.
26
K. Udaka
Figure 2 Gross appearance of the lesions induced by the tissue proteases and the haemorrhagic factor (HRo). HR 2 was prepared from lesions induced by SH-Pt. 0.1 ml of each sample was injected, and the section taken 30 minutes after injection.
Microscopically, the lesion induced by the SH-Ps showed a marked cellular infiltration chiefly by PMN-leucocytes and eosinophils. The lesion was very similar to a 12-hour-old Arthus reaction. In some lesions induced by SH-Pi, an intense vasculitis with necrosis and fibrin thrombi accompanied the leucocytic infiltration. Such a vasculitis is typical of the active Arthus reaction. These results indicate that the SH-Ps are one of mediators of the Arthus reaction.
The Possible Role of SH-Dependent Proteases in the Formation of a Haemorrhagic Factor (HR2) As shown in Figure 3, a haemorrhagic factor was isolated from cutaneous Arthus lesions in rabbits by chromatography, using a combination of molecular sieve and ion-exchange resins. This factor produced vascular congestion and haemorrhage from small vessels within a few minutes of injection and also caused thrombosis, the formation of intravascular hyaline masses, eosinophilic swelling around vessels, and sometimes necrosis of small vessels. In order to elucidate whether SH-Pi or SH-P2 produces the HR2, the same isolation procedure was carried out on the lesions induced by the SH-Ps. A similar factor was isolated from the lesions induced by SH-Pi, but not from the lesions induced by SH-P2. As shown in Figure 4, when 5 ;u,g of HR2 was injected intradermally into the
Proteolytic Mechanism of Allergic Inflammation
27
Figure 3 Procedure for the isolation of haemorrhagic factor (HR.) from inflamed skin.
Figure 4 The haemorrhagic reaction at a skin site injected with 5 ¿ig of HR2 (0.1 ml; 5 minutes (a) and 30 minutes (b) after injection), showing marked vascular congestion (a) and haemorrhage (b) from small vessel.
rabbits, vascular congestion and haemorrhage from small vessels were observed. Similar results were seen when 0.5 fig of HR2 was injected, and there was a parallel between the amount of HR2 injected and the intensity of haemorrhagic response. These results indicate that SH-Pi is involved in the production of HR2. DISCUSSION As has been summarized in a recent publication (1), the initiation of the Arthus reaction is characterized by a local microcirculatory disturbance characterized by early exudation, followed by stasis. These changes may be caused by the transient
28
K. Udaka
appearance of histamine releasers such as anaphylatoxin or the interaction of reagenic (anaphylactic) antibody with antigen or by the activation of enzymes, such as the SH-dependent proteases. All these events seem to be followed by the release of histamine or histamine-like substances. The early vascular response is rapid, transient, and not very intense. It is suppressible by antihistamines. The advanced stage, the well-known, typical Arthus reaction, is characterized by leucocytic sticking to the endothelium, the formation of 'white thrombi,' the emigration of leucocytes, and haemorrhage. The damage of the blood vessels and obstruction of the lymphatics may be so severe that the lesion is deprived of its blood supply and may undergo massive haemorrhage, necrosis, and ulcération. The observations described in this paper show that the action of the SH-dependent proteases activated during the Arthus reaction is associated with the mediation of this advanced stage, especially the haemorrhagic reaction. When the SH-dependent protease derived from Arthus lesions was injected intradermally into the abdominal skin of rabbits, petechial haemorrhage was observed, with the deposition of eosinophilic material in the wall of blood vessels and necrosis of vessels. There was a parallel between proteolytic and haemorrhage activities. The haemorrhage induced by these enzymes may either be due to direct enzyme action or be induced indirectly by the formation of a haemorrhagic factor (HR 2 ). Previously, Benacerraf (24) proposed that the haemorrhage seen in the Arthus reaction was related to vascular thrombosis, because in heparinized animals the reaction was milder. Since the lesions induced by the SH-Ps show an intensive vasculitis with fibrinous thrombi, it might be postulated that the SH-Ps cause vascular thrombosis, followed by haemorrhage. However, Humphrey (25) and Cochrane (26) found that even a large amount of heparin caused little or no suppression of the reaction. Furthermore, depletion of circulating platelets, one of the thrombosing elements, fails to inhibit the Arthus phenomenon (25, 27). These studies indicate that although thrombosis is readily observed in the early vascular lesions of the Arthus reactions, its role in the development of haemorrhage is questionable. The lesions produced by the injection of SH-Ps reproduce the main features of the Arthus reaction. The most conspicuous difference is in the pattern of leucocytic infiltration. The Arthus reaction is characterized by a very intense infiltration by leucocytes, chiefly PMN- leucocytes and eosinophils. This infiltration is most intense in the wall of vessels and perivascularly, with relatively few inflammatory cells beyond the perivascular tissue in the early stages ( 1 ). In contrast, most of leucocytic infiltration was diffuse in the lesions induced by SH-Ps. Two possible mechanisms have been suggested to explain this leucocytic emigration. First, Yoshinaga et al. isolated a chemotactic factor from cutaneous Arthus lesions (28) and showed that a similar factor was produced when immunoglobulin G (IgG) was incubated with SH-P (29). Such a factor could play an important role in the pathogenesis of the exudation. Alternatively, the fixation of complement by the immune precipitates with release of the chemotactic factor
Proteolytic Mechanism of Allergic Inflammation
29
C567 (30, 31) may be of importance. It should be noted, however, that though both factors induce chemotaxis in vitro, it remains to be ascertained whether they induce emigration and accumulation of leucocytes in the tissue in vivo. The evidence that proteolytic activity is associated with the allergic response has been summarized by Ungar and Hayashi (32), but the cellular origin of the different types of enzyme involved in the Arthus reaction has not been established with certainty. Recent results in our laboratory showed that the SH-dependent protease, SH-Pi; is present in the mononuclear cells of tissue and peripheral blood, since the application of antigen to living sensitized cells induces an immediate release of the protease into the extracellular fluid. The enzyme is active in a neutral pH range and differs from trypsin, chymotrypsin, and plasmin (8, 9). Immunofluorescent studies, using anti-SH-P antibodies, indicate that in cutaneous Arthus lesions SH-P! is localized in perivascular mononuclear cells (33). The cellular origin of SH-P2 has not been established. The SH-independent proteases may originate from PMN-leucocytes, because recent results in our laboratory indicate that the cutaneous Arthus reaction in rabbits has at least two components, each characterized by its morphological features and chronological sequence and by a distinctive antibody and protease. One component is due to 19S antibody and is characterized by the presence of an SH-dependent protease; the second component is due to 7S antibody and is associated with SH-independent proteases, similar to NSH-Ps noted above. The later lesions are significantly reduced by nitrogen mustard, an agent known to destroy PMN-leucocytes (1,2, 34). Recently Janoff and Zeligs (35) demonstrated that a lysate of human PMNleucocyte granules contained a neutral protease. When the lysate was injected intradermally into rabbits, it induced a rapid haemorrhagic inflammatory reaction. Renal basement membrane was degraded in vitro at neutral pH and ultrastructural studies showed that the lysate altered vascular basement membrane in vivo. Human PMN-leucocyte granules can also lyse elastic tissue (36). This neutral protease seems to differ from both lysosomal cathepsins and trypsin-like esterases. The manner in which it is activated and released from human PMN-leucocytes in the immune reaction is unknown, although some evidence was presented by Janoff and Zeligs that it was released during incubation of these cells with immune precipitates. This enzyme differs from the Arthus NSH-Ps, in that the Arthus NSH-Ps cannot induce significant tissue injury. It is well known that PMN-leucocyte lysosomes contain acid proteases or cathepsins which are able to injure tissue. These acid proteases can induce tissue injury by at least two mechanisms. First, they are capable of degrading many proteins (37), including basement membrane (38). Secondly, kinin is generated when leucocyte lysosomes are incubated at acid pH with a kininogen (39). These cathepsins also differ from Arthus NSH-Ps in that their optimum pH is in the acid range, while the optimum for NSH-Ps is neutral. Lagunoff and Beneditt (40) found yet another protease in extracts of mast
30
K. Udaka
cells obtained from the peritoneal cavity of rats. This enzyme resembles porcine and bovine chymotrypsin-A more than chymotrypsin-B or -C, since it hydrolyses benzoyl-L-tyrosine thylester more rapidly than either benzoyl-L-leucine or benzoylL-methionine ethylester. Recently, Pasten and Almquist (41) have purified a similar mast cell protease from rat thyroid homogenate. In preliminary studies in our laboratory, no evidence has been obtained to suggest that the Arthus NSH-P is identical with the mast cell protease. The precise role of proteases in the mechanism of the inflammatory process remains to be elucidated. As summarized recently ( 1 ), several types of permeability factor can be isolated from cutaneous Arthus lesions in rabbits. Most of these factors are polypeptides. By analogy with the formation of plasma kinins (bradykinin, kallidin, and others), it is postulated that the tissue proteases present in inflamed tissue may act by producing 'tissue kinins' with vasoactive properties. SUMMARY
The possible role of tissue proteases in the induction and progression of allergic inflammation has been investigated using the Arthus reaction as the principal model. 1 / From cutaneous Arthus lesions in rabbits, four tissue proteases, two SHdependent (SH-Pj and SH-P2) and two SH-independent (NSH-Pi and NSH-P2), have been isolated by chromatography, using a combination of molecular sieve and ion-exchange resins. One of the proteases (SH-Pi) is probably a specific enzyme activated during the Arthus reaction. It increases in parallel with the development of cutaneous Arthus lesions and decreases as the inflammation subsides. The other proteases isolated (SH-P2, NSH-P1? NSH-P;) probably occur in many inflammatory lesions, for example in thermal and chemical injury. 2 / When the proteases are injected intradermally into rabbits the SH-Ps induce a significant inflammatory response marked by haemorrhage, but neither of the NSH-Ps did so. There was a parallel between the proteolytic activity of the SH-Ps and the intensity of inflammatory response. The lesion produced by them reproduced the main features of the Arthus reaction. 3 / A haemorrhagic factor (HR 2 ), similar to the one isolated from Arthus lesions, is formed in the lesions induced by the SH-Pj. This factor causes vascular congestion and haemorrhage from small vessels. It is likely that the SH-Pj act on tissue to produce HR2. ACKNOWLEDGMENTS
The author wishes to express his gratitude to Drs A. C. Ritchie and H. Z. Movat for valuable suggestions and criticisms in the preparation of this manuscript.
Proleolytic Mechanism of Allergic Inflammation
31
REFERENCES 1 UDAKA, K. The Arthus reaction. In Inflammation, Immunity and Hypersensitivity, edited by H. Z. Movat (Harper and Row, New York, 1971 ), chap. 7, p. 389 2 UDAKA, K. Fed. Proc. 25: 681, 1966 3 UDAKA, K., and UDAKA, K. Fed. Proc. 29: 690, 1970 4 UDAKA, K., and UDAKA, K. Comparative study of tissue proteases in inflammation (in preparation) 5 UDAKA, K. Kumamoto Med. J. 16: 55, 1963 6 UDAKA, K., and HAYASHI, H. Symp. Enzyme Chem. 16: 71, 1964 7 HAYASHI, H., UDAKA, K., MiYosHi, H., and KUDO, s. Lab. Invest. 14: 665, 1965 8 UDAKA, K. Kumamoto Med. J. 16: 70, 1963 9 HAYASHI, H., TOKUDA, A., and UDAKA, K. J. Exp. Med. 112: 237, 1960 10 TAKEUCHI, Y., and UDAKA, K. Fed. Proc. 28: 311, 1969 11 UDAKA, K. Fed. Proc. 26: 310, 1967 12 UDAKA, K. Fed. Proc. 27: 249, 1968 13 UDAKA, K., and UDAKA, K. Evaluation of "H or "C-labelled antigen in immune reaction (in preparation) 14 PORATH, j. Biochim. Biophys. Acta 39: 193, 1961 15 SOBER, H. A., CUTTER, F. J., WYCKOFF, M. M., and PETERSON, E. A. J. Amer. Chem. Soc. 78: 1956 16 MOORE, s., and STEIN, w. H. J. Biol. Chem. 192: 663, 1951 17 UDAKA, K. Molecular mechanisms in inflammation. II. Isolation of vasoactive peptides from cutaneous Arthus reaction of rabbit and their role in inflammation (in preparation) 18 KUNITZ, M. J. Gen. Physiol. 30: 291, 1947 19 HURLEY, J. V. Aust. J. Exp. Blol. Med. Sci. 41: 171, 1963 20 UDAKA, K., and HAYASHI, H. Biochim. Biophys. Acta 97: 251, 1065 21 HARADA, Y., ITU, K., and UDAKA, K. Mie Med. J. 8: 343, 1958 22 HELLERMAN, L., and CHINARD, E. p. Determination of sulfhydryl groups in certain biological substances. In Methods of Biochemical Analysis, edited by D. Glick (Interscience Pub., New York, 1954), vol. l,p. 14 23 UDAKA, K., and HAYASHI, H. Biochim. Biophys. Acta 104: 600, 1965 24 BENACERRAF, B. Int. Cong. Microbiol. (6th) 2: 85, 1953 25 HUMPHREY, j. H. Brit. J. Path. 36: 268, 1955 26 COCHRANE, c. o. The Arthus reaction. In The Inflammatory Process, edited by B. W. Zweifach, L. Grant, and R. T. McCluskey (Academic Press, New York, 1965), p. 613 27 STETSON, c. A., JR. J. Exp. Med. 94: 347, 1951 28 YOSHIDA, K., YOSHINAGA, M., and HAYASHI, H. Nature (London) 218: 977, 1968 29 YOSHINAGA, M., MAYUMi, M., YAMAMOTO, s., and HAYASHI, H. Nature (London) 225: 1138, 1970 30 WARD, p. A., COCHRANE, c. o., and MÜLLER-EBERHARD, H. j. J. Exp. Med. 122: 327, 1965 31 WARD, p. A., COCHRANE, c. G., and MÜLLER-EBERHARD, H. j Immunology 11: 141, 1966 32 UNGAR, G., and HAYASHI, H. Ann. Allerg. 16: 542, 1958 33 UDAKA, K., and UDAKA, K. Fed. Proc. 28: 616, 1969 34 UDAKA, K. Molecular mechanisms in inflammation. I. Immunological and biochemical analysis of the cutaneous Arthus reaction in rabbits (in preparation) 35 JANOFF, A., and ZELIGS, J. D. Science 161: 702, 1968 36 JANOFF, A., and SCHERER, J. J. Exp. Med. 128: 1137, 1968 37 WASI, s., MURRAY, R. K., MACMORINE, D. R. L., and MOVAT, H. z. Brit. J. Exp. Path. 47: 411, 1966 38 COCHRANE, c. G., and AIKIN, B. s. J. Exp. Med. 124: 733, 1966 39 GREENBAUM, L. M., and KIM, K. s. Brit. J. Pharmacol. Chemother. 29: 238, 1967 40 LAGUNOFF, D., and BENEDITT, E. Ann. New York Acad. Sci. 103: 185, 1963 41 PASTEN, i., and ALMQUIST, s. J. Biol. Chem. 241: 5090, 1966
Immunoglobulin Complexes in Serum and Synovial Fluid of Persons with Rheumatoid Arthritis IRVIN BRODER, REUBEN BAUMAL, DUNCAN A. GORDON, M U R R A Y B. UROWITZ, AND EILLEEN SHINDER
It was demonstrated a decade ago that soluble antigen-antibody complexes were responsible for the widespread arteritis and glomerular injury seen in experimental serum sickness ( 1 , 2 , 3 ) . This finding stimulated considerable interest in the possibility that soluble immune complexes might be responsible for a number of previously unexplained diseases affecting both animals and man. Studies carried out since that time have yielded suggestive evidence that soluble immune complexes may be operative in the nephritis of New Zealand hybrid mice and of humans with systemic lupus erythematosus as well as in the lupus-like syndrome which affects Aleutian mink (4, 5, 6). In the case of Aleutian mink disease, the offending immune complexes appear to consist of virus combined with a nonneutralizing antiviral antibody, whereas the complexes in the nephritis of hybrid mice and systemic lupus contain DNA combined with anti-DNA. One of the problems encountered in investigating the role of soluble immune complexes in human disease has been in finding a practical and sensitive method for detecting the complexes in serum and other body fluids. Our initial approach has been to develop an assay system, based on the capacity of soluble immune complexes to stimulate histamine release from guinea-pig lung tissue in vitro (7). This biological assay is an extremely sensitive one and is capable of detecting soluble immune complexes present at a concentration of a few micrograms per millilitre. From the University of Toronto Departments of Medicine, Pathology, and Pharmacology and the Institute of Medical Science, the Immunology Laboratories, the Toronto Western Hospital, and the Rheumatic Disease Unit, the Wellesley Hospital, Toronto, Ontario. Supported by research grants from the Canadian Arthritis and Rheumatism Society and the Medical Research Council of Canada.
Immunoglobulin Complexes in Serum and Synovial Fluid
33
TABLE 1 EFFECT OF NORMAL RABBIT SERUM ELECTROPHORETIC FRACTIONS ON
HISTAMINE RELEASE
BY SOLUBLE IMMUNE COMPLEXES
(Residual histamine-releasing activity for 3 ug of soluble complexes mixed with 80 ug of electrophoretic fraction) Albumin Alpha globulin Beta globulin Gamma globulin Fast Slow Total
82 ±37% 167 + 45% 112±28% 3 ±2% 4±1% 5 ±2%
Since a number of agents have the capacity to activate this assay system, considerable attention was given to establishing criteria of specificity (8). Table I shows the results obtained when the electrophoretic fractions of serum were mixed with a fixed amount of soluble immune complexes before testing in the bioassay. The histamine-releasing activity was inhibited only in the presence of gamma globulin, because of competition between the immune complexes and gamma globulin for the same receptor in the lung tissue. Similar results are obtained with human or rabbit gamma globulin. Studies utilizing gel filtration on Sephadex G-200 demonstrated that the inhibitory activity was located in the middle fraction containing the 7S gamma globulins (7). Of the different agents which activate histamine release in the assay system, only soluble immune complexes and aggregated gamma globulin were totally inhibited by gamma globulin. This inhibitory relationship of gamma globulin was a disadvantage, since to detect the histaminereleasing activity of immune complexes present in serum or synovial fluid it was necessary to separate the complexes from the inhibitory 7S gamma globulins. However, separation was readily accomplished by gel filtration on Sephadex G-200, in which soluble complexes were eluted in the first or excluded fraction. On the other hand, the inhibitory relationship was advantageous, since it provided a test which specifically identified the histamine-releasing activity of soluble immunoglobulin complexes. This test of specificity was applied in all of the studies to be described. The methods and materials and all experimental details of the foregoing and following studies have been published (9). Table n shows the results obtained when 428 human sera were examined in the bioassay system. The sera of normal individuals and persons with a variety of diseases were consistently negative. However, a factor behaving biologically as a soluble immune complex was found in one-third of persons with rheumatoid arthritis, in one-sixth of persons with systemic lupus erythematosus, and in one person each with anaphylactoid purpura, polyarteritis, and scleroderma.
34
/. Broder et al.
TABLE II RESULTS OF SERUM TESTS FOR HISTAMINE-RELEASING ACTIVITY
Number of sera Tested Healthy Ankylosing spondylitis Charcot's joint Degenerative joint disease Gout Psoriatic arthritis Reiter's syndrome Undiagnosed arthritis Infectious mononucleosis Myocardial infarction Postcardiotomy syndrome Rheumatic fever, acute Urticaria, chronic Glomerulonephritis, acute Hepatitis, lupoid Polymyositis Serum sickness (horse) Sjogren's syndrome Miscellaneous Anaphylactoid purpura Polyarteritis Rheumatoid arthritis Scleroderma Systemic lupus erythematosus Total
30 15 1 14 10 7 7 6 2 13 10 5 4 10 2 4 10 2 11 1 4
210 14
36 428
Active 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 1
72 1
6
81
TABLE III RESULTS OF SYNOVIAL FLUID TESTS FOR HISTAMINE-RELEASING ACTIVITY
No. of synovial fluids
Rheumatoid arthritis Ankylosing spondylitis Degenerative joint disease Erythema multiforme Gout Psoriatic arthritis Reiter's syndrome Systemic lupus erythematosus Undiagnosed arthritis Total
Tested
Active
104 4 11 1 12 10 1 1 8 152
68 0 0 0 0 0 0 0 0 68
Immunoglobulin Complexes in Serum and Synovial Fluid
35
Table in displays the findings in a similar study of the synovial fluid of 152 persons suffering from different forms of arthritis. A factor behaving as a soluble immune complex was found only in rheumatoid arthritis and occurred here in 65 per cent of patients examined. This factor, found in serum and synovial fluid, was named the rheumatoid biologically active factor, or RBAF, and our studies to date have been mainly concerned with further investigations of its nature and determining its significance in rheumatoid arthritis. The RBAF was eluted from Sephadex G-200 in the excluded fraction, and in sucrose density-gradient ultracentrifugation it was found in association with immunoglobulin M (9). These characteristics are in keeping with a molecular weight in the range of one million or greater. However, the RBAF was removed in the precipitate obtained when positive samples were absorbed with antiserum specific for human immunoglobulin G (10). Similar studies carried out using anti-IgA or anti-IgM showed no absorption of the RBAF. Since the RBAF contained IgG, yet was several-fold heavier than IgG, these findings clearly indicated that the RBAF was a complex which contained immunoglobulin G. We are continuing our efforts to characterize the exact nature of this complex, and we have not yet proved whether it is an antigen-antibody complex or some other type of immunoglobulin complex. Townes and his associates have delivered several papers over the past few years describing a synovial fluid factor which was cryoprecipitable and was inferred to be an immune complex on the basis of exhibiting complement-fixing activity (11, 12). They also obtained indirect evidence that this factor was a complex of DNA and anti-DNA. In contrast with these findings, the RBAF is not cryoprecipitable and RBAF-positive samples of synovial fluid are not distinguishable from RBAF-negative samples in their beta 1C content or in their anticomplementary activity. These findings suggest that the factor under study by Townes and his associates is different from the RBAF. Nevertheless, a series of 16 rheumatoid sera and 23 synovial fluids were examined for the presence of free DNA, anti-DNA, and anti-single-stranded DNA (HDNA) by the use of double diffusion in 0.5 per cent agarose. Anti-HDNA was more commonly found than anti-DNA, but both were randomly distributed between RBAFpositive and RBAF-negative samples. However, free DNA was most commonly found in RBAF-positive synovial fluids (8/14). The occurrence of free DNA in serum was too infrequent to enable a comparison of frequency between RBAF-positive and RBAF-negative samples. These findings are in keeping with several interpretations, among which is the possibility that the RBAF is a complex of DNA and anti-DNA, in the presence of excess antigen. We are exploring this interpretation by several additional approaches, including treatment of the RBAF with DNAase. Our results to date indicate that there is no loss of RBAF activity following DNAase treatment at neutral pH, suggesting that DNA and the RBAF may merely parallel one another. Hannestad in 1967 (13) and Winchester and his associates in 1970 (14) reported that some samples of rheumatoid synovial fluid contained complexes consisting of IgG and 7S anti-IgG. Similar complexes were previously described in
36
I. Broder et al.
Figure 1 Analytical ultracentrifugation of serum of patient U.S. Top line, pH 6.3; bottom, pH 3.0.
rheumatoid serum by Kunkel and co-workers (15), Chodirker and Tomasi (16), and Schrohenloher (17). These complexes appear on ultracentrifugal analysis mainly between the 19S and 7S peaks and are referred to as intermediate complexes. Dissociation of these complexes is seen when ultracentrifugation is carried out at pH 3. Figure 1 shows these intermediate complexes in a sample kindly examined for us in analytical ultracentrifugation by Dr Murray Freedman. At pH 6.3 the intermediate complexes were seen between the 19S and 7S peaks, but they disappeared when the centrifugation was performed at pH 3. We have encountered only two samples of serum which contained intermediate complexes of this type and both were RBAF-negative. We have not performed similar studies on synovial fluid. Winchester and his associates have demonstrated that the presence of intermediate complexes in synovial fluid is associated with an increase in anticomplementary activity and a decrease in beta 1C content. However, we are unable to distinguish between RBAF-positive and RBAF-negative samples on the basis of either parameter, and have found that the RBAF is not absorbed by anti-human beta 1C. The same workers have also shown that intermediate complexes retain rheumatoid factor activity following reduction and alkylation, whereas we have found that the RBAF is stable to reduction and alkylation and following this treatment demonstrates no rheumatoid factor activity (10). Therefore, the foregoing differences suggest that the RBAF is not the same as an intermediate complex. We are continuing our efforts to characterize the RBAF further and to purify it. We have also been directing our attention towards clarifying the significance of the RBAF in a prospective study of a group of 127 patients with rheumatoid arthri-
Immunoglobulin Complexes in Serum and Synovial Fluid
37
tis. The initial assessment demonstrates that patients who exhibit the RBAF in their sera suffer from a more severe form of disease, as indicated by a weaker grip strength and more advanced articular x-ray changes; a more widespread form of disease was indicated by the presence of a higher frequency of extra-articular features (18). The RBAF was not an indicator of acute inflammatory activity in this assessment, since it did not correlate well either with the Lansbury index of articular inflammation or with the erythrocyte sedimentation rate. However, a relationship with the Lansbury index was found in the second assessment of the same patients, as shown below. The RBAF did not correlate with IgM rheumatoid factor since the mean latex titre was the same in both RBAF-positive and RBAFnegative groups. The RBAF also did not correlate with IgG rheumatoid factor, since the two patients we have encountered with this type of rheumatoid factor were both RBAF-negative. More recently we have completed the second assessments carried out on 107 of the original 127 patients. The mean interval between the first and second assessments was 36 weeks, during which 24 of the patients converted from positive to negative or vice versa. Table iv shows representative data indicating that persons who had converted to RBAF-positive were worse in various clinical parameters than persons who recently converted to negative. Thus, synovial effusions were present in 91 per cent of those converting to positive and in only 46 per cent of those converting to negative. The grip strength was similarly decreased in the positive group. The articular index was almost twice as high in the positive group, and the use of systemic steroids was correspondingly more frequent. When the over-all physician-patient evaluation was considered without the physician knowing the RBAF status of the patient, 9 per cent of the positive group were considered to be better and 56 per cent worse. Of the negative group, 62 per cent were considered to be better and only 15 per cent worse. The sedimentation rate and the latex fixation test did not change significantly. Thus, persons converting to positive exhibited more severe disease than those converting to negative. In order to examine whether a change in RBAF status was associated with a change in clinical status, we then compared the results of the same parameters within each group at both the first and second assessments. Table v shows that the group which converted from positive on the first assessment to negative on the second exhibited a corresponding decrease in disease severity. This was manifested by a lower frequency of synovial effusions, a higher grip strength, and a lower articular index, without an increased usage of corticosteroid therapy. These findings stand in contrast with those of persons remaining RBAF-positive at both assessments who did not exhibit these trends, with the exception of a smaller improvement in grip strength. Therefore, the group which converted from positive to negative appeared relatively improved. Table vi demonstrates that patients who converted from RBAF-negative on the first assessment to positive on the second exhibited an increased frequency of synovial effusions and of corticosteroid therapy. Although there was no corresponding worsening of the grip strength or articular index in these patients, their counter-
38
/. Broder et al.
TABLE IV SECOND ASSESSMENT RESULTS IN RBAF
CONVERTERS
RBAF conversion from first to second assessment Negative to positive Number of converters Presence of synovial effusion (%) Grip strength (mm Hg) Articular index Systemic corticosteroid (%) Over-all assessment Better (%) Worse (%)
Positive to negative
11
13
91 107 58 64
46 155 33 15
9 56
62 15
TABLE V RESULTS OF FIRST AND SECOND
ASSESSMENTS
IN 13 P A T I E N T S WHO C O N V E R T E D FROM RBAF-POSITIVE TO RBAF-NEGATIVE
RBAF status and assessment sequence Positive first Presence of synovial effusion (%) Grip strength (mm Hg) Articular index Systemic corticosteroid (%)
69 95 59 15
Negative second 46 155 33 15
TABLE VI RESULTS OF FIRST AND SECOND ASSESSMENTS IN 11 PATIENTS WHO CONVERTED
FROM
RBAF-NEGATIVE TO RBAF-POSITIVE
RBAF status and assessment sequence
Presence of synovial effusion (%) Grip strength (mm Hg) Articular index Systemic corticosteroid (%)
Negative first
Positive second
73 109 57 55
91 107 58 64
Immunoglobulin Complexes in Serum and Synovial Fluid
39
parts who remained negative at both assessments showed a marked improvement in these parameters. Therefore, it is noteworthy that the grip strength and articular index failed to improve in persons who converted from negative to positive. On the foregoing grounds, this group of converters was considered to be relatively worse. The two groups which underwent a conversion in their RBAF status consisted of relatively small numbers of patients, not suited for statistical analysis. However, it appeared to be significant that the parameters with the best capacity to show a short-term change all exhibited trends towards relative improvement when the RBAF conversion was to negative, and towards relative worsening when the conversion was to positive. In conclusion, our studies to date indicate that the RBAF is an immunoglobulincontaining complex, the presence of which shows a number of gross correlations with the clinical status of rheumatoid disease. However, the information available does not yet allow one to choose between the possibility that the RBAF is involved in pathogenesis or whether the RBAF is a by-product of severe rheumatoid disease, or whether both the RBAF and rheumatoid disease are separate manifestations of a common process. We have also yet to determine whether the RBAF contains a second component, such as a micro-organism, which is the antigen of the immunoglobulin G constituent identified at present. ACKNOWLEDGMENTS
We are grateful to Mrs Christine Gabay, Mrs Rose Hajdinjak, and Miss Donna McAvoy for their excellent technical assistance. REFERENCES 1 GERMUTH, F. J. Exp. Med. 97: 257, 1953 2 DIXON, F. j., VASQUEZ, j. j., WEioLE, w. o., and cocHRANE, c. o. Arch. Path. 65: 18, 1958 3 MCCLUSKEY, R. T., BENACERRAF, B., POTTER, J. L., and MILLER, F. J. Exp. Med. I l l : 1 8 1 ,
1960 4 KRISHNAN, c., and KAPLAN, M. H. J. Clin. Invest. 46: 569, 1967 5 PORTER, D. D., and LARSON, A. E. Proc. Soc. Exp. Biol. 126: 680, 1967 6 LAMBERT, p. H., and DIXON, F. J. J. Exp. Med. 127: 507, 1968 7 BAUMAL, R., and BRODER, i. Clin. Exp. Immunol. 3: 525, 1968 8 BRODER, i., BAUMAL, R., and KEYSTONE, E. Clin. Exp. Immunol. 3: 537, 1968 9 BRODER, i., BAUMAL, R., GORDON, D., and BELL, D. Ann. New York Acad Sci. 168: 126, 1969 10 BAUMAL, R., and BRODER, i. Clin. Exp. Immunol. 3: 555, 1968 11 TOWNES, A. s., STEWART, c. R., JR., and MARCUS, R. L. Arthritis Rheum. 9: 878, 1966 12 MARCUS, R. L., and TOWNES, A. s. Arthritis Rheum. 11: 497, 1968 13 HANNESTAD, K., and MELLBYE, o. J. Clin. Exp. Immunol. 2: 501, 1967 14 WINCHESTER, R. j., AGNELLO, v., and KUNKEL, H. G. Clin. Exp. Immunol. 6: 689, 1970 15 KUNKEL, H. G., MÜLLER-EBERHARD, H. J., FUDENBERG, H. H., and TOMASI, T. B. J. Clin. Invest.
40: 117, 1961 16 CHODIRKER, w. B., and TOMASI, T. B. J. Clin. Invest. 42: 876, 1963 17 SCHROHENLOHER, R. E. J. Clin. Invest. 45: 501, 1966 18 GORDON, D. A., BELL, D. A., BAUMAL, R., and BRODER, i. Clin. Exp. Immunol. 5: 57, 1969
The Complement System in Rheumatoid Synovitis III.
THE RELATIONSHIP OF SYNOVIAL FLUID
COMPLEMENT LEVELS TO THE CLINICAL, RADIOLOGICAL, AND PATHOLOGICAL CHANGES IN RHEUMATOID ARTHRITIS MELVIN C. BRITTON, S H A U N RUDDY, JOSEPH M. CORSON, J. LELAND SOSMAN, PETER H. SCHUR, AND K. FRANK AUSTEN
Synovial fluids from patients with rheumatoid arthritis contain less haemolytic complement than fluids from patients with other forms of arthritis (1, 2, 3, 4). Among patients with rheumatoid arthritis, the most profound depressions of synovial fluid complement have been observed in those whose sera contain rheumatoid factor (2). In a previous study (4), measurements of individual complement component levels in three groups of patients — those with séropositive and séronégative rheumatoid arthritis and with degenerative joint disease - have yielded patterns of component depletion consistent with activation of the complement system by an immune complex. In addition, immunofluorescent studies of synovial fluid leucocytes from these same patients revealed that intracytoplasmic deposits of complement proteins and immunoglobulins were most frequently found in leucocytes from joints with the most severe depressions of complement levels (5). This report presents clinical, pathological, and radiological information on these three groups of patients whose synovial fluids were previously studied for complement component levels and intraleucocytic protein deposits. MATERIALS AND METHODS
Ninety-three patients with rheumatoid arthritis - all but three either 'classical' or 'definite' by American Rheumatism Association criteria (6) - and 24 patients with From the Harvard Medical School Departments of Medicine, Pathology, and Radiology, the Robert B. Brigham Hospital, Boston, Massachusetts. Supported by research grants from the National Institute of Health Grants Nos. AM 05577, AM 12051, AM 11414, and AM 05076, and grants from the Massachusetts Chapter, Arthritis and Rheumatism Foundation and from the New England Peabody Home Foundation.
The Complement System in Rheumatoid Synovitis
41
degenerative joint disease were studied. The presence of an effusion in a joint, usually the knee, was regarded as sufficient to justify inclusion in the study. A deliberate attempt was made to select patients who had séronégative rheumatoid arthritis. Rheumatoid factor (RF) was determined by the tube dilution latex fixation method (7). Patients with rheumatoid arthritis whose sera or concentrated euglobulins (7) were positive for RF were designated as the séropositive group, RF + ; those who were negative in the tests were designated as the séronégative group, RF . The mean age of the RF+ group was 60 years and that of the RF~ group was 51 years. The mean duration of symptoms for the RF+ group was 10 years and for the RF~ group 6 years. The mean age of the group with degenerative joint disease was 58 years, and the mean duration of symptoms was 12 years. The arthrocenteses were performed with a Parker Pearson needle after the skin had been cleaned with iodine and alcohol. Routine studies of synovial fluids were performed as outlined by Ropes and Bauer (8). Whole haemolytic complement (CH50) was determined by the method of Kent and Fife (9). Sera and synovial fluids were obtained simultaneously whenever possible and were frozen at —70°c within 90 minutes after harvesting. Nearly all patients were biopsied, either at time of arthrotomy or with a Parker Pearson needle, and all biopsies were submitted for routine histologie examination. Studies on synovial fluid cells (5) and complement components (4) are reported elsewhere. Tissue was fixed in 10 per cent formalin and embedded in paraffin. Sections were stained routinely with haematoxylin and eosin. Selected sections were stained by standard methods for collagen, iron, reticulin fibres, or capillary basement membranes using the McManus modification of the periodic acid Schiff stain (10). From 1 to 10 slides of each case were reviewed. The histologie examination was used in the classification of patients by the American Rheumatism Association criteria. Clinical Studies All patients' charts were reviewed for evidence of systemic lupus, dermatomyositis, scleroderma, rheumatic fever, ulcerative colitis, regional enteritis, psoriasis, sarcoid, spondylitis, Reiter's syndrome, or gout. The presence of any of these excluded the patient from further consideration. All patients who had had their disease longer than two years were assessed as to clinical course using the criteria of Sharp et al. (11): remitting, unremitting, or intermediate. A history of nodules, uveitis, fever, or weight loss was noted. A history of involvement of any of the proximal interphalangeal, metacarpophalangeal, wrist, elbow, shoulder, hip, knee, ankle, or foot joints with swelling, pain, or tenderness, and limitation of motion was used in scoring the extent of joint involvement in a particular patient. The presence of nodules, splenomegaly, lymphadenopathy, and vasculitis was also noted. The use of gold, antimalarials, steroids, and other drugs during the three years prior to biopsy was recorded. Salicylates were generally used, and the mean daily dosage employed in the four weeks prior to biopsy was tabulated.
42
M. C. Briñón et al.
Radiological Findings x-rays were reviewed for 56 of the 93 patients with rheumatoid arthritis and most of those with degenerative joint disease by the radiologist, who had no knowledge of the clinical course or laboratory findings. Initially, x-rays of the joint which had been biopsied were reviewed; and the amount of periarticular demineralization, effusion, soft tissue swelling, and joint space narrowing and the presence of erosions and cysts, ankylosis, cortical impaction, and subluxation were assessed ( 12). Subsequently, all other x-rays of joints were examined in a similar manner and recorded separately. The number of joints involved was counted, using standard radiographie division of joints (13). If the radiographie picture alone was felt to be consistent with rheumatoid arthritis, the involvement was scored as 'early,' 'moderate,' or 'marked.' Pathology The histologie sections were examined without any knowledge of the clinical history or diagnosis. Morphologic alterations which were selected for review were assigned a score according to the severity of the changes with 0, 1, 2, or 3 being equated with no, slight, moderate, or severe changes, respectively. Sixteen specific findings were graded by the above criteria. These included, in the synovial surface layers of the biopsy, the amount of synoviocytic hyperplasia, the presence of giant cells which appeared to derive from synoviocytic lining cells, and the amount of polymorphonuclear invasion. At deeper levels, the amount of oedema, fibrosis, and haemorrhage was graded, and 'calcification,' as judged by the presence of dark blue staining material in the haematoxylin and eosin stain, was scored. In this layer also, the number of lymphocytes, plasma cells, and neutrophils was also graded. The blood vessels were graded as to the amount of leucocytic congestion, thrombosis, and 'capillary-venular occlusive change' (14). The last consisted of obliterative cellular lesions of the capillary venule comprising hypertrophied and hyperplastic endothelial cells or circulating mononuclear cells, but few or no erythrocytes and little or no fibrin. The entire slide was scanned and the amount of fibrin exudation and necrosis graded. When all of the above items had been graded, the cases which were felt to represent rheumatoid arthritis were assigned to one of four phases according to the following morphologic criteria: Phase i: 'exudative phase,' characterized by congestion, oedema, and some exudation of neutrophilic leucocytes and fibrin; Phase ii: 'infiltrative and proliferative phase,' characterized by infiltration by lymphocytes and plasma cells, proliferation of fibroblasts, synoviocytic hyperplasia, and increased numbers of capillaries and histiocytes; Phase in: 'necrotic phase,' characterized by variable areas of necrosis of lining cells and of deeper layers of synovium, associated with deposition of fibrin; and Phase iv: 'fibrotic phase,' characterized by a dominance of fibrosis, often with adhesions, and a relative absence of infiltration, cellular proliferation, and necrosis.
The Complement System in Rheumatoid Synovitis
43
Statistical Analysis Differences between groups were analysed by one-way analysis of variance, and the '/?' figure is given for the hypothesis that the differences among the groups would occur by chance alone (15). RESULTS Mean values for laboratory tests performed on serum and synovial fluid are given in Table i. Haematocrit levels were higher in the group with degenerative joint disease (DJD) than in either of the rheumatoid groups. There was no significant difference in the white blood cell (WBC) counts and the serum globulin levels for the three groups. The sedimentation index was higher in the patients with rheumatoid arthritis. The serum CH50 levels showed a significant difference, with the RF~ group having the highest mean value and the DJD group the lowest. Detailed information about serum and synovial fluid complement component levels has been presented previously (4). The mean synovial fluid white blood cell count for the RF+ group was slightly greater than for the RF~ group, and both were markedly higher than in the DJD group. The RF~ group had a slightly higher mean synovial fluid protein level than did the RF + group, and both had significantly higher protein values than the DJD TABLE I L A B O R A T O R Y V A L U E S FOR P A T I E N T S WITH S E R O P O S I T I V E , R F+ , O R S E R O N E G A T I V E , R F ~ , R H E U M A T O I D
ARTHRITIS
O R D E G E N E R A T I V E J O I N T D I S E A S E (DJD)
RF +
RF~
DJD
Serum globulin (gm-%) Serum CH50 (u/ml)i
41.2 (57)'¡ 8,833 (55) 0.84 (57) 1.36 (38) 240 (57)
42.0 (36) 8,926(31) 0.77 (35) 1.30 (28) 265 (35)
45.1 (24)*** 8,563 (19) 0.58 (24)* 1.13 (12) 228 (22)**
Synovial fluid values WBC (mm3) Protein (gm-%) Mucin§ Synovial fluid CH50 (u/ml)
11,980 (40) 4.2 (58) 2.1 (28) 52.2 (58)
9,135 (30) 4.6 (37) 1.9 (17) 123.6(37)
1,530(15)*** 3.3 (26)*** 1.3 (14)*** 79.5 (25)***
Mean serum values Haematocrit (%) WBC (mm3) BSlt
fSedimentation index: most rapid fall of RBC in mm/min in any 5-minute interval out of 60 minutes (normal BSI < 0.35 mm/min). ÎNormal serum CH50 150-250 u/ml. §Rated on a scale of 1 to 4, with 4 indicating total friability and lack of cohesion. UNumbers in parentheses represent the number of samples analysed. *p < 0.05. **p < 0.025. ***p < 0.01.
44
M. C. Britton et al.
group. The mucin test indicated friability in the group with rheumatoid arthritis. Synovial fluid CH50 levels in the RF~ group were significantly higher than in the RF+ group. When the patients were segregated according to this CH50 level, no significant differences were noted among the laboratory values shown in Table I for patients with low (0-50), intermediate (51-100), or high (>100) levels. Clinical characteristics for 84 patients with rheumatoid arthritis are given in Table n. The frequency of each characteristic in both RF+ and RF~ patients is noted as well as the frequency in patients with three ranges of synovial fluid CH50 levels. The clinical course as analysed by the criteria of Sharp et al. (11) revealed an association between low synovial fluid complement levels and an unremitting course. The presence of subcutaneous nodules was associated with the presence of RF and with low CH50 levels. No significant difference was found between the groups when they were analysed for the presence of weight loss, fever, splenomegaly, or vasculitis. Patients with RF and with low synovial fluid CH50 had a greater extent of joint involvement, both by history and at time of examination, than those patients who lacked RF or who had higher CH50s. Patients who were séropositive tended to be on higher doses of salicylates and to have received occasional systemic corticosteroids more frequently than patients who were séronégative; when patients were divided by complement level, no differences were apparent. The séropositive or low synovial fluid CH50 groups had a higher frequency of chrysotherapy than the séronégative, high CH50 groups. Radiological Findings x-ray findings in the biopsied joints are presented in Table in. The data were again analysed in two ways: first, for the presence of RF, and next by division of the patients into low, medium, and high synovial fluid CH50 groups. The biopsied joint in the RF+ patients was associated with significantly more periarticular demineralization and joint space narrowing. When the data were analysed by the CH50 level, the patients with a low level had more periarticular demineralization, joint space narrowing, and cortical impaction than did the patients with a high level. Radiological data for all joints at the time of the study are summarized in Table iv. The presence of RF was associated with periarticular demineralization, joint space narrowing, erosions or cysts, and cortical impaction. A larger number of joints were involved in the RF+ group. Except for the presence of erosions or cysts, all of the findings above were also present in the low synovial fluid CH50 group. In addition, there also tended to be more effusion or soft tissue swelling in this group. The over-all radiologie change was more severe in the RF+ and low CH50 groups. Pathology Synovia from 39 patients with rheumatoid arthritis were examined (Table v). Comparison of the synovia from the RF+ and the RF~ groups revealed more
TABLE II CLINICAL CHARACTERISTICS OF PATIENTS WITH RHEUMATOID ARTHRITIS
Synovial fluid CH50
1.
2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12.
Course (remitting/unremitting)! Presence of subcutaneous nodules Weight loss associated with illness Fever at any time Presence of splenomegaly at any time Vasculitis during course of illness Extent of joint involvement throughout illness (slight/moderate/severe) Extent of joint involvement at time of study (slightly/moderate/severe) >2.5 grams aspirin per day Systemic steroids within 3 years of study Antimalarials within 3 years of study Gold within 3 years of study
RF~
RF +
0-50
51-100
>100
12/14 0/31 3/30 0/30 1/31 0/31 15/11/15
16/35 12/53*** 12/53 2/53 0/53 2/53 4/14/35***
7/19 8/31 9/33 1/33 0/33 1/33 1/8/23
11/14 4/31 5/31 3/31 0/31 1/31 6/6/13
9/13** 0/28** 0/27 0/27 1/28 0/28 12/11/4***
24/4/3
10/24/19***
7/14/13
10/9/6
17/5/3***
24/31 6/31 9/31 3/31
50/53** 28/53*** 24/53 20/53***
32/33 16/33 15/33 10/33
24/31 15/31 11/31 12/31
24/28 23/28 9/28 1/28***
fThe few patients with an intermediate course are excluded. **p < 0.025. **p < 0.01.
TABLE III RADIOLOGIC FINDINGS IN BIOPSIED JOINTS OF PATIENTS WITH RHEUMATOID ARTHRITIS Synovial fluid CH50 Findings
Categories
RF~
RF +
0-50
51-100
>100
Periarticular demineralization Effusion or soft tissue swelling Joint space narrowing Erosions or cysts Cortical impaction Dislocation or subluxation Patellar involvement
None/moderate/marked Slight/moderate/marked None or slight/moderate/marked None/moderate/marked None/moderate/marked None/slight/moderate None/slight/moderate
21/4/1 6/7/13 18/6/2 20/4/2 22/2/2 25/1/0 22/3/1
9/12/13*** 3/15/16 6/18/10*** 17/8/9 17/8/9 29/4/1 16/12/6
4/6/10 2/8/10 3/9/8 9/5/6 8/6/6 16/3/1 9/8/3
10/6/2 2/8/8 5/10/3 12/2/4 10/4/4 16/2/0 12/5/1
16/4/2*** 5/6/11 16/5/1*** 16/5/1 21/0/1*** 22/0/0 17/2/3
*p < 0.01.
TABLE IV RADIOLOGIC FINDINGS IN ALL JOINTS OF BIOPSIED PATIENTS WITH RHEUMATOID ARTHRITIS Synovial fluid CH50 Findings
Categories
RF~
RF +
0-50
51-100
>\QO
Periarticular demineralization Effusion or soft tissue swelling Joint space narrowing Erosions or cysts Number of joints involved Ankylosis Cortical impaction Dislocation or subluxation Over-all severity
None/moderate/marked Slight/moderate/marked None or slight/moderate/marked None or slight/moderate/marked 1-10/1 1-20/ >21 None/slight/moderate or marked None/slight/moderate or marked None/slight/moderate or marked Early /moderate/marked
17/6/4 12/12/3 20/5/2 18/7/2 18/7/2 24/1/2 23/1/3 24/2/1 14/12/1
3/13/13*** 10/10/9 7/12/10*** 3/17/9*** 4/8/17*** 22/5/2 11/9/9*** 19/8/2 5/15/9***
1/6/8 4/3/8 2/6/7 2/8/5 2/4/9 9/4/2 4/4/7 9/4/2 3/6/6
5/7/6 7/10/1 6/8/4 5/9/4 6/5/7 16/1/1 9/5/4 13/4/1 7/7/4
14/6/3*** 11/9/3*** 19/3/1*** 13/8/7 14/6/3** 21/1/1 21/1/1*** 21/2/0 9/14/0*
*p < 0.05.
**p < 0.025.
***p < 0.01.
TABLE V PATHOLOGY
Synovial fluid CH50 Findings
Categories
RF
RF +
0-50
51-100
>100
Surface of synovium Synoviocytic hyperplasia Synoviocytic giant cells Neutrophilic infiltration
None or slight/moderate/marked None or slight/moderate/marked None or slight/moderate/marked
4/13/2 15/4/0 10/7/2
4/9/7 11/5/4 12/8/0
1/6/5 6/3/3 9/3/0
4/4/3 5/5/1 5/6/0
3/12/1 15/1/0** 8/6/2
None None None None None None None
1/5/13 13/5/1 10/8/1 18/1/0 15/4/0 4/7/8 9/7/3
2/9/9 3/8/9*** 9/6/5 14/4/2 12/6/2 3/6/11 6/11/3
2/4/6 2/3/7 4/4/4 8/3/1 6/5/1 2/3/7 4/7/1
1/7/3 2/6/3 6/3/2 8/2/1 6/4/1 3/3/5 4/5/2
0/3/13* 12/4/0*** 9/7/0 16/0/0 15/1/0** 2/7/7 7/6/3
None/slight/moderate None or slight/moderate/marked None/slight/moderate None/slight/moderate
6/9/4 4/10/5 14/4/1 11/13/5
8/11/1 14/6/2* 17/3/0 4/12/4
5/6/1 9/2/1 9/3/0 3/6/3
5/5/1 5/5/1 11/0/0 1/7/3
4/9/3 0/2/9*** 11/4/1 1/12/3
None/slight/moderate None/slight/moderate
10/6/3 14/3/2
4/5/11** 6/4/10**
1/5/7 3/3/6
3/3/5 5/2/4
10/3/3* 12/2/2
Subsurface of synovium (Edema Fibrosis Haemorrhage 'Calcification' Lymphocytes Plasmacytes Neutrophilic infiltration Vessels of synovium Leucostasis Congestion Thrombosis Occlusion General Fibrin exudation Necrosis *p v.iv
B10.D2-old B10.D2-new B10.D2-old B10.D2-new
10x4,11x8,12x2 10x5,11x7,12x1 10x5,11x6,12x1 10x5,11x9,12x1
10.9±0.6( 10.7±0.6Ç 10.7±0.6/ 10.7±0.6J
B10.D2-old
15x2,18x5,20x1,21x1,23x2, 24x1 12x1,13x4,15x2,16x4 15x1,16x1,17x5,18x1 11x1,12x2,15x5,16x2
19.3±3.H V 14.4±1.5j 16.8±1.1/ 14.2±1.?Í
20x2,21x1,24x2,25x2,27x2, 28x1,73x2 13x2,14x1,18x1,19x2,20x1, 21x1,23x1,24x1,26x1
32.3±18.4) > 19.4±4.2 J
0.002 < p< 0.02
13x1,14x2,15x4,16x1,17x2 12x1,13x5,14x2,15x1,16x1
15.1±1.2) 13.6±1.6\
p
B10.D2-new B10.D2-old B10.D2-new B10.D2-old B10.D2-new
Horse
ALS
68/65
-7to-l
B10.D2-old B10.D2-new
*Day zero being the day of transplantation. tMann Whitney U-test. Significant differences are shown in italics.
p
> n 10
pn
10
p < 0.002
0.002