Economics of Public Health: Measuring the Economic Impact of Diseases [Reprint 2016 ed.] 9781512808643
This book is a volume in the Penn Press Anniversary Collection. To mark its 125th anniversary in 2015, the University of
145 38 5MB
English Pages 144 Year 2016
Preface
Contents
List of Tables
List of Charts
Part One. Introduction, and Consideration of the Proposition That “Good Health Is Good Business”
Part Two. The Economic Nature of Health Activities. A Theoretical Analysis
Part Three. The Economic Losses from Poor Health.Their Form and Measurability
Part Four. The Economic Costs to the United States of Poor Health. Illustrative Quantifications for the Diseases Cancer, Tuberculosis, and Poliomyelitis
Appendices
Bibliography
Index
Recommend Papers








![Economics of Public Health: Measuring the Economic Impact of Diseases [Reprint 2016 ed.]
9781512808643](https://ebin.pub/img/200x200/economics-of-public-health-measuring-the-economic-impact-of-diseases-reprint-2016nbsped-9781512808643.jpg)
- Author / Uploaded
- Burton A. Weisbrod
File loading please wait...
Citation preview
Economics of Public Health
Economics of Public Health M e a s u r i n g the Economic Impact of Diseases
by
BURTON A. WEISBROD Washington University St. Louis
1
Philadelphia
University of Pennsylvania Press
Copyright © 1961 by the Trustees of the University of Pennsylvania
Second Printing, 1968
Library of Congress Catalog Card Number: 61-5545
7261 Printed in the United States of America
TO M Y FAMILY
Preface " Better Health is Purchasable." Society is not now making the fullest possible use of existing medical knowledge nor is the rate of increase of our medical knowledge at the maximum possible. Much present morbidity is unnecessary, much mortality premature. Better health is within our grasp if only we choose to pay its price. But what is true about the commodity, health, is equally true of virtually any other commodity one might mention. W e are not producing as many shoes as is possible nor is the rate of increase of shoe capacity at the maximum posssible. However, health is distinguishable from most other commodities in terms of the magnitude of the external economies which it provides and in terms of its "collective-good" nature. An individual is very limited in the extent to which he can economically control his own health unilaterally. As a result, when we think of the organizers of health programs today—programs involving both application of existing knowledge and research to expand that knowledge—we think of groups; we think of government agencies and private foundations such as the American Cancer Society, Heart Association, and National Foundation. W i t h " h e a l t h " being supplied by governmental groups and private philanthropic foundations, we have the case of a commodity which is provided outside the market mechanism. As a result, the usual market test of efficiency in the allocation of resources—profits—is not applied. T h e questions thus arise: are we spending too much, too little, or just the correct amount of money on health in general, and on particular health projects r How ought we determine the appropriate level and composition of health expenditures ? " T h e economist's creed compels him to maintain that decisions that result from deliberate choice among vii
viii
Economics of Public
Health
alternatives yield more satisfactory results than those made by less rational methods." 1 With all the many health-promoting activities that could be carried on, with all the many demands upon limited public health funds, administrators of public health engineering and research programs are sorely in need of some meaningful scientifically defensible standards against which to appraise contending expenditure proposals. The economist should be able to contribute to the establishment of such standards by specifying, within limits, the social benefits from alternative health programs. As the role of government in the economy has grown, the problem of efficient resource allocation in the public sector has received increasing attention from economists. Progress has been made in the analysis and estimation of costs and benefits of public programs, especially in the water resources area; 2 but cost-benefit analysis in the public health area has lagged. 3 The objective of the present stud)' is to reduce the extent of this lag. It is hoped that this study will be of interest to a variety of groups; for, whether from the viewpoint of the academic economist or that of decision makers—legislators, public health administrators, and hospital-planning council leaders—information about the economic consequences of improved health (or losses from poor health) is clearly essential to intelligent behavior. The following pages represent an attempt (1) to set forth a procedure to aid in making rational choices among alternative 'Arthur Smithies, The Budgetary Process in the United States, McGraw-Hill Book Company, Inc., New York, 1955, p. xv. *R. N. McKean, Efficiency in Government Through Systems Analysis, zvith Emphasis on Water Resources Development, John Wiley, New York, 1958; Otto Eckstein, Water-Resource Development: The Economics of Project Evaluation, Harvard University Press, Cambridge, 1958; J. V. Krutilla and Otto Eckstein, Multiple Purpose River Development: Studies in Applied Economic Analysis, Johns Hopkins Press, Baltimore, 1958. 'However, see C.-E. A. Winslow, The Cost of Sickness and the Price of Health, World Health Organization Monograph, Series No. 7, Geneva, 1951; R. Fein, Economics of Mental Illness, Basic Books, New York, 1958.
Preface
ix
p u b l i c h e a l t h p r o j e c t s — t h a t is, t o e s t a b l i s h a f r a m e w o r k f o r e s t i m a t i n g t h e social b e n e f i t s of i m p r o v e d h e a l t h ; and ( 2 ) t o e m p l o y t h e p r o c e d u r e , e v a l u a t i n g q u a n t i t a t i v e l y c e r t a i n of t h e b e n e f i t s t o society of successful a t t e m p t s t o e l i m i n a t e t h r e e specific d i s e a s e s — c a n c e r , t u b e r c u l o s i s , and p o l i o m y e l i t i s . It is h o p e d t h a t t h e p r o c e d u r e will assist in e s t a b l i s h i n g p r i o r i t i e s a m o n g p u b l i c h e a l t h p r o j e c t s , and p e r h a p s also m a k e possible t h e d e t e r m i n a t i o n of t h e m a g n i t u d e s of t h e b e n e f i t s of p a r t i c u l a r p r o j e c t s . In t h e q u a n t i f i c a t i o n a t t e m p t s I b e c a m e p a i n f u l l y a w a r e of t h e d e a r t h of r e l e v a n t d a t a . I w a s c o m p e l l e d , t h e r e f o r e , t o u t i l i z e w h a t s e e m e d t o be t h e best a v a i l a b l e d a t a o r t o m a k e m y o w n e s t i m a t e s — s o m e t i m e s on t h e basis of r a t h e r scanty i n f o r m a t i o n — w h e n n o u s a b l e d a t a w e r e available. I b e l i e v e t h a t t h e d a t a u s e d and t h e e s t i m a t e s m a d e a r e r e a s o n a b l e u n d e r t h e c i r c u m s t a n c e s . It s e e m e d i m p o r t a n t t o a t t e m p t some q u a n t i f i c a t i o n , a l b e i t v e r y i m p e r f e c t , t o s e r v e as an i l l u s t r a t i o n of w h a t could be d o n e t o p r o v i d e a basis f o r r e s o u r c e - a l l o c a t i o n decisions in t h e h e a l t h a r e a . It is h o p e d t h a t in t h e c o u r s e of t i m e m o r e of the n e e d e d d a t a can be o b t a i n e d , so t h a t t h e e s t i m a t e s of m o n e t a r y l o s s e s d u e t o p o o r h e a l t h can be i m p r o v e d , and t h e a p p r o a c h e x t e n d e d t o a d d i t i o n a l d i s e a s e s . M e a n w h i l e , any q u a r r e l which t h e r e a d e r m a y h a v e w i t h p a r t i c u l a r d a t a should n o t c a u s e h i m t o h a s t i l y r e j e c t t h e a n a l y t i c f r a m e w o r k and q u a n t i f i c a t i o n a p p r o a c h developed here. T h e p l a n of this s t u d y is as f o l l o w s : in t h e i n t r o d u c t o r y P a r t O n e , t h e r a t i o n a l e f o r t h i s i n v e s t i g a t i o n is discussed and s o m e p a s t a t t e m p t s t o e m p l o y e c o n o m i c r e a s o n i n g t o b o l s t e r t h e case f o r increased h e a l t h e x p e n d i t u r e s a r e criticized. T h i s is f o l l o w e d by an a n a l y s i s , in P a r t T w o , of t h e f a c t o r s m a k i n g t h e c o m m o d i t y , h e a l t h , u n u s u a l . In P a r t T h r e e a f r a m e w o r k is e s t a b lished f o r d e t e r m i n i n g t h e m o n e t a r y losses r e s u l t i n g f r o m a n y disease ; and use is m a d e of this f r a m e w o r k in P a r t F o u r t o e s t i m a t e l o s s e s in t h e U n i t e d S t a t e s d u e t o c a n c e r , t u b e r c u l o s i s , and p o l i o m y e l i t i s . Finally t h e significance of t h e m o n e t a r y - l o s s
χ
Economics
of Public
Health
estimates is discussed, and the relevance of such information on " l o s s e s " for decisions concerning the allocation of funds to research and other health programs is considered. This study is a revision of my Ph.D. dissertation, submitted to the Department of Economics at Northwestern University in 1958. The original manuscript benefited from comments by Professors Yale Brozen, Robert Eisner, and Elmo P. Hohman. I am particularly grateful to Professor Robert H. Strotz, under whose direction the dissertation was written, for originally interesting me in the economics of resource allocation in the public health field, and for his valuable suggestions and encouragement during the development of the study. Advice on medical aspects of the study was received from Dr. John Hanson of Carleton College, Northfield, Minnesota, and Dr. Ezra V. Bridge of Mineral Springs Sanatorium, Cannon Falls, Minnesota. Finally, revision of the manuscript prior to publication was aided materially bv the comments of Professor E. Douglass Burdick, of the Department of Economic and Social Statistics, Wharton School, University of Pennsylvania. St. Louis, Missouri June, 1960
B. A. W
Contents Chapter Preface List of Tables List of Charts
I. II.
Part One—Introduction, and Consideration of the Proposition T h a t " G o o d Health Is Good Business " Introduction Is Good Health " G o o d B u s i n e s s " ?
Page vii xiii xv
1 7
Part T w o — T h e Economic N a t u r e of Health Activities—A Theoretical Analysis III. IV.
V. VI.
VII.
Introduction to Part T w o
16'
T h e N a t u r e of the Commodity, Better Health Determining the Public's Demand for Health Activities
17 11
Part T h r e e — T h e Economic Losses from Poor H e a l t h — T h e i r Form and Measurability Introduction to Part T h r e e T h e M o n e t a r y Costs to Society of Poor Health— A Taxonomy M e t h o d s of and Prospects for Quantification
SO 33
Part F o u r — T h e Economic Costs to the United States of Poor Health—Illustrative Quantifications for the Diseases Cancer, Tuberculosis, and Poliomyelitis Quantification of Losses from Premature Death, with Application to Tuberculosis, Cancer, and Poliomyelitis
48
28
xii
Economics
of Public
Health
Chapter VIII. Quantification of Losses from Morbidity, and Including T r e a t m e n t Costs, with Application T o Tuberculosis, Cancer, and Poliomyelitis IX. Summary of Quantification, and Conclusions Appendices Appendix I : Consumption Appendix I I : T h e Value of W o m e n ' s Household Production Bibliography Index
Tables Table 1. Hypothetical Demand for Community Health Project
Page 22
2.
Data Used in the Computation of the Present Values of Net Future Earnings, by Age and Sex
.52
3.
Present Values of Net Future Earnings, by Age and Sex, for the United States, at 4 and at 10 Per Cent Discount Rates
60
4.
Preniatu -e-Mortality Losses Resulting from Cancer Death in 1954, by Age and Sex, at 4 and at 10 Per Cent Discount Rates
64
5.
Premature-Mortality Losses Resulting from Tuberculosis Deaths in 1954, by Age and Sex, at 4 and at 10 Per Cent Discount Rates
66
6.
Premature-Mortality Losses Resulting from Poliomyelitis Deaths in 1954, by Age and Sex, at 4 and at 10 Per Cent Discount Rates
68
7.
Production Losses from Cancer-Caused Morbidity, Year 1954 Cases, by Age and Sex
74
8.
Production Losses Expected from Tuberculosis-Caused Morbidity, Year 1954 Cases, by Age and Sex
76
..
Production Losses Expected from
Poliomyelitis-Caused
Morbidity, Year 1954 Cases, by Age and Sex
77
10.
Total Losses from Cancer Mortality in 1954 and from Cases with Incidence in 1954
83
11.
Total Losses from Tuberculosis Mortality in 1954 and from Cases with Incidence in 1954
83
12.
Total Losses from Poliomyelitis Mortality in 1954 and from Cases with Incidence in 1954
84
K'3.
" T o t a l " Economic Losses from Deaths and New Cases in 1954 of Cancer, Tuberculosis, and Poliomyelitis
84
Mortality Losses, Morbidity Losses, and Treatment Costs as Percentages of Total Losses from Cancer, Tuberculosis, and Poliomyelitis, 1954 Cases and Deaths
85
14.
xiii
xiv
Economics of Public Health
Table Page 15. Awards by National Granting Agencies for Research in Tuberculosis, Cancer, and Poliomyelitis, 1946-1955, Government and Non-Government Sources of Awards 88 16'. Total Losses per Case of Cancer, Tuberculosis and Poliomyelitis, 1954 90 17.
Hypothetical Costs of Preventing a Case of Cancer, Tuberculosis, and Poliomyelitis, As a Function of the Number of Cases Prevented
92
18.
Marginal Consumption, by Age
103
19.
Average Income and Family Size, According to Age of Family Head
111
Charts Chart
Page
1.
Hypothetical Demand for Community Health Project
23
2.
Present Values of Net Future Earnings, by Age and S e x , at 10 and at 4 Per Cent Discount Rates, circa 1950
6'2
3.
Present Values of Net Future Earnings, Males, by Age, 1920 and 1950
6" 3
4.
Marginal Consumption, by Age
5.
Marginal Consumption for Persons with T h r e e thetical Life Cycles ( A s Described in T e x t )
6.
Value of W o m e n ' s Household Production, According to Number of Responsibility Units
116
Average Number of W o m e n ' s Household Responsibility Units, by Age of W o m a n
118
7.
XV
104 Hypo-
113
PART ONE
Introduction, and consideration of the proposition that "good health is good business" CHAPTER Ι
Introduction The sign on the door read: Department of Health Better Health is Purchasable
Better health is purchasable—at a price! There exist today medical and engineering knowledge and techniques for applying and expanding this knowledge which are capable of preventing much current sickness and premature death. " E v e r y year," we read, "325,000 people die whom we have the knowledge and skills to save," 1 And countless thousands of others are victims of preventable illness. W h y does society allow premature death and preventable illness to continue ? W h y does society not fight death and illness with all the knowledge and tools at its command ? W h y should even one person become a victim of preventable sickness or premature death ? T o many persons the answers to such questions are selfevident. W r i t e s one author, lamenting the continued existence 'Federal Security Agency, The Nation's Health—A Ten Tear Program, A Report to the President by Oscar R. Ewing, U. S. Government Printing Office, Washington, D. C., 1948, p. 1. Β
2
Economics
of Public
Health
of unnecessarily poor health, "everybody . . . should have all the medical care that science can give." 2 On a similar note, the preamble to the Constitution of the World Health Organization declares: 3 The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being. . . . Finally :* We have the knowledge and the necessary resources for the control of disease. Obviously, we must put our knowledge to work. The case is clear: (1) Better health is desirable. (2) The knowledge exists to improve health, ( s ) Therefore, health should be improved. Clearly, the crucial premise is that " b e t t e r health is desirable," for once this is accepted, and the fact that better health is obtainable is admitted, the conclusion, statement ( s ) , follows directly. But what does it mean to say that better health is "desirable" ? T h e list of things which are " d e s i r a b l e " to someone is certainly lengthy ! W h a t is relevant is not desirability in an absolute sense, but rather relative desirability. T o make meaningful the view that the health of our nation should be improved, as we have seen it can be, it must be argued that improvements in health are more desirable than improvements in the quality or increases in the quantity of at least some of the many other things which people consider desirable. W e must decide which goods and services to forego as well as which to consume. W e must economize. If consumers are to be sovereign and determine through the •Henry E. Sigerist, Medicini and Human Welfare, Yale University Press, N e w Haven, 1941, p. 139. •Neville M . Goodman, International Health Organizations and Their Work, Blakiston Company, Philadelphia, 1952, p. 1. 4 Ffrangcon Roberts, The Cost of Health, Turnstile Press, London, 1952, pp. 15-16.
Introduction
3
market the allocation of resources, and thereby the composition of total output, and if a social optimum composition of output is to be achieved, the following three conditions must hold, in order that the marginal conditions for production and consumption optima be fulfilled: (1) Individuals must be able to determine the variety and quantities of goods and services upon which to spend their money. (2) A means must exist to permit individuals to transmit these wants to those who can and will satisfy them. (3) The consumption and production of these goods and services must occasion no significant external economies or diseconomies.5 If any or all of these conditions are not met, people will not obtain the combination of goods and services which they actually prefer. That is, unless people can and do make rational decisions regarding their wants, unless there is a mechanism for seeing to it that consumer wants lead to production, and unless the well-being of third parties is left unaffected by the production and consumption of the commodities—unless all these hold, production by the free, private market will not reflect the wants of all consumers.® The first two conditions seem clear; the third condition simply refers to the fact that where external—third party—effects are involved, these affected persons will have no way to register through the market mechanism their preference for, or opposition to, the particular goods; consequently, the likes and dislikes of these people are left unconsidered. For most objects of consumption these conditions are rather closely met. It is relatively easy for one to decide whether or not he wishes to purchase a pair of shoes ; to transmit the demand for shoes one need only take his money to a shoe store; and any 'This is to say that other producers and consumers must be unaffected—either favorably (external economies) or unfavorably (external diseconomies)—by the production and consumption of the product or service. •Given the distribution of purchasing power.
4
Economics of Public
Health
external economies of consumption or production of the pair of shoes are surely inconsequential. However, the commodity, better health, satisfies any of these conditions only quite imperfectly if at all. First, it may not be very simple for a person to decide whether to purchase a reduction of χ per cent in the probability of contracting disease y (for when one buys better health he buys nothing more than a reduction of a probability). Second, while better health is purchasable, it clearly cannot be purchased at a " s t o r e , " as can a pair of shoes. 7 Transmitting one's demand for better health is, therefore, difficult. Third, the external economies of improvements in health are substantial indeed—for example, when communicable diseases and public health facilities such as water purification and sewerage treatment plants are involved. As a matter of fact, we may identify a health problem as a public health problem if it is amenable to solution only or more efficiently through group as opposed to individual action. Communicable disease prevention and sewerage facilities construction are clearly of this sort. 8 Although consumers may not find it easy to choose between a reduction in the probability of becoming ill or dying prematurely and a more tangible commodity, decisions based upon nothing more than probability information are often made. People do ' T o some extent "better health" is purchasable at a "store." One can buy a doctor's services, and such health aids as vitamins and sun lamps. Nevertheless, the causes of poor health are frequently beyond the control of the individual, depending upon the state of health, and the activities, of others. * In general, preventable diseases fit the definition of public health problems; they are frequently communicable, or, like cancer, are so prevalent as to make group action, particularly in research, especially economical. (See Harry S. Mustard, An Introduction to Public Health, Macmillan Company, New York, 1935, pp. 11-12.) Public health programs involve both ( 1 ) altering the health environment, which includes providing new techniques for disease prevention and treatment, and ( 2 ) obtaining the necessary response from individuals to that environment. For example, improved sanitation facilities may not lead to improved public health unless individuals make proper use of the facilities. Thus, health education—bringing about the appropriate response to an improved environment—is itself sometimes an aspect of a public health project.
Introduction
5
decide to spend a part of their income on the promotion of their health, and they make other choices as well involving uncertain outcomes, as in gambling. The intangible, uncertain nature of "better health" does not, in itself, preclude people from adjusting their purchases of it optimally, as they tend to do in the case of other, more tangible objects of consumption. But once people decide how much health they wish to purchase an obstacle is reached. Since this commodity is, in general, not for sale in the manner of most goods and services which we consume, one cannot express his demand for the commodity through the market mechanism of dollar votes. The absence of market prices as guides in the determination of optimal output is at the root of the struggles between legislatures and health interests over the appropriation of health funds. If legislators could even approximate the social benefits of better health or the public's unexpressed demand for improvements in health, how much easier it would be to obtain agreement as to a desirable amount and distribution of expenditures. From an economic-efficiency viewpoint, decisions with respect to the allocation of funds to any and all public health projects should rest upon comparisons of the expected benefits of alternative programs, with their costs. The present study is limited to the consideration of benefits. Cost considerations, being logically separable, may be left for another investigation. Confining our attention to the benefits of better health, we shall analyze the means by which better health confers benefits upon society, and, where possible, make estimates of these benefits.* Indeed, such estimates must be made, for Public health administration is a business. As such it is subject to ordinary commercial laws, may be judged by commercial standards, •The distinction between benefits and costs is not always clear-cut. That which is a benefit from one point of view is a cost from another. For example, sanatorium treatment of tuberculosis patients is a cost of our present attempts to cope with the disease; yet, if we consider the desirability of research to find a tuberculosis vaccine, a major potential benefit would be the elimination of treatment costs.
6
Economics of Public Health
and compared with other lines of economic activity. . . . Cities, counties, states, and nations do not have unlimited funds for their various activities. Judged according to commercial standards the funds at their disposal should be applied where and in proportion as they will produce the greatest returns. . . ,10 T h e difficulties involved in ascertaining the economically desirable level and composition of health expenditures are great ; yet decisions must be made. The absence of an explicit decision is an implicit decision to spend nothing. Objective valuation of the economic benefits of better health, for comparison with the costs of securing it, would be of great aid to governments and to donors to private health organizations in making rational expenditure decisions. 11 10 Henry Bixby Hemenway, "Economics of Health Administration," American Journal of Public Health, 10 No. 2 (February 1920), 105, 106. 11 After this study was completed, Roland McKean's investigation of prospects for evaluating government activities appeared. (Efficiency in Government through Systems Analysis, with Emphasis on Water Resources Development, John Wiley, New York, 1958). Discussing the existence of "programs for which present values of tangible gains would be used as indicators of performance," he concludes with respect to health services: " T h e present value of outlays on preventive medicine, research, control of communicable disease, and training might be measured in terms of estimated savings of future costs for hospitalization and treatment plus the value of future manhours that would be saved" (p. 291). What McKean suggests is precisely what has been done in the present study.
C H A P T E R II
Is good health "good business"? Since, in a fully employed economy, a decision to produce certain things is, ipso facto, a decision not to produce something else, the success of the advocates of larger health expenditures in obtaining funds has been limited. In a number of instances, efforts have been made to demonstrate that the utilization of resources in the health area bestows large economic benefits upon society, the benefits presumably being substantial enough t o warrant the withdrawal of resources from other uses. In 1922 the Department of Health of the State of Connecticut estimated the annual loss from preventable disability, in an attempt to increase interest in health problems. T h e estimate included, in part, the following components: 1 Loss in income to individuals: One-fourth population are wage-earners = Average days lost yearly from preventable causes
350,000
= 4
Average wage = $2.50 350,000 χ 4 χ $2.50 =
$3,500,000
Loss to industry: It is accepted that the loss to industry in disorganization, idle overhead, and lessened production is 2 j times the wage loss 3 , 5 0 0 , 0 0 0 X 2£ =
8,750,000
As a measure of social losses, these figures are totally inadequate. W e are immediately struck with what appears to be evidence of double counting. If the loss to individuals is their M.S. Falk, The Principles of Vital Statistics, W. B. Saunders Company, Philadelphia, 1923, p. 126.
8
Economics of Public
Health
foregone earnings, then the loss to industry is its foregone earnings—i.e., its lost profits, and not the entire value of " lessened production." To include the latter is to count the lost wages twice, once from the standpoint of the recipient and again from that of the payer. Next we note the implicit identification of economic losses with reduced money payments. The real economic loss is the diminished production; the money-income loss is a measure of the real loss. But it is not a satisfactory measure. Reduced household production by females, due to disability, is an important loss; yet it is entirely overlooked in the Connecticut report because it does not involve a decrease of money income. "Tuberculosis: Why Not Get Rid of I t ? " is the question raised in another study. 2 Statistical evidence is offered, purporting to demonstrate the "good return" which would result were tuberculosis eradicated. It is estimated that tuberculosis cost the United States in 1943 about $174 million of combined public and private funds, which are broken down as follows: Care of the ill in sanatoriums and at home Control through finding cases, health education, rehabilitation . . . . . . Aid to families where wage earner had T.B. . Medical research . . . . . . Pensions to tuberculous veterans
$110,800,000 15,000,000 9,000,000 1,200,000 38,000,000 $174,000,000
Knowing how much T.B. costs, the study proceeds to estimate the cost of wiping it out. What needs to be done is to detect the cases, and then treat them. What would an all-out campaign for the detection and treatment of tuberculosis cases cost, and how would this compare with the current costs of $ 174 million per year? (The following cost estimates are from the tuberculosis study.) *Good Health Is Good Business, National Planning Association, Pamphlet No. 62, February 1948, pp. 4-13.
Is good health "good business"?
9 Annual Cost
Step O n e : X-ray everyone ( 1 ) T o examine by X ray everyone over 15 twice within a ten-year period (20,500,000 per y e a r ) at an estimated cost of 25 cents per film would cost annually . . . . ( 2 ) Additional X rays and test for those persons found with signs of tuberculosis . ( 3 ) " Follow-up w o r k ' ' and X rays for " contacts'' —those " w h o have been in close contact with those found to have tuberculosis " Step T w o : Care ( 1 ) Maintenance cost in sanitorium beds for one year for 133,000 tuberculosis patients, at $3.50 per day ( $1,300 per year) ( 2 ) Home treatment for patients after release from sanatorium (principally observation and check-ups); 133,000 patients at $10 per case .
$5,100,000 6,150,000
2,310,000
173,000,000
1,330,000
Step T h r e e : Tuberculosis Health Education " to help people understand the value of examinations and treatment, the need for continuous treatment until they recover, and the care needed to avoid infecting o t h e r s " . . . . . .
12,000,000
Step F o u r : Rehabilitation " . . . education and vocational guidance and training. . . . " . . . .
22,000,000
Step Five: Financial assistance to dependents to permit the tuberculosis victim to remain at rest the length of time required for complete recovery ($1,500 per family for the 38,460 families who need it; i.e., the 81 per cent of the tuberculous male heads of families in sanatoriums)
58,000,000
Step Six: Research "until science finds a chemical or antibiotic which can kill or definitely halt the growth of the tubercle bacillus"
$3,000,000
10
Economics of Public Health
Additional Cost: Pensions to tuberculosis veterans not a part of the campaign, but expected to continue during the campaign . . . . Total recurring expenditures during campaign
38,000,000 $320,890,000
Step Seven: Hospital construction Hospitals with 75,550 new tuberculosis beds and their equipment should be provided in addition to the 79,000 adequate beds now in existence. Costing some $377,750,000, and having a life of 50 years, of which only 10 would be spent in tuberculosis work, one-fifth of the cost of the hospitals should be charged to the 10-year tuberculosis campaign. Average annual cost of hospitals . Total Annual Cost of the Campaign
7,555,000s $328,445,000
It is estimated in the study that once the campaign has been completed about $37 million per year will be required for continued control. If the campaign is not undertaken a continuation of the 1943 level of expenditures of $174 million is forecast. Concludes the study: " $ 3 7 million—or $ 1 7 4 million?" Which shall it be ? But the choice is not quite this. Even assuming the validity of the analysis, what the study actually showed was the choice of $37 million [preceded by a period of some seven* years with annual costs of $328 million) or $174 million. And the correct choice between these alternatives is far less obvious. T o compare the costs of the two programs for the purpose of determining which is the cheaper, it is necessary to state costs in terms of present values. For the effect of introducing the " c r a s h " campaign to replace the then-current program would be to increase costs for 8 According to the "Good Health . . . " study, $67,995,000 should be charged to the tuberculosis program. This is evidently an arithmetic error, since it seems clear that one-fifth of the total cost of $377,750,000 was to be charged to the program— on an annual basis, one-fiftieth, or $7,555,000. * Some of the costs of the campaign last for ten years at constant amounts (hospital depreciation); some for only five (health education); and some for various durations at fluctuating amounts (hospital care). A rough average of seven years of peak expenditures has been assumed.
Is good health "good business" f
11
the early years ($328 million versus $174 million), while decreasing them for subsequent years ($37 million versus $174 million). Using the 10 per cent rate of discount, which we are assuming in Chapter VII to be the marginal productivity of capital (or using any greater rate), we find that the present value of the later-year savings is not sufficient to offset the extra early-year costs of the campaign. The present value of the cost stream of $328 million per year for seven years followed by $37 million per year thereafter, exceeds the present value of the continuous cost stream of $ 174 million per year. The economic case for the crash program falls. Moreover, there is the possibility that with the present rate of research efforts, some new, less expensive means may be developed for either curing or preventing tuberculosis. Research toward this end is being carried on continually; 5 its success would leave society with expanded and unneeded facilities for treating tuberculosis with costly, old techniques. Society would have spent a great deal more than was necessary in the fight against tuberculosis, since the costs of the eradication campaign are concentrated at the onset. The accelerated rate of development of "wonder drugs," vaccines, and the like in recent years has increased the likelihood that a large investment in facilities and personnel to cure tuberculosis cases by present methods of lengthy and costly periods of sanatorium care will prove to be unnecessary and uneconomical. As yet we have not questioned the accuracy of the cost estimates of the tuberculosis study, nor have we questioned the completeness or relevance of the particular kinds of costs which were considered. Both need to be done. 'For example, shortly after the study containing the program for tuberculosis eradication was considered, but even before it was published, a report of some successful results with a new vaccine appeared. (See C. W. Wells and E. W . Flahiff, "Results Obtained With Heat-Killed Tubercle Bacilli Administered in a General Population," American Journal of Hygient, Vol. 40, September 1944.)
12
Economics of Public
Health
The total cost of $5.1 million per year for X rays " i s based on a cost of 25 cents a film for each person X-rayed under the new mass X-ray techniques,"· Apparently, this figure represents the out-of-pocket (marginal) cost of X-raying a person, once the equipment and personnel are available. However, the large increase in the X-ray program proposed by the study would require additional equipment and workers; the marginal cost of X-raying would become the average total cost of additional X-ray pictures, and would include a portion of the cost of securing the necessary extra machinery and labor as well as the cost of the film and its processing. If the 25-cent figure does represent only the out-of-pocket cost of the film, its processing and handling, it seriously understates the extra costs which would be incurred were the eradication campaign, with its 20.5 million X rays per year, to be undertaken. A more basic shortcoming of the cost estimates in the study is the implicit assumption that all facilities and personnel used in the detection, cure, and rehabilitation of tuberculosis cases can be expanded at substantially constant average costs. For example, although under the campaign the number of patients occupying sanatorium beds is expected to double, the cost of caring for each patient is assumed to be unchanged. This constancy is unlikely in a fully-employed economy. Nurses in tuberculosis hospitals, already in short supply, 7 cannot be expected to more than double in number within a couple of years at prevailing real wage rates. And the hospital construction required for the campaign, which would almost double the 79,000 beds then in existence, also could not be expected to be accomplished within a short time at constant cost. This raises the question of the speed with which the campaign •Good Health . . p. 7. 7 Doris E. Roberts, "The Positive Approach to a Tuberculosis Nursing Program," Public Health Reports, Vol. 68, No. 3 (March 1953).
Is good health "good business"?
IS
is to be initiated and, specifically, how fast additional hospital facilities are to be constructed. Since the peak demand for these facilities would occur within one year of the beginning of the campaign, the speed with which tuberculosis could be wiped out would be limited by the time required to construct the required facilities. There is little point to detecting cases if they cannot be treated. A dilemma is confronted. On one hand, the faster the hospital facilities are constructed the sooner the case-finding and treatment can be started; but, at the same time, the greater will be the costs of construction. On the other hand, the more slowly the hospital facilities are constructed the longer the campaign must be postponed, but the lower will be the costs of construction. In the period 1 9 4 8 - 1 9 5 3 an average of approximately 4 , 5 0 0 tuberculosis hospital beds were constructed annually. 8 At this rate it would take seventeen years to ready the additional 7 5 , 0 0 0 beds needed before the case-finding could begin. One last reference to the conceptual accuracy of the cost estimates concerns the proposed allocation to the campaign of onefifth of the $ 3 7 7 , 7 5 0 , 0 0 0 cost of building and equipping the new tuberculosis hospitals. This is explained by the fact that only ten years of the fifty-year life of the facilities would be spent in tuberculosis work, at which time ". . . these facilities could be turned over for other uses." 9 It should scarcely be necessary to point out that the length of physical life of an asset is irrelevant for purposes of determining the proper amount of depreciation to be charged. W h a t is relevant is the economic life of the asset in a particular use, and the remaining usefulness (net revenue stream) of the asset when its economic life in that use is ended. T h e economic life of the tuberculosis hospital facilities is assumed to be ten years of use as tuberculosis facilities. 8 Computed from data in Public Health Reports, 68, No. 4 (April 1953), 427. »Good Health . . p. 12.
14
Economics of Public Health
Although the facilities can then be used for forty additional years for persons with other chronic diseases, it is not proper to charge only one-fifth of the total cost of the hospitals to the proposed campaign unless the value of the facilities in the other uses is as great per year as their value in tuberculosis work. That the facilities will not stand idle at the end of ten years means that they will have a value in excess of scrap, but it does not necessarily mean that four-fifths of their original usefulness (net revenue stream) remains. The fact that it is a campaign against tuberculosis rather than some other disease suggests that the hospitals would be less useful—that is, would provide a smaller annual net revenue stream—-in a non-tuberculosis use. 10 Thus, the appropriateness of the $7,555,000 per year actually estimated as a cost of the eradication program (in step seven of the foregoing cost estimates from the tuberculosis study) is questionable. The costs of tuberculosis to society include all losses sustained as a consequence of the disease, whether or not there were expenditures associated with the losses. And just as there may be social losses without expenditures, so there may be expenditures without social costs. Of the total cost of tuberculosis to the United States in 1943, some $47 million were in the form of aid to the families of tuberculosis patients and pensions to 10 In this discussion, the allocation of depreciation charges between the ten years of the tuberculosis program and the following forty years has been on the basis of the proportionate distribution over time of the total net revenue stream of the hospitals. In other words, depreciation was assumed to be charged on the basis of the proportion of the total expected net revenue stream which was realized in any given year. This seemed to be the implicit assumption behind the use of " straight line" depreciation by the authors of the " G o o d Health . . ." study. If, however, depreciation is used to reflect the decrease over time of the present value of the net future revenue stream of the asset, quite different conclusions would follow. Thus, with a constant revenue stream, for example, the present value of the asset (hospitals) would decrease by less than one-fifth during the first onefifth of the life of the asset; the greater the discount rate, the smaller being the decrease. While the question of what is the " p r o p e r " amount of depreciation to charge for any particular period is presently a controversial one, we shall not enter into the debate in this study.
Is good health "good business"t
15
tuberculous veterans. 11 These expenditures do not represent real economic cost to "society," unless " s o c i e t y " is defined to e x clude the sick and their dependents; for while the expenditures are private costs to the transferers, they are private benefits to the transferees. 12 Furthermore, it would surely be a double counting of social losses to include the amounts of money given to the tuberculous and their families after having already included the medical expenses which the disease entailed. Good health may or may not be " g o o d business"; but the economics employed in arguing the case leaves much to be desired. 11 See page 8, above. A publication of the U. S. Department of Health, Education and Welfare also considers the total economic cost of a disease to include cash outlays "attributable to the disease." Thus, "compensation payments" are included in the attempt to arrive " . . . at the total cost of tuberculosis. . . ." Joseph N. Gitlin, "Tuberculosis Expenditures in Fiscal 1952," Public Health Reports, 69, No. 9 (September 1954), 797. 11 These " t r a n s f e r s " might be considered as a measure of the lost earnings which they replace. It should be emphasized, though, that it is the lost earnings which ought to be counted, not the transfers as such. The amount of transfers may be an estimate of this loss, but certainly a quite low one.
PART T W O
The economic nature of health activities—a theoretical analysis
Introduction Whenever production or consumption of a commodity involves significant external effects, we may expect its volume in the free market to be non-optimal. There are few commodities which have greater external effects than improved health. As a matter of fact, the external effects of the reduction of morbidity and mortality are so substantial in the cases of many potential health projects that the projects are not undertaken at all through the market mechanism—internal benefits being of minor significance as compared with external benefits. As a result, many health activities are in the hands of extra-market organizations—governments or private foundations. In Part T w o we shall examine the forms taken by substantial external economies of public health projects and some implications of their existence; and we shall consider how information on the demand for various health programs may possibly be obtained
CHAPTER
III
The nature of the commodity, better health T h e r e e x i s t s a special class of g o o d s which are characterized . . . by the fact that they cannot be divided up into units of which any single individual can be given exclusive possession. They are, in this sense, indivisible. Such goods have the characteristic that they become part of the environment—available to all individuals who live within that environment. 1 . . . each individual's consumption of such a good leads to no subtraction from any other individual's consumption of that good. . . , a In the case of such indivisible g o o d s a f u n d a m e n t a l p r o b l e m of finance arises. As an illustration, t a k e t h e case of an area b e i n g c o n s i d e r e d f o r s p r a y i n g t o c o m b a t flies and m o s q u i t o s . W e r e t h e a r e a s p r a y e d , e v e r y o n e in it would benefit f r o m the reduced n u m b e r of insects and t h e c o n s e q u e n t r e d u c t i o n in t h e p r o b ability of c o n t r a c t i n g d i s e a s e s c a r r i e d by t h e m . T h e s e benefits w o u l d be realized w h e t h e r o r n o t any p a r t i c u l a r p e r s o n paid his " s h a r e " of the s p r a y i n g cost or any p a r t of it. It is clear that in cases in which individuals stand t o benefit j u s t as much w h e t h e r they pay or n o t , v o l u n t a r y p a y m e n t s f o r the p u r c h a s e of such a c o m m o d i t y m a y be e x p e c t e d t o be small o r n o n e x i s t e n t . T h e c o m m o d i t y ( h e a l t h p r o g r a m ) m a y n o t be supplied because of the a p p a r e n t absence of a d e m a n d . Of c o u r s e , it is possible t h a t one p e r s o n m i g h t be w i l l i n g t o b e a r the e n t i r e cost, in which case t h e c o m m o d i t y w o u l d be supplied, the health p r o j e c t u n d e r t a k e n . H o w e v e r , it is r a r e , and in n o case is it logically n e c e s s a r y , that one individual receives sufficiently g r e a t ' H o w a r d R. Bowen, Toward Social Economy, Rinehart and Company, Inc., N e w York, 1948, p. 173. •Paul A. Samuelson, " T h e Pure T h e o r y of Public Expenditure", The Review of Economics and Statistics, 36, No. 4 ( N o v e m b e r 1 9 5 4 ) , 387. c
18
Economics of Public
Health
benefits from such a project to warrant his financing it alone. 3 It is this danger that projects promising benefits far in excess of costs may not be undertaken that properly concerns us as welfare economists. It suggests that with proper reorganization it would be possible to improve the economic-welfare position of some persons while worsening that of no one. W e have already referred to the substantiality of the external effects of improvement in health as an explanation of the extramarket origin of many health activities. Now we shall discuss the particular forms of these external effects. Improvement in the health of one person has an impact upon the state of health of each of the rest of us in varying degree, when communicable diseases are involved. Each person, then, has a financial stake in the preservation of the health of others. Many persons gain, in terms of diminished chance of becoming ill, when the health of one person is improved. But these external gains are generally not taken into account when people determine the part of their income to allocate to health. When deciding how to utilize his income, a utility-maximizer would equate the marginal utility of a dollar in all uses; but since he ordinarily would gain no utility from the fact that his health expenditures increased the level of utility of others (i.e., improved their health), he would spend less on his health than would be socially desirable. Social and private benefits diverge. If it is true that all persons would like to see each person spend more on his health than he would wish to spend, this should, in principle, still cause no great concern—no deviation from a social optimum situation, for all people should be willing ' H o w a r d Bowcn, however, is also concerned with the equity of allowing one individual to bear the entire cost; ". . . in view of the fact that many individuals will derive benefit from the project, it would be eminently more fair if the cost were to be borne by the entire group of beneficiaries." (Bowen, op. cit., p. 173.) This should not concern us as " n e w " welfare economists. If one individual finances the project himself, then presumably he expects to receive as much satisfaction from using his money in this manner as he would from using it otherwise.
The nature
of the commodity,
better health
19
to subsidize those people who influence their health, until the optimum level of health expenditures is reached. In other words, if people are spending less than the socially desirable amount on health, they can be encouraged to increase their health expenditures with appropriate subsidies. Indeed, Professor Kemp concurs with Professor Reder in the view that subsidies will in fact be paid by those who stand to reap the external gains; and, as a result, ". . .unimpeded self-seeking will tend . . . to maximize welfare. . . ."* Will the subsidies be paid? If the answer is " y e s , " private and social optima will come to coincide. If the answer is " n o , " private expenditures on health will be less than the social optimum, and a prima facie case for concern over the economic adequacy of free-market-determined health expenditures will have been established. Of course, while this factor of external economies may lead to less-than-optimum health expenditures, the two factors—irrationality in decision making and lack of adequate information on costs and benefits—may result in either excessive or insufficient expenditures on health, either in the aggregate or on particular programs. What reason is there for thinking that the required interpersonal subsidies will be paid ? What is the mechanism of payment ? It would seem that there exist no satisfactory answers to these questions, at least with respect to the private, decentralized market mechanism. Hence the rationale for extramarket efforts to bring about the desired effects of subsidization —through government or private foundations. At the same time that one person's improved health bestows benefits upon others, the action which the person takes to improve his health (e.g., the facilities which he constructs, the spraying which he undertakes, etc.) may also have the effect of 4 M u r r a y C. K e m p , ' ' T h e Efficiency of Competition As an Allocator of Resources: II. External Economies of Consumption," Canadian Journal of Economics and Political Scienct, 21, No. 2 ( M a y 1955), 222n.
20
Economics of Public Health
improving the health of others. T h a t is, " o u t s i d e r s " may gain in t w o ways f r o m the decisions of others to improve their health: ( 1 ) t h r o u g h the effect of an improvement in one person's health on the health of others, and ( 2 ) t h r o u g h the effect of the actions which an individual or g r o u p takes to improve his or its own health, which has the simultaneous effect of improving the health of others. T h e f o r m e r is the consequence of the external effects discussed above; the latter is the consequence of the " i n d i v i s i b i l i t y " of health resources, referred to at the outset of this chapter. Using our earlier example, if an individual or g r o u p sprays an area in order to kill disease-carrying insects, non-members of the g r o u p will also gain because ( 1 ) the decreased incidence of communicable diseases a m o n g the members of the g r o u p doing the spraying will diminish the probability of non-members contracting the diseases from them, and ( 2 ) the reduction in the n u m b e r of disease-carrying insects will diminish the probability of non-members, as well as members, contracting the disease from the insects. T h e r e is a third way—different in character f r o m the first two, which involve benefits—by which " o u t s i d e r s " may gain when others decide to improve their health. T h e y may " g a i n " f r o m reduced costs of buying better health. As more people demand additional health facilities or activities, the average cost of providing them generally declines. It is, indeed, expensive for each of us to have his own water-filtration plant or medicalresearch p r o g r a m , but the cost p e r person of filtered water or research, when done on a large scale, is negligible. Health projects, with few if any exceptions, are supplied and operated under conditions of considerable economies of scale. Sewerage disposal, insect control, X - r a y detection of diseases are far more expensive on an individual than on a g r o u p basis. Once again, this time with respect to the cost of improving health, each person has an important economic interest in the behavior of others.
C H A P T E R IV
Determining the public's demand for health activities W e have seen that it is a feature of public health expenditures that benefits accruing to one person are in many cases benefits to others as well. Thus, any particular person finds that he will reap benefits from the combined expenditures of all others, while at the same time it is clear that the connection between (1) the size of his contribution to a health foundation or to any "indivisible" health program (e.g., mosquito spraying) and (2) the magnitude of the benefits he may receive from it, is, to say the least, remote. In such cases there is scarcely any economic rationale for contributing to such a program voluntarily. Small, sub-optimal contributions are the consequence whenever a person cannot prevent easily the fruits of his efforts from being enjoyed by others. 1 Without doubt, many persons fail to contribute anything to voluntary health organizations even though they do care about their success; 2 and it is probably safe to say that many who do contribute do so in spite of, not because of, economic considerations. A neighbor's request for a donation to a " worthy " cause can exert important social pressure, just as the solicitation of a "voluntary contribution" by one's employer may temper one's narrow economic calculations. This much seems evident: the amount of contributions to any and all such voluntary organizations as the polio, heart, and cancer foundations bear no •In this connection see Kemp, "The Efficiency of Competition As an Allocator of Resources: II, External Economies of Consumption," Canadian Journal of Economics and Political Science, 21, No. 2 (May 1955), 32. •Just as many persons do not vote in political elections, even though they do care about the outcome of the election.
22
Economics of Public Health
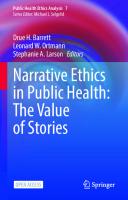
necessary relationship to an optimum allocation of resources based upon considerations of costs and anticipated social returns. Some method for harmonizing social with private benefits is needed to improve the allocation of resources in the health area. Government, with its tax-collecting powers, is a logical answer. The observed presence of government activity in the public health area is, therefore, quite expected. In principle, the authority (presumably government) which provides public health services should, first, question each person in the community or, more generally, each person suspected of having an interest in the proposed project {e.g., cancer research or swamp spraying), as to the quantity of the service which he would like to purchase at various prices per unit to him. 3 For a hypothetical three-person community we might obtain the following demand schedules: TABLE 1.
H Y P O T H E T I C A L DEMAND FOR COMMUNITY H E A L T H P R O J E C T
Price per Unit
%\
2 3 4 δ
Number of Units Demanded per Year by Person A
Β
C
3 3 3 1 0
4 2 1 1 0
5 3 2 0 0
Second, the individual demand curves would be added vertically so that the resulting curve would indicate the prices at which the community would demand various quantities of the •Or alternatively (but not equivalently), as Bowen put it, it would have to be determined what "amount of money he would be willing to give up in order to have successive additional quantities made available in the community." (Bowen, Toward Social Economy, Rinehart and Company, Inc., New York, p. 176. See also pp. 240-244.)
Determining the public's demand for health activities
23
4
service. This would be the community demand schedule (see Chart l ) . The reason for the vertical, rather than the usual C H A R T 1.
HYPOTHETICAL
DEMAND FOR COMMUNITY
HEALTH
PROJECT
0
I
2 3 4
5
Quantity per Year Source: Table 1. horizontal addition of individual demand curves to obtain a market demand is found in the social nature of the variety of ' T h e "community" consists of all beneficiaries.
24
Economics of Public Health
commodity under discussion; consumption by one person does not generally reduce the amount available to others. 6 In other words, with reference to the foregoing Table 1 and Chart 1, in order to satisfy all the demands of the members of the community at a price of, say, $3, no more than 3 units need be supplied. If the research, spraying, etc. is done for that period of time, the demand (at $3 per hour) of each and every individual will have been fulfilled; the same research or spraying satisfies all buyers. Third, the actual cost of supplying the commodity or service must be taken into account. The supply curve is drawn in Chart 1, under the assumption of constant costs, although the appearance of decreasing costs over a wide range is not unlikely. The fact that the supply curve (MC) does not intersect any of the individual demand curves illustrates a situation in which no one person acting in his own self-interest would find it profitable to finance the project, on even a small scale, himself. The procedure described above for obtaining the community demand for better health has two important shortcomings—one theoretical and the other pragmatic. In deriving a community demand function by vertically summing individual demand schedules, one implicitly assumes the absence of external economies •Paul Samuelson identified government expenditures with goods "which all enjoy in common in the sense that each individual's consumption of such a good leads to no subtractions from any other individual's consumption of that good. . . ." ("The.Pure Theory of Public Expenditure," The Review of Economics and Statistics, 36, No. 4 (November 1954), 387.) Julius Margolis was critical of this identification, claiming that "possibly the only goods which would seem to conform to Samuelson's definition are national defense and the aged light house illustration." (Julius Margolis, " A Comment on the Pure Theory of Public Expenditures," The Review of Economics and Statistics, 37, No. 4 (November 1955), 347-8.) Samuelson subsequently agreed with this criticism, but argued that almost all public expenditures possess some "trace of the defined public good. . . ." (Paul A. Samuelson, "Diagrammatic Exposition of a Theory of Public Expenditures," The Review of Economics and Statistics, 3, No. 4 (November 1955), 356.) Samuelson may have conceded a little too much. Public expenditures on preventive health and on medical research generally fulfill completely the requirement of his definition.
Determining the public's demand for health activities
25
of c o n s u m p t i o n , w h i c h w e h a v e a l r e a d y s e e n a r e o f t e n s u b s t a n tial in t h e h e a l t h a r e a . F o r m a n y h e a l t h p r o j e c t s an i n d i v i d u a l could a n s w e r t h e q u e s t i o n of h o w m u c h h e w o u l d like t o buy at v a r i o u s p r i c e s o n l y if h e h a d s o m e idea as t o w h o else w o u l d b e n e f i t f r o m the p r o j e c t . A n individual m a y d e m a n d a h e a l t h p r o j e c t n o t o n l y because of the direct b e n e f i t s w h i c h h e r e a l i z e s b u t b e c a u s e of its effects u p o n t h e h e a l t h of o t h e r s w h o , in t u r n , affect t h e s t a t e of his h e a l t h . T h e r e f o r e , t h e level of o u t p u t of h e a l t h s e r v i c e s d e t e r m i n e d by t h e i n t e r s e c t i o n of t h e c o m m u n i t y d e m a n d and m a r g i n a l - c o s t s c h e d u l e s will be less t h a n t h e social o p t i m u m unless each p e r s o n is a w a r e of t h e a d v a n t a g e t o h i m of i m p r o v e m e n t in t h e h e a l t h of t h e o t h e r c o m m u n i t y members. O n t h e p r a g m a t i c side, t h e p r o b l e m a r i s e s of o b t a i n i n g t h e t r u e i n d i v i d u a l d e m a n d c u r v e s ; i.e., of finding h o w m u c h p e o p l e r e a l l y d o w a n t of a social-health c o m m o d i t y o r service. T h e p r o b l e m is n o t m e r e l y o n e of e x p e n s e of g a t h e r i n g i n f o r m a t i o n but is a m o r e f u n d a m e n t a l o n e of g e t t i n g h o n e s t r e p l i e s t o q u e s t i o n s . E a c h p e r s o n r e a l i z e s t h a t h e will b e n e f i t f r o m t h e p r o j e c t if it is u n d e r t a k e n , i r r e s p e c t i v e of the size of his c o n t r i b u t i o n . As a r e s u l t , if h e h a s a n y r e a s o n t o believe t h a t t h e size of t h e c o n t r i b u t i o n r e q u i r e d of him will d e p e n d u p o n his s t a t e d v a l u a t i o n of t h e p r o j e c t , he will find it t o his a d v a n t a g e t o g i v e " f a l s e s i g n a l s " — f a l s e , u n d e r s t a t e d indications of t h e v a l u e t o h i m of t h e p r o s pective project.8 Since an h o n e s t , h i g h v a l u a t i o n m a y r e s u l t in g r e a t e r d e m a n d s u p o n o n e s e l f , w h a t has h e t o g a i n by such c a n d o r ? V i r t u a l l y n o t h i n g , f o r t h e p r o b a b i l i t y is v e r y small t h a t a l o w v a l u a t i o n by h i m , of t h e m a n y o b t a i n e d , will affect t h e g r o u p ' s decision on t h e ' A s Samuelson put it, ". . . it is in the selfish interest of each person to g i v e false signals, to pretend to have less interest in a given collective consumption activity than he really has, etc." (Samuelson, " T h e Pure Theory of Public Expenditures," The Review of Economics and Statistics, 36, No. 4 ( N o v e m b e r , 1954), 3 8 8 - 8 9 . ) T h i s is correct provided that a person has some reason to believe that the benefit principle of taxation may be employed. T h i s qualification is not made by Samuelson.
26
Economics of Public
Health
desirability of the project, and thus he may receive the same benefits at a lower cost to himself. A voting procedure is being employed, and the analogy to the relative unimportance of any one vote in a major political election is valid. 7 Such individual action may, of course, lead to unfavorable collective results— the failure of the project to be executed or the election of a minority candidate—but this cannot be attributed to the action of any single person. It is clear that The mode of conduct which is most likely to promote the welfare of the individual when he is acting in concert with others may not be the course of action most conducive to the welfare of that person when he is acting individualistically.8 Thus, it is here argued that the same rational individuals who had failed to make a voluntary contribution could with complete consistency vote in favor of an increase in taxation for the same purpose which would take from each citizen exactly the amount he had just refused to contribute voluntarily.' By voting for the tax he may be sure that others will also " c o n t r i b u t e " and thus may be more sure that the project will be undertaken, although there is a cost to this certainty—the contribution required of him. If the amount of the tax is n o greater than the value to him of the collective good obtained, it will pay for each individual to seek a device for forcing all beneficiaries (including himself) to contribute. Since the collective goods we have been discussing are n o t likely to be supplied by the free market, . . . the absence of coercion may be construed to result in a vitiation of consumer sovereignty, since the individual consumer is by himself in no position to obtain the object he desires.10 ' T h e greater the number of valuations, the smaller the importance of any one. •William J. Baumol, Welfare Economics and the Theory of the State, Harvard University Press, Cambridge, Massachusetts, 1952, p. 15. * Ibid., p. 16. 10 Ibid., p. 93.
Determining the public's demand for health activities
27
Any voluntary, non-coercive system is likely to break down ( o r , at best, be inadequately supported), for as long as others are behaving in a socially optimum manner any one person may be able to improve his position by behaving in & privately optimum manner. For example, to the extent that smallpox vaccination in an area is universal, any individual may be able to gain by avoiding the time and expense of being vaccinated himself. T h i s is so because the major part of one's protection against smallpox is the result of the vaccination of others. Perhaps partly because of the fear of such individualistic behavior, society has seen fit in many areas to require smallpox vaccination by law; and, in fact, has gone further to enforce or encourage compliance by giving the vaccine " f r e e " — t h a t is, at zero marginal cost to the person being vaccinated. In summary, our investigation of the nature of the collectivegood, better health, has led to the following conclusions: 1. Insofar as consumers are utility-maximizers, private e x penditures for the improvement of health are likely to be suboptimal. 2. Public attempts to provide these goods and services confront great problems in discovering the desires of the public.
PART THREE
The economic losses from poor health— their form and measurability
Introduction
In Chapter IV we noted the great difficulty, if not the practical impossibility, of determining the extent of the public's demand for improvements in health. How, then, should governments— or private voluntary organizations, for that matter—determine how much to spend on health, in general, and on which particular projects ? It is suggested here that information on the economic benefits expected from various health projects would serve as a useful, meaningful guide to demand, and, hence, to expenditure decisions. In Part Three we shall discuss the ways by which poor or good health brings about economic losses or benefits; and, where practicable, we shall evaluate these losses in money terms for the cases of three specific diseases. W e hope to show how, given even the limited data available, some of the most important economic losses due to a disease can be measured, and how these data can be useful in making a priority listing of health projects according to anticipated economic benefits. Such a listing can serve as a guide to the allocation of health funds among competing programs. It is not held out as a basis for determining the optimum level of aggregate health expenditures. This is the case because our calculations are limited to monetary considerations, and, in fact, to less than all of these.
The economic losses from poor health—their form and measurability T h i s limitation t o m o n e t a r y considerations
29
m a y be n o t e -
w o r t h y , for the n o n - m o n e t a r y , psychological-sentimental c o s t s o f sickness and death m a y be far m o r e i m p o r t a n t . 1 T h e policy implications o f o u r restriction t o m o n e t a r y losses and benefits are considered in C h a p t e r V I I I . ' O u r distinction between " m o n e t a r y " and " n o n - m o n e t a r y " costs does not imply a categorization of costs at the conceptual level. It is meant to suggest that certain costs of ( o r losses from) poor health seem to be amenable to measurement at the present time, though perhaps only at considerable expense; while the measurement of other costs (eg·, the psychological effects of sickness and death), while possible in principle, must await further developments at the theoretical level.
CHAPTER V
The monetary costs to society of poor health—a taxonomy The monetary losses which society sustains as a result of poor health take a number of forms. The significance of each form varies with the particular disease and with the nature of the economy under consideration. 1. One obvious source of economic loss attributable to poor health is premature death, with consequent loss of production. For, assuming full employment, a premature death means the loss of a present or future producer. 1 2. A second economic consequence of disease is sickness, with the loss of production (partial or complete inability to work) which it may occasion. 3. The fact that a person has survived after a case of some disease does not necessarily mean that the total economic costs associated with the disease have already been realized. The illness may have reduced the individual's resistance to other causes of disability, his future productivity, or both. 4. Temporary absence from work resulting from illness may necessitate certain adjustments of the production process which make the total cost of sickness greater than the cost to the individual worker. In an economy of widespread specialization and division of labor, the absence of one key worker may drastically reduce the productivity of others. 5. Poor health affects the size and composition (with respect to age, sex, geographic distribution, etc.) of the population 1 W e are treating public health expenditures as a problem of resource allocation; thus, we assume the existence of full employment, or, more precisely, as seen in our subsequent computations, the employment of 95 per cent of the labor force.
The monetary costs to society of poor health—a taxonomy
31
through effects on mortality. Economic effects of a disease which affects children may differ substantially from those of a disease which primarily affects persons of middle and old age. Such matters as the effect on per capita income of variation of the ratio of workers to total population and of change in the size of the labor force are relevant. In addition to the five forms of poor-health costs already enumerated—that is, in addition to those which are, in the short tun, inevitable forms of costs—are certain costs which society may choose to incur in an attempt to reduce the magnitude of the "inevitable" forms.2 Thus: 6. A disease may entail economic costs of detection, treatment, and rehabilitation of patients. 7. The existence of diseases may involve people in costly attempts to avoid the diseases. Thus, the additional cost of filter-tip cigarettes is an "avoidance" cost attributable to lung cancer, since it seems evident that the recent trend toward the use of these cigarettes represents an attempt—however misguided—to avoid the disease. Even though ineffective in coping with the problem, such attempts represent a use of resources which would not occur except for the health hazard. Avoidance costs are discussed further in Chapter VI. Consideration of some specific diseases will disclose that their effects differ greatly. The common cold involves rather small treatment costs per case but a substantial aggregate amount of short term absenteeism and reduced efficiency on the job. Acute poliomyelitis results in death in a small percentage of cases, in permanent loss of productive capacity in others; while the costs of treating and rehabilitating an average case are quite great. At the same time, its age incidence is such that little absenteeism is attributable to it. Cancer results in a high rate and high 1
It should be clear that in this discussion the word " c o s t " always refers to a loss or sacrifice resulting from some disease; it is the reduction or elimination of these costs which constitutes the "benefits" of better health.
32
Economics of Public
Health
absolute number of deaths, and has considerable incidence among adults of productive age in certain nations. Malaria has a generally small incidence of deaths, but reduces the productivity of its victims substantially, results in a great deal of absenteeism, and often involves large avoidance costs in areas where it is found. In general, the economic losses due to any particular disease will depend upon: a. Present and future earnings {i.e., productivity) of its victims; b. Its age and sex death incidence; c. Its age and sex case incidence; d. The average duration and severity of its temporarily disabling and efficiency-reducing effects; e. The extent to which it leaves (e x ) permanent disability or (e 2 ) increased probability of morbidity or mortality from other causes; f. The production problems created by its effect on absenteeism; g. The substantiality of the effect of the disease on the size, composition, and distribution of the population; and the influence of these effects on per capita income; h. The extent of attempts made to find and treat its victims; i. The extent of attempts to avoid it. In the absence of information on present, not to mention future, earnings of the victims of each particular disease, the quantification of the economic losses from any disease may be seen to require data on average earnings by age and sex, item a ; and, in addition, information regarding items b through i for the particular disease and geographic area under consideration. The availability of the needed data for the United States is discussed in the following pages.
CHAPTER VI
Methods of and prospects for quantification To what extent can we determine quantitatively the monetary loss resulting from any given source of poor health ? We now consider this question with respect to each of the loss categories discussed in the previous chapter. PREMATURE
DEATH
The loss of a life involves the loss of an actual or potential productive unit.1 Assuming that earnings (wages, salaries, and income from owner-operated business) are a reasonably adequate measure of the value of the marginal product of a worker,2 we may proceed to determine the economic value of a producer at any given age as follows: first, estimate the future income he would have earned had he not died. While it is not possible to know with certainty how much each person who dies prematurely would have earned, a meaningful statistical average of earnings can be useful.3 Information on median earnings of employed persons, according to age and sex, has been obtained from the 1952 Current Population Survey, and is shown in •And a consuming unit, as well. See our discussion on this point below. •Such is clearly not the case for housewives. The estimation of their production is described in Appendix II. •To assume that the social loss of death is (at least partly) the loss of earnings is to imply that a death results in a net population decrease of one; that is, that a death has no effect on the mortality rate among others nor on the birth rate. In such a case the loss of one person would result in the loss of that which he would have produced (in money terms, his earnings), for other things would have remained constant. However, there may be reason to doubt the independence of mortality, on the one hand, and the survival rate among others and the natality rate, on the other hand, in a country such as India, with an extremely high mortality rate and a very low living standard. If a death leads to an additional birth or to the survival of one who would otherwise die the net loss of production as a result of the death will certainly be different (smaller, if the marginal product of labor is greater than zero) from what it would have been if the death had no such effect. D
34
Economics of Public
Health
Table 2 (column 2 for males, 12 for females). 8 With such data we can estimate what an average worker would have earned had he not died prematurely. 4 Since our average earnings data apply to males with earnings, each earnings figure must be adjusted for the percentage of persons at each age who actually have earnings. This may be done by obtaining data on the proportion of males at each age who are in the labor force and by multiplying the average earnings of employed persons by 95 per cent of this factor, to reflect our definition of "full employment" as the employment of 95 per cent of the labor force. Next, these adjusted earnings by age must take into account the probability of a person actually living to each age to realize the earnings. Death eliminates all future production by the victim, but we must account for the fact that even if a person does not die at a given age, he faces the continued possibility of death at each subsequent age. 8 Thus we must multiply the adjusted average earnings for each age by the probability of a ' T h e r e is, perhaps, a cogent defense for the use of a median rather than a mean earnings profile. It has been pointed out that disease incidence is sometimes a function of race, as is expected earnings; that is, incidence of some diseases is higher among Negroes, whose expected income is lower than the average. Insofar as this is the case, earnings actually lost per case of a disease would be less than the mean earnings for the entire population at that age. Consequently, using median earnings, which are less than the mean, would probably give a less biased estimate. At the same time, some diseases may have greater incidence among the higherthan-average earnings group. In these cases, even the mean earnings would be too low an estimate of lost earnings, while the median would be still lower. Since mean earnings profiles were not available, we had little choice but to use medians. T o the extent that any bias exists in our estimates of earnings lost, it is likely, therefore, that it is on the side of understatement. 4 T h e use of cross-section data {i.e., data for a particular year) here and elsewhere in this study fails to account for possible change of the variables—for example, change in individual productivity and earnings. T h e difficulty of making meaningful predictions of the future magnitudes of the variables explains our implicit, conservative assumption of no change. W i t h modern electronic computers it is easy to re-perform computations under alternative data assumptions. * When we try to estimate the benefits of eliminating a disease—say, cancer— our calculations should, properly, include the survival probabilities of the population in which cancer is absent. These would consist of (a) current survival probabilities, as ( b ) increased by the elimination of cancer, but as (c) decreased by
Methods of and prospects for quantification
35
person of specified age living to that future age. The survivalprobability data is readily available from life insurance and Census Bureau sources and is published annually in the Statistical Abstract of the United States. In addition to involving the loss of a producer, a death also involves the loss of a consumer. Therefore, perhaps we should consider the economic value of a person to be measured by the value of his future earnings, net of consumption. The estimation of an individual's consumption involves conceptual as well as practical difficulties. T h e procedure actually employed is described in detail in Appendix I. Finally, after deducting consumption from gross earnings, the resulting net future income streams must be discounted back to the present, and summed.® This will give us data on the present value of net future earnings, by age and sex. This is the value of a person as a net producer; it is the net value lost in the event of his death. 7 any increased incidence of other diseases among those saved from cancer. Thus, to determine the benefits of the elimination of each disease, a different set of survival probabilities would be needed. However, in our computations we have not used separate survival-probability information for each disease since we do not know how age-specific death rates from other causes would change if some cause of death were eliminated. (It should be noted that this is not equivalent to knowing, as we do, the mortality experience of persons with a history of some disease.) Consider the following hypotheses: a. In the past, those persons who have contracted but did not die from the disease under consideration, X, were left in a weakened state, more susceptible to death from other causes. If this were the case, the elimination of X would reduce death rates from other causes, at least within some age interval. b. In the past, those persons who have died from X were among the "weaker" members of the population (as they were if Darwin was right and the '' fittest " d o survive); if this were the case, and if disease X were eliminated, there would occur an increase in age-specific death rates from other causes. Having no real foundation for recomputing the life tables, we have used a single current table in the calculations for all three diseases. Of course, this procedure has the incidental advantage of simplifying computation problems. •A precise mathematical formulation of the theories expressed in words, the present value of net future earnings, is presented and utilized in Chapter VII. ' W e might also consider the concept of the gross value of a producer; i.e., the present value of his future earnings, no account being taken of his consumption. The choice between the two measures of the economic value of a person—present
36
Economics of Public Health
These computations would enable us to determine the cost of the deaths from any disease (or other causes) by simply multiplying the appropriate present values by the number of deaths which the disease causes. This may be done provided that mortality data are reported by age and sex, as they are reported by the National Office of Vital Statistics, for a sizable number of causes of death. When considering the economic value of a person it would be very helpful if we could utilize existing market values, rather than resorting to the sort of computations described above; for example, it would seem that life insurance puchases could be useful as measuring rods of the value of a life. There are, however, a number of reasons why the amount of life insurance on an individual's life is an unsatisfactory indicator of his value to society. First, the rationale for purchasing life insurance is that value of g r o s s or net f u t u r e e a r n i n g s — r e s t s upon t h e viewpoint taken. W h i l e we a r e concerned in t h i s s t u d y with the economic value of a person t o society, we have failed t o define " s o c i e t y " precisely. If " s o c i e t y " is defined to include everyone, including t h e individual w h o s e value is being considered, then his contribution t o t h e g r o u p is t h e total value of his o u t p u t , and his " v a l u e " is the present value of his gross f u t u r e e a r n i n g s . But if " s o c i e t y " is so defined as t o exclude the individual whose life is b e i n g valued ( f o r e x a m p l e , as all those who would be left w e r e he t o d i e ) , t h e n his c o n t r i b u t i o n to " s o c i e t y " consists only of any excess of what h e adds t o total o u t p u t o v e r what he subtracts f r o m it, his c o n s u m p t i o n ; and his economic w o r t h is the p r e s e n t value of his nit f u t u r e earnings. Actually, o t h e r definitions of " s o c i e t y " are also possible. In the " G o o d Health . . . " study, discussed in C h a p t e r II, a " s o c i e t y " is implicitly defined in a way which excludes e v e n t h e d e p e n d e n t s of the victims of disease. Only under such a definition are c o m p e n s a t i o n p a y m e n t s social costs of disease, as they are alleged t o be in t h e " G o o d H e a l t h . . . " and other studies. U n d e r this definition, the value of a p e r s o n would be t h e p r e s e n t value of the difference betw een his f u t u r e earnings and t h e c o n s u m p t i o n e x p e n d i t u r e s of all m e m b e r s of his family who are dependent uj>on him. U n d e r e i t h e r of the n a r r o w definitions of " s o c i e t y , " in which the individual whose life is being valued is excluded, and p e r h a p s his d e p e n d e n t s also, the value of m a n y p e r s o n s is n e g a t i v e . T h i s is to say t h a t people such as those retired have no e a r n e d income and no e x p e c t e d future earnings, yet they do continue to consume. T h e y are an economic liability, r a t h e r than an asset, to " s o c i e t y . " O n the o t h e r hand, u n d e r the broad definition, which includes in " s o c i e t y " t h e p e r s o n w h o s e life is b e i n g valued, no one can be an economic liability. At w o r s t , one may be c o n t r i b u t i n g n o t h i n g to the sum total of wealth.
Methods of and prospects for quantification
37
other people, generally one's family, are directly dependent upon his earnings for their livelihood. Hence, a person without such dependents has no motive for carrying life insurance, regardless of his earning capacity and his contribution to society. (Actually, society is his dependent, having an interest in the life of each person whose production exceeds his consumption. No market mechanism exists, though, for permitting the members of society to pool their insurable interests in order to purchase life insurance on the lives of such persons. Public health expenditures are a possible alternative.) Second, the amount of insurance carried on the life of a housewife is virtually certain to be far less than the present value of her expected economic contribution to her family. One reason for this is that housewives' services are not purchased on the open market. Thus, a husband may not realize the additional expense he would have to incur to replace her services were she to die. Moreover, insurance companies have not seemed to exploit fully a woman's insurable interest to her family. Third, ignorance and irrationality with respect to life insurance purchases are quite common. It is still true today that some persons " d o n ' t believe i n " life insurance and do not buy it, their economic value to their dependents notwithstanding. On the other hand, insurance salesmen have been known to induce buyers of life insurance to purchase more than wisdom would dictate. And, insofar as life insurance is purchased not as pure insurance but as a form of forced saving, the amounts of life insurance in effect do not necessarily reflect the insured's future net earnings. Fourth, even fully informed people, if they have a preference for risk, do not insure at " f a i r " odds, and certainly not at the unfair odds ( " u n f a i r " because of the " l o a d i n g " of the insurance premium for operating expenses) offered by insurance policies. T h e i r failure to insure does not indicate that they value their lives at zero (though this may be the amount of life insurance
38
Economics of Public
Health
owned), but rather that, given their Neumann-Morgenstem utility functions and given the price of life insurance, the insurance is too expensive. In general, of course, any person's failure to purchase something does not imply that its value to him is zero or less. Finally, whereas the value of a producer is a function of his future earnings, his ability to pay insurance premiums is, in part, a function of present and past earnings. A medical student having no current income is not in a favorable position for buying insurance, in spite of his great present value. T o some extent, modern deferred-premium life insurance contracts have reduced the significance of this obstacle to insuring. However, considering all the factors discussed above, the shortcomings of life insurance purchases as indicators of the economic value of a person are substantial. SICKNESS ( T E M P O R A R Y
DISABILITY)
Disease may prevent a person from working, and thereby lead to a loss of production. If we knew for a given disease or other source of sickness ( l ) the average duration of temporary disability it causes, (2) the age- and sex-incidence of its cases, and ( s ) the average earnings of its victims, by age and sex, we could determine the amount of earnings lost during the period of sickness from the particular cause. Thus, if a male, age 32, falls victim to a disease which results in a mean period of disability from work of four weeks, the loss of his production will be 4/52 of the average annual earnings of males, age 32. 8 " N o t all the production lost due to illness is necessarily a consequence of absenteeism or complete inability to work; there may be reduced efficiency of persons who continue to appear at work. This is probably a principal form of the economic efTects of the common cold, for example. Also, for a disease which develops gradually (e.g., tuberculosis), the reduced-productivity loss may be noteworthy. For diseases which develop rapidly (e.g., poliomyelitis), absence from work is immediate and productivity loss complete. Recognizing the relevance of reduced efficiency as a form of economic loss from disease, we shall, nevertheless, make no attempt to estimate its magnitude. N o meaningful basis for estimation appears to exist.
Methods of and prospects for quantification
39
We have already referred to the availability of data on earnings by age and sex. Although the incidence according to age and sex of deaths from many causes is known, accurate data on the total number of cases of a disease, with an age and sex breakdown, are much less available. They are available on a rather accurate basis for certain "reportable" diseases, which include some, though not all, contagious diseases but exclude important non-contagious diseases such as cancer and heart diseases. Data on the duration of incapacitation by disease are not generally available in published form, but hospital and insurance company records can be helpful, as can the estimates of medical personnel having professional experience with the particular disease. It may frequently be necessary to settle for rough estimates of duration of temporary disability from work, until better data become available. PERMANENT DISABILITY AND INCREASED TO OTHER ILLNESSES
SUSCEPTIBILITY
To the extent that a disease results in any permanent disability, part of the value of the victim as a producer is destroyed. Finding the magnitude of the destruction requires determining the extent to which future earnings will have been reduced. For many diseases, permanently disabling effects are in general apparently absent. Measles, chicken pox, and the common cold may be cited as examples. At the opposite extreme, some victims of certain diseases, such as poliomyelitis, tuberculosis, and heart diseases may be permanently and, in some cases, totally disabled. A case of a disease which leaves the victim 100 per cent permanently disabled (that is, unable to do any work) would involve a loss of the present value of all his future earnings; a 50 per cent disability, a loss of the present value of 50 per cent of gross future earnings, etc.® It is necessary to have, for each disease the losses from which are being investigated, an estimate of the 'Assuming that a 50 per cent disability leads to a reduction of earnings at each future age by 50 per cent. This, of course, may be altered by rehabilitation efforts.
40
Economics of Public Health
percentage of total cases which leave some degree of permanent disability, as well as some measure of the extent of disability, in terms of reduced earning capacity. At present, estimates in which we can place much faith are unobtainable, particularly regarding the " e x t e n t " of disability in terms of reduced earnings. If the victim of a disease, X, survives but is left in a weakened condition, so that the probability that he will contract some other illness is increased, then any additional losses from these other causes should be " c h a r g e d " to disease X. The data which are needed are ratios of (1) the conditional probability of contracting disease Y for persons who have had disease X to (2) the probability of contracting Y for persons who have not had X ; also ratios for mortality from Y for persons who have had X to mortality from Y for persons who have not had X. It has not been possible to locate such data. The Impairment Study, 1951, of the Society of Actuaries, which describes the results of a study by life insurance companies of the effect on mortality of having a history of a number of diseases, approaches the kind of information needed. But even these excellent data are not quite what we want. People who have had tuberculosis may have a mortality rate twice that of the general population, but much of the excess mortality will be directly from tuberculosis. W h a t we want to know is: how does the mortality experience among persons who have had, but not died from, say tuberculosis, compare with the mortality experience of persons identical in all relevant aspects except that they have not had the disease ? A simple comparison of observed mortality rates for the extuberculous with that for the general population is unsatisfactory. Tuberculosis survivors might well show lower mortality rates; they will, if only the strongest of the disease victims survive. ABSENTEEISM
Absenteeism is a costly industrial problem. And illness is unquestionably the greatest single cause of absenteeism—accor-
Methods of and prospects for quantification
41
ding to one labor-relations executive of a large Chicago manufacturing concern amounting to two-thirds of all their absences. This is consistent with figures supplied this writer by a national grocery chain, which indicate that almost 80 per cent of their total work-time lost is due to illness or injury. Evidence indicates that a firm's difficulty in adjusting to a given total level of absenteeism is inversely related to the average length of absences and is directly related to the degree of variation of absences. Uncertainty regarding the daily volume of absences creates for many firms the necessity of employing extra " s t a n d - b y " workers who will not be needed on days when the rate of absenteeism is low. One long-term absence of, say, sixty days is considerably less costly to a typical firm than are thirty two-day absences. First, once it has begun the long-term absence is rather highly predictable as to duration. Second, it is generally simpler to find a replacement for one person that it is for a number of different persons with various jobs and skills. T h i r d , since absences are frequently not discovered by the firm until the worker has failed to arrive, there is usually time lost in finding a suitable replacement. T h e extent of this lost time is a function of the number of absences, not of their duration. Therefore, the diseases which have the greatest adverse effects on output through their effects on absenteeism are those which, ceteris paribus, ( 1 ) cause short- rather than long-term absences; and ( 2 ) have highly fluctuating incidence rates over time. T h i s much seems clear; but the precise functional relationship between duration and stability, on the one hand, and production losses, on the other, is certainly clouded, as is the significance to a firm of the absolute level of absenteeism. 1 0 10 The more industrialized the economy, the more would absenteeism appear to be a problem. Resource combinations in the agricultural sector will generally be more flexible. Thus, the seriousness of production losses associated with a given volume of absenteeism would seem to be correlated positively with the level of industrial development of the economy.
42
Economics of Public POPULATION
Health
EFFECTS
Each disease has its own peculiar incidence pattern. Some diseases attack children predominantly, others adults. Some strike whites with greater relative frequency than Negroes; some have a greater incidence in one part of the country than in others. Some take a greater toll among women than among men. Some have a greater ratio of deaths to cases than others. In short, diseases have differing impacts upon the (1) size, (2) age, sex, and racial composition, and ( 3 ) locational pattern of the population. Are there, at any moment of time, economic optimum values of these variables ? Are there optimum rates of change of the variables over time ( " o p t i m u m " being defined in terms of output per capita, or some other useful criterion) ? If the answer to any of these questions is " y e s , " to what extent does mortality from a particular disease take us further from or closer to the optimum ? The study of "optimum population" would take us into a very broad area requiring much additional scrutiny; and we shall not venture into it in this study. While the population effects of poor health are undoubtedly quite substantial in a country such as India, in the United States the effect on population, size, etc. of mortality from any one disease is surely minor. The great mass killers in the United States—typhoid fever, diphtheria, smallpox—are diseases of the past. W e assume that the effect on United States population and on per-capita income would be negligible from a reduction in mortality such as would occur if some small number of diseases were eliminated as causes of death. At the same time, the distribution of income might be altered if reductions in mortality were unevenly divided among geographic regions. In the United States, for example, differentials between the productivity of Southern workers and their more productive Northern counterparts might be increased further, at least temporarily, by an improvement in health which
Methods of and prospects for quantification
43
largely "benefited" the South. T h e point is that, at least in the short run, increases in the labor force, without concomitant increases in the supplies of cooperating resources (land, capital goods) may depress marginal, and even average, labor productivity. This would be the case of diminishing returns to labor. Such a regional impact of health activities must be considered if public policy includes a goal such as the minimization of regional income equalities. 11 In addition, the changing age composition of the population, which accompanies reduced mortality—in particular the possibly growing number of old persons—can be expected to bring important social and political problems. Attempts to aid the increasingly important group of old voters are certain to be made —perhaps at the expense of younger persons. Much has been written about the many consequences of an aging population; we need not reiterate it. 1 2 TREATMENT
AND A L L I E D
COSTS
The economic losses attributable to a disease include the value of resources devoted to finding, treating, and rehabilitating its victims. Some data on " t r e a t m e n t " costs for various diseases are available from hospitals and health insurance company records and reports, and from the various health foundations. It should be remembered, though, that the relevance of hospital 11 Arthur Smithies, it may be noted, asserts the existence of this goal, at least for the United States: " It is recognized as socially desirable that economic disparities among regions of the country should be reduced rather than increased. If a project increases the prosperity of a depressed region, it should be regarded as more beneficial than one which benefits a region that is already prosperous." (Smithies,The Budgetary Process in the United States, M c G r a w - H i l l Book Company, New York, 1955, p. 340.) " S e e , for example, Louis I. Dublin and M o r t i m e r Spiegelman, The Facts of Life from Birth to Death, Macmillan C o m p a n y , N e w Y o r k , 1951; Paul H. Landis, Population Problems, American Book Company, Chicago, 1943; C o m m i t t e e on Old Age Security of the Twentieth Century F u n d , The Townsend Crusade, N e w York, 1936'; Alfred Sauvy, "Social and Economic Consequences of the Ageing of W e s t e r n European Populations," Population Studies, 2, N o . 1 (June 1948), 115-124.
44
Economics of Public
Health
and insurance company records and reports depends upon the proportion of total cases which are hospitalized. This proportion may vary considerably among areas. T r e a t m e n t costs may be viewed as substitutes for sickness costs, treatment speeding recovery and return to full productivity. T h e poorer a g r o u p of sick people, the less likely they are to be able to spend money on t r e a t m e n t ; that is, the less likely they are to invest in increasing their productivity. Even in wealthy areas treatment costs will differ enormously a m o n g diseases, with some, like tuberculosis, involving long, costly periods of treatment, while others, such as the common cold and the childhood diseases, being of brief duration, generally entail no hospitalization, and only modest expenditures for medication. Regarding detection costs: for most diseases there are no such costs, symptoms appearing soon after the disease is contracted. For others, including cancer and tuberculosis, the symptoms of which appear only after the disease has reached a rather advanced stage, detection costs, representing attempts to find cases " e a r l y , " consist of the costs of chest X-rays, tuberculin tests, etc. In the broad sense, all general physical examinations represent detection costs. Like chest X rays, they are designed to detect more than one ailment and, consequently, their costs are not applicable to any one source of poor health. For this reason it was decided not to attempt a quantification of detection costs by disease. " R e h a b i l i t a t i o n " is involved in only a relative handful of diseases—in particular those which leave victims with orthopoedic impairments. It is most difficult to discover directly rehabilitation costs by disease. Sometimes it is possible to estimate, first, the average cost of rehabilitating a disabled victim of the disease and, second, the proportion of the total victims of the disease requiring rehabilitation. Again there is no organized source of such information, but the various health foundations
Methods of and prospects for quantification
45
will generally have useful data on rehabilitation, as well as treatment costs (though this data may be little more than " i m p r e s s i o n i s t i c " ) . Reports of the United States Department of Health, Education and Welfare can also be helpful. In particular, the United States' National Health Survey, now in progress, is providing much information on the impact of poor health. AVOIDANCE
COSTS
W e r e there no cases of a particular disease, it would not necessarily be valid to argue that the economic costs of the disease were zero. It might be that the incidence was being held down by taking costly steps to avoid it. If a disease were entirely unavoidable (as far as people knew), then the disease would cause no " s u b s t i t u t i o n " effect. But if it is believed, rightly or wrongly, that the disease is avoidable, then there will be a shift of expenditures toward those items which hold out the promise of preventing the disease from striking. T h e increasing popularity of filter-tipped cigarettes, the filter being viewed as a device for (possibly) avoiding lung cancer, represents an " a v o i d a n c e " cost in the forms of the increased price and the possibly inferior taste of the cigarettes. Many other examples of avoidance costs may be cited. T h e incidence of some diseases, including malaria and yellow-fever, is a function of environmental sanitation conditions. Since improvement in environmental sanitation is commonly prohibitively expensive for any one person, the individual is likely to seek asylum from the unhealthful environment. On the island of Sardinia, where, previous to the recent mosquito-eradication program, malaria had been endemic, many farmers adjusted to the threat of malaria by living a distance of as much as an hour's walk from their farms; the fertile farmlands were located near swampy, mosquito-breeding areas. T h e mosquitos were not troublesome during the daylight hours, when the farms were being operated; but the situation was quite different after dusk,
46
Economics of Public Health
and residing elsewhere became necessary. In this case the cost attributable to the presence of malaria was the unproductive time and effort devoted to commuting. In a number of areas in the Philippines, surveys in 1946 revealed vast fields, forests, and mineral deposits lying undeveloped due to the recognized hazard of malaria. The sacrifice made by children who observe the admonition during the polio season to "avoid crowds and public swimming pools" is a cost of poliomyelitis. Vitamins may be viewed as a cost of generalized illness avoidance. T o some extent, movement to and commuting from suburbia represent costs of avoiding the dangers or discomforts of air pollution. Briefly, then, one reason why the incidence of some diseases is not greater is that people have by a variety of measures substituted other costs for the direct costs of poor health—premature death, sickness, treatment. The significance of this realization for the question of the relative social costs of various diseases is that the extent of these avoidance costs, which are extremely difficult to quantify or even discover, since their forms may be so varied, differ among diseases. In general, the greater the opportunities, real or imagined, for individuals to avoid the disease, the greater will be the magnitude of avoidance costs. It is interesting to note that as research progresses, shedding more light on the causes of diseases, some avoidance costs may be expected to increase. There was little point in smoking cigarettes with filters, for example, before the findings of positive correlation between the incidence of lung cancer and the extent of smoking were announced. 13 Similarly, there would have been no reason for abandoning the Philippine areas already mentioned had it not been known that something in the immmediate environment was inimical to the health of the residents. " O f course, as knowledge of cancer improves even more, the correlation may prove to be spurious or the cigarette filters ineffective, in which case the extra cost of filters may disappear, as people cease buying them.
Methods of and prospects for quantification
47
T h e quantitatively most significant cases of avoidance costs involve diseases which are products of the environment and can, therefore, be avoided by leaving the area. Such environmental diseases as malaria and yellow fever have been almost completely eliminated in this country, though they remain serious problems in other parts of the world. Thus, avoidance costs in the United States are likely to be small relative to the costs of sickness, treatment, and premature death. In our work below, we shall make no attempt to quantify them. It has been found possible and practicable to make quantitative estimates of three important categories of losses from poor h e a l t h — ( l ) premature death, ( 2 ) sickness, and ( 3 ) treatment. T h e s e three classes of costs will be computed and compared for the diseases cancer, tuberculosis, and poliomyelitis for the year 1954.14 " A l l the monetary data in this study are at prices as of around 1950.
PART
FOUR
The economic costs to the United States of poor health—illustrative quantifications for the diseases cancer, tuberculosis, and poliomyelitis
CHAPTER
VII
Quantification of losses from premature death, with application to tuberculosis, cancer, and poliomyelitis
O u r approach to m e a s u r i n g the m o r t a l i t y effects of disease is to d e t e r m i n e the p r e s e n t value of the production which t h e deceased would have contributed {i.e., the income he w o u l d h a v e e a r n e d ) less what he would have consumed, had he not d i e d . T h e " p r e s e n t value of net f u t u r e e a r n i n g s " of a person of a g e a (Fa) is defined by the following f o r m u l a : 1
' T o facilitate computation, a variation of this formula was used. In the summing, the maximum value of η was considered as 74J, an adjustment factor, involving life expectancy at that age, being used to account for subsequent years. T h e V a formula, fundamentally, is the same as that presented by Dublin and Lotka, ( T h e Money Value of a Man, Ronald Press Company, New York, 1946 Edition, p. 171, formula 8), though the interpretations differ somewhat—in particular, the meaning of the "consumption" and " e a r n i n g s " components.
Quantification of losses from premature death
49
where a is the person's a g e at his last birthday; i is the discount rate ; 4 is the probability that a person of a g e a + £ will survive to a g e η ; a n d ^ „ is the a v e r a g e earnings, net of consumption, of a person of a g e n. 2 A v e r a g e annual gross earnings are computed as the product of ( 1 ) average annual earnings of all males ( o r f e m a l e s ) having earnings at a g e n, ( 2 ) the proportion of males ( o r f e m a l e s ) who are in the labor force at that a g e , and ( 3 ) the factor 0.95, which is the proportion of the labor force assumed to be employed under " f u l l - e m p l o y m e n t " conditions. T w o sorts of data needed to perform the operations in the " p r e s e n t v a l u e " formula, but unavailable, had to be developed. T h e y were : ( 1 ) " c o n s u m p t i o n , " as a function of a g e and s e x ; and ( 2 ) the value of non-market household production by females. T h e need for the latter follows from our attempt to determine the value of a person's total production, irrespective of the method of its renumeration. It is assumed that the earnings of {i.e., the production b y ) males is adequately measured by money incomes; but the production by females is considered to be the sum of money earnings and an estimate of the market value of household services. Estimation of an individual's consumption involved g r e a t problems at both the conceptual and empirical levels. W h a t is the magnitude of personal consumption which should be attributed to an a v e r a g e person over each year of his lifetime ? T h e annual consumption of an individual who lives alone is, clearly, his total annual consumption expenditures; but the consumption of an individual who is a member of a family is more difficult to define and still more difficult to determine. A simple method for • T h i s formulation does not include explicit consideration of a person's value as a prospective parent—i.e., as a producer of children. T o the extent that a death leads to a decrease in the number of subsequent marriages and hence births, there occurs the loss of the present value of a stream of future children. It is difficult to generalize about the long-run population effects of the relatively small drop in the number of deaths which would accompany even the complete elimination of some particular disease. Investigation of this matter shall be postponed to a future study.
t:
60
Economics of Public Health
obtaining the consumption of a family member is to divide total family consumption by the number of persons in the family, or by some such figure as the number of adult-equivalent units.11 This would give average consumption. What we really want, though, is a measure of marginal consumption—that is, the additional consumption associated with an additional person. W e might try to obtain this by imputing consumption expenditures to each family member. But problems quickly arise. If in response to a wife's insistence, part of family income is devoted to the purchase of a suit for her husband, should this be considered "consumption" of the husband ? Of the wife ? Of both ? The answer is not clear. The wife may have chosen to forego a new dress in order that her husband purchase the suit; in such a case she evidently derived more satisfaction from " h i s " purchase. Now, if he were to die, so that she then purchased the new dress, could we say that her consumption had increased ? For another example of the difficulty of making consumption imputations: is an expenditure for diaper service to be considered consumption by the baby, the mother, or the entire family? And on what basis are the " o v e r h e a d " expenditures (housing for example) to be allocated among family members ? The practical difficulty of making meaningful consumption imputations led us to consider consumption a group phenomenon, no consumption expenditures at all being imputed to any one family member. W e then proceeded to determine the change in total family consumption which on an average accompanied a change in family size, ceteris paribus·, this we call "marginal family consumption" with respect to a change in family size. Thus, we suggest that a measure of a person's consumption is the difference between the total consumption of his family when he is alive and the total consumption of the remainder of the family when he drops out, because of premature death (or •See, for example, Dublin and Lotka, op. tit., p. 65.
Quantification of losses from premature death
51
for any other reason), income being held constant. No attempt is made to hold constant the expenditures of other family members : we have already seen the difficulty of identifying the consumption of individual family members. We shall not debate further the merits of this approach as compared with that of making consumption imputations. Meaningful data of either sort has not been available. It was felt that in any case only a measure of "marginal" rather than "average" consumption was desired; the approach adopted does provide such a measure. Appendix I contains a detailed description of our method of estimating consumption, together with a discussion of the shortcomings and advantages of the method. Our present-value formula shows that in addition to consumption data by age, we need corresponding figures for average earnings and survival probabilities. These data, for both males and females, plus the consumption figures, appear in Table 2. In Table 2, column (1) shows, simply, age in years; columns ( 2 ) - ( 6 ) contain the figures needed for calculating the present values of net future earnings of males; columns (7)-( 14), the figures for females. In column (2) appear data on the median earnings of males having income—which is used as an estimate of the mean contribution to production of an employed male of specified age. Since these earnings data are limited to males with earnings, it is necessary to determine the percentage of all males who have earnings in order to find the average earnings for all males. Column (3) shows the percentage of males employed under full-employment (i.e., 95 per cent of labor force employed) conditions, this being an estimator of the percentage of all males who have earnings. Our series on earnings and on employment (labor-force participation rates) had to be smoothed,4 since the statistics were initially reported by age brackets.6 •The smoothing was done by free hand. 'For data sources, see Table 2.
Economics of Public Health
52
TABLE 2. DATA
USED IN THE COMPUTATION OF THE PRESENT
Data for Males
Age
Money Earnings
(1)
(2)
75 74-75 73-74 72-73 71-72 70-71 69-70 68-69 67-68 66-67 65-66 64-65 63-64 62-63 61-62 60-61 59-60 58-59 57-58 56-57 55-56 54-55 53-54 52-53 51-52 50-51 49-50 48—49 47-48 46-47 45-46 44-45 43-44 42-43 41-42 40—41 39-40 38-39 37-38 36-37 35-36
f 1050 1120 1220 1320 1500 1750 2000 2200 2400 2590 2690 2790 2860 2910 2950 2980 3000 3020 3040 3070 3100 3130 3160 3200 3270 3340 3400 3450 3500 3540 3570 3590 3600 3610 3620 3620 3610 S590 3570 3550
Per cent Employed
Consumption
(3)
(4)
2 7 14 24 37 49 58 65 69 72 75 78 80 82 84 85 86 86 87 88 89 90 90 91 91 91 91 92 92 92 92 92 92 93 93 93 93 93 93 93
$460 460 470 480 490 500 505 510 515 520 525 530 530 535 540 540 540 535 530 525 520 515 500 485 470 450 400 330 290 270 260 255 255 250 255 255 260 265 280 340 500
Excess of Income over Consumption (J)
Probability of Living through Year
(2).(3)-(4)
(.P'a +1 )
(5)
$-439 -392 -309 -173 55 353 650 915 1136 1340 1488 1646 1753 1846 1938 1993 2045 2067 2120 2182 2244 2317 2359 2442 2526 2639 2764 2884 2950 2997 3029 3048 3062 3102 3112 3107 3092 3059 2980 2802
(6)
α 0.9309 0.9361 0.9410 0.9454 0.9493 0.9529 0.9562 0.9593 0.9622 0.9647 0.9670 0.9692 0.9713 0.9733 0.9752 0.9769 0.9786 0.9802 0.9817 0.9831 0.9845 0.9858 0.9870 0.9881 0.9890 0.9900 0.9908 0.9916 0.9923 0.9930 0.9936 0.9942 0.9947 0.9952 0.9956 0.9960 0.9963 0.9966 0.9969 0.9971
Quantification of losses from premature death
53
V A L U E S O F N E T F U T U R E E A R N I N G S , BY A G E A N D S E X
Data for Females
Money Earnings (?)
Per cent Employed (8)
$ 420 440 460 490 520 560 610 670 740 820 .900 1000 1090 1180 1260 1320 1370 1410 1450 1490 1520 1530 1540 1550 1550 1550 15.50 1560 1560 1560 1560 1570 1570 1570 1580 1580 1590 1590 1600 1610
0 1 3 5 8 9 10 10 11 12 13 15 17 19 21 25 28 32 35 36 37 37 38 38 38 38 38 38 38 38 38 38 38 38 38 38 38 38 38 38 37
Average Money Earnings (7).(8) (9) $
0 4 13 23 39 47 56 61 74 89 107 135 170 207 248 315 370 438 494 522 551 562 581 585 589 589 589 589 593 593 593 593 597 597 597 600 600 604 604 608 596
Number of Responsibility Units (10) 0.00 0.05 0.12 0.20 0.30 0.42 0.55 0.72 0.88 1.02 1.13 1.21 1.28 1.34 1.40 1.45 1.48 1.51 1.54 1.57 1.60 1.64 1.68 1.72 1.77 1.83 1.90 2.00 2.10 2.22 2.31 2.40 2.46 2.51 2.54 2.56 2.57 2.56 2.54 2.52 2.50
Value of Household Services to others (11) $
0 50 180 300 400 470 620 800 960 1080 1190 1250 1320 1370 1430 1460 1490 1510 1540 1570 1590 1620 1650 1690 1720 1750 1820 1880 1950 2030 2080 2130 2160 2180 2200 2210 2220 2210 2200 2190 2180
Excess of ProbabilValue of Production ity of Total over Con- Living Production sumption t h r o u g h Year (9) + ( l l ) ( 1 2 - ( 4 ) (12) (13) (14) $
0 54 193 323 439 517 676 861 1034 1169 1297 1385 1490 1577 1678 1775 1860 1948 2034 2092 2141 2182 2231 2275 2309 2339 2409 2469 2543 2623 2673 2723 2757 2777 2797 2810 2820 2814 2804 2798 2776
$-460 -406 -277 - 157 -51 17 171 351 519 649 772 855 960 1042 1138 1235 1320 1413 1504 1567 1621 1667 1731 1790 1839 1889 2009 2139 2253 2353 2413 2468 2502 2527 2542 2555 2560 2549 2524 2458 2276
a 0.9485 0.9531 0.9575 0.9615 0.9652 0.9684 0.9714 0.9741 0.9764 0.9782 0.9798 0.9813 0.9827 0.9841 0.9854 0.9866 0.9876 0.9886 0.9895 0.9903 0.9910 0.9917 0.9923 0.9929 0.9934 0.9939 0.9943 0.9947 0.9951 0.9955 0.9959 0.9962 0.9965 0.9968 0.9970 0.9973 0.9975 0.9977 0.9978 0.9980
64
Economics of Public Health T A B L E 2. Data for Males (continued)
(1)
(2)
(3)
(*)
34-35 33-34 38-33 31-32 30-31 29-30 28-29 27-28 26-27 25-26 24-25 23-24 22-23 21-22 20-21 19-20 18-19 17-18 16-17 15-16 14-15 13-14 12-13 11-12 10-11 9-10 8-9 7-8 6-7 5-6 4-5 3-4 2-3 1-2 0-1
$3510 3470 3420 3370 3310 3250 3180 3100 2900 2600 2300 2000 1720 1460 1220 1000 800 620 460 320 200 0 0 0 0 0 0 0 0 0 0 0 0 0 0
93 93
$535 550 555 655 550 545 535 515 470 410 405 400 400 405 420 450 540 570 550 520 480 430 390 350 310 275 240 215 195 180 165 155 145 135 130
93
93 93 93 92 92 91 90 89 88 87 85 83 80 75 67 53 24 8 0 0 0 0 0 0 0 0 0 0 0 0 0 0
(5)
(6)
$2729 2677 2626 2579 2528 2478 2391 2337 2169 1930 1642 1360 1096 836 593 350 60 -155 -306 -443 -464 -430 -390 -350 -310 -275 -240 -215 - 195 - 180 - 165 -155 - 145 - 135 - 130
0.9973 0.9975 0.9976 0.9978 0.9979 0.9979 0.9980 0.9980 0.9980 0.9980 0.9980 0.9980 0.9980 0.9981 0.9982 0.9983 0.9984 0.9986 0.9987 0.9989 0.9990 0.9992 0.9993 0.9993 0.9994 0.9994 0.9993 0.9993 0.9992 0.9991 0.9990 0.9989 0.9985 0.9976 0.9666
ο For ages 75 and more, "present values" were computed by five-year age groups, using life-expectancy figures. At age 75, life expectancy was approximately eight years for males and nine years for females. SOURCES OF DATA IN T A B L E 2 : Columns ( 2 ) and (7)—free-hand smoothing of unpublished data on median earnings in 1951 obtained from the U. S. Bureau of the Census. The data are based on a sample, the 1952 Current Population Survey. Columns ( 3 ) and (8)—free-hand smoothing of the data on labor-force participation
Quantification of losses from premature death
55
continued) Data for Females (continued)
(7)
(8)
(9)
(10)
(11)
(12)
(13)
(14)
J1620 1630 1640 1650 1660 1660 1660 1660 1650 1620 1580 1530 1470 1390 1300 1200 1050 880 680 450 200 0 0 0
35 33 32 32 32 32 32 33 34 36 39 43 46 48 50 51 60 38 20 10 3
$567 538 525 528 531 531 531 548 561 583 616 658 676 667 650 612 525 334 136 45 6
2.47 2.43 2.39 2.34 2.30 2.25 2.19 2.12 2.04 1.95 1.85 1.70 1.50 1.25 0.65 0.40 0.26 0.15 0.05
$2160 2140 2120 2100 2070 2040 2000 1960 1920 1850 1780 1670 1510 1300 730 450 290 170 60
$2727 2678 2645 2628 2601 2671 2531 2508 2481 2433 2396 2328 2186 1967 1380 1062 815 504 196 45 6
$2192 2128 2090 2083 2051 2026 1996 1993 2011 2023 1991 1888 1786 1564 960 612 275 -66 -364 -455 -344 -280 -250 -235 -220 -210 -200 -190 -180 -170 - 165 -160 -155 -150 -145
0.9981 0.9982 0.9984 0.9984 0.9986 0.9986 0.9987 0.9988 0.9988 0.9989 0.9989
0 0 0 0
0 0 0
0 0 0 0
0 0 0 0 0 0 0 0 0 0
0 0 0 0
0 0 0 0 0 0 0 0 0 0
0 0 0 0
0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0
0 0 0
0 0 0 0
0.9990
0.9990 0.9990 0.9991 0.9991 0.9991 0.9992 0.9993 0.9994 0.9995 0.9995 0.9996 0.9996 0.9996 0.9996 0.9995 0.9995 0.9994 0.9993 0.9992 0.9990 0.9988 0.9978 0.9741
rates, in U . S. Bureau of the Census, Current Population Reports, Labor Force, Series P-50, No. 40, Annual Report of the Labor Force, 1951, Washington, D. C., p. 3. T h e smoothed figures were multiplied by 95 per cent, this being the percentage of the labor force assumed to be employed at "full employment." Columns ( 4 ) , ( 1 0 ) , and ( 1 1 ) — o u r computations. See Appendices I and II. Columns ( 6 ) and ( 1 4 ) — U . S. Department of Health, Education and Welfare, Public Health Service, National Office of Vital Statistics, "United States Life Tables, 1 9 4 9 - 1 9 5 1 , " Vital Statistics Special Reports, 41, No. 1 (November 23, 1954), 10-11 (males) and 12-13 (females).
66
Economics of Public Health
T h e product of column ( 2 ) , which is, essentially, average earnings of employed males, and column (3), percentage employed, is the average earnings of all males under current fullemployment conditions; and when from this, "consumption," column ( 4 ) , is subtracted, the result is column ( 5 ) , the excess of earnings over consumption at each age. The last data needed for males are the probabilities of surviving through a given year ; these are given in column ( 6 ) . Turning to the data for females we find that columns (7) and ( 8 ) are entirely analogous to the columns (2) and ( s ) for males. The median earnings of those females with earnings, column ( 7 ) , is multiplied by the percentage of females employed at full employment, column ( 8 ) , to obtain the average money earnings per female, column ( 9 ) . At this point we deviated from the procedure used for males to take into account the important, though financially unremunerated, production by females in the form of household services. W e hypothesized that the value of a housewife's services was directly related to (though not necessarily proportionate to) the number of other persons (termed "responsibility u n i t s " ) in the family. The size of families being related to the age of the woman of the house, the value of the average female's houshold production is, likewise, a function of her age. T h e particular methods we used to determine the number of responsibility units as a function of age and the value of household production as a function of the number of responsibility units are described in Appendix II. The results appear in Table 2. T h e value of total production by the average female is the sum, column (12), of her market-oriented production, column ( 9 ) , and her non-market, household production, column ( l l ) . From this value of total production, consumption is subtracted to obtain column (13), the excess of production over consumption. Due to a limitation imposed by the basic data, only one
Quantification of losses from premature death
SI
"consumption" series by age, for both sexes, could be derived; hence, the consumption deducted from females' total production is the same as that used for males. And, finally, column
(14)
shows the survival probabilities for females. One thing more is needed before the present values of net future earnings can be computed—an appropriate discount rate. W e have decided to make the computations at both 4 and 10 per cent rates of discount. W h y , it might be asked, discount net future earnings at two different rates; and why choose 10 per cent and 4 per cent ? First, it was felt that discounting both by a rather high and by a rather low rate would indicate the relative dependence upon the discount rate of our conclusions regarding the comparative losses from different diseases. Beyond this, the decision to use lOpercent came about as follows: one meaningful rate of discount to use would be the marginal productivity of capital—the rate of return obtainable on the best alternative use of the resources which might be devoted to improving health. In recent years common stocks of large American corporations have been yielding 5 per cent or more; when account is taken of the 52 per cent tax to which corporate profits have been subject, the average rate of return on investment is seen to be on the order of 10 per cent.® Of course, the rate of return on a corporate stock also includes the appreciation of its capital value resulting from the reinvestment of retained earnings. This tends to make the rate of return on investment in United States Industry even more than 10 per cent. T h e relative risk attached to investment in public health and in the activities of the average large corporation considered •Referring to current work by G e o r g e Stigler, Gary Becker reported that between 1948 and 1954 all U.S. corporations averaged between 10 and 13 per cent returns on assets; while for the unincorporated sector, returns were estimated at 5 to 8 per cent. Corporate capital was estimated at about 60 per cent of all business capital. ( G a r y S. Becker, "Underinvestment in College Education ? " , American Economic Review, Papers and Proceedings, 50, N o . 2 ( M a y I 9 6 0 ) , 349.) If we assume that corporate capital ( 6 0 per cent of total business capital) earned a mean return of 11.5 per cent, while non-corporate capital earned 6.5 per cent, we obtain a weighted mean return for all business capital of 9.5 per cent.
58
Economics of Public Health
above should also be considered. Insofar as investment in public health is less or more risky, the appropriate discount rate is thereby reduced or increased. All these factors being considered, the 10 per cent rate of discount seemed to be sensible. The 4 per cent rate was chosen as the cost to the federal government of borrowing long-term funds. If the government were to undertake any or all investments which would be expected to return more than the cost to the government of borrowing the funds (regardless of the existence of more productive private investment opportunities), then the 4 per cent rate would be appropriate. The following statement of President Eisenhower in a recent news conference suggests that the government's borrowing cost, rather than the society's opportunity cost, is the mark used to determine the wisdom of government investment; when queried about R. E. A. loans for electricity and telephones, the President replied: . . . after all let's not forget there is 2 per cent money being involved here, and the 2 per cent is money that on the long-term, the Government today has to pay 4 per cent or over.7 Still another rate which has been advocated is the social rate of time preference, which is a measure of the annual interest rate which consumers would require for postponing consumption. Use of such a rate implies acceptance of sovereignty of the present generation (vis-ä-vis the future generations) of consumers with respect to intertemporal choices. Otto Eckstein has estimated that under full-employment conditions this " social cost of federal capital" is approximately 6-6 per cent. 8 It seems clear that there exists no unique discount rate which is "correct" to use. For one thing the relative well-being of the '"President's News Conference," Wall Street Journal, August 22, 1957, p. 6. •See Otto Eckstein, Water-Resource Development : The Economics of Project Evaluation, Harvard University Press, Cambridge, 1958, p. 99; also John V. Krutilla and Otto Eckstein, Multiple Purpose River Development: Studies in Applied Economic Analysis, Johns Hopkins Press, Baltimore, 1958, ch. IV.
Quantification of losses from premature death
59
present generation and future generations is influenced by the choice of a discount rate because of the effect on investment; and so the rate chosen implies a value judgment regarding the importance of various generations. Such " i m p o r t a n c e " cannot be determined scientifically. For this reason it may be useful to present results of computations at two (as we have done) or more rates of discount, leaving it to government decision makers to choose.® Having all the data needed, and having decided to use both a 10 per cent and a 4 per cent discount rate, the calculations of the "present value of net future earnings," according to age and sex, have been made; and the results appear in Table 3 and in Chart 2. 10 With these present values we can compute the premature mortality losses from any disease (type of accident, etc.) once we have statistics on mortality, by age and sex. These computations of premature-mortality losses have been performed for cancer, tuberculosis, and poliomyelitis in Tables 4, 5, and 6, for the year 1954. An implicit assumption upon which the present value figures were constructed is that all cases of mortality from any disease are independent with respect to family—that is, occur in different families. If, in two different families, the husband in one and •This view is apparently shared by Julius Margolis ( " T h e Economic Evaluation of Federal Water Resource Development," American Economic Review, 49, No. 1 (March 1959), 103.) Itmay be added that with modern electronic computers it is easy to make calculations at a variety of discount rates. 11 It should be interesting and useful, as a sort of check of our work, to compare our figures for the present values of net future earnings, by age, with those computed by Dublin and Lotka some thirty years ago. Chart 3 shows our series and theirs, for males. Except that their series employed a 4 j per cent discount rate while ours was computed at 4 per cent (a difference which would tend to make our results greater in absolute size than theirs), the two are quite comparable. As between the two sets of figures, the source of income data differed, as did the method of computing "consumption"; other factors contributing to the differences in results are (1) the inflation which occurred in the period between the two calculations (which tended to increase the value of all assets, including a man) and (2) the reductions in age-specific mortality rates, which have been most pronounced at earlier ages. In this light, the two series seem reasonably consistent. Of course, labor productivity rose substantially in the period.
60
Economics of Public Health
TABLE SEX,
3.
P R E S E N T V A L U E S OF N E T
FOR T H E
UNITED STATES,
AT
RATES,
4
FUTURE E A R N I N G S , BY A G E AND AT
1 0 PER C E N T
1950
Males 10 Per Cent (1)
4 Per Cent (2)
f
$ -442 -850 -1227 -1573 -2180 -2686 -2880 -3009 -3057 -2984 -2710 -2186 - 1429 -484 601 1804 3068 4406 5769 7145 8541 9919 11285 12631 13938 15274 16615 17985 19343 20739 22168 23660 25221 26848 28484 30111 31715 33287 34821 36345 37830 39260
-418 -760 -1037 - 1257 - 1558 - 1717 -1850 - 1925 - 1923 -1807 - 1506 -981 -257 616 1584 2624 3680 4766 5833 6875 7898 8871 9801 10666 11504 12327 13140 13954 14741 15542 16356 17212 18114 19056 19982 20876 21726 22526 23273 23999 24676 25294
Females Age at Last Birthday
10 Per Cent
(3)
(4)
4 Per Cent (5)
100 97 92 87 82 77 74 73 72 71 70 69 68 67
$ -418 -760 -1037 -1257 -1558 - 1717 -1887 - 1886 - 1783 - 1605 -1392 - 1066 -616 -62 550 1210 1877 2574 3276 3999 4743 5496
$ -442 -850 - 1227 - 1573 -2180 -2686 -3185 -3235 -3171 -3020 -2822 -2495 -2022 - 1421 -733 34 837 1699 2598 3544 4541 5576
7048 7819 8570 9296 10017 10731 11427 12109 12845 13639 14470 15323 16158 16972 17748 18479 19161 19796 20382
7777 8913 10056 11197 12355 13526 14700 15877 17128 18458 19849 21285 22727 24171 25594 26991 28353 29676 30959
66 65
64 63 62 61 60 59 58 57
56 55
54 53 52 51 50 49 48 47 46 45 44 43 42 41 40 39
6265
AND
DISCOUNT
6654
Quantification
of losses from
premature
61
death
T A B L E 3 (continued) (2)
(3)
(4)
(5)
$25847
$40630
38
$20907
$32185
26324
41921
37
21363
33344
26689
43095
36
21717
34394
26856'
44054
35
21869
35229
26944
44912
34
21929
35953
26979
45692
33
21925
36589
26966
46396
32
21889
37169
26914
47032
31
21842
37711
26821
47603
30
21781
38217
26689
48099
29
21703
38677
26490
48494
28
21605
39095
26258
48826
27
21515
39496
25887
48969
26
21450
39899
25323
48879
25
21406
40303
24537
48507
24
21335
40659
23557
47879
23
21212
40942
22415
47017
22
20966
41077
21135
45939
21
20529
40985
19743
44670
20
19561
40312
18251
43220
19
18350
39324
16623
41548
18
16926
38045
14993
39741
17
15315
36487
(1)
13276
37862
16
13576
34711
11634
35929
15
11882
32888
10124
34058
14
10345
31142
8787
32299
13
8990
29506
7611
30651
12
7798
27977
6581
29108
11
6753
26546
5684
27667
10
5841
25210
4902
26316'
9
5046
23961
4225 3G33
25049 23857
8 7
4356 3753
22790 21G91
3114
22729
6
3224
20652
2657
21657
5
2757
19666
2256'
20641
4
2347
18732
1901
19672
3
1984
17841
1588
18744
2
1663
16992
1312
17847
1
1380
16170
1032
16461
0
1100
15018
N o t e : T h e present values for ages above 74 are computed at the mid-points of the five-year age brackets. Source: Our computations. For ages up to 74 years, present values of net future earnings were obtained from data in Table 2. For ages above 74, present values were approximated by the product of annual consumption at these ages ( $ 4 6 0 ) and the life expectancy in years—this product discounted for the vears of life L (F C ) expectancy—symbolically,
-
^
· where L a = life expectancy at age a,
Ε = earnings (assumed to equal 0 at ages above 74), and C = consumption.
Economics of Public Health
62
CHART
2.
P R E S E N T V A L U E S OF N E T F U T U R E E A R N I N G S , BY
AND S E X , A T 1 0 AND A T 4 P E R C E N T DISCOUNT R A T E S , C I R C A
AGE 1950
51 48 45
4 per cent
42 39 Male
36
Female
33 10 per cent
30 27 24 21 18 15 12 9 6 3 0 3 6 10
20
30
40
50
A g e in years at last birthday
Source: Table
3.
60
70
80
Quantification of losses from premature death
C H A R T 3.
P R E S E N T VALUES OF N E T FUTURE E A R N I N G S , BY A G E ,
1920
AND
63 MALES,
1950
Age in years at last birthday
S o u r c e : 1950
figures—Table
3.
1920 figures—Dublin and Lotka, op. cit., p. 220, column (4), by permission of the publisher.
64
TABLE
Age in Years (1)
Economics of Public Health 4.
PREMATURE MORTALITY
Number of Male Deaths (2)
LOSSES RESULTING
FROM C A N C E R
Present Value of Foregone Future Net Earnings of Males Dying from Cancer in 1954 ( $ 0 0 0 ) , at Discount Rate of 10% 4% (3) (4)
DEATHS
Number of Female Deaths (5)
1,048
$ 1,992
$20,616
871
5-10
653
2,372
15,579
529 333
0-5 10-15
448
3,410
13,732
15-20
515
7,696
20,467
315
20-25
586
13,136
27,552
465
25-30
862
22,634
42,088
849
SO-35
1,246
33,600
57,809
1,759
35—40
1,886
49,647
79,063
3,196
40-45
3,319
77,243
115,571
5,426
45-50
5,763
109,820
154,725
7,721
50-55
9,112
134,320
176,253
9,992
55-60
13,186
140,642
166,552
11,653
60-65
17,399
101,488
100,375
13,790
65-70
19,904
12,261
-9,634
15,029
70-75
18,121
- 34,847
-55,396
14,386
75-80
14,358
- 24,653
-38,566
12,159
80-85
8,997
-14,017
- 19,613
8,205
85-90
3,964
-4,983
-6,235
3.974
90-95
1,020
- 1,058
- 1,252
1,174
133
- 101
- 113
245
95-100 Over 100
19
All Ages
122,539
-8
$630,594«
-8
$859,56ό"
29
112,130
"Items may not sum to the column totals clue to rounding.
Source: Mortality data from Vital Statistics of the United States, 1954, V. 2, L'. S. Department of Health, Education and Welfare, Public Health Service, National
Quantification 1954,
BY
AGE
AND S E X ,
AT
of losses from premature 4
Present Value of Foregone Future Net Earnings of Females Dying from Cancer in 1954 ( $ 0 0 0 ) , at Discount Rate of 10% 4% (6) (7)
AND A T
10
PER
death
CENT
65
DISCOUNT
RATES
Total Present Value of Foregone Future Net Earnings of All Persons Dying from Cancer in 1954 ( $ 0 0 0 ) , at Discount Rate of 10% 4% (3) + (6)
(8)
(4) +
(9)
(7)
? 1,728
$ 15,540
$3,695
1,985
11,474 9,316
4,358
11,493
17,445
22,895 31,960
2,597 4,824
8,234
$36,156 27,053
9,749
19,100
31,401
46,653
18,266
33,532
46,901
38,503
65,380
72,102
75,620 123,190
69,408 103,968
106,567
119,054
185,630
146,453
181,211
262,024
112,157
153,850 135,152
221,477 241,544
308,575
107,224 82,130
90,625
272,772
275,178
45,176
35,826
146,664
136,201
-932
-21,356
11,329
- 25,650
-45,618
- 20,877 - 12,783
-32,659 - 17,887 -6,251
- 10,497 -45,430 -26,801
-30,990 - 101,014
311,405
-71,225 -37,500
- 1,217 -186
- 1,440
-9,978 -2,275
-208
-287
-2,692 -321
-12
- 13
-26
-212
- 4,995
$531,056«
$708,878«
$1,183,394«
-12,486
$1,568,443«
Office of Vital Statistics, U. S. Government Printing Office, Washington, 1956, 166-7. Cases for which age at death was not stated were distributed in proportion to the relative frequencies of those deaths which were reported by age. Present values are based on figures in Table 3 ; the present value of a person in a five-year age class was taken as of the age mid-point of the class. F
66
Economics of Public Health
TABLE
5.
PREMATURE
M O R T A L I T Y LOSSES R E S U L T I N G
FROM
10 PER
CENT
AT
Present Value of Foregone Future Net Earnings of Males Dying from Tuberculosis in 1954 ( $ 0 0 0 ) , at Discount Rate of 10% *%
Age in Years
Number of M a l e Deaths
(1)
(2)
(3)
217 30 17 56 118 270 387 586 832 1,023 1,293 1.406
(412
0-5 5-10 10-15 15-20 20-25 25-30 30-35 35-40 40—45 45-50 50-55 55-60 60-65 65-70 70-75 75-80 80-85 85-90 90-96 95—100
All Ages
109 129 837 2,645 7,090 10,436 15,426 19,363 19,494 19,060 14,996 8,160 870
(4) 14,269 716 521 2,225 5,548 13,183 17,955 24,566 28,971 27,4«6 25,010 17,759 8,071 -683
1,399 1,412 1,133 744 380 158 29 2
-2,179 - 1,277 -592 - 199 -30 -2
— 3,-K>4 - 1,998 -828 -248 -36 -2
11,494·
$114,750»
$169,000«
Number of Female Deaths (5) 207 31 18 110 182 336 399 460 444 393 354 296 286 378 377 302 216 82 18 4
4,898
»Items may not sum to the column totals due to rounding. Source: Mortality data—same as Table 4, only pp. 164—5. Cases for which age was not stated were handled as in Table 4. Present values are based on figures in Table 3 ; the present value of a person in a five-year age class was taken as of the age mid-point of the class.
67
Quantification of losses from premature death TUBERCULOSIS D E A T H S IN DISCOUNT
1 9 5 4 , BY A G E
A N D SEX, A T
4
AND
RATES
Present Value of Foregone Future Net Earnings of Females Dying from Tuberculosis in 1954 (1000), at Discount Rate of 10% 4%
(6)
(7)
Total Present Value of Foregone Future Net Earnings of All Persons Dying from Tuberculosis in 1954 (9000), at Discount Rate of >0% 4% (3) + (6) (4) + (7) (8) (9)
$411
$3,693
$828
116
672
225
$7,962 1,388
140
504
270
1,025
1,685
4,014
2,521
6,239
3,816
7,476
6,461
13,024
7,229
13,271
14,319
26,454
8,734
14,830
19,160
32,786
9,827
15,338
25,253
39,904
8,205
11,984
25,668
40,955
5,687
7,801
25,181
35,266
3,799
4,788
22,859
29,799
2,086
2,302
17,083
20,061
937
743
9,697
8,814
-23
537
846
-1,220
- 1,195
- 3,627
- 4,659
-518
-811
- 1,786
-2,810
-336
-471
-928
-1,299
-109
- 137
-307
-385
-19
-22
-48
-58
-3
-3
-4
-5
-672
$50,989«·
$84,239"
$ 165,568a
$253,239»
68
Economics of Public Health
TABLE
6 . P R E M A T U R E - M O R T A L I T Y LOSSES RESULTING FROM AT 1 0 PER C E N T
Age in Years (1)
Number of Male Deaths (2)
Present Value of Foregone Net Future Earnings of Males Dying from Poliomyelitis in 1954 ($000), at Discount Rate of 10% 4% (3) (4)
Number of Female Deaths (5)
0-5 5-10 10-15 15-20 20-25 25-30 30-35 35—40 40—45 45-50 50-55 55-60 60-65 65-70 70-75 75-80
148 128 96 65 61 108 88 39 25 17 5 7 2 2 1 0
$281 465 731 971 1,367 2,836 2,373 1,027 582 324 74 75 12 1 -2 0
$2,911 3,056 2,942 2,583 2,871 5,273 4,083 1,635 870 456 97 88 12 1 -3 0
106 105 65 45 57 75 64 23 12 9 6 4 3 2 0 0
All Ages
792
$11,116»
$26,875a
576
"Items may not sum to the column totals due to rounding.
Source: Mortality data—sameasTable4, only pp. 164-5. Cases for which age not stated were handled as in Table 4. Present values are based on figures in Table 3; the present value of a person in a five-year age class was taken as of the age midpoint of the class.
Quantification
of losses from premature
death
69
POLIOMYELITIS D E A T H S IN 1 9 5 4 , BY AGE AND S E X . A T 4 A N D DISCOUNT R A T E S
Present Value of Foregone Future Net Earnings of Females Dving from Poliomyelitis in 1954 ( ( $ 0 0 0 ) , at Discount Rate of 10% 4% (6)
(7)
Total Present Value of Foregone Future Net Earnings of All persons Dying from Poliomyelitis in 1954 ( $ 0 0 0 ) , at Discount Rate of 10% 4% (S) + ( 6 ) (4) + ( 7 ) (8) (9)
$210 398 507 689 1,195 1,614 1,401 491 222 130 64 28 10 0 0 0
$1,891 2,278 1,818 1,642 2,341 2,962 2,379 767 324 179 81 31 8 -3 0 0
$492 859 1,238 1,660 2,562 4,449 3,774 1,518 804 454 138 103 21 1 -2 0
$4,803 5,334 4,761 7,225 5,213 8,235 6,462 2,402 1,194 635 178 120 19 —4 -3 0
$6,955«
$16,698°
$18,072®
$43,573«·
70
Economics of Public Health
the wife in another were to die, the losses would be expected to be those we have computed. If, instead, the husband and wife in one family were to die, the total economic loss would be smaller; for example, if this were a two-person family there would be no need to replace the services of the housewife. The point is essentially this: much of the loss due to premature mortality is felt by the surviving family members; therefore, to the extent that there are no surviving family members, economic losses to all survivors are minimized. Were the appropriate mortality data available, this dependence of losses on family conditions could be considered. Since mortality data are not reported according to family size and presence of spouse, some working assumption had to be made. Our implicit assumption that deaths from any one disease (or other cause of death) occur one to a family would seem to be valid in varying degrees for different causes of mortality. It is probably less valid for contagious than for non-contagious diseases; it is probably more valid for diseases in general than it is for automobile fatalities. By and large, it would appear to be a reasonably satisfactory assumption. Premature mortality, is, we have noted, but one form of the poor health losses from a disease. 11 In the chapter which follows we shall continue to illustrate a means for quantifying the losses from a disease; we do this by measuring the sickness losses and treatment costs resulting from the incidence of cancer, tuberculosis, and poliomyelitis. 11 It may be interesting to compare magnitudes of the estimated present values of foregone future net earnings of 1954 victims of each disease with the 1954 United States figures on total compensation of employees—$207 billion. 1954 mortality losses from cancer (Table 4, column 8 total) were 0.57 per cent of total employee compensation; mortality losses from tuberculosis (Table 5, column 8 total), 0.08 per cent; and from poliomyelitis (Table 6, column 8 total), less than 0.01 per cent.
C H A P T E R VIII
Quantification of losses from morbidity, and including treatment costs, with application to tuberculosis, cancer, and poliomyelitis
MORBIDITY
LOSSES
Just as premature death means the permanent loss to society of a producer, so morbidity due to poor health means the temporary loss of a producer. 1 W e can determine the extent of these morbidity losses for any disease if we know ( 1 ) the age and sex incidence of the disease, ( 2 ) the average duration of illness it causes, and ( s ) earnings of its victims, or, lacking the latter, average earnings of the general population by age and sex. For example, if a male of specified age a has average annual earnings oiy dollars and if each case of a particular disease results in lost production for an average of t years, we would know that η cases of the disease among males of age a would result in lost production in the amount of n-t-y dollars. Performing similar computations for all ages and both sexes, and summing, we would have an estimate of total morbidity losses from the disease for the given period. Average earnings (value of production) by age and sex have already been used in the computation of present values of future earnings in Chapter VII and appear in Table 2 column (12) for females and as the product of columns ( 2 ) and ( s ) for males. But estimating the average duration of an illness from each disease and obtaining data on age and sex incidence involved additional work. How this information was derived for each of the three diseases we are considering is described below. The devices 1
But in the latter case, not the loss of a consumer.
72
Economics of Public
Health
and sources utilized may be suggestive to anyone interested in quantifying the losses from other diseases. Cancer. Case Incidence. Not being a "reportable " disease, cancer cases are not counted in official statistics. In a statement from the National Cancer Society it was estimated that there would be some half-million new cases of cancer in the United States in 1953.2 This estimate has been used in our computations for 1954, the number of new cases being assumed to change little in one year. Next we need to obtain an age and sex classification of these half-million cases. From a study of cancer incidence in 1947 in ten metropolitan areas of the United States 3 we determined that some 52 per cent of cancer cases occur among females. 4 From the same study we computed the percentages of total cases in each five-year age bracket. These percentages were applied to the total cases among females (52 per cent of 500,000) and among males (48 per cent of 500,000) to arrive at the figures on new cancer cases in 1954 by age and sex (see Table 7). Average duration of illness. For some diseases the average duration of hospital stay will serve as a good approximation of the length of illness-caused loss of production; especially is such the case for the dangerous contagious diseases, including poliomyelitis and tuberculosis. But cancer is a contrary example. Given our present unsatisfactory medical knowledge of how to treat cancer, there is often little reason for a cancer patient to be hospitalized continuously. Thus, the average total length of hospital stay (first admissions and readmissions) for hospital* Health Inquiry, Hearings before the Committee on Interstate and Foreign Commerce, House of Representatives, Eighty-third Congress, first session, U. S. Government Printing Office, Washington, D. C., 1953, Part 1, p. 228. •Harold F. Dorn and Sidney J. Cutler, Morbidity from Cancer in the United States, Public Health Monograph No. 29, U. S. Department of Health, Education and Welfare, U. S. Government Printing Office, Washington, 1955, pp. 92, 93. •A small excess of female over male victims of cancer is also disclosed by the "Report of Vermont Cancer Survey, January 1, 1947 to January 1, 1948" (dittoed), which showed that 54 per cent of persons hospitalized with cancer were females.
Quantification
of losses from morbidity
73
ized cancer patients is in the neighbourhood of only thirty days. 6 The mean period of disabling illness from cancer, certainly longer than thirty days, is quite difficult to determine, since results of the disease vary so much with the location of the cancer. It would seem reasonable to estimate the mean period of disabling illness at one year for the three-fourths of all cancer cases which currently prove fatal. For the one-fourth of all cases which are not fatal, disability is far more limited—perhaps on the order of one month.® For the average of all cancer cases, ten months of disabling illness is a likely approximation. T o be sure, these estimates are impressionistic; more precise data would be desirable. Now, having an estimate of the average period of illness from cancer, five-sixths years, and knowing the age and sex incidence of the disease and average earnings by age and sex, we can find the value of lost production expected to result from illness associated with the new (1954·) cancer cases. (See Table 7.) Tuberculosis. Case incidence. Useful, though imperfect, data are available on the incidence of newly reported cases of tuberculosis according to age 7 and according to sex ; 8 but, unfortunately, not according to age and sex. In the absence of this latter data we have assumed that the overall ratio of cases among males to cases among females—approximately two to one 9 —applies to all ages. Average duration of illness. Production losses due to tuber6 Twenty-seven days is the estimate in Health Inquiry, Part 1, p. 201; a few pages later in the same " Inquiry," the National Cancer Institute estimated thirtytwo days (p. 212). •Some cancers, such as lip cancers, are treatable in a doctor's office, thus requiring little, if any lost time. 'U.S. Department of Health, Education and Welfare, Public Health Service, Reported Tuberculosis Data, 1954·, Publication No. 471, U. S. Government Printing Office, Washington, D. C., 1956, p. 22. »Ibid., p. 18. •Sex-specific case rates of newly reported active and probably active (Group "A") tuberculosis cases, continental United States, 1954, for white persons were as follows: males—54.6; females—26.7 (per 100,000). (Source: Ibid.)
74
Economics of Public Health T A B L E 7.
PRODUCTION
LOSSES E X P E C T E D
FROM
CANCER-CAUSED
M O R B I D I T Y , Y E A R 1 9 5 4 C A S E S , BY A G E AND SEX
Age in Years (1)
N u m b e r of Cases, Males, 1954 (2)
Production Losses, Males ( $ 0 0 0 ) (3)
Number of Cases, Females, 1954 (4)
Production Losses, Females ( $ 0 0 0 ) (5)
0-5 5-10 10-15 15-20 20-25 25-30 SO-S5 35—40 40-45 45-50 50-55 55-60 60-65 65-70 70-75 75-80 80-85 85-90 90-95 95-100
1,440 960 720 1,200 1.440 2,400 3.840 5,760 9,360 13,920 24,480 33,360 39,360 35,040 29,760 20,880 11,040 4,080 720 240
0 0 0 415 1,795 5,704 10,180 16,027 25,834 36,818 58,018 72,191 75,060 41,768 4,241 0 0 0 0 0
1,300 520 780 1.040 1,830 3,910 7,290 11,720 17,720 24,230 30,480 33,090 34,390 30,740 25,530 18,500 10,680 4,950 1,040 260
0 0 0 437 3,334 8,172 16,067 27,390 41,004 51,343 57,790 56,088 45,188 26,486 6,870 0 0 0 0 0
All Ages
240,000
$348,050»
260,000
$340,168a
Totals, All Ages, Both Sexes: Cases—500,000; Losses ( $ 0 0 0 ) — $688,218 ο Items may not sum to the column totals due to rounding. Sources: Number of cases—text, above; loss figures for each a g e assume 5/6 years of lost production per case (see text, a b o v e ) ; values or production in each five-year bracket were taken (from Table 1) as of the age mid-point of the class.
culosis morbidity are based upon an estimated period of one year of unavailability for work per case. This one-year period was suggested by the records of the Mineral Springs Sanatorium, Cannon Falls, Minnesota, which show that the average length of stay of all patients discharged with medical approval
Quantification of losses from morbidity
76
10
was 370 days in 1954. At the same time, our analysis of data on recently discharged patients disclosed that a period of several months generally elapsed between sanatorium discharge and the onset of even part-time work. This would suggest a figure of more than one year of lost production per tuberculosis patient, except insofar as there are cases of tuberculosis which do not enter a hospital or sanatorium. These may include cases discovered early enough to be treated without confinement, or cases discovered only at the time of death, having developed quickly and thereby resulted in a relatively brief period of disabling illness. Such cases would reduce the average period of lost production. The appropriateness of our use of the figure of one year of unavailability for work per case was attested to by the National Tuberculosis Association in private correspondence. 11 The one year of illness per case is applied to the age- and sex-specific incidence of tuberculosis in 1954 in Table 8, in which the illness-caused productivity losses are calculated. Poliomyelitis. Case Incidence. In 1954· there were 38,476 cases of poliomyelitis reported. 12 T o estimate the age incidence of those cases we made use of hospital-admissions data for polio patients, by age group, 1 3 assuming the distribution of cases in the " 2 0 and o v e r " group to be proportional to the distribution of deaths from poliomyelitis at these ages. 14 The sex incidence of the cases was estimated on the assumption that it was the same as the sex incidence of deaths from polio in 1954. 16 The "Mineral Springs Sanatorium, Cannon Falls, Minnesota, 1955 Annual Report, p. 13. "Dated December 27, 1966. " U . S. Bureau of the Census, Statistical Abstract of the United States: 1957. (Seventy-eighth edition). Washington, D. C., 1957. p. 83. " T h e National Foundation for Infantile Paralysis, Polio Facts for Speakers and Writers, New York, 1957, p. 7. "See Table 6. "Table 6 discloses that 792, or 57.9 per cent of the 1,368 deaths from poliomyelitis in 1954 were among males. A study made in 1935-6 of polio cases showed 56.8 per cent were among males. See Selwyn D. Collins, " T h e Incidence of Poliomyelitis and Its Crippling Effects, as Recorded in Family Surveys," Public Health Reports, 61, No. 10 (March 8, 1946), 348.
Economics of Public Health
76
TABLE
8 . P R O D U C T I O N L O S S E S E X P E C T E D FROM
CAUSED MORBIDITY, Y E A R
Age in Years (1) 0-5 5-10 10-15 15-20 20-25 25-30 30-35 35—40 40—45 45-50 50-55 55-60 60-65 65-70 70-75 75-80 80-85 85-90 90-95 95-100 All Ages
Number of Cases, Males, 1954
(2)
1,741 854 854 2,078 4,157 4,680 4,735 4,735 4,677 4,500 4,285 3,985 3,476 2,951 2,500 2,186
0 0 0 0
52,394
Production Losses, Males ( $ 0 0 0 )
(3)
9
TUBERCULOSIS-
1 9 5 4 C A S E S , B Y A G E AND S E X
0 0 0 862 6,219 13,347 15,062 15,810 15,490 14,283 12,186 10,349 7,953 4,220 428
0 0 0 0 0
$116,210"
Number of Cases, Females, 1954 (4) 871 427 427 1,039 2,079 2,340 2,367 2,368 2,338 2,250 2,142 1,993 1,738 1,476 1,250 1,093
0 0 0 0
26,198
Production Losses, Fe-
males ($000) (5) $
0 0 0 524 4,545 5,869 6,261 6,640 6,493 5,722 4,873 4,054 2,741 1,526 404 0
0 0 θ
0
$49,650"
Totals, All Ages, Both Sexes: Cases—78,592 Losses ( $ 0 0 0 ) — $ 1 6 5 , 8 6 0 "Items may not sum to the column totals due to rounding. Sources: Number of cases—text, above. (Some smoothing was required to bring the data into five-year age classes.) Loss figures for each age assume one year of lost production per case (see text, above); values of production in each five-year age bracket were taken (from Table 1) as of the age mid-point of the class.
resulting estimates of numbers of cases according to age and sex are in Table 9. Average duration of illness. According to Leonard A. Scheele, then Surgeon General, Public Health Service, 16 an average of "Leonard A. Scheele, " W h a t Have W e Accomplished W i t h Polio and W h a t Are the Prospects for Other Virus Diseases and Illnesses," mimeographed copy of address delivered to the Economic Club of Detroit, October 3, 1955.
77
Quantification of losses from morbidity T A B L E 9.
PRODUCTION
CAUSED
MORBIDITY,
(1)
Number of Cases, Males, 1954 (2)
0-5 5-10 10-15 15-20 20-25 25-30 30-35 35—40 ΊΟ—45 45-50 50-55 55-60 60-65 65-70 70-75 75-80
5,525 6,082 3,341 1,871 1,053 1,637 1,358 556 332 234 98 98 43 38 11 0
Age in Years
All A g e s
22,277
LOSSES E X P E C T E D YEAR
1954
CASES,
Production Losses, Males ( $ 0 0 0 ) (3) $
0 0 0 194 394 1,167 1,080 464 283 186 70 64 24 14
b
$3,940®
FROM BY
POLIOMYELITIS-
AGE
Number of Cases, Females, 1954 (4) 4,017 4,422 2,430 1,361 765 1,190 988 405 242 170 71 71 31 28 8 0 16,199
AND
SEX
Production Losses, Females ( $ 0 0 0 ) (5) $
0 0 0 171 418 734 653 284 168 108 40 36 12 7
b
$2,634°
Totals, All Ages, Both Sexes: Cases—38,476 Losses ( $ 0 0 0 ) — $ 6 , 5 7 4 " I t e m s may not sum to the column totals due to rounding. ' L e s s than $1,000. Sources: Number of cases—see text, above. (Some smoothing was required to bring the data into five-year age classes.) Loss figures for each age assume one-fourth year of lost production per case (see t e x t ) ; values of production in each five-year bracket were taken ( f r o m Table 1 ) as of the age mid-point of the class.
two-thirds of polio cases are " p a r a l y t i c , " roughly half of these " r e c o v e r completely," while another 30 per cent " r e c o v e r with no disabling e f f e c t s " ; 10 to 15 per cent of the paralytic patients are " s e v e r e l y crippled," and 5 to 15 per cent of those with paralytic polio die. H a v i n g
this information w e can compute a
weighted average period of illness once w e are also able to determine the duration of illness for those cases which are fatal, those which are non-paralytic, and those from which patients ( a )
78
Economics of Public
Health
recover "completely," (b) recover with " n o disabling effects," and (c) are left "severely crippled." Discussions with medical personnel have suggested the following periods of illness by type of case: Type of Case Non-paralytic Paralytic Complete recovery No disabling effects Severe crippling Fatal
Period of Illness Two weeks Sixty to ninety days Four months One year17 Few days
Weighting these "periods of illness" by the relative frequency of the respective case types, as indicated above in the text, we estimate the average duration of illness from all cases of poliomyelitis at one-fourth of a year. As with cancer and tuberculosis, we can at this point compute the illness-caused production losses. This is done in Table 9, for all the year 1954 cases. TREATMENT
COSTS
Cancer. Morbidity surveys of the National Cancer Institute (1950-1952) disclosed 18 that three-fourths of the diagnosed cancer cases receive hospital care, the average total length of hospital stay (first admission and readmissions) being 32 days. " . . . a typical cost figure for room and board would be close to $10 a day." 1 9 According to the Vermont Cancer Report, 40 room and board charges accounted for three-fifths of the total amount billed by hospitals. Therefore, at a daily charge of ten dollars, the total cost per hospitalized-day equals sixteen to seventeen " " O n e year" until rehabilitation; private correspondence with the National Foundation for Infantile Paralysis (dated December 26, 1956) suggested the estimate of six months hospitalization plus six months in a respiratory and rehabilitation center. »Health Inquiry, Part 1, p. 212. »Ibid., " " R e p o r t of Vermont Cancer Survey . . .," p. 8.
Quantification
of losses from morbidity
79
dollars ; for thirty-two days the total hospital cost amounts to $535. " On the basis of the schedule of fees for surgery and supporting services contained in typical Blue-Shield plans, an individual from a low or moderate income group can be expected to pay at least an additional $350 for physicians' services (diagnosis, surgery, radiation, and followup care)." 2 1 Thus, the threefourths of all cancer victims who are hospitalized paid an average of around $885 for diagnosis and treatment. The one-fourth of diagnosed cancer cases which do not require hospitalization—either not sufficiently serious to warrant hospitalization or having been discovered too late to warrant treatment—"can be fixed at $100, at least. . . . For all cancer patients, whether hospitalized or not, the cost of diagnosis and treatment would average at least $700 per patient." 2 4 At $700 per case, the 500,000 new cases in 1954 would result in treatment costs of $350,000,000! Tuberculosis. Correspondence with the National Tuberculosis Association 23 revealed an estimate for " t h e cost of treatment, including hospitalization, drugs, nursing, medical and health services . . . in the magnitude of $5,000." This includes " a year's hospitalization at $ 10 per diem and about $ l ,400 for posthospitalization medical services and drugs." At $5,000 per case, the total hospitalization and treatment costs associated with the 78,592 active or probably active cases discovered in 1954 are $392,960,000. Treatment costs, as we noted earlier, may be viewed as alternatives to mortality costs; an active case of tuberculosis which goes untreated will generally be fatal. The incurrence of treatment costs to " b u y " reduced mortality from tuberculosis appears, on the whole, to be a wise investment for society ; the "Health Inquiry, Part 1, p. 212. "Letter dated December 27, 1956.
" Ibid.
80
Economics of Public
Health
value of an average person during most of his lifetime is far greater than the $5,000 cost of preventing his death from tuberculosis. (Note Table 3.) Poliomyelitis. Costs associated with the hospitalization and treatment of polio patients are commonly considered to be mammoth. For some cases the costs may, indeed, be enormous; some patients' . . . total expenses can be broken down into (a) Care in a local hospital at $14 to $18 a day for six months, and (b) Six months in a respiratory and rehabilitation center which will cost about $28 a day plus $700-$800 for special adaptive equipment. It is not unusual for a patient in his home to have approximately $ 3 0 0 0 worth of respiratory equipment, in addition to the above.*4 Thus, costs running as high as $10,000 are not impossible. However, such large expenses are associated with only a small fraction of total polio cases—those involving "severe crippling." These most severe cases constitute only approximately 8 per cent of the total cases. At the opposite extreme of expense are the non-paralytic third of all polio cases, the "mild attacks," which may hospitalize for only a week, as well as the 5 per cent of cases which are fatal, generally killing quickly. Analysis of 24,217 bills received by the National Foundation for Infantile Paralysis in the period January-May 1953 for care of 11,666 patients showed that the ". . . average cost for treatment per patient was $629. . . ." 2 5 Medical care prices (as measured in the Consumer Price Index) rose approximately 15 per cent between 1950 and 1953. Therefore, in terms of prices as of the year 1950, the $629 figure was around $550. For the 38,476 cases of poliomyelitis reported in 1954 this would amount to $21,161,800 as the cost of treating this one year's new cases. " P r i v a t e correspondence with the National Foundation for Infantile Paralysis, dated December 26, 1956. " Health Inquiry, Part 2, p. 771.
Quantification of losses from morbidity
81
In this chapter we have estimated morbidity losses and treatment costs for each of three diseases. 2 · In the following chapter we shall bring these estimates together with those of mortality losses (made in Chapter VII), in order to compare these total costs. " T o the extent that morbidity losses and treatment costs occur over time, they should be discounted back to the date of case incidence, just as foregone future net earnings were discounted, in Chapter VII. Where morbidity losses and treatment costs are spread out over many years, the discounting becomes particularly important. However, for the diseases considered here, direct losses from morbidity and treatment begin, in general, at the time of the discovery of the case, and continue only for a period of from a few days to a year. For periods of such length it did not seem worthwhile to discount the losses; even the one-year-duration losses would only be discounted for one-half year, since, on the average, they were incurred six months from the case-discovery date.
C H A P T E R IX
Summary of quantification, and conclusions
W e have now estimated for three diseases the aggregate monetary losses due to premature mortality, morbidity, and treatment requirements for all deaths and new cases in the year 1954. These losses are summarized by diseases in Tables 10, 11, and 12. As one would have expected, cancer proves to be clearly the most costly disease of the three studied. However, considering the great amount of public concern over cancer and, at the same time, the noticeable absence of widespread concern over tuberculosis, it is interesting that the latter disease proves to have had as much as one-fourth of the economic impact of cancer in 1954. Finally, polio is shown to be responsible for only a very small fraction of the losses attributable to either cancer or tuberculosis. Also impressive are the absolute magnitudes of the losses for this one year, particularly when it is recognized that not all losses were found measurable ; cancer costs annually approximately one per cent of our entire national income! Examination of the data in Tables 10, 11, and 12 shows that the total cost of treatment of tuberculosis victims exceeds the treatment costs of polio patients sixteenfold ($393 million to $21 million); and, in fact, exceeds even the treatment costs of cancer patients ($393 million to $350 million). Table 13 presents the " T o t a l Loss" figures for each disease, the "premature-death" component being computed by using first a 10 per cent rate of discount and second a 4 per cent rate. It may be observed that the choice of a discount rate makes comparatively little difference (12%) in the aggregate tuberculosis costs. This is a consequence of the fact (shown in Table
83
Summary of quantification, and conclusions T A B L E 10.
T O T A L L O S S E S FROM C A N C E R M O R T A L I T Y IN FROM C A S E S W I T H I N C I D E N C E IN
1954
AND
1954
Amount of Loss (in millions of dollars)
Form of Loss Mortality Morbidity (Earnings L o s t ) Treatment
$1,183»
All Forms ( T o t a l )
$2,222»
$1,568*
688 350
$2,607»
» Mortality losses computed at 10 per cent discount rate, δ Mortality losses computed at 4 per cent discount rate. Items may not sum to the column totals due to rounding. Source: Tables 4 and 7, and text, Part IV.
14) that only a comparatively small proportion of tuberculosis losses are from mortality, the category affected by the discount rate. By contrast, a far greater percentage of the economic losses from cancer are the result of premature mortality; however, the high average age of cancer victims acts to reduce the loss-increasing effect of the reduction from 10 to 4 per cent of the TABLE
1 1 . T O T A L L O S S E S FROM T U B E R C U L O S I S M O R T A L I T Y IN AND FROM C A S E S W I T H I N C I D E N C E IN
1954
1954
Amount of Loss (in millions of dollars)
Form of Loss Mortality Morbidity (Earnings L o s t ) Treatment
$166«
All Forms ( T o t a l )
$724»
166 393
"Mortality losses computed at 10 per cent discount rate. b Mortality losses computed at 4 per cent discount rate. Items may not sum to the column totals due to rounding. Source: Tables 5 and 8, and text, Part IV.
$253
$8126
Economics of Public Health
84
TABLE
1 2 . T O T A L LOSSES FROM POLIOMYELITIS M O R T A L I T Y IN A N D FROM C A S E S W I T H I N C I D E N C E IN
1954
1954
Amount of Loss (in millions of dollars)
Form of Loss Mortality Morbidity (Earnings Lost) Treatment
$18«
All Forms (Total)
$46«
$44& 7 21 $71»
β Mortality losses computed at 10 per cent discount rate. & Mortality losses computed at 4 per cent discount rate. Items may not sum to the column totals due to rounding. Source: Tables 6 and 9, and text. Part IV.
discount rate—total losses increasing by some 17 per cent (Table IS). The choice of discount rate is of the greatest relative significance when the economic losses from poliomyelitis are under consideration. This is the effect of the youthfulness of the victims of this disease. Most or all of their productive lifetimes are many years in the future, and a high discount rate attaches little significance to the distant future. Total losses from polio inTABLE
1 3 . " T O T A L " ECONOMIC LOSSES FROM D E A T H S A N D N E W
CASES IN 1 9 5 4 OF C A N C E R , TUBERCULOSIS, AND P O L I O M Y E L I T I S
Total Losses (in millions of dollars), Computed at Discount Rate of: Disease 10% Cancer Tuberculosis Poliomyelitis
$2,222 724 46
Source: Tables 10, 11, and 12.
Percentage Increase, Losses Computed at 10% and 4 % Rates of Discount
4% $2,607 812 71
17 12 56
85
Summary of quantification, and conclusions
crease by more than 50 per cent when the rate of discounting future income is reduced from 10 to 4 per cent (See T a b l e 13). T a b l e 14 discloses that the principal monetary cost to society of cancer is the result of the premature mortality it causes; while the largest cost component for both tuberculosis and polio is treatment cost. For the latter t w o diseases, highly expensive methods of treatment have been employed f o r many years, 1 while the late detection and rapid development of cancers have substantially held down the treatment costs for this disease. TABLE
14. M O R T A L I T Y
LOSSES, MORBIDITY
LOSSES, A N D
TREATMENT
COSTS AS PERCENTAGES OF T O T A L LOSSES FROM CANCER, TUBERCULOSIS, AND POLIOMYELITIS, 1 9 5 4 CASES A N D DEATHS 0
F o r m of Loss, and Per Cent of T o t a l Disease
Cancer Tuberculosis Poliomyelitis
Total Losses
Mortality
Morbidity (Earnings L o s t )
100% 100% 100%
53 23 40
31 23 14
Treatment
16 54
4β
» M o r t a l i t y component of total losses computed using 10 per cent discount rate. Source: Computed f r o m data in T a b l e s 10, 11, and 12.
Our estimates of monetary losses attributable to each of the three diseases studied—cancer, tuberculosis, and poliomyelitis —indicate that the order of their importance coincides with that which a thoughtful worker in the public health area would have expected. T h i s fact, rather than implying that little has been learned f r o m our quantification efforts, should tend to increase our faith in the usefulness of the procedure, for it does not g i v e results which are in striking contrast to the judgments of experts in public health work. T h e faith w e have in the methodology ' T h e Salk vaccine promises to make most of these costs unnecessary in the case o f polio.
86
Economics of Public Health
employed in this study is of great importance, for as our methodology is extended to the quantification of losses from other diseases we may no longer find that the rankings of diseases by magnitudes of social losses correspond to our ex ante expectations. Indeed, for other diseases we may have no expectations as to their rank position. And, moreover, mere rankings based on casual opinions and hunches fail to give any information on aggregate magnitudes of losses. These may be very useful in decision-making situations in which the level, as distinguished from the allocation, of health expenditures is under scrutiny. Quantitative data on disease losses would seem to be valuable in educating a population to the importance of support for health activities. Not only may the magnitudes of social losses from the diseases studied be striking but the development of public awareness that poor health affects the living standards of many persons other than those who become ill2 may cause the population to re-evaluate its attitude toward expenditures on health. 3 W e turn now to investigate some policy implications of our data on disease-caused monetary losses (and of similar data on other diseases which may be gathered). It is interesting to compare our data on total monetary losses from cancer, tuberculosis, and poliomyelitis with figures showing the volume of grants for research on each disease, the latter appearing in Table 15. The figures in Table 15 should not be interpreted as total research expenditures on each of the diseases since all research is not financed by awards from "national granting agencies"; governments perform a good deal of direct research, as do industrial enterprises; and not all university medical research is financed • It should be recognized that our approach has been to consider real losses due to poor health—principally losses which reduce living standards; the conversion of the real losses into money terms is made to permit their addition. • D r . Henry van Zile Hyde, formerly Chief, Division of International Health, U . S. Public Health Service, has pointed out that Congress was convinced of t h e importance of malaria control with economic arguments.
Summary of quantification, and conclusions
87
directly by national awards. Thus, whereas for each of the years 1951 and 1952, Table 15 shows awards for research on tuberculosis of less than $600,000, total research expenditures on the disease in fiscal 1952 have been estimated at $4,S96,000. 4 Unfortunately, we have been unable to obtain comparable and complete figures on total research expenditures for cancer and poliomyelitis; 5 the data in Table 15 may be useful insofar as they reflect the relative research interest in each disease, even though the totals are clearly understatements of aggregate research expenditures. Ideally, research funds would be allocated in such a way as to equate expected marginal returns per dollar. Doing this requires information on program costs per unit of output (which have not been considered in this study limited to benefits); yet, given the large degree of uncertainty regarding the likelihood of success of research into the causes and cures of diseases (i.e., given the uncertainty of research costs per unit of "success"), we would certainly expect to find the rankings of the amounts of research funds allocated among diseases to be the same as the rankings of diseases by losses (Tables 13). The relatively large volume of grants for polio research disclosed in Table 15 appears to have been unwarranted. The price we may be paying for the Salk polio vaccine is the continuation of the far greater rates of sickness and premature death and greater economic losses from cancer, tuberculosis, and other diseases. Of course, our loss statistics apply only to a single year. In principle, the distribution of research funds should be made with reference to the present value of all future losses. Still, because of •Gitlin, "Tuberculosis Expenditures in Fiscal 1952," Public Health Reports, 69 (September, 1954), 797. 'Some data on research expenditures for cancer and polio have appeared in Health Inquiry, Part 1, pp. 338, 348, and Part 3, p. 771 (House of Representatives, Hearings before the Committee on Interstate and Foreign Commerce, 83rd Congress, 1st Session, U. S. Government Printing Office, Washington, D. C., 1953, 4 parts), but the estimates are not complete, and we cannot be certain that the definitions of "research" were the same for each disease, since the sources differed.
88
Economics of Public Health
TABLE 15.
A W A R D S BY N A T I O N A L G R A N T I N G A G E N C I E S FOR R E S E A R C H AND
IN
NON-GOVERNMENT
Year
1946
1947
Tuberculosis Government Non-government
$30,331 30,331
229,228 204,647 24,581
656,749 528,384 128,365
817,049 647,384 169,665
545,539 493,704 51,835
Cancer Government Non-govemment
617,918 358,392 259,526
844,654 329,415 515,239
5,021,503 1,908,171 3,113,332
6,492,101 3,051,287 3,440,814
6,722,145 3,361,072 3,361,073
Poliomyelitis Government Non-govemment
242,186
491,918
746,267
1,513,123
1,729,027
-—
—
242,186
—
491,918
194β
—
746,267
1949
—
1,513,123
1950
—
1,729,027
Source: Data for 1946-51: Stella LecheDeignan and Esther Miller, "The Support of Research in Medical and Allied Fields for the Period 1946 through 1951," Scitrue, 115, No. 2987 (March 28, 1952), 342 (Poliomyelitis and Tuberculosis data), 336 (Cancer data). The government—non-government components of cancer figures for 1946-1951 were reported as percentages of total. Data for 1952-1956: Private correspondence with Stella Leche Deignan, Director, Bio-Sciences Information Exchange, Washington 6, D. C.
the uncertainty of the future incidence of diseases (extrapolation of trend is dangerous, in part due to the improving accuracy of case reporting) and because future losses are less important the further in the future they are, the relationships among current losses from the various diseases are not entirely unreasonable bases upon which to make expenditure decisions. Conceptually, we may state the necessary and sufficient conditions for an optimum allocation of funds between any disease programs. Denoting the benefits of preventing an additional case of a disease by M B (marginal benefit); denoting the cost of preventing an additional case by M C (marginal c o s t ) ; and
Summary TUBERCULOSIS, SOURCES OF
CANCER,
AND
of quantification, POLIOMYELITIS,
and conclusions 1946-1956,
89
GOVERNMENT
AWARDS"
Year
1951
1952
1953
1954
1955
1956
387,699 355,837 31,862
576,272 398,338 177,934
553,087 320,982 232,105
539,748 340,227 199,521
622,339 421,456 200,883
591,051 428,271 162,780
6,691,440 3,278,806 3,412,634
8,309,327 4,369,981 3,939,346
10,397,088 5,800,075 4,597,013
12,165,666 7,684,935 4,480,731
15,131,752 9,544,155 5,587,597
17,809,860 10,623,194 7,186,666
2,609,304
2,744,417 6,000 2,738,417
2.022,289 35,778 1,986,511
1,920,383 60,038 1,860,345
2,176,011 46,800 2,129,211
1,962,314 39,924 1,922,390
2,609,304
a " . . . funds awarded for nonsecurity classified grant and contract research in the bio-sciences by seven government agencies (Atomic Energy Commission, Department of the Air Force, Department of the Army, Department of the Navy, National Science Foundation, Public Health Service, and Veteran's Administration) and the funds awarded by the national offices of major fund-raising organizations and by the private foundations that make awards on a nation-wide scale."—Deignan and Miller (see "Source," above), p. 661.
denoting the particular disease by subscripts 1, 2, S, . . ., n\ a given health budget will be divided optimally when®
^ >
MBi _ MB2 _ _ MCj ~ MC2 - · · · -
MB, MC„
•Such an allocation will be optimal provided (1) that the MB's are not increasing functions of the number of cases prevented (i.e., provided that benefits of preventing an additional case do not rise as more cases are prevented); and provided (2) that the MC's are not declining functions of the number of cases prevented (i.e., provided that the cost of preventing an additional case does not fall as more cases are prevented). More precisely, the requirement is that the M C functions be declining more slowly or rising more rapidly than the corresponding MB functions. These conditions are quite likely to be met in practice.
90
Economics of Public Health
What this means, simply, is that maximum total benefits will have been obtained (from the given budget) when the benefits from an additional dollar's expenditure on each disease are equal. (Or, what is equivalent, when the ratios of marginal benefits equal the corresponding ratios of marginal costs.) If the ratios were unequal, then total benefits could be increased by re-allocating expenditures, without increasing the aggregate budget. 7 The discussion above is at the theoretical level. However, results of the present study may be used to estimate the numerTABLE
16. TOTAL LOSSES PER CASE OF CANCER, TUBERCULOSIS, AND POLIOMYELITIS,
Disease
Cancer Tuberculosis Poliomyelitis
Total Losses" ($000,000) (1) $2,222 724 46
1954
Total Cases (1954 Deaths plus N e w Cases) (2) 734,669
94,984 39,844
Total Losses Per Case (3) $3,024 7,622 1,154
« Mortality losses figured at 10 per cent discount rate. Source: Column ( 1 ) — T a b l e 13. Column ( 2 ) — T a b l e s 4 - 9 .
ators of the above ratios for the three diseases studied, and our techniques may be applied to other diseases. Table 16 indicates the average total losses per case of each disease, which are, of course, the average benefits obtainable by preventing a case. In the absence of more specific information we may expect these average benefit figures to be the same as the marginal benefit , -MB. $4 ,MB. $10, , MB, MB., t , 'For example, if j ^ r = ^ a n d ^ = ^ (so t h a t - - ? * _ • ) , then the transfer of $ 4 of resources from disease 1, at a loss of $ 8 of benefits, to disease 2, at a gain of $ 1 0 benefits, would result in a net gain of $2.
Summary
of quantification,
and conclusions
91
( M B ) figures which we need. If we had advance information as to the nature of the particular cases which would be prevented— that is, information from which we could estimate benefits of prevention—we would not assume that average benefits would result. Without such data, we may reasonably use the averagebenefit figures,8 in which case the marginal ratios for cancer (c), tuberculosis ( t ) , and poliomyelitis (p) which are to be equated become· $3024 $7622 $1154 (2) MC c MC t MC p Prevention costs ( M C ) , which are likely to rise as preventive efforts are extended, remain to be estimated, but they will not be investigated in the present study. Consequently, at this stage we cannot say how a given public health budget " o u g h t " to be allocated most efficiently among the three diseases; nevertheless, the problem has been reduced to one of cost estimates.·* In Table 17 are presented hypothetical prevention-cost data for each disease. Let us take the case of a $2.5 million budget to be spent on prevention of cancer, tuberculosis, and poliomyelitis. T h e funds would be spent most efficiently (that is, •In so doing we assume that benefits remain constant as prevention expenditures change, or, at least, that the MB's maintain a constant ratio. • It is assumed here that reduction of the incidence of one disease has no effect on the incidence of other diseases; that is, we assumed that the benefit of a unit reduction in the number of cases of some disease is the loss per case prevented, as estimated above. Actually, in general, the ratio of marginal benefits ( M B , ) to marginal cost ( M C , ) of preventing a case of disease 1 is as follows: M B , _ MB,« MC, ~ MC,
+
MB, MC~,
+
MB, MC, +
·
MB„ + MC,'
where M B , · = the additional benefits obtained directly by a unit reduction in disease 1 incidence, and MB,, MB MB„ = the additional benefits obtained indirectly by the altered incidence of diseases 2, 3 η resulting from expenditures on disease 1. Where expenditures directed toward disease 1 have no external effects on inciMB MB 1 * dence of other disease, the M B „ MB,, etc. = 0 and, therefore, , = , - , as MC, MC, we have assumed. "See note on bottom of page 98.
Economics of Public Health
92
with maximum total benefits) if allocated so that the costs of preventing an additional case of each disease (the M C ' s ) were in the ratio of $S024: $7622: $1154, which is also the ratio of benefits per additional case. Doing this would lead to these expenditures: Cancer
$
900,000
Tuberculosis
1,500,000
Poliomyelitis
100,000 $2,500,000
T A B L E 17.
H Y P O T H E T I C A L C O S T S OF P R E V E N T I N G
TUBERCULOSIS,
AND
POLIOMYELITIS, CASES
AS A
A
FUNCTION
CASE
OF
CANCER,
O F T H E N U M B E R OF
PREVENTED
Hypothetical Cost of Preventing a Case of Number of Cases Prevented
(1)
Cancer
Tuberculosis
Poliomyelitis
(2)
(3)
(4)
1-1000
$200
$ 50
f 100
1001-2000
210
80
200
2001-3000 SOOl^KXX) 4001-5000 5001-6000 6001-7000 7001-8000
230 260 290 350 520 700
120 200 390 660 920 1,320
300 500 700 900 1,100 1,300
This distribution would result from carrying cancer expenditures to the $260 cost point (4,000 cases), tuberculosis expenditures to the $660 cost point (6,000 cases), and poliomyelitis expenditures to the $ 100 cost point (1,000 cases). T h e marginal cost
ratios
are
equated
with
the
$260: $660: $100 = $3024 : $7622 : $ ,„„ 10
„
.
„
·
,
,
u
marginal
benefit
ratios.
1154.10 $3024
Referring to foregoing equation ( 2 ) , we have — —
=
$7622
$1154
= ^y— .
Summary
of quantification,
and conclusions
93
If a $6 million budget were available, expenditures on cancer would be pushed to the $520 cost point (an additional 3,000 cases), tuberculosis expenditures would be increased up to the $ 1,320 cost point (an additional 2,000 cases), and poliomyelitis expenditures would be increased to the $200 cost point (an additional 1,000 cases). Again, the ratio of marginal costs, $520: $1320: $200, is made equal to the ratio of marginal benefits, $3024·: $7622 : $ 1154. Total expenditures on prevention of each disease would be as follows: Cancer Tuberculosis Poliomyelitis
$2,060,000 3,740,000 200,000 $6,000,000
It should not be inferred from our discussion that each expenditure on the improvement of health (research, disease prevention, and treatment) is or ought be directed to a single disease. Basic research may be directed fruitfully to broad problem areas such as virology or cell development, both of which relate to numerous diseases. At the same time, some health research is of a narrower, applied sort in which activities are centered on a specific disease problem—for example, empirically-based research efforts to destroy cancer cells chemically. Even when a health program involves a number of diseases^ benefit figures such as ours should be useful. In such a case, program benefits will be the sum of the benefits from reduced incidence of each of the diseases affected. Further, the usefulness of quantitative estimates of diseasecaused losses is certainly not limited to decisions involving research funds. Also, and perhaps more importantly, such data can be helpful in deciding on the amounts of funds to use in public health action programs which apply existing knowledge. As an example, to what extent should hospital facilities be con-
94
Economics of Public Health
structed for the long-term patient (such as the tubercular), and to what extent for the short-term victims of acute illnesses? Quantitative information on social losses from the various diseases should be of aid in the decision process. At this point it is worthwhile to remind ourselves that our loss figures, and therefore the resulting rankings of diseases according to monetary costs, have explicitly left out of account any non-monetary—sentimental and psychological—costs of disease, either to the victim or to others. 1 1 The pain and anxiety felt by the sick person has been omitted because we have restricted our considerations to the losses to others of a person's poor health. The psychological burden carried by the victim's friends and relatives has been neglected simply because it seems to defy monetary measurement (at least for the present); but its omission from our calculations may not be critical. The principal effect of our failure to estimate the non-monetary costs of sickness and premature death is the understatement of the grandtotal (monetary plus non-monetary) losses from each disease— an understatement of unknown magnitude. 12 However, in part our objective has been to determine the relationships between the losses from various diseases; i.e., we have tried to illustrate a method of establishing priorities among health projects. Hence, if it were the case that the omission of non-monetary variables lead to a uniform proportionate understatement of losses for each disease, then the relative losses by disease as we compute them (i.e., the ratios of monetary disease costs) would be unaffected by the inclusion or omission of "intangible," non-monetary costs of sickness and premature death. W e turn, now, to the matter of what can be said about any 11 "Non-monetary" (sometimes called "intangible") costs are those for which no satisfactory measurement scales and devices have yet been developed. Our use of the term does not imply logical impossibility of measurement, even in money terms. "TTiese non-monetary costs may be very great, but we must be cautious about accepting at face value people's statements regarding the magnitudes. T o illustrate, consider the case of a sickly old man who lives with the family of a child in an
Summary of quantification, and conclusions
95
association of non-monetary with monetary costs. In our computations, the monetary costs to society of a disease are a function of the number of cases of sickness it causes, the number of deaths attributable to it, the age distribution of its victims, and the financial cost incurred in its treatment. While by no means certain, it is not improbable that the sentimental and psychological costs of poor health are roughly directly proportional to the number of cases and the number of deaths caused by a disease. Next, consider the possible relation between the non-monetary costs of a disease and the age distribution of its victims. Casual observation has suggested and informal sampling has tended to confirm the view that the sorrow experienced by the living when a death occurs does, in general, vary somewhat with the age of the deceased. It tends to be lowest (though, perhaps, still extremely high as measured on some absolute scale) when "old age" has been reached; it tends to be comparatively low, also, for very young children; and is highest somewhere in between. Possible reasons for this pattern are not hard to discover. The death of an old person is not so unexpected, and, Even when a health program involves a number of diseases^ benefit figures such as ours should be useful. In such a case, program benefits will be the sum of the benefits from reduced incidence of each of the diseases affected. Further, the usefulness of quantitative estimates of diseasecaused losses is certainly not limited to decisions involving research funds. Also, and perhaps more importantly, such data can be helpful in deciding on the amounts of funds to use in public health action programs which apply existing knowledge. As an example, to what extent should hospital facilities be conovercrowded apartment, where he contributes to family strife and imposes a financial as well as a psychological strain on the household. His death, while being sincerely mourned, would at the same time relieve pressures on the family. In our culture the family's feeling of relief would normally be suppressed by its equally genuine feeling of sadness. Still, this suggests that, on balance, the family's valuation of the old man's presence may have been less than its outward behavior would imply.
96
Economics of Public Health
structed for the long-term patient (such as the tubercular), and to what extent for the short-term victims of acute illnesses ? Quantitative information on social losses from the various diseases should be of aid in the decision process. At this point it is worthwhile to remind ourselves that our loss figures, and therefore the resulting rankings of diseases according to monetary costs, have explicitly left out of account any non-monetary—sentimental and psychological—costs of disease, either to the victim or to others. 1 1 The pain and anxiety felt by the sick person has been omitted because we have restricted our considerations to the losses to others of a person's poor health. The psychological burden carried by the victim's friends and relatives has been neglected simply because it seems to defy monetary measurement (at least for the present); but its omission from our calculations may not be critical. The principal effect of our failure to estimate the non-monetary costs of sickness and premature death is the understatement of the grandtotal (monetary plus non-monetary) losses from each disease— an understatement of unknown magnitude. 12 However, in part our in addition, the feeling that such a person has led a " f u l l " life, watched his family grow, etc., may be influential in determining the degree of non-monetary loss experienced by those who knew him. The death of a person in the " t h i r t i e s " or early " f o r t i e s " is frequently considered to be the greatest social tragedy; at this time he is in the " p r i m e " of life, and typically has a family with youthful children. On the other hand, while the loss of a young child may be a very great loss to the family, if the sentimental attachment of a family to one of its members is 11 " N o n - m o n e t a r y " (sometimes called " i n t a n g i b l e " ) costs are those for which no satisfactory measurement scales and devices have yet been developed. Our use of the term does not imply logical impossibility of measurement, even in money terms. " T h e s e non-monetary costs may be very great, but we must be cautious about accepting at face value people's statements regarding the magnitudes. T o illustrate, consider the case of a sickly old man who lives with the family of a child in an
Summary of quantification, and conclusions
97
even partly a function of the length of the association, the infant's loss may not be felt quite so strongly as the loss of a somewhat older member. In addition, the loss of a young child may be slightly cushioned if, as is commonly the case, the parents are young enough to have another. Actually, the reasons for this apparently peaked function relating the non-monetary mortality loss to age do not concern us. What is significant is that the function would appear to be uni-modal, and that this shape and the age span at which it may reach a peak correspond roughly to the shape of the function relating monetary costs of mortality to age—the present value of net future earnings. Whether there is a cause-and-effect relationship operating may be debated; in any case, the co-variation of non-economic with economic costs of mortality (as functions of age) adds plausibility to a contention that non-monetary costs are proportional to the monetary costs we have measured. And, we repeat, insofar as this is the case, the ratios of losses by disease as computed in this study, although limited to monetary cost considerations, would be unaffected by an explicit evaluation of the psychological-sentimental costs of mortality. Even if we reject the proportionality hypothesis, we may feel quite confident that the non-monetary and the monetary costs are, at least, positively correlated—that the former costs are directly related to (but not proportional to) the number of cases of and deaths from a disease. Allowing this less restrictive assumption about the relationship between monetary and nonmonetary losses, it would ordinarily follow that our rankings of diseases according to monetary losses would not likely be altered were the non-monetary losses included.13 We cannot be entirely satisfied with an attempt to measure the results of some course of action—in this case improvement of health—which omits some of the possibly very important non-monetary and, to some extent, monetary results. The fact remains, as we stated at the outset of this study, that decisions Η
98
Economics of Public Health
are being made, by governments and private extra-market health organizations, regarding the allocation of funds to various health projects; and at present there seems to be no relvant, objective standards for choosing between projects. In this study such a standard—albeit quite imperfect—is presented, in the form of a framework for measuring the economic benefits of improvement in public health. Specifying conditions of efficient resource allocation is a major preoccupation of theoretical economics. The need to apply the analytic apparatus is particularly great in an area such as public health work in which one person's benefits simultaneously benefit others, and in which, as a result, production (research, prevention, detection, hospital facilities construction) is often carried on outside the mechanism of the free market, by governmental agencies and private foundations. Guide lines for public policy on health expenditures are vital. It is hoped that this study represents a step toward providing them. 11 It is conceivable, even with positive correlations of non-economic losses with number of deaths from a disease and with number of cases, that our rankings could be changed by an unusual sentimental-psychological (abbreviated S.-P., below) loss function. For example, if the S.-P. loss mortality function increased at an increasing rate with respect to the number of deaths, while the S.-P. loss morbidity function increased at a decreasing rate with respect to the number of cases, then two diseases, one of which ranked above the other according to monetary loss factors and which caused more morbidity but fewer deaths, might change rank positions with the addition of non-monetary factors which attached far greater significance to a death than to any non-fatal case. "[added in second printing]. In a study that I am now (1968) completing, estimates have been made of the aggregate expenditures on polio research in the U. S. through the years, and they have been related to the estimates of expected losses from polio (based on adjustments of the data in Table 16 above). The tentative results indicate that research on polio has an expected internal rate of return—in terms of losses prevented—of 5 percent or more, considering only the forms of losses estimated in this book. Thus, it would appear that polio research has been a reasonably profitable investment, even in the narrowest of terms.
APPENDICES
APPENDIX I
Consumption The basic data utilized in making the marginal consumption calculations are from the Bureau of Labor Statistics, as published in the Study of Consumer Expenditures, Incomes and Savings, Volume 1, by the University of Pennsylvania. Before describing the method employed in obtaining the data relating per-capita consumption to age, we shall stop to consider the precise definition of "consumption" used in the Bureau's figures. Current consumption expenditures include: the total cost of goods and services bought for family living during the year, whether or not all payments were made in 1950. Consumer durable goods such as automobiles and household appliances are considered as consumption items but purchases and sales of homes are treated as changes in assets. Financing charges and interest on installment and other credit purchases, shipping and delivery charges, and sales and excise taxes were included as part of the expenditure for the item to which they apply. Discounts and trade-in allowances were deducted from the gross price.1 Two things should be noted about this definition: (1) certain expenditures are included which are not for "current consumption" in the economic sense—specifically, consumer durables, the entire cost of which is counted as consumption in the year of purchase rather than counting only the amount of depreciation; (2) "consumption" for which no money expenditure is involved is not included, the "consumption" of living quarters in one's own home being a conspicuous example. The inclusion of expenditures on consumer durables in "current consumption" introduces a possible bias of consequence, since durable goods purchases tend to be high for newly formed families, and the relative frequency of family formations is itself a function of age. 1 U . S. Bureau of Labor Statistics, Summary of Family Accounts (vol. 1 of Study of Consumer Expenditures, Incomes and Savings), University of Pennsylvania, Philadelphia, 1956, p. xxix. The data are for the urban United States in 1950.
Appendix I
101
However, the seriousness of this limitation of the data is more apparent than real as a result of the fact that the consumption data is presented in ten-year age brackets. Consider the case of a family which purchases an automobile for two thousand dollars, expecting it to depreciate fully in ten years. If consumption-expenditures data were gathered for this family over each of the ten years, the automobile purchase would appear, other things being the same, as "consumpt i o n " of $2,000 in one year and zero dollars in each of the other nine. But if, as is the case for the data we use, the time span covered is not one but ten years, then the automobile appears as one $2,000 purchase in the ten-year period; this is equivalent to $200 per year, which is the actual (average) consumption (in the economic sense) of the automobile by the family. Therefore, if the span of years for which data is gathered is such that all consumer durable depreciate fully within the period—for a ten-year period, if the average life of durables ( j ) is such that 1 0 j j is an integer—the inclusion of durables in "current consumption" is perfectly satisfactory. Since all consumer durables probably do not have such average lives, the BLS data on current consumption is thereby less than ideal. T h e failure of the BLS consumption statistics to include imputed rent is a real shortcoming for one interested in aggregate real consumption. But it is not so serious a shortcoming for our purpose; we are interested not in the absolute magnitude of family consumption but in the variation of consumption with respect to a change in family size. As a result, the omission of imputed rent from the " c u r r e n t cons u m p t i o n " data is of concern to us only to the extent that its amount may be expected to change with family size. And this variation may be small or even non-existent for a change of one in family size. A family consisting of a couple with two children living in a two-bedroom apartment would be unlikely to move to a one-bedroom dwelling were any one of the four to die. Contrary cases may be easily imagined, but it seems clear that the relatively slight responsiveness of (imputed or explicit) rent to a unit change in size of family means that the omission of imputed rent from the current consumption figures would appear not to be a major limitation of the data. It should also be noted that the BLS data are of a "cross-section" sort, and this kind of data might, under certain circumstances, be
102
Economics of Public Health
quite unsatisfactory. Suppose that families, regardless of size, plan to consume and succeed in consuming all their incomes over the lifetimes of their members. 8 Suppose also that the death of a family member, while leaving family income unchanged, brings an immediate, though temporary (according to the above supposition), drop in family consumption. Consumption figures estimated from cross-section data would show family consumption at all ages of head of family to diminish with a decrease in family size, since at all ages there will be some families which have only recently been reduced in size and have not yet adjusted spending. Thus, if the unproven hypothesis is correct that all income is consumed over the lifetime of the average family, the use of crosssection data would be treacherous, although, again, the gathering of data by ten-year age classes partly overcomes the effect of any temporary drop in consumption. Closely related to this is an additional potential limitation of crosssection analysis. Family income appears to vary with family size, in general. Thus, when we focus our attention on all the families in a given income bracket we may be including some small families whose income is above what they consider as "normal," and who therefore have a temporarily low average propensity to consume, as well as some large families whose income is below what they consider "normal," and who therefore have a temporarily high average propensity to consume. To the extent that this is the case—i.e., that the "normal" or "permanent" income of a family significantly influences its current consumption—cautious use of cross-section data is again required. Also, there may be a correlation of family size with other factors influencing consumption, such as expected future income and wealth. To the extent that this is the case, the variation of family consumption with family size, which we have noted, may in reality be the result of changes in these other variables rather than changes in family size per se. Recognizing these potential limitations of the data, we felt nevertheless that they were not so serious as to suggest discarding the data. • A similar hypothesis was suggested by Franco Modigliani and Richard Brumberg (in Post-Keynesian Economics, Κ. K. Kurihara, ed., Rutgers University Press, 1954, pp. 388-436).
Appendix I
103
After explaining the technique by which we have estimated the consumption associated with an individual, we shall consider further its appropriateness. But now we proceed to describe the method of computing marginal consumption, which gave the results shown in Chart 4 and Table 18. These data, when "smoothed," were used in our computations of "present values of net future earnings" (see Tables 2 and 3 and accompanying text). Consumption in each age bracket was calculated TABLE
1 8 . MARGINAL CONSUMPTION, BY AGE
Age (in years)
Marginal Consumption
Under 6 6-16 16-18 18-25 25-35 35-45 45-55 55-65 65-75
$ 157 per year 347 562 430 533 286 396 531 498
Source: Our computations, as described in text.
as a weighted mean of the marginal consumption of persons in meanincome families 3 of all sizes; thus, formally : 4 0» =
+ £ « # + . . .
+
C\p\
where is the consumption attributable to a person of age α in a family of size n, and is the probability of a person of age a being in a family of size n. (It may be noted that there is no separate computation of consumption by sex·, the BLS data did not permit it). Actually, data limitations precluded obtaining the consumption figures for each age, as required by the formula above, so that for 'That is, families in the income bracket which included the mean income of all the sampled families in the given age (of head) class. 4 In principle this series should include all family sizes, not merely those of five or less persons. However, this was impossible because in the tabulation of the raw data an open-end, "six persons or more" class was used. In any case, thep„/>,, etc. are surely negligibly small.
104
Economics of Public Health
families of three and more, the consumption figures (the c) are averages for all ages. Thus, as finally computed, £> = r j f l +
+
+ c^pi + cbp%.
Note, however, that the p, the probabilities of a person being in a family of given size, retain their age superscripts. T h e need for comC H A R T 4.
600 η
-
M A R G I N A L C O N S U M P T I O N , BY A G E
Ln
500
L_
υ a. c. 400 Ο 4-> Q.
Ε 300 ^
c Ο
U 200 ~ro c
So k_
n 100 τ.
10
20
30
40
50
60
70
Age in Years S o u r c e : T a b l e 18. puting a mean of consumption by persons with average income and in average size families stems from the absence of mortality data classified according to family income and family size. T h e consumption figures as a function of family size (the cn for each age) were determined as follows, the approach being to find the change in total family consumption resulting from the addition (or subtraction) of a person of given age, ceteris paribus·.6 • T h e BLS data which w e used covered urban areas ( l a r g e cities, suburbs, and small cities) in the N o r t h , South, and W e s t . Data of this type are not available
Appendix I
105
cj—find the total consumption expenditures of single-person consumption units in the given age bracket in the income bracket which includes the average income of persons at that age. eg—find the difference between the total consumption expenditures in a husband-wife family and in a single-person family,® with given age of head of family and average income of families at that age. ca> c v c 6 — c o n s u m P t i o n of a person (age unspecified) in a three-person family with average income was obtained by computing the weighted-mean family consumption of all three-person families having a husband, wife, and, alternatively, a child under six years of age, six to sixteen, sixteen to eighteen, and eighteen and over. 7 These four consumption figures were weighted by the frequency with which they appeared in the (proportional) sample data to obtain a mean consumption figure for three-person (two parents and one child) families. From this was subtracted the consumption by families consisting of one parent and one child to get our estimate of the marginal consumption with respect to an adult in a three-person family ( c 3 ) . for the entire country, and so there arose the problem of which urban area to utilize, weighing the variables accuracy and bias and considering advantages gained by increasing the amount of urban data utilized against the additional computations required. It was finally decided to use the sample data for " l a r g e cities in the N o r t h " and " l a r g e cities in the South," taking a simple mean between data for each. This was the rationale: some of the income data for small cities in the North seemed, upon inspection, to be somewhat closer to independently obtained average-income data than large-city, suburban, or other small-city data. However, the size of the sample in the small cities of the North was so small that in many of the cells of cross-classified tables there were no observations, and in numerous others but one or two. T o use such data, since there were so few observations, would be to introduce considerable inaccuracy into our consumption estimates. Instead, it was decided to use data for the two classes having the largest sample sizes, which would improve the accuracy of our estimates—large cities in the North and in the South. T h e " N o r t h " statistics, appeared to be somewhat higher than that for the small northern cities, while the " S o u t h " data were somewhat lower; hence the use of the means of the two sets of data. • Obtaining marginal family consumption by comparing consumption in families of different sizes (income and age of head, constant) poses the basic question of the comparability of such families. Are η — 1 person families former π-person families; do variables other than family size change importantly with family size? Are larger families those in which frugality is valued more highly than in smaller families ? D o larger-size families consist of a greater proportion of Negroes, whose short life-expectancies may give rise to a high average propensity to consume ? These questions can only be raised here, the desire being to indicate possible defects in our approach. ' T h e BLS data were presented by these age classes.
106
Economics of Public Health
For determining the consumption attributable to the presence of a person in a four-, and in a five-person family, the process was identical with that used in the three-person case. For a family of four or five persons a weighted mean was taken of family consumption expenditures in families with average income having husband, wife, and two (three) children, where the oldest child8 was, alternatively, under six, six to sixteen, sixteen to eighteen, and eighteen and over; from this was subtracted the mean family consumption by families in the same income bracket with only one parent and two (three) children. The difference was termed the (marginal) consumption with respect to an adult in a four (five) person family. It is the increment to family consumption with respect to an increase in family size, ceteris paribus. Next we considered the ρ in our consumption formula—the probabilities of persons in each age bracket being in a family of each size. First, the mean number of adults (persons eighteen years of age and over) in families of each size was estimated from the breakdown by family types of the BLS data. For example, there were a total of 929 three-person families in large cities in the North who were surveyed. They included:9 1. 308 families consisting of husband, wife, and child under six; 2. 188 families consisting of husband, wife, and child, age six to sixteen; 3. 41 families consisting of husband, wife, and child, age sixteen to eighteen; 4. 192 families consisting of husband, wife, and "child", age eighteen and over; 5. 25 families consisting of one parent and two children; 6. 126 families consisting of three adults; 7. 49 families consisting of either one or two adults and two children or one. Groups 1, 2, and 3 contain two adults per family. Group 4 and group 6 families each contain three adults (persons age eighteen or more); group 5 families each have one adult; and group 7 families, having either one or two adults per family, may be assumed, in the absence of further information, to have an average of 1.5 adults per family. Taking a mean, we find that three-person families have an e
T h e BLS data were classified by the age of the oldest child. •According to our computations.
Appendix I
107
average of 2.28 adults per family. Assuming these to consist of males and females in approximately equal proportions, we estimated the number of adult males (or females) per three-person family as 1.14, for large Northern cities. This was done for all family sizes, for both large Northern and large Southern cities. Next, for each age bracket the number of sampled families of each size was determined, and with this information we calculated the percentage of all adult males or females in the given age bracket in families of each size. These are the/) in our consumption formula. They are functions of age, since they are functions of the relative frequencies of various family sizes, which in turn are functions of age. Having the p's and c's we are able to compute the marginal consumption of an average adult in each age bracket. The results of the computations are given in Table 18.10. The same general technique was used in determining the marginal family consumption with respect to a child (less than eighteen years of age). For children under six, consumption was estimated as the weighted-mean difference between the total consumption of families with average income consisting of husband, wife, and η children under six years ( n = 1, 2, 3), and the total consumption of families consisting of husband, wife, and η-1 children under six years, the differences being weighted by the relative frequencies of occurrence of the family sizes in the sample. In computing consumption data for children age six to sixteen, we began by finding the difference between the consumption by a husbandwife family and that of a similar husband-wife-child (age six to sixteen) family—a difference which was $436. We could not, however, proceed to find the difference in total consumption between families with two and with one child age six to sixteen, or between families with three and two children of that age, for the data were classified "Our consumption figures probably exhibit a small amount of upward bias. The reason is that the family consumption figures were reported by income brackets, and even within the one-thousand-dollar brackets there was generally a positive correlation of family size with income. However, since the increase in income with family size was small, in most cases less than one hundred dollars, it would account for only a small part of the change in family consumption expenditures recorded, and therefore would not appear to introduce a substantial bias in our results.
108
Economics of Public Health
only by age of the oldest child. W e can be rather certain that to take as the marginal family consumption with respect to a child age six to sixteen the figure $436 would be to overstate consumption, for both a priori consideration and the data for children under six suggest that the change in family consumption with respect to a first child exceeds the change with respect to a second or third. What we have done to adjust for such an overstatement is to make use of the relationship for the under-six-year-old child (for which data were more adequate), between his marginal consumption in one-child families and in families in general (with one, two or three children). This ratio had a value of 1.0/0.81. Our figures for the consumption with respect to a child age six to sixteen and one sixteen to eighteen in one-child families ($435 and $694, respectively) were divided by this factor to obtain an estimate of the consumption associated with children of these ages in families in general. The use of empirical data should involve the user in some appraisal of the closeness of the relationship between theoretical construct and observed entities. Some appraisal has been made above, but more is worthwhile here. Marginal family consumption with respect to an individual was determined as part of the task of estimating the social loss due to premature death. W e needed a measure of how much total family consumption could be expected to decrease were a particular member to die. The method employed was to compare the consumption by families similar with regard to age of head and income but differing in size. The question arises: should we expect the decrease in family consumption resulting from the subtraction of one member to be significantly different from the increase in family consumption resulting from the addition of the same member ? And if so, which have we computed, recognizing that it is the former which we want ? In the case of adults our approach was to compare the consumption by families consisting of husband, wife, and η children with the consumption by families with only one parent and η children, age and income held constant. Since the one-parent families are former twoparent families, it would seem that our method does get at the marginal consumption in the desired way, by exploring the drop in family consumption accompanying a drop in family size. Regarding the consumption by children, we are not on as safe
Appendix I
109
ground. W e estimated a child's consumption by subtracting from the consumption of a family with husband, wife, and η children the consumption of a similar family with η-1 children (with age of children specified); but here, unlike the case of adults, we are quite certain that very few families having n-1 children are former η children families. However, given the data available, we have decided to use the procedure described above, as the estimator of the consumption attributable to a child; the presumption is that this is at least an approximation of the drop in family consumption that would accompany the loss of a child. Our consumption figures (Table 18) do not show consumption changing in a "regular" pattern over the average lifetime. Therefore it may be worthwhile to attempt to explain the character of this pattern of a number of successive increases and decreases in annual marginal consumption. As evident from our explanation above, the marginal family consumption figures are probability-weighted averages. That is, the consumption figures reflect the fact that the "average" person is a composite, in the age bracket 25-35, for example, being 4.2 per cent in a one-consumer family, 25.2 per cent in a two-person family, 32.1 per cent in a three-person family, and so on, with finally, 5.7 per cent of him being in a family of six or more. With the fraction of the "average" person in various family sizes varying with age and with the marginal family consumption being a function of the size of family, it is clear that marginal family consumption in this probabilistic sense will vary with age. To understand the age pattern of marginal family consumption, which is also diagramed in Chart 4, we need to consider how, in general, three variables change with age; they are: (1) family income, (2) family size, and ( s ) age of children. We shall now attempt to explain the rather strange silhouette in Chart 4 in terms of these three variables. The purpose shall be to synthesize our concept of marginal family consumption with the more familiar one involving the imputation of consumption to particular family members. It is to be emphasized that the two approaches, while different, are by no means either necessarily unrelated or conflicting. The rising consumption from birth to age eighteen—that is, the increasing expensiveness of children as they grow older—hardly needs
110
Economics of Public Health
extended explanation for a parent; food, clothing, and recreation expenses only too clearly grow along with the child. Consequently, the death of a child would permit a rather substantial reduction in family consumption. But why a sudden drop in marginal family consumption with respect to a person beyond age eighteen ? The age range 18-25 is characteristically an age of new family formation, of children leaving their parents to form single-person consumer units or, more commonly, to be married. The significance of this fact is that the child leaves a family which has far greater income than the new one being formed -,11 and, at the same time that income is falling, children, with their attendant expenses are beginning to arrive. In the face of all this, it is not at all surprising to observe that marginal family consumption with respect to the adult declines; the financial pressures on the young family become so great that the loss of a parent would permit only a small decrease in family consumption expenditures. In the age bracket 25-35 consumption rises. While mean family size is rising to 3.07 in this age bracket (see Table 19), from the 2.38 in the "under-25" bracket, and while the children are growing—both of which lead to reduced consumption possibilities for the parents— family income is rising sharply. Median annual income of males in 1950 was around $1,600 at age 21, and more than $3,100 at age 30. This dramatic increase makes possible an increase in marginal family consumption of the parents along with that of the children. But past age 35,the rise in income is much more gradual, increasing between ages 30 and 40 only from $3,100 to $3,550. The consumption expenditures required by the increasing family size, from 3.07 at ages 25-35 to 3.50 at ages 35-45, together with the increasing costs associated with the growth of children, reduce the possibility of adult consumption more than the small income rise increases it. Again, the 11 Income per family member also drops somewhat; however, family income is more important in its influence on consumption than per capita income, because of the existence of economies of scale in consumption. The members of a large family could have as high a living standard as those in a smaller family with smaller per capita consumption expenditures, due to scale economies; one kitchen and its equipment can serve as the food-preparation center for a two- or three-person family as well as for a single person. (For other example of consumption economies of scale in family size, see S. J. Prais and H. S. Houthakker, The Analysis of Family Budgets, Cambridge University Department of Applied Economics, Cambridge, 1955, pp. 146-8;also seep. 150andTableSl for magnitudes of these scale economies.)
Appendix I
111
pressure on the only moderately rising income of the increasing size and age of children in the family has the effect of limiting the family's opportunity to reduce significantly its total consumption expenditures (or increase its saving), were an adult to die. Thus, marginal family consumption with respect to a parent declines in the age bracket 35-45. Income continues to rise until around age 50, and by age 45 mean family size is beginning to decline as children set out to form their own TABLE 19.
A V E R A G E INCOME AND FAMILY SIZE, ACCORDING TO AGE OF FAMILY HEAD
Age of Family Head (1)
Mean Family Size« (2)
Median Incomei
18-25 25-35 35-45 45-55 55-65 65-75
2.38 3.07 3.50 3.09 2.55 2.08
$2,000 3,100 3,523 3,687 3,436 2,262
(3)
«Computed from data for large cities in the North. ( U . S. Bureau of Labor Statistics, op. cit., vol. 1. b Male high-school graduates with income, 1950 ( U . S. Bureau of the Census. 17. S. Census of Population: 1950, IV, Special Reports, Part 5, Chapter B, Education, U. S. Government Printing Office, Washington, D. C., 1953, 5B-128).
families. Mean family size declines from 3.50 at ages 35-45 to 3.09 at ages 45-55; at the same time, income rises from around $3,500 to almost $3,700. From such a situation we should expect an increase in marginal family consumption of the adults. This is to observe that with the decreasing family size and somewhat increasing income, total family consumption can be maintained, but it would be distributed among a smaller number of persons. Consequently, the death of a parent, ceteris paribus, makes possible a substantial drop in total consumption by the remaining family. The rate at which children leave their parents' families increases as we get to the 55-65 age bracket; mean family size declines by 23 per cent, to 2.55 from 3.09 in the previous age class (45-55), and 3.50 in the 35-45 class. And while the decline in family size proceeds at an
112
Economics of Public Health
increasing rate, income falls but little, being $3,700 at age 50 and $3,500 at age 60, a drop of around 5 per cent. The so much more rapid decline in family size than in income permits the rise in marginal family consumption which Chart 4 discloses. This is a continuation of the increase begun in the 45-55 age bracket. By age 65 virtually all children have left their parents' families, there being only 2.08 persons per family at ages 65-75. But while family size diminishes from 2.55 at ages 55-65—a reduction of less than 20 per cent—income has tumbled from $3,500 at age 60 to $2,300 at age 70—a drop of more than 50 per cent. As a result, marginal family consumption with respect to a person in this age bracket falls; due to the great drop in family income, the death of a family member would make possible only a rather small decrease in family consumption (or a small increase in family saving). Reviewing the explanations of the marginal family consumption pattern presented in Table 18 and Chart 4, we may point out that, while not displaying neat, unimodal properties, the pattern is none the less reasonable when understood in terms of variation, with respect to age, of three variables—family income, family size, and age of children. As an additional aid to understanding the concept of marginal family consumption and its pattern for the average person, it may be helpful if we compare lifetime consumption profiles for several different hypothetical persons, at least one of whom is quite non-average. In Chart 5 are shown the marginal family consumption with respect to each of three persons going through three distinct life cycles. The person described in part A of Chart 5 grows up in a family with both parents but without siblings; he leaves the family at age eighteen, forming a single-consumer unit; marries at age twenty-one; has a child at age twenty-three and another at twenty-six; sees his children leave home when they reach twenty-one, which occurs when he reaches forty-four and forty-seven and loses his spouse at age sixty. Person Β has the same childhood as A, but, leaving home at eighteen years of age, remains a bachelor for his entire lifetime. 12 Person C, with the same childhood, lives at home until he marries at age twenty-three; has one child at age 26; sees the child set out on " I t may be pointed out that the " l a r g e " consumption figures in parts A and Β of Chart 5 reflect the high cost of living alone in urban areas.
Appendix I C H A R T 5.
MARGINAL
HYPOTHETICAL
CONSUMPTION
LIFE CYCLES
113 FOR
PERSONS
WITH
( A S D E S C R I B E D IN T E X T
A
THREE
ABOVE)
Β Marginal Con»umption/Yr. $3.500
c Marginal C o n s u m p t i o n Per Year
II 000
10
20
30
40
50
60
70
A g e in Y e a r i
his own when the parent is forty-eight (the child being twenty-two); and continues to live with spouse until both die at age seventy-five. Chart 5 illustrates how our marginal approach to consumption will give substantially different lifetime consumption profiles, depending upon the family life cycles of the individuals. Person B's consumption profile exhibits the unimodel properties which, a priori, may be most " a p p e a l i n g . " Y e t , the life cycle on which it is based is very much less common than those for either person A or C.
APPENDIX II
The value of women's household production Morbidity and premature mortality of a housewife are economic losses just as in the case of a wage earner. To be sure, market prices exist to enable us to evaluate easily the loss in the latter case; nevertheless, the difficulty of valuing the production of non-market production in the form of housewives' services does not justify an assumption that the services are valueless. We must determine the market value of housewives' services if our estimates of the monetary costs of particular diseases are to approach completeness. Studies dealing with the cost of poor health which have equated lost production with lost wages, thereby implying a zero value for household services, have in this regard substantially understated the losses involved. Although the housewife performs her duties without direct remuneration, the performance of comparable duties by housekeepers is purchasable in the market. With this in mind, the estimation of the value of women's household production, according to age, follows. Correspondence with the Illinois State Employment Service led to the estimation of the salary of housekeeper for an average family, consisting of father and two children, at around $35 per week in addition to room and board. Estimating the market value of the living quarters furnished a housekeeper at $5 per week,1 and estimating the additional cost to the family of providing meals for the housekeeper at $6 per week; 8 and adding these amounts to the $35 per week money ' T h e estimated price of an "average" room with no services provided; i.e., the opportunity cost to the family of providing a room for a housekeeper. •This was estimated as follows: from the University of Pennsylvania publication of Bureau of Labor Statistics data, in Study of Consumer Expenditures . . . (Volume III) statistics were obtained on the total expenditures for food of one-consumer units and of two-person families in the same ($3-4000) income bracket. The difference in total food expenditure may be considered the additional food cost accompanying an increase in family size. The amounts were $322 per year in large Northern cities and $291 in the large Southern cities. As a round figure, $300 per year (roughly $6 per week) was taken as the estimate of the cost to the family of providing meals for a housekeeper. Two comments on this method are in order. First, analysis of the food-expendi-
Appendix
II
115
w a g e , w e o b t a i n t h e figure of $ 4 6 p e r w e e k , o r $ 2 , 3 9 2 p e r y e a r as t h e c o s t t o a f a m i l y c o n s i s t i n g of a f a t h e r a n d t w o c h i l d r e n of r e p l a c i n g t h e h o u s e h o l d s e r v i c e s of a h o u s e w i f e - m o t h e r . O f c o u r s e , such a
figure
does n o t represent any a t t e m p t to evaluate the affections between a w o m a n and her family. B u t w h a t can b e said a b o u t t h e v a l u e of h o u s e h o l d s e r v i c e s w h e n t h e f a m i l y c o n s i s t s of o t h e r t h a n t h r e e p e r s o n s ( " r e s p o n s i b i l i t y u n i t s " — R . U . , h e n c e f o r t h ) in a d d i t i o n t o t h e h o u s e w i f e ; h o w , if a t all, d o e s t h e v a l u e of t h e s e r v i c e s v a r y w i t h t h e s i z e of f a m i l y ? W e n o w h a v e o n e p o i n t o n t h e f u n c t i o n r e l a t i n g t h e v a l u e of h o u s e h o l d s e r v i c e s ( V h ) t o t h e n u m b e r of r e s p o n s i b i l i t y u n i t s — a t R . U . = 3, F/t = $ 2 , 3 9 2 p e r y e a r . A s e c o n d p o i n t m a y be o b t a i n e d e a s i l y ; f o r R . U . = 0 (i.e., f o r a " s i n g l e " p e r s o n ) , t h e v a l u e of h o u s e h o l d s e r v i c e s p e r f o r m e d for others (services which would cease w e r e the individual t o d i e ) is c l e a r l y z e r o . A t h i r d p o i n t , a t R . U . = 1, w a s o b t a i n e d in t h i s m a n n e r : it w a s e s t i m a t e d t h a t a single man could e m p l o y a housekeeper for a p p r o x i m a t e l y f o u r h o u r s p e r d a y t o p e r f o r m all t h e h o u s e h o l d t a s k w h i c h , w e r e h e m a r r i e d , his w i f e w o u l d p e r f o r m . A t a w a g e r a t e of s e v e n t y five c e n t s p e r h o u r t h i s a m o u n t s t o s o m e $ 2 0 p e r w e e k , o r $ 1 , 0 4 0 , p e r y e a r . T h i s p o i n t , R . U . = 1 a n d Fh = $ 1 , 0 4 0 , is p l o t t e d o n C h a r t 6 , together with the other t w o points determined above. A smooth curve was then drawn, connecting the three plotted points. H a v i n g a f u n c t i o n r e l a t i n g n u m b e r of r e s p o n s i b i l i t y u n i t s t o t h e v a l u e of h o u s e h o l d s e r v i c e s , w e n e x t n e e d i n f o r m a t i o n o n t h e a v e r a g e n u m b e r of r e s p o n s i b i l i t y u n i t s b y a g e of f e m a l e . T h e n
we
could
ture data discloses that single consumers make a good deal (around two-thirds) of their food expenditures in restaurants, while for two-person families the fraction is only around two-ninths. Therefore, the single-consumer food expenditures are higher than would be the case were he to eat as frequently at home as the person in a two-person family; the result is that our $300 per year figure tends to understate the additional cost to the family of feeding an additional adult. On the other hand, there are economies of scale in the purchase and preparation of food—economies which have the effect of making the additional cost of feeding one more adult less than in proportion to the size of the family. This means that our estimating procedure, which involved the cost of feeding a second adult in a childless family, actually overstated the increase in food costs associated with a marginal person, since families typically have more than two persons. (Data insufficiencies prevented our working with larger families.) The over- and understating factors tend to cancel out.
116
Economics of Public Health
estimate the value of household services performed by an average female of any specified age. If a woman lives alone she performs no household services for others. If she lives with her husband and children she performs services for them which have considerable value—the precise value being some C H A R T 6. V A L U E OF W O M E N ' S HOUSEHOLD PRODUCTION, A C C O R D ING TO N U M B E R OF R E S P O N S I B I L I T Y
UNITS
Responsibility Units
Source: see text above. function of the number of persons (and their ages, perhaps). A woman may, of course, neither live alone nor have her own family; she may live with others—chiefly her parents. In such circumstances it is difficult to generalize about the value of her household services. At one extreme may be the woman who lives with her younger siblings, father,
Appendix
II
117
and invalid mother, and has complete responsibility for " r u n n i n g " the household. At the other extreme is the woman, possibly a widow with children, who works full time while living with her parents, her mother performing most or all household duties. Attempts to estimate the proportion of women at various ages who are in each of these family types, in order to compute the value of a woman's household services as a weighted average of her value in each type household (as we did for "consumption") were not successful. Data regarding the size and type of families in which women of various ages live could not be found. While data on the total number of women in various age classes are available and while the numbers who a r e " married," "single," " widowed," and "divorced" are known, this is not sufficient. How many of the married women at each age are childless; how many have one child ? T w o ? How many of the single women live alone; and how many live in the households of others ? Answers to such questions are badly needed but are presently not available. In general it was not possible to determine the relative numbers of women, by age, who have various numbers of responsibility units. Under these circumstances it was decided to use our figures on mean "family" size (and subtract one) by age of head of household (Table 19) as an estimate of the average number of responsibility units of a woman of given age. In our computations, one-person " f a m i l i e s " are considered; thus the rather low figures on family size reported in Table 19 (low as compared with our knowledge that the average two-or-more person families has approximately two children, making total family size around four) is not quite so surprising. The basic data are for urban areas, however, which have somewhat smaller average family sizes than are found in rural areas; this does give our family size figures and therefore our "responsibility-unit" figures (family size minus one) a low bias. Since the family-size figures are classified by age of family head, who is generally the male, and since we wish responsibility-unit data by age of female, some adjustment is imperative. Realizing that the average wife is some three years younger than her husband, what we have done is simply to lower the limits of the age classes which apply to heads of families by three years.
118
Economics of Public Health
ζ ο PL. CO Μ
OS
Q -J Ο X u ΪΛ Ο X
ζ w
S ο £ u. Ο (β w « Σ 3 Ζ
Q! ~
m
ζ I
>« Η J
Η
OS < Κ Ο
•
'
ο s a i u f i
/ j i | i q | S u o d s a y
I -ο